

Abstract
Viral anterior uveitis (VAU) needs to be suspected in anterior uveitis (AU) associated with elevated intraocular pressure, corneal involvement, and iris atrophic changes. Common etiologies of VAU include herpes simplex, varicella-zoster, cytomegalovirus, and rubella virus. Clinical presentations can vary from granulomatous AU with corneal involvement, Posner-Schlossman syndrome, Fuchs uveitis syndrome, and endothelitis. Due to overlapping clinical manifestations between the different viruses, diagnostic tests like polymerase chain reaction and Goldmann-Witmer coefficient analysis on the aqueous humor may help in identifying etiology to plan and monitor treatment.
Keywords: Cytomegalovirus, herpes simplex virus, ocular hypertension, rubella virus, varicella-zoster virus, viral anterior uveitis
Viral anterior uveitis (VAU) is characterized by anterior uveitis (AU) with elevated intraocular pressure (IOP) diffuse stellate keratic precipitates (KPs), presence of pigmentation in active KPs and iris atrophic changes.[1,2,3,4] The most commonly implicated viruses include herpes simplex (HSV), varicella-zoster (VZV), cytomegalovirus (CMV), and rubella (RV).[5,6] Herpetic AU is the most common cause of VAU accounting for 5–10% of all uveitis cases in the western world and 0.9–8.3% of all infectious uveitis in India.[7,8,9,10] The severity and outcome of VAU depend on the type of the virus, clinical characteristics of the disease, immune status, and genetic makeup of the individual. In an aqueous-based polymerase chain reaction (PCR) study from South India, 2/3rd of cases were VZV, 19.4% were HSV-1, and 8.3% were CMV.[11] This review will focus on syndromes associated with viral etiology, different viruses causing AU, clinical features, diagnostic tools, and management of viral anterior uveitis.
Methods
Literature search pertaining to VAU published in PubMed, EMBASE, and MEDLINE. For PubMed related search, MESH terms “viral anterior uveitis” and “Herpetic”/”Cytomegalovirus”/”Rubella”/”Fuchs heterochromic iridocyclitis”/”Posner Schlossman syndrome”/”Diagnosis”, and “Therapy”. A manual search of references cited by retrieved articles for additional references was also done. All authors independently conducted a systematic review of the literature and extracted data.
Syndromes Associated with Viral Aetiology
Posner Schlossman syndrome (PSS)
PSS is characterized by recurrent, acute attacks of unilateral mild AU with few granulomatous KPs, and severely elevated intraocular pressure (IOP).[12] Symptoms include mild blurring of vision and haloes. It affects young adults more frequently in the 3rd decade in the European population but later in the Asian population (3–5th decade).[13,14,15,16,17] Males are at a higher risk of developing PSS (50.5–71.4%).[18] CMV appears to be a major cause of PSS, especially in Asia.[14,15,19] HSV is also known to cause PSS.[20] Posterior synechiae and vitritis are absent. Mild iris atrophic changes may occur. Glaucoma develops in 26% of which 17% require filtration surgery.[14] The course is recurrent and often unpredictable.
Fuchs uveitis syndrome (FUS)
FUS is a chronic low-grade inflammation involving the anterior uveal tract and vitreous and is most commonly unilateral (90%).[4,21] Fuchs initially described this condition as Fuchs heterochromic iridocyclitis, characterized by heterochromia, cyclitis with KPs, and cataract associated with vitreous involvement.[22] In the USA and Europe, RV is the main etiologic agent while CMV is the predominant cause in Asia.[23,24,25,26,27] Other associations include HSV, toxoplasmosis, toxocariasis, sarcoidosis, retinitis pigmentosa, Horner's syndrome, Ushers syndrome, and previous ocular trauma.[28,29,30] Clinical signs include mild with low-grade anterior chamber inflammation, absent ciliary injection, diffuse distribution of white stellate KPs over the entire endothelium, diffuse iris atrophy, posterior subcapsular cataract, presence of Koeppe nodules, absence of posterior synechiae, low-grade vitritis and with or without glaucoma.[31,32] Heterochromia is seen in light colored irides (12.7–82%) and often absent in heavily pigmented eyes and maybe noticed before the development of visual symptoms.[31] The affected eye is hypochromic due to diffuse pigment loss but maybe hyperchromic when anterior stromal atrophy occurs exposing the darker iris pigment epithelium. In the case of the absence of heterochromia, the occurrence of iris nodules together with cataract, vitritis, or glaucoma should alert the clinician on the likelihood of FUS.[25] FUS may begin in early childhood, but the diagnosis is often delayed for years, as the characteristic findings may not be present at disease onset.[21]
Structural changes in iris occur earlier than heterochromia. Atrophy affects all layers and radial markings at the pupillary border are less prominent.[33] A motheaten appearance develops. In later stages, there is a loss of iris tone and sphincter muscle causing widened iridocorneal angle and increased anterior chamber depth.[34]
In addition, normal radial iris vessels may appear like neovascularization in FUS patients with diffuse iris atrophy. Rubeotic-like “bridging vessels” in the chamber angle extension may cause hyphema during cataract surgery (Amsler sign).[35] A modified Amsler sign has been described after minor trauma, peribulbar anesthesia, contact tonometry, and sexual intercourse.[35,36,37] Rarely, iris crystals are seen (Russel bodies), which may represent plasma cells filled with antibodies.[33,38] Other ocular findings include peripheral chorioretinal scars (7.2–65% of FUS patients).[30,39] Disc and macula edema, snow banking, retinal vasculitis are typically absent in FUS.
Common Etiologies of Viral Anterior Uveitis
Herpes simplex virus
HSV AU is commonly caused by HSV-type 1 and accounts for a large proportion of viral AU in western populations.[40,41,42,43,44] It typically affects both genders and in the 4th–5th decades of life.[44] There may be a history of recurrent fever, blisters, grouped vesicles around the eyelid border with diffuse edema. HSV AU occurs more frequently during reactivation than in primary disease. The viral genome lying latent within the trigeminal ganglion reactivates. It is transported down the axon, manifesting in the periocular skin, cornea, or intraocular inflammation.[45] It is usually unilateral but can be bilateral in 18% cases.[3,4] Symptoms include acute severe eye pain, redness, tearing, photophobia, blurring of vision.
The incidence of corneal involvement in HSV ranges from 33–41% and can present as active keratitis (epithelial, stromal, interstitial, and disciform), old corneal scar, endotheliitis, and reduced corneal sensation. HSV dendritic ulcers are branching with well-developed terminal bulbs. The ulcer base and borders are stained by fluorescein and rose bengal, respectively.[4,5,6]
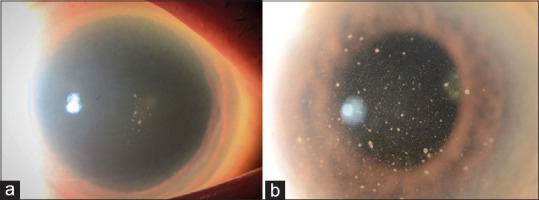
HSV AU is characterized by small to medium-sized KPs, some of these fresh KPs may be pigmented. The location may be central, paracentral, or diffuse. In keratouveitis, they are located in the same distribution as the inflamed cornea. Elevated intraocular pressures occur due to trabeculitis and this can be episodic. These may cause secondary glaucomatous optic neuropathy. Iris atrophy occurs in 41–48%.[42,43] During acute HSV, sectoral iridoplegia and flattening of the pupillary border occur in the affected area [Fig. 1]. The presence of patchy or sectoral iris atrophy is seen in recurrent or chronic disease and may be absent in very early disease. Spiral atrophy is typically associated with HSV. Diffuse iris atrophy is rather an uncommon finding and noted in 10% cases.[45,46,47] HSV AU causes iris pigment epithelitis. In severe inflammation, hypopyon, transient hyphema, posterior synechiae (38%), and vitritis (43%) may occur.[47] Focal iris stromal hemorrhage may be seen in acute HSV. Cataract occurs later in the disease course.
Figure 1.

