

Abstract
Background and Aims:
Erectile dysfunction (ED) is an inability to achieve and maintain erectile rigidity sufficient for satisfactory sexual performance. It is either organic or psychogenic in origin. This study was aimed at establishing vasculogenic causes among patients being evaluated for ED using Penile Doppler Ultrasound.
Methods:
Fifty-two consecutive patients with the clinical diagnosis of ED were evaluated with color Doppler ultrasound scan using a 7.5 MHz high-frequency linear transducer between July 2016 and June 2019. The examination was commenced 3 min after an intracavernosal injection with 10-20 μg of PGE1 and continued for 30 min. The measurements were obtained alternately from both deep penile arteries. The variables analyzed were the peak systolic velocity (PSV), end-diastolic velocity (EDV) and resistive index (RI), calculated as (PSV-EDV)/PSV. Erection Hardness was evaluated subjectively using the EH Score (EHS), a 5-point response score denoting how the patient would rate his erection. ED was subjectively assessed using the International Index of Erectile Function (IIEF-5) questionnaire. In patients with a diagnosis of vasculogenic ED, intracavernosal PGE1 injection was started with a 5 μg dose and then increased in 5 μg increments until the final dose of 20 μg was reached.
Results:
PSV of cavernosal arteries (CA) varied between 19.2 and 106.2 cm/s (mean: 43.8 ± 18.2) among the entire patients and between 19.7 and 80.2 cm/s (mean: 42.6 ± 11.3) among patients with arteriogenic ED. Arteriogenic ED was found in 8 patients (15.3%), while venogenic ED was observed in 12 patients, which constituted 23% of the entire study population and mixed arteriogenic-venogenic ED was found in 6 patients (11.5%) of the study population. DICC performed on patients diagnosed with venogenic ED on color Doppler ultrasonography revealed venous leakage and no statistically significant differences between results of DICC and color Doppler ultrasonography were found in EDV, RI, and PI measurements (P< 0.005). Among patients with venogenic ED and mixed arteriogenic-venogenic ED,2 patients had a normal erectile response and the remaining 16 received 2 mg phentolamine. A significant increase in PSV between baseline and 20 mg PGE1 (P < 0.001) was observed in all cases. Following phentolamine, there was a significant increase in grade of erection (P = 0.0001) and a significant reduction in the EDV (P = 0.0001). A reduction of the EDV to below 0.0 cm/s was observed in 12 patients. In patients with arteriogenic erectile dysfunction, mean (±standard deviation) duration of erection for consecutive doses of PGE15 μg, 10 μg, 15 μg, and 20 μg were 42.2±18.4, 55.4±24.1, 66.1 ± 31.1, and 83.3±36.7 minutes, respectively, with significant increase for each dose. In patients with veno-occlusive dysfunction, mean durations of erection significantly increased from 9.1±8.0 minutes at 10 μg to 19.2±9.8 minutes at 20 μg.
Conclusion:
In the current study, 50% of patients had vasculogenic ED and “false-positive’’ diagnosis of venous leakage was unmasked by phentolamine re-dosing. It is therefore imperative that patients with ED benefit from duplex color Doppler ultrasonography which is safe, cheap and non-ionizing diagnostic modality before initiating therapy as ED treatment is cause specific.
Keywords: Duplex color doppler ultrasonography, end diastolic velocity, erectile dysfunction, erection hardness score, International index of erectile function questionnaire, peak systolic velocity, phentolamine, prostaglandin – E1, time to erection
Background
Inadequate penile erection, also known as Erectile Dysfunction (ED), is the most common sexual disorder in men. It is defined as the inability to achieve and maintain penile erection of adequate value to perform satisfactory sexual activity. Although the exact prevalence of this disease in the male population is still not completely known, many studies have been conducted, with the Massachusetts Male Aging Study being the first large-scale community-based study of this pathology. This study reported the prevalence of erectile dysfunction to be 2.6%.[1] Another study reported the prevalence to be 52% among non-institutionalized males aged between 40 years and 70 years.[2]
ED is either organic, psychogenic or both in origin. Organic causes are found in 80-90% of patients, and include vasculogenic, neurogenic, anatomic and endocrine causes.[3] Diabetes mellitus, coronary artery disease, and systemic hypertension are systemic problems that could affect penile erection and should be ruled-out clinically. Hemodynamic dysfunction is responsible for most of the cases due to venous incompetency or arterial insufficiency, with a relatively small number of patients suffering from a psychological etiology alone. Arteriogenic ED is either due to impaired cavernosal smooth muscle relaxation or arterial inflow stenosis, which invariably leads to compromised filling of the corpora bodies. In the case of corpora veno-occlusive dysfunction or venous leak, the required intracavernosal pressure is not sustainable. Either point of failure may results in vasculogenic ED. Atherosclerotic disease of internal iliac artery or internal pudendal artery may limit the increase in blood flow required to fill the CC and achieve an erection. The sole aim of color Doppler evaluation in ED is to exclude vasculogenic causes which can be managed by medical and/or surgical means.
The cavernosal arteries are the primary source of blood flow to the corpora cavernosa while dorsal arteries supply blood to the skin and glans of the penis. Multiple anastomotic channels connect the cavernosal arteries with dorsal arteries. Arteriography with selective internal iliac angiography is considered the gold standard in evaluation of arteriogenic impotence.[4] However, this technique is invasive and therefore not suitable as a screening examination. Recently, studies screen for vasculogenic impotence by measuring their clinical response to an intra cavernosal injection of a vasodilating pharmacological agent.
Lue et al.[5] showed that precise Doppler sampling and blood velocity measurements of the deep cavernosal arteries could be performed before and after intracavernosal injection of vasodilating agents and 75% increase in vessel diameter is good indication of normal arterial flow into the cavernosal artery. Commonly many investigators use 60 mg of Papavarine in a 2 ml solution injected into either the right or left corpus cavernosum.
Benson et al.[6] have grouped impotent patients into A. Normal, with an average PSV of 47 cm/sec. B. Mild to moderate with average peak systolic velocity (PSV) of 35 cm/sec. And C. Severe arterial insufficiency with an average PSV of 7 cm/sec. The current study is aimed at using sonography to establish the proportion of ED patients with vasculogenic abnormalities, which could be arteriogenic, venogenic or both.
