

Abstract
Background The palmaris tendon inserts into the palmar fascia and is positioned in close association with the transverse carpal ligament. Loading of this tendon has been demonstrated to increase carpal tunnel pressures.
Purpose The purpose of this study was to determine if a relationship exists between the palmaris tendon, carpal tunnel syndrome (CTS), and handedness. The sensitivity, specificity, positive predictive value, and negative predictive value for Schaeffer's test were calculated.
Methods A retrospective review of patient charts undergoing endoscopic carpal tunnel release was performed. Rates of palmaris longus agenesis (PLA) were compared to a population matched data set. Statistical analysis was performed using a one-proportion z -test. Schaeffer's test for the palmaris longus tendon was performed on all patients and compared to intraoperative confirmation.
Results A total of 520 carpal tunnel releases were performed in 389 consecutive patients. The frequency of PLA in this surgical cohort was significantly lower compared to the population matched dataset. No correlation between handedness and laterality of CTS or PLA was found. Schaeffer's test was evaluated to yield sensitivity (93.6%), specificity (100%), positive predictive value (100%), and negative predictive value (50.8%).
Conclusion The palmaris tendon was more prevalent in a population of patients undergoing carpal tunnel release. These findings can be used to provide further insight into the pathophysiology of CTS. While Schaeffer's test was accurate in detecting the palmaris longus tendon, a negative test was frequently incorrect. Further imaging is recommended in patients with a negative Schaeffer's test when the palmaris longus is desired for surgical utilization.
Level of Evidence This is a Level III, prognostic study.
Keywords: carpal tunnel syndrome, congenital absence, endoscopic carpal tunnel release, palmaris longus tendon, median nerve compression
The pathophysiology of carpal tunnel syndrome (CTS) has been extensively investigated and has been related to a likely interplay between idiopathic, anatomic, systemic, and occupational factors. Previous associations with CTS are female gender, systemic fluid balance disorders, inflammatory conditions, hemorrhagic disorders, neuropathic conditions, occupational hazards, and anatomical variations. 1 2 3 4 5 6 7 8 9 10 11 12 More recently, an investigation into the palmaris longus tendon, an expected structure around the carpal tunnel, has been suggested to increase the incidence of the development of CTS. 1 2
Detrimental compression of the median nerve has been shown to occur with pressures exceeding 30 mm Hg in the carpal tunnel. This leads to a decrease in nerve conduction and, when sustained, may lead to a complete nervous blockade. 13 14 15 Both positional and anatomical factors have been shown to play a role in elevating carpal tunnel pressures. Prior in vivo and cadaveric studies have shown that terminal wrist positions, as well as loading of the palmaris longus in extension causes a significant rise in tunnel pressures. 13 16 In their study of carpal tunnel pressures, Keir et al 16 theorize that the palmaris tendon exerts a deforming force on the tunnel, particularly with wrist extension, leading to elevated canal pressures.
The palmaris longus has been shown to be absent in a sub portion of the population. Previous meta-analyses describe a range of palmaris longus agenesis (PLA) to be 15.6 to 20.25% with a predilection for agenesis in the nondominant arm. 17 18 19 Rates of PLA also differ between ethnicities with the lowest percentages of agenesis present in Asian populations at a rate of 2.9 to 4.5%, while Egyptian and Arab Middle Eastern population rates were found to be 55 and 41.7%, respectively. 16 18 20 Studies of Caucasian participants, being the majority of patients in this study, show a range of agenesis rates between 14.9 and 26.3%. 18 20 21 These pooled values provided a 15% baseline of PLA which was used to compare against a cohort of patients undergoing endoscopic carpal tunnel release for median nerve decompression.
This retrospective cohort study aims to determine if the palmaris longus tendon is found in a higher percentage of patients undergoing endoscopic carpal tunnel release when compared to the general public. Our hypothesis is that there will be a significantly smaller rate of PLA in our large cohort of operative patients when compared to a population matched cohort. Secondary outcomes measured include an analysis of hand dominance and laterality of carpal tunnel syndrome for which a positive correlation is expected. Further, a higher incidence of PLA is expected in the nondominant hand. The sensitivity, specificity, positive predictive value, and negative predictive value for Schaeffer's test was determined after intraoperative visualization of the tendon structure.
