

Abstract
Background:
It has been reported that polymorphisms of transferrin (TF) G258A and transferrin receptor (TFR) A82G might be associated with susceptibility to Parkinson disease (PD).
Objective:
Owing to limitation of sample size and inconclusive results, we conducted a meta-analysis to clarify the association.
Methods:
By searching PubMed, Embase, Chinese National Knowledge Infrastructure, China Biological Medicine Database, and Wanfang Databases, the published articles about studies of the association of the TF G258A, TFR A82G gene polymorphisms with the risk of PD were collected. Q-statistics and I2 statistics were calculated to examine heterogeneity and summary odds ratios (ORs) and 95% confidence intervals (95%CI) were evaluated the association.
Results:
Five studies assessed the relationship between TF G258A and risk of PD. A significant increased protective of A allele and AA genotype was observed in allele model and recessive model (the allele model A vs G: OR = 0.54, 95%CI 0.40–0.72, P < .001; the recessive model AA vs GA + GG: OR = 0.32, 95%CI 0.20–0.52, P < .001). The remaining models of the TF G258A genotype showed no significant association with PD risk, while the protective tendency were increased (the heterozygote model GA vs GG: OR = 0.93, 95%CI 0.61–1.43, P = .75; the homozygous model AA vs GG: OR = 0.47, 95%CI 0.21–1.04, P = .06; the dominant model GA + AA vs GG: OR = 0.75, 95%CI 0.50–1.11, P = .15). There was also a lack of association between TFR A82G polymorphism and PD (the allele model G vs A: OR = 0.92, 95%CI 0.75–1.13, P = .43; the heterozygote model AG vs AA: OR = 1.17, 95%CI 0.79–1.71, P = .43; the homozygous model GG vs AA: OR = 0.91, 95%CI 0.60–139, P = .66; the dominant model AG + GG vs AA: OR = 1.05, 95%CI 0.73–1.49, P = .81; the recessive model GG vs AG +AA: OR = 0.80, 95%CI 0.59–1.09, P = .16).
Conclusion:
Our study suggests that TF G258A polymorphism may be associated with PD, while TFR A82G polymorphism may not contribute to PD based on the current evidence.
Keywords: Parkinson disease, polymorphism, transferrin G258A, transferrin receptor A82G
1. Introduction
Parkinson disease (PD) is acknowledged as the second most neurodegenerative disorder after Alzheimer disease, with an overall prevalence in the general population of 0.3%.[1] It is a debilitating neurological disorder characterized by resting tremor, muscular rigidity, bradykinesia, and postural instability.[2] The main pathological feature is the progressive loss of dopaminergic neurons in the substantia nigra and presence of a-synuclein containing Lewy bodies.[3,4] Previous studies have shown that the accumulation of iron in the brain plays a key role in the pathogenesis of PD.[5] Iron increases oxidative stress, induces neuronal degeneration,[6,7] and accumulates in the substantia nigra of PD patients.[8] In view of this, genes coding proteins involved in iron metabolism could be considered as potential susceptibility genes for PD.
Transferrin (TF) is primarily involved in iron uptake through the transfer receptor (TFR).[9,10] TF-iron (TF-Fe) first binds to TFR on the cell surface and then the TF-Fe- TFR complex is rapidly endocytosed by cells, which eventually bud off to form coated vesicles, called endosomes. The endosomes pondus Hydrogenii (pH) is lowered to about 5 to 6. At this time, TF-Fe- TFR complex releases its bound iron, and the TF-TFR returns to the cell surface. At physiological pH, TFR dissociates and TF returns to the circulatory system and binds iron. Loss of transferrin receptor 1, involved in iron uptake, caused neuronal iron deficiency, age-progressive degeneration of a subset of dopaminergic neurons, and motor deficits.[11] There was gradual depletion of dopaminergic projections in the striatum followed by death of dopaminergic neurons in the substantia nigra. Although the functional significance of the TF G258A polymorphism is unclear, current studies suggest that the A allele encodes the mature serine and replaces the usual glycine,[12] and that TF G258A variants may be associated with the total value of the iron-binding capacity.
