

Abstract
Prior studies have investigated sperm retrieval rates in men with nonobstructive azoospermia (NOA) secondary to specific etiologies, yet most cases of NOA are idiopathic. We compared sperm retrieval rates and testicular histopathology in idiopathic NOA (iNOA) and nonidiopathic NOA (niNOA). We performed a retrospective review of men with NOA who underwent microdissection testicular sperm extraction (microTESE) between 2000 and 2016. Men with no history of malignancy or cryptorchidism and negative genetic evaluation were considered idiopathic. Multivariable regression determined the association between idiopathic etiology and primary outcomes of sperm retrieval and active spermatogenesis on histopathology. Among 224 men, 86 (38.4%) were idiopathic, 75 (33.5%) were nonidiopathic, and 63 (28.1%) did not undergo genetic testing. Median age and serum testosterone were higher among iNOA or no testing versus niNOA. Median follicle-stimulating hormone (FSH) was lower among iNOA or no testing versus niNOA. A higher proportion of iNOA or no testing versus niNOA had a clinical varicocele. Sperm retrieval rates were similar between iNOA, niNOA, and no testing (41.8% vs 48.0% vs 55.6%, respectively; P = 0.255). Active spermatogenesis was seen in a higher proportion of iNOA or no testing versus niNOA (31.4% and 27.0% vs 16.0%, P = 0.073). On multivariable analysis, iNOA was not associated with sperm retrieval or spermatogenesis (P = 0.430 and P = 0.078, respectively). Rates of sperm retrieval and spermatogenesis on testis pathology were similar in men with iNOA and niNOA. These data will be useful to clinicians in preoperative counseling for men with NOA and negative genetic evaluation.
Keywords: microdissection testicular sperm extraction, nonobstructive azoospermia, sperm retrieval rate
INTRODUCTION
Infertility affects 8%–12% of couples worldwide, and 40%–50% of infertile couples have a male factor.1 Approximately 5%–10% of these men are azoospermic, more than half of whom have nonobstructive azoospermia (NOA).2,3 Men with NOA may have primary spermatogenic failure due to a specific, identifiable cause such as genetic (Y chromosomal microdeletions and Klinefelter syndrome), congenital (cryptorchidism), postinfectious (mumps orchitis), gonadotoxic (radiotherapy, chemotherapy), or traumatic insult.4 However, a substantial proportion of men with NOA have no identifiable etiology, rendering these patients idiopathic.5
Regardless of etiology, microdissection testicular sperm extraction (microTESE) has emerged as the gold standard treatment for men with NOA. Testicular heterogeneity in these patients offers the possibility of sperm retrieval from small foci of active spermatogenesis, which can facilitate biological fatherhood through in vitro fertilization (IVF) with intracytoplasmic sperm injection (ICSI). Given the potential morbidity of a microTESE procedure, many studies have aimed to identify factors predictive of sperm retrieval in men with NOA, an inherently heterogenous group, to facilitate preoperative patient counseling regarding expectations and postoperative outcomes.6,7,8 While clinical and laboratory variables such as testicular volume, preoperative follicle-stimulating hormone (FSH), and testosterone are not strongly associated with successful sperm retrieval, multiple studies have characterized the prognostic significance of certain genetic abnormalities.9,10,11,12 Sperm retrieval rate (SRR) can be reliably predicted in men with specific etiologies of NOA such as karyotype abnormalities (i.e., Klinefelter syndrome) or azoospermic factor c (AZFc) deletions, which are associated with better SRR. In contrast, other genetic mutations such as AZFa and AZFb deletions harbor very poor prognosis.13,14,15,16 These data are useful to inform patients regarding the potential benefit of microTESE, an important element of preoperative counseling.
However, a substantial proportion of men with NOA have an idiopathic etiology (iNOA).5 While the rates of iNOA vary according to the definition of idiopathic across the literature, even when the most expansive definitions are utilized, approximately 22% of men with NOA will be idiopathic.17 Given the paucity of data characterizing SRR in men with iNOA, there is an inability to appropriately counsel these men regarding potential outcomes of microTESE. We sought to determine the SRR for men with iNOA at a single institution and identify prognostic factors associated with improved outcomes.
