

Abstract
Torsion of epididymal cyst (EC) is an exceedingly rare cause of acute scrotum in both children and adults. We add our case as the ninth case to literature which was an 8-year-old child presented with features of acute scrotum with history of EC on conservative management. Doppler sonography showed perfused normal bilateral testes and a 4.1 × 1.7 cm septate cystic lesion of right epididymis. On scrotal exploration, we found a haemorrhagic cystic lesion attached to the upper pole of right testis and twisted for 540 degrees with normal testis and appendage. Cyst was excised, and histopathology revealed a haemorrhagic EC. Our case was peculiar due to, presenting as acute scrotum in a child of 1-10 years age group who was conservatively managed for right-sided EC and presence of 540 degrees torsion.
1. Introduction
Acute scrotum can be considered as a urological equivalent of acute abdomen in general surgery. There are myriad of causes for acute scrotum ranging from torsion of testes or appendages, traumatic injuries, infections and inflammatory conditions of testes. Several conditions will require scrotal exploration, and patients should be assessed clinically along with imaging studies as it is time sensitive.
Epididymal cyst (EC) is a benign lesion in children and ranges from 5% to 20% in the literature in contrast to adults where it is common [1]. They are of unknown aetiology, common in testicular maldescent, and managed conservatively with spontaneous regression in most instances [2]. Torsion of EC is rare and a scarce finding on scrotal exploration for acute scrotum. There were eight paediatric cases reported in the literature (Table 1), and among them, seven cases were all adolescents, and one was an infant [1, 3–5]. Our patient is an 8-year-old child and the first case of EC torsion in this age group to be reported and added as the ninth case to the literature.
Table 1.
List of cases in literature with brief description.
| Case no. | Authors | Brief description |
|---|---|---|
| 1st case | RI. Kaye et al., 1990 | Left-sided 360° torsed EC in a 13-year-old boy |
| 2nd case | N. Liolios et al., 1997 | Left-sided 360° torsed EC in a 6-month-old male |
| 3rd case | E. Yılmaz et al., 2004 | Left-sided 720° torsed EC in a 13-year-old boy with history of scrotal trauma |
| 4th case | V. Erikçi et al., 2013 | Left-sided 720° torsed EC in an 11-year-old boy on conservative management for EC with no history of scrotal trauma |
| 5th case | Y. Akın et al., 2014 | Bilateral simple ECs in a 14-year-old boy with no history of scrotal trauma |
| 6th case | M. Ameli et al., 2015 | Left-sided 720° torsed EC in a 14-year-old boy with history of scrotal trauma |
| 7th case | C. Bleve et al., 2018 | Right-sided 720° torsed EC in a 16-year-old boy with no history of scrotal trauma |
| 8th case | M. Messina et al., 2019 | Left-sided twisted EC in a 13-year-old boy with no history of scrotal trauma |
| This case | Right-sided 540° torsed EC in an 8-year-old child with no history of scrotal trauma who was on conservative management for EC. |
2. Case Presentation
An 8-year-old boy was admitted to our casualty ward with persistent scrotal pain of 2 days duration associated with nausea and one episode of vomiting. He was treated by local general practitioner with analgesics the day prior and denied preceding trauma to scrotum. But he was investigated for right hemi-scrotal pain without any history of trauma 2 months back in a peripheral hospital. He was diagnosed to have a right-sided EC and opted for conservative management.
On examination, right hemi-scrotal tenderness and high riding right testis were found. Left hemi-scrotal palpation, abdominal examination, and hernial orifices were unremarkable. Urgent sonography with Doppler showed a septate cystic lesion of right epididymis, sized 4.1 cm × 1.7 cm (Figure 1) along with bilateral normally echogenic and perfused testes.
Figure 1.
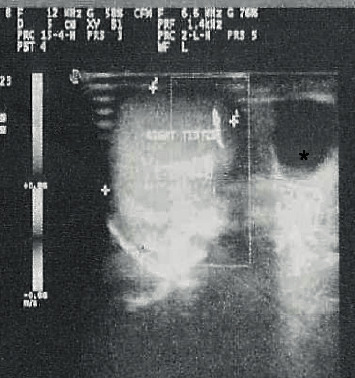
Ultrasound image of right testis with epididymal cyst∗ (on acute presentation).
Scrotal exploration under general anaesthesia was performed which revealed oedematous tunica vaginalis, age appropriately sized right testis, normal testicular appendage, and 4 cm × 2 cm sized dark haemorrhagic cystic lesion. The lesion appeared to be attached to the upper pole of right testis and was twisted for 540 degrees (Figure 2).
Figure 2.

