

Abstract
Unemployment is a risk factor for suicide. Unemployment insurance is the primary policy tool in the United States for alleviating the burden of unemployment on individuals. Our objective was to estimate the effect of state unemployment insurance accessibility on suicide rates, and effect modification by sociodemographic factors and unemployment rate. We used quarterly data from all 50 U.S. states and Washington, DC from 2000 to 2015, for a total of 3,264 state-quarter units of analysis. The exposure was the quarterly unemployment insurance recipiency rate, i.e. the percentage of unemployed persons who received unemployment insurance. The outcome was the state-quarterly suicide rate per 100,000 population. Linear regression models included state, year, and calendar quarter fixed effects, state time trends, and state-level economic covariates to account for state-specific time-varying confounding. We assessed effect modification by the state-level unemployment rate, educational attainment, age, gender, and race. Based on fully adjusted models, potential protective effects of higher unemployment insurance recipiency rates appear to be small and restricted to demographic groups at higher risk of suicide including men, non-Hispanic White Americans, and those 45–64 years of age. These groups also generally have higher UI recipiency rates, therefore differences in subgroup estimates may reflect variations in eligibility policies and accessibility of UI programs.
Keywords: unemployment, suicide, public policy, economic recession
INTRODUCTION
There is consistent evidence that experiencing unemployment adversely affects health and can increase suicide risk.1–4 Unemployment insurance (UI) programs have been one of the main policy tools in the United States for mitigating financial hardship for individuals experiencing unemployment. The COVID-19 pandemic has resulted in an unprecedented rapid increase in unemployment in the U.S. As during previous economic downturns, the U.S. federal government has responded by increasing resources to states to expand UI benefits. The Coronavirus Aid, Relief, and Economic Security (CARES) Act was signed into law on March 27, 2020 and provides direct support to the states to expand unemployment insurance benefits to workers who are unemployed, partially unemployed, or unable to work due to COVID-19.5 States administer UI benefits within federal guidelines, and there has been significant variation in eligibility, accessibility, and generosity across states and time.6
Limited prior research in the United States7 and Europe8 suggests that more generous UI programs may reduce suicide risk. Effects may not be homogenous across all sociodemographic groups; e.g., suicide rates9 and unemployment rates10 in the U.S. are higher among those with lower educational attainment, while the likelihood of receiving UI increases with education.11 Additionally, prior research in the U.S. has not examined the effect of emergency UI programs on suicide during the economic recession following the 2007–08 financial crisis, when the national unemployment rate rose from 4.4% in May 2007 to 10.0% in October 2009. While the impact of COVID-19 on unemployment is unique in its rapid development and scale, and thus results of new policy responses may differ from the past, it is important to understand how UI programs may impact population health outcomes.
The aim of this study was to estimate the effect of state-level UI program recipiency rates on suicide rates, using data from all 50 states and Washington, DC for the years 2000–2015. We estimated effects of the recipiency rate for regular UI programs for 2000–2015, and for regular plus emergency UI programs (i.e. “all programs”) that were in place from 2008–2013 as part of the federal government’s response to the Great Recession. We examined differences in estimated effects by unemployment rate, educational attainment, age, gender, and race. The recipiency rate is the percentage of unemployed individuals who receive UI benefits, and thus reflects factors beyond de jure policies (e.g. eligibility requirements), including administrative policy,12, 13 de facto implementation, and the application rate for UI benefits, which would not be captured in an analysis focused solely on policy dimensions. Potential barriers to accessibility may be reflected in the fact that overall UI recipiency is generally low,14 and that application and recipiency rates differ across demographic groups.11 Conditional on the unemployment rate and other potential confounders, including seasonal variation, factors affecting UI recipiency rates including and beyond state policies may impact population-level health effects of UI receipt, and thus are included in the hypothesized total effect of each state’s UI system over time.
METHODS
Exposure data:
The independent variable was the unemployment insurance (UI) recipiency rate for each of the 50 U.S. states and Washington, D.C. for each quarter (Jan-Mar, Apr-Jun, Jul-Sep, Oct-Dec) from 2000–2015, publicly available from the Unemployment Insurance Data provided by the United States Department of Labor.15 The recipiency rate represents the percentage of total unemployed who receive UI benefits. We estimated effects for recipiency rates for regular UI programs, which includes state UI programs, Unemployment Compensation for Federal Employees (UCFE), and Unemployment Compensation for Ex-Service members (UCX), and for all UI programs, which additionally includes emergency programs and extended benefit programs. The Unemployment Compensation Extension Act of 2008 and subsequent extensions funded additional emergency unemployment compensation from 2008–2013, thus we estimated the effect of the recipiency rate for all UI programs for these years only.16
Outcome data:
The dependent variable was the state suicide rate for adults ages 18–64 by quarter for 50 states and Washington, D.C. from 2000–2015. For the numerator, we obtained complete, longitudinal death certificate data on suicides by state, month, educational attainment (high school diploma or less/some college/college degree or higher), age (18–24/25–43/35–44/45–54/55–64), race (non-Hispanic White/all other groups), and gender (men/women) from the National Vital Statistics System. For the denominator, we estimated state-by-year populations by education level, gender, race, and age using weighted data from the Current Population Survey.17
Covariates:
We obtained quarterly data (the finest temporal resolution for which data were available) on the state unemployment rate from the United States Department of Labor, and yearly state data on the gross state product, personal income, number of Temporary Assistance for Needy Family (TANF) recipients, and minimum wage from the University of Kentucky Center for Poverty Research.