Penile anatomy
The penis consists of 3 cylinders, 2 dorsal hypoechoic Corpora Cavernosa (CC) surrounded by the thick fibrous sheath of the tunica albuginea and the ventral Corpus Spongiosum (CS) containing the urethra, often compressed and difficult to visualize optimally from the ventral aspect [Figures 1 and 2]. The corpora cavernosa consist of multiple smooth muscle and endothelial-lined sinusoids, which are capable of considerable volume expansion. The albuginea is a 2-layer tunica with outer longitudinal fibers and inner circular fibers visualized as a linear hyperechoic structure, generally less than 2 mm thick. The inner layer constitutes the intracavernosal septum, which is generally complete proximally and becomes fenestrated along the dorsal aspect in the mid-distal part. This anatomy is advantageous, making an injection to just one of the corporal bodies, enough for vasoactive medication to circulate to the contralateral side. The 3 corpora are surrounded by the more superficial Buck´s fascia.
Figure 1.
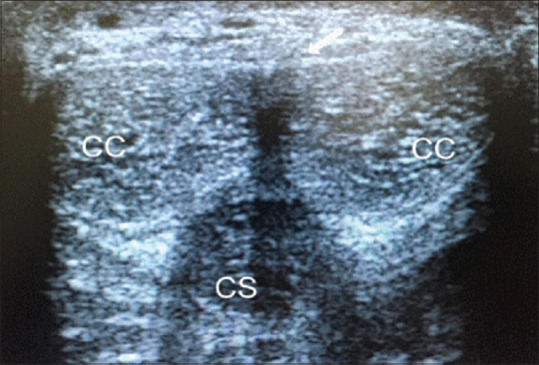
Transverse mid-shaft dorsal scan showing both Corpora Cavernosa (CC) surrounding by hyperechoic tunica albuginea (white arrow) and the more ventral Corpus Spongiosum (CS)
Figure 2.
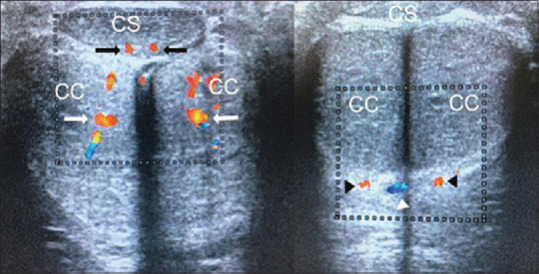
Transverse mid-shaft ventral scan showing both cavernosal arteries (white arrows), both bulbourethral arteries (black arrows), both dorsal arteries (black arrow´s heads) and deep dorsal vein (white arrow head)
The arterial supply of the penis arises from the branches of the common penile artery, which is the direct continuation of the internal pudendal artery. This artery branches into 3 named arteries. The bulbourethral artery enters de spongiosum superiorly and supplies the urethra, the spongiosum and the glans penis. The dorsal artery that courses between the dorsal vein and penile nerves. The cavernosal arteries enter and supply the corpora cavernosa via numerous helicine arteries, which supply the sinusoids via arterioles. These are recognized by their parallel hyperechoic walls [Figure 3]. Anatomical variation in the penile arterial distribution may be as high as 50%.[7] Emissary veins pierce the tunica albuginea to drain into the deep dorsal vein, via the spongiosal, circumflex, and cavernosal veins.
Figure 3.
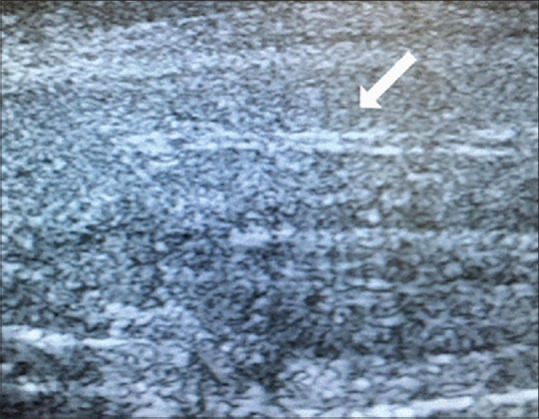
Cavernosal artery showing parallel hyperechoic walls (white arrow)
Methods
Fifty-two consecutive patients with clinical diagnosis of ED referred were evaluated using Doppler ultrasonography between July 2016 and June 2019. Those smoking cigarette among them were instructed to stop 72 h before the study as smoking causes penile vasospasm and increased sympathetic nervous system tone thus affecting penile erection. The procedure was explained in detail to the patients at booking and on the examination day. A drug (antihypertensive, anti-epileptic) and cardiac histories were also inquired before the study. After obtaining informed consent, they were evaluated with color Doppler ultrasound scan (logiQ 500 MD, GE Medical Systems) using high-frequency (7.5 MHz) linear transducer in a quiet and comfortable room to ensure patients’ privacy and cooperation. The study was performed with patients in supine position and penis in normal anatomical position.
After application of ultrasound coupling gel to the ventral surface of the penis, longitudinal and transverse penile scans were done on both grey scale and color Doppler studies before and after injection of PGE1 with the probe on the ventral surface of the penis. Pre-injection scan was to assess the echo pattern of the penis in the flaccid state for the presence of plaques, fibrosis or tunica albuginea defect/fracture. The diameter and peak systolic velocity (PSV) of the cavernosal arteries (CA) were also assessed before intracavernosal injection.
Data collection
About 10-20 μg of PGE1 was injected into either of the corpora cavernosa laterally at the distal two-third of the penis with a 30-gauge needle under aseptic condition. The variation in the doses of PGE1 was based on the patient's age; smaller doses were used for the younger ones while higher doses for the elderly. One-sided injection was also considered because the two corpora cavernosa are separated by a septum which has fenestrations that allow communication between the corpora bodies. The waveforms were obtained alternately using an angle of inclination equal or <60° when visualization of CA was optimal. Immediately after intracavernosal injection (ICI), the longitudinal diameter of each CA, spectral waveform and PSVs of the CAs were documented each at 5 min intervals, from 5-30 min (5, 10, 15, 20, 25 and 30 min). The study was terminated at 30 min for most of the patients except for few that had persistent diastolic flow (venogenic ED/venous leak), who had their studies extended to about 50 min. Due to the variation in the PSV of the CA at different locations across the penile shaft, PSV being higher proximally, CA was consistently interrogated for spectral waveform assessment and measurement at the junction of the proximal third and distal two-third of the penile shaft, where the artery bends. The PSV of CA was determined electronically with the software package of the ultrasound machine. Bilateral CA diameters and PSVs were measured in both flaccid and post-ICI state. The patients were kept in the observation room for 3 hours after the procedure to check for the possibility of complications such as priapism.