PATIENTS AND METHODS
Patient population
We performed a retrospective review of all men with NOA who underwent microTESE between 2000 and 2016 at Northwestern Memorial Hospital (Chicago, IL, USA). Semen analysis was performed according to the World Health Organization (WHO) 2010 guidelines.18 A 5 μl specimen was placed in 20-μl chamber to examine the specimen at ×200 magnification. A minimum of two fields were examined for each specimen. If no sperm was visualized, the specimen was further centrifuged and the pellet was examined for sperm at ×200 magnification. Nonobstructive etiology was determined according to the hormonal evaluation based on previously suggested cutoffs.19
Men were classified as iNOA if they had no history of malignancy or cryptorchidism, and genetic evaluation was negative for Y-chromosome and complete karyotype (46 chromosome) abnormalities. Men who did not undergo genetic evaluation were considered separately. Demographic and clinical variables including age, preoperative testosterone, and FSH were abstracted.
All microTESE procedures were performed by a single surgeon. The procedure has been described previously.20 In brief, a mid-pole transverse testicular incision in the tunica albuginea was utilized to open and subsequently expose the testicular parenchyma. Using the operating microscope (Leica Microcystems M500-N, Wetzlar, Germany), systematic microdissection was performed, and targeted tissue was processed for intraoperative microscopic evaluation with a phase-contrast microscope (Leica Microcystems DMLB) at ×200 and ×400 magnification. When spermatozoa were identified intraoperatively, further tissue processing was performed before cryopreservation in the laboratory. All men underwent intraoperative testis biopsy for formal pathological analysis. Pathological diagnosis was determined by an experienced genitourinary pathologist and categorized as active spermatogenesis, hypospermatogenesis, maturation arrest (MA), Sertoli cell-only pattern, or atrophy/fibrosis.
Primary outcome and statistical analyses
The primary outcome was successful sperm retrieval. The secondary outcome was spermatogenesis (active or hypospermatogenesis) on testis histopathology. The Chi-square test was used to determine the association between etiology of NOA and the outcomes of interest. Multivariable logistic regression was used to determine the factors associated with sperm retrieval and spermatogenesis on histopathology. Statistical significance for all testing was determined at a P = 0.05. All statistical analyses were performed using Stata version 13.0 (StataCorp, College Station, TX, USA). Northwestern University Institutional Review Board (IRB) approval was obtained with waiver of consent given the low risk of harm from study participation (protocol #STU00206101). A waiver of written consent and Health Insurance Portability and Accountability Act (HIPAA) authorization was also granted for retrospective analysis.
RESULTS
Patient characteristics
The total cohort consisted of 224 patients with NOA; 75 (33.5%) nonidiopathic NOA (niNOA), 86 (38.4%) iNOA, and 63 (28.1%) did not have genetic evaluation and thus could not be considered in either category. niNOA etiologies included history of malignancy (n = 30, 40.0%), genetic abnormality (n = 28, 37.3%), and history of cryptorchidism (n = 15, 20.0%). Two patients (2.7%) had both cryptorchidism and malignancy.
Patient characteristics are presented in Table 1. Median age was significantly higher among men with iNOA (34 years, interquartile range [IQR]: 31–39 years) or no testing (35 years, IQR: 32–38 years)versusniNOA (32 years, IQR: 29–35 years), P = 0.001. Median serum testosterone (ng dl−1) was higher among men with iNOA (365, IQR: 307–477) or no testing (378, IQR: 320–464)versusniNOA (343, IQR: 240–421) (P = 0.016). Median FSH (in mIU ml−1) was lower among men with iNOA (20.2, IQR: 10.3–26.8) or no testing (16.2, IQR: 6.2–24.9)versusniNOA (24.1, IQR: 15.1–31.2) (P = 0.003). A higher proportion of men with iNOA or no testingversusniNOA had a clinical varicocele (15.1% and 23.8% vs 5.3%, P = 0.008).