Design and Analysis
Design:
We used variation in the state-specific UI recipiency rate as a continuous exposure variable reflecting state-specific unemployment program accessibility. We compared state suicide rates across 3,264 state-quarter units of analysis (51 states, 16 years, 4 quarters per year) with varying UI recipiency rates to estimate an average effect across many changes in UI exposure intensity. The directed acyclic graph (DAG) in Figure 1 depicts the assumed causal relationships between relevant variables. Under this framework, the recipiency rate is a product of state UI statutes, administrative policy, and the application rate.18 Potential confounding of the relationship between the recipiency rate and suicide rate exists via the application rate, through factors such as the state unemployment rate, other economic and labor market conditions, and sociocultural factors (e.g. state-level demographic and educational composition) associated directly or indirectly with applying for UI benefits and with suicide risk. We employed a two-way fixed effects approach, with fixed effects for state to control for state-specific factors not varying over the study period (e.g. sociocultural factors), and fixed effects for year to control for time-dependent factors common across states (i.e. national secular trends). We further adjusted for several state-specific time-varying factors, including the state-by-quarter unemployment rate, and state-by-year markers of economic and labor market conditions including the state minimum wage, number of TANF recipients, gross state product, and state personal income. Suicide rates,19 unemployment,20 and UI recipiency vary seasonally, therefore we further adjusted for quarter as a control for potential confounding by seasonality. We estimated the overall effect of UI recipiency rates on suicide, and whether this effect varied by state-specific unemployment rate, education level, age, gender, or race.
Figure 1:
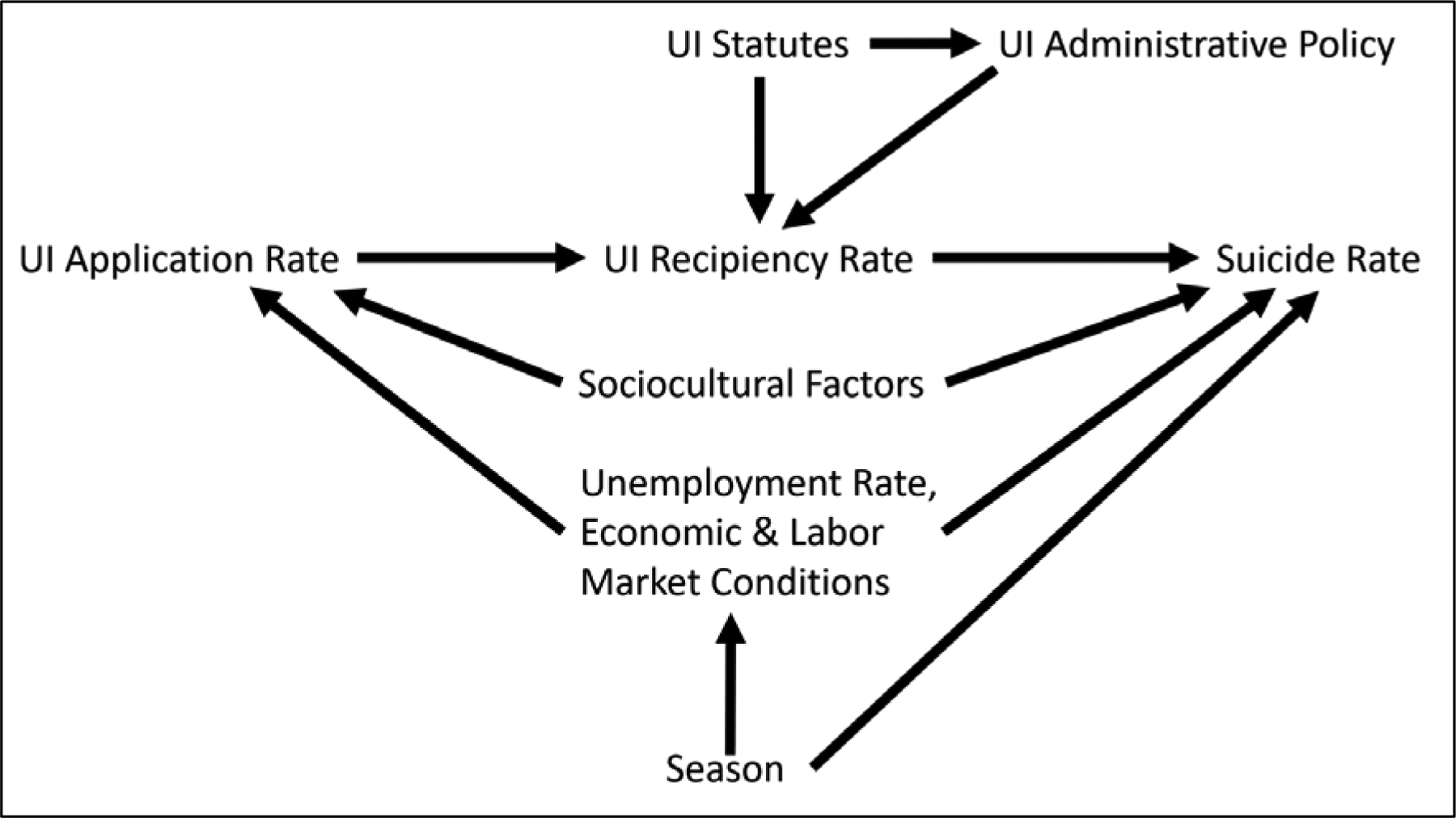
Directed Acyclic Graph (DAG) Depicting the Relationship between State-Level Unemployment Insurance (UI) Recipiency Rates, Suicide Rates, and other State-Level Factors
Analysis:
We used generalized estimating equations with robust standard errors to account for clustering by state and year. We estimated changes in suicide rates per 100,000 population via linear regression. The overall model has the following form:
where D is the suicide rate in state s in quarter q in year t, RR is the unemployment insurance recipiency rate, U is the quarterly unemployment rate, X is a vector containing four state-level annual time-varying factors (state minimum wage, gross state product, the number of AFDC/TANF recipients, and the personal income), Ѳ is a fixed effect for 3-month calendar quarter, δ is a fixed effect for state, ϒ is a fixed effect for year, and δxϒ and δxϒ2 are state-specific linear and quadratic time trends, respectively.
