

Abstract
Background
Blunt traumatic brachial plexus injuries (BTBPI) are severe peripheral nerve injuries which present in a small portion of trauma patients but can result in long-term neurological disability and severe chronic pain.
Objective
The goal of this study was to describe the epidemiology of BTBPI in a northern rural setting caused by motor-powered collisions, and to determine the relative risk of these injuries in shielded (cars, trucks, vans, and so on) and unshielded vehicles (snowmobiles, all-terrain vehicles and motorcycles).
Methods
This retrospective study describes the epidemiology of BTBPI caused by motor-powered collisions and treated at two level II trauma centers in northeast Minnesota and determines the relative risk of these injuries in shielded (cars, trucks, vans, and so on) and unshielded vehicles (snowmobiles, all-terrain vehicles and motorcycles). We hypothesized unshielded motor vehicle crashes in rural areas are at an increased risk of incurring BTBPI.
Results
Out of all injuries resulting from motor-powered collisions in a 20-year period (9951), BTBPIs were found in 63 trauma patients, a prevalence of 0.6%. The rate of BTBPI involving unshielded vehicles (1.0%) was significantly higher than those involving a shielded vehicle (0.4%) and primarily occurred in rural areas (70%).
Conclusions
Unshielded vehicle crashes, particularly snowmobiles, have the highest risk for BTBPI in our rural region. The overall incidence of these injuries appears to be declining.
Level of evidence
Level III.
Keywords: accidents, traffic, accidental injuries, epidemiology, neck injuries
Introduction
Blunt traumatic brachial plexus injuries (BTBPI) are severe peripheral nerve injuries which present in a small proportion (1.2%) of trauma patients but can result in long-term neurological disability and severe chronic pain.1 2 BTBPIs are primarily sustained by young males (19–35 years old) due to traction or stretching of the brachial plexus. Injuries can range from mild stretch resulting in temporary neuropraxia to complete and permanent loss of all neurological functions due to nerve avulsion.1 3 4
The major cause of this injury is high-velocity vehicle crashes. Worldwide, motorcycle crashes cause the majority of BTBPIs, with rates as high as 63% to 82% in high-density urban environments like Thailand and India, and as low as 22% in rural areas like Canada.1 5 6 These injuries are caused by motor vehicle collisions at a rate of 15% to 29%.1 7 In colder rural climates such as ours, BTBPIs can also be caused by snowmobile crashes (3% to 7.3%).1 8
In our primarily rural region, we have observed a seemingly higher risk for BTBPIs in snowmobile crashes. We retrospectively reviewed our region’s level II trauma centers data to determine the relative risk of BTBPI among various types of motor-powered vehicle crashes. We suspected that vehicles with an external protective shell that completely encloses the occupants within the vehicle would have less BTBPIs than vehicles that do not completely enclose the occupants. The enclosed vehicles are designated ‘shielded’ in this report and include cars, trucks, vans, and so on. We designated unenclosed vehicles ‘unshielded’ and include snowmobiles, all-terrain vehicles (ATV) and motorcycles. By this designation, other vehicles such as convertibles and dune buggies would be unshielded. Their incidence in this study is unknown, though given our region, we can confidently assume it would be very low.
This retrospective study describes the epidemiology and urban/rural differences of BTBPIs caused by motor-powered collisions and treated at two level II trauma centers which serve areas of northeastern Minnesota, northwestern Wisconsin, and the westernmost portion of the Upper Peninsula of Michigan. This study also determines the relative risk of these injuries in shielded and unshielded vehicles. We hypothesized that unshielded motor vehicle crashes (MVC) are at an increased risk of incurring BTBPI, and that these MVCs would occur in rural areas with higher frequency.
Methods
We retrospectively reviewed the medical records of adult patients (as defined by the American College of Surgeons Committee on Trauma) ≥15 years old who suffered a BTBPI during a 20-year period from January 1, 1995 to June 30, 2016. Patients with a BTBPI were identified from the two hospitals’ trauma registries. A variety of data elements were electronically and manually extracted from the trauma registries, electronic medical records, and paper medical records to describe the epidemiology of BTBPIs treated at the two trauma centers, and included: age, gender, BTBPI diagnosis, mechanism of injury (off-road vehicle crashes (ATVs, snowmobiles), motorcycle crashes, and MVCs), injury zip code, date and time of injury, alcohol use, and injury severity. Rural and urban variables were created using census tract zip code approximation of the Rural-Urban Commuting Area (RUCA) classification, where any RUCA code 4 and above (non-metropolitan) are considered rural.