Table 1.
Patient characteristics of men with nonobstructive azoospermia who underwent microdissection testicular sperm extraction
| Characteristics | Nonidiopathic | Idiopathic | No testing | P* |
|---|---|---|---|---|
| Total, n (%) | 75 (33.5) | 86 (38.4) | 63 (28.1) | |
| Malignancy | 30 (40.0) | 0 (0) | 0 (0) | <0.001 |
| Cryptorchidism | 15 (20.0) | 0 (0) | 0 (0) | <0.001 |
| Genetic abnormality | 28 (37.3) | 0 (0) | – | <0.001 |
| Multiple | 2 (2.7) | 0 (0) | 0 (0) | 0.135 |
| Age (year), median (IQR) | 32 (29–35) | 34 (31–39) | 35 (32–38) | 0.001 |
| Serum T (ng dl−1), median (IQR) | 343 (240–421) | 365 (307–477) | 378 (320–464) | 0.016 |
| Serum FSH (mIU ml−1), median (IQR) | 24.1 (15.1–31.2) | 20.2 (10.3–26.8) | 16.2 (6.2–24.9) | 0.003 |
| Varicocele, n (%) | 4 (5.3) | 13 (15.1) | 15 (23.8) | 0.008 |
*Chi-squared test comparing all three groups, where applicable. IQR: interquartile range; T: testosterone; FSH: follicle stimulating hormone; –: not applicable
Sperm retrieval and testicular histopathology
Sperm retrieval rates were similar among men with iNOA, niNOA, and no testing (41.8% vs 48.0% vs 55.6%, respectively; P = 0.255). On multivariate analysis, none of the aforementioned variables – etiology (niNOA as reference; P = 0.430 for iNOA and P = 0.374 for no testing), testosterone (P = 0.267), FSH (P = 0.796), and varicocele (P = 0.982) – were associated with sperm retrieval.
Distribution of testis histopathology is presented in Figure 1, and sperm retrieval rates according to the etiology of NOA and testis histopathology are presented in Figure 2. Spermatogenesis was seen in a higher proportion of men with iNOA or no testingversusniNOA, approaching but not reaching significance (31.4% and 27.0% vs 16.0%, P = 0.073). However, on multivariable analysis, etiology of NOA was not associated with spermatogenesis on testicular histopathology (niNOA as reference; P = 0.078 for iNOA and P = 0.237 for no testing).
Figure 1.
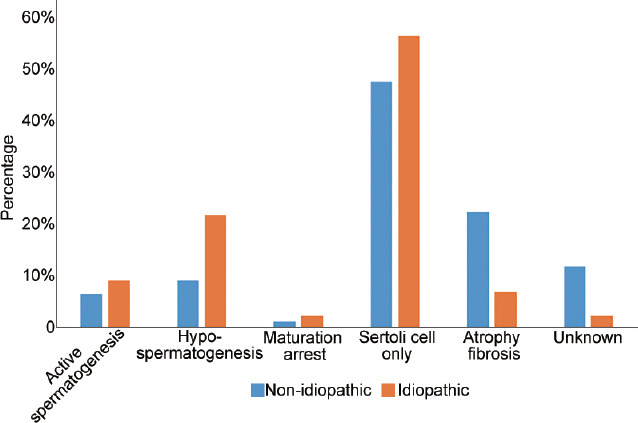
Testicular histopathology in men with azoospermia who underwent microdissection testicular sperm extraction.
Figure 2.