For models stratified by sociodemographic factors, we used the estimated state population within strata as the denominator. To estimate whether the effect of UI recipiency rates varied across level of unemployment, we included an additional model term for the interaction between the recipiency rate and state-quarterly unemployment rate. To estimate differences in the effect of UI recipiency on suicide rates by demographic factors, we modeled stratum-specific rates and included model terms for the demographic factor and the interaction between the demographic factor and UI recipiency rate. Z-scores for these interactions are reported in the results. We performed all analyses using SAS version 9.4 software (SAS Institute Inc., Cary, NC), and used PROC GENMOD for all models. We estimated beta coefficients per 10 percentage point increase in UI recipiency rates. We used an auto-regressive working correlation structure for overall estimates and for models testing differences by unemployment rate, and a compound symmetric correlation structure in models testing subgroup differences.
RESULTS
The mean recipiency rate over the study period for regular UI programs was 35.1 (SD=12.4, IQR: 26.1–42.4), and for all programs was 35.0 (SD=11.6, IQR: 26.2–42.0; 2008–2013 only). Variations in means and distributions of recipiency rates for regular and all programs from 2000–2015 are shown in Figure 2. In Figure 3 we present trends in the mean state quarterly suicide rate, UI recipiency rate, total unemployment rate, and insured unemployment rate (UI beneficiaries as a percentage of the total workforce) from 2000–2015. The mean total suicides per state-quarter was 142 (SD=138, IQR: 47–183). Of the 462,156 suicide deaths among 18–64 year-olds from 2000–2015 in the U.S., 58% were among those with a high school education or less, 78% were among men, and 90% were among non-Hispanic White Americans; the age group with the highest suicide rate were those 45–54 years of age (Supplemental Table 1).
Figure 2:
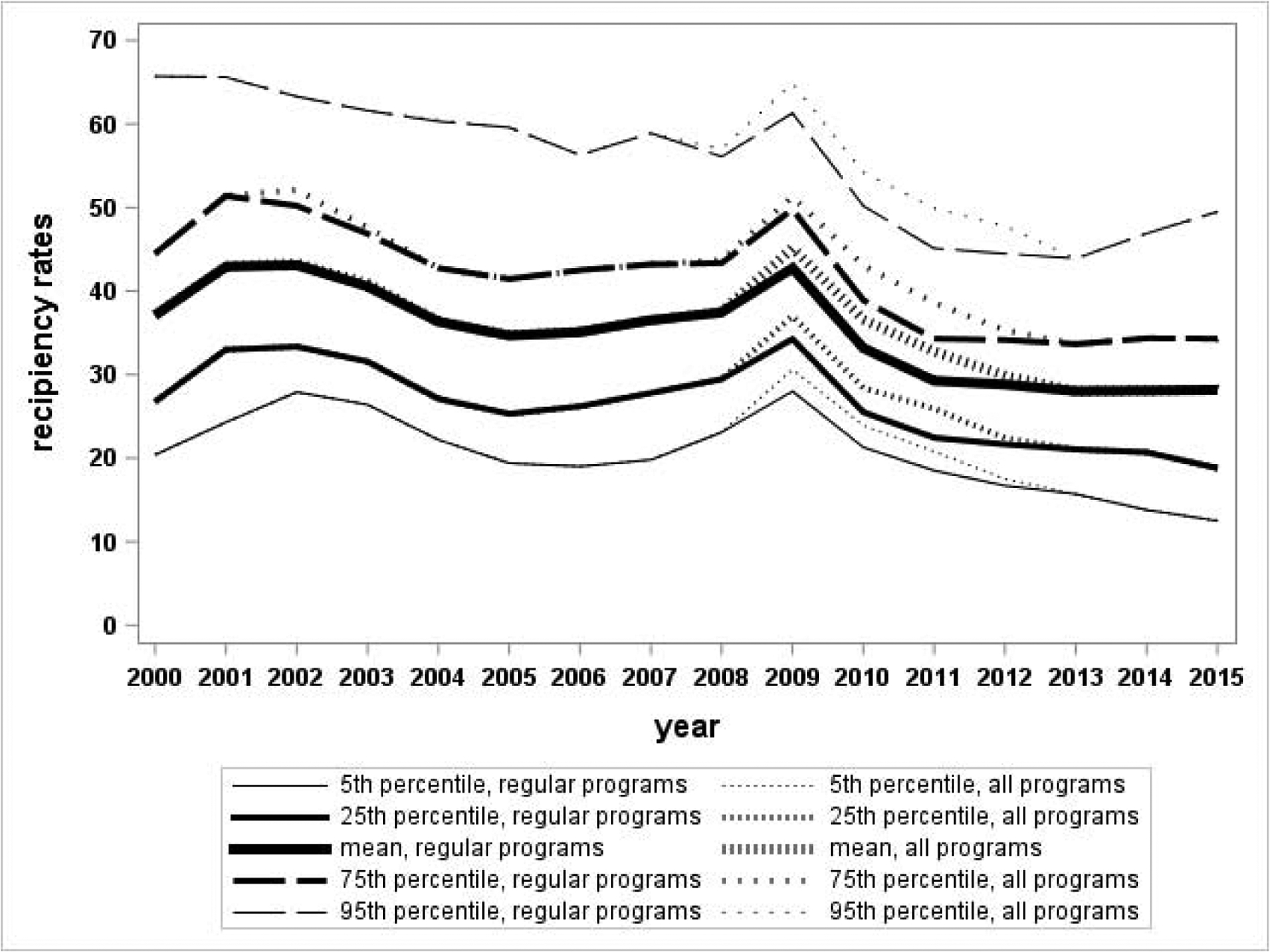
Distribution of annual state recipiency rates for regular and all unemployment insurance programs, 2000–2015 (5th, 25th, mean, 75th, and 95th percentiles)
Note: The recipiency rate reflects the percentage of unemployed individuals who receive unemployment insurance. Regular programs include state UI, UCFE, and UCX. All programs include emergency programs and extended benefit programs in addition to regular programs.