Methods
A retrospective chart review was performed on 389 consecutive patients undergoing endoscopic carpal tunnel release from September 2013 to July 2017 completed by a single fellowship-trained hand surgeon. Patients presented with the complaint of numbness and/or tingling in the median nerve distribution and were predominantly diagnosed with CTS through history and physical exam. Ultrasound or EMG/NCS (electromyography/nerve conduction study) was utilized when the diagnosis remained in question. Ultrasound testing supported the diagnosis with a measured cross-sectional area of the median nerve at the level of the pisiform of ≥12 mm 2 or EMG/NCS testing with cut-off values specific to the independent testing center. 22 23 24 Exclusion criteria for data collection included posttraumatic acute CTS and open carpal tunnel release. Patient demographics were recorded including age, race, and handedness. Schaeffer's test was used to document the presence of the palmaris longus tendon in the preoperative holding area. This test is performed by opposing the thumb to the small finger in partial wrist flexion and approximately 90 degrees of elbow flexion ( Fig. 1 ). The patients subsequently underwent an endoscopic carpal tunnel release where the presence or absence of the palmaris tendon was determined by direct visualization during the approach and recorded in the operative note.
Fig. 1.
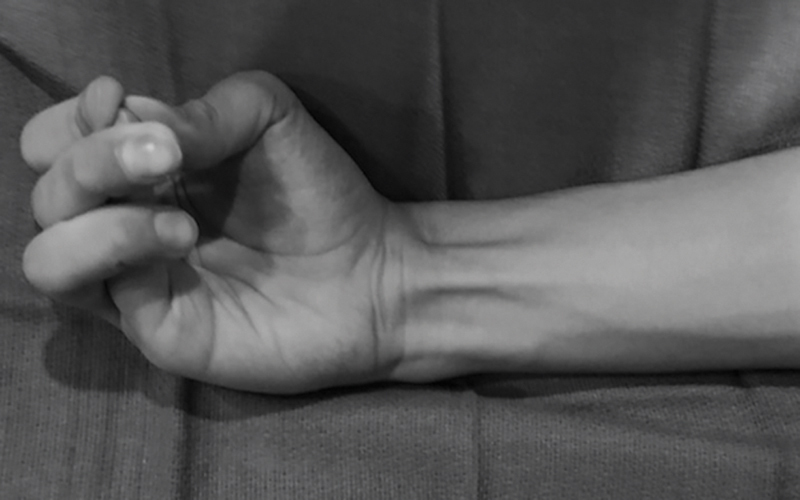
Example of a positive Schaeffer's test. Schaeffer's test performed with small finger opposition to the thumb in slight wrist flexion. Performed before endoscopic carpal tunnel release to identify the palmaris longus tendon.
The medical charts were reviewed after institutional review board (IRB) exemption was obtained. Data were collected including medical record number, age, handedness, gender, race, date of surgery, laterality of the endoscopic carpal tunnel release, results of Schaeffer's test preoperatively, and results of the observed findings of the palmaris tendon intraoperatively.
The rate of PLA in the surgical cohort was compared to a population matched rate of 15% using a one-proportion z -test to compare differences between two proportions. 18 20 21 Statistical significance was defined at the 5% ( p ≤ 0.05) level. Handedness and PLA, as well as handedness, and laterality of CTS were also compared using Chi-squared goodness of fit analysis between the collected data and the expected results. Sensitivity, specificity, negative predictive value, and positive predictive value were calculated from the results of the preoperative Schaeffer's test versus surgical confirmation of the palmaris longus tendon.
Results
A total of 520 endoscopic carpal tunnel procedures were performed on 389 patients. Bilateral procedures were done in 131 patients, 74 of which were performed in the same day. There were 145 males and 244 females. Patients' age ranged from 20 to 99 years old with the majority of patients between 50 and 79 years (69.4%) and an average patient age of 63 years. The patient population consisted of 360 Caucasian (92.5%), 14 Black (3.6%), 7 Hispanic (1.8%), 4 Asian/American Indian (1.05%), and 4 were not recorded (1.05%).