Defining arteriogenic ED: Arteriogenic ED was diagnosed when PSV was lower than 35 cm/s. The parameter that is most commonly used to define arteriogenic ED is peak systolic blood flow in the penile arteries. Peak flow rates less than 25cm/s are abnormally low and peak flow rates greater than 35cm/s are normal, but the range of 25-35cm/s is equivocal [Figure 4].
Figure 4.
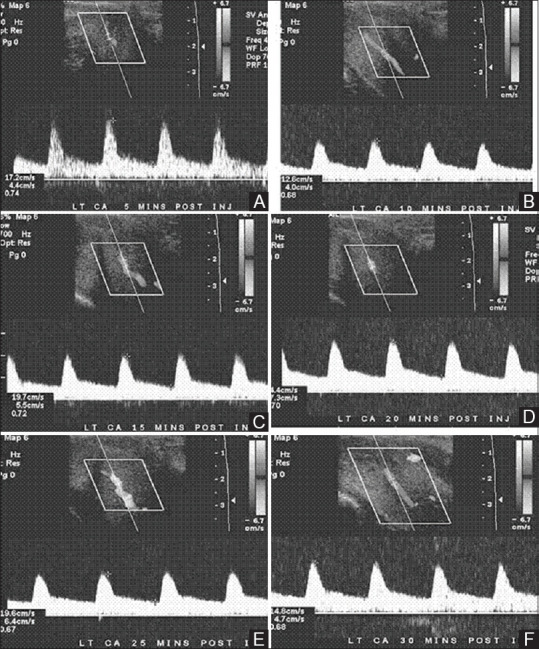
(A-F): Arteriogenic erectile dysfunction (A-F). Sequential timed (at 5, 10, 15, 20, 25 and 30 min) recordings of spectral Doppler waveforms of the cavernosal artery after injection of prostaglandin E1 demonstrating persistent low peak systolic velocity of the cavernosal artery (<25 cm/s)
Defining venogenic ED: Venogenic ED was diagnosed when PSV was higher than 30cm/s, EDV was higher than 5 cm/s and RI was lower than 0.9. The main limitation of this parameter is its lack of specificity for venous leak in the presence of arterial insufficiency [Figure 5].
Figure 5.
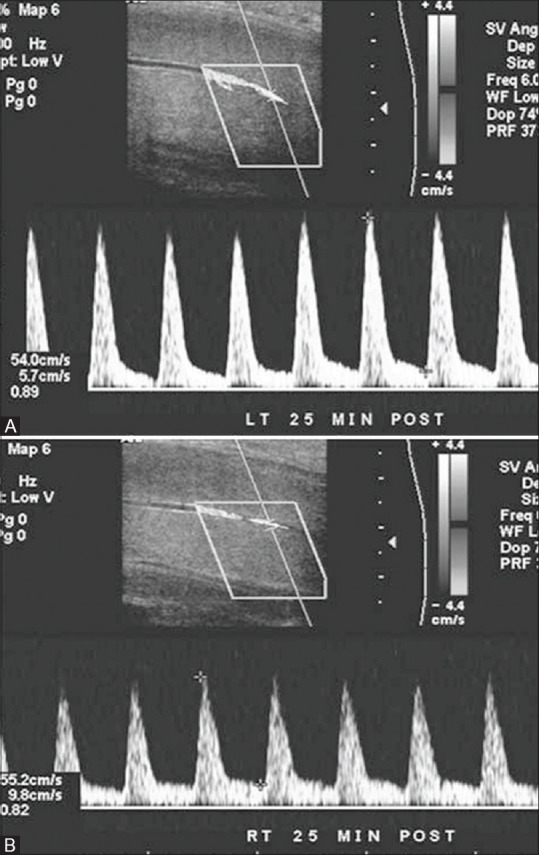
(A and B): Venous leak (veno-occlusive insufficiency). Bilateral spectral Doppler waveforms (A and B) of the cavernosal arteries at 25 min post-injection of prostaglandin E1 demonstrate a high peak systolic velocity (>40 cm/s), which excludes arterial insufficiency as a cause of erectile dysfunction in this patient. However, a persistent diastolic flow velocity of more than 5 cm/s is suggestive of venous leak
Defining arteriogenic-venogenic ED: Mixed arteriogenic-venogenic ED was diagnosed when PSV was lower than 35 cm/s and concomitant EDV was higher than 5 cm/s.
Defining dosages for younger and elderly subjects: Patients younger than 30 years were given 12μg, and patients 60 years or older were given 16 μg. Patients between the age group 30-60 were administered 20 μg of PGE1.
Erection hardness (EH) is a fundamental component of erectile functionand could best define the response to treatment for ED, and can be considered a suitable assessment. EH was evaluated subjectively using the EH Score (EHS), a 5-point response score denoting how the patient would rate his erection, with scores of 0 (penis does not enlarge), 1 (penis is larger but not hard), 2 (penis is hard but not hard enough for penetration), 3 (penis is hard enough for penetration, but not completely hard) and 4 (penis is completely hard and fully rigid).
The study included 52 patients with erectile dysfunction (ED), with a mean (SD) age of 48.4 (9.1) years. ED was subjectively assessed using the International Index of Erectile Function (IIEF-5) questionnaire. The features were measured in the proximal part of the penis with the transducer placed at the urethral (ventral) penile surface. The examination was commenced 3 min after an intracavernosal injection with 10-20 μg of PGE1 and continued for 30 min. The measurements were obtained alternately from both deep penile arteries. The variables analyzed were the peak systolic velocity (PSV), end-diastolic velocity (EDV) and resistive index (RI), calculated as (PSV-EDV)/PSV.
Ethical considerations
All examinations and procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Ethics Committee (IEC) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all patients prior to their enrollment in this study (IEC, Holy Family Hospital; IEC Approval Reference Number: HFH/12/2016; IEC Approval Date: June 20, 2016).
