

Abstract
Background:
The results of several international studies indicate a high prevalence of language and communication impairments among children who are referred to child psychiatric services. However, these impairments are likely to remain undetected unless language and communication impairments are evaluated during the psychiatric assessment.
Aims:
The aim of the present study is to investigate the specific association between general and specific mental health problems, as expressed by the problem scales of Child Behavior Checklist (CBCL) and Teachers Report Form (TRF), and pragmatic skills and pragmatic language impairments (PLI) as defined the Pragmatic Composite of the Child Communication Checklist (CCC-PC).
Methods:
Children aged from 8 to 13 years (n = 73) were recruited in sequence following referral to a child and adolescent psychiatry (CAMHS) outpatient clinic within 12 months. Children with possible or established autism or intellectual disability were excluded. Standardized instruments measuring language, communication and mental health symptoms were distributed to parents and teachers, an intelligence test administered for clinical purposes, and demographic information was included.
Results:
The parent reports showed PLI among 38% of the children and revealed strong associations with the CBCL scales for emotional problems, thought problems and, especially, social and withdrawal symptoms, which mean more associations to internalized and non-externalized problems. PC-scores were at similar levels and PLI was reported by teachers at similar rates (compared to parent reports) with moderate agreement. Teacher PC-scores showed associations to only one TRF-scale, social problems. The CCC-PC subscale with the strongest associations to mental health symptoms was «Use of Context» («Social Relationships» do not contribute to the CCC-PC scores).
Conclusion:
There was a general increase in PC-scores and increased prevalence of PLI in this clinical sample. PC-scores correlated with symptom scores for internalizing and non-externalizing problems scales. The strongest common factors appear to be related to the social aspects of mental health. Pragmatic skills should be considered as a protective factor for mental health rather than investigating pragmatic impairment as a risk or vulnerability factor.
Keywords: Pragmatic impairment, mental health problems, CAMHS, ASEBA
Introduction
Many children who are referred to psychiatric services have difficulties in communicating effectively in daily life and talking about their problems. The results of several international studies indicate a higher prevalence of language difficulties among children with mental health problems and that these difficulties often remain undiscovered unless specific assessments of language and communication are done (1). Cohen et al. (2) found undiagnosed language problems in 40% of their child psychiatric sample.
The associations between specific language problems and emotional problems and behavioral problems are well known, although the results are somewhat inconsistent (3,4). Regrettably, many studies of language and mental health did not specify the type of language impairment and included quite different aspects of language, such as form, content and communication (5). Although vocabulary, expressive deficits, phonological deficits, comprehension deficits and pragmatic language deficits may influence and correlate with each other, they may have different associations with mental health.
Bishop et al. (6) suggested PLI as a term for a language disorder that is especially relevant for mental health and developmental disorders, defined as the practical use of language in communication rather than vocabulary, vocal or structural aspects of language. The majority of children with PLI did not show any signs of autistic functioning but rather had other psychiatric or developmental problems (6). Several studies have indicated that the functional use of language in communication is more important for mental health than are the other aspects of language (7,8).
PLI refers to the inappropriate use and interpretation of language in different social contexts (9). Children with PLI may speak fluently and articulate well, but they have problems adhering to the needs of the conversational partner (10,11). Im-Bolter and Cohen (12) warned that PLI might be misinterpreted due to overlapping symptoms with social-emotional and developmental problems. There is still a controversy whether PLI is a separate developmental disorder, a specific “language disorder,” or an aspect or symptom of low-grade or high-function autism (3,13,14). This is the case despite the establishment of the diagnosis “social communication disorder” in the DSM5, which was tailored to label PLI as a separate disorder and has the additional requirement of both non-verbal and verbal communication problems (15).
Later studies of PLI have shown associations between PLI and both mental health and developmental disorders (16,17). Farmer et al. (18) claimed that PLI showed no association with emotional and behavioral problems but found an association to autism and hyperactivity in a special education sample, of whom 1/3 had autistic symptoms. St Clair, Pickles (3) reported PLI associations with all emotional and behavioral problem scales of the SDQ, but the association was least clear for hyperactivity in a three-stage longitudinal study of children with language problems. Ketalaars et al. (19) concluded that pragmatic problems was associated with behavioral problems, although their results showed associations with all SDQ scales, (least for emotional problems) in a study of 4-year-old primary school children, whereas Helland et al. (20) claimed a stronger association with ADHD and behavioral problems.
According to Leonard (21), pragmatic skills provide a unique contribution to the estimate of the children’s social skills, above and beyond the contributions of both hyperactivity and inattention. Mackie (22) reported clinically significant language impairments (pragmatic, structural and word decoding difficulties) in 91% of their sample selected by educational psychologists due to behavioral concerns. These findings strongly indicate that language impairments of some kind very often accompany behavioral disorders. Gilmour (23) found that two-thirds of their sample of children with conduct disorder had PLI. They also identified pragmatic language deficits in approximately two-thirds of a sample of children with antisocial behavior and suggested that these deficits may underlie the antisocial behavior. In line with this finding, Donno (24) argued that pragmatic language deficits should be considered a possible contributory factor to behavioral problems in primary school children.
