

Abstract
While fire-related deaths are regularly encountered by medical examiners, fire-related homicides are relatively uncommon. Although some large retrospective studies of fire-related deaths have been performed, few large studies have specifically reviewed fire-related homicides.
Autopsy, scene investigation, and ancillary studies were reviewed for 38 fire-related homicides evaluated at the Wayne County Medical Examiner’s Office in Detroit, Michigan.
The largest proportion of cases were inhalation-related deaths in dwelling fires (n = 21, 55%), followed by deaths from thermal injury after immolation (n = 8, 21%) and traumatic death with contemporaneous or subsequent immolation (n = 8, 21%). There was one case of postmortem immolation. Although carboxyhemoglobin (COHb) levels played a significant role in evaluation of these cases, no single factor was diagnostic of a particular cause or manner of death.
Fire-related homicides present unique diagnostic challenges because multiple insults frequently contribute to the cause death. Death at the scene and COHb level above 10% are the most useful factors in establishing smoke and soot inhalation as the cause of death. Some autopsy findings are helpful in establishing or ruling out smoke and soot inhalation as contributing to or sole cause of death, but an evaluation of the entire circumstances and autopsy findings is necessary.
Keywords: Forensic pathology, Homicide, Fire, Carbon monoxide, Trauma, Public health
Introduction
Fire is a significant cause of mortality worldwide. In the United States, approximately 2900 deaths per year occur due to structure fires and are among the most common causes of unintentional carbon monoxide poisoning (1,2). A substantial majority of fire-related deaths are accidental (3). Fire-related homicides are uncommon, with most studies reporting a rate of up to 9% of all fire-related deaths or carbon monoxide deaths, depending on the population being studied (3 -5). For the purposes of this article, we define a fire-related homicide as any homicide occurring in association with arson, accidental fire, or direct immolation of a victim.
Fire-related homicides may raise challenging questions about the cause of death. The majority of all fire deaths are due to smoke and soot inhalation. The most common toxic agent is carbon monoxide, measured as a decedent’s carboxyhemoglobin (COHb) level, although smoke and soot may contain a number of other toxic agents, including acetic acid, hydrogen cyanide, methane, and formic acid. Carboxyhemoglobin levels in the range of 40% to 60% are frequently cited as fatal, although the range of actual observed fatal levels is wide (6 -9). Additionally, fire-related deaths may also occur due to other causes, such as the sequelae of thermal injuries (10,11) or due to antecedent trauma. Fire-related homicides, in particular, raise the question of whether the decedent was burned postmortem to destroy evidence of homicide (12,13).
Multiple worldwide retrospective studies have examined the characteristics of fire-related deaths, including studies in Istanbul (3,5), Oslo (14), and Copenhagen (7). These studies have consistently demonstrated a high proportion of accidental deaths and small proportion of homicides. The largest of these studies to date have included a total of 31 homicides (3 -5,7,13,15). Fire-related homicides may share distinctive characteristics that distinguish them from other fire-related deaths. However, to the authors’ knowledge, only one large study has been performed specifically examining the characteristics unique to fire-related homicides, a review of 26 cases in Miami from 1977 to 1984 (15).
To better understand the characteristics of fire-related homicides, a 10-year retrospective review of the Wayne County Medical Examiner’s Office (WCMEO) was performed to examine the following: 1) the circumstances in which fire-related homicides occur; and 2) the autopsy and ancillary studies most important to consider when performing autopsies in suspected fire-related homicides.
Methods
Data Collection
The WCMEO is a large, urban medical examiner’s office located in Detroit, Michigan, that performs approximately 3000 autopsies per year. WCMEO autopsy reports from April 2007 through April 2017 were reviewed through the InQuest data management system. Possible fire-related homicides were identified by using search terms that included “carbon monoxide,” “smoke and soot inhalation,” “burns,” and “thermal injuries,” which identified 42 homicide cases. Excluded from this analysis were four cases that met these keywords but did not involve fires. The four excluded cases included two carbon-monoxide poisoning deaths associated with vehicle exhaust, a homicide victim found with thermal injuries of unclear origin, and a child who suffered thermal injuries from a space heater.
