

Abstract
Background
The Korean Society of Thoracic Radiology (KSTR) recently constructed a nation-wide coronavirus disease 2019 (COVID-19) database and imaging repository, referred to the Korean imaging cohort of COVID-19 (KICC-19) based on the collaborative efforts of its members. The purpose of this study was to provide a summary of the clinico-epidemiological data and imaging data of the KICC-19.
Methods
The KSTR members at 17 COVID-19 referral centers retrospectively collected imaging data and clinical information of consecutive patients with reverse transcription polymerase chain reaction-proven COVID-19 in respiratory specimens from February 2020 through May 2020 who underwent diagnostic chest computed tomography (CT) or radiograph in each participating hospital.
Results
The cohort consisted of 239 men and 283 women (mean age, 52.3 years; age range, 11–97 years). Of the 522 subjects, 201 (38.5%) had an underlying disease. The most common symptoms were fever (n = 292) and cough (n = 245). The 151 patients (28.9%) had lymphocytopenia, 86 had (16.5%) thrombocytopenia, and 227 patients (43.5%) had an elevated CRP at admission. The 121 (23.4%) needed nasal oxygen therapy or mechanical ventilation (n = 38; 7.3%), and 49 patients (9.4%) were admitted to an intensive care unit. Although most patients had cured, 21 patients (4.0%) died. The 465 (89.1%) subjects underwent a low to standard-dose chest CT scan at least once during hospitalization, resulting in a total of 658 CT scans. The 497 subjects (95.2%) underwent chest radiography at least once during hospitalization, which resulted in a total of 1,475 chest radiographs.
Conclusion
The KICC-19 was successfully established and comprised of 658 CT scans and 1,475 chest radiographs of 522 hospitalized Korean COVID-19 patients. The KICC-19 will provide a more comprehensive understanding of the clinical, epidemiological, and radiologic characteristics of patients with COVID-19.
Keywords: Coronavirus Infections; Radiography, Thoracic; Computed Tomography
Graphical Abstract
INTRODUCTION
Coronavirus disease 2019 (COVID-19) is an ongoing global emergency, and in October 2020 had resulted in 40 million cases and over one million deaths worldwide. Tremendous efforts have been and continue to be made in response to the COVID-19 pandemic in terms of epidemiology, diagnosis, treatment, and preventive measures. Nevertheless, the globe is being in the middle of the COVID-19 pandemic, and overcoming COVID-19 seems to take considerable time and resources, including a large multicenter database of COVID-19 patients to understand patients' characteristics in a wide spectrum of disease and to facilitate the development and validation of troubleshooting tools.
Radiology has remained at the center of patient' care since the COVID-19 outbreak began. Chest computed tomography (CT) is sensitive at detecting COVID-19 pneumonia though specificities vary between studies,1,2 and was used in the diagnosis of COVID-19 combined with clinico-epidermiological features in Wuhan where the use of reverse transcription-polymerase chain reaction (RT-PCR) is limited.3 Chest radiograph is less sensitive than chest CT4,5 but is useful to access the need for hospitalization in young to middle-aged patients,6 and to predict progression to critical illness.7 Chest imaging is recommended for managing COVID-19 patients with moderate to severe disease severities, to monitor disease progression and predict prognosis.8
The Korean Society of Thoracic Radiology (KSTR) has been much involved in professional activities designed to address the challenges posed by COVID-19 since February 2020, and also participates in academic research,1,4,9,10,11,12,13,14,15,16 shares representative cases,17,18 issues imaging guidelines,19 and provides COVID-19 education.20 In addition to these activities, the KSTR recently constructed a nation-wide COVID-19 database and imaging repository, referred to the Korean imaging cohort of COVID-19 (KICC-19) based on the collaborative efforts of its members. The purpose of this study was to provide a summary of the clinico-epidemiological data and imaging data of the KICC-19.