Summing up, previous studies have pointed toward quite different specific associations between pragmatics skills and mental health problems, possibly depending on the study samples as well as the selection of variables. The general aim of this study is to investigate the association with a broader perspective on mental health.
Pragmatic language deficits are relevant to mental health clinical practice because they may have detrimental effects on the development of successful peer relationships and negatively impact the child’s quality of life (25). However, the PLI association with mental health problems is likely to be bidirectional across development, because language, social problems and other mental health problems also can impair the development of pragmatic abilities (26). The present cross-sectional study cannot contribute to the understanding of this longitudinal interplay.
Aims
Our focus in the present study is on mental health symptom dimensions rather than developmental disorders. There may be both the general association between PLI and mental health problems, and differences in the strength of association for different types of mental health problems.
Many of the previous studies have used samples with educational problems or focused on a few mental health problems. We wanted to investigate the associations with a broader array of mental health problems, excluding the developmental problems of autistic functioning and intellectual disability. Furthermore, we wanted to investigate the associations between mental health problems and the specific aspects of PLI – the ‘Pragmatic Composite’ subscales and other subscales of CCC. We also wanted to use standardized measures of mental health symptoms to compare the level of mental health symptoms in a clinical sample to community baselines and to differentiate between covariation and severity by using both continuous and categorical approaches in the analyses. A CAMHS sample was chosen to ensure that there were sufficient mental health-problem frequencies to evaluate comorbidity.
These strategies were chosen to expand and detail our knowledge about the associations between mental health problems and PLI.
Research questions:
-
1)
Are there significant associations between PLI and eight dimensions of mental health symptoms among children referred to a CAMHS clinic?
-
2)
Do the associations between PLI and psychiatric symptoms differ depending on a) child age, b) child gender or c) parent or teacher informants?
-
3)
Do parent and teacher reports show different levels of PLI or different associations with mental health symptoms?
Method
Sample
Children aged 8–13 years who were referred to a child psychiatric outpatient clinic for 12 months were invited in consecutive order. All referrals came from family doctors and were often based on collaboration with health, educational or child welfare agencies in the community. Of those 186 who were originally referred, 42% (n = 73) were included and agreed to participate. Approximately one of four referred children (parents) did not receive the invitation due to failing clinics routines, but there was no indication of systematic bias due to this. The gender balance in the final sample was 75% boys (55) and 25% girls (18), whereas the gender balance in the clinic was 70/30 in this age group.
Rather than including a control group, we compared our results with results of studies among community children and CAMHS patients (17) as normal and clinical reference values.
Bishop (27) recommended basing evaluations of pragmatics on parent reports rather than on teacher reports. However, because this conclusion was based on a language impaired sample, we chose to initially include both parental and teacher information and compare the information in the first analytic stage. When not specified, the results regarding PLI, PC-scores or other CCC-scales refer to parental reports.
Instruments
Pragmatic language skills. The Children’s Communication Checklist (CCC) was developed to assess the pragmatic aspects of communication problems among children (6,28) and was later connected to normative community samples in England (27). The ‘Pragmatic Composite’ sum score has been used as a measure of pragmatic language problems, composed of the sum of six of the ten CCC-scales (‘Inappropriate Initiation’, ‘Coherence’, ‘Stereotyped Conversation’, ‘Use of Context’, ‘Rapport and Interests’). We chose the cut-off value of ≤ 140 for pragmatic problems (low score = PLI) based on the CCC ‘Pragmatic Composite’ (CCC-PC), because most other Norwegian and British studies used this cut-off, and we wanted to compare our own results to these. Norwegian CCC-norms or culture-specific validation are not established, but descriptive results from a community sample and a psychiatric sample have been published (17) and were used as a reference in the present study. These studies indicate that the cut-off ≤ 140 for PC also suits the distribution on the Norwegian version well. Reasonable agreement has been shown between Norwegian and British community mean values and PLI prevalence. Psychiatric samples from both countries (17,27) and the present study showed mean scores that were approximately two SD lower than community sample means in both countries.
To expand the scope of mental problems, we chose the parent- and teacher-report problem scales of the Achenbach System of Empirically Based Assessment (ASEBA) as our mental health instruments because of the broader array of scales with well available norms and reference materials. The parent and teacher forms of the ASEBA are the CBCL and the TRF from the ASEBA-package, the most highly used standardized instruments in both research and clinics in Norway for assessing child psychiatric symptoms and have established norms and validity in many countries, including Norway. CBCL and TRF have eight problem scales: ‘Anxious/Depressed’, ‘Withdrawn/Depressed’, ‘Somatic Complaints’, ‘Social Problems’, ‘Thought Problems’, ‘Attention Problems’, ‘Rule-Breaking Behavior’ and ‘Aggressive Behavior’; the first three may be combined into the ‘Internalized Problems’ sum score, the next two non-externalized (other) problems, and the last three can be combined into the ‘Externalized Problems’ and altogether they are combined into the ‘Total Problems’.
