

Abstract
Objective
To examine the availability and facility‐level predictors of LGBT‐specific mental health and substance abuse treatment in the United States.
Data Sources/Study Setting
2016 National Survey of Substance Abuse Treatment Services, 2016 National Mental Health Service Survey, and 2015‐2016 Gallup Daily tracking survey.
Study Design
Logistic regression models and average marginal effects were used to identify characteristics of facilities that offer LGBT‐specific programs. Linear regression models were used to estimate the association between the state‐level proportion of LGBT people and the proportion of facilities that offer LGBT‐specific programs.
Data Collection/Extraction Methods
Secondary data analysis. Cases with missing values for any predictor were excluded.
Principle Findings
12.6 percent of mental health and 17.6 percent of substance abuse facilities reported LGBT‐specific programs. Several facility characteristics were statistically associated with the likelihood of mental health and substance abuse facilities providing LGBT‐specific programs, including offering outpatient or residential treatment, private ownership, religious affiliation, and payment type. The proportion of LGBT adults living within each state was statistically associated with state‐level density of LGBT‐specific mental health programs, but not substance abuse programs.
Conclusions
Findings suggest limited availability of culturally competent mental health and substance abuse treatment, despite well‐documented need.
Keywords: mental health, sexual and gender minorities, substance abuse, treatment
What this study adds
Few state‐approved substance abuse and mental health facilities reported offering programs specifically for LGBT clients.
The likelihood of offering LGBT‐specific services varied by several contextual factors including private ownership, religious affiliation, and payment type.
The proportion of LGBT residents in a state was positively related to the proportion of mental health facilities in that state offering LGBT‐specific programs; this association was not present for substance abuse facilities.
1. INTRODUCTION
In the United States (US), nearly 47 million people meet the criteria for a mental, behavioral, or emotional disorder 1 and approximately 20 million people meet the criteria for a substance use disorder (SUD) in a given year. 1 , 2 Lesbian, gay, bisexual, and transgender (LGBT) people are populations at elevated risk for mental health disorders, substance abuse, and psychiatric comorbidity relative to their heterosexual and cisgender peers. 3 , 4 , 5 , 6 , 7 , 8 Sexual minority adults, for example, have between 1.6 and 3.1 times the odds of lifetime SUD compared to their heterosexual counterparts, 9 and LGBT adults are more likely to meet the criteria for major depression, anxiety, and to report suicidal ideation and attempt. 10 , 11 , 12 , 13 , 14
Minority stress theory helps to explain these disparities; 15 , 16 , 17 , 18 , 19 it identifies stigma and discrimination as key mechanisms of sexual orientation‐related health inequities. For example, evidence suggests that LGBT people in substance abuse treatment present with more complex needs, including higher mental health comorbidity, greater severity, and poorer physical health due to minority stress. 3 , 20 , 21 , 22 Additionally, this same stigma and discrimination prevent LGBT people from accessing and engaging with quality mental health care services attuned to their unique experiences and needs. In many ways, the lack of adequate mental health care compounds and maintains population‐level mental health inequities for this population. Conversely, mental health care services that are sensitive to the needs of LGBT clientele show promising reductions in mental health symptomology and substance use; 23 , 24 , 25 , 26 however, the availability of LGBT‐sensitive services is largely unknown. As such, the current study seeks to assess the degree to which LGBT‐specific services are available using two national samples of state‐approved mental health and substance abuse facilities in the United States, and the characteristics of facilities that offer LGBT‐specific services.
1.1. LGBT people and barriers to culturally competent care
Structural barriers prevent many people from engaging in mental health and substance use (MH/SU) treatment. These include cost, insurance coverage, stigma around MH/SU disorders, and availability of services. 27 , 28 From 2011 to 2013, approximately 86 percent of people with an SUD in the past year did not receive care, 2 and in 2017, only 43 percent of US adults with a mental illness received mental health services in the past year. 1 Although LGBT people are more likely to seek out treatment than their heterosexual peers, 3 , 9 , 29 , 30 they face a number of unique barriers in accessing quality treatment: Many service providers hold negative attitudes toward LGBT people or lack adequate knowledge about their unique mental health needs. 31 , 32 , 33 , 34 Further, heteronormative treatment practices that ignore the unique experiences of LGBT people (eg, assumptions about the sex/gender of partners, misgendering clients) may be perceived as exclusionary and discriminatory by LGBT clients. 32 , 35 , 36 , 37
Research consistently demonstrates that behavioral and mental health practitioners lack competence and comfort when working with LGBT clients which further alienates LGBT people when seeking care. 35 , 38 , 39 , 40 LGBT clients who experience nonaffirming behaviors from providers (eg, blaming the presenting problem[s] on LGBT identity, lacking basic knowledge of LGBT issues, prejudice against LGBT persons) are less satisfied with treatment and less likely to return after their first session. 33 , 41 Perhaps, not surprisingly, LGBT individuals often seek out health care providers that have a stated affirmative practice, even when the presenting problem is not related to their sexual orientation or gender identity. 42 Given these experiences and the unique barriers and needs of LGBT individuals seeking MH/SU treatment, researchers and informed practitioners have advocated for the cultivation of culturally competent treatment to address the MH/SU disparities evidenced by LGBT populations.
1.2. The importance and availability of LGBT‐specific treatment models
As health services research continues to document disparities in health outcomes and access to services, culturally competent care has emerged as one solution. The US Department of Health and Human Services defines culturally competent programs as those that “maintain a set of attitudes, perspectives, behaviors, and policies – both individually and organizationally – that promote positive and effective interactions with diverse cultures”. 43 Researchers have studied the impact of providing culturally competent health services, linking levels of provider cultural competence with increased client satisfaction and improved care access and utilization. 44 , 45 Indeed, mental and behavioral health practitioners recognize the importance of cultural competence, with many professional organizations setting expectations for cultural competence in their codes of ethics and training program accreditation guidelines. 46 , 47 , 48
Scholars have long called for LGBT‐specific treatment as a means of providing culturally competent care. 49 Several studies now show promising results for LGBT‐specific treatment modalities. A study of men in New York found that both heterosexual and gay/bisexual men had better treatment outcomes in LGBT‐specific substance abuse programs than gay/bisexual men in “traditional” (ie, non LGBT‐specific) programs. 23 In another study that investigated perceptions of treatment, LGB people who had recently participated in a traditional substance abuse program reported lower levels of satisfaction with treatment than their heterosexual counterparts; the majority perceived their sexual orientation as having a negative effect on their time in treatment. 24 Gay and bisexual men, as compared to heterosexual men, were less likely to have completed the traditional program and were more likely to have cited terminating treatment prematurely due to unmet needs. 24 There are similar findings regarding mental health treatment: LGB adults are often less satisfied with services than their heterosexual counterparts. 25 Importantly, LGB‐specific treatment strategies appear to be more efficacious for sexual minorities. Pachankis and colleagues 26 found preliminary support for the use of a cognitive‐behavioral treatment adapted to address sexual orientation‐related minority stress in young gay and bisexual men. Compared to waitlist clients, those receiving the adapted treatment experienced statistical reductions in depressive symptoms and alcohol use problems. Despite promising research on the efficacy of LGBT‐specific services, the availability of these services is largely unknown.