METHODS
Study population
The KSTR formed a task force team, consisting of 22 KSTR members including its board of directors, in March 2020, to determine the aims of KICC-19, to design the database and imaging repository, and to plan its future use. To build KICC-19, the task force team asked KSTR members in April to share details of anonymized COVID-19 cases voluntarily to help establish the KICC-19 registry. The inclusion criteria were consecutive patients with RT-PCR-proven COVID-19 in respiratory specimens who underwent diagnostic full inspiratory chest imaging, either by CT or radiograph, in each participating hospital. Seventeen researchers at 17 domestic institutions agreed to participate in this project, and most participating institutions were main referral centers for COVID-19 patients, and were located throughout the country. A total of 522 patients who were diagnosed having COVID-19 and admitted from February 2020 through May 2020 were included in the KICC-19 (Fig. 1).
Fig. 1. The number of patients with COVID-19 gathered at each institution.

COVID-19 = coronavirus disease 2019.
Data collection
To establish KICC-19, the 17 researchers retrospectively gathered imaging data and clinical information of the included patients. Radiographic data were Digital Imaging and Communications in Medicine (DICOM) images of frontal chest radiographs obtained at baseline, within 24 hours of chest CT examinations, and at discharge. We collected the thinnest axial DICOM images of chest CT examinations taken in the supine position between diagnosis and discharge, regardless of contrast enhancement and CT protocols.
Clinical information was collected using a standardized Excel form by reviewing electronic medical records. The collected items were determined by reviewing relevant publications about the outcomes of COVID-1921,22,23,24 and subsequent task force discussion, and included age, sex, epidemiological history, smoking history, comorbidities (e.g., hypertension, diabetes, coronary heart disease, chronic obstructive pulmonary disease, cancer, chronic kidney disease, and chronic liver disease), visiting sites, symptoms (fever, cough, dyspnea, and confusion), RT-PCR information (date and positivity), vital signs at admission, initial laboratory findings (white blood cells count, lymphocyte count, platelet count, total bilirubin, alanine aminotransferase, albumin, blood urea nitrogen, creatinine, lactate dehydrogenase, C-reactive protein, D-dimer, procalcitonin), treatment (fraction of inspired oxygen, medication), outcomes (acute respiratory distress syndrome, the necessity for intensive care, intubation, and extracorporeal membrane oxygenation), durations of hospital stay, and mortality. Other respiratory pathogens causing symptoms in all patients were evaluated through RT-PCR and sputum culture at admission.
Data repository
The KICC adopted the ISO 9001 certificated, encrypted cloud platform, Asan Image Metrics of Clinical Trial Center (AIM-Aicro), under the support of the KSTR and the Korean Society of Radiology for data management and researches. Imaging data were initially processed at local sites to remove institution names, patient names, and patient IDs to ensure anonymization, and were subsequently uploaded to the AIM-Aicro platform. Clinical information did not contain any data for personal identification at the time of data collection and was incorporated into electronic case report forms.
Ethics statement
This retrospective study was approved by the Institutional Review Boards of participating institutions (Seoul National University Hospital, 2004-122-1118; Kangbuk Samsung Hospital, KBSMC 2020-04-003; Soonchunhyang University Seoul Hospital, 2020-04-001; Jeonbuk National University Hospital, CUH 2020-04-021; Dankook University Hospital, 2020-05-023; Chungbuk National University Hospital, 2020-04-003; Kangwon National University Hospital, 2020-04-003; Keimyung University Dongsan Hospital, 2020-04-050; Chungnam National University Hospital, CNUH 2020-04-063; Daegu Fatima Hospital, DFE20ORIO063; Seoul St. Mary's Hospital, KC20RCDI0250; Kyungpook National University Hospital, KNUH202003023; Chonnam National University Hospital, CNUH-2020-123; Samsung Medical Center, SMC 2020-05-046-001; Seoul Medical Center, 2020-04-023; Yeungnam University Hospital, 2020-09-057; Pusan National University Hospital, H-2004-007-089) and the requirement for informed consent was waived.
RESULTS
Geographic distribution
Of the 522 patients, 77.8% (406 patients) were included from tertiary referral institutes, and 22.2% (116 patients) were included from secondary referral hospitals. The 86.8% of the patients were resided in one of the five major Korean metropolitan cities; 41.4% (216 patients) were from Daegu, which was much affected by the earliest outbreak, 15.3% (80 patients) were from Busan, and 14.8% (77 patients) were from Daejeon.