The Norwegian version of WISC-III (Wechsler Intelligence Scale for Children, third version) (29) was used as a measure of intelligence based on Swedish norms for the total score and 12 subscales.
Procedure
Written information with a consent form was sent to parents of all patients referred to a child psychiatry clinic over a 12-month period, restricted to the age groups between 8 and 13 years.
For those who were included and agreed to participate, the WISC, CBCL, and TRF results, information on age and referral reasons were collected as part of the clinical activity and transferred to the research database. CCC was collected by mail from parents and teachers.
Seven participants were excluded based on these criteria: 1) possible intellectual disability based on previous or present clinical diagnosis or total IQ-score below 70 based on WISC-III; 2) possible autism spectrum problems based on referral hypotheses or clinical diagnosis in CAMHS. These exclusion criteria were used to ensure a focus on mental health problems rather than general developmental problems. Benasich et al. argued that a low intellectual capacity could be mistaken as a specific language impairment (30). Furthermore, the DSM5 criteria for ‘Social Communication Disorder’ state that the disorder should not be better explained by autism spectrum disorders or intellectual disability. In addition to excluding individuals, we controlled for the influence of both general and verbal intelligence in the most central analyses without finding any influence.
Analyses
Group differences on continuous scales were tested with SPSS Multivariate Linear Model (GLM) and related by using one or two combined grouping variables and continuous or dichotomous covariates. The associations between continuous variables were tested using Pearson’s correlations. Cross-tables and χ2 were used to compare our prevalence rates with those of previous studies. The degree of concordance between informants was evaluated with Cohen’s kappa. The rate of pragmatics difficulties was defined as ≤ 140 on the CCC sum score (27). A clinical level of psychiatric symptoms l was defined as T ≥ 70 for each ASEBA symptom-scale. The ASEBA symptom scores were converted into standardized T-scores, which imply a correction for gender and age relative to the age-blocks of 6–11/12–18 years. Analyses of ASEBA scale scores were repeated using unadjusted raw-scores instead of T-scores to ensure that scoring did not alter the conclusions. The differences between the mean scale scores and standard deviance (SD) in our sample and similar data from earlier publications were compared in t-tests for independent samples using a web-based statistical tool, http://www1.assumption.edu/users/avadum/applets/applets.html. All other analyses were done using SPSS. A separation in two age-groups (8 to 10 and 11 to 13 years of age) was used to compare our results with previous studies using only the first age-span in the Norwegian community and psychiatry samples (17).
Results
Descriptive PC-scores and PLI prevalence
Our mean (SD) parental PC-scores M1 = 142.21 (10.7) in the 8 to 12 year old subgroup were similar to those reported in a psychiatric sample with this age range, but they were significantly lower than those from a community comparison group (17) (M2 = 152.60 (5.9); t (66) = 4.725, p < 0.001). The overall PLI prevalence (PC-score ≤ 140) in our psychiatric sample was 38% based on parent reports and 41% based on teacher reports. These rates were not significantly associated with age or gender.
A scatterplots between parental ‘Pragmatic Composite’ and CBCL ‘Social Problem’ scores show that only one participant above PC = 140 has a Social Problem score in the clinical range. A ROC-curve shows sensitivity of 0.83 and specificity of 0.33, and that an optimal sensitivity/specificity balance would follow using 136.5 as cut-off in this sample.
General or verbal intelligence, as measured by WISC-III, was not associated with PC-scores or PLI prevalence, regardless of whether parent or teacher information was used for CCC.
Covariation between pragmatic impairment and mental health symptom
Children with parent-reported PLI had significantly higher symptom scores on four of the eight CBCL problem scales: ‘Anxious/Depressed’, ‘Withdrawn/Depressed’, ‘Social Problems’ and ‘Thought Problems’. The same pattern appeared for PC-score correlations with CBCL symptom scores (see details in Table 1). However, for the first two CCC-scales not included in the ‘Pragmatic Composite’, ‘Speech’ and ‘Syntax’, there were no significant associations with any CBCL scales, whereas ‘Social Relationships’ correlated with 7/8 problem scales, and ‘Interests’ correlated significantly with two internalized scales, ‘Anxious/Depressed’, ‘Withdrawn/Depressed’. The overall PLI rate in our sample was 39% in both age ranges 8 to 10 years and 11 to 13 years which is considerably lower but not significantly different from the rate reported by Helland (17); 57%. Among children without any high CBCL symptom scores (T < 70 on all scales) the PLI rate was 27%, whereas among those with at least one high problem scale (T > 70) the PLI rate was 50%. The PLI rate was at its maximum of 87% among those with high scores (T > 70) on ‘Withdrawn/Depressed’ – which was significantly higher than all clinical or community comparison rates (see Figure 1).
