

Abstract
Research suggests that elite athletes are at increased risk of poor mental health, partly due to the intense demands associated with top-level sport. Despite growing interest in the topic, the factors that influence the mental health and well-being of elite athletes remain unclear. From a theoretical perspective, the accumulation of stress and adversity experienced over the life course may be an important factor. To investigate this possibility, we employed a mixed-method design to: (a) examine whether cumulative lifetime stress predicted depression, anxiety, and well-being in elite athletes; and (b) help explain why cumulative lifetime stress exposure might have resulted in poor mental health and well-being. Ninety-five elite athletes (Mage = 29.81, SD = 10.88) completed the Stress and Adversity Inventory, Patient Health Questionnaire, Generalized Anxiety Disorder 7-item scale, and the Scales of General Well-Being. Hierarchical regression analyses revealed that total count and severity of lifetime stressor exposure significantly predicted greater depression (β = .42, p < .001; β = .46, p < .001) and anxiety symptoms (β = .34, p = .003; β = .28, p = .018), and worse well-being (β = −.42, p < .001; β = −.30, p = .015). Semi-structured interviews were then conducted with six athletes. Thematic analysis revealed that cumulative lifetime stress exposure fostered poor mental health and well-being by promoting maladaptive long-term coping strategies, increasing susceptibility to future stress, and limiting interpersonal relationships. We believe these findings can help practitioners identify, and intervene accordingly with, elite athletes at risk of experiencing stress-related mental health problems.
Keywords: Adversity, Allostatic load, Life stress, Mental health, Performance, Pressure, Sport, Trauma
Recent research has suggested that elite athletes are at increased risk of mental health problems (Gorczynski, Coyle, & Gibson, 2017), partly due to the intense demands they encounter during their sporting careers, including sport (e.g., injury, pressure to perform) and non-sport (e.g., bereavement, abuse) stressors (Fletcher, Hanton, & Mellalieu, 2006). Indeed, research has found that elite-level athletes typically experience stressors that are associated with their sporting organization more frequently, at a higher intensity, and for longer durations than athletes competing at lower levels (Arnold, Fletcher, & Daniels, 2016). At times of increased stress, athletes appear to be more susceptible to experiencing depression and anxiety (Rice et al., 2016). Moreover, although some scholars suggest that the prevalence of psychiatric symptomology in elite athletes is similar to the general population (Gorczynski et al., 2017; Rice et al., 2016), elite athletes may not recognize, acknowledge, or seek support for their mental health problems (Gorczynski et al., 2017). As such, the increasing prevalence of mental ill-health among elite athletes (Foskett & Longstaff, 2018), coupled with the concealment of such illnesses, suggest that it is crucial to identify at-risk athletes to provide timely access to treatment. Despite increasing interest in the topic (e.g., Moesch et al., 2018), researchers have yet to clearly identify the factors that influence the mental health and well-being of elite athletes. To address this issue, this study examined how prior exposure to lifetime stress and adversity was related to the mental health and well-being of elite athletes, using the integrative model of lifespan stress and health as a theoretical framework (Epel et al., 2018).
The integrative model seeks to understand how individual components of the stress process interact over the lifespan to influence health and well-being (Epel et al., 2018). From this perspective, cumulative lifetime stress exposure refers to the total count or severity of all of the stressors that a person has experienced across their lifespan (Lam, Shields, Trainor, Slavich, & Yonelinas, 2019). The integrative model is of particular relevance as it introduces important conceptual dimensions of cumulative lifetime stress, whereby stressors are distinguished by their timing (i.e., early life vs. adulthood), type (i.e., acute life events vs. chronic difficulties), primary life domain (e.g., housing, education, work), and social-psychological characteristic (e.g., interpersonal loss, humiliation, entrapment). This conceptual differentiation is important, given that different types of stressors have varying effects on health and well-being (Epel et al., 2018). Well-being, in turn, is defined as a multidimensional and complex construct with two distinct perspectives: hedonic and eudaimonic (Neil, McFarlane, & Smith, 2017). Whereas the hedonic perspective focuses on the subjective experience of happiness and life satisfaction, the eudaimonic perspective focuses on psychological functioning and self-realization (Ryan & Deci, 2001). Moreover, mental health is defined by the World Health Organization (2004) as “a state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community” (p. 12). Pursuant with the predictions of the integrative model, it is important to identify the specific types of stressors that are particularly harmful for health (Epel et al., 2018).
Broadly speaking, the effect of cumulative lifetime stress exposure has recently been examined in relation to a variety of psychological, biological, and clinical outcomes (e.g., Olvera Alvarez et al., 2019; Pegg et al., 2019). The consensus from this body of work is that as the incidence of acute life events and chronic difficulties increases, so too does the risk for poor health outcomes (Slavich & Shields, 2018). For example, greater lifetime stress exposure has been associated with greater depression and anxiety in adolescents (e.g., Slavich, Stewart, Esposito, Shields, & Auerbach, 2019; Toussaint, Shields, Dorn, & Slavich, 2016), with cumulative stressor severity being a relatively stronger predictor than the total count of stressors experienced (Slavich et al., 2019). In addition, chronic difficulties have been found to be a marginally stronger predictor of depression and anxiety than acute life events (Slavich et al., 2019). Although this quantitative, population-based research is insightful, combining this approach with qualitative methods may help researchers better understand precisely how cumulative lifetime stress affects mental health and well-being (e.g., by highlighting potential underlying mechanisms; Greene, Caracelli, & Graham, 1989).
