

Abstract
目的
总结并对比分析机器人二尖瓣置换和常规开胸二尖瓣置换相关手术指标和术后的生活质量、伤口满意度及术后恢复时长。
方法
回顾性收集2007年1月~ 2015年12月我院47例接受da Vinci机器人二尖瓣置换术的患者的资料,并以此47例患者作为机器人组。2002年3月~2014年6月正中开胸二尖瓣置换手术患者共286例,依据7个指标从正中开胸患者中抽取47例作为开胸组进行1:1配对。通过收集围术期相关资料,随访患者出院后临床资料,使用生活质量调查量表(SF-12)调查术30 d、半年的生活质量,同时对比两组患者术后恢复工作时间和对手术切口的满意度。
结果
机器人组和开胸组的患者均成功完成二尖瓣置换手术,术中未见患者死亡。机器人组术后并发症仅有1例为胸腔积液。开胸组患者中1例因术后引流过多接受二次开胸止血,1例患者术后死于感染性休克。在手术输血量、术后引流量、术后监护时间、呼吸机时间及术后住院时间上,机器人组均优于正中开胸组,差异有统计学意义(P < 0.05)。两组患者术后并发症的发生率无明显区别。术后30 d生活质量调查(SF-12)显示机器人组有明显的优势,但在半年后两组趋于一致。术后患者对于切口的满意程度,机器人组明显优于开胸组(P < 0.001)。术后半年随访患者工作生活恢复情况,机器人组明显快于开胸组。
结论
机器人二尖瓣置换手术效果可靠,机器人组对比开胸组手术创伤更小,术后恢复更快,对于生活质量及伤口恢复更满意,是可供选择的良好微创手术方式。
Keywords: 微创外科, 机器人, 二尖瓣手术, 生活质量
Abstract
Objective
To compare the mid- and long-term outcomes of patients receiving mitral valve replacement through robotically assisted and conventional median sternotomy approach.
Methods
The data of 47 patients who underwent da Vinci robotic mitral valve replacement in our hospital between January, 2007 and December, 2015 were collected retrospectively (robotic group). From a total of 286 patients undergoing mitral valve replacement through the median thoracotomy approach between March, 2002 and June, 2014, 47 patients were selected as the median sternotomy group for matching with the robotic group at a 1:1 ratio. The perioperative data and follow-up data of the patients were collected, and the quality of life (QOL) of the patients at 30 days and 6 months was evaluated using the Quality of Life Short Form Survey (SF-12). The time of returning to work postoperatively and the patients' satisfaction with the surgical incision were compared between the two groups.
Results
All the patients in both groups completed mitral valve replacement successfully, and no death occurred during the operation. In the robotic group, only one patient experienced postoperative complication (pleural effusion); in median sternotomy group, one patient received a secondary thoracotomy for management of bleeding resulting from excessive postoperative drainage, and one patient died of septic shock after the operation. The volume of postoperative drainage, postoperative monitoring time, ventilation time, and postoperative hospital stay were significantly smaller or shorter in the robotic group than in the thoracotomy group (P < 0.05). There was no significant difference in the incidence of postoperative complications between the two groups. Assessment of the patients at 30 days after the operation showed a better quality of life in the robotic group, but the difference between the two groups tended to diminish at 6 months. The patients in the robotic group reported significantly better satisfaction with the incision than those in the thoracotomy group (P < 0.001). At 6 months after the operation, the patients in the robotic group showed significantly faster recovery of work and daily activities than those in the thoracotomy group.