Twisted right Epididymal cyst with normal testis.
Cyst was untwisted (Figure 3) and excised, and the testis was fixed. Histopathological assessment revealed haemorrhagic EC (Figure 4). Patient was discharged the next day following unremarkable recovery, with analgesics and oral antibiotics.
Figure 3.

Untwisted hemorrhagic right Epididymal cyst.
Figure 4.

(a) Low and (b) high power views of the epididymal cyst wall with columnar epithelium showing congestion and haemorrhage.
3. Discussion
Epididymal cysts occur in 94.9% of boys older than 10 years, and 71.2% of them are older than 14 years [2]. In our case, the patient was 8 years old and presented with features of an acute scrotum. At the time of admission to ward, neither history of previous ultrasound evidence of a right-sided EC was provided by the patient and guardian nor the previous medical records were available with the patient.
Our line of management was towards torsion of testis derived from the acuteness of presentation with swollen and high ridden testis. Even though Doppler sonography showed a perfused right testis, the patient had persistent scrotal pain with few bouts of vomiting. This prompted us to go ahead with scrotal exploration. Torsion of an EC was not considered into the differential diagnosis due to its rarity over a torsion of testicular appendage.
Intraoperative finding of a twisted haemorrhagic cystic lesion arising from the epididymal location of the right testis attached to its upper pole, confirmed the diagnosis of a torsed EC and led us to carry out excision. The twist was 540 degrees, whereas in the literature, it ranged from 360 to 720 degrees [1, 3–5]. In line with majority of the literature, there was no associated prior scrotal trauma.
Particularity of our case was due to being the first case of torsed EC in a child of 1-10 years age group and being torsed for 540 degrees. It is the second case of a right-sided EC and has an acute presentation in previously diagnosed case of an EC. Bleve et al. [3] reported the first case of torsed right sided EC and the remaining seven cases in the literature (Table 1) are left sided lesions.
Erikci et al. [1] also have reported a case of EC torsion in an 11-year-old boy who was put on conservative management for an EC [1]. Presentation with features of acute scrotum such as pain and swelling was similar among all reported cases [1, 3–5]. Management of an EC is usually conservative as 60% of the cases regress on its own more importantly if less than 3 cm in size [2].
4. Learning Points
In conclusion, in line with literature, it is acceptable to perform elective surgery in children for ECs more than 10 mm in size, which are symptomatic, and which are persistent in nature [2].
In cases of ECs opted for conservative management, patients and guardians should be advised on symptoms of acute scrotum and when to seek immediate medical help.
We emphasize the importance of adequate background history taking from the patient as well as the guardian. And it can help to consider a torsed EC as a differential diagnosis in acute scrotum, even though it is rare but important in cases with past history of an EC.
Consent
Informed written consent was obtained from the guardian for publication of this case report and the image. A copy of it is available for review in our unit.
Conflicts of Interest
The authors declare no conflict of interests.
References
- 1.Erikçi V., Hosgör M., Yildiz M., et al. Torsion of an epididymal cyst: a case report and review of the literature. The Turkish Journal of Pediatrics. 2013;55(6):659–661. [PubMed] [Google Scholar]
- 2.Niedzielski J., Miodek M., Krakós M. Epididymal cysts in childhood-conservative or surgical approach? Polski Przeglad Chirurgiczny. 2012;84(8):406–410. doi: 10.2478/v10035-012-0068-2. [DOI] [PubMed] [Google Scholar]
- 3.Bleve C., Conighi M. L., Bucci V., Costa L., Chiarenza S. F. Torsion of huge epididymal cyst in a 16-year-old boy: case report and review of the literature. La Pediatria Medica e Chirurgica. 2018;40:20–22. doi: 10.4081/pmc.2018.162. [DOI] [PubMed] [Google Scholar]
- 4.Messina M., Fusi G., Ferrara F., et al. A rare cause of acute scrotum in a child: torsion of an epididymal cyst. Case report and review of the literature. La Pediatria medica e chirurgica: Medical and surgical pediatrics. 2019;41(1) doi: 10.4081/pmc.2019.210. [DOI] [PubMed] [Google Scholar]
- 5.Ameli M., Boroumand-Noughabi S., Gholami-Mahtaj L. A 14-year-old boy with torsion of the epididymal cyst. Case Reports in Urology. 2015;2015:3. doi: 10.1155/2015/731987.731987 [DOI] [PMC free article] [PubMed] [Google Scholar]