Slit-lamp photograph of HSV AU showing granulomatous keratic precipitates adjacent to the inflamed cornea (a), iridoparesis (b) and diffuse iris stromal atrophy (c)
Varicella Zoster virus
VZV lies dormant in the neural sensory ganglia following primary infection usually in childhood and reactivates when VZV specific immunity wanes, typically during the 6th or 7th decade of life.[4,10,48,49,50,51,52,53,54,55,56,57,58,59] Alternatively, it may occur in young immunocompetent individuals, conditions causing immunosuppression like acquired immunodeficiency syndrome and immunosuppressive drugs.[60,61,62,63,64,65] Herpes zoster ophthalmicus (HZO) presents with severe pain followed by a vesicular eruption in the dermatome of the ophthalmic division of the trigeminal nerve. If the tip of the nose is involved, it is a predictor for ocular inflammation (Hutchinson's sign). VZV AU occurs in 40–60% of HZO in immunocompetent patients and may be present for many months.[48,50]
Typically, VZV AU presents 2 weeks following dermatological manifestations in the form of acute hypertensive AU with granulomatous or nongranulomatous uveitis. The inflammation in VZV is generally more severe than in HSV AU, possibly because VZV invades the root of iris epithelium and causes occlusive vasculitis. Segmental iris atrophy (triangular sectoral loss of iris pigment epithelium with the base at the iris root) may develop after the acute episode resolves causing transillumination defect (88%). It has been postulated that the severity of iris atrophy and pupil distortion is closely related to the viral load in aqueous [Fig. 2].[23,59] Corneal involvement has been reported in 25% of cases and includes nummular keratitis, limbal keratitis, and ring infiltrates. Profound reduced corneal sensation and coarse pseudo dendrites with an elevated appearance that lacks terminal bulbs may be seen. There may be associated episcleritis, scleritis, and choroidal vitiligo.[66] Posterior synechiae (40%) and vitritis (83%) can occur in VAV AU. Secondary glaucoma is noted in 15–43% of cases.[43,56,67] A detailed posterior segment examination is mandatory in all cases of herpetic uveitis.
Figure 2.

Slit-lamp photograph of VZV AU showing pigmented active keratic precipitates and D shaped pupil at initial presentation (a) and development of sectoral iris atrophy in the same eye over 6 months (b). External photograph showing facial scars of herpes zoster ophthalmicus scars over the left side of the forehead and nose (c)
Zoster sine herpete AU: At times, patients present with AU typical of viral AU in the absence of dermatological manifestations.[68,69]
Cytomegalovirus
CMV is an important cause of hypertensive AU in immunocompetent individuals and there is likely a prominent immunological component as it is not seen in immunocompromised individuals.[15] Ocular tissues like iris and ciliary body may be a site of CMV latency as suggested by murine studies.[70] An intraocular immunocompromised state with impairment of both innate and adaptive immunity, especially the virus-specific T-cell response, may trigger CMV reactivation (Example: ocular corticosteroid implants, topical cyclosporine A 0.05% ophthalmic emulsion, topical prostaglandin analogs, ophthalmic surgery).[71,72]
Most cases have been reported from Asia, particularly from Chinese and Japanese populations, which could be due to the higher seroprevalence of CMV in Asia.[15,18,40,73] CMV has been identified as the causative virus for 75% of hypertensive AU in Singapore, 67% of the chronic idiopathic recurrent AU and ocular hypertension in Korea, 33% of the viral AU in Thailand, 8.3% of viral AU in south India and only 2% of viral AU in the United States of America.[11,15,16,17,19,40,70,73,74,75,76] CMV AU usually affects individuals from the 3rd decade onwards, particularly Asians and males, those in their 3rd–5th decade present with PSS while those in their 5th –7th decade present with chronic CMV AU resembling FUS. It is acute and recurrent in patients younger than 40 years of age or chronic in those above 40 years of age. It is unilateral in most of the cases and bilateral in 7% cases.[16,17,74,75] The clinical manifestations of CMV AU vary.
Acute relapsing hypertensive anterior uveitis (Posner-Schlossman Syndrome)
CMV is thought to be the cause of PSS in Asian and western populations.[16,19,23,40,77,78] The typical presentation is a patient in the 3rd–5th decade with an acute onset of haloes, unilateral mild blurring of vision associated with an ipsilateral headache, possibly with a history of similar episodes. The IOP often exceeds 50 mm Hg during the attack in the presence of subtle subepithelial edema. The severely elevated IOP is often out of proportion to the findings of mild anterior segment inflammation. KPs are medium to large (39%), white or gray colored, and few located centrally or in the peripheral cornea.[4,6]
Chronic hypertensive CMV anterior uveitis
Chronic CMV AU more commonly affects older patients in the 5th –7th decade, at a mean of 65 years of age, who may present with ocular discomfort and blurring of vision. A geographic disparity is seen in the clinical presentation of chronic CMV AU in Asian and western populations. CMV is a major cause of FUS in East Asia, especially in Singapore, Taiwan and Japan.[14,15,18,19] It presents with mild ocular injection, mild-to-moderate anterior chamber activity and diffuse, fine, stellate uniformly distributed KPs. Chronic CMV AU in eyes of European patients has fewer KPs that are brown (pigmented) and located inferiorly, with minimal flare. The IOP is typically persistently elevated in chronic CMV AU. The iris may appear moth-eaten due to stromal atrophy, which is more commonly diffuse, although patchy and rarely sectoral atrophy have been reported, and the posterior pigment epithelium is often relatively intact with no transillumination defects.[79] Although findings of CMV in the smooth muscle cells of the iris led some to postulate that the iris stromal atrophy was due to ischemic necrosis of the iris stroma as a result of the direct viral invasion, Sakai et al. have suggested that the diffuse iris atrophy which is not associated with dyscoria may develop as a consequence of persistently elevated IOP rather than tissue damage by CMV.[58] Heterochromia (in which a naturally darker iris appears lighter, and lighter irides, particularly blue or light green, appear darker) is uncommon but may be present.[80] The diffuse iris atrophy may also result in fragile iris vasculature, which can be visualized on gonioscopy in the iris and trabecular meshwork or iridocorneal angle. These fragile vessels may be prone to bleeding easily, giving rise to Amsler's sign.
A posterior subcapsular cataract occurs in 81.3% of eyes later in the disease course. Unlike RV, vitritis is rare in CMV infection. Unlike in PSS, the inflammation tends to recur when topical corticosteroids are tapered.
Recurrent or chronic iridocyclitis
Unlike Asian patients who present similarly to FUS or PSS, patients in the West often present with less distinct syndromes, or overlap of features from both syndromes, manifesting as a mild unilateral recurrent or chronic iridocyclitis.[14]
Corneal endotheliitis
Corneal endotheliitis is the inflammation of the corneal endothelium characterized by localized corneal stromal edema and KPs.[81] It can involve a focal area or even the entire endothelium that presents similarly to diffuse bullous keratopathy with severe stromal edema. An immune ring formation similar to that seen in HSV-related keratitis may sometimes be present. The IOP may be elevated.[82] CMV corneal endotheliitis may be associated with AU in 30% of Asian or European patients or may occur in isolation.[19,80]
Other characteristic clinical signs
Coin-shaped lesions in which small-sized KPs are distributed in a ring pattern are pathognomonic of CMV with a positive predictive value of 90.9% and, maybe seen in both acute and chronic infection.[73] These coin-shaped KPs were seen in 53% of CMV AU cases in a recent Japanese study.[58] KPs may also be seen in a linear pattern in the peripheral cornea.[15] Nodular endothelial lesions, which possibly represent swollen endothelial cells, are white medium-sized nodular lesions with a surrounding translucent halo and may become pigmented over time. They are more common in chronic CMV AU and are significantly associated with CMV infection in eyes with presumed FUS [Fig. 3].[17] The endothelial cell count is significantly reduced in CMV positive eyes, a feature that is less commonly seen in other VAU in the absence of frank keratitis.[76,83]
Figure 3.
