

Abstract
Autoimmune retinopathy (AIR) refers to a group of rare autoimmune retinal degenerative diseases presumably caused by cross-reactivity of serum autoantibodies against retinal antigens. The pathogenesis of AIR remains largely presumptive and there are a significant number of antiretinal antibodies that have been detected in association with AIR. The diagnosis of AIR is largely based on the demonstration of antiretinal antibodies in the serum along with suggestive clinical features and ancillary investigations. A high index of suspicion along with early diagnosis and treatment may play a critical role to lower the risk of irreversible immunological damage to the retinal cells in these patients. A multi-disciplinary approach for complete management and evaluation is helpful in such conditions. Various therapeutic options have been described for the treatment of AIR, though there is no consensus on standard treatment protocol.
Keywords: Autoimmune retinopathy, cancer-associated retinopathy, enolase, melanoma-associated retinopathy, recoverin
Autoimmune retinopathy (AIR) is an umbrella term for a group of rare autoimmune retinal degenerative diseases presumably caused by aberrant cross-reactivity of serum autoantibodies directed against retinal antigens. The spectrum of AIR is broad and contains various clinical entities with an overlapping clinical and immunological phenotype. Many conditions in this spectrum have common clinical features such as rapidly progressive, bilateral, painless deterioration of vision. However, despite the common features, AIR remains one of the most challenging diagnoses because of the lack of definitive tests and standardized criteria.
AIR can be broadly classified as paraneoplastic and non-paraneoplastic (npAIR). Paraneoplastic AIR includes cancer-associated retinopathy (CAR) and melanoma-associated retinopathy (MAR). npAIR represents AIR that occurs in the absence of malignancy and is a diagnosis of exclusion. In this review, we aim to discuss three primary forms, i.e., CAR, MAR, and npAIR. Throughout the review, the term AIR has been used in a generalized manner to encompass all these three clinical subtypes. AIR or retinal degeneration secondary to conditions such as retinitis pigmentosa, ocular trauma or white dot syndromes, and paraneoplastic conditions that predominantly involve the retinal pigment epithelium (RPE) such as bilateral diffuse uveal melanocytic proliferation and the optic nerve are not included in this review.
AIR was first described in 1976 by Sawyer et al. when degenerative retinopathies were diagnosed in three elderly female with bronchial carcinoma following the onset of symptoms such as transitory visual obscuration and visual field loss.[1] The term paraneoplastic retinopathy was first used by Klingele et al. in 1984.[2] In the same year, Gass described a case of MAR in a patient with cutaneous melanoma.[3] It took almost a decade from the description of the first case of AIR, to correlate the presence of serum antibodies against an antigen of molecular weight 23 kDa, named later as recoverin.[4] npAIR was first described in 1997 as AIR similar in phenotype and electrophysiology to CAR, which was by then a well-established entity.[5]
Epidemiology
There is a lack of population-based epidemiological study on AIR. AIR has been estimated to constitute less than 1% of all cases seen at a tertiary eye clinic.[6] Presumed npAIR remains the most prevalent AIR, and CAR is the most common type of paraneoplastic AIR.[7] Females are affected twice as commonly as men by CAR and npAIR, whereas MAR occurs more frequently in men.[8,9,10] The mean age of onset of AIR ranges from 55 to 65 years; patients diagnosed with npAIR are relatively younger than patients with CAR and MAR.[8,9,10] Several malignancies have been reported to be associated with CAR, and small-cell carcinoma of the lung remains the most common malignancy associated with CAR, followed by breast, uterine, ovarian, and cervical carcinoma.[11] The time interval between the diagnosis of malignancy and onset of ocular symptoms, or detection of antiretinal antibodies in serum remains variable, but usually precedes the diagnosis of malignancy.[12] There are reports of diagnosis of primary malignancy after 11 years of manifestation of anti-recoverin antibody-associated CAR.[13]
Pathogenesis
The pathogenesis of AIR remains largely presumptive because there are very few histopathological studies and animal models of the disease. The salient feature of AIR is the presence of circulating antiretinal antibodies which can target and attack certain retinal antigens. Usually, these retinal antigens are retinal proteins with immunogenic properties. AIR is believed to be triggered by the formation of antibodies against these retinal proteins. Till date, more than 17 different antiretinal antibodies have been identified.[14] Among these, two retinal proteins have been studied extensively – recoverin and enolase. Recoverin is a 23 kDa neuronal calcium-binding protein that is primarily detected in the photoreceptor cells of the eye.[15,16] Recoverin plays a key role in the inhibition of rhodopsin kinase, which regulates the phosphorylation of rhodopsin. Antibody against recoverin has been found to cause degeneration of rods and cones by apoptosis after binding with these photoreceptors.[17] Enolase is another 48 kDa glycolytic enzyme present in various tissues in the human body. In the retina, it is found in cell membranes of ganglion cells, Muller cells, rods, and cones.[6] It is not clear what triggers these antibodies to recognize retinal proteins as antigens – molecular mimicry between tumour antigens and retinal proteins can be one probable cause.[6] For example, recoverin has been found to be expressed by the tumor cells in patients with AIR.[18] An infectious etiology such as viral or bacterial infection can also act as the inciting event by triggering cross-reaction between retinal protein and bacterial/viral protein.[6] Retinal toxicity may result as these cytotoxic antibodies can induce apoptosis leading to death of the retinal cells. Almost all the retinal cell line can be affected; photoreceptors, ganglion cells, and bipolar cells are primarily affected. Caspase-dependent and intracellular calcium influx apoptotic mechanisms have been implicated in retinal damage due to AIR.[16] However, vision loss in recoverin-associated retinopathy has been observed to be more severe when compared with enolase-associated retinopathy and usually has an acute onset with relatively faster progression [Fig. 1].[6]
Figure 1.
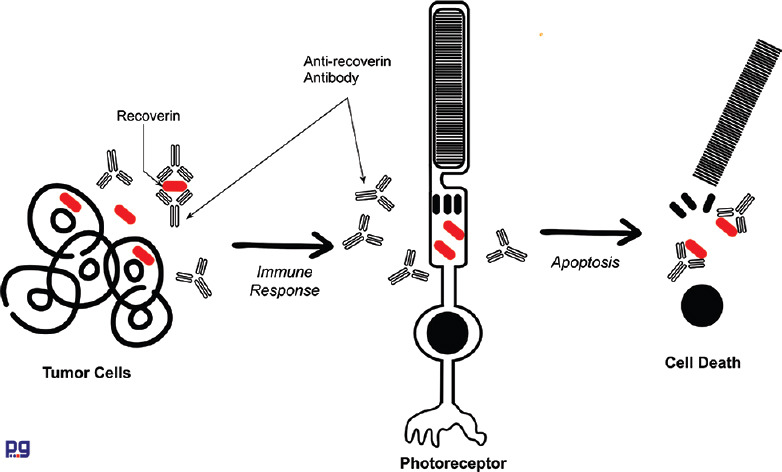
Graphical outline on proposed mechanism of autoimmune retinopathy involving anti-recovering antibody
However, many questions remain unanswered. For example, we do not know yet why selected individuals with such antibodies manifest the retinal degenerative disease whereas others do not. Normal individuals may have antiretinal antibodies which may originate due to degradation of cells, following exposure of self-antigens to the immune system.[19] In a study by Ko et al.,[20] antiretinal antibodies were detected in 42% normal healthy controls. Also, antiretinal antibodies have been detected in various systemic autoimmune diseases like Behçet's disease, systemic lupus erythematosus, and degenerative disease such as age-related macular degenerations.[16] The significance of the presence of these autoantibodies is not exactly known.
Also, it is unclear why toxicities of these retinal antibodies are only limited to the retina when retinal antigens are ubiquitous.