Among the 38 cases of fire-related homicides, 30 cases had available COHb levels to review. Postmortem COHb levels, obtained by gas chromatography-mass spectrometry, were collected from peripheral blood when possible, but by heart blood or tissue in cases of severe burns. When available, emergency room or in-hospital COHb levels were obtained and incorporated into the autopsy report.
Statistical Analysis
Analyses of statistical significance were performed between groups using Mann-Whitney U tests for continuous variables and Fischer exact tests for categorical variables.
Results
Baseline Characteristics
Thirty-eight cases of fire-related homicides were identified. The mean age was 41.5 years, 26 decedents (68%) were black, 10 decedents (26%) were white, 2 decedents (5%) were of an undetermined race, 24 decedents (63%) were male, and five (13%) were under the age of 18.
Circumstances of Death
Deaths were categorized based on circumstances of death. The most common circumstance was death by smoke and soot inhalation in arson of a dwelling fire (n = 21, 55%), followed by direct immolation (n = 8, 21%), and fatal trauma with contemporaneous immolation (n = 8, 21%). Two deaths involved car fires: one in which the decedent was ignited by an explosive device and died after a prolonged hospital course, and a second in which the decedent was discovered in the trunk with fatal trauma. In one case, death occurred by fatal trauma without evidence that the decedent was alive at the time of immolation ( Figure 1 ).
Figure 1:

Categorization of fire-related homicides by common causes of death and associated circumstances. Cases could typically fall into several distinct categories, with arson/dwelling fires being the most common circumstance. Most cases of fatal trauma either had evidence of elevated COHb or prolonged survival, suggesting that true postmortem immolation is rare.
An accelerant was used to start the fire in nine cases (24%) and an explosive device was used in four cases (11%). Twelve decedents were involved in a multiple-fatality incident, ranging from two to five decedents.
Characteristics by Survival Length
Decedents were found dead at the scene or pronounced dead upon arrival to the emergency department in 26 (68%) of cases and survived one day or more in 12 (32%) of cases. When compared with the deaths at the scene or in the emergency department, decedents with a longer survival length were less likely to be children, less likely to have been in a residential fire, and less likely to have died of an inhalation-related cause of death. At autopsy, decedents with a longer survival length were also less likely to have severe burns, charring, soot in the airways, and fatal levels of COHb level ( Table 1 ).
Table 1:
Characteristics of Decedents by Survival Length.
| Finding | Dead at scene or upon arrival (n = 26) | Survival beyond emergency room (n = 12) | p value |
|---|---|---|---|
| Circumstances and history | |||
| Dwelling fire, n (%) | 21 (81%) | 5 (42%) | 0.03 |
| Accelerant use, n (%) | 5 (19%) | 4 (33%) | 0.42 |
| Explosive use, n (%) | 0 (0%) | 4 (33%) | <0.01 |
| Multivictim incident, n (%) | 12 (46%) | 0 (0%) | <0.01 |
| Autopsy findings | |||
| Soot in airways, n (%) | 21 (81%) | 4 (33%) | <0.01 |
| Greater than 50% BSA burned, n (%) | 16 (62%) | 5 (42%) | 0.31 |
| Deep or charring burns, n (%) | 12 (46%) | 0 (0%) | <0.01 |
| Detectable COHb, n (%) | 24 (92%) | 2 (17%) | 0.02 |
| Fatal (greater than 40%) COHb, n (%) | 14 (54%) | 2 (17%) | 0.04 |
| Cause of death | |||
| Inhalation, n (%) | 21 (81%) | 3 (25%) | <0.01 |
| Burns, n (%) | 10 (38%) | 10 (83%) | 0.01 |
| Trauma, n (%) | 7 (27%) | 2 (17%) | 0.68 |
Abbreviations: BSA, body surface area; COHb, carboxyhemoglobin.