Clinical data
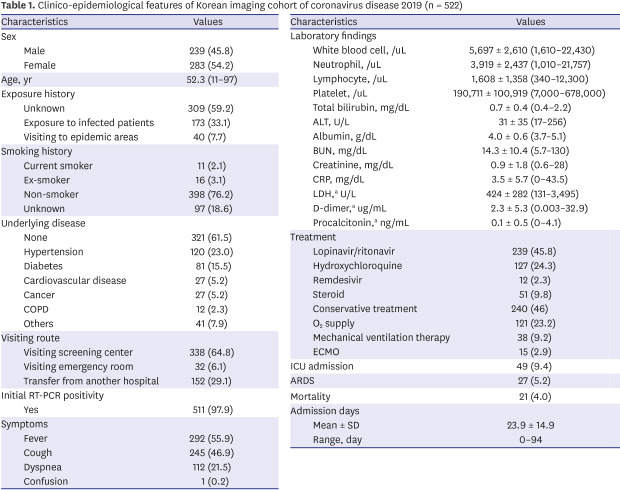
Table 1 presents a summary of the epidemiologic and clinical data of KICC-19. The cohort consisted of 239 men and 283 women. Mean age of the included patients was 52.3 ± 19.3 years (range, 11–97). Of the 522 study subjects, 11 patients were diagnosed between 1–18 days (mean ± standard deviation, 4.5 ± 5.7 days) after the negative initial RT-PCR results. The reasons for repeated RT-PCR were a recent history of exposure to COVID-19 infected patients (n = 6), visiting history of epidemic sites (n = 3), or prolonged symptoms (n = 2). Of the 522 study subjects, 201 (38.5%) had an underlying disease: hypertension (n = 120), diabetes (n = 81), cardiovascular disease (n = 27), or cancer (n = 27). The most common symptoms were fever (n = 292) and cough (n = 245). Of the 522 study subjects, 115 patients (22%) were asymptomatic. One hundred and fifty-one patients (28.9%) had lymphocytopenia, 86 had (16.5%) thrombocytopenia, and 227 patients (43.5%) had an elevated CRP at admission. Mean time interval between symptom onset and RT-PCR assay was 2.4 ± 2.1 days (range, 1–10 days). One patient was co-infected by Streptococcus pneumoniae at admission.
Table 1. Clinico-epidemiological features of Korean imaging cohort of coronavirus disease 2019 (n = 522).
| Characteristics | Values | |
|---|---|---|
| Sex | ||
| Male | 239 (45.8) | |
| Female | 283 (54.2) | |
| Age, yr | 52.3 (11–97) | |
| Exposure history | ||
| Unknown | 309 (59.2) | |
| Exposure to infected patients | 173 (33.1) | |
| Visiting to epidemic areas | 40 (7.7) | |
| Smoking history | ||
| Current smoker | 11 (2.1) | |
| Ex-smoker | 16 (3.1) | |
| Non-smoker | 398 (76.2) | |
| Unknown | 97 (18.6) | |
| Underlying disease | ||
| None | 321 (61.5) | |
| Hypertension | 120 (23.0) | |
| Diabetes | 81 (15.5) | |
| Cardiovascular disease | 27 (5.2) | |
| Cancer | 27 (5.2) | |
| COPD | 12 (2.3) | |
| Others | 41 (7.9) | |
| Visiting route | ||
| Visiting screening center | 338 (64.8) | |
| Visiting emergency room | 32 (6.1) | |
| Transfer from another hospital | 152 (29.1) | |
| Initial RT-PCR positivity | ||
| Yes | 511 (97.9) | |
| Symptoms | ||
| Fever | 292 (55.9) | |
| Cough | 245 (46.9) | |
| Dyspnea | 112 (21.5) | |
| Confusion | 1 (0.2) | |
| Laboratory findings | ||
| White blood cell, /uL | 5,697 ± 2,610 (1,610–22,430) | |
| Neutrophil, /uL | 3,919 ± 2,437 (1,010–21,757) | |
| Lymphocyte, /uL | 1,608 ± 1,358 (340–12,300) | |
| Platelet, /uL | 190,711 ± 100,919 (7,000–678,000) | |
| Total bilirubin, mg/dL | 0.7 ± 0.4 (0.4–2.2) | |
| ALT, U/L | 31 ± 35 (17–256) | |
| Albumin, g/dL | 4.0 ± 0.6 (3.7–5.1) | |
| BUN, mg/dL | 14.3 ± 10.4 (5.7–130) | |
| Creatinine, mg/dL | 0.9 ± 1.8 (0.6–28) | |
| CRP, mg/dL | 3.5 ± 5.7 (0–43.5) | |
| LDH,a U/L | 424 ± 282 (131–3,495) | |
| D-dimer,a ug/mL | 2.3 ± 5.3 (0.003–32.9) | |