Conclusion
Robotically assisted mitral valve replacement is safe and reliable. Compared with the median sternotomy approach, the robotic approach is less invasive and promotes faster postoperative recovery of the patients, who have better satisfaction with the quality of life and wound recovery.
Keywords: minimally invasive surgery, robotically assisted surgery, mitral valve surgery, quality of life
随着手术质量的不断提高和并发症率的下降,医生和患者们均不再仅满足于传统的正中开胸手术方式,因此微创外科技术发展迅速,这其中机器人心脏外科技术是目前的热点与长远发展的突破点。由于手术范围扩大和操作灵巧等优点,机器人二尖瓣(MV)修复在全球多个中心被广泛接受,表明机器人手术与传统手术具有相同的安全性和有效性[1-2]。然而,对于严重的MV钙化患者,特别是风湿性心脏病后严重粘连的患者,二尖瓣置换(MVR)是唯一的手术选择[3]。
2017年,我们报告了43例机器人MVR,证明机器人技术的安全有效性,并获得了良好的随访结果[4]。Senay团队[5-6]报道过机器人MVR的个案报道及18例的小样本研究,在2018年,Kuo等[7]也报告了52例机器人MVR的研究,证明该术式的安全和有效性,可能是传统开胸手术的替代方案。这些报告都是单样本的回顾性队列研究,而且结果主要集中在存活率、心脏不良事件的发生率以及手术的安全性和可行性等方面,却缺乏对比性的研究报告,而且没有患者术后的主观结果指标,如患者在机器人辅助的MVR后的满意程度,恢复工作时间和生活质量(QOL)并没有得到评估。
对于患者术后日常生活活动的能力的检测,是作为评估手术成功的一种手段;这些衡量标准评估身体康复、精神康复和重返工作岗位等。Liu等[8]使用简明健康调查表对接受微创二尖瓣置换的患者进行了生活质量对比评估,并得出微创腔镜技术可以在术后第6周改善生活质量的结论。然而,关于机器人腔镜辅助MVR术后生活质量评估的文献有限。因此,我们研究目的是通过比较机器人辅助和传统手术方法,使用对照临床试验来评估术后生活质量,这项工作的结果可能为手术决策提供依据。
1. 资料和方法
1.1. 临床资料
自2007年1月~2015年12月,我院心外科施行47例机器人MVR,其中男26例,女21例,平均年龄47.53±10.80岁。单纯二尖瓣狭窄18例,单纯二尖瓣关闭不全16例,二尖瓣狭窄伴关闭不全13例。单纯关闭不全者中有感染性心内膜炎3例。以该47例完全机器人辅助二尖瓣置换术作为机器人组。2002年3月~ 2014年6月正中开胸二尖瓣置换手术患者共286例,为尽量减少两组间偏差,根据7个指标:术前NYHA纽约心功能等级、病变类型及程度、Euro-ScoreⅡ评分、左室射血分数(LVEF)、年龄(相差≤10岁)、性别和人工瓣膜类型[9]从正中开胸组中抽取47例患者作为单纯正中开胸二尖瓣置换组进行1:1配对,在此过程中采用随机数字表选择。根据以上7项指标进行配对完成后,两组各47例进行回顾性对照研究。
1.2. 术前评估
术前所有两组的患者均经过完整的准备及检查,包括冠脉造影、外周动脉超声、胸部CT、经胸及经食管超声心动图等。所有的患者左心功能均为良好。患者其余术前资料(表 1)。手术排除标准包括肺动脉高压(收缩压>70 mmHg)、重度三尖瓣关闭不全、LVEF低(EF < 30%)、不能耐受单肺通气的严重肺部疾病、右侧胸部手术史、升主动脉钙化、严重的瓣周疾病、二尖瓣瓣环重度钙化等,排除二次手术和伴随除二尖瓣以外需要同期处理的其他心脏疾病。
1.
机器人组和常规开胸组手术患者的一般资料
Baseline characteristics and preoperative echocardiographic data of the patients
| Parameter | Robotically assisted surgery (n=47) | Median sternotomy (n=47) | P |
| BMI: Body mass index; COPD: Chronic obstructive pulmonary disease; LVEF: Left ventricular ejection fraction; MV: Mitral valve; NYHA: New York heart association classification; SD: Standard deviation. | |||
| Age (year) | 47.5±10.8 | 50.5±9.2 | 0.16 |
| Gender (male/female) | 26 (55.3) | 26 (55.3) | 1.00 |
| BMI (kg/m2) | 24.5±3.2 | 24.2±4.4 | - |
| Euro-score Ⅱ (%) | 0.8±0.3 | 0.8±0.4 | 0.44 |
| LVEF (%) | 64.0±7.4 | 61.3±8.7 | 0.14 |
| Cardiac comorbidities [n (%)] | |||
| Heart disease history | 2 (4.26) | 0 (0) | 0.50 |
| Diabetes mellitus | 1 (2.13) | 2 (4.3) | 1.00 |
| Hypertension | 8 (17.0) | 8 (17.0) | 1.00 |
| Hyperlipemia | 2 (4.3) | 1 (2.1) | 1.00 |
| Previous stroke | 3 (6.4) | 2 (4.3) | 0.62 |
