

Abstract
Background:
There are known associations between mental health symptoms and transgender identity among adults. Whether this relationship extends to early adolescents and to gender domains other than identity is unclear. This study measured dimensions of gender in a large, diverse, sample of youth, and examined associations between diverse gender experiences and mental health.
Methods:
The ABCD study is an ongoing, longitudinal, United States cohort study. Baseline data (release 2.0) includes 11,873 youth age 9/10 (48% female); and the 4,951 1-year follow-up visits (age 10/11; 48% female) completed prior to data release. A novel gender survey at the 1-year visit assessed felt-gender, gender contentedness, and gender nonconformity using a 5-point scale. Mental health measures included youth- and parent-reports.
Results:
Roughly half a percent of 9/10 year-olds (n=58) responded “yes” or “maybe” when asked, “Are you transgender” at baseline. Recurrent thoughts of death were more prevalent among these youth compared to the rest of the cohort (19.6% vs 6.4%, χ2=16.0, p<0.001). At the 1-year visit, when asked about the three dimensions of gender on a 5-point scale, 33.2% (n=1,605) provided responses that were not exclusively and totally aligned with one gender. Significant relationships were observed between mental health symptoms and gender diversity for all dimensions assessed.
Conclusions:
Similar to adult studies, early adolescents identifying as transgender reported increased mental health symptoms. Results also point to considerable diversity in other dimensions of gender (felt-gender, gender contentedness, gender nonconformity) among 10/11-year-olds, and find this diversity to be related to critical mental health symptoms. These findings add to our limited understanding of the relationship between dimensions of gender and wellness for youth.
Keywords: Gender diversity, gender expression, nonconformity, suicidality, early adolescent, transgender
Introduction
Transgender adults and adolescents experience striking rates of suicide, self-harm (Connolly et al 2016., Haas, 2014), and long-term mental health problems (Rider et al., 2018) compared with their cisgender peers (see Table 1 for definitions of gender-related terms, bolded in text at first use). With over 1.5 million transgender Americans (1–2% of youth age 12–19 from population-based surveys) this is of significant concern (Herman, 2017; Johns et al., 2019). In most surveys, transgender youth are identified through a single item (“are you transgender” yes/no)(Johns et al., 2019); or assessed using the two-step method which asks sex assigned at birth and gender identity using categorical options (boy, girl, transgender, something else) (Reisner et al., 2014).
Table 1:
Gender Terminology – definitions and assessment in the ABCD study.
| Definition | Item in ABCD Study | |
|---|---|---|
| SEX | The assignment as male or female, usually based on physical anatomy and/or chromosomes at birth. | What sex was your child assigned at birth, on the original birth certificate?a |
| GENDER | The social expectations placed on individuals based on their sex. | - |
| GENDER IDENTITY | Internal sense of oneself as boy, girl, or something else. | - |
| CISGENDER | Individuals whose gender identity is sex-congruent | Not asked |
| TRANSGENDER | Individuals whose gender identity differs from the sex they were assigned at birth | Are you transgender?b |
| ASSESSED IN THE QUANTITATIVE, MULTI-DIMENSIONAL GENDER SURVEY | ||
| Dimension | Definition | Itemc |
| FELT-GENDER | The degree of feeling (or not) like the gender aligned with sex and the gender aligned with the opposite sex. Felt gender can be sex-congruent or not. | How much do you feel like a girl? |
| How much do you feel like a boy? | ||
| GENDER EXPRESSION | The communication of gender through appearance, mannerisms, etc. Gender nonconformity is assessed in this study. | How much have you dressed/acted as a boy during play? |
| GENDER CONTENTEDNESS | Happiness with being the gender aligned with sex. Gender non-contentedness is assessed in this study. | How much have you had the wish to be a boy? |
Parent-report demographic survey.
Youth-report KSADS-5 background item.
The female version of the multi-dimensional gender survey; male items are identical with opposite gendered nouns.
Gender is defined as the attitudes, feelings, and behaviors that a culture associates with a person’s sex assigned at birth (American Psychiatic Association, 2015). Gender is increasingly understood to be multidimensional, with different aspects of gender following different developmental trajectories (McHale et al 2009). Among these dimensions are felt-gender, gender expression, and gender contentedness (Table 1). Growing evidence demonstrates that not all people experience gender as dichotomous (feeling exclusively like one gender). As many as 35% of cisgender adults feel, to some extent, like the “other” gender (Joel, 2013). Studies of gender expression in community samples of adolescents find 20–27% reporting moderate to high nonconformity, and gender nonconformity is associated with greater short- and long-term mental health problems (Rider et al., 2018). While this evidence suggests meaningful diversity in the experience of gender generally, research on youth frequently only asks about gender identity, potentially missing important individual differences in other aspects of gender.
Most studies on gender and mental health focus on minority populations of older adolescents and young adults. There remains a dearth of information about gender experiences in late childhood and early adolescence (9–13 years). Yet early adolescence is a time of active identity development involving exploration of roles and values across domains of identity (i.e., religious, academic, ethnic; Erikson 1968). Gender development is particularly linked to early adolescence because of physical puberty, changing gendered behavioral expectations, and shifts in peer groups from being predominantly sex-segregated to being more integrated (Byne et al., 2012; Kaltiala-Heino et al., 2003; Steensma et al., 2011). The lack of gender research in early adolescents may be in part due to methodological challenges such as youth having an emerging understanding of the abstract concept of identity and a lack of familiarity with terminology (i.e., transgender). The presumption that most youth, (i.e., cisgender youth) lack detectable and/or meaningful gender diversity has likely contributed to a lack of research as well.