Figure 3:
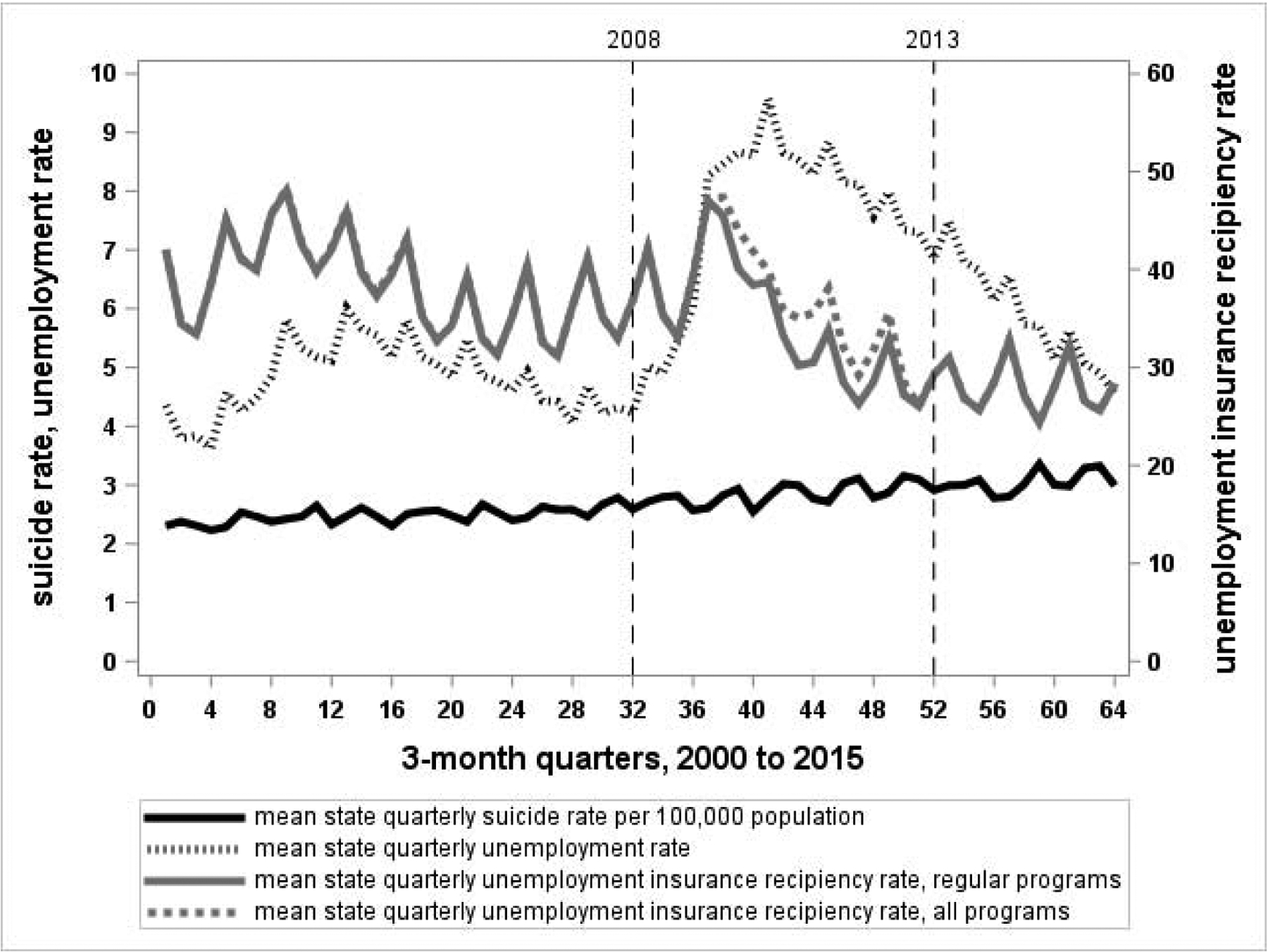
Mean state quarterly rates of suicide, unemployment, and unemployment insurance recipiency
Regular Programs (2000–2015, Table 1):
Table 1:
Beta estimates for the effect of regular and all unemployment insurance programs on suicide rates
| Regular UI programsa (2000–2015) | All UI programsb (2008–2013) | |||
|---|---|---|---|---|
| Bc | 95% confidence interval | Bc | 95% confidence interval | |
| Adults 18–64 | −0.009 | −0.041, 0.022 | −0.018 | −0.051, 0.014 |
| Educational attainment | ||||
| ≤high school | −0.028 | −0.118, 0.064 | −0.043 | −0.207, 0.122 |
| some college | −0.055 | −0.120, 0.011 | −0.129 | −0.270, 0.013 |
| ≥college grad | 0.053 | −0.052, 0.158 | 0.008 | −0.133, 0.149 |
| Race | ||||
| Non-Hispanic White | −0.228 | −0.329, −0.128 | −0.224 | −0.460, 0.013 |
| All other groups | 0.122 | −0.017, 0.260 | 0.239 | −0.029, 0.507 |
| Gender | ||||
| Men | −0.120 | −0.188, −0.051 | −0.085 | −0.237, 0.068 |
| Women | 0.081 | 0.016, 0.146 | −0.011 | −0.150, 0.128 |
| Age (years) | ||||
| 18–24 | 0.152 | 0.059, 0.245 | 0.227 | 0.027, 0.427 |
| 25–34 | −0.015 | −0.081, 0.051 | −0.021 | −0.166, 0.124 |
| 35–44 | −0.019 | −0.084, 0.046 | −0.051 | −0.186, 0.084 |
| 45–54 | −0.107 | −0.174, −0.040 | −0.146 | −0.291, −0.001 |
| 55–64 | −0.147 | −0.227, −0.067 | −0.136 | −0.309, 0.037 |
Regular Programs includes State UI, UCFE, and UCX. Estimates are expressed per 10 percentage point increase.