Clinical Course
The typical AIR patient would be an adult female in her fifth to sixth decade of life (a female predominance 63-66%) with a history of autoimmune disease,[8,21] most commonly hypothyroidism.[22] Patients with AIR typically present with bilateral (but often asymmetric) subacute vision loss, scotomas, photopsia, nyctalopia in the absence of intraocular inflammatory cells.[8,6,23] However, in the early stages of the disease, most patients' visual acuity is preserved[24] and diagnostic assessment of AIR is challenging and often delayed given its rarity and variety of clinical manifestations, including an unrevealing examination in many of the early states.[7]
When such patients present and a diagnostic suspicion arises, a family history of retinitis pigmentosa (RP) should be excluded as well as other degenerative eye diseases. Patients with RP can have similar clinical features compared to AIR and approximately 10–37% of patients with RP may have circulating antiretinal antibodies, which makes differentiating these two entities with overlapping findings and symptoms difficult.[25,26]
On examination, a subset of eyes (22%) have unremarkable fundus examination, a finding which appears to be more common early in the disease course, prior to the development of irreversible retinal and pigmentary degenerative changes [Fig. 1].[22] This might not only make the recognition of AIR more challenging but could also lead to delay in both diagnosis and initiation of systemic evaluation for autoimmune or neoplastic disease.
As might be expected for an entity with no consensus in diagnosis, retrospective studies in patients with npAIR, CAR and MAR show that clinical features vary considerably. The most common fundus findings are related to RPE changes in the form of hyperplasia, bony spicules, or atrophy. Because the RPE is a major component of the blood-retinal barrier, it contributes to immune regulation, and it is a target of the degenerative progress.[27] As such, damage to the RPE tends to mirror the processes affecting the neurosensory retina and can serve clinically as a tool for gauging the course of this condition over time. The fundus may demonstrate also retinal vascular attenuation and waxy disc pallor. Posterior pole changes do not show an association with vision.
Ancillary Investigations
The presence of autoimmune retinal antibodies is not considered a stand-alone, pathognomonic finding given that they are found in unaffected individuals as well as in patients suffering from other systemic or ocular conditions.[7] Multimodal imaging, including spectral-domain optical coherence tomography (SD-OCT) and fundus autofluorescence (FAF), can often reveal non-specific changes, especially early in the disease course.
Fundus autofluorescence imaging
Damage to the RPE is reflected in the patterns noted on FAF imaging. The majority of patients with abnormal FAF demonstrate a characteristic pattern of either diffuse or granular, stippled hyper-autofluorescence throughout the posterior pole, primarily centered in the macula and the peripapillary region. This pattern of increased autofluorescence has been shown to be a result of metabolically hyperactive RPE due to the abnormal accumulation of lipofuscin derivatives.[28] It has also been shown that hyper-autofluorescence can stem from a disrupted inner-outer segment junction and thinned outer nuclear and photoreceptor layers, which allows for increased visibility of underlying RPE autofluorescent signal.[29] Because the FAF can detect even subtle structural changes that are difficult to recognize on ophthalmoscopy, it represents an important tool in analyzing the progression of patients with AIR and should be part of the standard imaging protocol for patients with this condition [Fig. 2].
Figure 2.
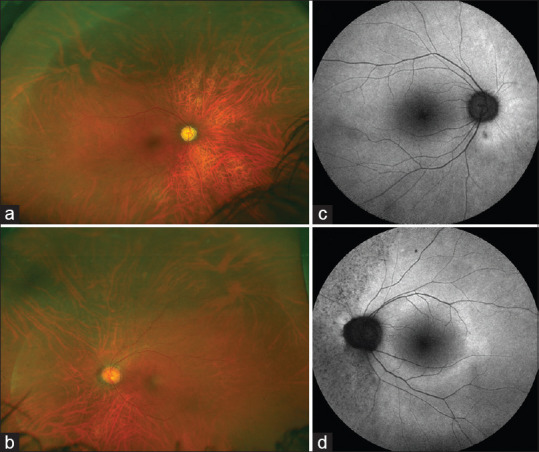
Ultra-wide field fundus imaging of a patient with autoimmune retinopathy (non-paraneoplastic subtype) in a 45-year-old female (a and b). The fundus does not show any significant clinically visible changes. The fundus autofluorescence images (c and d) show very subtle changes especially in the nasal part of the left eye (d). There are stippled areas of hypo-autofluorescence corresponding to the retinal pigment epithelial damage
Spectral-domain optical coherence tomography
SD-OCT provides objective measures of retinal damage and may offer clues toward the diagnosis of AIR [Fig. 2]. Prior studies have shown that retinal abnormalities seen on SD-OCT including loss of the outer retinal complex or disruption of the ellipsoid zone (EZ) may indicate a diagnosis of AIR before electroretinography (ERG) results and laboratory tests are available.[30,31,32,33] Lima et al. described EZ loss in four patients with AIR which corresponded to a hyper-autofluorescent ring.[32] Outer retinal abnormalities and/or decreased central macular thickness on SD-OCT were seen in all patients in a study by Abazari et al.[31] Similarly, Sepah et al. showed that patients with AIR had statistically significant loss of retinal tissue, particularly of the photoreceptor layer.[33] In the study by Khanna et al.,[22] the most common pattern of retinal damage on SD-OCT was attenuation of the outer nuclear layer (ONL) and EZ, with relative foveal preservation of the outer retinal elements.
Treatment does not appear to be associated with an increase in the anatomic extent or robustness of the EZ in any of the reports.[22,30,32,33] Because the photoreceptor outer segments can undergo renewal, it is possible that the treatment initiation and duration of the current published cases was not long enough to assess for anatomic changes on SD-OCT. All published data seem to agree that the longer time to diagnosis can lead to both visual acuity deterioration and greater reduction in the sub-foveal EZ extent on SD-OCT measurements over time[22] and the delay in diagnosis frequently reported in the literature could represent the amount of time at which regeneration of the photoreceptor outer segments cannot occur anymore.
Interestingly, though on average AIR is associated with a decrease in EZ extent over time, the integrity of the external limiting membrane (ELM) seems to predict regeneration of the EZ. Matsui et al. did demonstrate in acute zonal occult outer retinopathy (AZOOR) that at 6 months, the ELM and EZ can regenerate; however, they did not correlate their findings with treatment.[34] Other articles have shown recovery of the EZ after intravitreal injection of dexamethasone (in a patient with AZOOR) and recovery of the EZ reflectivity with difluprednate (in a patient with npAIR).[35,36] In one series, eyes where there was regeneration of the EZ had milder forms of npAIR and had intact ELMs overlying the EZ, suggesting a common pathway to other similar maculopathies.[22] This shows that in rare cases experiencing some degree of recovery, there are potentially other variables influencing this process, such as the time to diagnosis, choice and duration of treatment, and management of the associated systemic disease [Fig. 3].
Figure 3.