Recent inter-agency recommendations from the United States government for assessing gender in surveys include using a quantitative scale (i.e., how much do you…), asking both male and female questions, and asking (at a minimum) about both identity and expression (Evaluations of Sexual Orientation and Gender Identity Survey Measures: what have we learned?, 2016). Taken together, the literature suggests that using quantitative scales and assessing multiple dimensions may help to elucidate how individual differences in gender experiences relate to mental health among youth.
This study
In the Adolescent Brain Cognitive Development (ABCD) study, we extend the science of gender and mental health in late childhood and early adolescence. We first ascertain the prevalence of transgender-identified participants age 9/10 years. We next evaluate the following hypotheses: (1) a multi-dimensional gender survey will be acceptable to this age group (measured by completion rates), (2) there will be evidence of gender diversity indicated by response patterns using the full range of the quantitative scales in all youth, and (3) this diversity will relate to mental health symptoms for those who are and are not transgender.
Methods
Participants
The ABCD Study is an ongoing, longitudinal study that began in 2016 and includes 11,875 youth recruited at ages 9/10 from 22 sites who are followed today at 21 sites across the United States. Detailed information regarding recruitment strategies and study procedures can be found at www.ABCDstudy.org. Exclusion criteria included sensory, intellectual, medical or neurological issues that would interfere with participation or data quality (Garavan et al., 2018). ABCD study measures of demographics and mental health are detailed in (Barch et al., 2018).
Measures
A 4-item gender survey measuring felt-gender, gender non-contentedness, and gender nonconformity was administered to youth at the 1-year visit (items are in Table 2). This survey was part of a large battery, administered by trained research personnel. Parent-reported sex was used to assign the male or female version of the survey (items were identical, but with opposite gendered nouns).
Table 2.
Demographics for complete baseline cohort and 1-year follow-up subset.
| Baseline Cohort n = 11873 |
1-Year Subset n = 4951 |
||
|---|---|---|---|
| Age in months, M (SD) | 118.9 (7.5) | 132.0 (7.6) | |
| Female | 5681 (47.9) | 2369 (47.9) | |
| Race & Ethnicity | n=11857 | n=4933 | |
| Asian | 252 (2.1) | 115 (2.3) | |
| Black | 1779 (15.0) | 464 (9.4) | |
| Hispanic | 2407 (20.3) | 941 (19.0) | |
| White | 6174 (52.1) | 2942 (59.4) | |
| Other | 1245 (10.5) | 489 (9.9) | |
| Highest Household Education | n=11869 | n=4934 | |
| < HS Degree | 601 (5.1) | 187 (3.8) | |
| HS Degree | 802 (6.8) | 250 (5.1) | |
| GED | 330 (2.8) | 97 (2.0) | |
| College/Associate/Vocational | 3079 (25.9) | 1208 (24.4) | |
| Bachelor’s | 3014 (25.4) | 1355 (27.4) | |
| Advanced Degrees | 4043 (34.1) | 1851 (37.4) | |
| Items from KSADS-5 youth interview |
Raw n=11858 |
Weighteda n=8221422 |
Raw n=4942 |
| Are you Transgender? | |||
| Yes | 12 (0.1) | 6892 (0.1) | 7 (0.1) |
| Maybe | 46 (0.4) | 34435 (0.4) | 42 (0.9) |
| No | 7111 (60.0) | 4867491 (59.2) | 4017 (81.3) |
| I don’t understand | 4689 (39.5) | 3312604 (40.3) | 876 (17.7) |
No. (%) unless otherwise specified. Ns are included when missing data. Numbers may not sum to group totals because of missing data. Group percentages may not add to 100 due to rounding. Abbreviations: HS, high school; GED, general education development; Prof/Doct, Professional or Doctoral degree.
Weighted prevalence refer to US population estimates.
Transgender participants were identified with the item “Are you transgender?” administered as background to the mental health semi-structured interview (the Kiddie Schedule for Affective Disorders and Schizophrenia; KSADS-5; (Kaufman et al., 2013). Responses of “yes” and “maybe were combined to indicate transgender youth, consistent with prior literature (Calzo & Blashill, 2018). For participants who responded “yes” or “maybe”, the question “Has this caused problems for you at school?” was asked next.
Mental health measures we report include items from the youth KSADS-5 suicide module, a semi-structured interview, administered to the youth, and validated for assessment in ages 6–18 (Kaufman et al., 1997). The total problems score from the Child Behavior Checklist (CBCL), a parent-report measure of emotional and behavioral problems (Achenbach, 2009), is also reported.
The Puberty Development Scale (PDS; Petersen et al.,) was completed by both youth and parent. A composite score (the average of the parent and youth scores, range 1–5) was used. When only one informant responded (parent n=32; youth n=8) the available score was used.