The only known large‐scale study on the availability of specialized LGBT services used the National Survey of Substance Abuse Treatment Services (N‐SSATS) to explore whether facilities with specialized programming provided the corresponding key services as defined by the Substance Abuse and Mental Health Services Administration (SAMHSA). 50 Researchers found that facilities with LGBT‐specific programs were more likely than those without to provide key services including HIV testing, STD testing, hepatitis testing, and HIV education, counseling, and support. 51 These findings suggest that organizations with LGBT‐specific programming may be better attuned to the unique needs of LGBT clients.
1.3. The current study
Given the disproportionate mental and behavioral health burden among LGBT populations, 3 , 4 , 5 , 6 , 7 , 8 and the promising solutions offered by LGBT‐specific services, 23 , 24 , 25 , 26 the current study seeks to address three aims about the availability of LGBT‐specific services using two national samples of state‐approved mental health and substance abuse service organizations. First, we assess how many mental health and substance abuse facilities offer LGBT‐specific programs. Second, we are interested in assessing the characteristics (eg, treatment type, ownership and funding, capacity, and payment types) of mental health and substance abuse facilities that offer LGBT‐specific programs (as compared to those who do not). Specifically, we examine the type of treatment offered (ie, inpatient, outpatient, and residential), as the clients utilizing these treatment types vary in the frequency and duration of their use of the facility. 52 , 53 Additionally, hospital affiliation, 54 religious affiliation, 55 ownership type, 56 and receipt of government funds 56 may affect a facility's population‐specific program offerings. These factors reflect differences in the bureaucracies and structures of mental health substance abuse treatment facilities that dictate how they operate and their ability to adapt program components to client needs. The ways that facilities allow their clients to pay (Medicaid, Medicare, sliding fee scale, free services) may also reflect the resources available to the facility and the types of clients they typically serve. 57 , 58 Finally, we test the association between state‐specific density of LGBT people and the number of facilities that offer LGBT‐specific mental health and substance abuse programs in each state. Findings offer structural‐level context for the availability of LGBT culturally competent programs as one approach to eliminating mental and behavioral health disparities.
2. METHODS
2.1. Data sources and samples
Three sources of data were used in the current study. Information about treatment facilities comes from the 2016 N‐SSATS and the 2016 National Mental Health Services Survey (N‐MHSS). State‐level LGBT population density data come from the Gallup Daily Tracking Survey.
The N‐SSATS and N‐MHSS are directed by SAMHSA’s Center for Behavioral Health Statistics and Quality. Both surveys are designed to collect information on the location, characteristics, and use of outpatient, residential, and hospital inpatient programs throughout the United States. All facilities surveyed are licensed by their respective states as specialty mental health and/or substance abuse clinics or centers. The N‐SSATS and N‐MHSS do not include Department of Defense military treatment facilities, individual private practitioners, small group practices not licensed as a mental health clinic or center, or jails and prisons. 59 , 60 Survey responses are collected via web‐based questionnaire, paper questionnaire by mail, and telephone interview. As part of the survey, facilities were asked whether they offered programs for specific populations, including those who identify as LGBT. Facilities also offered information about their operations and service provision. The surveys provide prevalence information for a given day as opposed to annual totals. Both the N‐SSATS and N‐MHSS reported an item response rate of approximately 98 percent. 59 , 60 For analysis of the N‐SSATS, we excluded facilities missing on facility characteristic items (n = 1355 or 9.4 percent of 14 399 facilities)—there were no missing values for the item assessing whether or not facilities offered LGBT‐specific services. This resulted in a final analytic sample of 13 044 facilities. For the N‐MHSS, we used the same exclusion criteria, which removed 896 facilities, leaving an analytic sample of 11 269 facilities.
Gallup LGBT population estimates are based on the Gallup Daily Tracking Survey. Gallup conducts daily phone interviews of 1000 US adults aged 18 and older living in all 50 states and the District of Columbia, 350 days a year. Participants are contacted using random‐digit‐dial methods for landline and cellphone numbers. Landline respondents are chosen at random within each household based on members’ next upcoming birthday. Daily samples are evenly split between cellphone and landline respondents. Gallup also implements minimum quotas across time zones within each region to prevent, for example, disproportionate inclusion of individuals in the Central Time Zone in the Southern US region. The data used in this analysis were collected between January 1, 2015, and December 30, 2016 (N = 710 252).
2.2. Measures
2.2.1. Dependent variables
To gauge whether N‐MHSS and N‐SSATS facilities were offering LGBT‐specific programs, facilities were asked “Does this facility offer a mental health treatment program or group that is dedicated or designed exclusively for clients in any of the following categories?” of which “Lesbian, gay, bisexual, transgender (LGBT) clients” was one category. Respondents were instructed “If this facility treats clients in any of these categories, but does not have a specifically tailored program or group for them, DO NOT mark the box for that category.”
State‐level densities of MH/SU facilities were calculated by generating the proportion of each state's total number of facilities that reported offering LGBT‐specific programs. State‐level density of LGBT people was captured by the Gallup Daily Tracking Survey, which asked participants “Do you personally identify as lesbian, gay, bisexual, or transgender?” Gallup reports the proportion of individuals surveyed in each state that responded in the affirmative. These estimates have been used in previous studies 61 , 62 , 63 and may be higher than other population‐based surveys (eg, National Health Interview Survey, General Social Survey) for two reasons. First, the Gallup survey is administered over the phone, while similar surveys are conducted as in‐home interviews. The relative anonymity of data collection over the phone may increase a respondent's willingness to identify as LGBT. Second, Gallup is unique in that rather than asking respondents to enumerate their identity (Are you heterosexual, homosexual, bisexual, etc?), they ask “Do you personally identify as lesbian, gay, bisexual, or transgender?”, allowing respondents to identify as a member of the LGBT community without the level of specificity required in other surveys. 64
2.2.2. Independent variables
For the N‐SSATS, we were interested in assessing several facility characteristics in relation to offering LGBT‐specific programs, including facility type (ie, inpatient, outpatient, residential, and hospital affiliation), receipt of government grants, and payment options (ie, sliding fee, free services, Medicare, and Medicaid). Response options for each of these questions were yes or no. We were also interested in whether these facilities varied in ownership, which was assessed with the question “Is this facility operated by (mark only one).” Response options included private for‐profit organization, private nonprofit organization, state government, local, county or community government, tribal government, and federal government. We assessed similar facility characteristics in the N‐MHSS: facility type (ie, inpatient, outpatient, residential, and religious), and payment options (ie, sliding fee, free, Medicare, and Medicaid), with a yes or no response. Respondents were asked whether the facility was private for‐profit, private nonprofit, or public.