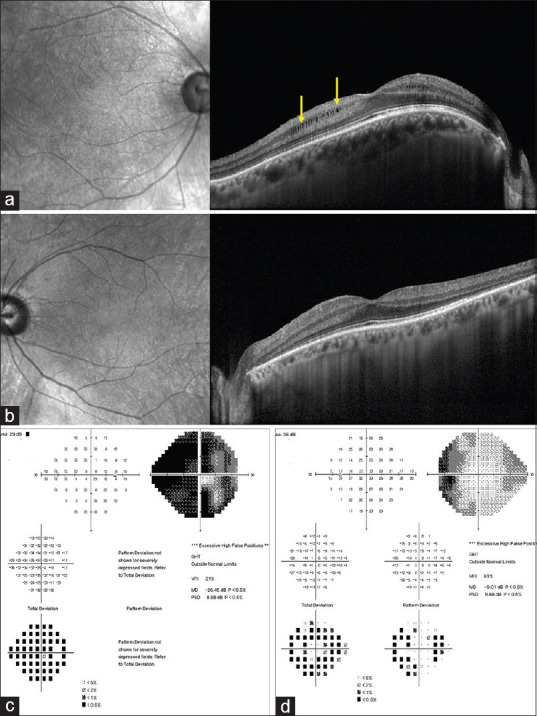
Spectral-domain optical coherence tomography (SD-OCT) of the same patient shows presence of intraretinal cystic spaces in the right eye (yellow arrows) in the perifoveal region. There is increase in the overall central macular thickness (a). The left eye shows mild increase in central retinal thickness (b). The visual field analysis (c and d) shows severe generalized field loss especially in the right eye and loss of nasal field in the left eye
These studies have shown that EZ disruption and loss on OCT is a frequent finding in AIR and one that can be both used to help diagnose and monitor disease progression. Cystoid macular edema (CME) is observed relatively frequently in eyes with AIR. In a recent abstract, Larson et al. described prevalent fundus findings among 17 patients with AIR, 13 with npAIR, and 4 with CAR/MAR. Among their patients, CME was one of the most common fundus findings, seen in 24% of eyes.[37] Similarly, Ferreyra et al. described CME as a prominent feature of patients with npAIR; 11 of 24 (45.8%) such patients had CME. However, the reported frequency of this finding in SD-OCT is quite variable and ranges from 24 to 50%.[21] In the series by Khanna, over half (66%) of the eyes had CME on presentation.[22] Antiretinal antibody testing in their study revealed a higher percentage of anti-enolase antibody and photoreceptor layer staining in eyes that developed CME compared to eyes that did not have CME. Overall, in the published studies, when CME is identified in eyes with AIR at initial presentation or when it develops subsequently, the retinal disease is more severe and more aggressive, as manifested by decreased ERG a- and b-wave amplitudes compared to eyes without CME at initial presentation.[38] Moreover, eyes with CME at initial presentation seem to have a greater rate of loss in the EZ length between baseline and final follow-up compared to eyes without CME.[22]
Visual field and electrophysiology
Visual field testing shows constriction and central or paracentral scotomas [Fig. 3].[39] There are no pathognomonic electrophysiological findings in AIR [Fig. 2]. The literature has few data and the small studies and reports of existing cases demonstrate and suggest heterogeneity in the electrophysiological features. Full-field ERG shows abnormalities and specific findings depending on the predominance of cone, rod, and other neural elements dysfunction.[25,40] There are reports with delayed b-wave, reduced amplitudes of both a- and b-waves, reduced b-wave, and an electronegative ERG, in patients with CAR.[41] CAR is typically associated with anti-recoverin antibody, and ERG in CAR typically shows involvement of cone responses.[4,42] MAR is characterized by a negative waveform on standardized full-field ERG due to reduction in b-wave amplitudes.[10] Full-field ERG was extinguished in one patient and selective b-wave loss in other patients with npAIR.[5] In one AIR series, all eyes showed abnormal findings on full fields ERG at presentation, compared to 73% of eyes with abnormal results on mf ERG.[22]
Systemic evaluation
An extensive investigation to rule out any malignancy should be undertaken in any patient that presents with clinical or imaging signs and symptoms suggestive of AIR. This investigation may be facilitated by an internist or primary care physician, who would take an inventory of the patients' history, review of systems, physical exam findings, and basic laboratory investigations in order to determine the patients' individual risk factors and, as such, determine the need to image with brain magnetic resonance imaging (MRI), chest, abdomen and pelvis computerized tomography (CT), colonoscopy and other age and gender appropriate testing such as mammogram, prostate evaluation, among others. Because of significant implications, it is important to differentiate the paraneoplastic type from the nonparaneoplastic subtype. Paraneoplastic retinopathies, similar to nonparaneoplastic, are characterized by vision loss, photopsia, nyctalopia, and scotomas with a more rapid decline. CAR is most commonly associated with small cell carcinoma of the lung, whereas MAR is commonly associated cutaneous melanoma. Therefore, examination and investigations can be directed toward these commonly encountered entities. CAR can precede the diagnosis of cancer, whereas MAR typically presents after the diagnosis of melanoma, usually metastatic melanoma.
If these features, and the circulating antiretinal antibodies are present, and if there is no malignancy at presentation or following a thorough investigation, a tentative diagnosis can be made.
Differential Diagnosis
Differential diagnosis of AIR includes white dot syndrome spectrum disorders (particularly AZOOR), retinal degenerative disorders (such as RP and cone-rod dystrophy), and non-infectious and infectious uveitis syndromes.
AZOOR can present with similar symptoms, visual field, and ERG findings. This entity is typically bilateral but can be asymmetric. Most patients either stabilize or show partial recovery without treatment. Multiple evanescent white dot syndrome (MEWDS), despite having similar symptoms, is a unilateral retinopathy which is characterized by afferent pupillary defect, optic nerve swelling, and spontaneous recovery; hence it is more readily differentiated from autoimmune retinopathy. Both AZOOR and MEWDS may show enlarged blind spot on visual fields. In addition, the majority of eyes affected by AZOOR may show characteristic and striking FAF abnormalities with well-demarcated areas of hypo-autofluorescence which have not been observed in AIR.[43,44]
Diagnostic Approaches
Diagnosis of AIR is a challenging task, relying on clinical and ERG signs of retinal damage supported by the detection of antibodies against specific retinal antigens.[14] In this setting, laboratory investigations have a significant role in the diagnosis of AIR. Antiretinal antibodies might help to gain insights into the pathogenesis of AIR and contribute to explaining the protean clinical manifestations observed. Different methods can be used to detect the presence of autoantibodies, including immunohistochemistry, Western blot, and enzyme-linked immunosorbent assay. Each method has its limitations and controls are often required to assess the reliability of the analysis. Many specific antiretinal antibodies have been identified using these techniques. However, their presence should be correlated with clinical findings and ERG. Some antiretinal antibodies might rather be an epiphenomenon, being present in different disorders and even in healthy subjects. Overall, antiretinal antibodies are more often observed in patients with a significant history of autoimmune disorders, which may predispose toward autoimmune responses.[14]
Diagnostic aspects in CAR
In CAR, a significant number of antibodies have been described. These antibodies often result from an over-expression of specific antigens by cancers, which can elicit an immune response and antibodies cross-reacting with retinal cells. Anti-recoverin antibodies are among the first described in AIR and showed evidence for their use.[45] Recoverin is a protein found in photoreceptors with calcium-binding properties. Increased expression of recoverin has been found in cancers associated with AIR, which included small cell lung cancer, breast cancer, cervical cancer, ovarian cancer, and other tumors.[14] Predisposed individuals may develop an immune response cross-reacting with recoverin photoreceptors leading to their apoptosis. When associated with tumors, the presence of anti-recoverin antibodies is suggestive of CAR.[25] However, anti-recoverin antibodies have been also found in npAIR in the absence of cancer.[42] It is difficult to assess whether these antibodies developed in the absence of tumor or after its spontaneous remission associated with the immune response. Anti-enolase antibodies are another type of antiretinal antibodies that showed sufficient evidence for their use in CAR and have been described in association with breast, prostate, and hematologic cancers among others.[14] However, they have also been detected in other autoimmune conditions not associated with cancer. Enolase presents three different isoforms (α, β, and γ) and mostly anti-α-enolase antibodies have been reported in CAR.[46] Patients with CAR and anti-enolase antibodies often show a characteristic presentation; profound abnormalities can be detected on multifocal electroretinogram, contrast-sensitivity and visual acuity, with an almost normal full-field ERG.[14] Among others, antiretinal antibodies associated with CAR, anti-TULP1 antibodies, anti-heat shock cognate protein antibodies, and anti-carbonic anhydrase II antibodies have been reported.[14]
Diagnostic aspects in MAR
In MAR, different antiretinal antibodies have been described but these should be correlated with clinical findings.[14] The majority of patients with MAR shows characteristic ERG findings with reduced B-wave and preserved dark-adapted A wave, revealing bipolar cells dysfunction similar to congenital stationary night blindness.[10] Indeed, antibodies against retinal bipolar cells have been observed using indirect immunohistochemical staining in some patients with MAR.[10] Besides, circulating anti-TRPM1 (transient receptor potential cation channel, subfamily M, member 1) antibodies were found in MAR patients. TRPM1 gene anomalies were also observed in some forms of congenital stationary night blindness and contribute to explaining some retinal similarities between these two disorders.[47,48] TRPM1 gene product is a cation channel on bipolar cells, known with the same name of the gene TRPM1, and have been found also in melanocytes where is named MART1. It is possible that uncontrolled melanocytes grow leads to MART1 overexpression and favors immune responses.