Available data
This manuscript uses data from the 2018 ABCD Data Release 2.0 (see acknowledgements). This release consists of 11,875 youth at baseline and 4,951 youth who had completed the 1-year visit when the data set was closed for release 2.0. The 1-year follow-up sample is representative of the full sample, and full-cohort data from this visit will be available in a future ABCD data release. Two participants were excluded from baseline for missing data, leaving 11,873 subjects. Participants who did not complete the gender survey (n=12) and those who completed the wrong version (n=4) were excluded, leaving 4,935 subjects in the 1-year analysis.
Statistical analyses
The American Community Survey (ACS) 2011–2015 was used as the U.S. population benchmark for youth. The propensity methodology is described by Elliott (2017). Raked propensity weights were used to estimate U.S. population prevalence.
Stepwise logistic regression (implemented in SAS 9.4) was used for the KSADS-5 item assessing recurrent thoughts of death. Models were fit with and without gender variables, with the demographic-only model including age, puberty, sex, highest household education, race, site and family (to accommodate the non-independence of siblings and twins in ABCD).
Linear mixed models were used to examine the relationship between gender variables and parent-reported total problems on the CBCL. Fixed effects included age, puberty, sex, highest household education, and race/ethnicity. Families nested within site were modeled as a random effect. Residuals were not normally distributed, so a square root transform was applied. Post-hoc tests used Dunnett’s method to correct for multiple comparisons.
Additional statistical tests (an elastic net regularized logistic regression and a split-half linear mixed model) were used to demonstrate robustness (Appendix S1).
Ethical considerations
Parents provided written informed consent and youth provided assent to a research protocol that was approved by the relevant institutional review boards.
Results
Prevalence and assessment of transgender identity
The demographics for baseline and 1-year samples, and weighted U.S. population prevalence estimates are presented in Table 2. Transgender identity (“yes” or “maybe” to “Are you transgender?”) was present in n=58 participants at baseline, representing 0.5% of the sample; translating to a weighted estimate of 41,327 youth in the US. In the available 1-year follow-up sample (n=4,942), 1.0% (n=49) responded yes or maybe. 39.5% (n=4,689) of youth at baseline and 17.7% (n=876) at 1-year, indicated they did not understand the question.
KSADS-5 suicide module items were examined and at baseline, 19.6% (n=11) of transgender participants indicated that they had experienced recurrent thoughts of death and 17.9% (n=10) endorsed non-suicidal self-harm, compared to 6.4% (n=750) and 5.9% (n=700) of peers (“no” or “I don’t understand”), respectively. While only 10.3% of transgender youth report their identity causing problems at school or home, thoughts of death (χ2=15.3, p<0.001) and non-suicidal self-harm (χ2 = 13.1, p < 0.001) were significantly more frequent in transgender youth compared to the rest of the sample. At the 1-year visit, 26.5% (n=13) of transgender participants endorsed recurrent thoughts of death and 22.5% (n=11) endorsed self-harm compared to 5.9% (n=286) and 4.6% (n=225) in the rest of the sample.
Acceptability and diverse response patterns on the multi-dimensional gender survey at 1-year
We hypothesized (Hypotheses 1 and 2) that the gender survey would be acceptable to youth (measured by completion rates) and that it would capture gender diversity with response patterns using the full range of the quantitative scale. Summaries of youth responses to the multi-dimensional gender survey are presented in Table 3. Only 8 (0.2%) youth “declined” all 4 items, and the rates of declining individual items were low (range 0.4% – 1.2%) (Table 3). Responses by both males and females spanned the entire scale for all 4 items. The majority of participants 65.2% (n=3,217) endorsed the anchor response aligned with their sex, or the “sex-congruent anchor”, on all items; and males were more likely to do so than females (Item 1 “totally”, χ2=157.3, p<.001; Item 2 “not at all”, χ2=193.4, p<.001; Item 3 “never”, χ2=33.1, p<.001; Item 4 “never”, χ2=150.7, p<.001; Table 3).
Table 3.
