

Abstract
Aims
The COVID-19 pandemic has had a significant impact on the provision of orthopaedic care across the UK. During the pandemic orthopaedic specialist registrars were redeployed to “frontline” specialties occupying non-surgical roles. The impact of the COVID-19 pandemic on orthopaedic training in the UK is unknown. This paper sought to examine the role of orthopaedic trainees during the COVID-19 and the impact of COVID-19 pandemic on postgraduate orthopaedic education.
Methods
A 42-point questionnaire was designed, validated, and disseminated via e-mail and an instant-messaging platform.
Results
A total of 101 orthopaedic trainees, representing the four nations (Wales, England, Scotland, and Northern Ireland), completed the questionnaire. Overall, 23.1% (23/101) of trainees were redeployed to non-surgical roles. Of these, 73% (17/23) were redeployed to intensive treatment units (ITUs), 13% (3/23) to A/E, and 13%(3/23%) to general medicine. Of the trainees redeployed to ITU 100%, (17/17) received formal induction. Non-deployed or returning trainees had a significant reduction in sessions. In total, 42.9% (42/101) % of trainees were not timetabled into fracture clinic, 53% (53/101) of trainees had one allocated theatre list per week, and 63.8%(64/101) of trainees did not feel they obtained enough experience in the attached subspecialty and preferred repeating this. Overall, 93% (93/101) of respondents attended at least one weekly online webinar, with 79% (79/101) of trainees rating these as useful or very useful, while 95% (95/101) trainees attended online deanery teaching which was rated as more useful than online webinars (p = 0.005)
Conclusion
Orthopaedic specialist trainees occupied an important role during the COVID-19 pandemic. COVID-19 has had a significant impact on orthopaedic training. It is imperative this is properly understood to ensure orthopaedic specialist trainees achieve competencies set out in the training curriculum.
Cite this article: Bone Joint Open 2020;1-11:676–682.
Keywords: COVID-19, Surgical Training, Pandemic surgery, Redeployment, Postgraduate education
Introduction
The COVID-19 pandemic has had a significant impact on the provision of standard healthcare across the UK.1 As of 18 June 2020, there are a recorded 299,251 laboratory confirmed COVID-19 cases and 42,153 COVID-19 associated deaths in the UK.2 Numerous published accounts in the literature describe how various orthopaedic departments, both large university hospitals and district general hospitals, have restructured their workforce to face this pandemic.3-6 This has permitted adjustment to a “new normal”, to provide support to “frontline” staff treating critically unwell patients with coronavirus.
With terminology akin to the military, trainees specializing in orthopaedics and other surgical specialties were “redeployed” to increase the capacity of frontline specialties.4 Orthopaedic specialist registrars were tasked with temporarily extending their scope of practice through new non-surgical roles.7 Published accounts in the literature, in the UK and overseas, describe the important roles orthopaedic specialist trainees occupied in intensive care units (ICU) through tasks such as “proning” and peripheral line insertion of patients unwell with COVID-19. 4-6,8
The provision of formal teaching and training of surgeons has also been negatively impacted during this of pandemic. As the UK government advocated two-metre social distancing and travel limited to “essential-only”, the continuation of deanery teaching, courses, conferences, and postgraduate examinations was unjustifiable during the COVID-19 pandemic.9,10 The orthopaedic community rapidly adapted to this changing environment, as the rise of online group video platforms such as Zoom connected orthopaedic trainees with their mentors, obviating the need for travel and clustering in a classroom. Formal orthopaedic education could proceed through deanery teaching and online webinars using these platforms.10
To the authors’ knowledge, the distribution of orthopaedic trainees redeployed across the four nations in the UK (England, Wales, Scotland, and Northern Ireland) during the COVID-19 pandemic remains unpublished. The collective gain of new skills and potential loss of expertise due to prolonged redeployment is also unclear and undocumented. The role and benefit of online interactive educational platforms in formal orthopaedic education also requires further investigation.
This paper describes the results of a survey distributed among orthopaedic specialist registrars across the UK. The primary aim was to characterize the role orthopaedic registrars occupied during the COVID-19 pandemic. Secondary aims were to assess the impact of COVID-19 on their training progression and Orthopaedic trainees’ experience of online interactive educational platforms.