| Procalcitonin,a ng/mL | 0.1 ± 0.5 (0–4.1) | |
| Treatment | ||
| Lopinavir/ritonavir | 239 (45.8) | |
| Hydroxychloroquine | 127 (24.3) | |
| Remdesivir | 12 (2.3) | |
| Steroid | 51 (9.8) | |
| Conservative treatment | 240 (46) | |
| O2 supply | 121 (23.2) | |
| Mechanical ventilation therapy | 38 (9.2) | |
| ECMO | 15 (2.9) | |
| ICU admission | 49 (9.4) | |
| ARDS | 27 (5.2) | |
| Mortality | 21 (4.0) | |
| Admission days | ||
| Mean ± SD | 23.9 ± 14.9 | |
| Range, day | 0–94 | |
Values are presented as number (%), mean (range), or mean ± SD.
COPD = chronic obstructive pulmonary disease, RT-PCR = reverse transcription-polymerase chain reaction, ALT = alanine aminotransferase, BUN = blood urea nitrogen, CRP = C-reactive protein, LDH = lactate dehydrogenase, ECMO = extracorporeal membrane oxygenation, ICU = intensive care unit, ARDS = acute respiratory distress syndrome, SD = standard deviation.
aD-dimer test was performed in 86 patients, procalcitonin in 334 patients, and LDH in 412 patients.
One hundred and seventy-three of the study subjects were treated with lopinavir/ritonavir, and 66 were additionally treated with hydroxychloroquine. Sixty-one patients were treated with only hydroxychloroquine and 12 with only remdesivir. Mean hospital stay was 23.9 ± 14.9 days (range, 0–94 days). One hundred and twenty-one (23.4%) of the study subjects needed nasal oxygen therapy or mechanical ventilation (n = 38; 7.3%), and 49 patients (9.4%) were admitted to an intensive care unit. Although most patients had cured, 21 patients (mean age, 74 ± 8.5 years; age range, 63–93 years) (4.0%) died. Of 21 patients who died, 15 had underlying diseases (diabetes [n = 11], cancer [n = 3], chronic obstructive pulmonary disease [n = 2], chronic kidney disease [n = 1]).
Imaging data
Four hundred and sixty-four (89.1%) of the study subjects underwent a low to standard-dose chest CT scan at least once during hospitalization, resulting in a total of 658 CT scans. Chest CT scans were performed: 1) when pneumonia was suspected clinically although pneumonia was not definite on a chest radiograph, 2) when complications were suspected. Numbers of CT scans per patients were as follows; one scan in 326 patients (70.1%); two in 97 patients (20.9%); three in 32 patients (6.9%); four in 8 patients (1.7%), and five in 2 patients (0.4%). Chest CT scans were performed using Siemens Healthineers (569 scans, 86.5%), GE Healthcare (9.0%), Canon Medical Systems (2.7%), or Phillips Medical Systems (1.8%) scanners. The two most commonly used CT scanners were SOMATOM Definition Flash (256 scans) and SOMATOM Definition AS+ (192 scans; Siemens Healthineers, Erlangen, Germany). Of the 658 scans, 328 (49.8%) and 315 (47.9%)were obtained using a slice thickness of ≤ 1.5 mm or between 1.5 and 3 mm, respectively; only 15 CT scans (2.3%) were constructed using a slice thickness of > 3 mm.