Youth Multi-Dimensional Gender Survey by Assigned Sex
| Item 1. How much do you feel like a <boy/girl>? (sex-congruent felt-gender) | ||||||
|---|---|---|---|---|---|---|
| Totally | Mostly | Somewhat | A Little | Not at All | Decline | |
| All | 4222 (85.6) | 497 (10.1) | 149 (3.0) | 36 (0.7) | 13 (0.3) | 18 (0.4) |
| Male <boy> | 2356 (91.6) | 170 (6.6) | 26 (1.0) | 8 (0.3) | 5 (0.2) | 8 (0.3) |
| Female <girl> | 1866 (79.0) | 327 (13.8) | 123 (5.2) | 28 (1.2) | 8 (0.3) | 10 (0.4) |
| Item 2. How much do you feel like a <girl/boy>? (sex-incongruent felt-gender) | ||||||
| Not at All | A Little | Somewhat | Mostly | Totally | Decline | |
| All | 4304 (87.2) | 421 (8.5) | 96 (2.0) | 39 (0.8) | 14 (0.3) | 61 (1.2) |
| Male <girl> | 2407 (93.6) | 106 (4.1) | 14 (0.5) | 6 (0.2) | 2 (0.1) | 38 (1.5) |
| Female <boy> | 1897 (80.3) | 315 (13.3) | 82 (3.5) | 33 (1.4) | 12 (0.5) | 23 (1.0) |
| Item 3. How much have you had the wish to be a <girl/boy>? (gender non-contentedness) | ||||||
| Never | Rarely | Sometimes | Often | Always | Decline | |
| All | 4426 (89.7) | 317 (6.4) | 101 (2.1) | 25 (0.5) | 20 (0.4) | 46 (0.9) |
| Male <girl> | 2369 (92.1) | 132 (5.1) | 30 (1.2) | 8 (0.3) | 5 (0.2) | 29 (1.1) |
| Female <boy> | 2057 (87.1) | 185 (7.8) | 71 (3.0) | 17 (0.7) | 15 (0.6) | 17 (0.7) |
| Item 4. How much have you dressed or acted as a <girl/boy> during play? (gender nonconformity) | ||||||
| Never | Rarely | Sometimes | Often | Always | Decline | |
| All | 3894 (78.9) | 611 (12.4) | 283 (5.7) | 73 (1.5) | 26 (0.5) | 48 (1.0) |
| Male <girl> | 2206 (85.7) | 237 (9.2) | 85 (3.3) | 11 (0.4) | 3 (0.1) | 31 (1.2) |
| Female <boy> | 1688 (71.5) | 374 (15.8) | 198 (8.4) | 62 (2.6) | 23 (1.0) | 17 (0.7) |
No. (%) Group percentages may not add to 100 due to rounding. The sex-congruent anchor response is first.
Characterizing felt-gender
Felt-gender was examined by looking at the first two items together, “I feel like a <boy/girl>” and “I feel like a <girl/boy>”, to interrogate whether felt-gender is dichotomous (feeling “totally” like one gender and “not at all” like the other gender). Figure 1 shows the crosstabs of responses. Of those who responded to both items (n=4,869), 17.8% did so non-dichotomously (something other than the scale anchors - the top left and bottom right cells outlined in bold in Figure 1).
Figure 1.
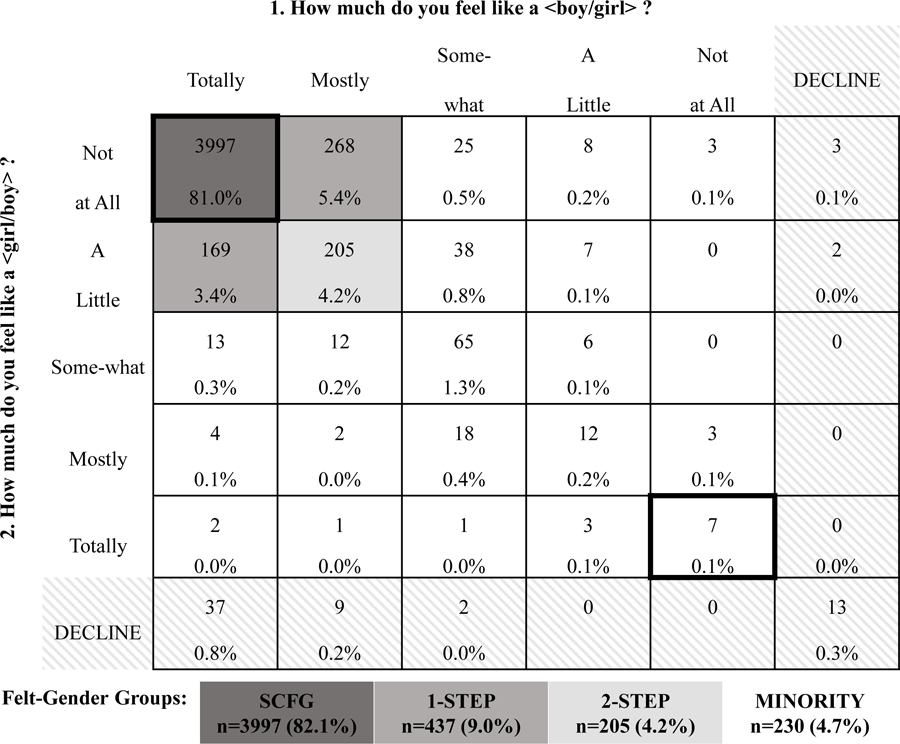
Multi-Dimensional Felt-Gender Response Patterns and Felt-Gender Groups.
No. (%). The dichotomous, anchor responses are outlined in bold. Abbreviation: SCFG, sex-congruent felt-gender.
To examine the relationship between felt-gender, and mental health participants were grouped based on felt-gender response patterns (Figure 1). The first group (sex-congruent felt-gender; SCFG) responded with sex-congruent anchors on both items (i.e., a female feeling “totally” like a girl and “not at all” like a boy). The 1-STEP group endorsed the sex-congruent anchor on one item and the response option 1-step away from the anchor on the other item (i.e., a female feeling “totally” like a girl and “a little” like a boy; or “mostly” like a girl and “not at all” like a boy). The 2-STEP group responded with the response option 1-step from the sex-congruent anchor on both felt-gender items (i.e., a female feeling “mostly” like a girl and “a little” like a boy). All other responses (unshaded cells) comprised the MINORITY felt-gender group.