Slit-lamp photograph of CMV AU in diffuse illumination showing a couple of granulomatous keratic precipitates in the center of the steamy cornea in an eye presenting acutely with elevated intraocular pressure typical of CMV associated Posner Schlossman syndrome (a) and diffusely distributed fine filiform keratic precipitates typical of Fuchs uveitis syndrome admixed with scattered pigmented, medium-sized keratic precipitates in an eye with cytomegalovirus chronic anterior uveitis (b)
The pupil is usually round and posterior synechiae are notably absent. Associated posterior segment abnormalities are uncommon and include periphlebitis, disc, and macular edema and epiretinal membrane. Prolonged arm to retina time on fluorescein angiography has been hypothesized to reflect subclinical vasculitis.[84]
Rubella virus
RV AU is chronic, often unilateral but may be bilateral (14%) in the presentation.[6] It is a common cause of FUS in the western population. The definitive finding of anti-RV antibodies in the anterior chamber fluid of FUS patients clearly shows that rubella may be participating in the pathogenesis.[24,46,85,86] On the other side, the very rare finding of RV-PCR may be a sign that FUS is less an infectious but more an immune response to rubella. The hypothesis of FUS as a RV-induced disease was supported by the decreased number of FUS patients after the introduction of the rubella vaccination program in the United States (from 4.48% to 1% FUS patients/year).[25] However, the question rises if a living attenuated vaccine or a subclinical RV infection before vaccination may induce FUS.[39] Analysis of the aqueous humor in FUS patients also showed elevated levels of the inflammatory cytokine (IL-6, IL-10), interferon-γ, and low IL-12 levels suggesting a Th1-type response.[87,88]
RV AV usually presents in relatively younger patients (mean age 35 ± 12 years) with posterior subcapsular cataract (47%) with a chronic blurring of vision and or floaters with minimal redness and pain.[6] It has a chronic course and presents with diffuse stellate KPs (do not become pigmented and persist despite treatment), diffuse iris atrophy, and mild anterior chamber reaction. Koeppe nodules may be present. Low-grade vitritis is often present and frequently mistaken for intermediate uveitis [Fig. 4].
Figure 4.
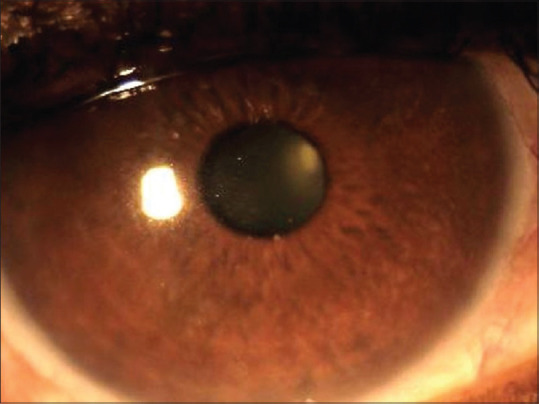
Slit-lamp photograph of the right eye in a case of Fuchs heterochromic iridocyclitis syndrome showing fine to medium-sized keratic precipitates on the corneal endothelium and moth-eaten appearance of iris
Absence of redness, pain, posterior synechiae, and cystoid macular edema are characteristic features. RV AU can be complicated by ocular hypertension (25%) leading to secondary glaucoma.
Other viral etiologies
Less common causes include, human T-cell lymphotropic virus-type 1 (Seen in southern Japan and Africa and frequently presents as intermediate uveitis), Human immunodeficiency virus (anterior segment inflammation is mild with small or medium-sized KPs on the corneal endothelium which disappear quickly with the administration of highly active retroviral therapy), Chikungunya virus (nongranulomatous AU or FUS like presentation with a history of systemic Chikungunya virus infection and, responds to topical corticosteroids), ZIKA virus (mild in adults and presents as AU with nonpurulent conjunctivitis and treated with topical steroids) and Ebola virus (AU with KPs, posterior synechiae, cataract and ocular hypertension and, is unclear if it is caused by a cytopathic effect or an immune response). The role of Epstein–Barr virus and parvovirus B19 virus (link with juvenile idiopathic arthritis) in VAU is uncertain[89,90,91,92,93,94,95,96] Vitiligo iridis and secondary glaucoma may also be seen as a long term sequelae of smallpox.[97]
Table 1 summarizes the clinical manifestations between HSV, VZV, CMV, and RV
Table 1.
Comparison of the clinical features between the common viral anterior uveitis aetiologies
| Variables | Herpes simplex virus (HSV) | Varicella-zoster virus (VZV) | Cytomegalovirus (CMV) | Rubella virus (RV) Rubella associated FUS | ||
|---|---|---|---|---|---|---|
| Acute (Posner Schlossman like syndrome) | Chronic | |||||
| Chronic CMV anterior uveitis | CMV-associated Fuchs uveitis syndrome (FUS) | |||||
| Age | 40-50 years | >60 years Immuncompromised patients (any age) | 30-50 years | 40-70 years | 40-70 years | 20-40 years (Mean: 35±12 years) |
| Gender | No predilection | No predilection | Males (65%) | Males | Males (80%) | No predilection |
| Race | All | All | Predominantly Asian population | Western population | Predominantly Asian population | Western population |
| Laterality | Mostly unilateral (bilateral in 18%) | Unilateral | Unilateral | Mostlty unilateral (bilateral in 7%) | Mostly unilateral (bilateral in 7%) | Mostly unilateral (bilateral in 14%) |
| Course | Acute, recurrent | Acute, recurrent | Acute, recurrent | Chronic | Chronic | Chronic |
| Intraocular pressure | Acute spikes (38-90%) | Acute spikes (40-75%) | Very high (up to 50 mmHg) during acute episodes (100%) | Very high (43.5±9.8 mmHg); persistently elevated | Very high (43.5±9.8 mmHg); persistently elevated (73.3%) | Persistent elevation (25%) |
| Dermal manifestations | h/o fever or blisters/grouped vesicles occurring at the border of the eyelids with diffuse edema | Vesicular rash involving the ophthalmic division of the trigeminal nerve | None | None | None | None |
| Conjunctival injection | Moderate to severe | Moderate to severe | Mild | Mild | Mild | None |
| Corneal sensation | May be reduced | May be reduced (more profound and diffuse hypoaesthesia than HSV) | Intact | Intact | Intact | Intact |
| Epithelial keratitis | Dendritic ulcers (usually branching, with well-developed terminal bulb) | Pseudodendritic ulcers (less regular branching, few terminal dilatations) | None | None | None | None |
| Stromal keratitis | Disciform keratitis; Interstitial keratitis; Immune ring keratitis | Nummular keratitis; Limbal keratitis; Immune ring keratitis | Immune ring keratitis | None | ||
| Corneal scars | Present (33%) | Present (25%) | Rare | None | ||
| Endotheliitis | May be present | May be present | May be present | May be present | Nodular endothelial lesions surrounded by a translucent halo and occasional pigmentation | None |
| Keratic precipitates | ||||||
| Size | Small to medium | Small to medium | Medium to large (39%) | Small | Fine and stellate (44%) | Fine, may be stellate |
| Distribution | Central, paracentral, diffuse, may be in Arlt’s triangle or in the same distribution as inflamed cornea | Central, paracentral, diffuse, may be in Arlt’s triangle or in the same distribution as inflamed cornea | Single or few, distributed centrally or in peripheral cornea; may have coin like lesions | May have a coin like lesions | Diffusely distributed; may have a coin like lesions (ring or linear pattern) | Diffuse |
| Colour | White, may be pigmented | White, may be pigmented | White or gray | White or gray, may be brown | White or gray, may have pigmentation | White, never pigmented |
| Endothelial cell count | Normal | Normal | Reduced | Reduced | Reduced | Normal |
| Anterior chamber inflammation | Moderate to severe | Severe. Usually more than HSV | Mild | Mild | Mild | Mild |
| Iris | ||||||
| Iridoplegia | May be present during acute phase causing pupil flattening or D shaped pupil | May be present during acute phase causing pupil flattening or D shaped pupil | Absent | Absent | Absent | Absent |
| Iris atrophy | Sectoral or patchy atrophy with transillumination defects, spiral iris atrophy | Sectoral atrophy with transillumination defects, rarely massive iris atrophy with gross sphincter damage | Mostly absent, rarely diffuse stromal iris atrophy | Rarely sectoral, stromal iris atrophy, no transillumination defects | Diffuse stromal iris atrophy, no transillumination defects | Diffuse atrophy, fine iris transillumination defects |
| Posterior synechiae | May be present | May be present | Absent | Absent | Absent | Absent |
| Pupil shape | May be irregular | May be irregular | Round | Round | Round | Round |
| Elevated IOP | Elevated (38-90%) | Elevated (40-75%) | Elevated (100%) | Elevated (69%) | Elevated (25%) | |
| Cataract | Present in 28-35%, later in onset | Present in 27-30%, later in onset | 23%, later in onset | 75%, later in onset | At the time of presentation (47%) | |
| Glaucoma | Present in 18-54% | Present in 30-40% | 23% | 36% | ||
| Vitritis | 43% | 83% | 0% | 9% | Very rare | Always present |
Investigations
Anterior chamber tap
Aqueous humor analysis is a useful method to determine the etiology and estimate the viral load as it may difficult to differentiate the etiology based on clinical manifestations in all cases. Tests done include PCR, Goldmann–Witmer coefficient (GWC) analysis, metagenome sequencing.[6,25,77,98,99]
Polymerase chain reaction
PCR can detect minimal amounts of viral DNA and enable rapid confirmation of diagnosis. Aqueous tap for PCR should be done during the IOP spike, preferably before initiation of therapy especially in CMV.[16] A negative PCR does not exclude a viral etiology. This could be due to the limited volume of aqueous sample, low intraocular viral load, transient rapid rise in IOP, and self-limiting tendency of ocular inflammation with rapid elimination of viral DNA and presence of inhibitory compounds in the sample or microorganism polymorphism.[6] In some cases, a positive result may only be obtained after repeated aqueous taps. Conversely, PCR may give a false positive result by detecting DNA from latent viruses in leukocytes present in the anterior chamber during inflammation. A qualitative multiplex PCR can be done to screen for viruses and subsequent real-time PCR can help to identify the causative virus and quantify the viral load as a marker of severity of the infection. Real-time PCR can also be used to monitor response to therapy and any drug resistance.[77,83]
Goldmann–Witmer coefficient analysis
GWC helps to determine pathogen-specific intraocular antibody production. Unlike PCR which tends to be positive at the early reactivation, when the viral load is higher, GWC analysis may take up to 2 weeks to become positive but remains positive for longer periods and hence more useful when patients present later (chronic) as in RV AU. RV is commonly detected via positive GWC results but only sporadically by PCR. However, it is less specific than PCR due to possible cross-reactivity of antibodies. As the diagnostic utility of the above tests depends on the patient's immune status, the chronicity of infection and the time of aqueous sampling, it is best to perform both the tests in parallel to increase the diagnostic yield. GWC analysis is not widely available in most countries and hence most countries rely solely on PCR.[6,40,98]
Viral cultures are difficult and time-consuming. It is not commonly done.