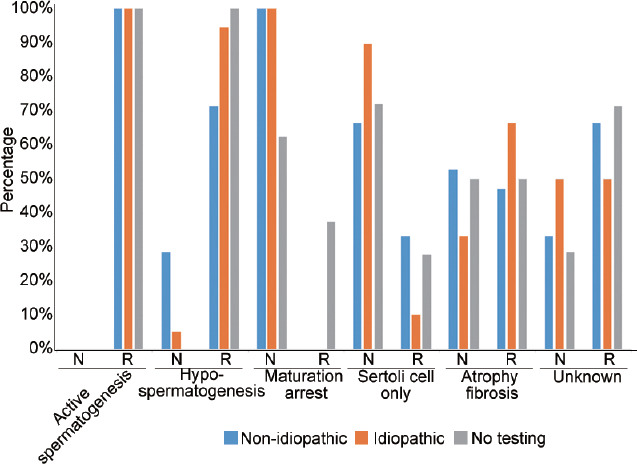
Success of sperm retrieval according to etiology of nonobstructive azoospermia and testicular histopathology. N: no retrieval; R: retrieval.
DISCUSSION
Before the development of TESE, NOA was a clinical condition with limited treatment options. The advent of microTESE, along with the arrival of IVF/ICSI, rendered it possible for men with NOA to father biological children.20 Since then, microTESE has emerged as the gold standard for the treatment of men with NOA.
Owing to the significant potential morbidity of microTESE, it is critical that men be informed of the likelihood of success to determine the tradeoff between the potential risks and benefits of the procedure. Testicular pain, injury, and, in rare circumstances, atrophy are all potential complications. Schlegel and Su21 demonstrated that 82% of men had ultrasonographic evidence of inflammation or hematoma formation at the site of biopsy 3 months after conventional TESE, two of whom had impaired testicular blood flow. While hematoma is less likely with microTESE, microTESE is still associated with a risk of bleeding and damage to testicular tissue.22 Postoperative hypogonadism is also an important concern as a recent systematic review found that a significant, albeit transient, drop in total testosterone occurs within 6 months after the procedure.23 Weighing these complications against the potential benefit of microTESE is an important aspect of preoperative counseling. For example, men with AZFa and AZFb deletions, in whom successful sperm retrieval has never been reported, would not be good candidates for surgery.
We found that SRR in iNOA was similar to those in niNOA. For comparison, we abstracted estimates of SRR for iNOA from other series in the literature, many of which did not expressly report SRR for the iNOA cohort (Table 2). The mean SRR across 15 studies was 37.9% (range 9.1%–50.1%), which is similar to the present findings.5,9,16,24,25,26,27,28,29,30,31,32,33,34,35 The heterogeneity among these studies can be explained by the inconsistent definition of iNOA. Only seven studies evaluated patients for Y chromosome microdeletions, while the remaining studies identified patients with 46, XY karyotypes as idiopathic.5,16,28,29,33,34,35 We utilized a more stringent definition of iNOA, including only those men who had both karyotype and Y chromosome microdeletion testing, which must be considered when using these data to counsel patients in the preoperative setting.
Table 2.
Rates of sperm retrieval in idiopathic nonobstructive azoospermia as reported in the literature
| Author | Year | Patients (n) | Retrieval rate (%) | Testing and definition for idiopathic | ||
|---|---|---|---|---|---|---|
| XXY | Y microdeletion | Other causes | ||||
| Tsujimura and Matsumiya9 | 2004 | 100 | 41 | x | – | – |
| Ishikawa et al.24 | 2009 | 100 | 41 | x | – | – |
| Yarali et al.25 | 2009 | 113 | 44 | x | – | – |
| Stahl et al.16 | 2010 | 385 | 48.8 | x | x | – |
| Bakircioglu et al.26 | 2011 | 379 | 50 | x | – | – |
| Arafa et al.28* | 2015 | 97 | 45.4 | x | x | x |
| Arafa et al.28** | 2015 | 22 | 9.1 | x | x | x |
| Sabbaghian et al.27 | 2014 | 537 | 22.2 | x | – | – |
| Enatsu et al.29 | 2016 | 194 | 21.1 | x | x | |
| Alfano et al.5 | 2017 | 47 | 49 | x | x | x |
| Iwatsuki et al.31 | 2017 | 172 | 26.2 | x | – | – |
| Takeda et al.32 | 2017 | 144 | 27.1 | x | – | – |
| Binsaleh et al.30 | 2017 | 138 | 41.3 | x | – | – |
| Klami et al.33 | 2018 | 65 | 31 | x | x | x |
| Ozkanli et al.34 | 2018 | 70 | 47.1 | x | x | x |
| Johnson et al.35 | 2019 | 423 | 50.1 | x | x | – |
*Nonfamilial idiopathic NOA; **familial idiopathic NOA. x: patients tested and evaluated for this condition were included in the study and considered “idiopathic”; –: patients were not tested or evaluated for this condition in the study when defining “idiopathic”; NOA: nonobstructive azoospermia
These data can be useful in preoperative counseling before microTESE. In our cohort, over one-third of men did not have an identifiable etiology of NOA, which is likely an underestimate owing to the substantial proportion of men without genetic testing. For these men with iNOA, the present data can be useful in setting expectations regarding success of sperm retrieval with microTESE.