The palmaris longus tendon was visually confirmed to be present in 483 wrists (93.6%) and absent in 33 wrists (6.4%). In four cases, the data were not recorded. A one-proportion z -test was used as it compares an observed proportion to a theoretical one when two categories are being investigated. Thus, is was used to compare the 6.4% rate of PLA in the operative cohort compared to the expected 15% rate of PLA from the population matched cohort. This resulted in statistical significance with p < 0.01 (95% confidence interval [CI]). This supports the alternative hypothesis that the proportion of patients diagnosed with CTS exhibited higher rates of intact palmaris longus tendon structure than would be expected from population matched data.
This data were further analyzed to determine if there was a relationship between agenesis and handedness in the carpal tunnel cohort. A total of 305 patients were right handed, 44 were left handed, 10 identified as bilateral handed, and in 30 patients' handedness was not recorded. The unidentified and bilateral patients were excluded from this portion of the analysis. Expected values for the cohort were based on the percentages calculated since they were deemed statistically significant. Results are summarized in Table 1 . Due to the insufficient sample size, a Chi-squared goodness of fit analysis was unable to be done on the data concerning left handedness. However, there was no statistically significant deviation from the actual and expected values for agenesis on the right ( p > 0.05) implying that no relationship could be established between handedness and the presence or absence of the palmaris longus tendon.
Table 1. Calculation of palmaris longus agenesis association with handedness.
| Right handed | Left handed | |||
|---|---|---|---|---|
| Results | Expected | Results | Expected | |
| PL on R | 216 | 217.15 | 24 | 24.34 |
| PLA on R | 16 | 14.85 | 2 | 1.66 |
| PL on L | 167 | 165.6 | 28 | 28.08 |
| PLA on L | 10 | 11.33 | 2 | 1.92 |
Abbreviations: L, left; PL, palmaris longus; PLA, PL agenesis; R, right.
Note: Summary of actual and expected results of palmaris longus presence and agenesis based on handedness. There was no statistical significance to support right handedness being associated with agenesis. There was insufficient sample size to determine significance on the left.
Furthermore, a Chi-squared goodness of fit analysis was performed to identify a relationship between reported handedness and laterality of CTS. Patient with unidentified handedness or bilateral handedness were again excluded from this analysis. No correlation was found between handedness and laterality of CTS.
The results and analysis of Schaeffer's test are shown in Table 2 . The sensitivity, specificity, positive predictive value, and negative predictive value of Schaeffer's test were determined to be 93.6, 100, 100, 50.8%, respectively.
Table 2. Statistical analysis of Schaeffer's test.
| Result | ||
| Analysis of results for Schaeffer's test | (%) | |
| Sensitivity | 93.6 | |
| Specificity | 100 | |
| Positive predictive value | 100 | |
| Negative predictive value | 50.8 | |
| Analysis | ||
| Palmaris longus tendon present intraoperatively | Palmaris longus tendon absent intraoperatively | |
| Schaeffer's test positive | 453 | 0 |
| Schaeffer's test negative | 31 | 32 |
Note: results and analysis from Schaeffer's test to determine if the palmaris longus tendon was present or absent compared with the direct intraoperative visualization of the tendon. Note that approximately half of the time when the tendon was not detected preoperatively, the tendon was found intraoperatively (negative predictive value of 50.8%). Also, when Schaeffer's test was positive, the tendon was always identified intraoperatively (specificity and positive predictive value were 100%).
Discussion
The palmaris tendon inserts into the palmar fascia and is an extra-tunnel structure; however, it is positioned in close association with the transverse carpal ligament. Keir et al 16 demonstrated that loading of the palmaris tendon can increase carpal tunnel pressure, particularly with the wrist loaded in extension. These authors postulated that the palmaris tendon may exert a structural force onto the carpal tunnel altering the geometry of the tunnel. Thus, it seems plausible that an increased incidence of CTS would be present in patients with an intact tendon structure.