TABLE 1.
Parent-reported ‘Pragmatic Composite’ scores (PC-scores) correlated with CBSL symptom scale scores, and the difference in CBCL symptom scores between groups with pragmatic language impairment prevalence and not (defined by PC-scores below 140)
| ASEBA-scales: | Pragmatic Composite | PLI ANOVA |
|---|---|---|
| Anxious/Depressed | r = 0.34, p = 0.003 | F = 9.996 p = 0.002 |
| Withdrawn/Depressed | r = 0.32, p = 0.008 | F = 5.565 p = 0.021 |
| Somatic Complaints | r = 0.02, p = 0.877 | F = 0.058 p = 0.811 |
| Social Problems | r = 0.47, p < 0.001 | F = 16.295 p < 0.001 |
| Thought Problems | r = 0.38, p = 0.001 | F = 8.834 p = 0.004 |
| Attention Problems | r = 0.29, p = 0.013 | F = 3.739 p = 0.057 |
| Rule-Breaking Behavior | r = 0.15, p = 0.206 | F = 1.706 p = 0.196 |
| Aggressive Behavior | r = 0.19, p = 0.116 | F = 2.498 p = 0.118 |
FIGURE 1.

Prevalence rates of Pragmatic Language Impairment - PLI (Child Communication Checklist - PC-score < 140) within groups defined by T-score > 70 on CBCL problem scales (Child Behavioral Checklist) and within two reference samples from child psychiatry and the community (17) * Significant contrasts (χ2-test, p < 0.05) to subjects with any CBCL-scale T>70 [*] ¤ Significant contrasts (χ2 -test, p < 0.05) to subjects with no CBCL-scale T>70 [¤] # Significant contrasts (χ2 -test, p < 0.05) to community children; Helland et al. (17) [#] @ Total clinical sample
Children with teacher reported PLI had significantly higher TRF symptom scores than did those without PLI on only one of the eight TRF problem scales: ‘Social Problems’ (F (1.69) = 10.89, p = 0.002), which was also significantly correlated with PC-scores. This association was not moderated by gender, age, or intelligence in regression models.
There were no significant correlations between WISC-III total, verbal IQ, performance IQ-score, parental CCC-scales ‘Speech’ and ‘Syntax’, and CBCL/TRF symptom scores on any problem scales
Teacher vs. parent reports
The mean teacher reported PC-scores or PLI prevalence were not different from the parental reports and was not associated with gender or age. Teacher and parent PC-scores showed a moderate correlation (r = 0.44, p > 0.01), and the agreement between PLI prevalence (scores below cut-off) was 71.3% (kappa = 0.40, p < 0.001).
There was no significant difference in mean level between the parent CBCL and teacher TRF T-score levels on any ASEBA problem scale. The correlations between teacher- and parent-reported ASEBA symptoms were moderate for the scales ‘Rule-Breaking Behavior’ and ‘Aggressive Behavior’ (r = 0.51–0.54, p > 0.01), weak for the scales ‘Anxious/Depressed’, ‘Somatic Complaints’ and ‘Social Problems’ (r = 0.26–0.33, p >0.01), and non-significant and low for the remaining scales ‘Withdrawn/Depressed’, ‘Somatic Problems’ and ‘Attention Problems’.
TABLE 2.
Correlations between CBCL problem scales and CCC subscales
| Anx | Wdr | Som | Social | Tho | Att | Rul | Agg | |
|---|---|---|---|---|---|---|---|---|
| A Speech | −0.116 | −0.178 | 0.106 | −0.228 | −0.120 | −0.176 | −0.087 | −0.058 |
| B Syntax | −0.173 | −0.019 | 0.135 | −0.044 | 0.226 | 0.067 | 0.087 | 0.095 |
| C Inappropriate Initiation | −0.177 | −0.198 | −0.091 | −0.390** | −0.372** | −0.279* | −0.110 | −0.153 |
| D Coherence | −0.271* | −0.231 | 0.002 | −0.323** | −0.143 | −0.298* | −0.058 | −0.082 |
| E Stereotyped Conversation | −0.237* | −0.245* | 0.027 | −0.294* | −0.331** | −0.126 | −0.116 | −0.124 |
| F Use of context | −0.303* | −0.223 | 0.036 | −0.473** | −0.317** | −0.246* | −0.235* | −0.263* |
| G Rapport | −0.191 | −0.252* | −0.102 | −0.212 | −0.304* | −0.151 | .026 | −0.033 |
| H Social Relationships | −0.352** | −0.487** | −0.024 | −0.614** | −0.417** | −0.368** | −0.416** | −0.457** |
| I Interests | −0.248* | −0.489** | 0.051 | −0.227 | −0.303** | −0.107 | −0.116 | −0.240* |
Note. Scales contributing to the ‘Pragmatic Composite’ marked with Bold and Italics Statistical significance is accentuated with bold types
p < 0.05;
p <0.001
Discussion
The parent reports in the present study indicate that pragmatic skills tend to be lower and PLI rates highly prevalent among children with mental health problems, compared to children in the community. The results also indicate two components, first a moderate negative association between pragmatic skills and mental health problems in general and more so for internalized and non-externalized problems. The specific component shows itself as strong to moderate associations between pragmatic skills and internalized and social problems (problems of social interaction and social withdrawal, including depressive symptoms followed by anxiety and rumination (as reflected in the ‘Thought Problems’ scale of CBCL)). These problems significant correlations between problem-specific symptom levels and PC-scores, as well as highest PLI prevalence among those with clinical symptom levels. In contrast, no significant correlations were found between PC-scores and the level of attention problems, rule-breaking behavior, and the potentially stress-related somatic symptoms. However, children with these problems also showed a significantly higher prevalence of PLI than found in a community study (31).