Twenty-two patients had missing date and time of BTBPI injury data. Where this occurred, we used admission date and time. Data were entered into a Microsoft Excel (Microsoft) spreadsheet and analyzed in SAS (SAS Enterprise Guide Ver.7.15). The 95% CI was used to estimate the precision of the OR, and a p value <0.05 was considered statistically significant. Standard, unadjusted ORs, with Woolf’s 95% CIs, were used to compare MVC events to each other type of vehicle and MVC (shielded) to all other types of vehicles (unshielded). Statistical software for these computations was not used, because only aggregate data were available for total exposures, so the appropriate 2×2 calculations were conducted using Excel.
Results
A total of 76 patients with BTBPI were found during the 20-year study period for an overall incidence rate of 0.76%. Thirteen of these injuries were the result of non-motor-powered vehicular trauma and were excluded from the study (figure 1). Non-motor vehicle events excluded from the study included pedestrians struck by motor vehicles; loss of control while riding a bicycle; water sport crashes, including boating; assaults with and without weapons; falls from varying heights; being pinned under machinery and trees; and being struck in sports. The remaining BTBPIs were caused by collisions involving motor-powered vehicles, which is the primary focus of our analysis. Out of all injuries resulting from motor-powered collisions (9951), BTBPIs were found in 63 trauma patients, an incidence of 0.6% (table 1).
Figure 1.
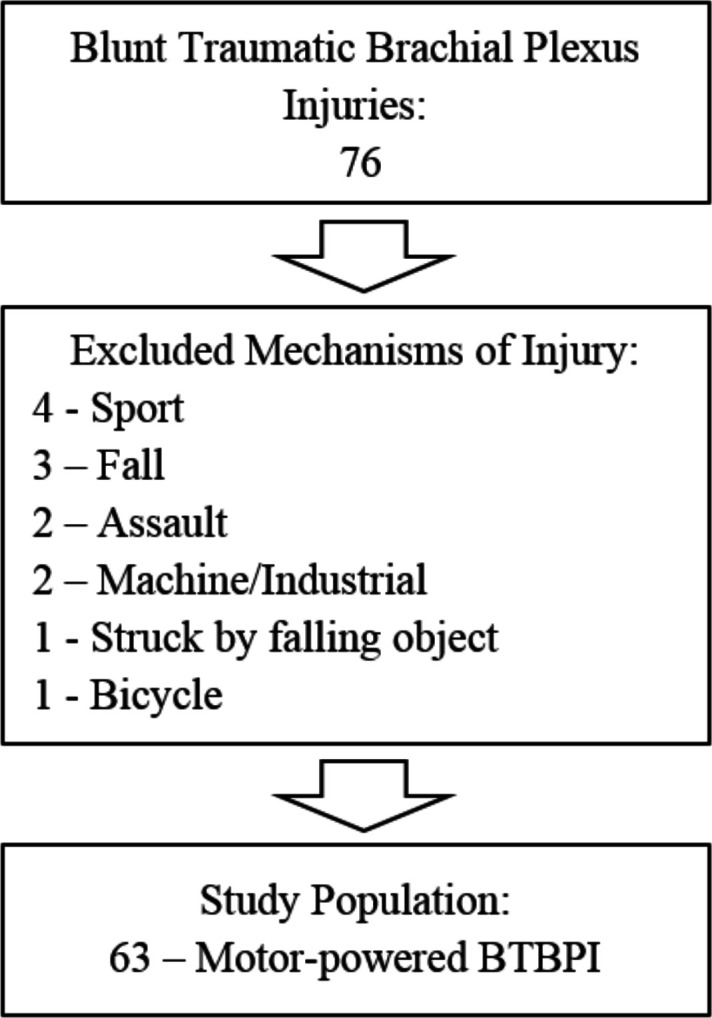
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of study population inclusion and exclusions of blunt traumatic brachial plexus injuries (BTBPI).
Table 1.