International Index of Erectile Function (IIEF): The IIEF is a validated self-administered questionnaire used to assess therapeutic efficacy of ERD therapy. It is composed of 5 domains: 1. Erectile function (Questions 1-5 and 15, total maximum score of 30; score of 26 = normal erectile function; 22-25 = mild ERD; 17-21 = mild-to-moderate ERD; 11-16 = moderate ERD; and 1-10 = severe ERD). The International Index of Erectile Function (IIEF) has been proposed as a sensitive and specific tool in the investigation of male sexual dysfunction. The IIEF is a standardized patient questionnaire that has been validated in several languages. This instrument measures multiple domains of male sexual behavior and has already been used in the evaluation of pharmacologic therapy for ED. The current study prospectively scored the erectile specific questions of the IIEF.
A total of 52 patients completed the IIEF at their physician's office. The IIEF includes elements investigating the following domains of male sexual behavior: erectile function, orgasmic function, desire, intercourse satisfaction, and global sexual satisfaction. All questions were scored from 0 to 5. Six of the questions in the IIEF evaluate male sexual performance. An IIEF score of 25 is expected in a normal individual. The original IIEF (International Index of Erectile Function) questionnaire was validated using 15 questions, which helped in assessing the severity of the disease and the efficacy of treatment. The IIEF-5 questionnaire consists of five important questions to quickly identify a need for further consultation and diagnosis: How do you rate your confidence that you could get and keep an erection?Very low (1 point) - low (2 points) - moderate (3 points) - high (4 points) - very high (5 points). When you had erections with sexual stimulation, how often were your erections hard enough for penetration?Almost never or never (1 point) - Much less than half the time (2 points) - About half the time (3 points) - Much more than half the time (4 points) - Almost always or always (5 points). During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner?Almost never or never (1 point) - Much less than half the time (2 points) - About half the time (3 points) - Much more than half the time (4 points) - Almost always or always (5 points). During sexual intercourse how difficult was it to maintain your erection to the completion of intercourse?Extremely difficult (1 point) - very difficult (2 points) - difficult (3 points) - slightly difficult (4 points) - not difficult (5 points). When you attempted sexual intercourse, how often was it satisfactory for you?Almost never or never (1 point) - Much less than half the time (2 points) - About half the time (3 points) - Much more than half the time (4 points) - Almost always or always (5 points). Evaluation of the IIEF-5:no erectile dysfunction (22–25 points), mild erectile dysfunction (17–21 points), mild to moderate erectile dysfunction (12–16 points), moderate erectile dysfunction (8–11 points), severe erectile dysfunction (less than 8 points).
All patients underwent a complete history and physical examination. Patients with presumed neurogenic impotence were excluded and all patients underwent age-specific dosing of PGE1 and color duplex Doppler ultrasound scanning 5 minutes after injection. They were then given privacy for self-stimulation, and subsequently underwent ultrasound scanning again (15 to 20 minutes after injection). The flow associated with the best erectile response (either before or after self-stimulation) was used for analysis. If erectile responses were equal before and after self-stimulation, the higher flow rate was analyzed. All studies were performed using a high-frequency (7.5 MHz) linear transducer on logiQ 500 MD, GE Medical Systems. Flow velocities were measured in the sagittal plane with the shaft extended. Cavernous arteries were assessed bilaterally for peak systolic velocity (PSV), end-diastolic velocity, and resistive index (RI). Investigator performing the diagnostic testing was unaware of the IIEF scores and rated erections. To statistically compare PGE1 pharmacologic testing to the IIEF, the visual erectile responses were assigned 3 categories: inadequate for penetration, adequate for penetration, or excellent with sustained rigidity for at least 20 minutes after injection. Erectile responses to PGE1 were graded according to EHS scores – E0: no response E1: elongation of shaft E2: moderate tumescence E3: full tumescence, easily bendable E4: erection, partial rigidity E5: rigid, well sustained >20 minutes. Patients with an erection EHS score <3, even in the presence of an EDV >5 cm/s proceeded to intracavernosal administration of 2 mg phentolamine. Blood pressure was measured prior to and 15 min after phentolamine administration. Repeat measurements were recorded at 5 min intervals and grade every 10 min for 30 min.
The results were reported as mean ± (standard deviation). The collected data were analyzed using Statistical Package for the Social Sciences (IBM SPSS) version 26 (United States). All test of significance were two-tailed, and P < 0.05 was considered statistically significant. ANOVA test was applied between variables like age and peak systolic velocities of the cavernosal arteries (cm/s) among the entire participants. For statistical analysis, non-parametric Friedman test for significant differences between repeated measurements in small groups and Wilcoxon test for differences between doses were used.
Technique of dynamic infusion cavernosometry and cavernosography (DICC)
A total of 10 microgram (2mL) of PGE1 was given intracavernosally with a 24 gauge needle with pressure application at the base of the penis. 10 minutes later, two 21 gauge scalp vein needles were introduced into both corpora, one attached to the flow and the other to the pressuretransducer to record intracavernous pressure (ICP). Cavernosometry was started with the infusion of saline with an IVAC 770 infusion pump device until full erection was achieved. The flow to induce an erection and the flow to maintain the erection were noted and when full erection was achieved the flow was stopped and ICP was recorded for 30 s and 5 min. Simultaneous cavernosography was performed to correlate the findings. The patient is positioned with one hip (usually the right) down and the other elevated on a foam wedge so as to form an angle of 30 degrees with the table. Omnipaque 300 is added to the heparinized saline in 1:1 dilution and infused through the pump. One hundred ml of contrast are infused at a rate to stabilize ICP at 90 cm H20. Radiographs are taken when 90 ml have been refused and again after stopping the infusion. The presence of contrast material in the deep dorsal vein and crural veins was noted. Minimal leakage on cavernosography is maintenance flow rate of 30-50 ml/min, an ICP drop of 50-70 cm H20 from 150 cm H20 after 30 s of stopping infusion and ICP measurement of 31-50 cm H2O after 5 min. Moderate leakage relates to maintenance flow rate of 51-100 ml/min, an ICP drop of 71-120 cm H20 from 150 cm H20 after 30 s of stopping and ICP measurement of 21-30 cm H20 after 5 min. Severe leakage relates to maintenance flow rate of >120 ml/min, an ICP drop of >120 cm H20 from 150 cm H20 after 30 s of stopping infusion and ICP measurement of <20 cm H2O after 5 min.