Methods
A questionnaire was designed by the first and second authors (GG, KR) and reviewed and edited for content and construct validity by four orthopaedic specialist registrars and supervising orthopaedic consultants (RG, JB, KR, AK, NS, HP). A pilot survey was conducted with six orthopaedic registrars to assess for time taken to complete survey, need and relevance of study. The survey was developed using an open access online survey (Googleforms).11
The survey was circulated to all training programme directors in the UK to distribute among their respective trainees. Group-instant messaging platforms like WhatsApp were used to contact trainees from various deaneries to distribute among their colleagues. The survey was open between May 18 2020 and 11 June 2020. Partially completed questionnaires were not permitted. No financial incentives were provided for participation.
The survey was divided into three sections. An initial six-point questions explored participant demographics, training region, and role during the COVID-19 pandemic. Depending on the participant’s response to their role in the COVID-19 pandemic (redeployed to intensive treatment unit (ITU), redeployed to the accident and emergency (A&E) department, redeployed to medicine, returned/remained within orthopaedics), the participant was directed to answer a 19-point section related to their role. A final 17-point section was related to impact of the COVID-19 pandemic on orthopaedic training.
For continuous variables, results are expressed as means and standard deviations and for categorical variables as counts and percentages. The denominator for percentages is the full respondent cohort unless otherwise specified. Likert data descriptive statistics was used in data analysis in the form of median, mean, and standard deviation. Likert scales throughout the questionnaire were taken from 1 to 5, 5 being in most agreement with the statement and 1 least agreement. The Kruskal-Wallis rank sum test was performed to assess statistically significant differences between subgroups. A p-value of < 0.05 was considered as statistically significant.
All analyses were performed using the R 3.6.2 programme via RStudio for Windows, R Core Team (2013) by the first author (GG).12 Graphs presented in this article were generated using Microsoft Excel (Redmond, Washington, USA).
Results
A total of 101 participants completed the questionnaire, demographics of respondents are presented in Table I. Trainees from all four home nations completed the survey. Percentage of respondents and respective deaneries are presented in respective tables and figures (Table I and Figures 1 and 2) The range of trainees completing the questionnaire were from ST1 to ST8 and post-Certificate of Completion of Training (CCT) fellow. ST1/ST2 trainees who completed the survey were trainees on run-through programmes (Scotland deanery), and 2%(2/101) of participants were post-CCT fellows.
Table I.
Questions related to experience of orthopaedic trainees redeployed to intensive treatment units.
| Demographics | Total |
|---|---|
| Age group, n (%) | |
| 25 to 30 | 22 (21.6) |
| 30 to 35 | 52 (51) |
| 35 to 40 | 16 (15.7) |
| > 40 | 12 (11.8) |
| Sex, n (%) | |
| Male | 87 (85.3) |
| Female | 15 (14.7) |
ITU, intensive treatment unit.
Fig. 1.
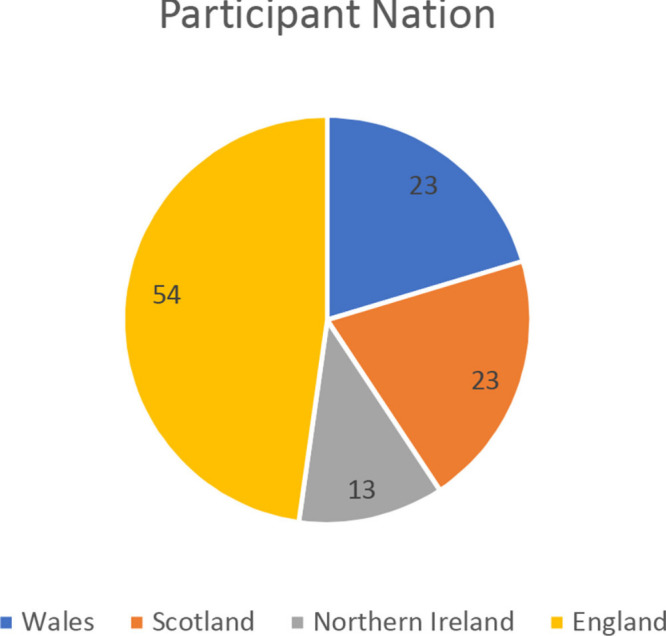
Distribution of responses from the four respective nations.