2.3. Analytic approach
Stata 15.1 65 was used for data management and analysis. First, we used chi‐square test of independence to examine the bivariate association between each facility characteristic and LGBT‐specific program offerings. Next, logistic regression models were fit to assess which characteristics were most strongly associated with LGBT‐specific service offerings. Finally, linear regression was used to test the association between the state‐level proportions of LGBT people and facilities offering LGBT‐specific programs.
3. RESULTS
Just under 18 percent of state‐approved substance abuse facilities and 12.6 percent of state‐approved mental health facilities reported offering programs specifically for LGBT clients.
3.1. Facility characteristics associated with LGBT‐specific programs
Several characteristics were statistically associated with offering LGBT‐specific programs among mental health and substance abuse facilities (Table 1). In mental health facilities, those offering inpatient services (10.69 percent) were less likely to offer LGBT‐specific services than those that did not offer inpatient services (12.35 percent). Facilities offering outpatient treatment (12.70 percent) and residential care (13.60 percent) were more likely to offer LGBT‐specific programs compared to those not offering these types of care (10.21 and 11.77 percent, respectively). Facilities that were not religiously affiliated (12.28 percent) were more likely to offer LGBT‐specific programs than those with some religious affiliation (9.28 percent). LGBT program offerings also varied by ownership, with public facilities being least likely (9.93 percent) to offer these programs compared to private nonprofit (11.84 percent) and private for‐profit (14.84 percent). Facilities that accepted payment types often indicative of serving lower socioeconomic status clients (sliding fee scale, free treatment, Medicare, or Medicaid) did not differ in offering LGBT‐specific programs from facilities that did not offer these payment and insurance options.
TABLE 1.
Bivariate associations between facility characteristics and LGBT services
| Mental health facilities (n = 11 269) | Substance abuse facilities (n = 13 044) | |||||||
|---|---|---|---|---|---|---|---|---|
| LGBT services | No LGBT services | χ2(df) | P | LGBT services | No LGBT services | χ2(df) | P | |
| % | % | % | % | |||||
| Treatment type | ||||||||
| Inpatient | ||||||||
| Yes | 10.69 | 89.31 | 4.05 (1) | .044 | 16.19 | 83.81 | 0.93 (1) | .334 |
| No | 12.35 | 87.65 | 17.70 | 82.30 | ||||
| Outpatient | ||||||||
| Yes | 12.70 | 87.30 | 12.38 (1) | <.001 | 17.36 | 82.64 | 2.88 (1) | .090 |
| No | 10.21 | 89.79 | 18.85 | 81.15 | ||||
| Residential | ||||||||
| Yes | 13.60 | 86.40 | 4.98 (1) | .026 | 21.24 | 78.76 | 37.14 (1) | <.001 |
| No | 11.77 | 88.23 | 16.84 | 83.52 | ||||
| Religious affiliation | ||||||||
| Yes | 9.28 | 90.72 | 5.94 (1) | .015 | ||||
| No | 12.28 | 87.72 | ||||||
| Ownership type | ||||||||
| Private for‐profit | 14.84 | 85.16 | 22.90 (2) | <.001 | 21.79 | 78.21 | 100.43 (5) | <.001 |
| Private nonprofit | 11.84 | 88.16 | 15.86 | 84.14 | ||||
| Public | 9.93 | 90.07 | ||||||
| State government | 15.25 | 84.75 | ||||||
| Local or county government | 10.02 | 89.98 | ||||||
| Tribal government | 16.31 | 83.69 | ||||||
| Federal government | 13.50 | 86.50 | ||||||
| Hospital affiliation | ||||||||
| Yes | 11.95 | 88.05 | 28.79 (1) | <.001 | ||||
| No | 18.19 | 81.81 | ||||||
| Government funds | ||||||||
| Yes | 15.88 | 84.12 | 32.79 (1) | <.001 | ||||
| No | 19.72 | 80.28 | ||||||
| Payment types | ||||||||
| Sliding fee scale | ||||||||
| Yes | 12.34 | 87.66 | 0.94 (1) | .333 | 18.40 | 81.60 | 8.00 (1) | .005 |
| No | 11.74 | 88.26 | 16.48 | 83.52 | ||||
| Free treatment | ||||||||
| Yes | 12.05 | 87.95 | 0.01 (1) | .932 | 18.53 | 81.47 | 6.26 (1) | .012 |
| No | 12.11 | 87.89 | 16.85 | 83.15 | ||||
| Medicare | ||||||||
| Yes | 11.76 | 88.24 | 2.57 (1) | .109 | 17.19 | 82.81 | 0.89 (1) | .346 |
| No | 12.85 | 87.15 | 17.85 | 82.15 | ||||
| Medicaid | ||||||||
| Yes | 11.89 | 88.11 | 3.79 (1) | .052 | 16.80 | 83.20 | 10.17 (1) | .001 |
| No | 14.03 | 85.97 | 19.00 | 81.00 | ||||
Blank spaces in the table reflect the absence of those variables in the dataset and exclusion from analysis.
Among substance abuse facilities, those offering residential care (21.24 percent) were significantly more likely to offer LGBT‐specific programs than facilities that did not offer residential treatment (16.84 percent). Facilities located in hospitals (11.95 percent) were less likely than those outside of hospital locations (18.19 percent) to offer LGBT‐specific programs. Again, offering LGBT‐specific programs varied significantly by ownership type, with private for‐profit facilities most likely (21.79 percent) and local or county government facilities least likely (10.02 percent) to offer LGBT‐specific programs. Facilities receiving government funds were less likely to offer LGBT‐specific programs (15.88 percent) than those who reported no government funding (19.72 percent). Facilities that provided a sliding fee scale (18.40 percent) or free treatment (18.53 percent) were more likely to report LGBT‐specific programs than those that did not offer these payment options (16.48 and 16.85 percent, respectively). Facilities accepting Medicaid (16.80 percent) were significantly less likely to offer LGBT‐specific programming than those facilities that did not (19.00 percent); Medicare acceptance was not associated with offering LGBT‐specific programs. Providing outpatient care or inpatient care was not associated with having LGBT‐specific programs.