Parents and teachers reported the same rate of PLI and rate of externalized problems. As in earlier studies, they only agreed moderately on who has PLI (27), and teachers generally seemed less able to detect internalized symptoms.
Comparison with earlier studies
The levels of parent-reported PLI that we found among children referred to child psychiatry were similar to those reported in Canada (2) and in another Norwegian study (17). Compared to the community rates of 1/10 reported by Helland et al. (17), our PLI rates in a clinical sample was much higher −38% overall in general and 73–88% among children with social problems and social withdrawal. Even children who did not have clinical levels on any CBCL scale showed a three-fold rate of PLI (27%).
According to our two-component hypothesis, the association between ADHD and pragmatic language reported by Helland et al. (20) may reflect an underlying general association rather than a specific association to ADHD. The stable association with behavioral problems reported by others (32) probably reflects an impact mediated by social skills and social problems.
We have found no studies using the ASEBA problem scales in relation to pragmatic language in a psychiatric sample. However, in a general language impaired sample, Coster et al. (33) found a somewhat lower comorbidity of 9% externalized and 16% internalized problems according to parent reports. A study using the SDQ among language impaired children (3) found longitudinal decrease in the associations to conduct and emotional problems but an increase in associated social problems, whereas a group with behavioral problems diagnosed with Kiddie-SADS in a community study (32) found consistent presence of PLI across five years in preadolescence.
Possible explanations for the associations between PLI and mental health
Longitudinal studies suggest that the combination of language impairments tend to persist through development and precede and predict mental health problems rather than follow from them (3, 34-36), although general language problems and social problems also predict future PLI (26), and that children with language problems show an increase in social and emotional problems through childhood (37). Language, communication, social and emotional development are closely connected throughout child development, and considering them as separate well-defined phenomena could lead to oversimplification. They are rather aspects of developmental adaptation connected to emotions and self-regulation as possible driving forces according to Bloom (38). Bishop and Baird (27) have maintained that pragmatic language functioning might also be situationally influenced.
The strong association between pragmatic skills and mental health problems may arise from simple content overlap between the scales regarding social functioning, however, this interpretation does not hold since the PC items and most of the CBCL problem scales do not include social items. In this perspective, the strong associations and high rates of ve, the strong associations and high rates of PLI we found in groups with social problems and social withdrawal may be interpreted as results of reduced social interaction and communicative behavior secondary to social problems and emotional problems. However, deteriorating relationships through the years of development may trigger or worsen emotional problems, behavioral and social problems as well as withdrawal, resulting in a further reduction of communication activity in a vicious circle. The possibility of mutually maintaining effects between poor pragmatic skills and mental health should be studied as individual trajectories rather than longitudinal group differences. Another model worth evaluating is the potential for good pragmatic skills as a protective factor against mental health problems rather than considering pragmatic language problems as a risk factor.
Clinical significance
A routine evaluation of language and communicative skills has not been a standard element of child psychiatric assessments in Norway or most other countries (2,17,39-41). Toppelberg and Shapiro (42) conclude that PLI/low pragmatic skills is likely to remain undiscovered without targeted evaluation. A standard evaluation of language and communication could increase our clinical understanding of the dynamic interplay between each child and his/her context in creating and maintaining the type of problems that result in referral to child psychiatry. More important, the effectiveness of common treatment methods for improving communication and social function should be evaluated (43).
Finding more comorbidity with PLI than linear associations with PC-scores could indicate a third confounding or mediating factor common for PLI and all mental health problems rather than a direct association. However, internalized and social problems may be directly associated to pragmatic skills. The scatterplot in Figure 2 indicates that pragmatic skills is a protective factor against mental health problems, rather than that PLI is a risk factor for or consequence of mental health problems. This clinically meaningful approach could be utilized in prevention as well as treatment, but should be studied more closely longitudinally.
FIGURE 2.