Studies of the palmaris longus tendon epidemiology show that it is absent in 14.9 to 26.3% of the Caucasian patient population. 18 20 21 Using these numbers to establish a baseline of agenesis, this study aimed to determine whether there was a significantly smaller percentage of agenesis noted in the cohort of operative patients. After reviewing the results of the operative cohort showing a PLA rate of 6.4%, this demonstrates a higher incidence of an intact palmaris tendon structure in this cohort. This correlates well with previous studies on the subject. 1 2
Analogous to this study, Keese et al 1 performed a case-control analysis on 72 patients to evaluate for a correlation of the palmaris longus tendon and CTS. This study used Schaeffer's test to similarly find a significantly lower PLA rate of 2.8% in their CTS cohort versus their control group where PLA was found at a rate of 22.2%. They calculated an odds ratio (OR) of 7.0 (95% CI) indicating the palmaris tendon having a higher association with CTS than industrial exposure (OR = 4.72), thyroid disease (OR = 3.70), diabetes (OR = 3.02), previous wrist fracture (OR = 2.29), rheumatoid arthritis (OR = 2.23), and obesity (OR = 1.77). 25 26 27 This current study aims to expand on this subject by evaluating a larger patient study group that removes the clinical exam as a potential confounding variable by intraoperatively confirming the presence of the palmaris tendon.
A preoperative clinical exam for the palmaris tendon becomes particularly important in procedures involving tendon harvesting and provides a useful landmark in endoscopic carpal tunnel release. Schaeffer's test which involves thumb opposition to the small finger in slight wrist flexion is a well-known and supported clinical exam for the identification of the palmaris longus tendon. 18 28 29 This test was originally described by Schaeffer in 1909, and in a series of 800 patients was compared to related clinical exams including the Thompson test, the Pushpakumar's “two-finger sign,” and Bhattacharya's flexion test, amongst others. Schaeffer's test was shown to have the highest diagnostic ability to identify the palmaris tendon at a rate of 98.1%. 28 30 Endoscopic carpal tunnel release offers the ability to directly visualize the palmaris tendon and this presented an interesting opportunity to evaluate the accuracy of this test. The calculated sensitivity of Schaeffer's test was found to be 93.6% and its specificity to be 100% which correlates well with previously described numbers. 28 29 30 Interestingly, the test had a negative predictive value of 50.8% which suggests that when presented with a negative result, the addition of another clinical exam or imaging may be of use to practitioners to reveal the palmaris tendon.
Prior research has been completed to decipher if there is an exertional basis for the development of CTS. Many of these studies include industrial work, repetitive wrist postures, and vibration as a workplace job description as being positive predictive factors for the development of CTS. 6 8 9 10 11 Furthermore, it has been debated in the literature, as to whether the development of CTS is more commonly found in the dominant hand which would correlate with its increased presence in manually demanding jobs. 4 31 However, this study did not show a relationship between handedness and CTS which reached significance.
Limitations
There are several limitations to this study. One limitation was that it is a retrospective cohort analysis of patients with CTS and the data were not prospectively gathered. However, thorough records of patient demographics, as well as preoperative clinical exam findings, and the postoperative notation of the presence of the palmaris tendon was routinely gathered. This would not have changed whether the data were prospectively gathered or retrospectively reviewed. A control group was not present to compare rates of palmaris longus agenesis but this number was conferred from multiple sources on the subject. 16 18 20 Further, heterogeneous methods to support the diagnosis of CTS including NCS/EMG and ultrasound were used. However, the clinical examination is the gold standard in diagnosing CTS and both of these adjunctive diagnostic modalities are supported in the literature. 22 23 24 Lastly, although the results further establish a correlation between the presence of the palmaris longus tendon and CTS, this study does not provide causation for this occurrence.
Conclusion
This study reveals that, when compared to the general population, the palmaris longus tendon was more prevalent in a cohort of patients with CTS as confirmed by its visualization during an endoscopic carpal tunnel release. The operatively challenged Schaeffer's test also demonstrated that additional clinical examination maneuvers or imaging should be considered in light of a negative examination when the palmaris longus is desired for surgical utilization. Further research on this subject is necessary to provide more information on the pathophysiology of this condition and its association with the palmaris longus tendon to have future implications on treatment methods. We did not routinely record percentage improvement following surgery for the purposes of this study. However, this would make for an interesting prospective, case-control study evaluating patient's recovery in relation to their palmaris longus status.
Conflict of Interest None declared.
Note
The work was performed at Hand & Upper Extremity Surgery, Orthopaedic Specialties of Tampa Bay 1011 Jeffords Street Building D Clearwater, FL 33756 USA.