Other investigations
Anterior segment imaging includes specular microscopy to demonstrate lowered endothelial cell counts (ECC) compared to the fellow eye is known to occur in CMV AU. The extent of endothelial cell loss is correlated with the viral disease burden.[67,83] Anterior segment optical coherence tomography can demonstrate the nodular endothelial lesions as thickened, highly reflective endothelial cells layer. Confocal microscopy demonstrates the owl eye cells (large endothelial cells containing nuclei with a high reflection area surrounded by a halo of low reflection within the cornea) and to monitor the response to therapy.[100,101] Serology has limited value as most adults have had prior exposure to the viruses. Metagenomic deep sequencing can detect deoxyribonucleic acid (DNA) and ribonucleic acid (RNA) viruses in as little as 20 μL of intraocular fluid samples in a single assay and holds promise in diagnosis of infectious uveitis.[102]
Treatment
Treatment of HSV AU
Though the management of HSV keratitis is well studied, the role of acyclovir in the treatment of HSV AU is not evaluated. Studies suggest that the duration of AU may be shortened by the prompt use of therapeutic doses of antiviral therapy and, maintenance therapy is effective in decreasing disease recurrence.[51]
Oral acyclovir 400 mg five times daily for 4 weeks in conjunction with topical corticosteroids that reduce the anterior segment inflammation, cycloplegics/mydriatic agents that reduce the pain and prevent posterior synechiae. In severe and recurrent disease, maintenance therapy of oral acyclovir 400 mg twice daily is useful to prevent a relapse. Alternatively, valacyclovir, which is a prodrug with better bioavailability, may also be used at a dose of 500 mg three times a day for 4 weeks followed by 500 mg twice a day for maintenance.[47] Systemic antiviral therapy combined with low-dose corticosteroid drops may have to be used for several years, to prevent relapses. In eyes with raised IOP, antiglaucoma medications are given topically. Severe elevation of IOP may require oral carbonic anhydrase inhibitors and filtration surgery. When preparing the eye with a viral AU for cataract surgery, the eye should be quiescent and prophylactic oral antiviral therapy is found to be useful. Lucy M Lu et al. noted the recurrence of herpes zoster in 23 (40.4%) patients after phacoemulsification cataract surgery. An increased risk for recurrence was associated with shorter periods of quiescence and a greater number of recurrences before surgery. Acyclovir prophylaxis protected against recurrences after cataract surgery and, may be required in cases with a history of multiple disease recurrences.[103]
Treatment of VZV AU
Acyclovir given 800 mg five times daily for 10 days given within 72 h of the onset of skin lesions in HZO reduces the incidence and severity of episcleritis, dendritiform keratopathy, stromal keratitis, and anterior uveitis. Topical steroids and cycloplegics/mydriatic agents are used to alleviate inflammation and pain. However, the duration of treatment for chronic VZV AU should be as long as the uveitis is active. Oral acyclovir 400 mg twice a day is used as prophylaxis for recurrent uveitis. Owing to the predictability of its resorption, oral valacyclovir is generally preferred to oral acyclovir. A thrice daily dose of 0.5-1 gm for 10-14 days is the standard protocol. Thereafter a prophylactic course of thrice-weekly dose of 500 mg or 500 mg daily should be continued for 3–12 months depending upon the topical demand for corticosteroids. Acyclovir and valacylovir need to be used with caution in HIV as they may cause thrombocytopenia.[51] Acute renal failure is a known complication with these drugs. Alternatively famciclovir 500 mg three times daily or brivudin 125 mg once a day may be used.[104] Topical steroids are given to control the inflammation and need to be tapered very slowly to avoid rebound inflammation.
Treatment of CMV AU
The acute recurrent phenotype of CMV AU frequently exhibits quiescence without antiviral treatment. However, it is reported that early antiviral treatment seems to lower the risks of sight-threatening complications that may develop from recurrent and chronic inflammation. CMV AU responds to oral valganciclovir, ganciclovir, and foscarnet. Ganciclovir and valganciclovir diffuse into CMV infected cells and inhibit CMV's DNA polymerase UL54 following phosphorylation by CMV'S viral kinase encoded by the UL97 gene while, foscarnet is a direct inhibitor of the viral DNA polymerase and does not require phosphorylation.[105,106,107] At present, there are no clear guidelines regarding the management of CMV AU. Studies have evaluated the efficacy of systemic (intravenous ganciclovir or foscarnet, oral ganciclovir) and local therapy (intravitreal ganciclovir, topical ganciclovir drops and gel) and have compared the various forms of antiviral therapy.
The induction regimen of oral valganciclovir followed is, 900 mg twice daily for 3 weeks followed by, a maintenance regimen of 450 mg twice daily for a minimum of 4 weeks.[108] CMV AU may require long term antiviral therapy to reduce the risk of recurrences. Regular laboratory monitoring for bone marrow suppression, renal and hepatic toxicity and the cost of treatment makes it less feasible as long-term therapy in developing countries.[98] Intravitreal ganciclovir has a lower risk of systemic toxicity and has been explored as an alternative to systemic ganciclovir. However, the recurrence rates were high. Topical ganciclovir is an alternative form of antiviral therapy in CMV AU. The topical concentration ranged between 0.15%–2% and applied 6–8 times/day for induction and 1–4 times/day for maintenance.[109,110] Ganciclovir 2% eye drops have reported good results in CMV corneal endotheliitis and AU. Ganciclovir ophthalmic gel 0.15% is well tolerated with minimal toxicity. As this is less expensive and does not require laboratory monitoring, this may be a more viable option for long term antiviral therapy. The systemic and topical control of CMV anterior uveitis-treatment outcomes (STACCATO) is an ongoing randomized trial comparing the efficacy of oral valganciclovir and 2% topical ganciclovir along with placebo which, may provide further insight of effective routes of antiviral therapy in CMV AU.[110] Some authors favor the administration of intravitreal ganciclovir. An injection of 2 mg/0.05–0.1 ml is given weekly for 3 months either with or without adjunctive oral valganciclovir. The treatment of CMV induced endotheliitis with either topical or systemic ganciclovir has been reported to be partially successful.[51] Topical nonsteroidal anti-inflammatory drugs (NSAIDs) may also be considered in CMV AU recalcitrant to topical steroids.[108]
Treatment of Rubella AU
Topical steroids may not be necessary due to the low-grade inflammation. Prolonged use can hasten cataract and glaucoma formation. Systemic immunosuppressive therapy is not recommended. Topical NSAIDs are considered to retard progression especially if required long term. Antiglaucoma medications may be used for secondary glaucoma. In glaucoma cases resistant to topical treatment, filtration surgeries are recommended.