All Programs includes Emergency programs and Extended Benefit programs in addition to regular programs. Estimates are expressed per 10 percentage point increase.
Models include terms for state, year, and quarter (Jan-Mar, Apr-Jun, Jul-Sep, Oct-Dec) fixed effects, state specific linear (state*year) and quadratic (state*year*year) time trends, state quarterly unemployment rate and minimum wage, state yearly gross state product, personal income, and number of Temporary Assistance for Needy Families recipients. Referent groups are strata with the largest number of suicides: high school or less for education, White for race, men for gender, and 45–54 years for age.
In fully adjusted models the estimated effect of a 10 percentage point increase in the regular UI recipiency rate for 18–64 year-olds was null (β= −0.009, 95% CI: −0.041, 0.022), as was the estimated effect of the interaction between the UI recipiency rate and unemployment rate (β=0.002, 95% CI: −0.007, 0.011). Effect estimates appeared potentially protective for men (β= −0.120, 95% CI: −0.188, −0.051), White Americans (β= −0.228, 95% CI: −0.329, −0.128), 45–54 year-olds (β= −0.107, 95% CI: −0.174, −0.040), and 55–64 year-olds (β= −0.147, 95% CI: −0.227, −0.067), and potentially harmful for women (β=0.081, 95% CI: 0.016, 0.0146) and 18–24 year-olds (β=0.152, 95% CI: 0.059, 0.245). Effect estimates did not differ significantly by educational attainment, though point estimates were in the hypothesized negative direction for those with some college and those with a high school education or less. We found statistically significant differences by demographic subgroup for age (z=2.87, p=0.004 for 35–44 years compared to 45–54 years; z=4.61, p<0.0001 for 18–24 years compared to 45–54; z=2.48, p=0.01 for 25–34 years compared to 45–54), gender (z= 4.44, p<0.0001 for women compared to men), and race (z=4.12, p<0.0001 for all other groups compared to non-Hispanic White Americans). When not adjusting for potential confounding by season, effect estimates were more negative, i.e. appearing more protective against suicide (Supplemental Table 2).
All Programs (2008–2013):
The estimated effect on the suicide rate for 18–64 year-olds for all UI programs from 2008–2013, when emergency UI programs were in place in response to the Great Recession, was null (β= −0.018, 95% CI: −0.051, 0.014), as was the estimated effect of the interaction between the recipiency rate and unemployment rate (β=0.002, 95% CI: −0.007, 0.011). Compared to subgroup estimates for regular programs, effect estimates remained similar in magnitude and direction for all programs from 2008–2013, with the exception of the estimate for women, which was negative rather than positive. Fewer results for this metric remained statistically significant, likely in part due to the reduced sample size from restricting the analytical sample from 16 to 6 years.We observed statistically significant differences by age (z=3.32, p=0.0009 for 18–24 years compared to 45–54 years), and for race (z=2.88, p=0.004 for all other groups compared to non-Hispanic White Americans). When not adjusting for seasonality, effect estimates were more strongly negative (i.e. appeared more protective), and were stronger than for regular programs from 2000–2015.
DISCUSSION
We estimated a null overall effect of regular UI programs on the suicide rate among all 18–64 year-olds when adjusting for seasonality, but potentially protective effects for groups with higher suicide rates and higher UI recipiency rates including men, 45–64 year-olds, and non-Hispanic White Americans. Similar patterns held when examining all programs from 2008–2013, when state UI programs were supplemented by federal Unemployment Compensation Extension funds. Effect estimates for other groups were null or above the null. These differences in group estimates may result from differences in UI accessibility and suicide risk, and may be partly attributable to bias from data limitations.
UI programs can be measured in multiple dimensions including accessibility, ratio of benefits to lost wages, and benefit duration.21 Studies using different metrics may result in different policy implications, and direct comparisons may be difficult. We used the recipiency rate as it is a measure of accessibility that reflects eligibility requirements and program implementation, and is not affected by cost of living differences between states or years. State UI policies affect accessibility through requirements such as having worked a minimum number of hours and received a minimum amount of compensation at a prior job, actively seeking work, ability to begin work immediately, nature of job loss (i.e. involuntary, through no fault of the applicant), and type of job lost (e.g. typically not self-employed).6 In addition to policy, program administration can affect accessibility through the ease of the application process, availability of information and personnel to assist potential applicants, amount of time it takes to start benefits, and leniency of application reviewers.12, 13
A study by Cylus et al. did not find an effect of maximum UI benefits, defined as maximum weekly benefit multiplied by the maximum number of weeks, on annual suicide rates from 1968–2008.7 They did find a significant negative interaction between maximum UI benefits and the unemployment rate, suggesting that more generous UI programs may offset impacts of higher unemployment rates on increasing suicide rates. They did not find significant differences by gender or age. The discrepancy between Cylus et al.’s findings and our’s is likely due to our focus on accessibility rather than maximum benefit. Given the relatively low average recipiency rate during our study period (mean 35.1, SD=12.4 [Figure 2]), changes in the generosity of UI benefits may have little population-level effect on suicides, though individuals who actually receive UI may benefit.