Of the decedents who survived beyond the emergency department, 82% died of documented complications from their fire-related injuries. The most common complications were pneumonia (44%), sepsis (33%), and multi-organ failure (33%) ( Table 2 ).
Table 2:
Complications in Decedents With Survival Beyond Emergency Room.
| Decedent | Survival (days) | COHb | Pneumonia | ARDS | Multi-organ failure | Anoxic brain injury | Coagulopathy | Sepsis | Compartment syndrome |
|---|---|---|---|---|---|---|---|---|---|
| 37 y/o male doused with gasoline and immolated | 1 | N/A | - | - | + | - | + | - | - |
| 35 y/o male shot and set on fire | 2 | N/A | - | - | + | - | - | - | - |
| 40 y/o female found in dwelling after firebombing | 3 | 44% | + | - | - | - | - | - | - |
| 20 y/o female found in a burning house | 4 | 41% | + | - | - | - | - | - | - |
| 38 y/o female doused with gasoline and immolated | 6 | N/A | + | + | + | + | + | + | - |
| 24 y/o male found in dwelling after firebombing | 11 | N/A | - | + | - | - | - | - | - |
| 38 y/o male directly immolated | 13 | N/A | - | - | - | - | - | + | + |
| 53 y/o male doused withlighter fluid and immolated | 21 | N/A | - | - | - | - | - | - | - |
| 25 y/o female in a car explosion set by a propane tank | 109 | N/A | + | - | - | - | - | + | - |
| Total number of cases | 4 | 2 | 3 | 1 | 2 | 3 | 1 |
Abbreviations: ARDS, acute respiratory distress syndrome; COHb, carboxyhemoglobin; N/A, not available for review.
Cause of Death
The causes of death in the cases reviewed were related to either smoke and soot or carbon monoxide inhalation (n = 24, 63%), burns/thermal injuries (n = 20, 53%), and/or trauma (n = 9, 24%). In 15 cases (39%), the cause of death was multifactorial, overlapping between inhalation and burns, inhalation and trauma, or burns and trauma.
Autopsy Findings and COHb Levels
Among all cases, the most common autopsy findings were thermal injuries (n = 37, 97%) and soot in the airways (n = 26, 68%). The extent of the burns was less than or equal to 50% of body surface area (BSA) in 13 cases (34%) and greater than 50% in 25 cases (66%). Ten decedents (26%) had complete (>95% BSA) burns.
Carboxyhemoglobin testing was available for 30 decedents. Carboxyhemoglobin was undetectable in three cases. In one case, COHb was detected on an initial screen and the quantitative assay was unsatisfactory; therefore, this case was excluded from analysis. The mean COHb level was 41% (95% CI = 31%-51%). When stratified by factors contributing to the cause of death, cases with an inhalation-related cause of death had a median COHb level of 46% (range = 0%-91%), cases with thermal injuries contributing to the cause of death had a median COHb level of 16% (range = 0%-59%), and cases with trauma contributing to the cause of death had a median COHb level of 24% (range = 0%-59%) ( Figure 2 ).
Figure 2:
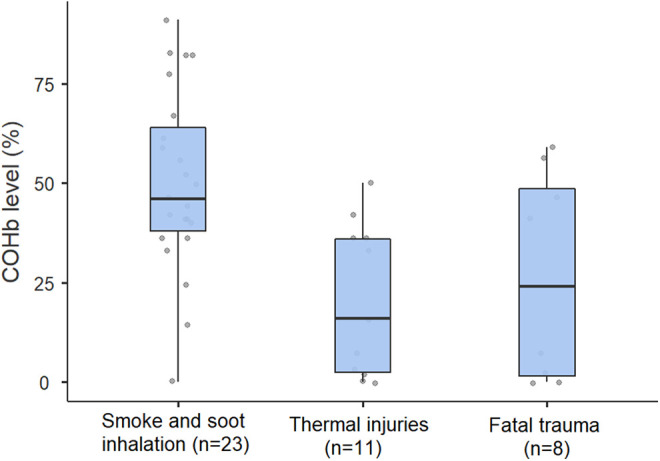
Distribution of COHb levels in the 30 decedents with available COHb data. Regardless of factors contributing to death, cases showed a wide range of COHb, highlighting the multifactorial nature of these deaths. Boxes indicate median with interquartile ranges, lines indicate minimum and maximum, and dots indicate individual values.