Recent studies have also shown that single nucleotide polymorphisms in TF and TFR have a functional impact on PD. There are some reports on the correlation between TF G258A, TFR A82G gene polymorphism, and PD in different populations, but the results are contrary.[13–17] There is no review that has attempted to synthesize the total available evidence of the TF G258A and TFR A82G gene polymorphisms in the risk of PD. The purpose of the present paper is to investigate the association of the TF G258A and TFR A82G gene polymorphisms with the risk of PD by meta-analysis.
2. Materials and methods
2.1. Study collection
We search for relevant papers that had been published in English or Chinese through PubMed, Embase, Chinese National Knowledge Infrastructure (CNKI), China Biological Medicine (CBM) Database, and Wanfang Database (up to December 2019). The search strategy was limited to the following keywords (Transferrin or TF G258A), (Transferrin receptor or TFR A82G), and (Parkinson disease or PD).
2.2. Inclusion and exclusion criteria
All papers included in this meta-analysis must be meet the following criteria: investigating the association TF G258A and (or) TFR A82G gene polymorphism and PD, human studies and case-controlled studies, the number of studies of genotypes must be completely provided in both case and control groups directly or indirectly. On the contrary, studies without control, abstract, review, comment, unsuitable genotype frequency data (not TF G258A or TFR A82G), and duplicate publication are excluded.
2.3. Data extraction
Data were extracted by 2 independent reviewers. Extraction of literature, including: first author, year of publication, country of study, and the numbers of genotyped cases and controls. Any disagreements on data extraction were resolved through discussion with other researchers.
2.4. Ethical approval
All data in this meta-analysis were extracted from the previous published studies, no ethical approval or patient consent was required.
2.5. Statistical analysis
Review Manager 5.3 software (Cochrane Collaboration, Oxford, UK) was used for meta-analysis as following: five different odds ratio (ORs) were computed: allele model (A vs G for TF G258A and G vs A for TFR A82G); heterozygote model (GA vs GG for TF G258A and AG vs AA for TFR A82G); homozygous model (AA vs GG for TF G258A and GG vs AA for TFR A82G); dominant model (GA + AA vs GG for TF G258A and AG + GG vs AA for TFR A82G); recessive model (AA vs GA + GG for TF G258A and GG vs AG + AA for TFR A82G). Heterogeneity between studies was assessed using the Chi-square-based Q test and the I2 test. If the I2 was >50%, the pooled study OR estimate of the study was calculated using a random-effects model. Otherwise, the fixed effects model was used. P < .05 was considered statistically significant. Stata (version12.0) was used for this article as follows: Hardy–Weinberg equilibrium (HWE) test, Begg test, and Egger test for publication bias.
3. Results
3.1. Characteristics of studies
According to the above retrieval methods, a total of 130 relevant studies were selected. After reviewing the full text, 125 studies were excluded due to duplicated studies and irrelevant articles (Fig. 1). Finally, 5 studies[13–17] were included, 3 published in English[13–15] and 2 in Chinese.[16,17] The main characteristics of the eligible studies are presented in Table 1. All 5 studies evaluated the association between TF G258A and PD susceptibility,[13–17] and 4 of them evaluated the roles of TFR A82G in the risk of PD.[13,15–17] The 5 case–control studies included in this meta-analysis encompassed a total of 708 PD cases and 619 controls on the TF G258A polymorphism, and 4 of them included 433 PD cases and 459 controls for the TFRA82G polymorphism. The genotype for each study and HWE of controls are summarized in Table 1.
Figure 1.