Four hundred and ninety-seven of 522 study subjects (95.2%) underwent chest radiography at least once during hospitalization, which resulted in a total of 1,475 chest radiographs (Fig. 2). Two hundred and twenty-four of these 497 patients (45.1%) underwent chest radiography three times, 153 patients (30.8%) twice, and 110 patients (21.9%) underwent chest radiography ≥ four times. Ten patients (2.0%) underwent chest radiography only at admission. Chest radiographs were obtained using various radiographic machines (46 machine types) from more than 17 vendors. The two most commonly used machines were INNOVISION series (477 images; DK Medical Systems, Seoul, Korea) and GM85 (214 images; Samsung Electronics, Seoul, Korea).
Fig. 2. Distribution of the number of curated chest radiographic examinations in the Korean imaging cohort of COVID-19.

COVID-19 = coronavirus disease 2019.
DISCUSSION
KICC-19 contained of 1475 chest radiographs and 658 CT scans of 522 consecutive patients with COVID-19 from 17 institutions across the Korea and relevant information about baseline characteristics and outcomes. Almost all chest CT scans were performed using multi-detector CT scanners, usually Siemens machines, and image slices thinner than 3 mm. Chest radiographs were obtained using 46 radiographic machine types, which reflects the heterogeneity of chest radiographic examinations in real practice. Several COVID-19 imaging databases are currently being built in the UK,25 and the United States,26 and thus, to the best of our knowledge, KICC-19 can serve as a unique database that compromises Asian populations.
KICC-19 patients shared common clinical features but experienced more severe disease than COVID-19 patients in the general Korean population. The patients included in KICC-19 were registered at main COVID-19 referral centers and most were hospitalized; average hospital stay was 23.9 days. As compared with a summary of the 3,060 patients of the general Korean population with COVID-19,27 KICC-19 registered patients were older (52 vs. 43 years), more frequently developed fever (55.9% vs. 28.8%), or dyspnea (21.5% vs. 7.4%), and had higher comorbidity (e.g., diabetes, 15.5% vs. 8.4%), intensive care unit admission (9.6% vs. 4.8%), and mortality (4.0% vs. 1.1%). Overall disease severity of in the KICC-19 was slightly less than that of patients hospitalized in Wuhan,21 and Italy,28 or New York City.29
KICC-19 contained data on patients with RT-PCR-proven COVID-19 and did not contain data on patients with a negative RT-PCR result, which was unavoidable because these patients rarely underwent chest imaging studies in Korea. Thus, the main benefits of the KICC-19 are; 1) to improve radiologic understanding of COVID-19 at baseline and aid prediction of prognosis, and 2) to enable the development and validation of deep learning algorithms for assessing disease severity and determining prognoses. Those applications are in line with the current indications of chest imaging studies in the relevant COVID-19 guidelines. The KICC-19 registry might also be useful for developing deep learning algorithms for the differential diagnosis of COVID-19 and other pneumonia which requires additional data on negative controls outside KICC-19.
This project has several limitations. First, the patient cohort was relatively small and included only 2.5% of all confirmed cases in Korea as of August 31st 2020. Nevertheless, we consider the present study meaningful as it is the first to be conducted using a national database established for COVID-19. Second, because we collected clinical information by referring to early studies on COVID-19 outcomes, the clinical information collected in this study could be insufficient to reflect the various symptoms of COVID-19. Third, we collected chest radiographic data of frontal chest radiographs obtained at baseline, within 24 hours of chest CT examinations, and at discharge, which might be not insufficient to capture full individual disease courses. Finally, we did not analyze radiologic abnormalities in this article because these are subject to ongoing studies and will be reported separately.
In conclusion, the KICC-19 was successfully established and collecting 658 CT scans and 1,475 chest radiographs of 522 hospitalized Korean COVID-19 patients were included between February 1st and May 31st 2020. It is hoped the KICC-19 will provide a more comprehensive understanding of the clinical, epidemiological, and radiologic characteristics of patients with COVID-19 and trigger the development and validation of deep learning algorithms for chest imaging in COVID-19.