3.2. Multivariate analyses
Predicted probabilities and average marginal effects from multivariate logistic regression models assessing the degree to which facility characteristics were associated with the presence of LGBT‐specific services are presented in Table 2. Among mental health care facilities, LGBT‐specific services were more prevalent among facilities providing residential (marginal effect [ME] =5.61 percent; 95% CI, 3.10 to 8.11 percent) and outpatient services (ME = 5.03 percent; 95% CI, 3.40 to 6.66 percent) than those facilities that did not offer these services. Compared to private for‐profit facilities, a significantly smaller proportion of private nonprofit (ME = −3.18 percent; 95% CI, −5.00 to −1.37 percent) and public facilities (ME = −5.36 percent; 95% CI, −7.53 to −3.19 percent) offered LGBT‐specific services. Facilities that were affiliated with a religious organization were less likely to offer LGBT‐specific programs when compared to those with no religious affiliation (ME = −2.66 percent; 95% CI, −4.92 to −0.41 percent). The prevalence of LGBT‐specific mental health services did not significantly vary by whether a facility offered inpatient treatment or by payment type (ie, acceptance of Medicare or Medicaid, offering services on a sliding fee scale or at no‐cost).
TABLE 2.
Predicted probabilities and average marginal effects (AME) of facility characteristics on offering LGBT services
| Mental health facilities (n = 11 269) | Substance abuse facilities (n = 13 044) | ||||||
|---|---|---|---|---|---|---|---|
| Probability | AME | 95% CI | Probability | AME | 95% CI | ||
| Treatment type | Treatment type | ||||||
| Inpatient | Inpatient | ||||||
| No | 11.92% | No | 17.51% | ||||
| Yes | 13.05% | 1.12% | −0.97%, 3.22% | Yes | 20.40% | 2.89% | −1.40%, 7.18% |
| Outpatient | Outpatient | ||||||
| No | 8.51% | No | 15.44% | ||||
| Yes | 13.55% | 5.03%* | 3.40%, 6.66% | Yes | 18.19% | 2.75%* | 0.57%, 4.94% |
| Residential | Residential | ||||||
| No | 11.30% | No | 15.66% | ||||
| Yes | 16.90% | 5.61%* | 3.10%, 8.11% | Yes | 24.93% | 9.27%* | 6.79%, 11.76% |
| Religious affiliation | |||||||
| No | 12.25% | ||||||
| Yes | 9.59% | −2.66%* | −4.92%, −0.41% | ||||
| Ownership type | Ownership type | ||||||
| Private for‐profit | 15.05% | Private for‐profit | 23.10% | ||||
| Private nonprofit | 11.86% | −3.18%* | −5.00%, −1.37% | Private nonprofit | 15.12% | −7.98%* | −9.93%, −6.03% |
| Public | 9.69% | −5.36%* | −7.53%, −3.19% | State government | 14.49% | −8.61%* | −12.98%, −4.23% |
| Local or county government | 10.06% | −13.04%* | −15.96%, −10.11% | ||||
| Tribal government | 17.24% | −5.86%* | −11.16%, −0.55% | ||||
| Federal government | 16.74% | −6.36%* | −12.11%, −0.61% | ||||
| Hospital affiliation | |||||||
| No | 18.12% | ||||||
| Yes | 12.43% | −5.69%* | −8.29%, −3.09% | ||||
| Government funds | |||||||
| No | 19.21% | ||||||
| Yes | 16.25% | −2.96%* | −4.72%, −1.20% | ||||
| Payment types | Payment types | ||||||
| Sliding fee scale | Sliding fee scale | ||||||
| No | 11.61% | No | 15.58% | ||||
| Yes | 12.44% | 0.82% | −0.55%, 2.20% | Yes | 19.11% | 3.53%* | 2.10%, 4.97% |
| Free treatment | Free treatment | ||||||
| No | 11.71% | No | 15.76% | ||||
| Yes | 12.42% | 0.70% | −0.58%, 1.98% | Yes | 20.08% | 4.32%* | 2.81%, 5.83% |
| Medicare | Medicare | ||||||
| No | 12.38% | No | 16.82% | ||||
| Yes | 11.95% | −0.43% | −1.91%, 1.04% | Yes | 19.44% | 2.62%* | 0.98%, 4.27% |
| Medicaid | Medicaid | ||||||
| No | 13.63% | No | 17.93% | ||||
| Yes | 11.93% | −1.70% | −4.04%, 0.64% | Yes | 17.43% | −0.50% | −2.09%, 1.10% |
Blank spaces in the table reflect the absence of those variables in the dataset and exclusion from analysis.
AME = average marginal effect (difference in predicted probabilities) 95% CI = 95% confidence interval
AME significant at P < .05, **AME significant at P < .01,***AME significant at P < .001.
Among substance abuse treatment facilities, results revealed several characteristics associated with LGBT‐specific programs. Facilities providing residential (ME = 9.27 percent; 95% CI, 6.79 to 11.76 percent) and outpatient services (ME = 2.75 percent; 95% CI, 0.57 to 4.94 percent) were more likely to offer LGBT‐specific programs than facilities that did not offer these services. Private nonprofit (ME = −7.98 percent; 95% CI, −9.93 to −6.03 percent) and all types of publicly funded facilities (ME from −13.04 to −5.86 percent) were less likely than private for‐profit facilities to offer LGBT‐specific programs. Facilities that were affiliated with a hospital were less likely to offer LGBT‐specific programs when compared to those without a hospital affiliation (ME = −5.69 percent; 95% CI, −8.29 to −3.09 percent) and facilities receiving government funding were less likely than facilities that did not receive government dollars to offer these programs (ME = −2.96 percent; 95% CI, −4.72 to −1.20 percent). Facilities that provide a sliding fee scale (ME = 3.53 percent; 95% CI, 2.10 to 4.97 percent) or free services (ME = 4.32 percent; 95% CI, 2.81 to 5.83 percent) were more likely to offer LGBT‐specific programs compared to those that did not offer these payment options. Further, 19.44 percent of facilities that accepted Medicare offered LGBT‐specific programs compared to 16.82 percent of facilities that did not accept Medicare (ME = 2.62 percent; 95% CI, 0.98 to 4.27 percent). Acceptance of Medicaid did not predict LGBT‐specific programs.
3.3. Associations between state‐level LGBT population density and LGBT‐specific program density
Fifty states were included in the regression analysis testing the association between LGBT population and LGBT program density. The District of Columbia was identified as a multivariate outlier for both the proportion of LGBT individuals and the proportion of facilities offering specialized programs using the DFBETA function in Stata. Results from our linear regression model (see Figure 1) demonstrate a significant relationship between the proportion of LGBT people within a given state and the proportion of facilities in that same state that offer LGBT‐specific mental health programs (b = 3.38, P < .001). There was not a statistical association between LGBT population density and the proportion of substance abuse facilities that offered LGBT‐specific programs (b = 2.03, P = .11).