Despite the typical normal fundus appearance in MAR, other possible presentations thought to be part of its clinical spectrum include paraneoplastic vitelliform retinopathies, with multiple serous retinal detachments and vitelliform material.[49] It is not surprising that circulating autoantibodies against bestrophin-1 have been found in patients with MAR. These can show ocular findings similar to best macular dystrophy, including anomalous electrooculogram.[50] Among others, anti-aldolase A and C, anti-recoverin, anti-α-enolase, anti-transducin, anti-rhodopsin, and anti-interphotoreceptor retinoid-binding protein antibodies have been associated with MAR.[14]
Diagnostic aspects in npAIR
In npAIR, the most common subtype of AIR, different antiretinal antibodies have been reported.[14] Clinical presentation, electrophysiologic findings and antiretinal antibodies may overlap with CAR, requiring a careful interpretation. Among the other antiretinal antibodies described in association with npAIR, it is worth mentioning anti-recoverin, anti-carbonic anhydrase II, anti-α-enolase, and anti-rod transducin-α. antibodies. The onset of ocular symptoms may precede by years the diagnosis of cancer and clinicians managing npAIR should always maintain a vigilant attitude toward neoplastic disorders.
Summary of diagnosis
There are a significant number of antiretinal antibodies that have been detected in association with CAR, MAR, and npAIR. The presence of these antibodies is not diagnostic per se but should be related to a compatible clinical picture. Anti-recoverin and anti-enolase are those that showed the most significant evidence for their use in this setting.[14] Other antiretinal antibodies, including anti-retinal bipolar cells, anti- TRPM1 and anti- bestrophin-1, showed a plausible correlation with the clinical findings observed in MAR, even if the evidence supporting their use is more limited. Besides, any patients with AIR showed positivity of multiple anti-retinal antibodies, complicating the interpretation of each antibody. Standardized assay systems should be used to detect antiretinal antibodies.[51] Further studies are needed to assess the real pathogenicity of many antiretinal antibodies and their role in the development of AIR.[52]
Treatment
AIR, a systemic disease, can progress rapidly and cause diffuse retinal degeneration; hence, a high index of suspicion along with early diagnosis and treatment is critical to lower the risk of irreversible immunological damage to the retinal cells.[5,53,54,55,56,57] Early diagnosis, although difficult, carries a high visual and systemic prognostic significance. It can be a clue to early detection of metastasis in both CAR and MAR and can even precede the diagnosis of cancer.[58,59,60,61] A multi-disciplinary approach is often needed, working in association with oncology, rheumatology, dermatology, and radiology, for complete management and evaluation.
There is no standard treatment protocol currently but the various therapeutic options described for AIRs, in the previous literature[7,10,21,22,23,39,40,51,59,60,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96] are (1) immunosuppression through systemic and/or topical (intravitreal/sub-tenon/depot) corticosteroids, (2) immunomodulators like cyclosporine (calcineurin inhibitor which prevents IL-2 transcription), infliximab (anti-TNFα antibody), mycophenolate mofetil (IMP dehydrogenase inhibitor, preventing purine synthesis), azathioprine (purine antimetabolite), (3) biologics such as monoclonal antibodies like rituximab (anti-CD20 antibody), alemtuzumab (anti-CD52 antibody), ipilimumab (antagonist antibody against cytotoxic T-lymphocyte antigen-4), tocilizumab (anti-IL-6 receptor antibody), sarilumab (anti-IL-6 receptor antibody), (4) and others like intravenous immunoglobulin (IVIG), plasmapheresis. IVIG has been hypothesized to have several mechanisms of action like neutralization of autoantibodies, binding of complement components, inhibition of dendritic cells maturation, modulation of intercellular adhesion, and contribution of IgG4.[14] Antioxidant vitamins like lutein, Vitamin C, Vitamin E, and beta carotene (in non-smokers) have also been advocated to stabilize the retinal degeneration and disease course.[7,25]
Corticosteroids
Once a diagnosis of AIR is established, the best approach is to first reduce the tumor burden using chemotherapy, radiotherapy, and/or surgery[10,59,70] as indicated, in paraneoplastic retinopathies. For all cases of AIR, it is generally suggested to begin with steroids (local or systemic) and/or with antimetabolites/T-cell inhibitors, as the first or second-line treatment respectively,[21,25,51,62,63,66,73,74,79,90,92] after systemic management of the underlying autoimmune disease, if present. A short-term treatment trial with intravitreal or sub-tenon triamcinolone (40-80 mg, two injections over 8 months) has been suggested, before starting systemic steroids (60-80 mg oral prednisone daily), to both confirm the diagnosis as well as to avoid the adverse effects of treatment.[25,74,97] Intravenous methylprednisolone has been associated with more favorable outcomes than oral prednisone and has been used for the initiation of treatment.[10,64,66] A case report of CAR describing complete restoration of retinal anatomy on optical coherence tomography (OCT) and improvement in vision, has been described with repeat serial intravitreal triamcinolone injections.[74] More recently, a case report describes improvement in visual acuity, visual field, and retinal function with bilateral intravitreal sustained-release fluocinolone acetonide implant in a patient with MAR, in the absence of any systemic therapy.[90] Since AIR has an autoimmune basis, long-term treatment was initially advocated (4 months to a year or more) for both stabilization and regain of the lost visual function,[25] but there is still a controversy on the potential benefit of the same[21,69,98] and hence a prospective randomized placebo-controlled clinical trial is warranted.[51]
IVIG and plasmapheresis
IVIG and plasmapheresis have also been considered appropriate if given before the onset of irreversible neuronal degeneration.[10,51,94,14,25] The results of clinical response with IVIG are better if initiated early from the time of diagnosis, and especially in syndromes affecting the CNS. A case report describes sustained improvement in visual acuity and visual fields in a patient with CAR, with IVIG 400 mg/kg/per day for 5 days.[64] In MAR, published data have used IVIG 100 g for 2 consecutive days and then every 4 to 8 weeks documenting improved visual outcomes.[10,68] There is no standard dose recommended because of limited literature and evidence to support this as a monotherapy. Plasmapheresis, in MAR, may help to remove the anti-renal antibodies, immune complexes, and cytokines.[10] Some suggest its use only for non-responders or patients who are not eligible for other treatments.[70] Data are conflicting in regard to the benefit of plasmapheresis for npAIR.[51]
Immunosuppressive therapies and biological agents
Long-term immunosuppression with triple therapy regimen was studied in a retrospective review[21] consisting of cyclosporine (100 mg/day), azathioprine (100 mg/day), and prednisone (20-40 mg/day) was advocated to a cohort of 30 patients (6 CAR and 24 npAIR), for 3 to 89 months, along with IVIG in three patients. Treatment response was seen in 70% of patients overall, 54% npAIR patients without CME, and 73% of npAIR with CME. There were several limitations in this study design as it was retrospective with no predefined treatment protocols and the baseline characteristics were not comparable. There have been two recent case reports describing the use of anti-interleukin (IL)-6 receptor antibody for refractory CME in npAIR, both resulting in complete resolution. The first used five infusions of tocilizumab at a dose of 8 mg/kg every 4 weeks[89] and the second used four injections of subcutaneous sarilumab at a dose of 200 mg every 2 weeks.[91] MAR, generally refractory to steroids,[10] has shown to be responsive to radiotherapy and cytoreductive surgeries. For patients who cannot undergo surgeries, immunomodulatory treatment is advised.[70] A case report describes ipilimumab (antagonist antibody against cytotoxic T-lymphocyte antigen-4) to be helpful in a case of melanoma relapse, refractory to surgery and chemotherapy.[77]
Multiple case series[82,85,86] and case reports[71,75,76,80,81,87,93] in the recent years describe the potential use of rituximab for improvement in retinal anatomy, function, and an overall good response, in both CAR and npAIR. A retrospective case series of 16 AIR patients (one MAR, six CAR, and nine npAIR) who underwent treatment with rituximab, along with concomitant immunosuppressive agents (mycophenolate/cyclophosphamide/IVIG/bortezomib/topical steroids), demonstrated 77% of eyes having stable or improved visual outcomes. Two different loading regimens were used every 6 months (1) two doses of 1000 mg every alternate week (2) loading dose of 375 mg/m2 weekly for 4 weeks.[82] Another retrospective analysis of four npAIR patients suggested rituximab infusion to be useful in stabilizing the progression of retinal dysfunction.[85] Yet another case series of six patients with npAIR, who received rituximab and/or combination treatment, reported stabilization of visual acuity in two-thirds of them and overall improvement of visual fields or ERG parameters in 75% of patients.[86] The potential benefit of alemtuzumab (30 mg IV three times a week for 4 months) has also been described in a CAR patient with up to 8 years of follow-up.[67]
Unfortunately, there is no consensus and there are data suggesting no difference in the clinical outcomes of patients being treated with or without immunomodulatory therapy.[6,21,39] It is difficult to conclude the clinical effectiveness of these approaches due to overall rare incidence, small sample size, lack of randomization, delayed diagnosis, and hence worse prognosis.