| COPD | 0(0) | 0 (0) | NA |
| Atrial fibrillation | 20 (42.6) | 23 (48.9) | 0.84 |
| NYHA class [n (%)] | |||
| Ⅰ | 2 (4.3) | 2 (4.3) | 1.00 |
| Ⅱ | 25 (53.2) | 25 (53.2) | - |
| Ⅲ | 20 (42.6) | 20 (42.6) | - |
| Ⅳ | 0 (0) | 0 (0) | - |
| MV pathologies [n (%)] | |||
| Degenerative (Barlow's) | 6(12.8) | 8 (17.0) | 0.31 |
| Rheumatic | 36 (76.6) | 36 (76.6) | - |
| Infective endocarditis | 2 (4.3) | 2 (4.3) | - |
| Congenital | 3 (6.4) | 1 (2.1) | - |
1.3. 手术方法
1.3.1. 机器人组
机器人二尖瓣手术的麻醉,打孔,阻断和灌注的过程如以前本中心的文献所述[10],待心脏停搏后左房被平行房间隔的切口切开。大多数患者的瓣叶因钙化而导致了僵硬,瓣周结构有时也会同样受累,出现钙化。处理这些僵硬的结构具有一定的挑战性,此时严重钙化的瓣膜组织会被抓持器固定并被切除。术中应予以切除前瓣叶并保留后瓣组织。但瓣膜周围组织钙化严重时应同时也被切除,相连的乳头肌及腱索予以保留,然后使用人工腱索固定到瓣环上。
人工瓣膜的缝合一般需10~12针的双头针带垫片缝合到原瓣环结构上,将人工瓣膜从持瓣器拆下后直接通过工作孔放入胸腔内,并通过小切口垂直固定。缝合方式一般采取两种,第一,所有打结过程均利用打结器通过切口送入结点完成。第二,即使用自动打结器系统(Cor-Knot, LSI Solution, Victor, NY, USA)完成打结过程。该过程可使每个人工假体的置换减少10~15 min,进而缩短心脏缺血时间。
瓣膜置换结束后,先通过心内留置针仔细排气,再采用4-0 Gortex线连续缝合关闭心房。撤离Chitwood血管钳开放升主动脉,缝合穿刺点。常规右心室表面放置起搏导线。辅助平稳后患者从体外心肺转流中撤离出来,鱼精蛋白中和肝素。沿原孔道进入内窥镜并探查心脏表面,仔细止血后放置胸腔引流管。停机后及手术结束前经食道超声心动图检查人工瓣膜工作情况,确认无反流或瓣周漏等并发症后手术结束。术后常规监护治疗及进行随访。
1.3.2. 正中开胸组
全麻后患者予以单腔气管插管。常规正中开胸后打开心包,动静脉插引流管后升主动脉放置停跳液针,体外循环转流后大血管钳阻断升主动脉,顺或逆行灌注HTK心脏停搏液。心脏停跳后切开右房组织,经右房-房间隔入路暴露二尖瓣组织,切除前瓣叶,保留或部分保留后瓣组织,瓣膜置换后测试人工瓣膜开闭情况,确认工作良好并依次缝合房间隔及右房切口并排气,开放升主动脉,心脏复跳。复跳后术中常规经食道心脏超声评估瓣膜工作情况。
1.4. 数据记录及随访
通过检索我院病历管理系统查阅患者病史,(1)术前一般资料:姓名、年龄、性别、身高、体质量、症状、风湿性疾病病史、感染性心内膜炎病史、心功能(NYHA分级)、心律失常、超声心动图数据;(2)术中情况:术中TEE监测手术前后人工瓣膜情况、体外循环(CPB)时间、主动脉阻断时间、围术期血制品输注量;(3)术后结果:ICU停留时间、呼吸机辅助时间、住院时间、术后超声心动图、术后并发症(术后新发房颤、死亡、脑卒中),其中术后新发房颤(POAF)定义为[11]:围术期任何需要治疗的房颤(AF),每次AF≥20 min且24 h的AF累计时间≥60 min。随访方式采用定期门诊复查、电话访谈,问卷调查等系统方式对患者进行随访。
1.5. 术后生活质量评价
生活质量(QOL)量表(SF-12)被用来记录患者术后生活质量,该量表是美国波士顿健康教育研究所研制出的普适性简明生命质量量表SF-36的简化版本,共有12项,评价了健康相关生命质量的8个维度,分别为总体健康(GH)、生理功能(PF)、生理职能(RP)、躯体疼痛(BP)、活力(VT)、社会功能(SF)、情感职能(RE)、心理健康(MH),以上的维度分别计算百分制得分,再依据公式换算为标准分,其中GH、PF、RP及BP经计算可得生理总评分(PCS),SF、RE、MH及VT经计算可得心理总评分(MCS)。本次操作中,依据患者问卷回答情况,输入SF-12官方网站测评,直接计算PCS与MCS评分。
1.6. 术后恢复工作时间和对手术切口的满意度
电话随访对比机器人组和正中开胸组患者术后恢复工作的时间,采用Kaplan-Meier生存分析曲线分析比较两组患者的相应恢复时长。随访两组患者对伤口的恢复的满意程度,分为非常满意,满意,一般,不满意,非常不满意5个维度。
1.7. 统计学方法
全部资料均用SPSS19.0统计学软件进行统计学处理,计数资料统计学描述使用率(%)来表示,两样本率的比较使用χ2检验,组间反应变量有序的计数资料采用单向有序的秩和检验。连续变量数据用均数±标准差表示,两组连续变量的比较采用配对t检验。术后恢复时间上采用乘积基线法(Kaplan-Meier法)进行分析。对于SF-12量表采用美国评分方案对所有调查者的PCS与MCS进行评分,分数位于0~100之间,采用t检验对两组数据比较。Euro-ScoreⅡ评分使用网上的专用公式计算[12]。P < 0.05认为差异具有统计学意义。
2. 结果
2.1. 围术期资料及并发症
机器人组中所有患者均在机器人辅助下成功接受了MVR,其中1例同期行房间隔缺损修补术。所有病人最终都顺利恢复出院。住院期间的术后并发症包括了1例(2.12%)术后右侧胸腔积液,行胸腔闭式引流术后恢复良好。未见术后新发房颤,未见器官功能不全及脑梗、肾衰等并发症。CPB时间是122.02±25.45(78~198)min,主动脉阻断时间85.68±20.70(52~151)min。且CPB时间及阻断时间均随着手术经验的累积明显下降。术中经食道3D实时心脏超声及出院前心脏超声显示,所有患者人工心脏瓣膜功能良好。其余患者随访复查恢复良好,心脏超声未见明显异常。开胸组中有1例因术后引流多二次开胸止血,后恢复顺利出院。1例患者术后出现感染性休克后多器官功能衰竭,死于术后第6天。其余常规开胸组患者均恢复良好出院。两组患者术后并发症未见明显统计学差异,其余各项手术后相关指标(表 2)。
2.