FIGURE 1.
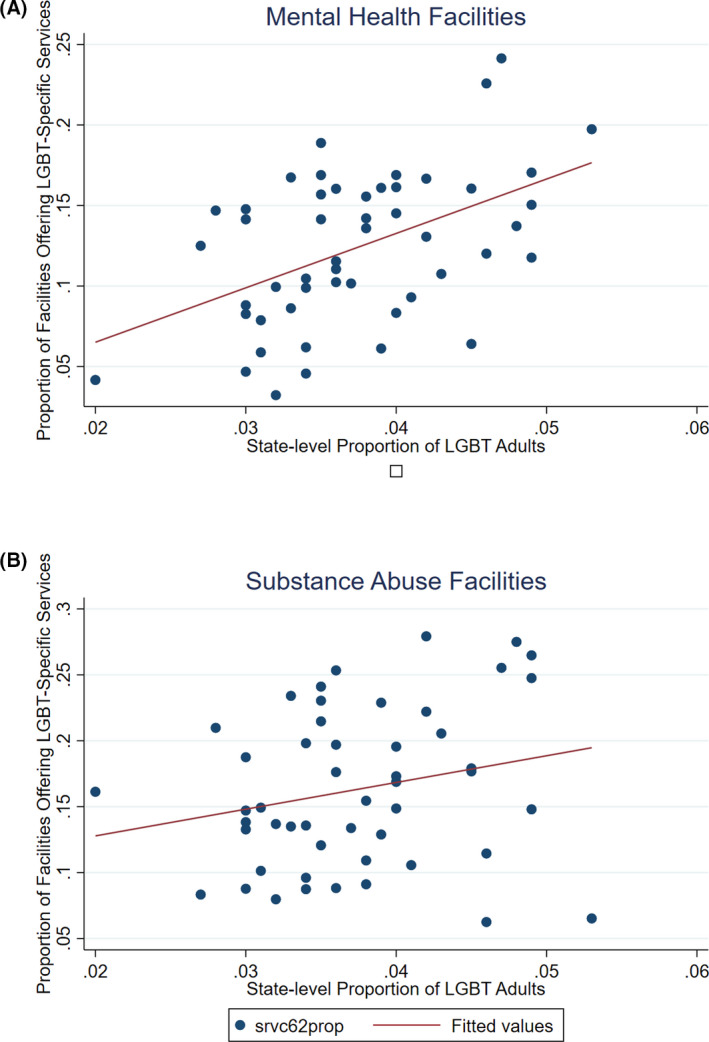
Association between state‐level LGBT population density and LGBT‐specific programs Note: Mental health facilities (b = 3.38, P < .001); substance abuse facilities (b = 2.03, P = .11)[Color figure can be viewed at wileyonlinelibrary.com]
4. DISCUSSION
The current study sought to document the prevalence of LGBT‐specific programs, examine the characteristics of facilities that offer LGBT‐specific programs, and test the association between LGBT population and program density across the United States. Generally, findings suggest a lack of LGBT‐specific programs in state‐approved mental health and substance abuse treatment facilities. Fewer than one in five substance abuse facilities and one in eight mental health facilities reported LGBT‐specific programs, suggesting that many facilities may not be equipped to meet the unique needs of LGBT clients. Given well‐documented sexual orientation and gender identity disparities in mental health and substance use disorders, 3 , 4 , 5 , 6 , 7 , 13 , 17 coupled with research highlighting the efficaciousness of LGBT‐specific services, 23 , 24 , 25 , 26 the lack of LGBT‐specific service availability is concerning. Culturally competent treatment services are important for improving the disparities experienced by LGBT individuals. The findings presented here extend current LGBT mental health and substance abuse treatment research by offering a more macrosystemic investigation into the availability of culturally competent, LGBT‐specific treatment options in the United States. Findings urge policymakers and practitioners to consider the unmet treatment needs of this population, and solutions to address them.
Our results also suggest that facilities that offer LGBT‐specific programs systematically differ in important ways from facilities that do not offer these programs. For example, 15 percent of private for‐profit mental health facilities and 23 percent of private for‐profit substance abuse facilities offered LGBT‐specific services relative to 10‐12 percent of private nonprofit and 10‐17 percent of public mental health and substance abuse facilities. These findings suggest that there may be a degree of flexibility in private for‐profit facilities regarding population‐specific programs that public and nonprofit facilities may not have. The consistency with which we see the associations between specific facility characteristics and LGBT program offerings across mental health and substance abuse treatment facilities offer additional support in our findings. For example, for both types of treatment, facilities providing residential or outpatient care were more likely to offer LGBT‐specific services. This may be related to the frequency and duration of services based on treatment type. For instance, inpatient treatment is typically intensive but short in duration as facilities work to stabilize clients in mental health crisis or in need of detoxification. The need for population‐specific services may be better met in residential facilities where clients are in the treatment environment 24 hours a day, or in outpatient settings where treatment may be less frequent but longer in duration.
At the same time, we see that mental health and substance abuse facility characteristics associated with LGBT‐specific service offerings diverge in important ways. For example, payment options (eg, sliding fee scale, free services, and Medicaid acceptance) were not significantly associated with LGBT‐specific services for mental health facilities, but increased the odds of substance abuse facilities offering LGBT‐specific services. It is possible that substance abuse facilities are better able to offer services at lower cost due to receipt of government grants, a characteristic that was also associated with offering LGBT‐specific programs. Although not assessed among substance abuse facilities, it is important to note that mental health facilities with a religious affiliation were significantly less likely than those without a religious affiliation to offer LGBT‐specific services. This likely reflects the complex relationship between many dominant US religious organizations and LGBT people. 66 , 67 , 68 Even with acknowledging the diversity of LGBT acceptance across different religious denominations, 69 there is still a strong and prominent history that reflects a tenuous relationship between religious organizations and LGBT people. Our findings likely reflect this ongoing tension.
We were also interested in understanding whether states that had a greater proportion of LGBT people might be more likely to have state‐approved facilities that offer LGBT‐specific programs. Although state‐level LGBT population density was associated with the availability of LGBT‐specific mental health treatment programs, this was not the case for substance abuse treatment programs. For mental health treatment facilities, a 1 percent change in LGBT population density was associated with a 3 percent change in the proportion of facilities that offer LGBT‐specific services. These findings are promising in that it appears that mental health facilities are recognizing the needs of their local LGBT populations, or it may be that state‐level policies and recommendations encourage LGBT‐specific services in states with larger LGBT populations. Future research should examine the relationship between LGBT population density, policy, and availability of LGBT‐specific services. The null association between LGBT population density and the proportion of substance abuse facilities offering LGBT‐specific programs indicates a gap between population need and supply of services. Considering that LGBT people report high rates of substance abuse, 70 , 71 , 72 , 73 , 74 the lack of available substance abuse treatment programs that consider the needs of LGBT people deserves focused research and policy attention.