ORs of BTBPIs caused by motor vehicles and BTBPI crash details
| Crash details | |||||||||||||||
| Vehicle | All injuries | BTBPI (%) | OR | 95% CI | p-value | Age Median (IQR) |
Male (%) | Night (%) | Season (%) | Alcohol related (%) | ISS Median (IQR) |
||||
| LL | UL | Winter | Spring | Summer | Fall | ||||||||||
| MVC | 5734 | 22 (0.4) | Ref | – | – | – | 32 (19) | 82 | 55 | 23 | 27 | 27 | 18 | 50 | 17.0 (17) |
| ATVC | 1590 | 10 (0.6) | 1.64 | 0.7 | 3.5 | 0.190 | 24 (20) | 90 | 20 | 0 | 50 | 30 | 20 | 30 | 33.5 (18) |
| SMC | 1367 | 24 (1.8) | 4.64 | 2.5 | 8.3 | <0.001 | 39 (12) | 92 | 38 | 79 | 21 | 0 | 0 | 38 | 14.0 (10) |
| MCC | 1260 | 7 (0.6) | 1.45 | 0.6 | 3.2 | 0.390 | 32 (34) | 86 | 29 | 0 | 14 | 43 | 43 | 43 | 17.0 (5) |
| Shielded | 5734 | 22 (0.4) | Ref | – | – | – | 32 (19) | 82 | 55 | 23 | 27 | 27 | 18 | 50 | 17.0 (17) |
| Unshielded | 4217 | 41 (1) | 2.55 | 1.52 | 4.29 | <0.001 | 38 (20) | 90 | 32 | 46 | 27 | 15 | 12 | 36 | 17.0 (14) |
| Total | 9951 | 63 (0.6) | – | – | – | – | 35 (19) | 87 | 40 | 38 | 27 | 19 | 16 | 41 | 17.0 (14) |
Bolded values have a p-value <0.05, which was considered statistically significant.
ATVC, all-terrain vehicle crash; BTBPI, blunt traumatic brachial plexus injuries; ISS, Injury Severity Score; LL, lower limit; MCC, motorcycle crash; MVC, motor vehicle crash; Ref, reference category; SMC, snowmobile crash; UL, upper limit.
Table 1 also shows the details of the 63 cases of BTBPI caused by a motor-powered vehicle collision, of which 87.5% were male, with a mean age of 36 years (range 16–73). Drivers of the vehicle made up 87.7% of those who sustained a BTBPI, and alcohol was found to be involved 40.6% of the time. The average BTBPI injury severity score was 20.2.
The overall percentage of BTBPI sustained in a motor-powered collision was found to dramatically drop over the study period (figure 2). The types of motor-powered vehicles involved in these collisions were snowmobiles (38%), motor vehicles (35%), ATVs (16%) and motorcycles (11%). The rate of BTBPI resulting from snowmobile collisions (1.8%) was significantly higher than those resulting from motor vehicle collisions (0.4%). Additionally, the number of BTBPIs involving unshielded vehicles (1.0%) was significantly higher than those involving a shielded vehicle (0.4%).
Figure 2.

Year of blunt traumatic brachial plexus injuries (BTBPI) for shielded and unshielded motorized vehicle mechanisms of injury.
Of the 63 patients with a BTBPI, 50 (79%) had a documented injury zip code. Out of these 50 patients, 35 (70%) were in a rural area when their BTBPI occurred. Of patients with BTBPI from snowmobile crashes, 84% were in rural areas. For BTBPIs from ATVs, 78% were in rural areas. For BTBPIs from motor vehicles, 56% were in rural areas. BTBPIs from motorcycles were split evenly between urban and rural.
Discussion
BTBPIs are a rare but significantly morbid type of traumatic injury. Whereas the most common etiology of BTBPI in the USA is from motorcycle crashes,1 our regional data show that the proportion of BTBPI in snowmobile crashes (24 out of 1367 injured (1.8%)) exceeds those in motorcycle crashes (7 out of 1260 injured (0.6%)) and far outweighs shielded motor-powered mechanisms with an OR of 4.64. When comparing the unshielded to the shielded group, there is an OR of 2.55 suggesting a protective mechanism to the shielded component of the vehicle and likely decreasing the extent of stretch trauma sustained by the brachial plexus. Our overall BTBPI rate was half the North America rate (0.6% vs. 1.2%) which is likely due to the small number of motorcycle crashes in our region and smaller sample size.
The weather in and rurality of our region play a key role in our findings as well. First, the rural incident rate of BTBPI at 84% caused by snowmobile crashes is noteworthy when considering that the rate of all rural traumatic injuries seen at these hospitals is around 55%. The general use of recreational snowmobiles in our region is high with over 196,687 snowmobiles registered in the state of Minnesota (second highest number of registrations in the country) compared with 229,377 motorcycles (12th highest).9 10 Second, the meteorological season length of winter is significantly longer than the lunar season length especially in the northernmost portion of the state that sees 33% more snow days throughout the calendar year compared with the southernmost (41.1 days vs. 28.0 days).11 This weather trend favors a higher frequency of snowmobile use and a lower frequency of motorcycle and ATV use in our region.