机器人二尖瓣置换围术期的相关指标及并发症
Perioperative data and complications of the patients after mitral valve replacement through robotic and median sternotomy approach (n=47)
| Parameter | Robotically assisted surgery (n=47) | Median sternotomy (n=47) | P |
| AF: Atrial fibrillation; CPB: Cardiopulmonary bypass; *New-onset AF: Any perioperative AF continuing for ≥20 min every time; cumulative time ofAF ≥60 min in 24 hour; anyAF needs to be treated. Data are presented as Mean±SD or number of cases [n (%)]. | |||
| CPB time (min) | 122.02±25.45 | 90.70±26.258 | 0.00 |
| Cross-clamp time (min) | 85.68±20.70 | 63.77±21.248 | 0.00 |
| Drainage volume (ml) | 349.21±152.63 | 514.43±76.65 | 0.00 |
| Ventilation time (h) | 7.49±3.29 | 20.05±19.973 | 0.00 |
| ICU length of stay (h) | 46.68±16.32 | 89.12±32.16 | 0.00 |
| Postsurgical hospital stay (day) | 6.77±2.49 | 13.00±5.320 | 0.00 |
| Mechanical valve / biovalve | 35 (74.5)/12 (25.5) | 33 (70.2)/14 (29.8) | 0.65 |
| Perioperative complications | |||
| 30-Day mortality | 0 (0) | 1 (2.13%) | 1.00 |
| Stroke | 0 (0) | 0 (0) | NA |
| New-onset AF* | 0 (0) | 4(8.51%) | 0.12 |
| Acute Renal Failure | 0 (0) | 1 (2.13%) | 1.00 |
| Postoperative pleural effusion | 1(2.12) | 1 (2.1) | 1.00 |
2.4. 术后生活质量随访结果
2.4.1. 生活质量量表评估
SF-12量表评估患者术后30 d及半年的生活质量,机器人手术组比开胸组生理活动增高,且生理功能及心理功能的评分对比都有统计学差异(P < 0.01,表 3)。
3.
比较机器人组和开胸组手术后30 d和6月SF-12的结果
Results of SF-12 evaluation of the patients at 30 days and 6 months after mitral valve replacement through robotic and median sternotomy approach
| Item | Robotically assisted surgery | Median sternotomy | P |
| PCS: Physical component summary; MCS: Mental component summary. | |||
| SF-12(30d) | n=47 | n=46 | |
| PCS | 54.2±5.1 | 47.3±4.1 | 0.000 |
| MCS | 53.5±3.7 | 48.6±3.4 | 0.000 |
| SF-12 (6 months) | n=42 | n=40 | |
| PCS | 52.3±4.4 | 51.6±2.9 | 0.911 |
| MCS | 54.5±3.5 | 53.6±3.7 | 0.229 |
2.4.2. 切口恢复满意程度
患者对于切口恢复满意程度分成5级,结果显示两组患者对于术后切口恢复满意程度均较高,机器人组患者对于切口恢复程度满意的比例高于开胸组(P < 0.001)。相比正中开胸组,机器人组伤口范围小,美容效果好(表 4,图 1)。
4.
两组患者对手术切口的满意程度
Level of satisfaction of the patients with the surgical incision in the two groups
| Satisfaction degree | Robotically assisted surgery (n=47) | Median sternotomy (n=46) | P < 0.001 |
| Very satisfied | 43 (91.5%) | 2 (4.25%) | - |
| Satisfied | 4 (8.5%) | 33 (72.34%) | - |
| Average | 0 | 6(12.77%) | - |
| Unsatisfied | 0 | 5 (10.64%) | - |
| Very unsatisfied | 0 | 0 | - |
1.
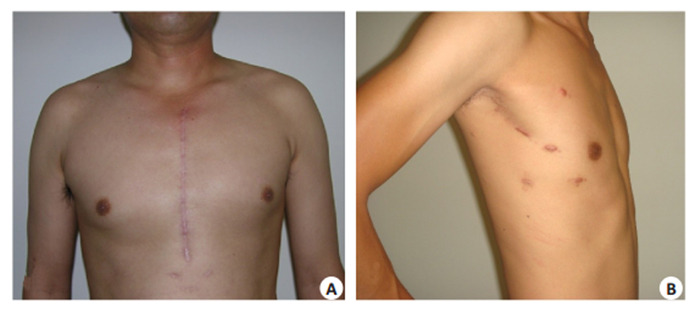
正中开胸组(A)与机器人组(B)患者术后半年伤口对比
Comparison of surgical incision following mitral valve replacement through median sternotomy approach (A) and robotically assisted approach (B) at 6 months.
2.4.3. 术后恢复工作时间
机器人术后恢复工作的平均时间为3.7±0.4周,而开胸组为13.2±1.0周,因此机器人组相比开胸组,术后恢复工作时间明显缩短(P < 0.01,图 2)。
2.