Results
Fifty-two consecutive patients with clinical diagnosis of ED between 28 and 70 years (mean age, 48.4 ± 9.8 years) presented for this study. Age group of the majority of patients were in fourth to fifth decades. The mean PSV of CA on the right and left sides, respectively, were 42.4 ± 19.2 cm/s and 41.6 ± 17.7 cm/s. Paired samples correlation and paired samples test showed no significant differences between the PSVs of the right and left CA [Tables 1 and 2]. Hence, the PSV of the right and left were analyzed together. The measured PSV varied post-injection of PGE1 between 16.8 and 51.6 cm/s among the patients [Table 3] and between 16.4 and 22.4 cm/s among patients with arteriogenic ED [Table 4]. Abnormal response to PGE1(arteriogenic ED) was found in six (13%) of the patients. No significant discrepancies were noted between right and left CA PSV among the entire patients (P = 0.44) and among the patients with arteriogenic ED (P = 0.521). The mean PSV of CA among the entire patients was 42.57 ± 11.28 cm/s [Table 3], while mean PSV among the patients with arteriogenic ED was 20.1 ± 1.97 cm/s [Table 5]. Persistent diastolic flow in CA after injection of PGE1 and dorsal vein peak velocity >5 cm/s, both being consistent with venogenic ED, were found in 12 patients, which constitutes 23% of the patients. No patient had combined arteriogenic and venogenic ED. Arteriogenic ED had no direct relationship with age [Table 5], but the PSV of the entire patients had a strong positive relationship with age, with P < 0.0001 [Table 6]. A significant decline in the PSV of CA was observed with respect to age of the patients.
Table 1.
Means and standard deviations of the right and left cavernosal artery peak systolic velocities
| Variable | n | Minimum | Maximum | Mean +/- SD |
|---|---|---|---|---|
| Age (years) | 52 | 28 | 70 | 48.4 +/- 9.8 |
| Right CA PSV (cm/s) | 52 | 20.1 | 106.8 | 42.4 +/- 19.2 |
| Left CA PSV (cm/s) | 52 | 19.7 | 92.4 | 41.6 +/- 17.7 |
Table 2.
Paired samples test of right and left cavernosal artery peak systolic velocities
| Paired differences | t | df | Significant (two-tailed) | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | SEM | 95% CI of difference | |||||
| Lower | Upper | |||||||
| Right CA PSV (cm/s)-Left CA PSV (cm/s) | 0.89 | 7.94 | 1.10 | -1.63 | 3.72 | 0.68 | 38 | 0.44 |
The average difference (0.89) between the right and left CA PSV of 52 patients is not significant (P=0.44). PSV: Peak Systolic Velocity. CA: Cavernosal arteries. SD: Standard Deviation. CI: Confidence Interval. SEM: Standard error of Mean
Table 3.
Frequency distribution of the entire patients with the respective cavernosal artery peak systolic velocities
| Age (years) | n | Mean PSV (cm/s) | SD | Minimum PSV (cm/s) | Maximum PSV (cm/s) |
|---|---|---|---|---|---|
| <30 | 1 | - | - | 68.2 | 80.2 |
| 31-35 | 2 | 41.3 | 6.2 | 38.3 | 44.3 |
| 36-40 | 4 | 44.4 | 10.2 | 40.2 | 48.6 |
| 41-45 | 9 | 39.75 | 8.3 | 32.4 | 47.1 |
| 46-50 | 11 | 35.55 | 7.6 | 25.6 | 45.5 |
| 51-55 | 11 | 38.45 | 11.7 | 22.8 | 54.1 |
| 56-60 | 8 | 45.4 | 20.1 | 33.1 | 57.7 |
| 61-65 | 4 | 33.2 | 15.3 | 21.6 | 44.8 |
| 66-70 | 2 | 30.9 | 17.4 | 19.7 | 42.1 |
| Total | 52 | 42.57 | 11.28 | 16.77 | 51.6 |
PSV: Peak Systolic Velocity, SD: Standard Deviation
Table 4.
Mean peak systolic velocities of the right and left cavernosal artery among patients with arteriogenic erectile dysfunction descriptive statistics
| Variable | n | Minimum | Maximum | Mean +/- SD |
|---|---|---|---|---|
| Age (years) | 8 | 28.0 | 64.0 | 46.4 +/- 10.8 |
| Right CA PSV (cm/s) | 8 | 18.4 | 22.2 | 20.3 +/- 1.21 |
| Left CA PSV (cm/s) | 8 | 18.2 | 23.8 | 21.0 +/- 1.42 |
PSV: Peak Systolic Velocity, CA: Cavernosal arteries, SD: Standard Deviation
Table 5.
Relationship between age (years) and peak systolic velocities of cavernosal arteries (cm/s) among patients with arteriogenic erectile dysfunction (ANOVA)
| Age (years) | n | Mean PSV (SD) | P |
|---|---|---|---|
| 31-35 | 2 | 21.3 (2.2) | 0.762 |
| 41-45 | 4 | 19.7 (1.7) | |
| 56-60 | 1 | 20.4 (-) | |
| 61-65 | 1 | 19.2 (-) | |
| Total | 8 | 20.1 (1.97) |
PSV: Peak Systolic Velocity, SD: Standard Deviation
Table 6.
Relationship between age and peak systolic velocities of the cavernosal arteries (cm/s) among the entire participants (ANOVA)
| Age (years) | n | Mean PSV (SD) | F (df) | P |
|---|---|---|---|---|
| <30 | 1 | - | 4.732 (8.92) | 0.0001 |
| 31-35 | 2 | 41.3 (6.2) | ||
| 36-40 | 4 | 44.4 (10.2) | ||
| 41-45 | 9 | 39.75 (8.3) | ||
| 46-50 | 11 | 35.55 (7.6) | ||
| 51-55 | 11 | 38.45 (11.7) | ||
| 56-60 | 8 | 45.4 (20.1) | ||
| 61-65 | 4 | 33.2 (15.3) | ||
| 66-70 | 2 | 30.9 (17.4) | ||
| Total | 52 | 42.57 (11.28) |
Significant differences exist between PSV of CA among age groups (P<0.0001). PSV: Peak Systolic Velocity, CA: Cavernosal arteries, SD: Standard Deviation
Twenty-six patients (50%) had Doppler criteria of vascular ED and were further subcategorized based on their penile duplex color Doppler study. Eight patients (15.3%) with a mean PSV less than 25 cm/s were classified as having arterial insufficiency. Twelve patients (23%) with a mean PSV greater than 35 cm/s and an RI less than 0.9 were classified as having cavernous venous occlusive disease (CVOD), and 6 patients (11.5%) with a PSV between 25 and 35 cm/s were classified as having mixed vascular ED [Table 7].