The management course is also guided by follow-up testing[25,51] with ERG, visual field testing, visual acuity, OCT (especially for CME), and color vision testing, generally every 3 to 6 months but can be individualized. The role of follow-up testing with repeat serum antibodies has questionable clinical significance.[99] The response to treatment is variable and depends on a lot of factors, and generally worse response have been reported in patients with family history of autoimmune diseases.[25] The patient should be counselled for the prognosis and treatment expectations aiming stabilization or prevention of further deterioration of vision.
Conclusion
A high index of suspicion along with early diagnosis and treatment may play a critical role to lower the risk of irreversible immunological damage to the retinal cells in patients with AIR. A multi-disciplinary approach for complete management and evaluation is helpful in such conditions. Various therapeutic options have been described for the treatment of AIR, though there is no consensus on standard treatment protocol.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Sawyer RA, Selhorst JB, Zimmerman LE, Hoyt WF. Blindness caused by photoreceptor degeneration as a remote effect of cancer. Am J Ophthalmol. 1976;81:606–13. doi: 10.1016/0002-9394(76)90125-2. [DOI] [PubMed] [Google Scholar]
- 2.Klingele TG, Burde RM, Rappazzo JA, Isserman MJ, Burgess D, Kantor O. Paraneoplastic retinopathy. J Clin Neuroophthalmol. 1984;4:239–45. [PubMed] [Google Scholar]
- 3.Gass J. Acute Vogt-Koyonagi-Harada-like Syndrome Occuring in a Patient with Metastatic Cutaneous. Melanoma Amsterdam, Netherland. 1984 [Google Scholar]
- 4.Thirkill CE, Roth AM, Keltner JL. Cancer-associated retinopathy. Arch Ophthalmol Chic Ill. 1960;1987(105):372–5. doi: 10.1001/archopht.1987.01060030092033. [DOI] [PubMed] [Google Scholar]
- 5.Mizener JB, Kimura AE, Adamus G, Thirkill CE, Goeken JA, Kardon RH. Autoimmune retinopathy in the absence of cancer. Am J Ophthalmol. 1997;123:607–18. doi: 10.1016/s0002-9394(14)71073-6. [DOI] [PubMed] [Google Scholar]
- 6.Grange L, Dalal M, Nussenblatt RB, Sen HN. Autoimmune retinopathy. Am J Ophthalmol. 2014;157:266–72e1. doi: 10.1016/j.ajo.2013.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Canamary AM, Takahashi WY, Sallum JMF. Autoimmune retinopathy: A review? Int J Retina Vitr. 2018;4:1. doi: 10.1186/s40942-017-0104-9. doi: 10.1186/s40942-017-0104-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Adamus G, Ren G, Weleber RG. Autoantibodies against retinal proteins in paraneoplastic and autoimmune retinopathy? BMC Ophthalmol. 2004;4:5. doi: 10.1186/1471-2415-4-5. doi: 10.1186/1471-2415-4- [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Adamus G. Autoantibody targets and their cancer relationship in the pathogenicity of paraneoplastic retinopathy. Autoimmun Rev. 2009;8:410–4. doi: 10.1016/j.autrev.2009.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Keltner JL, Thirkill CE, Yip PT. Clinical and immunologic characteristics of melanoma-associated retinopathy syndrome: Eleven new cases and a review of 51 previously published cases. J Neuroophthalmol. 2001;21:173–87. doi: 10.1097/00041327-200109000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Dot C, Guigay J, Adamus G. Anti-alpha-enolase antibodies in cancer-associated retinopathy with small cell carcinoma of the lung. Am J Ophthalmol. 2005;139:746–7. doi: 10.1016/j.ajo.2004.10.044. [DOI] [PubMed] [Google Scholar]
- 12.Adamus G, Aptsiauri N, Guy J, Heckenlively J, Flannery J, Hargrave PA. The occurrence of serum autoantibodies against enolase in cancer-associated retinopathy. Clin Immunol Immunopathol. 1996;78:120–9. doi: 10.1006/clin.1996.0021. [DOI] [PubMed] [Google Scholar]
- 13.Saito W, Kase S, Ohguro H, Furudate N, Ohno S. Slowly progressive cancer-associated retinopathy. Arch Ophthalmol Chic Ill. 1960;2007(125):1431–3. doi: 10.1001/archopht.125.10.1431. [DOI] [PubMed] [Google Scholar]
- 14.Grewal DS, Fishman GA, Jampol LM. Autoimmune retinopathy and antiretinal antibodies: A review. Retina. 2014;34:827–45. doi: 10.1097/IAE.0000000000000119. [DOI] [PubMed] [Google Scholar]
- 15.Braithwaite T, Holder GE, Lee RWJ, Plant GT, Tufail A. Diagnostic features of the autoimmune retinopathies. Autoimmun Rev. 2014;13:534–8. doi: 10.1016/j.autrev.2014.01.039. [DOI] [PubMed] [Google Scholar]
- 16.Forooghian F, Cao S, Cui J, Matsubara JA. The enigma of autoimmune retinopathy. Int Ophthalmol Clin. 2015;55:81–91. doi: 10.1097/IIO.0000000000000063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hooks JJ, Tso MOM, Detrick B. Retinopathies Associated with Antiretinal Antibodies. Clin Diagn Lab Immunol. 2001;8:853–8. doi: 10.1128/CDLI.8.5.853-858.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Polans AS, Witkowska D, Haley TL, Amundson D, Baizer L, Adamus G. Recoverin, a photoreceptor-specific calcium-binding protein, is expressed by the tumor of a patient with cancer-associated retinopathy. Proc Natl Acad Sci U S A. 1995;92:9176–80. doi: 10.1073/pnas.92.20.9176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shimazaki K, Jirawuthiworavong GV, Heckenlively JR, Gordon LK. Frequency of anti-retinal antibodies in normal human serum. J Neuro-Ophthalmol Off J North Am Neuro-Ophthalmol Soc. 2008;28:5–11. doi: 10.1097/WNO.0b013e318167549f. [DOI] [PubMed] [Google Scholar]
- 20.Ko AC, Brinton JP, Mahajan VB, Zimmerman B, Brinton GS, Stone EM, et al. Seroreactivity against aqueous-soluble and detergent-soluble retinal proteins in posterior uveitis. Arch Ophthalmol Chic Ill. 1960;2011(129):415–20. doi: 10.1001/archophthalmol.2011.65. [DOI] [PubMed] [Google Scholar]
- 21.Ferreyra HA, Jayasundera T, Khan NW, He S, Lu Y, Heckenlively JR. Management of autoimmune retinopathies with immunosuppression. Arch Ophthalmol. 2009;127:390–7. doi: 10.1001/archophthalmol.2009.24. [DOI] [PubMed] [Google Scholar]
- 22.Khanna S, Martins A, Oakey Z, Mititelu M. Non-paraneoplastic autoimmune retinopathy: Multimodal testing characteristics of 13 cases. J Ophthalmic Inflamm Infect. 2019;9:6. doi: 10.1186/s12348-019-0171-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chan JW. Paraneoplastic retinopathies and optic neuropathies. Surv Ophthalmol. 2003;48:12–38. doi: 10.1016/s0039-6257(02)00416-2. [DOI] [PubMed] [Google Scholar]