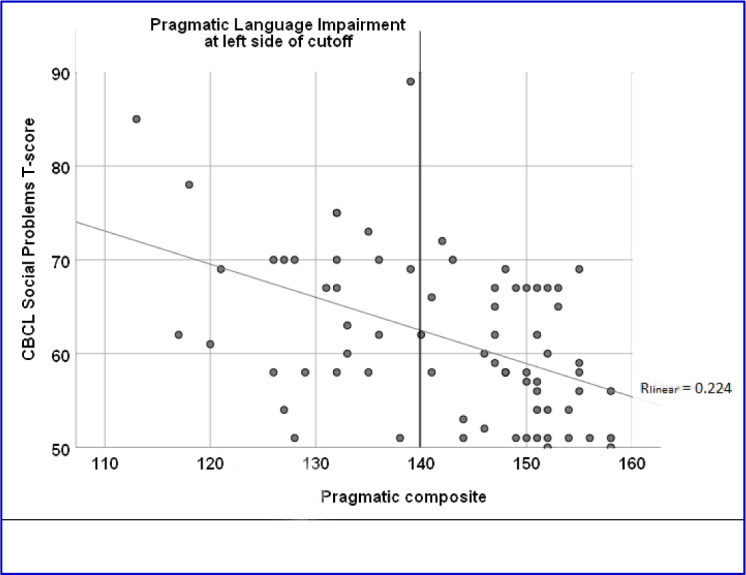
Scatterplot between parental Pragmatic Composite scores and CBCL Social problems T-scores. Cutoff-line for PLI and regression line for the correlation
Strong and weak aspects of the present study
Using a combined dimensional and categorical approach and a simultaneous differentiation between several dimensions of mental health problems expands and clarifies the relationship between pragmatic skills and mental health.
Sample. The sample is a strongly selected sample especially suited to highlight the study aim, but not representing the population variation in any of the focused variables, limiting the possibility for general extrapolations. The sample is, however, a fair representation of mental health problems referred to child psychiatry and has a larger sample than most studies of PLI and mental health. The high prevalence of PLI may reflect a referral practice disproportionally selecting children with combined problems. The lack of a control sample is compensated by comparing to results from reference samples. Excluding autism and intellectual disability focuses the study more clearly on more common mental health problems with a less strong genetic determination, instead of the less frequent an more genetically determined developmental problems. However, this exclusion implies that the sample is not fully representing the variation among children with PLI. Excluding possible autism based of symptom could have led to over-exclusion of social problems, but resulted only in exclusion of two participants. The limited age distribution implies that the influence of age could not be fully evaluated, although analyses were controlled for age. The gender imbalance is also problematic for extrapolation to the total population but is typical for CAMHS clinics. However, control for gender in the analyses did not reveal any gender influence.
Methods. The way of excluding developmental problems may have missed cases with subthreshold disorders, but exclusion based on subclinical symptoms would have excluded cases with social problems with special interest for the study aim. Several earlier studies have not differentiated PLI from other language difficulties and general learning problems or autistic problems, or separated such developmental problems from emotional, social, and behavioral problems. The strength of our study is including all these mental health problems and studying linear associations rather than simple comorbidity. The primary weakness is the cross-sectional design, leaving the process of influence to speculation. The CCC has not been broadly standardized or validated in Norway, and the basis for choosing the cut-off of 140 is limited, but strengthened by the results of the study. The primary argument for using this cut-off was the possibility for comparing with other studies, and is balanced by also analyzing the continuous PC-scores. We therefore maintain that the results are not merely a product of the cut-off point.
Using the CCC-2 might have been better than using the earlier version of the CCC, but the CCC-2 in Norwegian was not available to us at the time of data collection. However, the Norwegian comparison study (17) used CCC rather than CCC2.
The associations between pragmatic scores and symptom scores cannot be explained by content overlap between CBCL and CCC, since the CCC subscale ‘Social Relationships’ does not contribute to the ‘Pragmatic Composite’, and only two items overlap regarding social functioning in other scales.
Conclusion
Pragmatic skills and mental health problems show general as well as specific associations. PLI seems highly comorbid with mental health problems in general, and low PC-scores show especially strong associations specifically with social problems and withdrawal, but also anxiety and rumination. Despite comorbidity between PLI and externalizing problems, there is no significant association between PC-scores and externalizing symptom scores, indicating a third common or mediating factor between pragmatic skills and mental health problems.
Much earlier research did not differentiate between pragmatic and specific language problems, did not compare specific categories of mental health problems, did not focus on children without more pervasive developmental disorders such as autism and intellectual disability and did not use a combination of dimensional and categorical approach. These differences in specification may in part explain the inconsistent reports regarding symptom associations and comorbidity reported from research on language impairment and mental health problems.
The high prevalence of PLI among children who are referred to child psychiatry suggests the need to introduce a standard evaluation of language and communication skills to be used before referring a child to psychiatry or as a mandatory element of clinical assessment procedures.