Table 7.
Data summary for penile blood flow study using duplex color Doppler ultrasonography and IIEF questionnaire
| Doppler Diagnosis | Patients (n) | Mean PSV | Mean EDV | RI | IIEF |
|---|---|---|---|---|---|
| Arterial insufficiency | 8 | 20.1±1.9 cm/s | 0.4±0.7 cm/s | 0.71 | 7.2 |
| Mixed | 12 | 32.7±2.2 cm/s | 9.8±1.3 cm/s | 0.82 | 8.8 |
| Cavernous venous occlusive disease | 6 | 46.3±3.1 cm/s | 8.8±0.5 cm/s | 0.76 | 9.1 |
Among patients with venogenic ED and mixed arteriogenic-venogenic ED, 2 patients had a normal erectile response and the remaining 16 received phentolamine. A significant increase in PSV between baseline and 20 mg PGE1 (P < 0.001) was observed in all cases. Following phentolamine there was a significant increase in grade of erection (P = 0.0001) and a significant reduction in the EDV (P = 0.0001). A reduction of the EDV to below 0.0 cm/s was observed in 12 patients. In patients with arteriogenic erectile dysfunction, mean (±standard deviation) duration of erection for consecutive doses of PGE15 μg, 10 μg, 15 μg, and 20 μg were 42.2±18.4, 55.4±24.1, 66.1 ± 31.1, and 83.3±36.7 minutes, respectively, with significant increase for each dose. In patients with veno-occlusive dysfunction, mean durations of erection significantly increased from 9.1±8.0 minutes at 10 μg to 19.2±9.8 minutes at 20 μg [Table 8].
Table 8.
Longitudinal changes in the response variables following 20 μg of prostaglandin E1 (PGE1) and 2 mg phentolamine
| 20 mg PGE1 | 2 mg Phentolamine | P | |
|---|---|---|---|
| PSV | 48 cm/s | 52.6 cm/s | P<0.001 |
| EDV | 7.7 cm/s | 1.8 cm/s | P=0.0001 |
Sixteen out of 18 study patients received phentolamine. (PSV, peak systolic velocity measured in cm/s; EDV, end diastolic velocity measured in cm/s)
Arteriogenic erectile dysfunction
Mean age ± SD of the patients in this group was 56.4±10.3 years. Mean peak systolic velocity in this group was 20.1 ± 1.97 cm/s, and mean end diastolic velocity was 0.4±0.7 cm/s. Mean duration of erection significantly increased with the increasing dose, from 42.2±18.4 at 5 μg to 83.3±36.7 at 20 μg (Friedman test, P < 0.001). Wilcoxon signed rank test revealed a significant increase in duration of erection with each higher dose.
Veno-occlusive dysfunction
Patients in this group had a mean age of 37.6±22.0 years, mean peak systolic velocity of 46.3±3.1 cm/s, and mean end diastolic velocity of 8.8±0.5 cm/s. In statistical analysis, the value of zero (0) minutes was used for these patients. Mean duration of the erections increased 6.4±7.3 minutes at the 5 μg to 19.2±9.8 minutes at the 20 μg (Friedman test, P=0.005). Wilcoxon signed rank test revealed significant increase in duration of erection with highest dose, but not in low dose range of PGE1.
Dynamic infusion cavernosometry and cavernosography (DICC)
Following intracavernous injection of intracavernosal PGE1, peak systolic velocity (PSV), end diastolic velocity (EDV), resistance index (RI), and pulsatility index (PI) were measured in the cavernous arteries over 30 min. The presence of persistent diastolic flow and elevated end-diastolic velocities were indirect indicators of veno-occlusive failure and the diagnosis of venous incompetence is made only if the patient has normal peak systolic velocity (>25 cm/sec). The results were compared with independent measurements based on Dynamic infusion cavernosometry and cavernosography (DICC) which is the reference standard for diagnosis of venous impotence. DICC performed on patients diagnosed with venogenic ED on color Doppler ultrasonography revealed venous leakageand no statistically significant differences between results of DICC and color Doppler ultrasonography were found in EDV, RI, and PI measurements (P < 0.005). Eight patients demonstrated minimal leakage, 4 patients demonstrated moderate leakage and none demonstrated severe leakage.
Discussion
The threshold values for the diagnosis of arterial insufficiency vary in the literature,[6] with values of 25–35 cm/ssuggested. A PSV of <25 cm/s has been correlated with severe arterial disease on angiographic imaging.[8] Penile Doppler ultrasonography not only enables the arterial waveform to be analyzed but also allows for visualization of stenoses, damped waveforms and high-velocity that may occur as a result of a proximal stenosis elsewhere. Venous incompetence can cause ED through failure of cavernosal engorgement. On Penile Doppler ultrasonography this is manifested by persistent diastolic flow and elevated end-diastolic velocity. Again, various threshold EDV values have been suggested between 5 and 7 cm/sas diagnostic of venous incompetence.[9] However, such threshold values for EDV can be misleading if arterial insufficiency is present. In these cases, resistive indices (RI) <0.75 may be helpful in predicting venous leakage, although measurement of RI is not usually undertaken in our practice.[10]
Role of penile Doppler ultrasonography has been discussed because it provides operator dependent information and, considering currently available therapy for ED (especially PDE5-inhibitors), rarely alters following patient management. In patients showing normal PSV value associated with incomplete erectile response and RI value under 0.85, a probable veno-occlusive mechanism alteration should be considered as cause of erectile dysfunction.[11] Nevertheless, penile dynamic color-duplex Doppler ultrasonography is not sufficient to make diagnosis of venous leak because of its low specificity due to incomplete rigidity of corpora cavernosa and persistence of diastolic flow. In order to formulate a correct diagnosis of venous leak, cavernosometry/cavernosography remains the gold standard.[12]
Out of all patients in the present study, 20 (38.4%) had ED of vasculogenic origin; 23% venogenic and 15.3% arteriogenic which affirmed the observation of Quam et al.[13] where a good number of their patients had ED of vascular origin, hence the need for ultrasound in the evaluation of ED. Similarly, Sen et al.[14] and Roy et al.[15] in their respective studies observed that 22.5% and 29%, respectively, had arteriogenic ED while it was 23% in the current study. In the current study, none of the patients had secondary criteria for diagnosis of arteriogenic ED. Majority of the patients in the current study ranged between 40 and 60 years, which constitutes 75%, while only 3 patients (5.7%) were <35 years of age. The mean age of patients with arteriogenic ED in the present study was 53.4 ± 11.2 years and the mean CA PSV of the patients was 20.1 ± 1.97 cm/s. Furthermore, the mean age of those with venogenic ED (venous leak) was 57.1 ± 6.3 years. A positive correlation was also established between patients’ age and PSV of CA. The highest PSV of CA was found in patients <30 years with a mean PSV of 74.2 cm/s, while the lowest PSV (30.9 cm/s) was found in patients between 66 and 70 years of age. Only one patient aged 28 years had arteriogenic ED, and the youngest with venogenic ED was 47 years of age making it obvious from the findings that vasculogenic ED is age-related and has further reaffirms the previous submissions of other authors that ED is seen commonly in patients above 40 years of age.