Fig. 2.
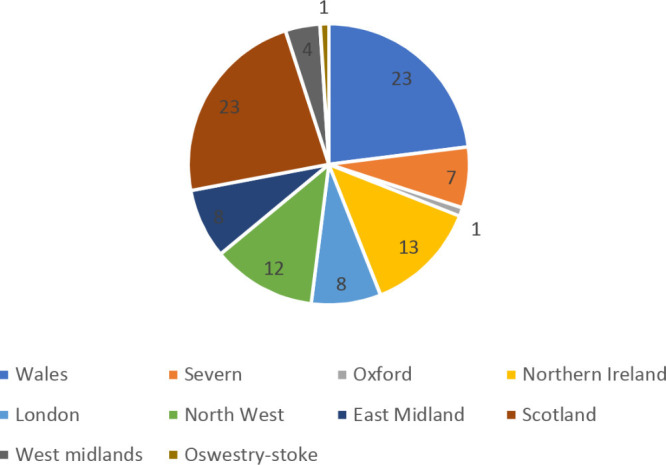
Distribution of responses from respective postgraduate deaneries.
A total of 77.2% (78/101) trainees remained within their parent speciality during the acute period of COVID-19 in the UK, with 22.7%(23/101) of trainees were redeployed to other specialties. Of these, 73% (17/23) were redeployed to ITU, 13%(3/23) were redeployed to A&E, and 13% (3/23) were redeployed to medicine.
Trainees redeployed to ITU
The duration of redeployment varied from two weeks to two months, and the majority 52.9% (9/17) were redeployed for four weeks (Figure 3). Overall, 94.1% (16/17) participants were informed a minimum a week in advance prior to deployment and 58.8% (10/17) had mandatory redeployment while 41.2% (7/17) had been voluntarily redeployed.
Fig. 3.
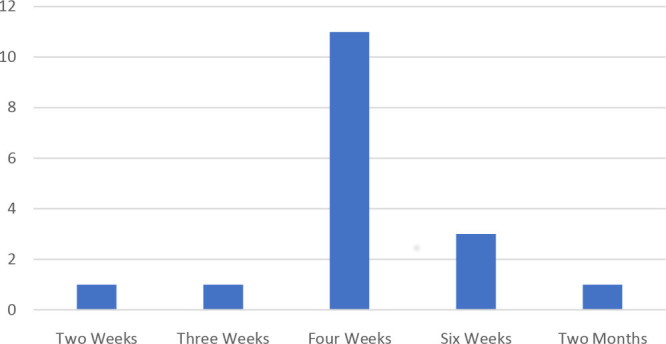
Duration of trainee redeployment to intensive treatment unit (ITU) during the COVID-19 pandemic.
All trainees (17/17) received departmental induction prior to redeployment. Most participants received training on correct “donning and doffing” of personal protective equipment (PPE), proning and supineing. A minority received training on intubation, ventilator trouble shooting and critical care training and while 29.4% (5/17) had prior critical care experience , 70.6% (12/17) reported no prior experience (Figure 4).
Fig. 4.
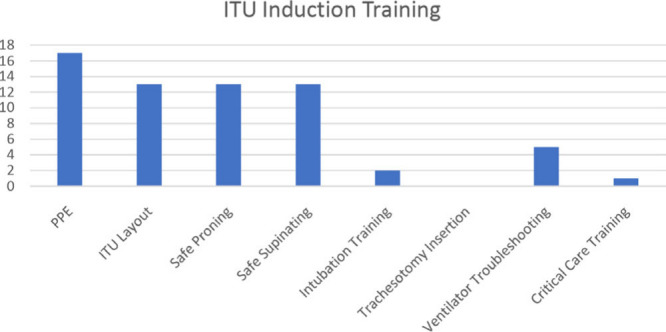
Topics covered during intensive treatment unit (ITU) induction training. PPE, personal protective equipment.
Of trainees redeployed to ITU 76.5% (13/17,) felt they had adequate training regarding PPE, while 23.9% (4/17) did not feel this was adequate. Results of Likert-style questions relating to the trainee experience of redeployment to ITU are presented in Table II.
Table II.