The demographics of the 1-year sample by felt-gender group are in Table S1. The percent of females increased significantly in each felt-gender group as you move away from SCFG (compared to SCFG - 1-STEP, χ2=69.3, p<.001; 2-STEP, χ2=76.7, p<.001; MINORITY, χ2=129.0, p<.001). All groups were significantly younger than the SCFG group (by at most 1.9 months; 1-STEP, t=−3.30, p=.001; 2-STEP, t=−3.42, p<.001; MINORITY, t=−2.79, p=.005). In addition, all groups were significantly further in puberty than the SCFG group (1-STEP, t=6.05, p<.001; 2-STEP, t=5.13, p<.001; MINORITY, t=6.07, p<.001). Most but not all transgender youth were in the MINORITY group (n=32/47). Finally, all racial/ethnic groups and all sites with 1-year data (data not shown) were represented in each of the 4 groups, except site07 which only had 9 participants with 1-year data when the database was closed for release. Responses to the non-contentedness and nonconformity survey items are presented by felt-gender group in Table S2.
Association of gender diversity with youth self-reported mental health
The relationship between responses on the gender survey and mental health was examined to test our third hypothesis (that gender diversity would relate to mental health for all participants). Recurrent thoughts of death were endorsed by 6.0% (n=298) of the total 1-year sample. In the demographic-only regression, puberty was the only significant predictor (AIC=2249; adjusted R2=0.002). The model including felt-gender group performed better (AIC=2124; adjusted R2=0.054) with felt-gender, sex and puberty as significant predictors. All three felt-gender groups were significantly more likely than the SCFG group to have recurrent thoughts of death with odds ratios of 2.3 (95%CI 1.6 – 3.4) for the 1-STEP group; 4.0 (95%CI 2.6 – 6.2) for the 2-STEP group; and 5.4 (95%CI 3.7 – 7.9) for the MINORITY group (Table S3).
Scores on gender non-contentedness improved the model fit (AIC=2130; adjusted R2 = 0.048) over demographics-only with increased likelihood of recurrent thoughts of death for those who responded rarely (OR=3.3, 95%CI 2.3 – 4.6), sometimes (OR=4.9,95%CI 2.9 – 8.1), or often (OR=13.1, 95%CI 5.8 – 29.5) compared to never wishing to be of the opposite sex (Table S3). The gender nonconformity item (acting and/or playing like the opposite sex) improved model fit over demographics-only (AIC=2154; adjusted R2=0.040) with the item, sex and puberty as significant predictors. All responses (compared to “never”) were associated with greater likelihood of recurrent thoughts of death (“rarely” OR=2.5, 95%CI 1.8 – 3.4; “sometimes” OR=2.5, 95%CI 1.7–3.9; “often” OR=5.8, 95%CI 3.2 – 10.5; and “always” OR=5.7, 95%CI 2.1 – 15.5) (Table S3). Associations of gender items with non-suicidal self-injurious behavior were similar (Table S4).
Association of gender diversity with parent-reported child mental health
Felt-gender group was significantly associated with parent-reported CBCL Total Problems score (F(3,733)=13.77; p<.001), and sex did not interact with felt-gender. The SCFG group had lower scores than the 1-STEP (t=−3.18, p=.002); 2-STEP (t=−2.06, p=.039) and MINORITY groups (t=−5.74, p<.001) (Figure 2). The MINORITY group had significantly higher scores than all other groups (1-STEP, t=−2.87, p=.004; and 2-STEP, t=−2.60, p=.010); while the 1-STEP and 2-STEP groups did not differ (t=0.17, p=.867).
Figure 2.
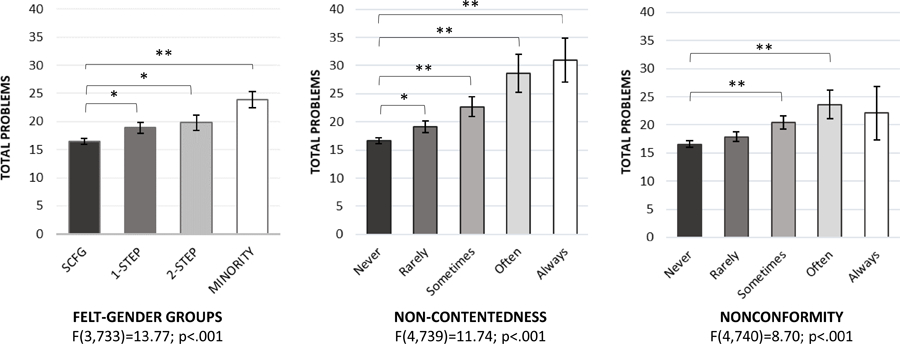
Association of Dimensions of Gender with Parent-Reported Emotional/Behavior Total Problems.
LS Means and SEs for raw scores are plotted for interpretability. Significance determined by linear mixed models with demographics as fixed effects and families nested within site as random effect, with square root transformed Total Problems scores. Only significant differences from the sex-congruent anchor (SCFG group or “Never”) are shown (all differences are listed in text); * p<.05, ** p<.001. Abbreviation: SCFG, sex-congruent felt-gender.
Gender non-contentedness was also significantly associated with CBCL Total Problems (F(4,739)=11.74; p<.001), with lower problems among those who responded that they never wished to be the opposite sex compared to all other responses (“rarely” t=2.92, p=.004; “sometimes” t=3.96, p<.001; “often” t=3.37, p<.001; “always” t=3.88, p<.001) (Figure 2). Those who endorsed “rarely” had fewer problems than those who endorsed “sometimes” (t=2.05, p=.041), “often” (t=2.46, p=.014), or “always” (t=3.02, p=.003).