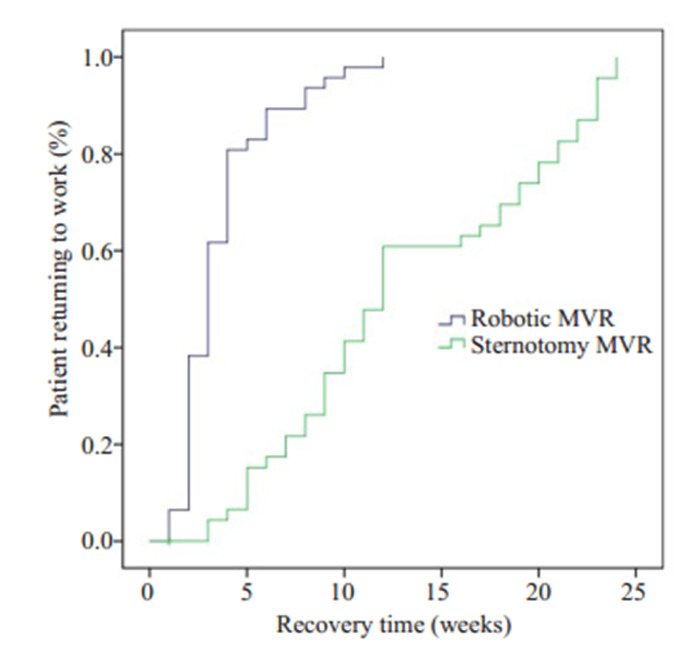
Kaplan-Meier生存分析比较两组患者手术后恢复工作时间
Kaplan-Meier analysis of the time of returning to work after median sternotomy (green line) versus robotic surgery (violet line).
3. 讨论
机器人技术已经在全球心脏手术领域得到广泛应用[13-15]。在国内,我院由高长青教授首次将机器人系统运用于心脏手术,到2015年已完成各类心脏手术累计900余例[16-17],其中包括二尖瓣修复与置换分别110例[18]和47例。对于MVR,目前有三种微创手术方式:胸骨(旁)小切口手术;2D或3D胸腔镜手术;机器人手术。这些微创手术在减少术后疼痛、提高美容效果及缩短恢复时间方面具有优势[19-21]。经历多种类型手术后,我们认为da Vinci机器人系统处理微创心脏手术优势明显:(1)手术视野良好。机器人术中的3D视野系统能够放大10倍,相比2D胸腔镜拥有明显优势。Endo.等[22]报道了3D胸腔镜手术的研究,但仍存在景深不够、放大倍数小的局限。此外Zang等[23]的研究也表明,3D胸腔镜MVR因镜头角度固定而出现手术盲区,不利于止血,而机器人技术可以有效克服该缺点;(2)术中对于MV显露效果最好,从肺静脉左房切口入路对于小左房的患者,通过机器人技术可以更好地呈现心脏各腔室;(3)机器人MVR操作更稳定,机器人手术系统具有动作比例化、手振动消除等优势并高度仿真人的手腕,较传统及腔镜手术更平稳准确。
目前机器人二尖瓣成形术在国内外已经成为多中心的标准术式,Murphy等[24]研究中报道了1257例二尖瓣手术研究,其中MVR有88例,证明了机器人瓣膜手术的安全性和有效性,国外亦有多中心的联合研究及荟萃分析中证实机器人在二尖瓣成形中应用的效果[25-26],本中心的团队也报道过机器人二尖瓣成形的研究进展[18]。而与欧美等发达国家二尖瓣病变以退行性改变为主不同,我国二尖瓣仍以风湿性钙化为主,而这种不适合成形的改变常被作为机器人二尖瓣手术的排除标准[1]。Senay等[3, 5]对于机器人MVR的研究证实了该技术在风湿性二尖瓣钙化后的处理方面也具有安全性和有效性。同样,对比前者的结果,本组病例手术效果佳,术中及术后效果良好。
关于机器人二尖瓣置换手术后效果和并发症,本中心已经有所报道[4],然而随着心脏手术患者所关注的手术有效性和安全性的难题被逐一克服,目前患者对于手术的美观程度、术后恢复工作时间及生活质量越来越重视。随访中我们常能发现患者对于正中开胸后所留下的巨大瘢痕的失望、以及一系列社会心理上的负面影响,尤其在年轻患者及女性患者为甚。对于美观的小切口的迫切需求与微创机器人手术的理念正好符合。机器人心脏手术对于术后切口方面占有着巨大的优势,仅如钥匙孔般大小的数个切口在术后恢复半年内已经基本不可见。正如本次研究中随访结果显示机器人组患者对于手术满意度明显高于开胸组(P < 0.05),机器人组中有91.5%的患者对于手术非常满意。以上结果与Casselman[27]的研究相似,其指出微创心脏手术中约有94%患者表现出满意态度。
机器人瓣膜手术后相关的生活质量研究仍然较少,Suri等[28]使用SF-12量表用以对比评价机器人二尖瓣手术术后的生活质量,并得出结论机器人MVR在生活质量的促进及恢复工作时间上起到了积极作用。SF-12量表对患者的生理及心理情况进行评估,生理评分部分主要包括生理机能、生理职能、躯体疼痛以及一般健康状况,心理评分部分主要包括患者的精力、社会功能、情感职能及精神健康。因为它简单、短小、易于理解及测评时间短等优点[29],并且与SF-36同样具有良好的信度和效度,所以经常被作为评价慢性疾病的良好选择[30]。对患者术后30 d的随访研究过程中可以了解到,机器人组生理功能和心理功能的测评分均明显高于正中开胸组。半年后患者生活质量量表则提示两组患者未见明显差异,考虑患者正常情况下开胸术后约3月胸骨已经完全愈合,此时生活质量受到手术的影响较小,这也从实际上解读了我们结果的可靠性。
总的来说,机器人二尖瓣置换手术可以用于严重二尖瓣病变的患者,手术效果良好,手术并发症少。同时在操作上也更具有优势,是一种优秀的可供选择的微创手术方式。
Biographies
赵海智,博士,医师,E-mail: 95Hz@163.com
张华军,博士,主治医师,E-mail: huajun.zhang@yahoo.co.uk
Funding Statement
国家高技术研究发展计划(863计划)(2012AA021104)
Supported by National High Technology Research and Development Program of China (2012AA021104)
Contributor Information
赵 海智 (Haizhi ZHAO), Email: 95Hz@163.com.