Conclusion
A high index of suspicion for a viral etiology is required in the presence of the following features: Raised IOP at presentation, corneal scars, fresh pigmented KPs, and iris atrophy. HSV, VZV, CMV, RV are common etiologies. Variable clinical presentations with overlapping manifestations in different viruses may require diagnostic tests like PCR, GWC analysis for confirmation of etiology. This is important for planning therapy. Glaucoma is the most common vision-threatening complication of VAU.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Groen-Hakan F, Babu K, Tugal-Tutkun I, Pathanapithoon K, de Boer JH, Smith JR, et al. Challenges of diagnosing viral anterior uveitis. Ocul Immunol Inflamm. 2017;25:710–20. doi: 10.1080/09273948.2017.1353105. [DOI] [PubMed] [Google Scholar]
- 2.Cunningham ET., Jr The expanding spectrum of viral anterior uveitis. Ophthalmology. 2011;118:1903–4. doi: 10.1016/j.ophtha.2011.07.014. [DOI] [PubMed] [Google Scholar]
- 3.Jap A, Chee S-P. Viral anterior uveitis. Curr Opin Ophthalmol. 2011;22:483–8. doi: 10.1097/ICU.0b013e32834be021. [DOI] [PubMed] [Google Scholar]
- 4.Chan NS, Chee S-P. Demystifying viral anterior uveitis: A review. Clin Exp Ophthalmol. 2019;47:320–33. doi: 10.1111/ceo.13417. [DOI] [PubMed] [Google Scholar]
- 5.Relvas LJ, Caspers L, Chee S-P, Zierhut M, Willermain F. Differential diagnosis of viral-induced anterior uveitis. Ocul Immunol Inflamm. 2018;26:726–31. doi: 10.1080/09273948.2018.1468470. [DOI] [PubMed] [Google Scholar]
- 6.Pleyer U, Chee S-P. Current aspects on the management of viral uveitis in immunocompetent individuals. Clin Ophthalmol. 2015;9:1017–28. doi: 10.2147/OPTH.S60394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cunningham ET., Jr Diagnosing and treating herpetic anterior uveitis. Ophthalmology. 2000;107:2129–30. doi: 10.1016/s0161-6420(00)00287-6. [DOI] [PubMed] [Google Scholar]
- 8.Biswas J, Narain S, Das D, Ganesh SK. Pattern of uveitis in a referral uveitis clinic in India. Int Ophthalmol. 1996;20:223–8. doi: 10.1007/BF00175264. [DOI] [PubMed] [Google Scholar]
- 9.Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol. 2007;55:173–83. doi: 10.4103/0301-4738.31936. [DOI] [PubMed] [Google Scholar]
- 10.Babu K, Mahendradas P, Sudheer B, Kawali A, Parameswarappa DC, Pal V, et al. Clinical profile of herpes zoster ophthalmicus in a south indian patient population. Ocul Immunol Inflamm. 2018;26:178–83. doi: 10.1080/09273948.2017.1381272. [DOI] [PubMed] [Google Scholar]
- 11.Babu K, Kini R, Philips M, Subbakrishna DK. Clinical profile of isolated viral anterior uveitis in a South Indian patient population. Ocul Immunol Inflamm. 2014;22:356–9. doi: 10.3109/09273948.2013.841482. [DOI] [PubMed] [Google Scholar]
- 12.Jap A, Sivakumar M, Chee S-P. Is Posner Schlossman syndrome benign? Ophthalmology. 2001;108:913–8. doi: 10.1016/s0161-6420(01)00551-6. [DOI] [PubMed] [Google Scholar]
- 13.Paivonsalo-Hietanen T, Tuominen J, Vaahtoranta-Lehtonen H, Saari KM. Incidence and prevalence of different uveitis entities in Finland. Acta Ophthalmol Scand. 1997;75:76–81. doi: 10.1111/j.1600-0420.1997.tb00255.x. [DOI] [PubMed] [Google Scholar]
- 14.Chan NS, Chee S-P, Caspers L, Bodaghi B. Clinical features of CMV-associated anterior uveitis. Ocul Immunol Inflamm. 2018;26:107–15. doi: 10.1080/09273948.2017.1394471. [DOI] [PubMed] [Google Scholar]
- 15.Chee S-P, Bacsal K, Jap A, Se-Thoe SY, Cheng CL, Tan BH. Clinical features of cytomegalovirus anterior uveitis in immunocompetent patients. Am J Ophthalmol. 2008;145:834–40. doi: 10.1016/j.ajo.2007.12.015. [DOI] [PubMed] [Google Scholar]
- 16.Hedayatfar A, Chee S-P. Posner-Schlossman syndrome associated with cytomegalovirus infection: A case series from a non-endemic area. Int Ophthalmol. 2014;34:1123–9. doi: 10.1007/s10792-014-9928-6. [DOI] [PubMed] [Google Scholar]
- 17.Chee S-P, Jap A. Presumed fuchs heterochromic iridocyclitis and Posner-Schlossman syndrome: Comparison of cytomegalovirus-positive and negative eyes. Am J Ophthalmol. 2008;146:883–9e1. doi: 10.1016/j.ajo.2008.09.001. [DOI] [PubMed] [Google Scholar]
- 18.Woo JH, Lim WK, Ho SL, Teoh SC. Characteristics of cytomegalovirus uveitis in immunocompetent patients. Ocul Immunol Inflamm. 2015;23:378–83. doi: 10.3109/09273948.2014.950384. [DOI] [PubMed] [Google Scholar]
- 19.Park SW, Yu HG. Association of cytomegalovirus with idiopathic chronic anterior uveitis with ocular hypertension in Korean patients. Ocul Immunol Inflamm. 2013;21:192–6. doi: 10.3109/09273948.2012.754908. [DOI] [PubMed] [Google Scholar]
- 20.Yamamoto S, Pavan-Langston D, Tada R, Yamamoto R, Kinoshita S, Nishida K, et al. Possible role of herpes simplex virus in the origin of Posner-Schlossman syndrome. Am J Ophthalmol. 1995;119:796–8. doi: 10.1016/s0002-9394(14)72788-6. [DOI] [PubMed] [Google Scholar]
- 21.Tappeiner C, Dreesbach J, Roesel M, Heinz C, Heiligenhaus A. Clinical manifestation of Fuchs uveitis syndrome in childhood. Graefes Arch Clin Exp Ophthalmol. 2015;253:1169–74. doi: 10.1007/s00417-015-2960-z. [DOI] [PubMed] [Google Scholar]
- 22.Rothova A. The riddle of fuchs heterochromic uveitis. Am J Ophthalmol. 2007;144:447–8. doi: 10.1016/j.ajo.2007.06.024. [DOI] [PubMed] [Google Scholar]
- 23.Anwar Z, Galor A, Albini TA, Miller D, Perez V, Davis JL. The diagnostic utility of anterior chamber paracentesis with polymerase chain reaction in anterior uveitis. Am J Ophthalmol. 2013;155:781–6. doi: 10.1016/j.ajo.2012.12.008. [DOI] [PubMed] [Google Scholar]
- 24.Quentin CD, Reiber H. Fuchs heterochromic cyclitis: Rubella virus antibodies and genome in aqueous humor. Am J Ophthalmol. 2004;138:46–54. doi: 10.1016/j.ajo.2004.02.055. [DOI] [PubMed] [Google Scholar]
- 25.Ruokonen PC, Metzner S, Ucer A, Torun N, Hofmann J, Pleyer U. Intraocular antibody synthesis against rubella virus and other microorganisms in Fuchs' heterochromic cyclitis. Graefes Arch Clin Exp Ophthalmol. 2010;248:565–71. doi: 10.1007/s00417-009-1239-7. [DOI] [PubMed] [Google Scholar]
- 26.Babu K, Adiga M, Govekar SR, Kumar BR, Murthy KR. Associations of Fuchs heterochromic iridocyclitis in a South Indian patient population. J Ophthalmic Inflamm Infect. 2013;3:14. doi: 10.1186/1869-5760-3-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yang P, Fang W, Jin H, Li B, Chen X, Kijlstra A. Clinical features of Chinese patients with Fuchs' syndrome. Ophthalmology. 2006;113:473–80. doi: 10.1016/j.ophtha.2005.10.028. [DOI] [PubMed] [Google Scholar]
- 28.Barequet IS, Li Q, Wang Y, O'Brien TP, Hooks JJ, Stark WJ. Herpes simplex virus DNA identification from aqueous fluid in Fuchs heterochromic iridocyclitis. Am J Ophthalmol. 2000;129:672–3. doi: 10.1016/s0002-9394(00)00409-8. [DOI] [PubMed] [Google Scholar]