Our effect estimates shifted upwards after adjusting for calendar quarter to account for potential confounding by season. Suicide rates tend to peak in spring, though drivers of this seasonality are not understood.19 Employment rates also vary seasonally in response to weather patterns and business cycles.20 We are unaware of published literature on whether and how seasonality of employment affects seasonality of suicide; seasonal unemployment variations could contribute to seasonal suicide variations. However, given the potential for confounding, we focus on results adjusted for season. A strength of the two-way fixed effects design is the ability to control for measured and unmeasured confounders.22 State fixed effects absorb state-specific time-invariant factors (e.g. relative generosity of state policies, demographic factors23 correlated with policies and suicide risk), and year fixed effects absorb time-varying factors common across states (e.g. federal policy changes, national suicide dynamics). We additionally adjust for state-specific time-varying factors to reduce the influence of unmeasured contemporaneous policies potentially confounding the UI-suicide relationship, though cross-state UI program generosity has been found to correlate very little over time or with other income maintenance programs.24 Our use of quarterly rather than annual UI recipiency rates also may reduce the chance of confounding by social or health policy changes co-occurring with UI policy changes. Quarterly data are also less likely to correlate with changes in state budgets, which are typically decided annually. However, using quarterly rather than annual data reduces the suicide count per unit of analysis, potentially reducing our ability to detect effects. While our study design does not focus on people experiencing unemployment, it captures potential effects among employed and unemployed individuals and their dependents. Some research has suggested that generous UI programs offer psychological benefits to employed individuals experiencing job insecurity through knowing that UI is available to buffer effects of income loss.21
Data limitations may have biased some group-specific effect estimates. While we used suicide rates based on group-specific counts and population estimates, our data for the overall UI recipiency rate and unemployment rate were not group-specific. Some group estimates may be affected by residual confounding from the unemployment rate and exposure mismeasurement from the UI recipiency rate. Results most likely to represent causal relationships are for groups for whom the group-specific UI recipiency rate and unemployment rate are well approximated by the overall UI recipiency rate and unemployment rate. In general, when unemployment increases, suicide and UI recipiency rates both increase, though not necessarily for the same groups. For groups with relatively low recipiency rates, we would expect a null relationship between the overall UI recipiency rate and the group-specific suicide rate. However, because these two factors tend to increase in response to higher unemployment, the UI-suicide relationship could be biased upwards due to residual confounding by unemployment for groups with group-specific unemployment rates poorly approximated by the overall unemployment rate.
By age, we observed the strongest potential protective effects for ages 55–64, followed by ages 45–54. Results were null but in the negative direction for ages 25–44, and above the null for ages 18–24. Adults 45–54 generally have the highest suicide rate, though research has shown that 55–64 year-olds experience the largest suicide increases during high unemployment periods, and thus may benefit more from UI.25 Longer unemployment duration has been found to increase suicide risk more than initial job loss,1 and older unemployed individuals experience more difficulty getting reemployed than younger job-seekers, with sharper wage declines once reemployed.26 The likelihood of applying for and receiving UI increases with age, while the unemployment rate decreases with age: a 2018 survey of unemployed persons who had worked in the past 12 months (a UI requirement) found that since their last job, 29% of those 55+ received UI compared to 3% of those 16–24.11 The percentage of UI applicants who received benefits also increased with age: 48% of 16–24 year-olds, 64% of 25–54 year-olds, and 78% of those 55+. Our findings support the notion that higher-risk adults with better access to the UI system may receive protection against suicide. With low UI recipiency rates, 18–24 year-olds as a group may not see much effect of higher UI recipiency, and in general have the lowest suicide risk. With higher than average unemployment rates, this group would be more likely to have residual confounding by unemployment, potentially explaining observed apparent harmful effect estimates for this group.
By broad race groups, we observed a potential protective effect for non-Hispanic White Americans, and a null but positive effect estimate for all others. Non-Hispanic White Americans comprised a majority of the U.S. population from 2000–2015 (69% in 2000,27 62% in 201528), and are likely to have group-specific UI recipiency and unemployment rates better approximated by the overall UI recipiency and unemployment rates. This group also comprised 90% of suicides in our data, precluding assessment of effect measure modification by more meaningful race groupings for those not in this category. The majority of the other races group were African American or Hispanic American, groups generally with higher unemployment and lower UI recipiency, and which would likely have more residual confounding and exposure mismeasurement from our use of the overall UI recipiency and unemployment rates. Near the height of the Great Recession in 2010, the unemployment rate was 16% for African Americans and 9% for non-Hispanic White Americans.29 UI recipiency rates in 2018 were approximately 18% for non-Hispanic White Americans, 14% for African Americans and Hispanic Americans, and 11% for Asian Americans.11 Non-Hispanic White Americans who applied for UI were more likely to receive UI benefits at 68%, compared to 61% of African Americans, 59% of Hispanic Americans, and 50% of Asian Americans. Thus, data limitations may explain why we observed a positive point estimate for the combined other races group.
We did not detect differences in effect estimates by educational attainment in fully-adjusted models. In models not adjusted for season, effect estimates appeared protective for regular UI programs for adults with some college and adults with a high school education or less, and null for adults with a college degree or more; these were stronger for all programs from 2008–2013. Individuals with lower educational attainment generally have higher rates of unemployment and suicide, and lower UI recipiency rates. An analysis of 2000–2014 data reported that those with a high school education or less saw the largest suicide increase during this time.30 Rates of more common outcomes including depression, suicidal thoughts, and attempted suicides are also higher among those with less education.31 However, UI recipiency rates increase with education: in 2018 the recipiency rate was 11% for those who did not complete high school, 20% for high school graduates, 23% for those with some college, and 30% for college graduates.11 Among UI applicants, those with more education were more likely to receive UI, with 75% of applicants with a college degree receiving UI compared to 52% of those who did not complete high school and 66% of high school graduates. Death certificate data on education may lead to some information bias, as these data may be misclassified for 28% of deaths.32
By gender, we observed an apparent protective effect of UI recipiency rates for men, and an apparent harmful effect among women for regular UI programs from 2000–2015; effect estimates were null but in the negative direction for both men and women for all programs from 2008–2013. Overall unemployment rates among men and women have been similar since the early 1980s, except during most economic recessions when men tend to have higher unemployment.33 Suicide rates are also nearly 4x higher among men than women in the U.S. Based on 2018 data, men are slightly more likely than women to receive UI benefits (18% compared to 15%).11 Research in Europe has found that increases in unemployment have had a greater effect on increasing suicides among men than among women.34 It is unclear why our effect estimates for women differ between regular (2000–2015) and all programs (2008–2013).