Data from the current study shows a limited role for the IIEF in the clinical setting. IIEF scores were unable to distinguish among etiologies of ED as determined by duplex Doppler testing. When patients were separated into two groups on the basis of pharmacologic testing and visual ratings of excellent versus inadequate, the IIEF scores showed an appropriate arithmetic trend and were statistically different from one another. However, the mean score for the excellent responders was still dramatically abnormal. The overall variations in IIEF scores between groups in this study were quite small, and it is doubtful that they would be useful in the selection of treatment doses. Pastuszak[16] reinforces this concept in a recent study in which he found no differences in pretreatment scores between individuals with organic, psychogenic, or mixed ED.
False-positive results when diagnosing venous ED via duplex color doppler ultrasonography
The reference standard for diagnosis of venous impotence remains dynamic cavernosography with cavernosometry, a procedure that is invasive, involves ionizing radiation and use of iodinated contrast media.[17] Doppler ultrasound (US), performed following intracavernosal administration of prostaglandin E1 (PGE1) to induce an erection, is less invasive and reliably documents venous leakage in the presence of maximal corporeal smooth muscle relaxation. Cavernosometry quantifies intracorporal pressure after intracavernosal injection and is useful primarily for establishing a diagnosis of veno-occlusive dysfunction.[18] Typically, cavernosometry is performed in conjunction with cavernosography (intracorporal installation of a radio-opaque dye), permitting detailed localization of areas of leak. However, Doppler US assessment may lead to an erroneous interpretation of venous leakage when there is a suboptimal response to PGE1 injection due to anxiety related elevated adrenergic tone. There was a 35% (statistically significant) improvement in color Doppler US parameters in the group receiving both PGE1 and phentolamine compared with a 15% observed in the control group of patients re-dosed with PGE1 alone.[19] The percentage of ‘’false positive’’ diagnosis of venous leakage unmasked by phentolamine re-dosing was particularly high in our study (67%). Doppler ultrasonography is recognized as a reliable investigation to assess penile arterial integrity, although some authors report a lower sensitivity of Doppler US over cavernosometry in the assessment of venogenic impotence.[20] In the current study, following 20 μg PGE1, a small number of patients responded with a normal Doppler ultrasonography pattern and developed full rigidity. In the majority an equivocal and a suboptimal erection pattern of venous leakage emerged. Interpretation may lead to a possible diagnosis of venogenic impotence, leading to further and more invasive investigations. A completely normal unequivocal response would be full rigidity (grade IV) and reversal of flow in diastole. With the addition of intracavernous phentolamine 12 out of 52 patients (23%) achieved a fully rigid erection. Following the addition of phentolamine a slight (although not significant) increase in the PSV was evidenced compared with 20 μg PGE1. This effect may be explained by the blockade of sympathetic neuronal tone that phentolamine exerts on the arteriolar smooth muscle.
Further ultrasonography findings
The penis was also assessed for the presence of non-vascular abnormalities such as plaques, areas of fibrosis and defects in the tunica albuginea once full tumescence has been achieved. The current study encountered 2 patients with Peyronie's disease which is a localized benign connective tissue disorder that results in fibrous thickening of the penile tunica albuginea. Ultrasonography revealed hyperechoic thickened plaques of the tunica albuginea, which demonstrated calcification and hyperperfusion surrounding the plaques. The circumferential narrowing of the corpora cavernosa resulted in an “hourglass appearance” in the erect penis. Peyronie disease is characterized by progressive curvature and shortening of the penile shaft, and may be associated with a palpable nodule, eventually leading to the development of pain during erection and dyspareunia. Gray-scale penile ultrasonography shows multiple calcified nodules along the tunical envelope of the cavernosum, associated with veno-occlusive ED. In the early stage of the disease, inflammation predominates and lasts for 12-18 months, causing erectile discomfort and unstable curvature. In this early phase, hyperperfusion can be demonstrated around the plaques by power Doppler. A more chronic phase follows with stable deformity and plaque size. Peyronie's disease has a prevalence up to 3%, and typical features include pain upon erection, penile curvature, loss of girth and veno-occlusive ED.[21] One patient developed priapism (an erection that lasts for more than 4 hours) after intracavernosal injection of PGE1, was put under observation in the emergency department and was treated conservatively with analgesia, hydration and oxygenation. Priapism was relieved after 5 hours and the patient was discharged.
Conclusion
In conclusion, penile Doppler ultrasonography is of vital importance in documenting any vascular abnormalities contributing to ED. In the current study, fifty percentage of patients had vasculogenic ED and “false positive’’ diagnosis of venous leakage was unmasked by phentolamine re-dosing. IIEF is a useful tool in the taking of the male sexual history and is a good starting point for the evaluation of ED. However, IIEF scores did not correlate with duplex color Doppler ultrasonography assessments. It is therefore imperative that patients with ED benefit from prostaglandin induced duplex color Doppler ultrasonography which is safe, cheap and non-ionizing diagnostic modality before initiating therapy as ED treatment is cause-specific.