Ethical Approval
This study is exempt from further institutional review board (IRB) review under 45 CFR 46.101(b) (Exempt Category 4).
References
- 1.Keese G R, Wongworawat M D, Frykman G. The clinical significance of the palmaris longus tendon in the pathophysiology of carpal tunnel syndrome. J Hand Surg [Br] 2006;31(06):657–660. doi: 10.1016/j.jhsb.2006.07.015. [DOI] [PubMed] [Google Scholar]
- 2.Jafari D, Taheri H, Shariatzadeh H. The clinical significance of the palmaris longus tendon and functional superficial flexor of the little finger in the pathophysiology of carpal tunnel syndrome. Med J Islam Repub Iran. 2008;22(01):8–11. [Google Scholar]
- 3.Server F, Miralles R C, Galcerá D C.Carpal tunnel syndrome caused by an anomalous palmaris profundus tendon J Anat 1995187(Pt 1):247–248. [PMC free article] [PubMed] [Google Scholar]
- 4.Reinstein L. Hand dominance in carpal tunnel syndrome. Arch Phys Med Rehabil. 1981;62(05):202–203. [PubMed] [Google Scholar]
- 5.Mondelli M, Aprile I, Ballerini M. Sex differences in carpal tunnel syndrome: comparison of surgical and non-surgical populations. Eur J Neurol. 2005;12(12):976–983. doi: 10.1111/j.1468-1331.2005.01099.x. [DOI] [PubMed] [Google Scholar]
- 6.Nathan P A, Meadows K D, Istvan J A. Predictors of carpal tunnel syndrome: an 11-year study of industrial workers. J Hand Surg Am. 2002;27(04):644–651. doi: 10.1053/jhsu.2002.34003. [DOI] [PubMed] [Google Scholar]
- 7.Cranford C S, Ho J Y, Kalainov D M, Hartigan B J. Carpal tunnel syndrome. J Am Acad Orthop Surg. 2007;15(09):537–548. doi: 10.5435/00124635-200709000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Roquelaure Y, Ha C, Pelier-Cady M C. Work increases the incidence of carpal tunnel syndrome in the general population. Muscle Nerve. 2008;37(04):477–482. doi: 10.1002/mus.20952. [DOI] [PubMed] [Google Scholar]
- 9.Spahn G, Wollny J, Hartmann B, Schiele R, Hofmann G O. [Metaanalysis for the evaluation of risk factors for carpal tunnel syndrome (CTS) Part II. Occupational risk factors] (in German) Z Orthop Unfall. 2012;150(05):516–524. doi: 10.1055/s-0032-1315346. [DOI] [PubMed] [Google Scholar]
- 10.Kozak A, Schedlbauer G, Wirth T, Euler U, Westermann C, Nienhaus A. Association between work-related biomechanical risk factors and the occurrence of carpal tunnel syndrome: an overview of systematic reviews and a meta-analysis of current research. BMC Musculoskelet Disord. 2015;16(16):231. doi: 10.1186/s12891-015-0685-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Roquelaure Y, Ha C, Nicolas G. Attributable risk of carpal tunnel syndrome according to industry and occupation in a general population. Arthritis Rheum. 2008;59(09):1341–1348. doi: 10.1002/art.24002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Geoghegan J M, Clark D I, Bainbridge L C, Smith C, Hubbard R. Risk factors in carpal tunnel syndrome. J Hand Surg [Br] 2004;29(04):315–320. doi: 10.1016/j.jhsb.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 13.Gelberman R H, Hergenroeder P T, Hargens A R, Lundborg G N, Akeson W H. The carpal tunnel syndrome. A study of carpal canal pressures. J Bone Joint Surg Am. 1981;63(03):380–383. [PubMed] [Google Scholar]
- 14.Rydevik B, Lundborg G, Bagge U. Effects of graded compression on intraneural blood blow. An in vivo study on rabbit tibial nerve. J Hand Surg Am. 1981;6(01):3–12. doi: 10.1016/s0363-5023(81)80003-2. [DOI] [PubMed] [Google Scholar]