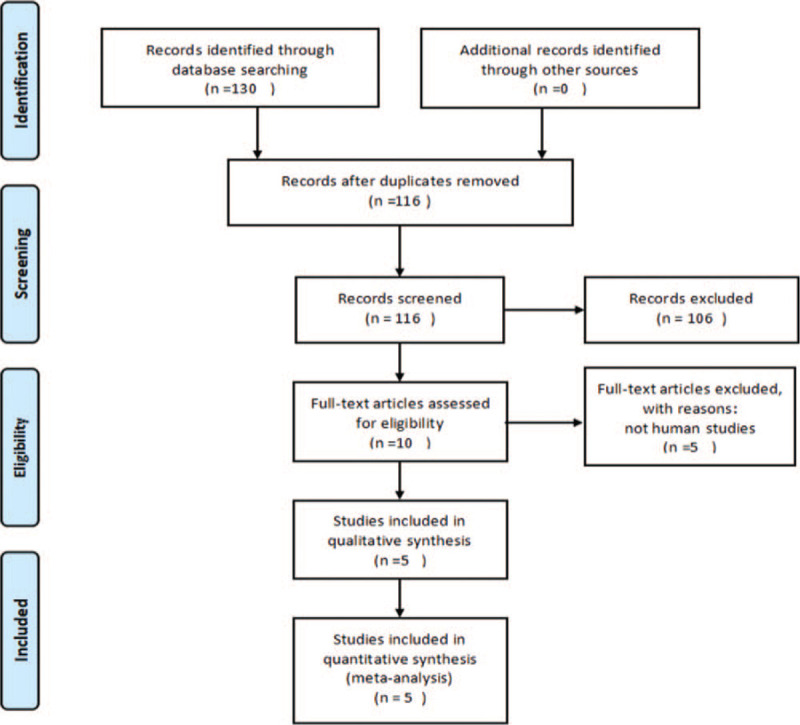
Flowchart of study selection for the present study.
Table 1.
The characteristics of the included studies in the meta-analysis.
| Study | Area | No. of cases | No. of controls | Cases | Controls | P for HWE |
| TF G258A | GG GA AA | GG GA AA | ||||
| Borie et al, 2002 | France | 133 | 116 | 122 8 3 | 98 12 6 | <.001 |
| Ezquerra et al, 2005 | Spain | 210 | 103 | 190 20 0 | 95 7 1 | .06 |
| Greco et al, 2011 | Italy | 181 | 180 | 165 16 0 | 159 21 0 | .41 |
| Xiao et al, 2015 | China | 117 | 140 | 6 31 80 | 5 13 122 | <.001 |
| Xiao et al, 2018 | China | 67 | 80 | 2 19 46 | 2 8 70 | .01 |
| TFR A82G | AA AG GG | AA AG GG | ||||
| Borie et al, 2002 | France | 68 | 59 | 15 36 17 | 15 26 18 | .37 |
| Greco et al, 2011 | Italy | 181 | 180 | 47 96 38 | 50 89 41 | .91 |
| Xiao et al, 2015 | China | 117 | 140 | 12 25 80 | 12 26 102 | <.001 |
| Xiao et al, 2018 | China | 67 | 80 | 3 11 53 | 3 8 69 | <.001 |
3.2. Meta-analysis results
Five studies assessed the relationship between TF G258A gene polymorphisms and PD. The I2 value was lower 50%, indicating no heterogeneity. Therefore, a fixed-effects model was used in all genetic models. The combined results suggested that TF G258A polymorphism could be associated with PD (the allele model A vs G: OR = 0.54, 95%CI 0.40–0.72, P < .001; the recessive model AA vs GA + GG: OR = 0.32, 95%CI 0.20–0.52, P < .001) (Table 2, Supplemental Digital Content [Figure S1, Figure S5]), and A allele and AA genotype showed significant protective. Although the heterozygous model, homozygous model and the dominant model did not show a significant association with the risk of PD, the protective tendency increased (the heterozygote model GA vs GG: OR = 0.93, 95%CI 0.61–1.43, P = .75; the homozygous model AA vs GG: OR = 0.47, 95%CI 0.21–1.04, P = .06; the dominant model GA + AA vs GG: OR = 0.75, 95%CI 0.50–1.11, P = .15) (Table 2, Supplemental Digital Content [Figures S2, S3, and S4]). One study with a small number of cases was eliminated for sensitivity analysis, and the other 4 studies were re-analyzed. The results showed that the lack of cases still had no effect on the results of the meta-analysis in these 4 studies (data are not shown).