- 29.Teyssot N, Cassoux N, Lehoang P, Bodaghi B. Fuchs heterochromic cyclitis and ocular toxocariasis. Am J Ophthalmol. 2005;139:915–6. doi: 10.1016/j.ajo.2004.10.054. [DOI] [PubMed] [Google Scholar]
- 30.Schwab IR. The epidemiologic association of Fuchs' heterochromic iridocyclitis and ocular toxoplasmosis. Am J Ophthalmol. 1991;111:356–62. doi: 10.1016/s0002-9394(14)72322-0. [DOI] [PubMed] [Google Scholar]
- 31.Fearnley IR, Rosenthal AR. Fuchs' heterochromic iridocyclitis revisited. Acta Ophthalmol Scand. 1995;73:166–70. doi: 10.1111/j.1600-0420.1995.tb00661.x. [DOI] [PubMed] [Google Scholar]
- 32.Jones NP. Fuchs' Heterochromic Uveitis: A reappraisal of the clinical spectrum. Eye (Lond) 1991;5(Pt 6):649–61. doi: 10.1038/eye.1991.121. [DOI] [PubMed] [Google Scholar]
- 33.La Hey E, de Jong PT, Kijlstra A. Fuchs' heterochromic cyclitis: Review of the literature on the pathogenetic mechanisms. Br J Ophthalmol. 1994;78:307–12. doi: 10.1136/bjo.78.4.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Basarir B, Altan C, Pinarci EY, Celik U, Satana B, Demirok A. Analysis of iris structure and iridocorneal angle parameters with anterior segment optical coherence tomography in Fuchs' uveitis syndrome. Int Ophthalmol. 2013;33:245–50. doi: 10.1007/s10792-012-9680-8. [DOI] [PubMed] [Google Scholar]
- 35.Bloch-Michel E, Frau E, Chhor S, Tounsi Y. Amsler's sign associated significantly with Fuch's heterochromic cyclitis (FHC) Int Ophthalmol. 1995;1996(19):169–71. doi: 10.1007/BF00133733. [DOI] [PubMed] [Google Scholar]
- 36.Srinivasan S, Lyall D, Kiire C. Amsler-Verrey sign during cataract surgery in Fuchs heterochromic uveitis? BMJ Case Rep. 2010;2010:bcr1120092456. doi: 10.1136/bcr.11.2009.2456. doi: 10.1136/bcr. 11.2009.2456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sleep TJ, Chisholm IH. Pre-operative hyphaema in Fuchs' heterochromic uveitis. Eye (Lond) 1999;13(Pt 5):673–4. doi: 10.1038/eye.1999.185. [DOI] [PubMed] [Google Scholar]
- 38.Callear AB, Reynolds A, Harry J, Murray PI. Iris crystals in chronic uveitis. Br J Ophthalmol. 1999;83:703–6. doi: 10.1136/bjo.83.6.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Norrsell K, Sjodell L. Fuchs' heterochromic uveitis: A longitudinal clinical study. Acta Ophthalmol. 2008;86:58–64. doi: 10.1111/j.1600-0420.2007.00990.x. [DOI] [PubMed] [Google Scholar]
- 40.Kongyai N, Sirirungsi W, Pathanapitoon K, Tananuvat N, Kunavisarut P, Leechanachai P, et al. Viral causes of unexplained anterior uveitis in Thailand. Eye (Lond) 2012;26:529–34. doi: 10.1038/eye.2011.363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.de-la-Torre A, Valdes-Camacho J, Foster CS. Bilateral herpes simplex uveitis: Review of the literature and own reports. Ocul Immunol Inflamm. 2017;25:497–502. doi: 10.3109/09273948.2016.1142572. [DOI] [PubMed] [Google Scholar]
- 42.Tabbara KF, Chavis PS. Herpes simplex anterior uveitis. Int Ophthalmol Clin. 1998;38:137–47. doi: 10.1097/00004397-199803840-00013. [DOI] [PubMed] [Google Scholar]
- 43.Tugal-Tutkun I, Otuk-Yasar B, Altinkurt E. Clinical features and prognosis of herpetic anterior uveitis: A retrospective study of 111 cases. Int Ophthalmol. 2010;30:559–65. doi: 10.1007/s10792-010-9394-8. [DOI] [PubMed] [Google Scholar]
- 44.Young RC, Hodge DO, Liesegang TJ, Baratz KH. Incidence, recurrence, and outcomes of herpes simplex virus eye disease in Olmsted County, Minnesota, 1976-2007: The effect of oral antiviral prophylaxis. Arch Ophthalmol. 2010;128:1178–83. doi: 10.1001/archophthalmol.2010.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Van der Lelij A, Ooijman FM, Kijlstra A, Rothova A. Anterior uveitis with sectoral iris atrophy in the absence of keratitis: A distinct clinical entity among herpetic eye diseases. Ophthalmology. 2000;107:1164–70. doi: 10.1016/s0161-6420(00)00115-9. [DOI] [PubMed] [Google Scholar]
- 46.Wensing B, Relvas LM, Caspers LE, Valentincic NV, Stunf S, de Groot-Mijnes JD, et al. Comparison of rubella virus- and herpes virus-associated anterior uveitis: Clinical manifestations and visual prognosis. Ophthalmology. 2011;118:1905–10. doi: 10.1016/j.ophtha.2011.03.033. [DOI] [PubMed] [Google Scholar]
- 47.Wensing B, Mochizuki M, De Boer JH. Clinical characteristics of herpes simplex virus associated anterior uveitis. Ocul Immunol Inflamm. 2018;26:333–7. doi: 10.1080/09273948.2017.1420806. [DOI] [PubMed] [Google Scholar]
- 48.Zaal MJ, Volker-Dieben HJ, D'Amaro J. Visual prognosis in immunocompetent patients with herpes zoster ophthalmicus. Acta Ophthalmol Scand. 2003;81:216–20. doi: 10.1034/j.1600-0420.2003.00057.x. [DOI] [PubMed] [Google Scholar]
- 49.Thean JH, Hall AJ, Stawell RJ. Uveitis in Herpes zoster ophthalmicus. Clin Exp Ophthalmol. 2001;29:406–10. doi: 10.1046/j.1442-9071.2001.d01-29.x. [DOI] [PubMed] [Google Scholar]
- 50.Tugal-Tutkun I, Cimino L, Akova YA. Review for disease of the year: Varicella zoster virus-induced anterior uveitis. Ocul Immunol Inflamm. 2018;26:171–7. doi: 10.1080/09273948.2017.1383447. [DOI] [PubMed] [Google Scholar]
- 51.Zandi S, Bodaghi B, Garweg JG. Review for disease of the year: Treatment of viral anterior uveitis: A perspective. Ocul Immunol Inflamm. 2018;26:1135–42. doi: 10.1080/09273948.2018.1498109. [DOI] [PubMed] [Google Scholar]
- 52.Sy A, McLeod SD, Cohen EJ, Margolis TP, Mannis MJ, Lietman TM, et al. Practice patterns and opinions in the management of recurrent or chronic herpes zoster ophthalmicus. Cornea. 2012;31:786–90. doi: 10.1097/ICO.0b013e31823cbe6a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kahloun R, Attia S, Jelliti B, Attia AZ, Khochtali S, Yahia SB, et al. Ocular involvement and visual outcome of herpes zoster ophthalmicus: Review of 45 patients from Tunisia, North Africa. J Ophthalmic Inflamm Infect. 2014;4:25. doi: 10.1186/s12348-014-0025-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kong CL, Thompson RR, Porco TC, Kim E, Acharya NR. Incidence rate of herpes zoster ophthalmicus: A retrospective cohort study from 1994 through 2018. Ophthalmology. 2020;127:324–30. doi: 10.1016/j.ophtha.2019.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lightman S, Marsh RJ, Powell D. Herpes zoster ophthalmicus: A medical review. Br J Ophthalmol. 1981;65:539–41. doi: 10.1136/bjo.65.8.539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kaufman SC. Anterior segment complications of herpes zoster ophthalmicus. Ophthalmology. 2008;115(2 Suppl):S24–32. doi: 10.1016/j.ophtha.2007.10.010. [DOI] [PubMed] [Google Scholar]
- 57.Miserocchi E, Fogliato G, Bianchi I, Bandello F, Modorati G. Clinical features of ocular herpetic infection in an italian referral center. Cornea. 2014;33:565–70. doi: 10.1097/ICO.0000000000000129. [DOI] [PubMed] [Google Scholar]