Footnotes
Funding: This study was supported by the Korean Society of Radiology and Korean Society of Thoracic Radiology on May 2020, and National IT Industry Promotion Agency (A2201-20-1002).
Disclosure: Soon Ho Yoon is the chief medical officer of MEDICALIP, Co. Ltd. Other authors have no potential conflicts of interest to disclose.
- Conceptualization: Yoon SH, Jeong YJ.
- Data curation: Yoon SH, Jeong YJ.
- Investigation: Ham SY, Nam BD, Chae KJ, Lee D, Yoo JY, Bak SH, Kim JY, Kim JH, Kim KB, Jung IJ, Lim JK, Lee JE, Chung MJ, Lee YK, Kim YS, Jo JE.
- Methodology: Yoon SH, Jeong YJ.
- Writing - original draft: Yoon SH.
- Writing - review & editing: Yoon SH, Jeong YJ, Park CM, Kwon W, Lee SM, Kim YH.
References
- 1.Kim H, Hong H, Yoon SH. Diagnostic performance of CT and reverse transcriptase polymerase chain reaction for coronavirus disease 2019: a meta-analysis. Radiology. 2020;296(3):E145–E155. doi: 10.1148/radiol.2020201343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Herpe G, Lederlin M, Naudin M, Ohana M, Chaumoitre K, Gregory J, et al. Efficacy of chest CT for COVID-19 pneumonia in France. Radiology. 2020 doi: 10.1148/radiol.2020202568. Forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zu ZY, Jiang MD, Xu PP, Chen W, Ni QQ, Lu GM, et al. Coronavirus disease 2019 (COVID-19): a perspective from china. Radiology. 2020;296(2):E15–E25. doi: 10.1148/radiol.2020200490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Choi H, Qi X, Yoon SH, Park SJ, Lee KH, Kim JY, et al. Extension of coronavirus disease 2019 (COVID-19) on chest CT and implications for chest radiograph interpretation. Radiol Cardiothorac Imaging. 2020;2:e200107. doi: 10.1148/ryct.2020204001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wong HYF, Lam HYS, Fong AH, Leung ST, Chin TW, Lo CSY, et al. Frequency and distribution of chest radiographic findings in patients positive for COVID-19. Radiology. 2020;296(2):E72–E78. doi: 10.1148/radiol.2020201160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Toussie D, Voutsinas N, Finkelstein M, Cedillo MA, Manna S, Maron SZ, et al. Clinical and chest radiography features determine patient outcomes in young and middle-aged adults with COVID-19. Radiology. 2020;297(1):E197–E206. doi: 10.1148/radiol.2020201754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schalekamp S, Huisman M, van Dijk RA, Boomsma MF, Freire Jorge PJ, de Boer WS, et al. Model-based prediction of critical illness in hospitalized patients with COVID-19. Radiology. 2020 doi: 10.1148/radiol.2020202723. Forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rubin GD, Ryerson CJ, Haramati LB, Sverzellati N, Kanne JP, Raoof S, et al. The role of chest imaging in patient management during the COVID-19 pandemic: a multinational consensus statement from the fleischner society. Radiology. 2020;296(1):172–180. doi: 10.1148/radiol.2020201365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yoon SH, Lee KH, Kim JY, Lee YK, Ko H, Kim KH, et al. Chest radiographic and CT findings of the 2019 novel coronavirus disease (COVID-19): analysis of nine patients treated in Korea. Korean J Radiol. 2020;21(4):494–500. doi: 10.3348/kjr.2020.0132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jung HK, Kim JY, Lee MS, Lee JY, Park JS, Hyun M, et al. Characteristics of COVID-19 patients who progress to pneumonia on follow-up chest radiograph: 236 patients from a single isolated cohort in Daegu, South Korea. Korean J Radiol. 2020;21(11):1265–1272. doi: 10.3348/kjr.2020.0564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Park B, Park J, Lim JK, Shin KM, Lee J, Seo H, et al. Prognostic implication of volumetric quantitative ct analysis in patients with COVID-19: a multicenter study in Daegu, Korea. Korean J Radiol. 2020;21(11):1256–1264. doi: 10.3348/kjr.2020.0567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hwang EJ, Kim H, Yoon SH, Goo JM, Park CM. Implementation of a deep learning-based computer-aided detection system for the interpretation of chest radiographs in patients suspected for COVID-19. Korean J Radiol. 