张 华军 (Huajun ZHANG), Email: huajun.zhang@yahoo.co.uk.
王 嵘 (Rong WANG), Email: wangrongd@126.com.
References
- 1.Suri RM, Burkhart HM, Rehfeldt KH, et al. Robotic mitral valve repair for all categories of leaflet prolapse: improving patient appeal and advancing standard of care. Mayo Clin Proc. 2011;86(9):838–44. doi: 10.4065/mcp.2010.0733. [Suri RM, Burkhart HM, Rehfeldt KH, et al. Robotic mitral valve repair for all categories of leaflet prolapse: improving patient appeal and advancing standard of care[J]. Mayo Clin Proc, 2011, 86(9): 838-44.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nifong LW, Chitwood WR, Pappas PS, et al. Robotic mitral valve surgery: a United States multicenter trial. J Thorac Cardiovasc Surg. 2005;129(6):1395–404. doi: 10.1016/j.jtcvs.2004.07.050. [Nifong LW, Chitwood WR, Pappas PS, et al. Robotic mitral valve surgery: a United States multicenter trial[J]. J Thorac Cardiovasc Surg, 2005, 129(6): 1395-404.] [DOI] [PubMed] [Google Scholar]
- 3.Senay S, Gullu AU, Alhan C. Robotic mitral valve replacement for rheumatic mitral disease. Ann Cardiothorac Surg. 2017;6(1):64–6. doi: 10.21037/acs.2016.08.03. [Senay S, Gullu AU, Alhan C. Robotic mitral valve replacement for rheumatic mitral disease[J]. Ann Cardiothorac Surg, 2017, 6(1): 64-6.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.刘 国鹏, 高 长青, 杨 明, et al. 43例机器人二尖瓣置换术后单中心中长期随访结果. http://d.wanfangdata.com.cn/Periodical/jfjyxzz201706014. 解放军医学杂志. 2017;42(6):549–52. [刘国鹏, 高长青, 杨明, 等. 43例机器人二尖瓣置换术后单中心中长期随访结果[J].解放军医学杂志, 2017, 42(6): 549-52.] [Google Scholar]
- 5.Senay S, Gullu AU, Kocyigit M, et al. Robotic mitral valve replacement for severe rheumatic mitral disease: perioperative technique, outcomes, and early results. Innovations (Phila) 2014;9(4):292–6. doi: 10.1097/imi.0000000000000078. [Senay S, Gullu AU, Kocyigit M, et al. Robotic mitral valve replacement for severe rheumatic mitral disease: perioperative technique, outcomes, and early results[J]. Innovations (Phila), 2014, 9(4): 292-6.] [DOI] [PubMed] [Google Scholar]
- 6.Suri RM, Dearani JA, Mihaljevic T, et al. Mitral valve repair using robotic technology: Safe, effective, and durable. J Thorac Cardiovasc Surg. 2016;151(6):1450–4. doi: 10.1016/j.jtcvs.2016.02.030. [Suri RM, Dearani JA, Mihaljevic T, et al. Mitral valve repair using robotic technology: Safe, effective, and durable[J]. J Thorac Cardiovasc Surg, 2016, 151(6): 1450-4.] [DOI] [PubMed] [Google Scholar]
- 7.Kuo CC, Chang HH, Hsing CH, et al. Robotic mitral valve replacements with bioprosthetic valves in 52 patients: experience from a tertiary referral hospital. Eur J Cardiothorac Surg. 2018;54(5):853–9. doi: 10.1093/ejcts/ezy134. [Kuo CC, Chang HH, Hsing CH, et al. Robotic mitral valve replacements with bioprosthetic valves in 52 patients: experience from a tertiary referral hospital[J]. Eur J Cardiothorac Surg, 2018, 54 (5): 853-9.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Liu J, Chen B, Zhang YY, et al. Mitral valve replacement via minimally invasive totally thoracoscopic surgery versus traditional Median sternotomy: a propensity score matched comparative study. Ann Transl Med. 2019;7(14):341. doi: 10.21037/atm.2019.07.07. [Liu J, Chen B, Zhang YY, et al. Mitral valve replacement via minimally invasive totally thoracoscopic surgery versus traditional Median sternotomy: a propensity score matched comparative study [J].Ann Transl Med, 2019, 7(14): 341.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Arif R, Farag M, Zaradzki M, et al. Ischemic colitis after cardiac surgery: can we foresee the threat? PLoS One. 2016;11(12):e0167601. doi: 10.1371/journal.pone.0167601. [Arif R, Farag M, Zaradzki M, et al. Ischemic colitis after cardiac surgery: can we foresee the threat[J]? PLoS One, 2016, 11(12): e0167601.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.杨 明, 高 长青, 王 刚, et al. 机器人微创二尖瓣手术60例临床观察. http://www.j-smu.com/oa/pdfdow.aspx?Sid=2011101721. 南方医科大学学报. 2011;31(10):1721–3. [杨明, 高长青, 王刚, 等.机器人微创二尖瓣手术60例临床观察[J].南方医科大学学报, 2011, 31(10): 1721-3.] [PubMed] [Google Scholar]
- 11.张 凯, 王 联群. 单纯非体外循环冠状动脉旁路移植术后新发房颤术前相关危险因素分析. 天津医药. 2018;46(7):708–11. [张凯, 王联群.单纯非体外循环冠状动脉旁路移植术后新发房颤术前相关危险因素分析[J].天津医药, 2018, 46 (7): 708-11.] [Google Scholar]