By age, gender, and race, we observed apparent protective effects for strata with higher suicide risks and higher UI recipiency rates. We did not see this pattern by educational attainment, where those with the highest suicide risk are least likely to receive UI. Applying for UI is a prerequisite for receiving UI, thus it is important to recognize potential barriers to application, especially for higher suicide risk groups, including those with lower educational attainment.9 Of surveyed unemployed individuals who had worked in 2017–2018 and who had not applied for UI, 59% did not believe they were eligible (e.g. type of job separation, insufficient past work, prior exhaustion of benefits), and 12% did not apply because of views about or perceived barriers to applying (e.g. did not know to apply, did not need the money, negative attitude about UI, problems with application process).11 Another study focused on barriers to access among low-wage and part-time workers found that while most met minimum income requirements for UI, primary barriers resulted from individuals assuming they were ineligible, and from non-monetary requirements.35 Low UI recipiency may have contributed to the observed null overall effect. As UI eligibility is designed to aid with short-term unemployment for recent job losses, another possible contributor to the null overall effect is that individuals with chronic mental and physical health conditions face both higher suicide risk and higher rates of long-term unemployment.36
We detected potential protective effects of higher unemployment insurance recipiency rates on suicide rates among men, adults ages 45–64, and non-Hispanic White Americans, all groups with higher than average suicide rates and higher UI recipiency rates. While the effects we estimate do not fully reflect the many factors shaping suicide risk, our findings may be meaningful at the population level. The COVID-19 pandemic has resulted in an unprecedented rapid increase in unemployment, and increases in depression have been reported.37 Even before COVID-19, >48,300 preventable suicide deaths occurred in the US in 2018,38 accounting for 8% of years of life lost before age 65.39 In addition to causing tremendous suffering to families and communities, suicide has a large economic cost; estimated lifetime medical and work loss costs associated with suicide in the U.S. in 2013 totaled $50–90 billion.40, 41 As population-level interventions with potential mental health benefits, social welfare polices may offer the benefit of not requiring individuals to be identified for treatment based on individual risk factors including mental illness, substance use, or gun ownership.1 Future work could improve on this analysis by using group-specific rates for unemployment and UI recipiency, estimating effects for more specific intersections of demographic characteristics, and from examining more common outcomes including suicide attempts, suicidal ideation, and depression.
Supplementary Material
Highlights.
First U.S. study on unemployment benefit accessibility and suicides during the Great Recession
Groups at higher suicide risk may be protected by higher unemployment insurance recipiency
Expanding access to unemployment insurance programs may offer protections against suicide
Sources of Funding:
This work was supported by the National Institutes of Health [R01MD010241, T32ES012870].
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of interest: None
REFERENCES
- 1.Classen TJ, Dunn RA. The effect of job loss and unemployment duration on suicide risk in the United States: a new look using mass-layoffs and unemployment duration. Health Econ. March 2012;21(3):338–350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Junna L, Moustgaard H, Huttunen K, Martikainen P. The Association Between Unemployment and Mortality: a Cohort Study of Workplace Downsizing and Closure. Am J Epidemiol. January 24 2020. [DOI] [PubMed] [Google Scholar]
- 3.Haw C, Hawton K, Gunnell D, Platt S. Economic recession and suicidal behaviour: Possible mechanisms and ameliorating factors. Int J Soc Psychiatry. February 2015;61(1):73–81. [DOI] [PubMed] [Google Scholar]
- 4.Blakely TA, Collings SCD, Atkinson J. Unemployment and suicide. Evidence for a causal association? Journal of epidemiology and community health. 2003;57(8):594–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gigante ECMH, Martin AL. CARES Act Expands Unemployment Insurance Benefits. The National Law Review. 2020. [Google Scholar]
- 6.Whitaker JMIK. Unemployment Insurance: Programs and Benefits. Congressional Research Service Report No. RL33362. 2019. [Google Scholar]
- 7.Cylus J, Glymour MM, Avendano M. Do generous unemployment benefit programs reduce suicide rates? A state fixed-effect analysis covering 1968–2008. Am J Epidemiol. July 1 2014;180(1):45–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Norström T, Grönqvist H. The Great Recession, unemployment and suicide. Journal of Epidemiology and Community Health. 2015;69(2):110–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Phillips JA, Hempstead K. Differences in US Suicide Rates by Educational Attainment, 2000–2014. American Journal of Preventive Medicine. October 2017;53(4):E123–E130. [DOI] [PubMed] [Google Scholar]
- 10.Bureau of Labor Statistics. Unemployment rates and earnings by educational attainment, 2018. U.S. Department of Labor, Bureau of Labor Statistics. Available at: https://www.bls.gov/emp/chart-unemployment-earnings-education.htm.
- 11.Bureau of Labor Statistics. Characteristics of Unemployment Insurance Applicants and Benefit recipiencts, 2018. : United States Department of Labor; 2019. [Google Scholar]
- 12.W V. Unemployment Insurance: Problems and Prospects 2011.