- 58.Sakai JI, Usui Y, Suzuki J, Kezuka T, Goto H. Clinical features of anterior uveitis caused by three different herpes viruses. Int Ophthalmol. 2019;39:2785–95. doi: 10.1007/s10792-019-01125-5. [DOI] [PubMed] [Google Scholar]
- 59.Babu K, Kini R, Murthy KR. Unique presentation of 3rd and 6th cranial nerve palsies, nodular scleritis and nummular keratouveitis in an immunocompetent patient following an attack of herpes zoster ophthalmicus. Ocul Immunol Inflamm. 2012;20:365–7. doi: 10.3109/09273948.2012.701702. [DOI] [PubMed] [Google Scholar]
- 60.Kestelyn P, Stevens AM, Bakkers E, Rouvroy D, Van de Perre P. Severe herpes zoster ophthalmicus in young African adults: A marker for HTLV-III seropositivity. Br J Ophthalmol. 1987;71:806–9. doi: 10.1136/bjo.71.11.806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.LoBue SA, Tailor P, Carlson SM, Mano F, Giovane RA, Schaefer E, et al. Recurrent herpes zoster ophthalmicus in a young, healthy individual taking high doses of l-Arginine. Am J Ophthalmol Case Rep. 2019;16:100547. doi: 10.1016/j.ajoc.2019.100547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Yau TH, Butrus SI. Presumed bilateral herpes zoster ophthalmicus in an AIDS patient: A case report. Cornea. 1996;15:633–4. [PubMed] [Google Scholar]
- 63.Kielar RA, Cunningham GC, Gerson KL. Occurrence of herpes zoster ophthalmicus in a child with absent immunoglobulin A and deficiency of delayed hypersensitivity. Am J Ophthalmol. 1971;72:555–7. doi: 10.1016/0002-9394(71)90852-x. [DOI] [PubMed] [Google Scholar]
- 64.Gupta N, Sachdev R, Sinha R, Titiyal JS, Tandon R. Herpes zoster ophthalmicus: Disease spectrum in young adults. Middle East Afr J Ophthalmol. 2011;18:178–82. doi: 10.4103/0974-9233.80710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.De Freitas D, Martins EN, Adan C, Alvarenga LS, Pavan-Langston D. Herpes zoster ophthalmicus in otherwise healthy children. Am J Ophthalmol. 2006;142:393–9. doi: 10.1016/j.ajo.2006.03.059. [DOI] [PubMed] [Google Scholar]
- 66.Kawali A, Mahendradas P, Sanjay S, Shetty R. Viral kerato-uveitis with choroidal vitiligo? Ocul Immunol Inflamm. 2020:1–4. doi: 10.1080/09273948.2020.1741649. doi: 10.1080/09273948.2020.1741649. [DOI] [PubMed] [Google Scholar]
- 67.Kido S, Sugita S, Horie S, Miyanaga M, Miyata K, Shimizu N, et al. Association of varicella zoster virus load in the aqueous humor with clinical manifestations of anterior uveitis in herpes zoster ophthalmicus and zoster sine herpete. Br J Ophthalmol. 2008;92:505–8. doi: 10.1136/bjo.2007.125773. [DOI] [PubMed] [Google Scholar]
- 68.Karbassi M, Raizman MB, Schuman JS. Herpes zoster ophthalmicus. Surv Ophthalmol. 1992;36:395–410. doi: 10.1016/s0039-6257(05)80021-9. [DOI] [PubMed] [Google Scholar]
- 69.Borkar DS, Tham VM, Esterberg E, Ray KJ, Vinoya AC, Parker JV, et al. Incidence of herpes zoster ophthalmicus: Results from the Pacific Ocular Inflammation Study. Ophthalmology. 2013;120:451–6. doi: 10.1016/j.ophtha.2012.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Koizumi N, Inatomi T, Suzuki T, Shiraishi A, Ohashi Y, Kandori M, et al. Clinical features and management of cytomegalovirus corneal endotheliitis: Analysis of 106 cases from the Japan corneal endotheliitis study. Br J Ophthalmol. 2015;99:54–8. doi: 10.1136/bjophthalmol-2013-304625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Babu K, Murthy GJ. Cytomegalovirus anterior uveitis in immunocompetent individuals following topical prostaglandin analogues. J Ophthalmic Inflamm Infect. 2013;3:55. doi: 10.1186/1869-5760-3-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Ashwell JD, Lu FW, Vacchio MS. Glucocorticoids in T cell development and function*. Annu Rev Immunol. 2000;18:309–45. doi: 10.1146/annurev.immunol.18.1.309. [DOI] [PubMed] [Google Scholar]
- 73.Hwang YS, Shen CR, Chang SH, Lai CC, Liu CL, Chen KJ, et al. The validity of clinical feature profiles for cytomegaloviral anterior segment infection. Graefes Arch Clin Exp Ophthalmol. 2011;249:103–10. doi: 10.1007/s00417-010-1510-y. [DOI] [PubMed] [Google Scholar]
- 74.Hsiao YT, Kuo MT, Chiang WY, Chao TL, Kuo HK. Epidemiology and clinical features of viral anterior uveitis in southern Taiwan-diagnosis with polymerase chain reaction. BMC Ophthalmol. 2019;19:87. doi: 10.1186/s12886-019-1093-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Touhami S, Qu L, Angi M, Bojanova M, Touitou V, Lehoang P, et al. Cytomegalovirus anterior uveitis: Clinical characteristics and long-term outcomes in a french series. Am J Ophthalmol. 2018;194:134–42. doi: 10.1016/j.ajo.2018.07.021. [DOI] [PubMed] [Google Scholar]
- 76.Takase H, Kubono R, Terada Y, Imai A, Fukuda S, Tomita M, et al. Comparison of the ocular characteristics of anterior uveitis caused by herpes simplex virus, varicella-zoster virus, and cytomegalovirus. Jpn J Ophthalmol. 2014;58:473–82. doi: 10.1007/s10384-014-0340-6. [DOI] [PubMed] [Google Scholar]
- 77.Miyazaki D, Shimizu D, Shimizu Y, Inoue Y, Inoue T, Higaki S, et al. Diagnostic efficacy of real-time PCR for ocular cytomegalovirus infections. Graefes Arch Clin Exp Ophthalmol. 2018;256:2413–20. doi: 10.1007/s00417-018-4111-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Teoh SB, Thean L, Koay E. Cytomegalovirus in aetiology of Posner-Schlossman syndrome: Evidence from quantitative polymerase chain reaction. Eye (Lond) 2005;19:1338–40. doi: 10.1038/sj.eye.6701757. [DOI] [PubMed] [Google Scholar]
- 79.Markomichelakis NN, Canakis C, Zafirakis P, Marakis T, Mallias I, Theodossiadis G. Cytomegalovirus as a cause of anterior uveitis with sectoral iris atrophy. Ophthalmology. 2002;109:879–82. doi: 10.1016/s0161-6420(02)00961-2. [DOI] [PubMed] [Google Scholar]
- 80.van Boxtel LA, van der Lelij A, van der Meer J, Los LI. Cytomegalovirus as a cause of anterior uveitis in immunocompetent patients. Ophthalmology. 2007;114:1358–62. doi: 10.1016/j.ophtha.2006.09.035. [DOI] [PubMed] [Google Scholar]
- 81.Khodadoust AA, Attarzadeh A. Presumed autoimmune corneal endotheliopathy. Am J Ophthalmol. 1982;93:718–22. doi: 10.1016/0002-9394(82)90466-4. [DOI] [PubMed] [Google Scholar]
- 82.Xi L, Zhang L, Fei W. Cytomegalovirus-related uncontrolled glaucoma in an immunocompetent patient: A case report and systematic review. BMC Ophthalmol. 2018;18:259. doi: 10.1186/s12886-018-0917-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Miyanaga M, Sugita S, Shimizu N, Morio T, Miyata K, Maruyama K, et al. A significant association of viral loads with corneal endothelial cell damage in cytomegalovirus anterior uveitis. Br J Ophthalmol. 2010;94:336–40. doi: 10.1136/bjo.2008.156422. [DOI] [PubMed] [Google Scholar]