Likert questions related to experience of orthopaedic trainees redeployed to intensiive treatment unit (ITU), with 5 being in most agreement with the statement and 1 least agreement.
| Questions (n = 17) | 5 (%) | 4 (%) | 3 (%) | 2 (%) | 1 (%) | Mean (SD) | Median |
|---|---|---|---|---|---|---|---|
| How comfortable did you feel being redeployed to a COVID ITU environment? | 0 | 3 (17.6) | 4 (23.5) | 10 (58.8) | 0 | 2.58 (0.919) | 2 |
| How useful did you think you would be PRIOR TO REDEPLOYMENT in ITU? | 0 | 3 (17.6) | 3 (17.6) | 8 (47.1) | 3 (17.6) | 2.35 (0.99) | 2 |
| How useful did you feel you WERE in a COVID-19 ITU setting? | 1 (5.9) | 7 (41.2) | 4 (23.5) | 1 (5.9) | 4 (23.5) | 3.00 (1.32) | 3 (p = 0.702*) |
| How useful has the ITU redeployment been to your training? | 0 | 3 (17.6) | 5 (29.4) | 6 (35.3) | 3 (17.6) | 2.47 (1.007) | 2 |
Kruskal-Wallis rank sum test.
ITU, intensive treatment unit.
The most common task performed by redeployed orthopaedic trainees in ITU was proning and supineing patients (94%; 16/17). No orthopaedic trainee was tasked with advanced airway skills (intubation and front of neck access). New skills such as arterial line and central line insertion were also performed by redeployed orthopaedic trainees at 47% (8/17) and 35% (6/17), respectively (Figure 5).
Fig. 5.
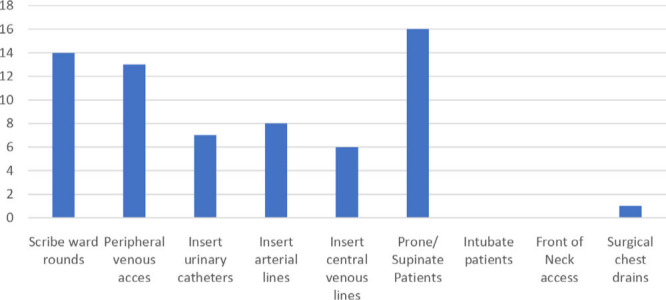
Tasks performed in ITU by redeployed Orthopaedic Specialist Trainees.
Trainees redeployed to A&E
Redeployment of trainees to A&E did not exceed three weeks. All trainees were informed more than a week in advance of redeployment. In total, 66.7% (2/3) attended departmental induction while 33.3% (1/3) did not have induction. Training consisted of overview of department, correct application of personal protective equipment, arterial blood gas analysis and assessment of medically unwell patients.
Most trainees reported being “comfortable” working in A&E on the 5-point Likert scale. No trainees felt that redeployment to A&E was beneficial to their training. None of the trainees recorded their experience on intercollegiate surgical curriculum programme (ISCP) through a formal placement or through workplace-based assessments (WBAs). Results of Likert-style questions relating to the trainee experience of redeployment to A&E is presented in Table III.
Table III.
Questions related to experience of orthopaedic trainees redeployed to the accident and emergency department (A&E), with 5 being in most agreement with the statement and 1 least agreement.
| Questions (n = 3) | 5 (%) | 4 (%) | 3 (%) | 2 (%) | 1 (%) | Mean (SD) | Median |
|---|---|---|---|---|---|---|---|
| How comfortable did you feel being redeployed to a COVID A&E environment? | 0 | 2 (66.7) | 1 (33.3) | 0 | 0 | 3.6 (0.57) | 4 |
| How useful did you think you would be PRIOR TO REDEPLOYMENT in A&E? | 0 | 2 (66.7) | 0 | 1 (33.3) | 0 | 3.33 (1.16) | 4 |
| How useful did you feel you WERE in a COVID-19 A&E setting? | 0 | 2 (66.7) | 1 (33.3) | 0 | 0 | 3.6 (0.57) | 4 |
| How useful has the A&E redeployment been to your training? | 0 | 0 | 0 | 1 (33.3) | 2 (66.7) | 1.33 (0.577) | 1 |
Likert score: 5, agree with statement; 1, disagree with statement.