2020;21(10):1150–1160. doi: 10.3348/kjr.2020.0536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chon Y, Kim JY, Suh YJ, Lee JY, Park JS, Moon SM, et al. Adverse initial CT findings associated with poor prognosis of coronavirus disease. J Korean Med Sci. 2020;35(34):e316. doi: 10.3346/jkms.2020.35.e316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lee SE, Kim YS. Clinical and radiological findings of coronavirus disease 2019 pneumonia: 51 adult patients from a single center in Daegu, South Korea. J Korean Soc Radiol. 2020;81(3):591–603. doi: 10.3348/jksr.2020.81.3.591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rho JY, Yoon KH, Jeong S, Lee JH, Park C, Kim HW. Usefulness of mobile computed tomography in patients with coronavirus disease 2019 pneumonia: a case series. Korean J Radiol. 2020;21(8):1018–1023. doi: 10.3348/kjr.2020.0541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yoon SH, Kim M. Anterior pulmonary ventilation abnormalities in COVID-19. Radiology. 2020;297(2):E276–E277. doi: 10.1148/radiol.2020203043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shim SS. COVID-19 in Korea: what actions have been taken by radiologists to support the fight against the disease? J Korean Soc Radiol. 2020;81(3):604–607. doi: 10.3348/jksr.2020.81.3.604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lee HJ, Moon JW, Woo JY, Kim YN. Clinical and radiologic findings of COVID-19 pneumonia: South Korean experience from three cases. J Korean Soc Radiol. 2020;81(3):583–590. doi: 10.3348/jksr.2020.81.3.583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jin KN, Yoon SH, Park CH, Beck KS, Do KH, Yong HS. KSR/KSTR guidelines for the use of diagnostic imaging for COVID-19. J Korean Soc Radiol. 2020;81(3):577–582. doi: 10.3348/jksr.2020.81.3.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jeong YJ, Kim YH. Korean imaging cohort of COVID-19: potential role in education and research. J Korean Soc Radiol. 2020;81(3):608–609. doi: 10.3348/jksr.2020.81.3.608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi: 10.1001/jama.2020.1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi: 10.1001/jamainternmed.2020.0994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi: 10.1016/S0140-6736(20)30566-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi: 10.1016/S2213-2600(20)30079-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hare SS, Rodrigues JC, Jacob J, Edey A, Devaraj A, Johnstone A, et al. A UK-wide British Society of Thoracic Imaging COVID-19 imaging repository and database: design, rationale and implications for education and research. Clin Radiol. 2020;75(5):326–328. doi: 10.1016/j.crad.2020.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kundu S, Elhalawani H, Gichoya JW, Kahn CE. How might AI and chest imaging help unravel COVID-19's mysteries? Radiol Artif Intell. 2020 doi: 10.1148/ryai.2020200053. Forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sung HK, Kim JY, Heo J, Seo H, Jang YS, Kim H, et al. Clinical course and outcomes of 3,060 patients with coronavirus disease 2019 in Korea, January-May 2020. J Korean Med Sci. 2020;35(30):e280. doi: 10.3346/jkms.2020.35.e280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Palmieri L, Vanacore N, Donfrancesco C, Lo Noce C, Canevelli M, Punzo O, et al. Clinical characteristics of hospitalized individuals dying with COVID-19 by age group in Italy. J Gerontol A Biol Sci Med Sci. 2020;75(9):1796–1800. doi: 10.1093/gerona/glaa146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Goyal P, Choi JJ, Pinheiro LC, Schenck EJ, Chen R, Jabri A, et al. Clinical characteristics of COVID-19 in New York city. N Engl J Med. 2020;382(24):2372–2374. doi: 10.1056/NEJMc2010419. [DOI] [PMC free article] [PubMed] [Google Scholar]