Finally, gender nonconformity was also associated with Total Problems (F(4,740)=8.70; p<.001). Those who responded “never” or “rarely” had fewer problems than those who responded “sometimes” (t=4.42, p<.001; t=2.84, p=.005) or “often” (t=3.64, p<.001; t=2.89, p=.004) (Figure 2).
Replicability
To guard against spurious effects, the logistic regression for the KSADS-5 item assessing recurrent thoughts of death was repeated using an elastic net, regularized regression. 20% of the sample was held out for final model testing, and 80% was used for model generation using 2-folds (a split-half approach). Results replicated the effects of felt-gender, gender non-contentedness, and gender nonconformity seen in the original analysis. The linear mixed model examining CBCL Total problem scores and felt-gender was repeated using a split half framework and the effects were unchanged in both replicates. Full replicability results are described and presented in Appendix S1 and Table S5.
Discussion
The prevalence of transgender youth in the ABCD study ranged from 0.5% at 9/10 years to 1.0% a year later. Very little published data exists on the rate of transgender identity in late childhood and/or early adolescence, and yet health disparities later in life are dire (Johns et al., 2019). Our findings are consistent with the available literature, estimating 0.7% of 13–17 year-olds in the US identify as transgender (Herman, 2017; Johns et al., 2019). Of concern, we found 39.5% of youth reported not understanding the term “transgender” at age 9/10. Thus, while there is intuitive appeal in directly asking youth about gender identity, the data suggest this to be an unreliable and perhaps developmentally inappropriate way to evaluate gender identity in this age group.
Despite this limitation, transgender youth at this young age (9–11 years), had significantly elevated rates of recurrent thoughts of death and self-injurious behavior compared to peers, a finding that is well supported in the literature from middle to late adolescence into adulthood (Becerra-Culqui et al., 2018; Connolly et al., 2016; Eisenberg et al., 2017; Johns et al., 2019; Rider et al., 2018). Of note, few participants reported problems caused by being transgender when asked, supporting the assertion of Connolly and colleagues (2016) that diverse identity is not problematic per se. These findings highlight the importance of directly measuring mental health rather than relying on youth attributions of problems related to their gender identity.
The ABCD study used a quantitative survey to assess gender dimensions at ages 10/11. The rates of declining to answer were minimal, suggesting the items were acceptable and appropriate. Most participants (65.2%, n=3,217) responded to the survey with the anchor responses aligned with their sex. Consistent with our hypothesis that gender dimensions are not dichotomous, (i.e., that the full scale of responses would be used), one third of youth (33.2%, n=1,605) endorsed a response that was not a scale anchor on one or more items.
Analysis of felt-gender revealed broad gender diversity. Felt-gender does not directly measure gender identity, however the responses are consistent with how gender identities are described. For example, non-binary identities include feeling like both genders, neither gender, or some combination of the two – all of which are represented in these data. To what extent, or if, these dimensions translate to current identity or predict future identities is an empirical question that can be addressed in this sample over time. The ABCD participants are a US sample and because gender is learned through cultural socialization additional empirical work to assess whether these dimensions could be used to understand youth in other geographical contexts is warranted. A recent study from Germany found that among 10–16 year-olds (n=940), 4.1% had “variant” gender experience (Becker et al. 2017), which is on par with our 4.7% “minority” felt-gender. Regardless, the current data provide robust evidence for diversity in the experiences of gender among 10/11-year-olds in the US, well beyond those who identify as transgender.
Females showed greater gender diversity than males. This may relate to greater social tolerance for nonconformity in young females compared to males. Interestingly, SCFG youth were the earliest in pubertal development although they were older than those with more diverse felt-gender. The relationship between the physical changes that occur during puberty and awareness of gender diversity may be driving this relationship. For example, during puberty, high levels of body dissatisfaction related to primary and secondary sex characteristics is reported among gender diverse youth (Steensma et al., 2013). It may be that in the ABCD study gender diverse youth recognize during puberty that their changing body is not fully in-line with their gender identity and/or with society’s expectations resulting in the relationship between more advanced puberty and greater gender diversity. The onset of puberty is also linked generally to mental health problems, with early puberty having a relationship to depression and anxiety (Kaltiala-Heino et al., 2003). In the current study we found a relationship between gender diversity and mental health symptoms after controlling for puberty, so we do not believe that pubertal status alone explains these findings.
Puberty is known to be related to brain maturation including development of the pre-frontal cortex (Herting et al 2015; Nguyen et al 2013) which is important integrating information and underlies the development of behavioral control (Forbes & Dahl 2010). Puberty is also associated with heightened neural sensitivity to emotional stimuli (Ladouceur 2012). Taken together, it may be that early puberty increases the saliency of gender diversity during a stage of brain development characterized by relatively immature cognitive processes, and relatively advanced emotional processing. This could contribute to the distress that is seen in early adolescents who are gender diverse. The longitudinal nature of ABCD will help untangle how sex and the timing of puberty relate to gender diversity and mental health.