Trauma
Fatal trauma was present in nine cases (24%). The most common types of trauma included blunt force injuries (n = 5), gunshot wounds (n = 2), and sharp force injuries (n = 2). Signs of vitality, defined as either the presence of soot in the airways or detectable COHb in the blood, were present in seven of these cases, and in seven, the decedent was dead at the scene or upon arrival to the emergency department. In one case, the decedent had a finding of fatal trauma with no signs of vitality, suggesting true postmortem immolation ( Table 3 ).
Table 3:
Patterns of Traumatic Injury.
| Finding | Signs of vitality | Survival Length | |
|---|---|---|---|
| Soot | COHb | ||
| Blunt force injury | |||
| 21-year-old male discovered in house fire | No | Negative | Dead at scene |
| 21-year-old male discovered in burning car | Yes | 56% | Dead at scene |
| 56-year-old female discovered in house fire | Yes | 2% | Dead at scene |
| 89-year-old male discovered in house fire | Yes | 59% | Dead at scene |
| 91-year-old male discovered in house fire | Yes | 7% | Dead at scene |
| Gunshot wounds | |||
| 35-year-old male shot, then set on fire | No | Not performed | 2 days |
| 55-year-old male shot, then set on fire | Yes | 46% | Dead at scene |
| Sharp force injury | |||
| 26-year-old male discovered in house fire | Yes | 41% | Dead at scene |
| 39-year-old male kidnapped and set on fire | Yes | Negative | 1 day |
Abbreviation: COHb, carboxyhemoglobin.
Discussion
This retrospective review of fire-related homicides shows that these deaths fall into several distinct categories, most commonly arson/dwelling fires, followed by direct immolation, and trauma with contemporaneous/subsequent immolation. The presence of fatal trauma, an evaluation of the clinical circumstances (particularly whether the decedent survived for a period of time), and COHb remain the primary tools for categorizing these deaths.
The general characteristics observed in these fire-related homicides are similar to earlier studies, particularly the study by Copeland examining fire-related homicides in Miami from 1977 to 1984. Copeland found that the stereotypical decedent was a white male who died in a residential fire of an inhalation-related death. The high rate of residential fires in this cohort (68% of all decedents) and inhalation-related deaths is similar to the typical case in Copeland’s study (15). Unlike Copeland’s findings, however, the cohort presented here contains a substantial minority of decedents who were immolated and who ultimately died of burns rather than inhalation-related causes. Furthermore, this study identified a much higher proportion of traumatic injuries than Copeland’s study. Given that our study and Copeland’s study both involved a single medical examiner’s office, these findings may represent geographic variability.
Compared to large-scale reviews of all fire deaths, including accidents and suicides, a high proportion of cases with an inhalation-related cause of death were identified (63%). Previous studies have varied in the proportion of inhalation-related cases, with the large review by Büyük and Koçak in Istanbul identifying only 32.5% such cases (3) and the study by Rogde and Olving in Oslo identifying 74% (14). In the cohort presented here, a wide range of COHb levels were noted both across all cases (2%-91% when detected) and across the inhalation-related cases (14%-91% when detected). These findings are consistent with previous literature that reports a wide range of COHb levels in fire-related and carbon monoxide-related deaths (8). A wide number of factors, including the underlying cardiovascular health of an individual, play a role in the potentially fatal COHb level (16). The heterogeneity observed in these homicides likely contributes to the range of COHb levels, consistent with the high proportion of multifactorial causes of death in our cohort.