- 12.Leahey PA, LaSalvia MT, Rosenthal ES, et al. High morbidity and mortality among patients with sentinel admission for injection drug use-related infective endocarditis. Open Forum Infect Dis. 2019;6(4):ofz089. doi: 10.1093/ofid/ofz089. [Leahey PA, LaSalvia MT, Rosenthal ES, et al. High morbidity and mortality among patients with sentinel admission for injection drug use-related infective endocarditis[J]. Open Forum Infect Dis, 2019, 6 (4): ofz089.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Whellan DJ, McCarey MM, Taylor BS, et al. Trends in roboticassisted coronary artery bypass grafts: a study of the society of thoracic surgeons adult cardiac surgery database, 2006 to 2012. Ann Thorac Surg. 2016;102(1):140–6. doi: 10.1016/j.athoracsur.2015.12.059. [Whellan DJ, McCarey MM, Taylor BS, et al. Trends in roboticassisted coronary artery bypass grafts: a study of the society of thoracic surgeons adult cardiac surgery database, 2006 to 2012[J]. Ann Thorac Surg, 2016, 102(1): 140-6.] [DOI] [PubMed] [Google Scholar]
- 14.Balkhy HH, Lewis CTP, Kitahara H. Robot-assisted aortic valve surgery: State of the art and challenges for the future. Int J Med Robot. 2018;14(4):e1913. doi: 10.1002/rcs.1913. [Balkhy HH, Lewis CTP, Kitahara H. Robot-assisted aortic valve surgery: State of the art and challenges for the future[J]. Int J Med Robot, 2018, 14(4): e1913.] [DOI] [PubMed] [Google Scholar]
- 15.Yang M, Yao MH, Wang G, et al. Comparison of postoperative quality of life for patients who undergo atrial myxoma excision with robotically assisted versus conventional surgery. J Thorac Cardiovasc Surg. 2015;150(1):152–7. doi: 10.1016/j.jtcvs.2015.01.056. [Yang M, Yao MH, Wang G, et al. Comparison of postoperative quality of life for patients who undergo atrial myxoma excision with robotically assisted versus conventional surgery[J]. J Thorac Cardiovasc Surg, 2015, 150(1): 152-7.] [DOI] [PubMed] [Google Scholar]
- 16.杨 明, 高 长青, 刘 帅, et al. 机器人分站式杂交技术治疗冠心病的近期随访. http://www.j-smu.com/oa/pdfdow.aspx?Sid=2015081166. 南方医科大学学报. 2015;35(8):1166–9. [杨明, 高长青, 刘帅, 等.机器人分站式杂交技术治疗冠心病的近期随访[J].南方医科大学学报, 2015, 35(8): 1166-9.] [PubMed] [Google Scholar]
- 17.Yang M, Gao CQ, Wang G, et al. Totally robotic mitral valve surgery in 60 cases. http://link.springer.com/10.1007/978-3-7985-1867-4_13. J South Med Univ. 2011;31(10):1721–3. [Yang M, Gao CQ, Wang G, et al. Totally robotic mitral valve surgery in 60 cases[J]. J South Med Univ, 2011, 31(10): 1721-3.] [PubMed] [Google Scholar]
- 18.Liu GP, Zhang HJ, Yang M, et al. Robotic mitral valve repair: 7-year surgical experience and mid-term follow-up results. http://www.ncbi.nlm.nih.gov/pubmed/30698368. J Cardiovasc Surg (Torino) 2019;60(3):406–12. doi: 10.23736/S0021-9509.19.10602-7. [Liu GP, Zhang HJ, Yang M, et al. Robotic mitral valve repair: 7-year surgical experience and mid-term follow-up results[J]. J Cardiovasc Surg (Torino), 2019, 60(3): 406-12.] [DOI] [PubMed] [Google Scholar]
- 19.Westhofen S, Conradi L, Deuse T, et al. A matched pairs analysis of non-rib-spreading, fully endoscopic, mini-incision technique versus conventional mini-thoracotomy for mitral valve repair. Eur J Cardiothorac Surg. 2016;50(6):1181–7. doi: 10.1093/ejcts/ezw184. [Westhofen S, Conradi L, Deuse T, et al. A matched pairs analysis of non-rib-spreading, fully endoscopic, mini-incision technique versus conventional mini-thoracotomy for mitral valve repair[J]. Eur J Cardiothorac Surg, 2016, 50(6): 1181-7.] [DOI] [PubMed] [Google Scholar]
- 20.Ito T, Maekawa A, Hoshino S, et al. Three-port (one incision plus two-port) endoscopic mitral valve surgery without robotic assistance. Eur J Cardiothorac Surg. 2017;51(5):913–8. doi: 10.1093/ejcts/ezw430. [Ito T, Maekawa A, Hoshino S, et al. Three-port (one incision plus two-port) endoscopic mitral valve surgery without robotic assistance [J]. Eur J Cardiothorac Surg, 2017, 51(5): 913-8.] [DOI] [PubMed] [Google Scholar]