Another notable trend found in our data was that the overall number of these injuries from all mechanisms has decreased significantly since 2012. We did not have any BTBPI in the shielded group and only three in the unshielded group since 2012. We suspect this is likely attributable to an increase in motor vehicle safety with the implementation of mandatory airbag installation (including most resale vehicles), better seat belt use,12 as well as emphasis on safe operation of vehicles in the unshielded groups. Within the shielded group, 45.5% of those patients sustaining a BTBPI were ejected from their vehicle. This mechanism essentially eliminates the protective component of the ‘shielded’ vehicle and increases the relative risk of BTBPI.
Although limited by its retrospective observational design, small numbers and lack of clinical details (presentation, anatomic details of injury and the clinical course), this study provides a unique description of BTBPI that reflects the types of vehicle crashes common in the northern rural climates.
Conclusion
Unshielded vehicle crashes, particularly snowmobiles, have the highest risk for BTBPI in rural northern regions where they are commonly used. Although the overall incidence of these injuries appears to be declining, they can result in long-term neurological disability and severe chronic pain.
Footnotes
Contributors: JB, SE, MO, and CR contributed to the conception and design of the work. CR, TW, JV, SL, HN and MO contributed to the data collection. CR, SE, SL, and JB contributed to the data analysis and interpretation. SL, TW, CR, SE, and JV contributed to the drafting of the article. TW and CR contributed to the critical revision of the article. Final approval of the version to be published was completed by the entire author group.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: This project was a multicenter, observational, retrospective cohort study, which was reviewed and approved by the Institutional Review Boards of both hospitals. The study was deemed exempt and need for patient consent was waived. This article adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request.
References
- 1.Midha R. Epidemiology of brachial plexus injuries in a multitrauma population. Neurosurgery 1997;40:1182–9. 10.1097/00006123-199706000-00014 [DOI] [PubMed] [Google Scholar]
- 2.Moran SL, Steinmann SP, Shin AY. Adult brachial plexus injuries: mechanism, patterns of injury, and physical diagnosis. Hand Clin 2005;21:13–24. 10.1016/j.hcl.2004.09.004 [DOI] [PubMed] [Google Scholar]
- 3.Dubuisson AS, Kline DG. Brachial plexus injury: a survey of 100 consecutive cases from a single service. Neurosurgery 2002;51:673–83. 10.1097/00006123-200209000-00011 [DOI] [PubMed] [Google Scholar]
- 4.Kim DH, Murovic JA, Tiel RL, et al. Mechanisms of injury in operative brachial plexus lesions. Neurosurgical Focus 2007;16:1–8. [PubMed] [Google Scholar]
- 5.Jain DKA, Bhardwaj P, Venkataramani H, Sabapathy SR. An epidemiological study of traumatic brachial plexus injury patients treated at an Indian centre. Indian J Plast Surg 2012;45:498–503. 10.4103/0970-0358.105960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Songcharoen P. Brachial plexus injury in Thailand: a report of 520 cases. Microsurgery 1995;16:35–9. 10.1002/micr.1920160110 [DOI] [PubMed] [Google Scholar]
- 7.Kaiser R, Waldauf P, Haninec P. Types and severity of operated supraclavicular brachial plexus injuries caused by traffic accidents. Acta Neurochir 2012;154:1293–7. 10.1007/s00701-012-1291-7 [DOI] [PubMed] [Google Scholar]
- 8.Braun BL, Meyers B, Dulebohn SC, Eyer SD. Severe brachial plexus injury as a result of snowmobiling: a case series. J Trauma 1998;44:726–30. 10.1097/00005373-199804000-00030 [DOI] [PubMed] [Google Scholar]
- 9.International Snowmobile Manufacturers Association Snowmobiling Fact Book. 2017. http://www.snowmobile.org/docs/isma-snowmobiling-fact-book.pdf.
- 10.State Motor-Vehicle Registrations - 2016 in Information USDoT-OoHP 2017
- 11.Current Results Average Annual Snowfall Totals in Minnesota. https://www.currentresults.com/Weather/Minnesota/annual-snowfall.php.
- 12.Pickrell T. Washington, DC: National Highway Traffic Safety Administration; 2017. Seat belt use in 2016-use rates in the states and territories. (Report No. dot HS-812-417) [Google Scholar]