4.1. Limitations and future directions
There are several limitations in the current study that spark fruitful areas of future research. It is possible that LGBT‐specific programs were over‐reported in the data. At least one study has found that facilities may inaccurately report offering these programs. 75 Therefore, our results may in fact overestimate the degree to which LGBT‐specific services are offered in the United States. Future work should develop more accurate assessments of the availability and delivery of LGBT‐specific programs. We also were not able to ascertain which types of programs were deemed to be LGBT‐specific. For example, were treatment modalities adapted specifically for LGBT clients? Or did facilities interpret policies that enumerate LGBT identities as being LGBT‐specific programs? Future work should explore how facilities define cultural competency and delineate “LGBT‐specific” programs. Additionally, offering these culturally competent services may differ by treatment modality (eg, group therapy, individual therapy, and family therapy); unfortunately, the data did not allow for us to assess these factors. Furthermore, it would be important to explore how these facilities come to offer LGBT‐specific programs. Are facilities mandated to provide LGBT‐specific services by governing bodies (eg, state policy, mental health accreditation, and ethical standards)? Or are facilities responding to the needs of clientele?
It is also important to note that the N‐MHSS and N‐SSATS only survey state‐approved facilities. Given that licensing and credentialing requirements for mental health and substance abuse facilities vary by state, it is difficult to broadly report on the implications of this inclusion criterion. Given that individual practitioners and small group practices were generally excluded (unless a state board explicitly requested their inclusion), it is possible that the prevalence of LGBT‐specific services is underestimated by this dataset. There are numerous LGBT affirming individual clinicians nationwide that were likely not captured in these surveys.
We were also limited in our ability to make more precise estimates of how LGBT population density is related to the availability of LGBT‐specific services. Future research should consider how to assess population and facility density associations for more granular geographic areas (eg, county, zip code), and investigate additional geographic indicators that influence mental health and substance abuse treatment availability, like urbanicity and local funding allocations for treatment service access. It is likely that LGBT‐specific program providers are in more urban areas, 76 which further disenfranchises LGBT people living in rural areas. Finally, it is notable that both facility surveys assessed program offerings for sexual and gender minorities together (ie, LGB and T). However, social and scientific progress of cisgender sexual minorities have outpaced that of transgender and gender diverse people. Therefore, it is likely that many of the service providers who stated offering services for LGBT people are reporting services specifically tailored to LGB people, but not explicitly transgender people. 77 This distinction is important as there are critical differences in the experiences and health needs of sexual and gender minorities. Future work should seek to explore availability of services for both sexual and gender minorities together, and independently, as findings would offer vital information for the availability of services for these two distinct groups.
5. CONCLUSIONS
Given the overwhelming mental health and substance abuse burden among LGBT populations, as well as emergent evidence on the efficaciousness of LGBT‐tailored programs, it is critical that LGBT people have access to culturally competent treatment options. Our findings highlight that the national prevalence of LGBT‐specific mental health and substance abuse treatment programs is alarmingly low. Researchers should continue to draw attention to the availability, or lack thereof, of LGBT‐specific mental health and substance abuse services in the hopes that practitioners, policymakers, and other key stakeholders address the unmet needs of LGBT people seeking affirming services. This is a critical task in a multipronged effort to eliminate LGBT population health disparities in the United States.
Supporting information
Author Matrix
ACKNOWLEDGMENTS
Joint Acknowledgment/Disclosure Statement: Williams gratefully acknowledges fellowship support from the Southern Regional Education Board. This work was also supported by the Eunice Kennedy Shriver National Center for Child Health and Human Development grant P2CHD041041, Maryland Population Research Center and the University of Maryland Prevention Research Center.
Williams ND, Fish JN. The availability of LGBT‐specific mental health and substance abuse treatment in the United States. Health Serv Res. 2020;55:932–943. 10.1111/1475-6773.13559
REFERENCES
- 1. Substance Abuse and Mental Health Services Administration . Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health; 2018:124.
- 2. Grant BF, Saha TD, Ruan WJ, et al. Epidemiology of DSM‐5 drug use disorder. JAMA Psychiatry. 2016;73(1):39‐47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Cochran BN, Cauce AM. Characteristics of lesbian, gay, bisexual, and transgender individuals entering substance abuse treatment. J Subst Abuse Treat. 2006;30(2):135‐146. [DOI] [PubMed] [Google Scholar]
- 4. Herbst JH, Jacobs ED, Finlayson TJ, et al. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: A systematic review. AIDS Behav. 2008;12(1):1‐17. [DOI] [PubMed] [Google Scholar]
- 5. Hughes TL, Eliason M. Substance use and abuse in Lesbian, Gay, bisexual and transgender populations. J Prim Prev. 2002;22(3):263‐298. [Google Scholar]
- 6. Kerridge BT, Pickering RP, Saha TD, et al. Prevalence, sociodemographic correlates and DSM‐5 substance use disorders and other psychiatric disorders among sexual minorities in the United States. Drug Alcohol Depend. 2017;170:82‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. McCabe SE, Hughes TL, Bostwick WB, West BT, Boyd CJ. Sexual orientation, substance use behaviors and substance dependence in the United States. Addict Abingdon Engl. 2009;104(8):1333‐1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Bränström R, Pachankis JE. Sexual orientation disparities in the co‐occurrence of substance use and psychological distress: a national population‐based study (2008–2015). Soc Psychiatry Psychiatr Epidemiol. 2018;53(4):403‐412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. McCabe SE, West BT, Hughes TL, Boyd CJ. Sexual orientation and substance abuse treatment utilization in the United States: results from a national survey. J Subst Abuse Treat. 2013;44(1):4‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am J Public Health. 2010;100(3):468‐475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry. 2008;8(1):70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Marshal MP, Dietz LJ, Friedman MS, et al. Suicidality and depression disparities between sexual minority and heterosexual youth: a meta‐analytic review. J Adolesc Health. 2011;49(2):115‐123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Plöderl M, Tremblay P. Mental health of sexual minorities. A systematic review. Int Rev Psychiatry. 2015;27(5):367‐385. [DOI] [PubMed] [Google Scholar]