- 24.Gass JD, Agarwal A, Scott IU. Acute zonal occult outer retinopathy: A long-term follow-up study. Am J Ophthalmol. 2002;134:329–39. doi: 10.1016/s0002-9394(02)01640-9. [DOI] [PubMed] [Google Scholar]
- 25.Heckenlively JR, Ferreyra HA. Autoimmune retinopathy: A review and summary. Semin Immunopathol. 2008;30:127–34. doi: 10.1007/s00281-008-0114-7. [DOI] [PubMed] [Google Scholar]
- 26.Heckenlively JR, Aptsiauri N, Nusinowitz S, Peng C, Hargrave PA. Investigations of antiretinal antibodies in pigmentary retinopathy and other retinal degenerations. Trans Am Ophthalmol Soc. 1996;94:179. [PMC free article] [PubMed] [Google Scholar]
- 27.Detrick B, Hooks JJ. Immune regulation in the retina. Immunol Res. 2010;47:153–61. doi: 10.1007/s12026-009-8146-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mititelu M, Wong BJ, Brenner M, Bryar PJ, Jampol LM, Fawzi AA. Progression of hydroxychloroquine toxic effects after drug therapy cessation: New evidence from multimodal imaging. JAMA Ophthalmol. 2013;131:1187–97. doi: 10.1001/jamaophthalmol.2013.4244. [DOI] [PubMed] [Google Scholar]
- 29.Holz F, Spaide R, Bird AC, Schmitz-Valckenberg S, editors. Atlas of Fundus Autofluorscence Imaging. Berlin, Heidelberg: Springer; 2007. Autofluorescence from the outer retina and subretinal space [Internet] pp. 241–311. Available from: https://doi.org/10.1007/978-3-540-71994-6_17 . Last cited on 2020 Mar 28. [Google Scholar]
- 30.Pepple KL, Cusick M, Jaffe GJ, Mruthyunjaya P. SD-OCT and autofluorescence characteristics of autoimmune retinopathy. Br J Ophthalmol. 2013;97:139–44. doi: 10.1136/bjophthalmol-2012-302524. [DOI] [PubMed] [Google Scholar]
- 31.Abazari A, Allam SS, Adamus G, Ghazi NG. Optical coherence tomography findings in autoimmune retinopathy. Am J Ophthalmol. 2012;153:750–6, 756e1. doi: 10.1016/j.ajo.2011.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lima LH, Greenberg JP, Greenstein VC, Smith RT, Sallum JM, Thirkill C, et al. Hyperautofluorescent ring in autoimmune retinopathy. Retina Phila Pa. 2012;32:1385–94. doi: 10.1097/IAE.0b013e3182398107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sepah YJ, Sadiq MA, Hassan M, Hanout M, Soliman M, Agarwal A, et al. Assessment of retinal structural and functional characteristics in eyes with autoimmune retinopathy. Curr Mol Med. 2015;15:578–86. doi: 10.2174/1566524015666150731104626. [DOI] [PubMed] [Google Scholar]
- 34.Matsui Y, Matsubara H, Ueno S, Ito Y, Terasaki H, Kondo M. Changes in outer retinal microstructures during six month period in eyes with acute zonal occult outer retinopathy-complex. PLoS One. 2014;9:e110592. doi: 10.1371/journal.pone.0110592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kuo YC, Chen N, Tsai RK. Acute Zonal Occult Outer Retinopathy (AZOOR): A case report of vision improvement after intravitreal injection of Ozurdex. BMC Ophthalmol. 2017;17:236. doi: 10.1186/s12886-017-0638-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Irizarry FJ, Kopplin LJ, Salek SS, Adamus G, Saleh M, Biggee K, et al. Recovery of outer retinal laminations on optical coherence tomography after treatment of cancer associated retinopathy. Am J Ophthalmol Case Rep. 2017;8:11–3. doi: 10.1016/j.ajoc.2017.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Autoimmune Retinopathy: Prognosis and Treatment | IOVS | ARVO Journals [Internet] Available from: https://iovsarvojournalsorg/articl easpxarticleid=2374977 . Last cited on 2020 Mar 28.
- 38.Finn AP, Thomas AS, Stinnett SS, Keenan RT, Grewal DS, Jaffe GJ. The role of cystoid macular edema as a marker in the progression of non-paraneoplastic autoimmune retinopathy. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2018;256:1867–73. doi: 10.1007/s00417-018-4084-8. [DOI] [PubMed] [Google Scholar]
- 39.Braithwaite T, Vugler A, Tufail A. Autoimmune retinopathy. Ophthalmologica. 2012;228:131–42. doi: 10.1159/000338240. [DOI] [PubMed] [Google Scholar]
- 40.Rahimy E, Sarraf D. Paraneoplastic and non-paraneoplastic retinopathy and optic neuropathy: Evaluation and management. Surv Ophthalmol. 2013;58:430–58. doi: 10.1016/j.survophthal.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 41.Link B, Schlötzer-Schrehardt U, Jünemann A. Carcinoma-associated retinopathy-an electrophysiological and immunohistochemical correlation. Retina Phila Pa. 2009;29:69–72. doi: 10.1097/IAE.0b013e3181853d06. [DOI] [PubMed] [Google Scholar]
- 42.Whitcup SM, Vistica BP, Milam AH, Nussenblatt RB, Gery I. Recoverin-associated retinopathy: A clinically and immunologically distinctive disease. Am J Ophthalmol. 1998;126:230–7. doi: 10.1016/s0002-9394(98)00149-4. [DOI] [PubMed] [Google Scholar]
- 43.Fujiwara T, Imamura Y, Giovinazzo VJ, Spaide RF. Fundus autofluorescence and optical coherence tomographic findings in acute zonal occult outer retinopathy. Retina Phila Pa. 2010;30:1206–16. doi: 10.1097/IAE.0b013e3181e097f0. [DOI] [PubMed] [Google Scholar]
- 44.Yeh S, Forooghian F, Wong WT, Faia LJ, Cukras C, Lew JC, et al. Fundus autofluorescence imaging of the white dot syndromes. Arch Ophthalmol Chic Ill. 1960;2010(128):46–56. doi: 10.1001/archophthalmol.2009.368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Polans AS, Burton MD, Haley TL, Crabb JW, Palczewski K. Recoverin, but not visinin, is an autoantigen in the human retina identified with a cancer-associated retinopathy. Invest Ophthalmol Vis Sci. 1993;34:81–90. [PubMed] [Google Scholar]
- 46.Magrys A, Anekonda T, Ren G, Adamus G. The role of anti-alpha-enolase autoantibodies in pathogenicity of autoimmune-mediated retinopathy. J Clin Immunol. 2007;27:181–92. doi: 10.1007/s10875-006-9065-8. [DOI] [PubMed] [Google Scholar]
- 47.Nakamura M, Sanuki R, Yasuma TR, Onishi A, Nishiguchi KM, Koike C, et al. TRPM1 mutations are associated with the complete form of congenital stationary night blindness. Mol Vis. 2010;16:425–37. [PMC free article] [PubMed] [Google Scholar]