Trainees redeployed to medicine
From the 3% of participants who were redeployed to medicine, 66.7% (2/3) redeployments exceeded five weeks while one trainee described alternate weeks in medicine and in orthopaedics. All trainees (3/3) were informed a week in advance of their redeployment and noted that redeployment was mandatory.
None of the trainees redeployed to medicine were offered an induction nor underwent departmental training. Tasks performed by orthopaedic trainees included: scribing ward rounds, performing peripheral venous cannulas, arterial blood gas testing, and reviewing medically unwell patients. No trainees felt that redeployment to medicine was beneficial to their training.
Experience in orthopaedics
All trainees who completed the questionnaire had returned to their parent speciality: 6% (6/101) of respondents undertook more than three theatre sessions per week, while 94% (93/101) of trainees were timetabled for less than two theatre session per week. In total, 57.1% (56/101) of trainees were timetabled to attend clinic while 42.9% (42/101) of trainees did not have any clinic commitments, and 50% (50/101) of trainees’ stated that they were involved in virtual or telephone clinics.
Overall, 73% (72/101) of trainees did not feel they advanced their operative skills. Only 11% (11/101) felt they had advanced in their operative skills during this period while 15.4% (15/101) were unsure, and 76.1% (76/101) did not feel they advanced the clinical skills during the COVID-19 pandemic.
A subgroup analysis comparing the operative experience of trainees redeployed versus who remained within orthopaedics was carried out (Table IV). There were no statistically significant differences in operative experience between both groups during the COVID-19 pandemic.
Table IV.
Comparison of orthopaedic experience between redeployed and non-redeployed trainees, with 5 being in most agreement with the statement and 1 least agreement.
| Questions | Redeployed during COVID-19 pandemic (n = 33) | Median | Mean (SD) | Remained within orthopaedics (n = 78) | Median | Mean (SD) | p-value* | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Timetable theatre sessions | 4 (three theatre sessions), % | 3 (two theatre sessions), % | 2 (one theatre session), % | 1 (no theatre sessions), % | 4 (three theatre sessions), % | 3 (two theatre sessions), % | 2 (one theatre session), % | 1 (no theatre sessions), % | |||||
| Response | 4.34 | 26 | 56 | 13 | 2 | 2.72 (0.70) | 5 | 19.3 | 55 | 20.5 | 2 | 2.089 (0.77) | 0.89 |
| Cases performed perform as TS/TU/P | 4 (same caseload to pre-COVID), % | 3 (50% to 75% of cases), % | 2 (25% to 50% of cases), % | 1 (all cases performed by consultant), % | 4 (same caseload to pre-COVID), % | 3 (50% to 75% of cases), % | 2 (25% to 50% of cases), % | 1 (all cases performed by consultant), % | |||||
| Response | 8.7 | 39.1 | 43 | 4.34 | 2.5 | 2.54 (0.73) | 23.07 | 23.07 | 34.6 | 15 (19.23) | 2 | 2.5 (1.05) | 0.850 |
| Cases performed since official lockdown | 4 ( > 75), % | 3 (50 to 25), % | 2 (25 to 0), % | 1 (0 cases), % | 4 ( > 75), % | 3 (50 to 25), % | 2 (25 to 0), % | 1 (0 cases), % | |||||
| Response | 0 | 13 | 87 | 4.35 | 2 | 2.09 (0.42) | 3.9 | 18 | 64 | 14.1 | 2 | 2.11 (0.68) | 0.210 |
| How useful did you feel during the COVID-19 pandemic? | 4 (very useful), % | 3 (useful), % | 2 (not useful), % | 1 (not useful at all), % | 4 (very useful), % | 3 (useful), % | 2 (not useful), % | 1 (not useful at all), % | |||||
| Response | 39 | 47.8 | 13 | 0 | 3 | 3.13 (0.64) | 42 | 39 | 9 | 9 | 3 | 3.15 (0.93) | 0.220 |
Kruskal-Wallis rank sum test.
Orthopaedic trainees formal training experience
Overall, 93% (92/101) of participants stated they attended deanery arranged teaching through online group video methods; 81% of participants used Zoom as the most popular platform followed by 11% utilizing “GoToMeeting”. Over a 5-point likert scale, 38% (37/101) found teaching very useful and 41%(41/101) useful with median of 4 and mean 3.97 (SD 1.13.)