Table 2.
Meta-analysis of TF G258A/TFR A82G polymorphism and risk of PD.
| Genetic comparison | Begg test (z, p) | Egger test (z, p) | I2 (%) | Fixed model OR [95%CI] POR |
| TF G258A | ||||
| A vs G | 0.73, 0.462 | 1.36, 0.266 | 33 | 0.54 [0.40, 0.72] <.001 |
| GA vs GG | 0.24, 0.806 | 1.48, 0.235 | 14 | 0.93 [0.61, 1.43] .75 |
| AA vs GG | 0.00, 1.000 | 0.43, 0.744 | 0 | 0.47 [0.21, 1.04] .06 |
| GA + AA vs GG | 0.24, 0.806 | 0.18, 0.870 | 0 | 0.75 [0.50, 1.11] .15 |
| AA vs GA + GG | 0.00, 1.000 | 1.84, 0.316 | 0 | 0.32 [0.20, 0.52] <.001 |
| TFR A82G | ||||
| G vs A | 1.02, 0.308 | -2.33, 0.145 | 0 | 0.92 [0.75, 1.13] .43 |
| AG vs AA | -0.34, 1.000 | 0.32, 0.781 | 0 | 1.17 [0.79, 1.71] .43 |
| GG vs AA | 0.34, 0.734 | -1.21, 0.351 | 0 | 0.91 [0.60, 1.39] .66 |
| AG + GG vs AA | 0.34, 0.734 | -0.87, 0.478 | 0 | 1.05 [0.73, 1.49] .81 |
| GG vs AG + AA | 1.70, 0.089 | -2.94, 0.099 | 0 | 0.80 [0.59, 1.09] .16 |
The association between TFR A82G polymorphism and the risk of PD was analyzed in 4 independent studies. Fixed-effects model was used in all genetic models. When all eligible studies were pooled in this meta-analysis, no significant association was seen in all genetic models (the allele model G vs A: OR = 0.92, 95%CI 0.75–1.13, P = .43; the heterozygote model AG vs AA: OR = 1.17, 95%CI 0.79–1.71, P = .43; the homozygous model GG vs AA: OR = 0.91, 95%CI 0.60–1.39, P = .66; the dominant model AG + GG vs AA: OR = 1.05, 95%CI 0.73–1.49, P = .81; the recessive model GG vs AG +AA: OR = 0.80, 95%CI 0.59–1.09, P = .16) (Table 2, Supplemental Digital Content [Figures S6, S7, S8, S9, and S10]). A consistent result was obtained when the sensitivity analysis was used to evaluate the association between TFR A82G polymorphism and PD susceptibility (data are not shown).
3.3. Publication bias
Begg test and Egger test were performed to evaluate the publication bias. No evidence of publication bias was existed in all genetic models (Table 2).