- 48.Dhingra A, Fina ME, Neinstein A, Ramsey DJ, Xu Y, Fishman GA, et al. Autoantibodies in melanoma-associated retinopathy target TRPM1 cation channels of retinal ON bipolar cells. J Neurosci. 2011;31:3962–7. doi: 10.1523/JNEUROSCI.6007-10.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Nieuwendijk TJP, Hooymans JMM. Paraneoplastic vitelliform retinopathy associated with metastatic choroidal melanoma. Eye Lond Engl. 2007;21:1436–7. doi: 10.1038/sj.eye.6702949. [DOI] [PubMed] [Google Scholar]
- 50.Eksandh L, Adamus G, Mosgrove L, Andréasson S. Autoantibodies against bestrophin in a patient with vitelliform paraneoplastic retinopathy and a metastatic choroidal malignant melanoma. Arch Ophthalmol Chic Ill. 1960;2008(126):432–5. doi: 10.1001/archopht.126.3.432. [DOI] [PubMed] [Google Scholar]
- 51.Fox AR, Gordon LK, Heckenlively JR, Davis JL, Goldstein DA, Lowder CY, et al. Consensus on the diagnosis and management of nonparaneoplastic autoimmune retinopathy using a modified Delphi approach. Am J Ophthalmol. 2016;168:183–90. doi: 10.1016/j.ajo.2016.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Adamus G. Are anti-retinal autoantibodies a cause or a consequence of retinal degeneration in autoimmune retinopathies? Front Immunol. 2018;9:765. doi: 10.3389/fimmu.2018.00765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Milam AH, Saari JC, Jacobson SG, Lubinski WP, Feun LG, Alexander KR. Autoantibodies against retinal bipolar cells in cutaneous melanoma- associated retinopathy. Invest Ophthalmol Vis Sci. 1993;34:91–100. [PubMed] [Google Scholar]
- 54.Adamus G, Guy J, Schmied JL, Arendt A, Hargrave PA. Role of anti-recoverin autoantibodies in cancer-associated retinopathy. Invest Ophthalmol Vis Sci. 1993;34:2626–33. [PubMed] [Google Scholar]
- 55.Weinstein JM, Kelman SE, Bresnick GH, Kornguth SE. Paraneoplastic retinopathy associated with andretinal bipolar cell antibodies in cutaneous malignant melanoma. Ophthalmology. 1994;101:1236–43. doi: 10.1016/s0161-6420(94)31183-3. [DOI] [PubMed] [Google Scholar]
- 56.Heckenlively JR. Autoimmune retinopathy: Patients with antirecoverin immunoreactivity and panretinal degeneration. Arch Ophthalmol. 2000;118:1525–33. doi: 10.1001/archopht.118.11.1525. [DOI] [PubMed] [Google Scholar]
- 57.Adamus G. Antirecoverin antibodies and autoimmune retinopathy. Arch Ophthalmol. 2000;118:1577–8. doi: 10.1001/archopht.118.11.1577. [DOI] [PubMed] [Google Scholar]
- 58.Scott CL, Cher LM, O'Day J. Cancer associated retinopathy and non-small cell lung cancer. J Clin Neurosci. 1997;4:355–7. doi: 10.1016/s0967-5868(97)90106-5. [DOI] [PubMed] [Google Scholar]
- 59.Stead RE, Fox MA, Staples E, Lim CS. Delayed presentation of melanoma-associated retinopathy and subsequent resolution with cytoreduction surgery. Doc Ophthalmol. 2013;127:165–71. doi: 10.1007/s10633-013-9398-6. [DOI] [PubMed] [Google Scholar]
- 60.Hoogewoud F, Butori P, Blanche P, Brézin AP. Cancer-associated retinopathy preceding the diagnosis of cancer. BMC Ophthalmol. 2018;18:1–5. doi: 10.1186/s12886-018-0948-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Elsheikh S, Gurney SP, Burdon MA. Melanoma-associated retinopathy. Clin Exp Dermatol. 2020:147–52. doi: 10.1111/ced.14095. [DOI] [PubMed] [Google Scholar]
- 62.Keltner JL. Management and monitoring of cancer-associated retinopathy. Arch Ophthalmol. 1992;110:48–53. doi: 10.1001/archopht.1992.01080130050025. [DOI] [PubMed] [Google Scholar]
- 63.Ohnishi Y, Ohara S, Sakamoto T, Kohno T, Nakao F. Cancer-associated retinopathy with retinal phlebitis. Br J Ophthalmol. 1993;77:795–8. doi: 10.1136/bjo.77.12.795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Guy J, Aptsiauri N. Treatment of paraneoplastic visual loss with intravenous immunoglobulin: Report of 3 cases. Arch Ophthalmol. 1999;117:471–7. doi: 10.1001/archopht.117.4.471. [DOI] [PubMed] [Google Scholar]
- 65.Katsuta H, Okada M, Nakauchi T, Takahashi Y, Yamao S, Uchida S. Cancer-associated retinopathy associated with invasive thymoma. Am J Ophthalmol. 2002;134:383–9. doi: 10.1016/s0002-9394(02)01598-2. [DOI] [PubMed] [Google Scholar]
- 66.Jacobzone C, Cochard-Marianowski C, Kupfer I, Bettembourg S, Dordain Y, Misery L, et al. Corticosteroid treatment for melanoma-associated retinopathy. Arch Dermatol. 2004;140:1258–61. doi: 10.1001/archderm.140.10.1258. [DOI] [PubMed] [Google Scholar]
- 67.Espandar L, O'Brien S, Thirkill C, Lubecki LA, Esmaeli B. Successful treatment of cancer-associated retinopathy with alemtuzumab. J Neurooncol. 2007;83:295–302. doi: 10.1007/s11060-006-9326-7. [DOI] [PubMed] [Google Scholar]
- 68.Subhadra C, Dudek AZ, Rath PP, Lee MS. Improvement in visual fields in a patient with melanoma-associated retinopathy treated with intravenous immunoglobulin. J Neuroophthalmol. 2008;28:23–6. doi: 10.1097/WNO.0b013e31816754c4. [DOI] [PubMed] [Google Scholar]
- 69.Jampol LM, Fishman GA. Immunosuppression for autoimmune retinopathy. Arch Ophthalmol. 2009;127:573–5. doi: 10.1001/archophthalmol.2009.51. [DOI] [PubMed] [Google Scholar]
- 70.Powell SF, Dudek AZ. Treatment of melanoma-associated retinopathy. Curr Treat Options Neurol. 2010;12:54–63. doi: 10.1007/s11940-009-0057-x. [DOI] [PubMed] [Google Scholar]
- 71.Mahdi N, Faia LJ, Goodwin J, Nussenblatt RB, Nida Sen H. A case of autoimmune retinopathy associated with thyroid carcinoma. Ocul Immunol Inflamm. 2010;18:322–3. doi: 10.3109/09273941003802379. [DOI] [PubMed] [Google Scholar]
- 72.Shildkrot Y, Sobrin L, Gragoudas ES. Cancer-associated retinopathy: Update on pathogenesis and therapy. Semin Ophthalmol. 2011;26:321–8. doi: 10.3109/08820538.2011.588657. [DOI] [PubMed] [Google Scholar]
- 73.Sakamori Y, Kim YH, Okuda C, Togashi Y, Kinose D, Masago K, et al. Two cases of cancer-associated retinopathy combined with small-cell lung cancer. Jpn J Clin Oncol. 2011;41:669–73. doi: 10.1093/jjco/hyr025. [DOI] [PubMed] [Google Scholar]
- 74.Huynh N, Shildkrot Y, Lobo AM, Sobrin L. Intravitreal triamcinolone for cancer-associated retinopathy refractory to systemic therapy. J Ophthalmic Inflamm Infect. 2012;2:169–71. doi: 10.1007/s12348-012-0067-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Dy I, Chintapatla R, Preeshagul I, Becker D. Treatment of cancer-associated retinopathy with rituximab. JNCCN J Natl Compr Cancer Netw. 2013;11:1320–4. doi: 10.6004/jnccn.2013.0156. [DOI] [PubMed] [Google Scholar]