Another key finding from this study is the association between mental health and gender diversity that extends beyond those youth with a transgender identity. Single items measuring gender non-contentedness and nonconformity related quantitatively to parent and youth reported mental health problems. In addition, youth whose felt-gender was only one or two steps from responses that were completely sex-congruent, had significantly more mental health symptoms. These are largely youth who did not report being transgender and yet their responses show variability that is meaningfully associated with mental health outcomes. It is important to note that the mechanism for these effects (i.e., how environmental effects contribute to this relationship) is not addressed in this study. However, the link between discrimination and prejudice resulting from being part of a minority group, and mental health problems is well known (Meyer 2003). Indeed, for those experiencing gender diversity, there is likely tension resulting from being outside of society’s binary expectations that may contribute to psychiatric distress. A deeper understanding of the factors conferring both risk and resilience associated with gendered experiences is needed.
Conclusion
This study found that roughly 0.5% of 9/10-year-olds and 1.0% a year later report being or possibly being transgender. In addition, this study demonstrates the feasibility of a quantitative, multi-dimensional gender survey in youth, including measurement of felt-gender. The data demonstrates the utility of and need for this type of measure, as 33.3% of participants endorsed a response other than the sex-congruent anchor on one or more items; and this gender diversity was related to critical mental health symptoms regardless of gender identity.
Supplementary Material
Table S1. Demographics and KSADS-5 background transgender item assessed at 1-year by felt-gender groups.
Table S2. 1-Year Youth Multi-Dimensional Gender Survey by Felt-Gender Groups.
Table S3. Association of Dimensions of Gender with Self-Reported “Recurrent Thoughts of Death” and Parent-Reported Emotional/Behavior Problems.
Table S4. Associations of Dimensions of Gender with Self-Injurious Behavior from the KSADS-5
Appendix S1. Replicability.
Table S5. Replicability: Split-Half Linear Mixed Model for Association of Felt-Gender with CBCL Total Problems
Key points.
Transgender and gender non-conforming youth experience high rates of mental health symptoms compared to their cisgender peers; yet the experiences of gender are understudied in this age group.
At age 9/10, 0.5% of youth respond “yes” or “maybe” when asked if they are transgender, consistent with literature in adolescents. 39.5% of 9/10 year olds respond “I don’t understand”.
Quantitative measurement of the dimensions felt-gender, gender non-contentedness, and gender nonconformity in 10/11-year-olds is feasible, and captures meaningful diversity beyond those who identify as transgender.
Critical mental health symptoms were related to all measured gender dimensions (felt-gender, gender non-contentedness, and gender nonconformity) for all youth, not just transgender youth.
Acknowledgements
Data used in this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive. The ABCD Study is supported by the U.S. National Institutes of Health and additional U.S. federal partners under award numbers U01DA041022, U01DA041028, U01DA041048, U01DA041089, U01DA041106, U01DA041117, U01DA041120, U01DA041134, U01DA041148, U01DA041156, U01DA041174, U24DA041123, and U24DA041147. The ABCD data repository grows and changes over time. The ABCD data used in this report came from 2018 ABCD Data Release 2.0 (DOI 10.15154/1503209). A full list of supporters is available at https://abcdstudy.org/nih-collaborators. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/principal-investigators.html. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in analysis or the writing of this report. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or ABCD consortium investigators.
Footnotes
Conflict of interest statement: No conflicts declared.
The authors have declared that they have no competing or potential conflicts of interest.
Supporting information
Additional supporting information may be found online in the Supporting Information section at the end of the article:
References
- Achenbach TM (2009). The Achenbach System of Empirically Based Assessment (ASEBA): Development, Findings, Theory, and Applications. Burlington, VT: University of Vermont Reserach Center for Children, Youth, & Families. [Google Scholar]
- American Psychiatic Association. (2015). Key Terms and Concepts in Understanding Gender Diversity and Sexual Orientation in Students.