- 14. Borgogna NC, McDermott RC, Aita SL, Kridel MM. Anxiety and depression across gender and sexual minorities: Implications for transgender, gender nonconforming, pansexual, demisexual, asexual, queer, and questioning individuals. Psychol Sex Orientat Gend Divers. 2019;6(1):54‐63. [Google Scholar]
- 15. Friedman MR, Dodge B, Schick V, et al. From bias to bisexual health disparities: attitudes toward bisexual men and women in the United States. LGBT Health. 2014;1(4):309‐318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bostwick WB, Boyd CJ, Hughes TL, West BT, McCabe SE. Discrimination and mental health among lesbian, gay, and bisexual adults in the United States. Am J Orthopsychiatry. 2014;84(1):35‐45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bockting WO, Miner MH, Swinburne Romine RE, Hamilton A, Coleman E. Stigma, mental health, and resilience in an online sample of the US transgender population. Am J Public Health. 2013;103(5):943‐951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Meyer IH. Minority stress and mental health in Gay Men. J Health Soc Behav. 1995;36(1):38. [PubMed] [Google Scholar]
- 19. Meyer IH. Prejudice, social stress, and mental health in Lesbian, Gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. 2003;129(5):674‐697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Lombardi E. Substance use treatment experiences of transgender/transsexual men and women. J LGBT Health Res. 2007;3(2):37‐47. [DOI] [PubMed] [Google Scholar]
- 21. Flentje A, Livingston NA, Roley J, Sorensen JL. Mental and physical health needs of Lesbian, Gay, and bisexual clients in substance abuse treatment. J Subst Abuse Treat. 2015;58:78‐83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Hardesty M, Cao D, Shin H‐C, Andrews CM, Marsh J. Social and health service use and treatment outcomes for sexual minorities in a national sample of substance abuse treatment programs. J Gay Lesbian Soc Serv. 2012;24(2):97‐118. [Google Scholar]
- 23. Senreich E. Are specialized LGBT program components helpful for Gay and Bisexual men in substance abuse treatment? Subst Use Misuse. 2010;45(7–8):1077‐1096. [DOI] [PubMed] [Google Scholar]
- 24. Senreich E. A comparison of perceptions, reported abstinence, and completion rates of Gay, Lesbian, bisexual, and heterosexual clients in substance abuse treatment. J Gay Lesbian Ment Health. 2009;13(3):145‐169. [Google Scholar]
- 25. Avery AM, Hellman RE, Sudderth LK. Satisfaction with mental health services among sexual minorities with major mental illness. Am J Public Health. 2001;91(6):990‐991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Pachankis JE, Hatzenbuehler ML, Rendina HJ, Safren SA, Parsons JT. LGB‐affirmative cognitive‐behavioral therapy for young adult gay and bisexual men: A randomized controlled trial of a transdiagnostic minority stress approach. J Consult Clin Psychol. 2015;83(5):875‐889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Priester MA, Browne T, Iachini A, Clone S, DeHart D, Seay KD. Treatment access barriers and disparities among individuals with co‐occurring mental health and substance use disorders: an integrative literature review. J Subst Abuse Treat. 2016;61:47‐59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Mojtabai R, Chen L‐Y, Kaufmann CN, Crum RM. Comparing barriers to mental health treatment and substance use disorder treatment among individuals with comorbid major depression and substance use disorders. J Subst Abuse Treat. 2014;46(2):268‐273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Cochran SD, Sullivan JG, Mays VM. Prevalence of mental disorders, psychological distress, and mental health services use among lesbian, gay, and bisexual adults in the United States. J Consult Clin Psychol. 2003;71(1):53‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Platt LF, Wolf JK, Scheitle CP. Patterns of mental health care utilization among sexual orientation minority groups. J Homosex. 2018;65(2):135‐153. [DOI] [PubMed] [Google Scholar]
- 31. Hughes T. Alcohol use and alcohol‐related problems among sexual minority women. Alcohol Treat Q. 2011;29(4):403‐435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Eliason MJ, Hughes T. Treatment counselor’s attitudes about lesbian, gay, bisexual, and transgendered clients: urban vs. rural settings. Subst Use Misuse. 2004;39(4):625‐644. [DOI] [PubMed] [Google Scholar]
- 33. Garnets L, Hancock KA, Cochran SD, Goodchilds J, Peplau LA. Issues in psychotherapy with lesbians and gay men: a survey of psychologists. Am Psychol. 1991;46(9):964‐972. [DOI] [PubMed] [Google Scholar]
- 34. Shipherd JC, Green KE, Abramovitz S. Transgender clients: Identifying And Minimizing Barriers To Mental Health Treatment. J Gay Lesbian Ment Health. 2010;14(2):94‐108. [Google Scholar]
- 35. Eliason MJ. Substance abuse counselor’s attitudes regarding lesbian, gay, bisexual, and transgendered clients. J Subst Abuse. 2000;12(4):311‐328. [DOI] [PubMed] [Google Scholar]
- 36. Kreiss JL, Patterson DL. Psychosocial issues in primary care of lesbian, gay, bisexual, and transgender youth. J Pediatr Health Care Off Publ Natl Assoc Pediatr Nurse Assoc Pract. 1997;11(6):266‐274. [DOI] [PubMed] [Google Scholar]
- 37. Lombardi EL, van Servellen G. Building culturally sensitive substance use prevention and treatment programs for transgendered populations. J Subst Abuse Treat. 2000;19(3):291‐296. [DOI] [PubMed] [Google Scholar]
- 38. McGeorge CR, Carlson TS, Toomey RB. An exploration of family therapists’ beliefs about the ethics of conversion therapy: the influence of negative beliefs and clinical competence with Lesbian, Gay, and bisexual clients. J Marital Fam Ther. 2015;41(1):42‐56. [DOI] [PubMed] [Google Scholar]
- 39. Corturillo EM, McGeorge CR, Carlson TS. How prepared are they? Exploring couple and family therapy faculty members’ training experiences in Lesbian, gay, and bisexual affirmative therapy. J Fem Fam Ther. 2016;28(2–3):55‐75. [Google Scholar]
- 40. Logie C, Bridge TJ, Bridge PD. Evaluating the phobias, attitudes, and cultural competence of master of social work students toward the LGBT populations. J Homosex. 2007;53(4):201‐221. [DOI] [PubMed] [Google Scholar]
- 41. Johnson DE. The impact of microaggressions in therapy on transgender and gender‐noncomforming clients: a concurrent nested design study. 2014.
- 42. Martos AJ, Wilson PA, Gordon AR, Lightfoot M, Meyer IH. “Like finding a unicorn”: Healthcare preferences among lesbian, gay, and bisexual people in the United States. Soc Sci Med. 2018;208:126‐133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. U.S. Department of Health and Human Services . Cultural Competence. HHS.gov. https://www.hhs.gov/ash/oah/resources‐and‐training/tpp‐and‐paf‐resources/cultural‐competence/index.html. Published March 1, 2017. Accessed February 1, 2020
- 44. Govere L, Govere EM. How effective is cultural competence training of healthcare providers on improving patient satisfaction of minority groups? A systematic review of literature. Worldviews Evid Based Nurs. 2016;13(6):402‐410. [DOI] [PubMed] [Google Scholar]
- 45. Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: a systematic review of reviews. BMC Health Serv Res. 2014;14(1):99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Educational Policy and Accreditation Standards for Baccalaureate and Master’s Social Work Programs . Council on Social Work Education. 2015.