4. Discussion and conclusions
PD is considered a multi-factorial disease, in which iron overload and alterations of iron-related genes play an important role. More recent studies showed an involvement of iron-mediated oxidative stress in the pathogenesis of PD.[18] Increased levels of iron deposits have been described in the substantia nigra and globus pallidus by both postmortem and imaging studies.[19,20] Meanwhile, human studies investigating various genes involved in iron metabolism or homeostasis for associations with PD have been reviewed.[21]
Previous studies have evaluated the association between the genetic polymorphisms TF G258A and TFR A82G and the risk of PD with controversial results. In this meta-analysis, we have observed a significant increase in protection of the A allele and the AA genotype between TF G258A genetic polymorphisms and susceptibility of PD. These results are consistent with 3 previous studies,[13,16,17] contrasting the results of 2 others.[14,15] However, the TFR A82G genotype models did not show a significant association, consistent with previous research results.[13,15–17]
In the present meta-analysis, 5 case–control studies with total of 708 PD cases and 619 controls on TF G258A polymorphism were finally identified to be eligible studies. And 4 studies including 433 PD cases and 459 controls for TFR A82G polymorphism were identified. As the I2 < 50%, the fixed-effect model was used to calculate the pooled OR in this meta-analysis. These pooled results demonstrated a protective effect on TF G258A polymorphism, while analysis of the TFR A82G polymorphism in PD patients did not revealed a significant association. Not all studies conformed to the HWE. In the sensitivity analysis, eliminating a study with a small number of cases gave a similar result. There was no evidence of publication bias in our meta-analysis. However, it should be noted that the power of the Egger regression test and Begg test to detect bias will be low with a small number of studies. The Begg test is nonparametric, which reduces its power.
There were some limitations in our study. First, our research only focuses on English and Chinese articles, which could bias the result. Second, the results of this study are subject to large sample, multicenter collaboration, and more randomized controlled trials for validation. Due to limited data, we did not perform a subgroup analysis for another factor that may contribute to PD. Moreover, the study may be influenced by gene–environment interactions and intergenic interactions.
In summary, the results of this meta-analysis indicate that TF G258A polymorphism was associated with genetic susceptibility of PD, while TFR A82G polymorphism may not contribute to PD base on the currently published studies. We need more high-quality, well-designed studies with large sample sizes to confirm these findings.
Author contributions
Conceptualization: Xun Deng.
Methodology: Deqi Jiang.
Resources: Xun Deng.
Software: Minhua Zhou.
Writing – original draft: Yan Wang.
Writing – review & editing: Yong Wang.
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Footnotes
Abbreviations: 95%CI = 95% confidence intervals, HWE = Hardy–Weinberg equilibrium, ORs = odds ratios, PD = Parkinson disease, pH = pondus Hydrogenii, TF = transferrin, TFR = transferrin receptor.
How to cite this article: Wang Y, Wang Y, Zhou M, Jiang D, Deng X. Association of transferrin G258A and transferrin receptor A82G polymorphisms with the risk of Parkinson disease in certain area. Medicine. 2020;99:48(e23432).
This study was supported by the Medical Research Projects of Foshan Municipal Health Bureau (NO.20200352) and the Foshan Science and Technology Innovation Project (NO.1920001001440).
The authors have no conflicts of interest to disclose.
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Supplemental digital content is available for this article.
HWE assumes that allele and genotype frequencies in population will remain constant from generation to generation in the absence to other evolutionary influences. Consider a population of monoecious diploids, where each organism produces male and female gametes at equal frequency, and has 2 alleles at each gene locus. The allele frequencies at each generation are obtained by pooling together the alleles from each genotype of the same generation according to the expected contribution from the homozygote and heterozygote genotypes.
HWE = Hardy–Weinberg equilibrium, TF = transferrin, TFR = transferrin receptor.
The values in bold represent that there are statistically significant differences between cases and controls.
CI = confidence interval, OR = odds ratio, TF = transferrin, TFR = transferrin receptor.