At the time of completion of this survey 70.6% (71/101) participants had been informed by their TPD regarding the planned rotations; 73% (52/71) confirmed that they would rotate hospital and subspecialty, 12.7%(9/71) informed that they will remain in the same hospital but rotate speciality, 9.9% (7/71) that they will rotate hospital but repeat the same speciality, 4.4% (3/71) had been informed that they will repeat the same hospital and rotations.
In all, 63.8% (64/101) of trainees stated they did not have enough exposure and would prefer to repeat the same sub-specialty again or later in their training; 36.3% (37/101) of trainees deemed they had sufficient exposure in the subspecialty they were attached to and preferred rotating hospital and speciality, and 85% (86/101) of trainees responded that they preferred progressing to the next respective grade. Of the 15% (15/101) of trainees who preferred deferring progression, 60% (9/15) stated they preferred an ARCP in six months while 40% (6/15) preferred a repeat ARCP in 12 months.
Trainees' views on online orthopaedic webinars
Overall, 92% (93/101) of trainees attended online orthopaedic webinars in addition to regular deanery teaching; 70.8% (71/101) attended one webinar a week, 18% (18/101) twice a week, and 11.2% (12/101) three times a week. In total, 39.8% (40/101) stated they recorded attendance of online orthopaedic webinars on their ISCP (intercollegiate surgical curriculum programme). Over a 5 point likert scale, 20% 21/101 rated webinars “very useful,” 41% (41/101) rated webinars “useful” while a median of 4 and mean of 3.7 (SD 0.93.) Trainees experience of deanery teaching achieved a higher mean likert score as compared to online webinars which was statistically significant (p < 0.001).
Trainees were more likely to attend online webinars advertised through their registrar WhatsApp group and by their TPD (Figure 6). 90% (90/101) of participants responded that webinars should proceed following the COVID-19 pandemic, 9.2% (10/101) responded maybe and 1% (1/101) disagreed.
Fig. 6.
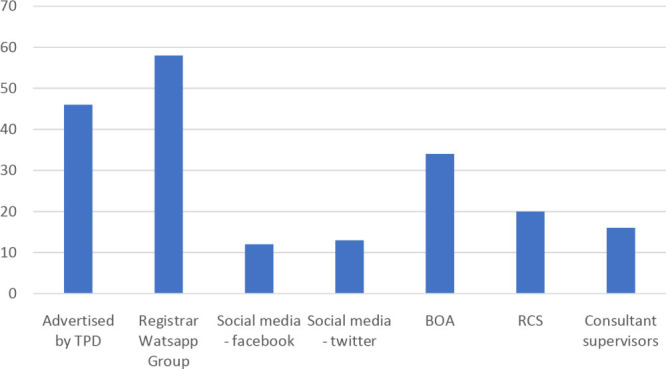
Advertisement of online orthopaedic webinars. BOA – British Orthopaedic Association. RCS- Royal College of Surgeons.
Discussion
The disruption of trauma and orthopaedic care in the UK during the COVID-19 pandemic has now been well recorded in medical literature. Detailed descriptions of departmental restructuring, redeployment of orthopaedic surgeons in training and complete cancellation of routine elective operations have been described as measures taken during this pandemic.3–6,13–16 The impact of national lockdown had notably diminished the trauma workload during this period. In Scotland a 27% reduction in operative cases performed 23 March and 28 March 2020 in comparison to the previous year was reported as a result of national lockdown.17 The repercussions of these cumulative effects of current orthopaedic surgeons in training is unknown and unquantified.
As with other surgical specialties, orthopaedic trainees were “redeployed” to various non-surgical frontline specialties responsible for caring of increasing number of patients with COVID-19. In our survey 25% of respondents had been redeployed, ITU being the common area of redeployment of orthopaedic trainees.4,14. A total of 16 orthopaedic trainees occupied a supportive role, generally through completion of ancillary tasks. Overeall, 47% of trainees reported the opportunity to gain practical skills such as arterial line and central lines. In our survey, most trainees expressed low levels of comfort of being redeployed and did not feel that this enhanced their training. Some trainees did express in free comment text boxes that this experience did enhance their understanding of critical care and would enhance multidisciplinary communication when managing polytrauma patients.