Limitations of the study
The findings of the current study should be noted in the light of the following limitations. First, a psychogenic cause was determined based on the combination of the patient's history and normal ultrasound findings. Identifying the cause-and-effect relationship of the psychogenic causes related to anxiety, depression, and other social factors, and research utilizing standardized questionnaires should be carried out for this purpose. The second limitation of this study is that the arterial velocities are the maximum near the base of the penis and decrease as they advance; operator dependency may have led to variability in recording the velocities. To minimize this variability, we need to record the velocities near the base of the penis where they are highest. Third, organic causes of erectile dysfunction were identified on the basis of color Doppler findings, and their relationship with risk factors such as hypertension, diabetes, and metabolic syndrome could not be clarified. Various studies have reported diabetes mellitus, hypertension, hyperlipidemia, metabolic syndrome, depression, and lower urinary tract symptoms to be causes of erectile dysfunction. The current study was not able to determine the developmental cause of erectile dysfunction in the study population.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Huang ST, Hsieh ML. Different hemodynamic responses by color Doppler ultrasonography studies between sildenafil non-responders and responders. Asian J Androl. 2007;9:129–33. doi: 10.1111/j.1745-7262.2007.00227.x. [DOI] [PubMed] [Google Scholar]
- 2.Araujo AB, Travison TG, Ganz P, Chiu GR, Kupelian V, Rosen RC, et al. Erectile dysfunction and mortality. J Sex Med. 2009;6:2445–54. doi: 10.1111/j.1743-6109.2009.01354.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dick B, Reddy A, Gabrielson AT, Hellstrom WJ. Organic and psychogenic causes of sexual dysfunction in young men. Int J Med Rev. 2017;4:102–11. [Google Scholar]
- 4.Foresta C, Caretta N, Palego P, Selice R, Garolla A, Ferlin A. Diagnosing erectile dysfunction: Flow-chart. Int J Androl. 2005;28:64–8. doi: 10.1111/j.1365-2605.2005.00588.x. [DOI] [PubMed] [Google Scholar]
- 5.Aiyekomogbon JO, Igashi JB, Lawan RO, Bioku MJ, Ameadaji M. Colour doppler sonography of the penis in the evaluation of erectile dysfunction: Our experience in Abuja, Nigeria. Niger Postgrad Med J. 2017;24:210. doi: 10.4103/npmj.npmj_144_17. [DOI] [PubMed] [Google Scholar]
- 6.Khanzada U, Khan SA, Hussain M, Adel H, Masood K, Adil SO, et al. Evaluation of the causes of erectile dysfunction in patients undergoing penile Doppler ultrasonography in Pakistan. World JMens Health. 2017;35:22–7. doi: 10.5534/wjmh.2017.35.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jung DC, Park SY, Lee JY. Penile Doppler ultrasonography revisited. Ultrasonography. 2018;37:16–24. doi: 10.14366/usg.17022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Altinbas NK, Hamidi N. Penile Doppler ultrasonography and elastography evaluation in patients with erectile dysfunction. PolJRadiol. 2018;83:e491. doi: 10.5114/pjr.2018.80301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yafi FA, Libby RP, McCaslin IR, Sangkum P, Sikka SC, Hellstrom WJ. Failure to attain stretched penile length after intracavernosal injection of a vasodilator agent is predictive of veno-occlusive dysfunction on penile duplex Doppler ultrasonography. Andrology. 2015;3:919–23. doi: 10.1111/andr.12073. [DOI] [PubMed] [Google Scholar]
- 10.Pezzoni F, Scroppo FI. Penile vascular diagnostic categorization using penile duplex Doppler ultrasound: Differences in vascular hemodynamics parameters by differences in anatomic sampling location. Arch ItalUrolAndrol. 2016;88:183–5. doi: 10.4081/aiua.2016.3.183. [DOI] [PubMed] [Google Scholar]
- 11.Gandaglia G, Briganti A, Jackson G, Kloner RA, Montorsi F, Montorsi P, et al. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur Urol. 2014;65:968–78. doi: 10.1016/j.eururo.2013.08.023. [DOI] [PubMed] [Google Scholar]
- 12.Bella AJ, Brant WO, Lue TF. Penile anatomy. In: Bertolotto M, editor. Color Doppler US of the Penis. Berlin: Springer; 2012. pp. 11–4. [Google Scholar]
- 13.Belgrano E, Bucci S, Liguori G, Trombetta C. Clinical evaluation of erectile dysfunction in the era of PDE-5 inhibitors: The residual role of penile color Doppler US. In: Bertolotto M, editor. Color Doppler US of the penis. Berlin: Springer; 2008. pp. 21–3. [Google Scholar]
- 14.Sen J, Godara R, Singh R, Airon RK. Colour Doppler sonography of flaccid penis in evaluation of erectile dysfunction. Asian J Surg. 2007;30:122–5. doi: 10.1016/S1015-9584(09)60144-5. [DOI] [PubMed] [Google Scholar]
- 15.Golijanin D, Singer E, Davis R, Bhatt S, Seftel A, Dogra V. Doppler evaluation of erectile dysfunction: Part 1. Int J Impot Res. 2007;19:37–42. doi: 10.1038/sj.ijir.3901477. [DOI] [PubMed] [Google Scholar]
- 16.Pastuszak AW. Current diagnosis and management of erectile dysfunction. Curr Sex Health Rep. 2014;6:164–76. doi: 10.1007/s11930-014-0023-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gao QQ, Chen JH, Chen Y, Song T, Dai YT. Dynamic infusion cavernosometry and cavernosography for classifying venous erectile dysfunction and its significance for individual treatment. Chin Med J (Engl) 2019;132:405–10. doi: 10.1097/CM9.0000000000000099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gontero P, Sriprasad S, Wilkins CJ, Donaldson N, Muir GH, Sidhu PS. Phentolamine re-dosing during penile dynamic colour Doppler ultrasound: A practical method to abolish a false diagnosis of venous leakage in patients with erectile dysfunction. Br J Radiol. 2004;77:922–6. doi: 10.1259/bjr/51141708. [DOI] [PubMed] [Google Scholar]
- 19.Bernie HL, Segal R, Le B, Burnett A, Bivalacqua TJ. An empirical vs risk-based approach algorithm to intracavernosal injection therapy: A prospective study. Sex Med. 2017;5:e31–6. doi: 10.1016/j.esxm.2016.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cavallini G, Maretti C. Unreliability of the duplex scan in diagnosing corporeal venous occlusive disease in young healthy men with erectile deficiency. Urology. 2018;113:91–8. doi: 10.1016/j.urology.2017.11.005. [DOI] [PubMed] [Google Scholar]
- 21.Patel DV, Halls J, Patel U. Investigation of erectile dysfunction. Br J Radiol. 2012;85:S69–78. doi: 10.1259/bjr/20361140. [DOI] [PMC free article] [PubMed] [Google Scholar]