Beyond specific etiologies for NOA, testicular histology is perhaps the best predictor of successful or unsuccessful microTESE.36,37,38,39 While preoperative testicular biopsy in clinical practice has limited utility, the presence of active spermatogenesis on intraoperative biopsy is strongly correlated with successful sperm extraction.6 In our cohort, men with iNOA had a higher incidence of active spermatogenesis compared to niNOA, although the difference was not statistically significant (31.4% vs 16.0%, P = 0.07). While it remains impractical to perform a diagnostic biopsy before a microTESE when preoperative evaluation is sufficient for accurate diagnosis, diagnostic biopsy at the time of the initial microTESE for iNOA may provide prognostic evidence as to whether repeat microTESE would be reasonable.19
Our study must be interpreted within the context of limitations in study design. First, this is a retrospective study that is subject to the typical biases of such analyses. Second, we did not exclude patients with varicoceles from the analysis, nor did we consider varicocele as a distinct etiology for NOA. That is, men with varicocele could be considered idiopathic, despite the presence of pathology that could impair semen parameters. While there are limited data to suggest that varicocele repair in men with NOA can improve SRR, this does not necessarily imply that varicocele alone is a sufficient etiology for NOA in the absence of other identifiable abnormalities.40 Nonetheless, a greater proportion of men in the iNOA and no testing cohorts had varicoceles compared with the niNOA cohort, which does raise the possibility of varicocele as a distinct etiology for NOA that should be considered separately. Third, as is the case at most institutions, we did not routinely perform tissue digestion in cases where no spermatozoa were identified intraoperatively, which in one retrospective series led to additional sperm identification in 7% of cases.41 However, a thorough, microdissection approach was utilized in all cases with meticulous intraoperative assessment of all tissue samples.
CONCLUSIONS
In a retrospective analysis of men with NOA who underwent microTESE, the rates of sperm retrieval and spermatogenesis on testicular pathology were similar in men with iNOA and niNOA. These data will be useful to patients and clinicians in preoperative counseling for men with NOA and negative genetic evaluation.
AUTHOR CONTRIBUTIONS
AD performed the literature review and synthesis, and helped to draft the manuscript. JAH helped with conception of the study, performed the statistical analysis, and helped with the initial draft and critical revision of the manuscript. ALDB and MP assisted with the literature synthesis, data interpretation, and critical revision of the manuscript. JW helped with conception of the study, data interpretation, and critical revision of the manuscript. MKK helped with statistical analysis, data interpretation, and critical revision of the manuscript. REB helped the conception of the study, oversight, and critical revision of the manuscript. All authors read and approved the final manuscript.
COMPETING INTERESTS
All authors declared no competing interest.