Other surgical specialties reported a higher proportion of redeployment compared to trauma and orthopaedics. In a survey involving cardiothoracic 66% of trainees were redeployed to ITU. This may be due to an ongoing clinical demand for trauma care and less adaptability of orthopaedic training to the critical care environment.18
The clinical activity of trainees who were not redeployed or had returned from redeployment to orthopaedic trainees was also significantly impacted. 50% of trainees were not timetabled to outpatient clinic (fracture or elective) and were timetabled for one trauma list per week. 25% of trainees were not timetabled to any theatre lists but were tasked to occupy more junior positions through ward support. Most cases which were previously performed by trainees, were performed by consultants, as demonstrated by 66% reduction of allocated cases to trainees. Our survey showed no statistically significant differences in operative exposure between trainees who were redeployed compared to trainees who remained within orthopaedics showing the scale of overall reduction in operative work.
While clinical and operative exposure were significantly impacted during the pandemic, formal orthopaedic education rapidly adapted. 93% of responded replied that their deaneries had adapted towards online group discussion platforms, with Zoom being the most popular platform. Formal teaching continued to be of high quality as this was positively rated by trainees across all regions. Didactic teaching was moreover supplemented by online webinars organized by various specialist societies as 70% of trainees attended at least one webinar a week which were also highly rated by trainees.
Completion of orthopaedic training requires trainees to demonstrate competencies through completing a set number of procedures and verified by workplace-based assessments.19,20 It is unclear whether trainees impacted by the COVID-19 pandemic will achieve this during a their allocated training time or whether extended training time will be required. 63.8% of UK based trainees preferred repeating the sub-specialty they were rotating through during the pandemic and 15% of trainees preferred deferring progression.
A similar survey investigating the impact of the COVID-19 pandemic on European orthopaedic was published by the European federation of orthopaedic surgeons (FORTE.) This had similar results to our survey with trainees impacted with redeployment and diminished operative opportunities through cancellation of elective cases and reduction in trauma load. 20% of European orthopaedic trainees were redeployed to settings outside of orthopaedics. 58.2% of the European cohort were concerned about achieving annual training goals. UK orthopaedic training stands out in comparison with the persistence of didactic teaching programmes, while 52% of European trainees reported a reduction of faculty-led education.21,22
To the authors’ knowledge, this is the first published survey investigating the impact of the COVID-19 pandemic on orthopaedic training in the UK. The authors recognize that while there is a wide distribution of participants the sample size is small in certain regions due to poor uptake which may affect the generalisability of results. The survey does not capture how orthopaedic trainees have utilized time out during the pandemic. This time may have been used by trainees towards self-directed learning, following online webinars and completion of quality improvement and research projects.
Further study is required to fully understand the impact of COVID-19 pandemic on orthopaedic training. This is essential for key stakeholders to ensure any deficiencies are overcome and that training programs continue to produce high-quality consultant orthopaedic surgeons. A recommended study by the authors would be a comparison of logbook data and workplace-based assessments (WBA) of a cohort of trainees to a similar matched cohort a year prior in a pre-COVID environment.
It is evident that the COVID-19 pandemic has had a significant impact on orthopaedic training. It is important that this impact is properly understood to ensure orthopaedic specialist trainees achieve competencies set out in the training curriculum.
Acknowledgements
The authors would like the acknowledge the contribution of Alice Campion, Abhijeet Kumar, Ahmed Abdelaal, Matthew Horner, Simon Aquilina, Matthew Farrugia and Martinique Vella Baldachino in designing and distributing the survey.
Footnotes
Author contributions: G. Gonzi: Designed the study, Designed the survey, Analyzed the data and statistics, Wrote and revised manuscript.