- 21.Gao CQ, Yang M, Xiao CS, et al. Robotically assisted mitral valve replacement. http://www.ncbi.nlm.nih.gov/pubmed/22306218. J Thorac Cardiovasc Surg. 2012;143(4 Suppl):S64–7. doi: 10.1016/j.jtcvs.2012.01.045. [Gao CQ, Yang M, Xiao CS, et al. Robotically assisted mitral valve replacement[J]. J Thorac Cardiovasc Surg, 2012, 143(4 Suppl): S64-7.] [DOI] [PubMed] [Google Scholar]
- 22.Endo Y, Nakamura Y, Kuroda M, et al. The utility of a 3D endoscope and robot-assisted system for MIDCAB. Ann Thorac Cardiovasc Surg. 2019;25(4):200–4. doi: 10.5761/atcs.oa.18-00254. [Endo Y, Nakamura Y, Kuroda M, et al. The utility of a 3D endoscope and robot-assisted system for MIDCAB[J]. Ann Thorac Cardiovasc Surg, 2019, 25(4): 200-4.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zang X, Huang HL, Xie B, et al. A comparative study of threedimensional high-definition and two-dimensional high-definition video systems in totally endoscopic mitral valve replacement. J Thorac Dis. 2019;11(3):788–94. doi: 10.21037/jtd.2019.02.27. [Zang X, Huang HL, Xie B, et al. A comparative study of threedimensional high-definition and two-dimensional high-definition video systems in totally endoscopic mitral valve replacement[J]. J Thorac Dis, 2019, 11(3): 788-94.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Murphy DA, Moss E, Binongo J, et al. The expanding role of endoscopic robotics in mitral valve surgery: 1, 257 consecutive procedures. Ann Thorac Surg. 2015;100(5):1675–81. doi: 10.1016/j.athoracsur.2015.05.068. [Murphy DA, Moss E, Binongo J, et al. The expanding role of endoscopic robotics in mitral valve surgery: 1, 257 consecutive procedures[J]. Ann Thorac Surg, 2015, 100(5): 1675-81; discussion 1681-2.] [DOI] [PubMed] [Google Scholar]
- 25.Seco M, Cao C, Modi P, et al. Systematic review of robotic minimally invasive mitral valve surgery. Ann Cardiothorac Surg. 2013;2(6):704–16. doi: 10.3978/j.issn.2225-319X.2013.10.18. [Seco M, Cao C, Modi P, et al. Systematic review of robotic minimally invasive mitral valve surgery[J]. Ann Cardiothorac Surg, 2013, 2(6): 704-16.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cao C, Wolfenden H, Liou K, et al. A meta-analysis of robotic vs. conventional mitral valve surgery. http://www.ncbi.nlm.nih.gov/pubmed/26309839. Ann Cardiothorac Surg. 2015;4(4):305–14. doi: 10.3978/j.issn.2225-319X.2014.10.05. [Cao C, Wolfenden H, Liou K, et al. A meta-analysis of robotic vs. conventional mitral valve surgery[J]. Ann Cardiothorac Surg, 2015, 4(4): 305-14.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Casselman FP, van Slycke S, Wellens F, et al. Mitral valve surgery can now routinely be performed endoscopically. http://europepmc.org/abstract/MED/12970208. Circulation. 2003;108(Suppl 1):Ⅱ48–Ⅱ54. doi: 10.1161/01.cir.0000087391.49121.ce. [Casselman FP, van Slycke S, Wellens F, et al. Mitral valve surgery can now routinely be performed endoscopically[J]. Circulation, 2003, 108(Suppl 1): Ⅱ48-Ⅱ54.] [DOI] [PubMed] [Google Scholar]
- 28.Suri RM, Antiel RM, Burkhart HM, et al. Quality of life after early mitral valve repair using conventional and robotic approaches. Ann Thorac Surg. 2012;93(3):761–9. doi: 10.1016/j.athoracsur.2011.11.062. [Suri RM, Antiel RM, Burkhart HM, et al. Quality of life after early mitral valve repair using conventional and robotic approaches[J]. Ann Thorac Surg, 2012, 93(3): 761-9.] [DOI] [PubMed] [Google Scholar]
- 29.Sampogna F, Fania L, Mastroeni S, et al. Age-specific physical and mental health status in Italian patients with hidradenitis suppurativa: a comparison with the general population. Arch Dermatol Res. 2020 doi: 10.1007/s00403-020-02063-4. [Sampogna F, Fania L, Mastroeni S, et al. Age-specific physical and mental health status in Italian patients with hidradenitis suppurativa: a comparison with the general population[J]. Arch Dermatol Res, 2020:DOI:10.1007/s00403-020-02063-4.] [DOI] [PubMed] [Google Scholar]
- 30.Kontodimopoulos N, Pappa E, Niakas D, et al. Validity of SF-12 summary scores in a Greek general population. Health Qual Life Outcomes. 2007;5:55. doi: 10.1186/1477-7525-5-55. [Kontodimopoulos N, Pappa E, Niakas D, et al. Validity of SF-12 summary scores in a Greek general population[J]. Health Qual Life Outcomes, 2007, 5: 55.] [DOI] [PMC free article] [PubMed] [Google Scholar]