References
- [1].Nussbaum RL, Ellis CE. Alzheimer's disease and Parkinson's disease. N Engl J Med 2003;348:1356–64. [DOI] [PubMed] [Google Scholar]
- [2].Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17:427–42. [DOI] [PubMed] [Google Scholar]
- [3].Pollanen MS, Dickson DW, Bergeron C. Pathology and biology of the Lewy body. J Neuropathol Exp Neurol 1993;52:183–91. [DOI] [PubMed] [Google Scholar]
- [4].Kuzuhara S, Mori H, Izumiyama N, et al. Lewy bodies are ubiquitinated. A light and electron microscopic immunocytochemical study. Acta Neuropathol 1988;75:345–53. [DOI] [PubMed] [Google Scholar]
- [5].Gerlach M, Double KL, Youdim MB, et al. Potential sources of increased iron in the substantia nigra of parkinsonian patients. J Neural Transm Suppl 2006;133–42. [DOI] [PubMed] [Google Scholar]
- [6].Shoham S, Youdim MB. Iron involvement in neural damage and microgliosis in models of neurodegenerative diseases. Cell Mol Biol (Noisy-le-grand) 2000;46:743–60. [PubMed] [Google Scholar]
- [7].Wang X, Manganaro F, Schipper HM. A cellular stress model for the sequestration of redox-active glial iron in the aging and degenerating nervous system. J Neurochem 1995;64:1868–77. [DOI] [PubMed] [Google Scholar]
- [8].Dexter DT, Wells FR, Lees AJ, et al. Increased nigral iron content and alterations in other metal ions occurring in brain in Parkinson's disease. J Neurochem 1989;52:1830–6. [DOI] [PubMed] [Google Scholar]
- [9].Aisen P, Wessling-Resnick M, Leibold EA. Iron metabolism. Curr Opin Chem Biol 1999;3:200–6. [DOI] [PubMed] [Google Scholar]
- [10].Ponka P. Cellular iron metabolism. Kidney Int Suppl 1999;69:S2–11. [DOI] [PubMed] [Google Scholar]
- [11].Matak P, Matak A, Moustafa S, et al. Disrupted iron homeostasis causes dopaminergic neurodegeneration in mice. Proc Natl Acad Sci USA 2016;113:3428–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Beckman LE, Van Landeghem GF, Sikstrom C, et al. DNA polymorphisms and haplotypes in the human transferrin gene. Hum Genet 1998;102:141–4. [DOI] [PubMed] [Google Scholar]
- [13].Borie C, Gasparini F, Verpillat P, et al. Association study between iron-related genes polymorphisms and Parkinson's disease. J Neurol 2002;249:801–4. [DOI] [PubMed] [Google Scholar]
- [14].Ezquerra M, Campdelacreu J, Munoz E, et al. Association study of the G258S transferrin gene polymorphism and Parkinson's disease in the Spanish population. J Neurol 2005;252:1269–70. [DOI] [PubMed] [Google Scholar]
- [15].Greco V, De Marco EV, Rocca FE, et al. Association study between four polymorphisms in the HFE. TF and TFR genes and Parkinson's disease in southern Italy. Neurol Sci 2011;32:525–7. [DOI] [PubMed] [Google Scholar]
- [16].Huang W, Zhou R, Li J, et al. Association of the TNF-alpha-308, TNF-alpha-238 gene polymorphisms with risk of bone-joint and spinal tuberculosis: a meta-analysis. Biosci Rep 2019;39:BSR20182217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Shen ML, Xiao A, Yin SJ, et al. Associations between UGT2B7 polymorphisms and cancer susceptibility: a meta-analysis. Gene 2019;706:115–23. [DOI] [PubMed] [Google Scholar]
- [18].Snyder AM, Connor JR. Iron, the substantia nigra and related neurological disorders. Biochim Biophys Acta 2009;1790:606–14. [DOI] [PubMed] [Google Scholar]
- [19].Dexter DT, Wells FR, Agid F, et al. Increased nigral iron content in postmortem parkinsonian brain. Lancet 1987;2:1219–20. [DOI] [PubMed] [Google Scholar]
- [20].Loeffler DA, Connor JR, Juneau PL, et al. Transferrin and iron in normal. Alzheimer's disease, and Parkinson's disease brain regions. J Neurochem 1995;65:710–24. [DOI] [PubMed] [Google Scholar]
- [21].Rhodes SL, Ritz B. Genetics of iron regulation and the possible role of iron in Parkinson's disease. Neurobiol Dis 2008;32:183–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.