- 15.Hargens A R, Romine J S, Sipe J C, Evans K L, Mubarak S J, Akeson W H. Peripheral nerve-conduction block by high muscle-compartment pressure. J Bone Joint Surg Am. 1979;61(02):192–200. [PubMed] [Google Scholar]
- 16.Keir P J, Wells R P, Ranney D A, Lavery W. The effects of tendon load and posture on carpal tunnel pressure. J Hand Surg Am. 1997;22(04):628–634. doi: 10.1016/S0363-5023(97)80119-0. [DOI] [PubMed] [Google Scholar]
- 17.Pękala P A, Henry B M, Pękala J R. Congenital absence of the palmaris longus muscle: A meta-analysis comparing cadaveric and functional studies. J Plast Reconstr Aesthet Surg. 2017;70(12):1715–1724. doi: 10.1016/j.bjps.2017.08.002. [DOI] [PubMed] [Google Scholar]
- 18.Yammine K. Clinical prevalence of palmaris longus agenesis: a systematic review and meta-analysis. Clin Anat. 2013;26(06):709–718. doi: 10.1002/ca.22289. [DOI] [PubMed] [Google Scholar]
- 19.Erić M, Koprivčić I, Vučinić N. Prevalence of the palmaris longus in relation to the hand dominance. Surg Radiol Anat. 2011;33(06):481–484. doi: 10.1007/s00276-010-0751-0. [DOI] [PubMed] [Google Scholar]
- 20.Soltani A M, Peric M, Francis C S. The variation in the absence of the palmaris longus in a multiethnic population of the United States: an epidemiological study. Plast Surg Int. 2012;2012:282959. doi: 10.1155/2012/282959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thompson N W, Mockford B J, Cran G W. Absence of the palmaris longus muscle: a population study. Ulster Med J. 2001;70(01):22–24. [PMC free article] [PubMed] [Google Scholar]
- 22.Roghani R S, Holisaz M T, Norouzi A AS. Sensitivity of high-resolution ultrasonography in clinically diagnosed carpal tunnel syndrome patients with hand pain and normal nerve conduction studies. J Pain Res. 2018;11:1319–1325. doi: 10.2147/JPR.S164004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McDonagh C, Alexander M, Kane D. The role of ultrasound in the diagnosis and management of carpal tunnel syndrome: a new paradigm. Rheumatology (Oxford) 2015;54(01):9–19. doi: 10.1093/rheumatology/keu275. [DOI] [PubMed] [Google Scholar]
- 24.Beekman R, Visser L H. Sonography in the diagnosis of carpal tunnel syndrome: a critical review of the literature. Muscle Nerve. 2003;27(01):26–33. doi: 10.1002/mus.10227. [DOI] [PubMed] [Google Scholar]
- 25.Goeghegan J M, Clark D I, Bainbridge L C, Smith C, Hubbard R. Risk factors in carapal tunnel syndrome. J Hand Surg [Br] 2004;29B:315–320. doi: 10.1016/j.jhsb.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 26.Karpitskaya Y, Novak C B, Mackinnon S E. Prevalence of smoking, obesity, diabetes mellitus, and thyroid disease in patients with carpal tunnel syndrome. Ann Plast Surg. 2002;48(03):269–273. doi: 10.1097/00000637-200203000-00007. [DOI] [PubMed] [Google Scholar]
- 27.Yagev Y, Carel R S, Yagev R. Assessment of work-related risks factors for carpal tunnel syndrome. Isr Med Assoc J. 2001;3(08):569–571. [PubMed] [Google Scholar]
- 28.Schaeffer J P. On the variations of the palmaris longus muscle. Anat Rec. 1909;3:275–278. [Google Scholar]
- 29.Erić M, Krivokuća D, Savović S, Leksan I, Vucinić N. Prevalence of the palmaris longus through clinical evaluation. Surg Radiol Anat. 2010;32(04):357–361. doi: 10.1007/s00276-009-0573-0. [DOI] [PubMed] [Google Scholar]
- 30.Kigera J WM, Mukwaya S. Clinical assessment of the palmaris longus- accuracy of common tests. Ann of African Surgery. 2012;9(02):104–107. [Google Scholar]
- 31.Shiri R, Varonen H, Heliövaara M, Viikari-Juntura E. Hand dominance in upper extremity musculoskeletal disorders. J Rheumatol. 2007;34(05):1076–1082. [PubMed] [Google Scholar]