- Barch DM, Albaugh MD, Avenevoli S, Chang L, Clark DB, Glantz MD, … Sher KJ (2018). Demographic, physical and mental health assessments in the adolescent brain and cognitive development study: Rationale and description. Dev Cogn Neurosci, 32, 55–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becerra-Culqui TA, Liu Y, Nash R, Cromwell L, Flanders WD, Getahun D, … Goodman M (2018). Mental Health of Transgender and Gender Nonconforming Youth Compared With Their Peers. Pediatrics, 141(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker I, Ravens-Sieberer U, Ottova-Jordan V, & Schulte-Markwort M (2017). Prevalence of Adolescent Gender Experiences and Gender Expression in Germany. J Adolesc Health, 61(1), 83–90. [DOI] [PubMed] [Google Scholar]
- Byne W, Bradley SJ, Coleman E, Eyler AE, Green R, Menvielle E, … Tompkins DA (2012). Treatment of gender identity disorder. Am J Psychiatry, 169(8), 875–876. [DOI] [PubMed] [Google Scholar]
- Calzo JP, & Blashill AJ (2018). Child Sexual Orientation and Gender Identity in the Adolescent Brain Cognitive Development Cohort Study. JAMA Pediatr, 172(11), 1090–1092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connolly MD, Zervos MJ, Barone CJ 2nd, Johnson CC, & Joseph CL (2016). The Mental Health of Transgender Youth: Advances in Understanding. J Adolesc Health, 59(5), 489–495. [DOI] [PubMed] [Google Scholar]
- Eisenberg ME, Gower AL, McMorris BJ, Rider GN, Shea G, & Coleman E (2017). Risk and Protective Factors in the Lives of Transgender/Gender Nonconforming Adolescents. J Adolesc Health, 61(4), 521–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott MV, R. (2017). Inference for nonprobability samples. Statistical Science, 32(2), 249–264. [Google Scholar]
- Erikson EH (1968). Identity: Youth and crisis (No. 7). WW Norton & Company. [Google Scholar]
- Evaluations of Sexual Orientation and Gender Identity Survey Measures: what have we learned? (2016). Retrieved from Federal Committee on Statistical Methodology: https://nces.ed.gov/FCSM/interagency_reports.asp
- Forbes EE, & Dahl RE (2010). Pubertal development and behavior: hormonal activation of social and motivational tendencies. Brain and cognition, 72(1), 66–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garavan H, Bartsch H, Conway K, Decastro A, Goldstein RZ, Heeringa S, … Zahs D (2018). Recruiting the ABCD sample: Design considerations and procedures. Dev Cogn Neurosci, 32, 16–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas AP, Rodgers PL, & Herman JL (2014). Suicide Attempts Among Transgender and Gender Non-Conforming Adults: Findings from the National Transgender Discrimination Survey. Retrieved from UCLA School of Law: https://williamsinstitute.law.ucla.edu/wp-content/uploads/AFSP-Williams-Suicide-Report-Final.pdf
- Herman JL, Flores AR, Brown TNT, Wilson BDM, & Conron KJ (2017). Age of Individuals who Identify as Transgender in the United States. Retrieved from UCLA Law School: https://williamsinstitute.law.ucla.edu/wp-content/uploads/TransAgeReport.pdf
- Herting MM, Gautam P, Spielberg JM, Dahl RE, & Sowell ER (2015). A longitudinal study: Changes in cortical thickness and surface area during pubertal maturation. PLoS ONE, 10, e0119774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joel D, Tarrasch R, Berman Z, Mukamel M, Ziv E (2013). Queering Gender: Studying Gender Identity in ‘Normative’ Individuals. Psychology & Sexuality.
- Johns MM, Lowry R, Andrzejewski J, Barrios LC, Demissie Z, McManus T, … Underwood JM (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students — 19 states and large urban school districts. MMWR Morb Mortal Wkly Rep 68, 67–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaltiala-Heino R, Marttunen M, Rantanen P, & Rimpelä M (2003). Early puberty is associated with mental health problems in middle adolescence. Social science & medicine, 57(6), 1055–1064. [DOI] [PubMed] [Google Scholar]
- Kaufman J, Birmaher B, et al. (2013). KSADS-PL New Haven, CT: Yale University. [Google Scholar]
- Ladouceur CD (2012). Neural systems supporting cognitive-affective interactions in adolescence: the role of puberty and implications for affective disorders. Frontiers in integrative neuroscience, 6, 65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McHale SM, Kim JY, Dotterer AM, Crouter AC, & Booth A (2009). The development of gendered interests and personality qualities from middle childhood through adolescence: A biosocial analysis. Child Development, 80(2), 482–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological bulletin, 129(5), 674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nguyen TV, McCracken J, Ducharme S, Botteron KN, Mahabir M, Johnson W, … Grp BDC (2013). Testosterone-related cortical maturation across childhood and adolescence. Cerebral Cortex, 23, 1424–1432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petersen AC, Crockett L, Richards M, & Boxer A (1988). A self-report measure of pubertal status: Reliability, validity, and initial norms. J Youth Adolesc, 17(2), 117–133. [DOI] [PubMed] [Google Scholar]
- Reisner SL, Conron KJ, Tardiff LA, Jarvi S, Gordon AR, & Austin SB (2014). Monitoring the health of transgender and other gender minority populations: validity of natal sex and gender identity survey items in a U.S. national cohort of young adults. BMC Public Health, 14, 1224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rider GN, McMorris BJ, Gower AL, Coleman E, & Eisenberg ME (2018). Health and Care Utilization of Transgender and Gender Nonconforming Youth: A Population-Based Study. Pediatrics, 141(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steensma TD, Biemond R, de Boer F, & Cohen-Kettenis PT (2011). Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study. Clin Child Psychol Psychiatry, 16(4), 499–516. [DOI] [PubMed] [Google Scholar]
- Steensma TD, Kreukels BP, de Vries AL, & Cohen-Kettenis PT (2013). Gender identity development in adolescence. Horm Behav, 64(2), 288–297. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Demographics and KSADS-5 background transgender item assessed at 1-year by felt-gender groups.
Table S2. 1-Year Youth Multi-Dimensional Gender Survey by Felt-Gender Groups.
Table S3. Association of Dimensions of Gender with Self-Reported “Recurrent Thoughts of Death” and Parent-Reported Emotional/Behavior Problems.
Table S4. Associations of Dimensions of Gender with Self-Injurious Behavior from the KSADS-5
Appendix S1. Replicability.
Table S5. Replicability: Split-Half Linear Mixed Model for Association of Felt-Gender with CBCL Total Problems