REFERENCES
- 1.Kumar N, Singh AK. Trends of male factor infertility, an important cause of infertility: a review of literature. J Hum Reprod Sci. 2015;8:191–6. doi: 10.4103/0974-1208.170370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Practice Committee of the American Society for Reproductive Medicine. Management of nonobstructive azoospermia: a committee opinion. Fertil Steril. 2018;110:1239–45. doi: 10.1016/j.fertnstert.2018.09.012. [DOI] [PubMed] [Google Scholar]
- 3.Wosnitzer M, Goldstein M, Hardy MP. Review of azoospermia. Spermatogenesis. 2014;4:e28218. doi: 10.4161/spmg.28218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Esteves SC. Clinical management of infertile men with nonobstructive azoospermia. Asian J Androl. 2015;17:459–70. doi: 10.4103/1008-682X.148719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alfano M, Ventimiglia E, Locateli I, Capogrosso P, Cazzaniga W, et al. Anti-Mullerian hormone-to-testosterone ratio is predictive of positive sperm retrieval in men with idiopathic non-obstructive azoospermia. Sci Rep. 2017;7:17638. doi: 10.1038/s41598-017-17420-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Raheem A, Garaffa G, Rushwan N, De Luca F, Zacharakis E, et al. Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia. BJU Int. 2013;111:492–9. doi: 10.1111/j.1464-410X.2012.11203.x. [DOI] [PubMed] [Google Scholar]
- 7.Bernie AM, Ramasamy R, Schlegel PM. Predictive factors of successful microdissection testicular sperm extraction. Basic Clin Androl. 2013;23:5. doi: 10.1186/2051-4190-23-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cissen M, Meijerink AM, D'Hauwers KW, Meissner A, van der Weide N, et al. Prediction model for obtaining spermatozoa with testicular sperm extraction in men with non-obstructive azoospermia. Hum Reprod. 2016;31:1934–41. doi: 10.1093/humrep/dew147. [DOI] [PubMed] [Google Scholar]
- 9.Tsujimura A, Matsumiya K. Prediction of successful outcome of microdissection testicular sperm extraction in men with idiopathic nonobstructive azoospermia. J Urol. 2004;172:1944–7. doi: 10.1097/01.ju.0000142885.20116.60. [DOI] [PubMed] [Google Scholar]
- 10.Ramasamy R, Lin K, Gosden LV, Rosenwaks Z, Palermo GD, et al. High serum FSH levels in men with nonobstructive azoospermia does not affect success of microdissection testicular sperm extraction. Fertil Steril. 2009;92:590–3. doi: 10.1016/j.fertnstert.2008.07.1703. [DOI] [PubMed] [Google Scholar]
- 11.Ramasamy R, Trivedi NN, Reifsnyder JE, Palermo GD, Rosenwaks Z, et al. Age does not adversely affect sperm retrieval in men undergoing microdissection testicular sperm extraction. Fertil Steril. 2014;101:653–5. doi: 10.1016/j.fertnstert.2013.11.123. [DOI] [PubMed] [Google Scholar]
- 12.Bryson CF, Ramasamy R, Sheehan M, Palermo GD, Rosenwaks Z, et al. Severe testicular atrophy does not affect the success of microdissection testicular sperm extraction. J Urol. 2014;191:175–8. doi: 10.1016/j.juro.2013.07.065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ramasamy R, Ricci JA, Palermo GD, Gosden LV, Rosenwaks Z, et al. Successful fertility treatment for Klinefelter's syndrome. J Urol. 2009;182:1108–13. doi: 10.1016/j.juro.2009.05.019. [DOI] [PubMed] [Google Scholar]
- 14.Hopps CV, Mielnik A, Goldstein M, Palermo GD, Rosenwaks Z, et al. Detection of sperm in men with Y chromosome microdeletions of the AZFa, AZFb and AZFc regions. Hum Reprod. 2003;18:1660–5. doi: 10.1093/humrep/deg348. [DOI] [PubMed] [Google Scholar]