Cases of burning subsequent to or concurrent with fatal traumatic injury accounted for a large minority of cases in this review. Previous studies have suggested that signs of vitality are frequently absent or incomplete in posttraumatic burning, even when the decedent may have been alive during the fire (12,17). In nine cases involving posttraumatic burns, however, only two lacked signs of vitality, one of which could be attributed to a two-day survival in the hospital. With one exception, traumatized decedents were all burned while still alive, showing low or even sometimes potentially fatal COHb levels. Therefore, the presence or absence of signs of vitality should not rule out a significant role for trauma, but rather should be interpreted in context of the other circumstances and autopsy findings.
This cohort contained two cases in which decedents survived for a prolonged period of time (three days and four days) but had potentially fatal COHb levels upon admission to the hospital (44% and 41%, respectively). Cases such as these should generally be understood as death due to complications of thermal injuries, rather than smoke and soot inhalation, unless the underlying cause of death was anoxic end-organ damage or other delayed sequelae of smoke and soot inhalation. Another rare circumstance seen in only one case was that of a dwelling fire in which the decedent showed evidence of soot in the airways but undetectable COHb. Based on the circumstances, this likely represents a false negative COHb or may result from delayed testing of the sample, but raises the possibility that other toxic agents such as hydrogen cyanide played a primary role in death. No cases in our series suggested the situation of a COHb-negative flash fire in which death occurred due to rapid oxygen deprivation in an enclosed space and therefore showed no detectable COHb, a circumstance that has previously been described by Hirsch et al. (18).
The primary strength of this study is the sample size. The 38 cases represent, to the authors’ knowledge, the largest series of fire-related homicides reviewed in the literature. Through access to well-documented, standardized and templated investigative, autopsy, and COHb results, an analysis and comparison was completed of circumstances of these uncommon cases in a standardized fashion.
The primary limitations of this study are its retrospective nature and the heterogeneous nature of fire-related homicides, which limits the ability to draw general conclusions from these cases. Additionally, the data presented here were drawn entirely from one large, urban medical examiner’s office in the United States, although the findings may be generalizable to fire-related homicides in other settings.
While fire-related homicides are a heterogeneous group of cases, our data show that they can generally be classified based on similar characteristics and autopsy findings. Individual findings are rarely specific for a particular cause of death. Particularly in cases with potentially fatal trauma, weighing the relative contribution of trauma, smoke and soot inhalation, and thermal injuries remain an important diagnostic challenge.
AUTHORS
Kyle S. Conway MD, JD, University of Michigan, Department of Pathology
Roles: Project conception and/or design, data acquisition, analysis and/or interpretation, manuscript creation and/or revision, approved final version for publication, writing assistance and/or technical editing.
Carl J. Schmidt, MD, University of Michigan, Department of Pathology; Wayne County Medical Examiner’s Office
Roles: Project conception and/or design, data acquisition, analysis and/or interpretation, manuscript creation and/or revision, approved final version for publication, writing assistance and/or technical editing.
Theodore T. Brown, MD, Western Michigan University Homer Stryker M.D. School of Medicine, Department of Pathology and Office of the Medical Examiner.
Roles: Project conception and/or design, data acquisition, analysis and/or interpretation, manuscript creation and/or revision, approved final version for publication, writing assistance and/or technical editing.
Footnotes
Statement of Human and Animal Rights: This article does not contain any studies conducted with animals or on living human subjects.
Statement of Informed Consent: No identifiable personal data were presented in this manuscript.
Disclosures & Declaration of Conflicts of Interest: The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.
Financial Disclosure: The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript.