R. Gwyn: Designed the study, Analyzed the data, Wrote and revised the manuscript.
K. Rooney: Designed the survey, Analyzed the data, Revised the manuscript.
J. Boktor: Piloted the survey, Analyzed the data, Revised the manuscript.
N. C. Sciberras: Designed the survey, Analyzed the data, Revised the manuscript.
H. Pullen: Designed the study, Revised the manuscript.
K. Mohanty: Designed study, revised manuscript, overall supervision.
Funding statement: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Twitter: Follow G. Gonzi @GonziGianluca
Follow R. Gwyn @rhodrigwyn
References
- 1. COVIDSurg Collaborative Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. United Kingdom Government Coronavirus (COVID-19) cases in the UK, 2020. [Google Scholar]
- 3. Nana S, Forrester LA, Levine WN. What’s Important: Redeployment of the Orthopaedic Surgeon During the COVID-19 Pandemic. J Bone Joint Surg Am. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Gonzi G, Gwyn R, et al. Our experience as orthopaedic registrars redeployed to the ITU emergency rota during the COVID-19 pandemic published 14 may 2020. 2020. https://www.boa.ac.uk/policy-engagement/journal-of-trauma- [DOI] [PubMed]
- 5. Dayananda KSS, Yasin T, et al. COVID-19: the impact and changes to trauma services in Cardiff. 2020. https://www.boa.ac.uk/policy-engagement/journal-of-trauma-orthopaedics/journal-of-trauma-orthopaedics-and-coronavirus/covid-19-the-impact-and-changes-to-trauma-services.html (date last accessed 19 May 2020).
- 6. Tadros BJ, Black J, Dhinsa BS. COVID-19 outbreak: the early response of a UK orthopaedic department. J Clin Orthop Trauma. 2020;11:S301–S303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. RCS England COVID-19: good practice for surgeons and surgical teams published Tuesday 31/03/2020, 2020. [Google Scholar]
- 8. Culp BM, Frisch NB. COVID-19 impact on young arthroplasty surgeons. The Journal of Arthroplasty. 2020;1:e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Public Health England COVID-19 Guidance on social distancing and for vulnerable people, 2020. [Google Scholar]
- 10. Khan A, Singh A, Pearse M. How to organise a successful orthopaedic webinar. transient Journal of orthopaedic and coronavirus. 2020. [Google Scholar]
- 11. Google Google Forms. [Internet]. 2019. https://www.google.co.uk/forms/about/
- 12. R The R Project for Statistical Computing [Internet]. 2015. https://www.r401 project.org/
- 13. Chui K, Thakrar A, Shankar S. Evaluating the efficacy of a two-site (‘COVID-19’ and ‘COVID-19-free’) trauma and orthopaedic service for the management of hip fractures during the COVID-19 pandemic in the UK. Bone & Joint Open. 2020;1(6):190–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chui K, Thakrar A, Shankar S. Evaluating the efficacy of a two-site (‘COVID-19’ and ‘COVID-19-free’) trauma and orthopaedic service for the management of hip fractures during the COVID-19 pandemic in the UK. Bone & Joint Open. 2020;1(6):190–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dyer GSM, Lipa SA, George D, Shaina l. What's important: COVID-19-Helpers, not heroes. J Bone Joint Surg Am. 2020;102(12):1032–1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sarpong NO, Forrester LA, Levine WN. What's important: redeployment of the orthopaedic surgeon during the COVID-19 pandemic: perspectives from the trenches. J Bone Joint Surg Am. 2020;102(12):1019–1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Scott CEH, Holland G, Powell-Bowns MFR, et al. Population mobility and adult orthopaedic trauma services during the COVID-19 pandemic: fragility fracture provision remains a priority. Bone & Joint Open. 2020;1(6):182–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Caruana EJ, Patel A, Kendall S, Rathinam S. Impact of coronavirus 2019 (COVID-19) on training and well-being in subspecialty surgery: a national survey of cardiothoracic trainees in the United Kingdom. J Thorac Cardiovasc Surg. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Academy of Medical Royal Colleges Plans regarding trainee redeployment during the COVID-19 pandemic. 2020. https://www.aomrc.org.uk/atdg-papers-reports/plans-regarding-trainee-redeployment-during-the-covid-19-pandemic/ (date last accessed 26/03/2020).
- 20. Joint Committee on Surgical Training Intercollegiate surgical programme (ISCP.). 2020. www.iscp.ac.uk
- 21. British Orthopaedic Association Management of patients with urgent orthopaedic conditions and trauma during the coronavirus pandemic. 2020. https://www.boa.ac.uk/resources/covid-19-boasts-combined.html (date last accessed 21/04/2020).
- 22. Megaloikonomos PD, Thaler M. Impact of the COVID-19 pandemic on orthopaedic and trauma surgery training in Europe. Int Orthop. 2020:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]