- 84.Wong MH, Cheung GC, Chee SP. Posterior segment findings of ocular cytomegalovirus infection in immunocompetent patients. Graefes Arch Clin Exp Ophthalmol. 2014;252:1811–6. doi: 10.1007/s00417-014-2743-y. [DOI] [PubMed] [Google Scholar]
- 85.Suzuki J, Goto H, Komase K, Abo H, Fujii K, Otsuki N, et al. Rubella virus as a possible etiological agent of Fuchs heterochromic iridocyclitis. Graefes Arch Clin Exp Ophthalmol. 2010;248:1487–91. doi: 10.1007/s00417-010-1434-6. [DOI] [PubMed] [Google Scholar]
- 86.de Visser L, Braakenburg A, Rothova A, de Boer JH. Rubella virus-associated uveitis: Clinical manifestations and visual prognosis. Am J Ophthalmol. 2008;146:292–7. doi: 10.1016/j.ajo.2008.04.011. [DOI] [PubMed] [Google Scholar]
- 87.Murray PI, Hoekzema R, van Haren MA, de Hon FD, Kijlstra A. Aqueous humor interleukin-6 levels in uveitis. Invest Ophthalmol Vis Sci. 1990;31:917–20. [PubMed] [Google Scholar]
- 88.Murray PI, Hoekzema R, Luyendijk L, Konings S, Kijlstra A. Analysis of aqueous humor immunoglobulin G in uveitis by enzyme-linked immunosorbent assay, isoelectric focusing, and immunoblotting. Invest Ophthalmol Vis Sci. 1990;31:2129–35. [PubMed] [Google Scholar]
- 89.Khairallah M, Mahendradas P, Curi A, Khochtali S, Cunningham ET., Jr Emerging viral infections causing anterior uveitis. Ocul Immunol Inflamm. 2019;27:219–28. doi: 10.1080/09273948.2018.1562080. [DOI] [PubMed] [Google Scholar]
- 90.Mahendradas P, Shetty R, Malathi J, Madhavan HN. Chikungunya virus iridocyclitis in Fuchs' heterochromic iridocyclitis. Indian J Ophthalmol. 2010;58:545–7. doi: 10.4103/0301-4738.71707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Babu K, Murthy GJ. Chikungunya virus iridocyclitis in Fuchs' heterochromic iridocyclitis. Indian J Ophthalmol. 2012;60:73–4. doi: 10.4103/0301-4738.90495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Usui M, Sakai J. Three cases of EB virus-associated uveitis. Int Ophthalmol. 1990;14:371–6. doi: 10.1007/BF00163559. [DOI] [PubMed] [Google Scholar]
- 93.Yoshimura K, Mochizuki M, Araki S, Miyata N, Yamaguchi K, Tajima K, et al. Clinical and immunologic features of human T-cell lymphotropic virus type I uveitis. Am J Ophthalmol. 1993;116:156–63. doi: 10.1016/s0002-9394(14)71279-6. [DOI] [PubMed] [Google Scholar]
- 94.Jampol LM, Goldstein DA. Zika Virus infection and the eye. JAMA Ophthalmol. 2016;134:535–6. doi: 10.1001/jamaophthalmol.2016.0284. [DOI] [PubMed] [Google Scholar]
- 95.Shantha JG, Crozier I, Hayek BR, Bruce BB, Gargu C, Brown J, et al. Ophthalmic manifestations and causes of vision impairment in Ebola virus disease survivors in monrovia, liberia. Ophthalmology. 2017;124:170–7. doi: 10.1016/j.ophtha.2016.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Maini R, Edelsten C. Uveitis associated with parvovirus infection. Br J Ophthalmol. 1999;83:1403–4. doi: 10.1136/bjo.83.12.1403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Kavitha S, Patel SR, Mohini P, Venkatesh R, Sengupta S. Vitiligo iridis and glaucoma: A rare sequelae of small pox. Eye (Lond) 2015;29:1392–4. doi: 10.1038/eye.2015.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.De Groot-Mijnes JD, Rothova A, Van Loon AM, Schuller M, Ten Dam-Van Loon NH, De Boer JH, et al. Polymerase chain reaction and Goldmann-Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am J Ophthalmol. 2006;141:313–8. doi: 10.1016/j.ajo.2005.09.017. [DOI] [PubMed] [Google Scholar]
- 99.Pathanapitoon K, Riemens A, Kongyai N, Sirirungsi W, Leechanachai P, Ausayakhun S, et al. Intraocular and plasma HIV-1 RNA loads and HIV uveitis. AIDS. 2011;25:81–6. doi: 10.1097/QAD.0b013e328340fe91. [DOI] [PubMed] [Google Scholar]
- 100.Yokogawa H, Kobayashi A, Sugiyama K. Mapping owl's eye cells of patients with cytomegalovirus corneal endotheliitis using in vivo laser confocal microscopy. Jpn J Ophthalmol. 2013;57:80–4. doi: 10.1007/s10384-012-0189-5. [DOI] [PubMed] [Google Scholar]
- 101.Shiraishi A, Hara Y, Takahashi M, Oka N, Yamaguchi M, Suzuki T, et al. Demonstration of “owl's eye” morphology by confocal microscopy in a patient with presumed cytomegalovirus corneal endotheliitis. Am J Ophthalmol. 2007;143:715–7. doi: 10.1016/j.ajo.2006.11.026. [DOI] [PubMed] [Google Scholar]
- 102.Doan T, Acharya NR, Pinsky BA, Sahoo MK, Chow ED, Banaei N, et al. Metagenomic DNA sequencing for the diagnosis of intraocular infections. Ophthalmology. 2017;124:1247–8. doi: 10.1016/j.ophtha.2017.03.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Lu LM, McGhee CNJ, Sims JL, Niederer RL. High rate of recurrence of herpes zoster-related ocular disease after phacoemulsification cataract surgery. J Cataract Refract Surg. 2019;45:810–5. doi: 10.1016/j.jcrs.2019.01.003. [DOI] [PubMed] [Google Scholar]
- 104.Cobo LM, Foulks GN, Liesegang T, Lass J, Sutphin JE, Wilhelmus K, et al. Oral acyclovir in the treatment of acute herpes zoster ophthalmicus. Ophthalmology. 1986;93:763–70. doi: 10.1016/s0161-6420(86)33678-9. [DOI] [PubMed] [Google Scholar]
- 105.Wong VW, Chan CK, Leung DY, Lai TY. Long-term results of oral valganciclovir for treatment of anterior segment inflammation secondary to cytomegalovirus infection. Clin Ophthalmol. 2012;6:595–600. doi: 10.2147/OPTH.S30476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Faulds D, Heel RC. Ganciclovir. A review of its antiviral activity, pharmacokinetic properties and therapeutic efficacy in cytomegalovirus infections. Drugs. 1990;39:597–638. doi: 10.2165/00003495-199039040-00008. [DOI] [PubMed] [Google Scholar]
- 107.Harada Y, Fukuda K, Nakahira A, Tada K, Sumi T, Fukushima A. Requirement of longer term antiviral therapy in patients with cytomegalovirus anterior uveitis with corneal endothelial cell damage. Clin Ophthalmol. 2018;12:1311–6. doi: 10.2147/OPTH.S164184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Chee S-P, Jap A. Cytomegalovirus anterior uveitis: Outcome of treatment. Br J Ophthalmol. 2010;94:1648–52. doi: 10.1136/bjo.2009.167767. [DOI] [PubMed] [Google Scholar]
- 109.Waduthantri S, Zhou L, Chee S-P. Intra-cameral level of ganciclovir gel, 0.15% following topical application for cytomegalovirus anterior segment infection: A pilot study. PLoS One. 2018;13:e0191850. doi: 10.1371/journal.pone.0191850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Takhar JS, Joye AS, Somkijrungroj T, Laovirojjanakul W, Lin CP, Lietman TM, et al. A double masked randomised 4-week, placebo-controlled study in the USA, Thailand and Taiwan to compare the efficacy of oral valganciclovir and topical 2% ganciclovir in the treatment of cytomegalovirus anterior uveitis: Study protocol. BMJ Open. 2019;9:e033175. doi: 10.1136/bmjopen-2019-033175. [DOI] [PMC free article] [PubMed] [Google Scholar]