- 47. AMHCA Code of Ethics . American Mental Health Counselors Association. 2015.
- 48. Standards and Indicators for Cultural Competence in Social Work Practice . National Association of Social Workers. 2015.
- 49. Hicks D. The importance of specialized treatment programs for Lesbian and Gay patients. J Gay Lesbian Psychother. 2000;3(3–4):81‐94. [Google Scholar]
- 50. Center for Substance Abuse Treament . A Provider’s Introduction to Substance Abuse Treatment for Lesbian, Gay, Bisexual, and Transgender Individuals. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2019. [Google Scholar]
- 51. Olmstead T, Sindelar JL. To what extent are key services offered in treatment programs for special populations? J Subst Abuse Treat. 2004;27(1):9‐15. [DOI] [PubMed] [Google Scholar]
- 52. Center for Substance Abuse Treament . What is Substance Abuse Treatment? A Booklet for Families. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004. [Google Scholar]
- 53. Mental Health America . Mental Health Treatments. Mental Health America. https://www.mentalhealthamerica.net/types‐mental‐health‐treatments. Published August 19, 2013. Accessed July 29, 2019
- 54. Healthcare Equality Index 2019 . Human Rights Campaign. 2019.
- 55. Religious Refusals in Health Care: A Prescription for Disaster . Movement Advancement Project, National Center for Transgender Equality. 2018.
- 56. Duggan MG. Hospital ownership and public medical spending. Q J Econ. 2000;115(4):1343‐1373. [Google Scholar]
- 57. Busch SH, Meara E, Huskamp HA, Barry CL. Characteristics of adults with substance use disorders expected to be eligible for Medicaid under the ACA. Psychiatr Serv. 2013;64(6):520‐526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Substance Abuse and Mental Health Services Administration . The TEDS Report: Health Insurance Status of Adult Substance Abuse Treatment Admissions Aged 26 or Older: 2011. The TEDS Report. https://www.samhsa.gov/data/sites/default/files/sr134‐health‐insurance‐2014/sr134‐health‐insurance‐2014/sr134‐health‐insurance‐2014.htm. Accessed January 24, 2020 [PubMed]
- 59. Substance Abuse and Mental Health Services Administration . National Mental Health Services Survey (N‐MHSS): 2016. Data on Mental Health Treatment Facilities. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2017. [Google Scholar]
- 60. Substance Abuse and Mental Health Services Administration . National Survey of Substance Abuse Treatment Services (N‐SSATS): 2016. Data on Substance Abuse Treatment Facilities. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2017. [Google Scholar]
- 61. Hatzenbuehler ML, Flores AR, Gates GJ. Social attitudes regarding same‐sex marriage and LGBT health disparities: results from a national probability sample. J Soc Issues. 2017;73(3):508‐528. [Google Scholar]
- 62. Gates GJ. LGBT Parenting in the United States. Los Angeles, CA: The Williams Institute, UCLA School of Law; 2013. [Google Scholar]
- 63. Gates GJ. Marriage and family: LGBT individuals and same‐sex couples. Future Child. 2015;25(2):67‐87. [Google Scholar]
- 64. Gates GJ. LGBT Demographics: Comparisons among Population‐Based Surveys. The Williams Institute, UCLA School of Law; 2014. [Google Scholar]
- 65. StataCorp . Stata Statistical Software: Release 15. College Station, TX: StataCorp, LLC; 2017. [Google Scholar]
- 66. Wright N. Attendance matters: religion and ethical affirmation of Gay and Lesbian Sexuality. Rev Relig Res. 2014;56(2):245‐273. [Google Scholar]
- 67. Halkitis PN, Mattis JS, Sahadath JK, et al. The meanings and manifestations of religion and spirituality among Lesbian, Gay, Bisexual, and transgender adults. J Adult Dev. 2009;16(4):250‐262. [Google Scholar]
- 68. Page MJL, Lindahl KM, Malik NM. The role of religion and stress in sexual identity and mental health among Lesbian, Gay, and bisexual youth. J Res Adolesc. 2013;23(4):665‐677. 10.1111/jora.12025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Human Rights Campaign . Faith Positions. Human Rights Campaign. http://www.hrc.org/resources/faith‐positions/. Accessed July 29, 2019
- 70. McCabe SE, Bostwick WB, Hughes TL, West BT, Boyd CJ. The relationship between discrimination and substance use disorders Among Lesbian, Gay, and bisexual adults in the United States. Am J Public Health. 2010;100(10):1946‐1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Drabble LA, Trocki KF, Korcha RA, Klinger JL, Veldhuis CB, Hughes TL. Comparing substance use and mental health outcomes among sexual minority and heterosexual women in probability and non‐probability samples. Drug Alcohol Depend. 2018;185:285‐292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Drabble L, Midanik LT, Trocki K. Reports of alcohol consumption and alcohol‐related problems among homosexual, bisexual and heterosexual respondents: results from the 2000 National Alcohol Survey. J Stud Alcohol. 2005;66(1):111‐120. [DOI] [PubMed] [Google Scholar]
- 73. Hughes TL, Johnson TP, Steffen AD, Wilsnack SC, Everett B. Lifetime victimization, hazardous drinking, and depression among heterosexual and sexual minority women. LGBT Health. 2014;1(3):192‐203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Wilsnack SC, Hughes TL, Johnson TP, et al. Drinking and drinking‐related problems among heterosexual and sexual minority women. J Stud Alcohol Drugs. 2008;69(1):129‐139. [DOI] [PubMed] [Google Scholar]
- 75. Cochran BN, Peavy KM, Robohm JS. Do specialized services exist for LGBT individuals seeking treatment for substance misuse? A study of available treatment programs. Subst Use Misuse. 2007;42(1):161‐176. [DOI] [PubMed] [Google Scholar]
- 76. Martos AJ, Wilson PA, Meyer IH. Lesbian, gay, bisexual, and transgender (LGBT) health services in the United States: Origins, evolution, and contemporary landscape. Prestage G, ed. PLoS One. 2017;12(7):e0180544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Russell ST, Fish JN. Mental health in Lesbian, Gay, bisexual, and transgender (LGBT) youth. Annu Rev Clin Psychol. 2016;12(1):465‐487. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Author Matrix