- 15.Friedler S, Raziel A, Schachter M, Strassburger D, Bern O, et al. Outcome of first and repeated testicular sperm extraction and ICSI in patients with non-obstructive azoospermia. Hum Reprod. 2002;17:2356–61. doi: 10.1093/humrep/17.9.2356. [DOI] [PubMed] [Google Scholar]
- 16.Stahl PJ, Masson P, Mielnik A, Marean MB, Schlegel PN, et al. A decade of experience emphasizes that testing for Y microdeletions is essential in American men with azoospermia and severe oligozoospermia. Fertil Steril. 2010;94:1753–6. doi: 10.1016/j.fertnstert.2009.09.006. [DOI] [PubMed] [Google Scholar]
- 17.Fedder J, Cruger D, Oestergaard B, Petersen GB. Etiology of azoospermia in 100 consecutive nonvasectomized men. Fertil Steril. 2004;82:1463–5. doi: 10.1016/j.fertnstert.2004.06.035. [DOI] [PubMed] [Google Scholar]
- 18.Cooper TG. World Health Organization Laboratory Manual for the Examination and Processing of Human Semen. Geneva: WHO Press; 2010. [Google Scholar]
- 19.Schoor RA, Elhanbly S, Niederberger CS, Ross LS. The role of testicular biopsy in the modern management of male infertility. J Urol. 2002;167:197–200. [PubMed] [Google Scholar]
- 20.Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision. Hum Reprod. 1999;14:131–5. doi: 10.1093/humrep/14.1.131. [DOI] [PubMed] [Google Scholar]
- 21.Schlegel PN, Su LM. Physiological consequences of testicular sperm extraction. Hum Reprod. 1997;12:1688–92. doi: 10.1093/humrep/12.8.1688. [DOI] [PubMed] [Google Scholar]
- 22.Deruyver Y, Vanderschueren D, Van der Aa F. Outcome of microdissection TESE compared with conventional TESE in non-obstructive azoospermia: a systematic review. Andrology. 2014;2:20–4. doi: 10.1111/j.2047-2927.2013.00148.x. [DOI] [PubMed] [Google Scholar]
- 23.Eliveld J, van Wely M, Meibner A, Repping S, van der Veen F, et al. The risk of TESE-induced hypogonadism: a systematic review and meta-analysis. Hum Reprod Update. 2018;24:442–54. doi: 10.1093/humupd/dmy015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ishikawa T, Yamaguchi K, Chiba K, Takenaka A, Fujisawa M. Serum hormones in patients with nonobstructive azoospermia after microdissection testicular sperm extraction. J Urol. 2009;182:1495–9. doi: 10.1016/j.juro.2009.06.029. [DOI] [PubMed] [Google Scholar]
- 25.Yarali H, Polat M, Bozdag G, Gunel M, Aplas I, et al. TESE-ICSI in patients with non-mosaic Klinefelter syndrome: a comparative study. Reprod Biomed Online. 2009;18:756–60. doi: 10.1016/s1472-6483(10)60023-5. [DOI] [PubMed] [Google Scholar]
- 26.Bakircioglu ME, Ulug U, Erden HF, Tosun S, Bayram A, et al. Klinefelter syndrome: does it confer a bad prognosis in treatment of nonobstructive azoospermia? Fertil Steril. 2011;95:1696–9. doi: 10.1016/j.fertnstert.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 27.Sabbaghian M, Modarresi T, Hosseinifar H, Hosseini J, Farrahu F, et al. Comparison of sperm retrieval and intracytoplasmic sperm injection outcome in patients with and without Klinefelter syndrome. Urology. 2014;83:107–10. doi: 10.1016/j.urology.2013.09.021. [DOI] [PubMed] [Google Scholar]
- 28.Arafa MM, ElBardisi HT, AlSaid SS, Majzoub A, AlMalki AH, et al. Outcome of microsurgical testicular sperm extraction in familial idiopathic nonobstructive azoospermia. Andrologia. 2015;47:1062–7. doi: 10.1111/and.12378. [DOI] [PubMed] [Google Scholar]