Acknowledgements
Thanks to the clinicians at Levanger hospital recruiting patient and their parents for the study and contributing in the data-collection as part of their daily clinical work.
Footnotes
Ethics
The Norwegian Social Science Data Services approved the study after the Regional Board of Medical Research Ethics had evaluated the project as being outside their scope. The study complies with the Helsinki Declaration.
Conflicts of interest
None of the authors has any conflicting interests to report.
References
- 1.Cohen NJ. (Ed.). Unsuspected language impairments in psychiatrically disturbed children: developmental issues and associated conditions. Cambridge: University Press; 1996. [Google Scholar]
- 2.Cohen NJ, Barwick MA, Horodezky NB, Vallance DD, Im N. Language, achievement, and cognitive processing in psychiatrically disturbed children with previously identified and unsuspected language impairments. J Child Psychol Psychiatry 1998;39:865-77. [PubMed] [Google Scholar]
- 3.St Clair MC, Pickles A, Durkin K, Conti-Ramsden G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (SLI). J Commun Disord 2011;44:186-99. [DOI] [PubMed] [Google Scholar]
- 4.Conti-Ramsden G, Botting N. Emotional health in adolescents with and without a history of specific language impairment. J Child Psychol Psychiatry 2008;49:516-25. [DOI] [PubMed] [Google Scholar]
- 5.Bloom LJ, Lahey M. Language development and language disorders. New York, NY: Wiley; 1978. [Google Scholar]
- 6.Bishop DV. Development of the Children’s Communication Checklist (CCC): a method for assessing qualitative aspects of communicative impairment in children. J Child Psychol Psychiatry 1998;39:879-91. [PubMed] [Google Scholar]
- 7.Baker L, Cantwell DP. Psychiatric disorder in children with different types of communication disorders. J Commun Disord 1982;15:113-26. [DOI] [PubMed] [Google Scholar]
- 8.Beitchman JH, Wilson B, Johnson CJ, Atkinson L, Young A, Adlaf E, et al. Fourteen-year follow-up of speech/language-impaired and control children: psychiatric outcome. J Am Acad Child Adolesc Psychiatry 2001;40:75-82. [DOI] [PubMed] [Google Scholar]
- 9.Bishop DVM. Uncommon understanding: development and disorders of language comprehension in children. Hove: Psychology Press; 1997. [Google Scholar]
- 10.Fujiki M, Brinton B. Pragmatics and social communication in child language disorders In: Schwartz RG. (Ed.). Handbook of child language disorders, New York, Psychology Press; 2009:406-23. [Google Scholar]
- 11.Poletti M. A neuropsychological approach to the etiology of pragmatic language impairment. Clin Neuropsychiatry. 2011;8:287-94. [Google Scholar]
- 12.Im-Bolter N, Cohen NJ. Language impairment and psychiatric comorbidities. Pediatr Clin N Am 2007;54:525-42. [DOI] [PubMed] [Google Scholar]
- 13.Anglada E, Kinoo P, Poncin F, Wintgens A. Semantic-pragmatic disorder: syndrome or symptom? Ann Med-Psychol 2016;174:665-71. [Google Scholar]
- 14.Ebbels S. Introducing the SLI debate. Int J Lang Commun Disord 2014;49:377-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Swineford L, Thurm A, Baird G, Wetherby A, Swedo S. Social (pragmatic) communication disorder: a research review of this new DSM-5 diagnostic category. J Neurodevelop Disord 2014;6:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Conti-Ramsden G, Botting N. Social difficulties and victimization in children with SLI at 11 years of age. J Speech Lang Hear Res 2004;47:145-61. [DOI] [PubMed] [Google Scholar]
- 17.Helland WA, Heimann M. Assessment of pragmatic language impairment in children referred to psychiatric services: A pilot study of the Children’s Communication Checklist in a Norwegian sample. Logoped Phoniatr Vocol 2007;32:23-30. [DOI] [PubMed] [Google Scholar]
- 18.Farmer M, Oliver A. Assessment of pragmatic difficulties and socio-emotional adjustment in practice. Int J Lang Commun Disord 2005;40:403-29. [DOI] [PubMed] [Google Scholar]
- 19.Ketelaars MP, Cuperus J, Jansonius K, Verhoeven L. Pragmatic language impairment and associated behavioural problems. Int J Lang Commun Disord 2010;45:204-14. [DOI] [PubMed] [Google Scholar]
- 20.Helland WA, Posserud MB, Helland T, Heimann M, Lundervold AJ. Language impairments in children with ADHD and in children with reading disorder. J Atten Disord 2016;20:581-9. [DOI] [PubMed] [Google Scholar]
- 21.Leonard MA, Milich R, Lorch EP. The role of pragmatic language use in mediating the relation between hyperactivity and inattention and social skills problems. J Speech Lang Hear Res 2011;54:567-79. [DOI] [PubMed] [Google Scholar]