- 76.Or C, Collins DR, Merkur AB, Wang Y, Chan CC, Forooghian F. Intravenous rituximab for the treatment of cancer-associated retinopathy. Can J Ophthalmol. 2013;48:35–8. doi: 10.1016/j.jcjo.2012.11.010. [DOI] [PubMed] [Google Scholar]
- 77.Audemard A, De Raucourt S, Miocque S, Comoz F, Giraud JM, Dreno B, et al. Melanoma-associated retinopathy treated with ipilimumab therapy. Dermatology. 2013;227:146–9. doi: 10.1159/000353408. [DOI] [PubMed] [Google Scholar]
- 78.Lin CJ, Chen SN, Hwang JF, Tseng CC, Li KH. Nonparaneoplastic autoimmune retinopathy presenting with peripheral retinal vasoocclusion: Case report. Retin Cases Brief Rep. 2013;7:41–5. doi: 10.1097/ICB.0b013e3182618d55. [DOI] [PubMed] [Google Scholar]
- 79.Bursztyn LLCD, Belrose JC, Coupland SG, Fraser JA, Proulx AA. Remission of nonparaneoplastic autoimmune retinopathy after minimal steroid treatment. Retin Cases Brief Rep. 2015;9:173–6. doi: 10.1097/ICB.0000000000000131. [DOI] [PubMed] [Google Scholar]
- 80.Fox A, Jeffrey B, Hasni S, Nussenblatt R, Sen HN. Rituximab treatment for nonparaneoplastic autoimmune retinopathy. Can J Ophthalmol. 2015;50:e101–4. doi: 10.1016/j.jcjo.2015.08.009. [DOI] [PubMed] [Google Scholar]
- 81.Uludag G, Onal S, Arf S, Sayman Muslubas I, Selcukbiricik F, Koc Akbay A, et al. Electroretinographic improvement after rituximab therapy in a patient with autoimmune retinopathy. Am J Ophthalmol Case Rep. 2016;2:4–7. doi: 10.1016/j.ajoc.2016.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Davoudi S, Ebrahimiadib N, Yasa C, Sevgi DD, Roohipoor R, Papavasilieou E, et al. Outcomes in autoimmune retinopathy patients treated with rituximab. Am J Ophthalmol. 2017;180:124–32. doi: 10.1016/j.ajo.2017.04.019. [DOI] [PubMed] [Google Scholar]
- 83.Sen HN, Grange L, Akanda M, Fox A. Autoimmune retinopathy: Current concepts and practices (An American Ophthalmological Society thesis) by H. Nida Sen MD MHSc, Landon Grange MD, Marib Akanda BS, and Austin Fox MD. Trans Am Ophthalmol Soc. 2017;115:1–13. [PMC free article] [PubMed] [Google Scholar]
- 84.Sierpina DI, Skale DM, Fan JT. Effect of plasmapheresis and passage of anti-retinal antibodies through the placenta in a case of non-paraneoplastic autoimmune retinopathy. Retin Cases Brief Rep. 2017;11:S34–7. doi: 10.1097/ICB.0000000000000395. [DOI] [PubMed] [Google Scholar]
- 85.Boudreault K, Justus S, Sengillo JD, Schuerch K, Lee W, Cabral T, et al. Efficacy of rituximab in non-paraneoplastic autoimmune retinopathy. Orphanet J Rare Dis. 2017;12:1–15. doi: 10.1186/s13023-017-0680-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Maleki A, Lamba N, Ma L, Lee S, Schmidt A, Foster CS. Rituximab as a monotherapy or in combination therapy for the treatment of non-paraneoplastic autoimmune retinopathy. Clin Ophthalmol. 2017;11:377–85. doi: 10.2147/OPTH.S120162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Roels D, Ueno S, Talianu CD, Draganova D, Kondo M, Leroy BP. Unilateral cancer-associated retinopathy: Diagnosis, serology and treatment. Doc Ophthalmol. 2017;135:233–40. doi: 10.1007/s10633-017-9605-y. [DOI] [PubMed] [Google Scholar]
- 88.Forooghian F, MacDonald IM. Rituximab for the Treatment of Autoimmune Retinopathy. Am J Ophthalmol. 2017;180:xv–xvi. doi: 10.1016/j.ajo.2017.06.006. [DOI] [PubMed] [Google Scholar]
- 89.Finn AP, Keenan RT, Jaffe GJ. Reconstitution of the ellipsoid zone with tocilizumab in autoimmune retinopathy. Retin Cases Brief Rep. 2018 doi: 10.1097/ICB.0000000000000766. doi: 101097/ICB0000000000000766. [DOI] [PubMed] [Google Scholar]
- 90.Karatsai E, Robson AG, Taylor SRJ. Outcomes associated with sustained-release intraocular fluocinolone implants in a case of melanoma-associated retinopathy treated without systemic immunosuppression. JAMA Ophthalmol. 2019;137:564–7. doi: 10.1001/jamaophthalmol.2019.0284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Grewal DS, Jaffe GJ, Keenan RT. Sarilumab for recalcitrant cystoid macular edema in non-paraneoplastic autoimmune retinopathy. Retin Cases Brief Rep. 2019 doi: 10.1097/ICB.0000000000000872. doi: 101097/ICB0000000000000872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Kim MS, Hong HK, Park KH, Woo SJ. Intravitreal dexamethasone implant with plasma autoantibody monitoring for cancer-associated retinopathy. Korean J Ophthalmol. 2019;33:298–300. doi: 10.3341/kjo.2018.0091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Benson MD, Plemel DJA, Yacyshyn E, Sandhu I, MacDonald IM, Baker CF. Combination treatment with rituximab and bortezomib in a patient with non-paraneoplastic autoimmune retinopathy. Ocul Immunol Inflamm. 2019:1–8. doi: 10.1080/09273948.2019.1636094. doi: 101080/0927394820191636094. [DOI] [PubMed] [Google Scholar]
- 94.Ramos-Ruperto L, Busca-Arenzana C, Boto-de los Bueis A, Schlincker A, Arnalich-Fernández F, Robles-Marhuenda Á. Cancer-associated retinopathy and treatment with intravenous immunoglobulin therapy A seldom used approach. Ocul Immunol Inflamm. 2019:1–4. doi: 10.1080/09273948.2019.1681471. doi: 101080/0927394820191681471. [DOI] [PubMed] [Google Scholar]
- 95.Takiuti JT, Takahashi VKL, Xu CL, Jauregui R, Tsang SH. Non-paraneoplastic related retinopathy: Clinical challenges and review. Ophthalmic Genet. 2019;40:293–7. doi: 10.1080/13816810.2019.1650072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Carrera W, Tsamis KA, Shah R. A case of cancer-associated retinopathy with chorioretinitis and optic neuritis associated with occult small cell lung cancer. BMC Ophthalmol. 2019;19:4–9. doi: 10.1186/s12886-019-1103-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Javaid Z, Rehan SM, Al-Bermani A, Payne G. Unilateral cancer-associated retinopathy: A case report. Scott Med J. 2016;61:155–9. doi: 10.1177/0036933015598124. [DOI] [PubMed] [Google Scholar]
- 98.Weleber RG, Watzke RC, Shults WT, Trzupek KM, Heckenlively JR, Egan RA, et al. Clinical and electrophysiologic characterization of paraneoplastic and autoimmune retinopathies associated with antienolase antibodies. Am J Ophthalmol. 2005;139:780–94. doi: 10.1016/j.ajo.2004.12.104. [DOI] [PubMed] [Google Scholar]
- 99.Comlekoglu DU, Thompson IA, Sen HN. Autoimmune retinopathy. Curr Opin Ophthalmol. 2013;24:598–605. doi: 10.1097/ICU.0b013e3283654e1e. [DOI] [PubMed] [Google Scholar]