- 29.Enatsu N, Miyake H, Chiba K, Fujisawa M. Predictive factors of successful sperm retrieval on microdissection testicular sperm extraction in Japanese men. Reprod Med Biol. 2016;15:29–33. doi: 10.1007/s12522-015-0212-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Binsaleh S, Alhajeri D, Madbouly K. Microdissection testicular sperm extraction in men with nonobstructive azoospermia: experience of King Saud University medical city, Riyadh, Saudi Arabia. Urol Ann. 2017;9:136–40. doi: 10.4103/0974-7796.204188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Iwatsuki S, Sasaki S, Taguchi K, Hamakawa T, Mizuno K, et al. Effect of obesity on sperm retrieval outcome and reproductive hormone levels in Japanese azoospermic men with and without Klinefelter syndrome. Andrology. 2017;5:82–6. doi: 10.1111/andr.12281. [DOI] [PubMed] [Google Scholar]
- 32.Takeda T, Iwatsuki S, Hamakawa T, Mizuno K, Kamiya H, et al. Chromosomal anomalies and sperm retrieval outcomes of patients with non-obstructive azoospermia: a case series. Andrology. 2017;5:473–6. doi: 10.1111/andr.12338. [DOI] [PubMed] [Google Scholar]
- 33.Klami R, Mankonen H, Perheentupa A. Microdissection testicular sperm extraction in Finland – Results of the first 100 patients. Acta Obstet Gynecol Scand. 2018;97:53–8. doi: 10.1111/aogs.13243. [DOI] [PubMed] [Google Scholar]
- 34.Ozkanli S, Basar MM, Selimoglu S, Erol B, Ozkanli O, et al. The ghrelin and orexin activity in testicular tissues of patients with idiopathic non-obstructive azoospermia. Kaohsiung J Med Sci. 2018;34:564–8. doi: 10.1016/j.kjms.2018.04.001. [DOI] [PubMed] [Google Scholar]
- 35.Johnson M, Raheem A, De Luca F, Hallerstrom M, Zainal Y, et al. An analysis of the frequency of Y-chromosome microdeletions and the determination of a threshold sperm concentration for genetic testing in infertile men. BJU Int. 2019;123:367–72. doi: 10.1111/bju.14521. [DOI] [PubMed] [Google Scholar]
- 36.Jezek D, Knuth UA, Schulze W. Successful testicular sperm extraction (TESE) in spite of high serum follicle stimulating hormone and azoospermia: correlation between testicular morphology, TESE results, semen analysis and serum hormone values in 103 infertile men. Hum Reprod. 1998;13:1230–4. doi: 10.1093/humrep/13.5.1230. [DOI] [PubMed] [Google Scholar]
- 37.Ezeh UI, Taub NA, Moore HD, Cooke ID. Establishment of predictive variables associated with testicular sperm retrieval in men with non-obstructive azoospermia. Hum Reprod. 1999;14:1005–12. doi: 10.1093/humrep/14.4.1005. [DOI] [PubMed] [Google Scholar]
- 38.Tournaye H, Verheyen G, Nagy P, Ubaldi F, Goossens A, et al. Are there any predictive factors for successful testicular sperm recovery in azoospermic patients? Hum Reprod. 1997;12:80–6. doi: 10.1093/humrep/12.1.80. [DOI] [PubMed] [Google Scholar]
- 39.Su LM, Palermo GD, Goldstein M, Veeck LL, Rosenwaks Z, et al. Testicular sperm extraction with intracytoplasmic sperm injection for nonobstructive azoospermia: testicular histology can predict success of sperm retrieval. J Urol. 1999;161:112–6. [PubMed] [Google Scholar]
- 40.Esteves SC, Miyaoka R, Roque M, Agarwal A. Outcome of varicocele repair in men with nonobstructive azoospermia: systematic review and meta-analysis. Asian J Androl. 2016;18:246–53. doi: 10.4103/1008-682X.169562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ramasamy R, Reifsnyder JE, Bryson C, Zaninovic N, Liotta D, et al. Role of tissue digestion and extensive sperm search after microdissection testicular sperm extraction. Fertil Steril. 2011;96:299–302. doi: 10.1016/j.fertnstert.2011.05.033. [DOI] [PubMed] [Google Scholar]