- 22.Mackie L, Law J. Pragmatic language and the child with emotional/behavioural difficulties (EBD): a pilot study exploring the interaction between behaviour and communication disability. Int J Lang Commun Disord 2010;45:397-410. [DOI] [PubMed] [Google Scholar]
- 23.Gilmour J, Hill B, Place M, Skuse D, Gilmour J. Social communication deficits in conduct disorder: a clinical and community survey. J Child Psychol Psychiatry 2004;45:967-78. [DOI] [PubMed] [Google Scholar]
- 24.Donno R, Parker G, Gilmour J, Skuse DH. Social communication deficits in disruptive primary-school children. Br J Psychiatry 2010;196:282-9. [DOI] [PubMed] [Google Scholar]
- 25.Gibson J, Adams C, Lockton E, Green J. Social communication disorder outside autism? A diagnostic classification approach to delineating pragmatic language impairment, high functioning autism and specific language impairment. J Child Psychol Psychiatry 2013;54:1186-97. [DOI] [PubMed] [Google Scholar]
- 26.Helland WA, Lundervold AJ, Heimann M, Posserud M-B. Stable associations between behavioral problems and language impairments across childhood – the importance of pragmatic language problems. Res Dev Disabil 2014;35:943-51. [DOI] [PubMed] [Google Scholar]
- 27.Bishop DVM, Baird G. Parent and teacher report of pragmatic aspects of communication: use of the children’s communcation checklist in a clinical setting. Dev Med Child Neurol 2001;43:809-18. [DOI] [PubMed] [Google Scholar]
- 28.Schjølberg S, Thorkildsen NP. Sjekkliste for barns kommunikasjon (CCC). [Bishop D. Children’s Communication Checklist]. Oslo: Senter for barne og ungdomspsykiatri; 1998. [Google Scholar]
- 29.Wechsler D. Wechsler intelligence scale for children. San Antonio, TX: The Psychological Corporation; 1991. [Google Scholar]
- 30.Benasich A, Curtiss S, Tallal P. Language, learning, and behavioral disturbances in childhood; a longitudinal perspective. J Am Acad Child Adolesc Psychiatry 1993;32:585-94. [DOI] [PubMed] [Google Scholar]
- 31.Helland WA, Biringer E, Helland T, Heimann M. The usability of a Norwegian adaptation of the Children’s Communication Checklist Second Edition (CCC-2) in differentiating between language impaired and non-language impaired 6- to 12-year-olds. Scand J Psychol 2009;50:287-92. [DOI] [PubMed] [Google Scholar]
- 32.Helland WA, Lundervold AJ, Heimann M, Posserud MB. Stable associations between behavioral problems and language impairments across childhood – the importance of pragmatic language problems. Res Dev Disabil 2014;35:943-51. [DOI] [PubMed] [Google Scholar]
- 33.Coster F, Goorhuis-Brouwer S, Nakken H, Spelberg H. Specific language impairments and behavioural problems. Folia Phoniatr Logop 1999;51:99-107. [DOI] [PubMed] [Google Scholar]
- 34.Snowling M, Bishop D, Stothard S, Chipchase B, Kaplan C. Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment. J Child Psychol Psychiatry 2006;47:759-65. [DOI] [PubMed] [Google Scholar]
- 35.Cohen NJ. Language impairment and psychopatology in infants, children and adolescents. Thousand Oaks, CA: Sage Publications; 2001. [Google Scholar]
- 36.Cohen NJ. Language impairment and psychopathology in infants, children, and adolescents. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- 37.Beitchman JH, Brownlie EB, Inglis A, Wild J, Ferguson B, Schachter D, et al. Seven-year follow-up of speech/language impaired and control children: psychiatric outcome. J Child Psychol Psychiatry 1996;37:961-70. [DOI] [PubMed] [Google Scholar]
- 38.Bloom L. The transition from infancy to language: acquiring the power of expression Cambridge: Cambridge University Press; 1993. [Google Scholar]
- 39.Gallagher T. Interrelationships among children with language, behaviour and emotional problems. Top Lang Disord 1999;19:1-15. [Google Scholar]
- 40.Goodyear IM. (Ed.). Language difficulties and psychopatology. Hove: Psychological Press; 2000. [Google Scholar]
- 41.Ottem E, Thorseng LA, Duna KE, Green T. Språkvansker og psykisk helse [Language difficulties and mental health]. Norsk tidsskrift for spesialpedagogikk. 2002;80:114-24. [Google Scholar]
- 42.Toppelberg CO, Shapiro T. Language disorders: a 10-year research update review. J Am Acad Child Adolesc Psychiatry 2000;39:143-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Prizant B, Audet L, Burke G, Hummel L, Maher S, Theadore G. Communication disorders and emotional/behavioral disorders in children and adolescents. J Speech Hear Disord 1990;55:179-92. [DOI] [PubMed] [Google Scholar]