References
- 1. Homer CD, Engelhart DA, Lavins ES, Jenkins AJ. Carbon monoxide-related deaths in a metropolitan county in the USA: an 11-year study. Forensic Sci Int. 2005;149(2-3):159–165. [DOI] [PubMed] [Google Scholar]
- 2. Fire in the United States 2005-2014. [Internet] 2017. https://www.usfa.fema.gov/downloads/pdf/publications/fius18th.pdf Accessed May 28, 2020. [Google Scholar]
- 3. Büyük Y, Koçak U. Fire-related fatalities in Istanbul, Turkey: analysis of 320 forensic autopsy cases. J Forensic Leg Med. 2009;16(8):449–454. [DOI] [PubMed] [Google Scholar]
- 4. Parks JG, Noguchi TT, Klatt EC. The epidemiology of fatal burn injuries. J Forensic Sci. 1989;34(2):399–406. [PubMed] [Google Scholar]
- 5. Melez IE, Arslan MN, Melez DO, Gürler AS, Büyük Y. Manner of death determination in fire fatalities: 5-year autopsy data of Istanbul city. In: American Journal of Forensic Medicine and Pathology; 2017. 59–68. [DOI] [PubMed] [Google Scholar]
- 6. Przepyszny LM, Jenkins AJ. The prevalence of drugs in carbon monoxide-related deaths: a retrospective study, 2000-2003. Am J Forensic Med Pathol. 2007;28(3):242–248. [DOI] [PubMed] [Google Scholar]
- 7. Gormsen H, Jeppesen N, Lund A. The causes of death in fire victims. Forensic Sci Int. 1984;24(2):107–111. [DOI] [PubMed] [Google Scholar]
- 8. Gerostamoulos D, Beyer J, Wong K, Wort C, Drummer OH. Carbon monoxide concentrations in the 2009 Victorian bushfire disaster victims. Forensic Sci Int. 2011;205(1-3):69–72. [DOI] [PubMed] [Google Scholar]
- 9. Yoshida M, Adachi J, Watabiki T, Tatsuno Y, Ishida N. A study on house fire victims: age, carboxyhemoglobin, hydrogen cyanide and hemolysis. Forensic Sci Int. 1991;52(1):13–20. [DOI] [PubMed] [Google Scholar]
- 10. Gerling I, Meissner C, Reiter A, Oehmichen M. Death from thermal effects and burns. Forensic Sci Int. 2001;115(1-2):33–41. [DOI] [PubMed] [Google Scholar]
- 11. Makhlouf F, Alvarez JC, de la Grandmaison GL. Suicidal and criminal immolations: an 18-year study and review of the literature. Leg Med. 2011;13(2):98–102. [DOI] [PubMed] [Google Scholar]
- 12. Keten A, Odabaşı AB, Kanburoğlu Ç, et al. Postmortem burning of the corpses following homicide. J Forensic Leg Med. 2012;19(4):223–228. [DOI] [PubMed] [Google Scholar]
- 13. Fanton L, Jdeed K, Tilhet-Coartet S, Malicier D. Criminal burning. Forensic Sci Int. 2006;158(2-3):87–93. [DOI] [PubMed] [Google Scholar]
- 14. Rogde S, Olving JH. Forensic science international characteristics of fire victims in different sorts of fires. Forensic Sci Int. 1996;77(1-2):93–99. [DOI] [PubMed] [Google Scholar]
- 15. Copeland AR. Homicide by fire. Zeitschrift für Rechtsmedizin. 1985;95(1):59–65. [DOI] [PubMed] [Google Scholar]
- 16. Conway K, Rayes O, Brown T, Webb M. Atherosclerotic and Hypertensive Cardiovascular Disease are Associated with Death at Sublethal Carboxyhemoglobin Levels: A Postmortem Study. J Forensic Sci. 2019; 65(3):855–859. [DOI] [PubMed] [Google Scholar]
- 17. Bohnert M, Werner CR, Pollak S. Problems associated with the diagnosis of vitality in burned bodies. Forensic Sci Int. 2003;135(3):197–205. [DOI] [PubMed] [Google Scholar]
- 18. Hirsch CS, Bost RO, Gerber SR, Cowan ME, Adelson L, Sunshine I. Carboxyhemoglobin concentrations in flash fire victims: report of six simultaneous fire fatalities without elevated carboxyhemoglobin. Am J Clin Pathol. 1977;68(3):317–320. [DOI] [PubMed] [Google Scholar]