- 13.Wittenburg DCFM, Stapleton D, Scrivner S, Tucker A. Literature Review and Empirical Analysis of Unemployment Insurance Recipiency Ratios. In: The Lewin Group ftDoRaPotUSDoLUIS, ed; 1999. [Google Scholar]
- 14.McHugh RKW. How Low Can We Go? State Unemployment Insurance Programs Exclude Record Numbers of Jobless Workers Economic Policy Institute; 2015. [Google Scholar]
- 15.Employment and Training Administration, U.S. Department of Labor. Unemployment Insurance Data. Available at: https://oui.doleta.gov/unemploy/data_summary/DataSum.asp.
- 16.Isaacs KPWJ. Emergency Unemployment Compensation (EUC08): Status of Benefits Prior to Expiration. Congressional Research Service Report No. R42444 2014. [Google Scholar]
- 17.Sarah Flood MK, Renae Rodgers, Steven Ruggles, and Warren J. Robert. Integrated Public Use Microdata Series, Current Population Survey: Version 6.0 [dataset]. In: IPUMS, ed. Minneapolis, MN; 2018. [Google Scholar]
- 18.Vroman W. Low Benefit Recipiency in State Unemployment Insurance Programs: The Urban Institute; 2001. [Google Scholar]
- 19.Woo J-M, Okusaga O, Postolache TT. Seasonality of suicidal behavior. International journal of environmental research and public health. 2012;9(2):531–547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Geremew MGF. Seasonal and business cycles of U.S. employment. Economic Perspectives. 2018;42(3). [Google Scholar]
- 21.O’Campo P, Molnar A, Ng E, et al. Social welfare matters: a realist review of when, how, and why unemployment insurance impacts poverty and health. Soc Sci Med. May 2015;132:88–94. [DOI] [PubMed] [Google Scholar]
- 22.Wing C, Simon K, Bello-Gomez RA. Designing Difference in Difference Studies: Best Practices for Public Health Policy Research. Annual Review of Public Health. 2018/April/01 2018;39(1):453–469. [DOI] [PubMed] [Google Scholar]
- 23.Ivey-Stephenson AZ CA, Jack SP, Haileyesus T, Kresnow-Sedacca M. Suicide Trends Among and Within Urbanization Levels by Sex, Race/Ethnicity, Age Group, and Mechanism of Death — United States, 2001–2015. MMWR Surveill Summ. 2017(66(No. SS-18):1–16). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fishback P, Allen S, Fox J, Livingston B. A Patchwork Safety Net: A Survey of Cliometric Studies of Income Maintenance Programs in the United States in the First Half of the Twentieth Century. National Bureau of Economic Research, Inc, NBER Working Papers; December/01 2010;24. [Google Scholar]
- 25.Lin Y-H, Chen W-Y. Does unemployment have asymmetric effects on suicide rates? Evidence from the United States: 1928–2013. Economic Research-Ekonomska Istraživanja; 2018/January/01 2018;31(1):1404–1417. [Google Scholar]
- 26.Johnson RW Mommaerts C. Age differences in job loss, job search, and reemployment. 2100 M Street, N.W., Washington, D.C. 20037: The Urban Institute; 2011. [Google Scholar]
- 27.U.S. Census Bureau. U.S. Summary: 2000 - Census 2000 Profile: U.S. Department of Commerce, Economics and Statistics Administation, U.S. Census Bureau; 2002. [Google Scholar]
- 28.U.S. Census Bureau. 2015: American Community Survey Demographic and Housing Estimates.
- 29.Bureau of Labor Statistics. Unemployment rates by race and ethnicity, 2010. In: Labor USDo, ed; 2010. [Google Scholar]
- 30.Phillips JA, Hempstead K. Differences in U.S. Suicide Rates by Educational Attainment, 2000–2014. Am J Prev Med. October 2017;53(4):e123–e130. [DOI] [PubMed] [Google Scholar]
- 31.Center for Behavioral Health Statistics and Quality. 2017 National Survey on Drug Use and Health: Detailed Tables: Substance Abuse and Mental Health Services Administration, Rockville, MD; 2018. [Google Scholar]
- 32.Rostron BL, Boies JL, Arias E. Education reporting and classification on death certificates in the United States. Vital Health Stat 2. May 2010(151):1–21. [PubMed] [Google Scholar]
- 33.Hout MCE. The Labor Force and the Great Recession. Stanford, CA: Stanford Center on Poverty and Inequality; 2012. [Google Scholar]
- 34.Antonakakis N, Collins A. The impact of fiscal austerity on suicide: on the empirics of a modern Greek tragedy. Soc Sci Med. July 2014;112:39–50. [DOI] [PubMed] [Google Scholar]
- 35.Shaefer HL. Identifying Key Barriers to Unemployment Insurance for Disadvantaged Workers in the United States. Journal of Social Policy. 2010;39(3):439–460. [Google Scholar]
- 36.Agerbo E. Effect of psychiatric illness and labour market status on suicide: a healthy worker effect? J Epidemiol Community Health. July 2005;59(7):598–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Network Open. 2020;3(9):e2019686–e2019686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.U.S. Centers for Disease Control and Prevention. Leading Causes of Death and Injury, 2018. In: National Vital Statistics System NCfHS, ed; 2020. [Google Scholar]
- 39.U.S. Centers for Disease Control and Prevention. WISQARS Years of Potential Life Lost (YPLL) Report, 1981 – 2018. In: U.S. Centers for Disease Control and Prevention NCfIPaC, ed. Atlanta, GA; 2020. [Google Scholar]
- 40.Florence C, Simon T, Haegerich T, Luo F, Zhou C. Estimated Lifetime Medical and Work-Loss Costs of Fatal Injuries--United States, 2013. MMWR Morb Mortal Wkly Rep. October 2 2015;64(38):1074–1077. [DOI] [PubMed] [Google Scholar]
- 41.Shepard DS, Gurewich D, Lwin AK, Reed GA Jr, Silverman MM. Suicide and Suicidal Attempts in the United States: Costs and Policy Implications. Suicide and Life-Threatening Behavior. 2016;46(3):352–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.