In addition to the aforementioned findings, emerging research within a sport context suggests that experiencing moderate amounts of adversity can lead to enhanced psychological resilience (e.g., Fletcher, 2019; Fletcher & Sarkar, 2012), psychosocial growth (e.g., Howells & Fletcher, 2015), and more optimal sports performance (e.g., Moore, Young, Freeman, & Sarkar, 2017). For example, Hardy et al. (2017) reported that early life non-sport adversity was a consistent feature in Olympic and world champions lives, particularly when experienced closely to a positive sport-related event. Despite these emergent findings, researchers in sport have predominantly examined how the frequency of adverse life events is associated with performance-related outcomes (e.g., Moore et al., 2017). This differs from examining the combined and cumulative effect of stressors occurring across an athlete’s lifespan (Fletcher, 2019). Accordingly, additional research is required that adopts a more multidimensional and life course perspective, where researchers identify and examine the underlying dimensions of a stressful exposure (e.g., frequency, timing, duration, and severity), in order to better understand how different aspects of lifetime stress exposure are related to mental health and well-being in elite sport.
The purpose of the present study was to examine how cumulative lifetime stress exposure was associated with symptoms of depression and anxiety, as well as well-being, among elite athletes. Given that the majority of research on this topic outside of sport has found linear relationships between lifetime stress exposure and mental health and well-being (e.g., Slavich & Shields, 2018), it was hypothesized that greater cumulative lifetime stress exposure (both total stressor count and severity) would be associated with poorer mental health and well-being, but that these associations would differ by stressor timing, type, life domain, and social-psychological characteristic (e.g., Slavich et al., 2019). This study also collected qualitative data to help explain why cumulative lifetime stress exposure might have resulted in poor mental health and well-being.
1. Method
1.1. Study design
This study was underpinned by methodological pluralism (i.e., drawing on both positivism and interpretive epistemologies) as opposed to methodological puritanism (i.e., affinity to a single paradigm; Onwuegbuzie & Leech, 2005). This approach enabled a more comprehensive understanding of phenomena, whereby the weaknesses of one approach were addressed by the strengths of the other (Johnson & Onwuegbuzie, 2004). Driven by this approach, the underlying theme of this research was pragmatism (Teddlie & Tashakkori, 2011).
Consistent with this research paradigm, a mixed-method explanatory sequential (two-phase) study design was employed, with qualitative data (phase two) used to help explain the quantitative results (phase one). As such, integration of methods occurred across chronological phases of the study, where the collection and analysis of quantitative data (i.e., phase one) sought to inform the direction of the qualitative phase (i.e., phase two). Consistent with this approach, the weighting of each method was unequal. Specifically, since the quantitative data informed the qualitative method, greater attention was focused on the quantitative data (Creswell & Plano-Clark, 2011).
1.2. Participants
Phase one was completed by 95 participants between 18 and 60 years old (58 females, 37 males; Mage = 29.81, SD = 10.88) from a variety of sports (e.g., athletics, swimming, triathlon, netball, football, and hockey). All participants were classified as elite athletes because they had competed, or were currently competing, at an international or professional level (Swann, Moran, & Piggott, 2015). An a priori power calculation using G*Power software revealed that a minimum sample of 60 participants was required given a medium effect size of 0.30, an alpha of 0.05, and power of 0.80. During phase two, criterion-based purposeful sampling identified participants who were in the top 10% of lifetime stressor count (M = 38.60, SD = 13.26) and severity (M = 97.30, SD = 30.50). Six participants (five females, one male) between 28 and 36 years old (Mage = 32.17, SD = 3.19) were interviewed. These participants were from a range of sports, including triathlon, ultrarunning, and powerlifting. The sample size for phase two offered sufficient information power given the quality of data garnered from in-depth interviews (Malterud, Siersma, & Guassora, 2016). Specifically, the quality of the data was assessed via the communication between the researcher and the participant. Due to the explanatory nature of the qualitative data, semi-structured interviews had a specific aim, which promoted a clear and focused dialogue. Next, the homogeneity of the sample provided sufficient information power, given that participants had experienced the phenomena in question (i.e., lifetime stress exposure), thus, belonging to the specified target group. Finally, the mean duration of interviews suggested that participants provided in-depth and rich detail relating to lifetime stress and health (Malterud et al., 2016).
1.3. Procedure
Following institutional ethical approval, participants were recruited using the researchers’ existing contacts and social media (e.g., Twitter). After providing informed consent, participants completed the online questionnaire, which took approximately 30 minutes. Once the quantitative data had been analyzed, participants in the top 10% of self-reported cumulative lifetime stressor count and severity were emailed to arrange an in-depth interview at a convenient time. Six participants agreed to be interviewed and completed semi-structured interviews on Skype (Mduration = 57.90 min, SD = 12.85; range = 40–76 min). A semi-structured interview format was adopted as this was considered the most effective and convenient method for gathering in-depth information (Kvale & Brinkmann, 2009). These interviews were informed by an interview guide that contained questions relating to lifetime stress and health, and comprised of four sections, including: introductory questions (e.g., “how did you first get involved in your sport?“); questions relating to the stressors experienced over the life course (e.g., “can you tell me about an event or period during your childhood that you found particularly difficult?“); questions relating to how participants reacted to the culmination of stressors over the life course (e.g., “how did you respond to these stressors and adversities?“); and questions identifying the impact of lifetime stress on mental health and well-being (e.g., “can you please explain how these stressors and adversities affected your mental health and well-being?“). The interviews were recorded with audio equipment and manually transcribed.
1.4. Measures
1.4.1. Cumulative lifetime stressor exposure
Cumulative lifetime stress exposure was assessed using the Stress and Adversity Inventory for Adults (Adult STRAIN; Slavich & Shields, 2018). The Adult STRAIN is an online stress assessment system that enquires about 55 major stressors (e.g., job loss, death of a relative). For every stressor that is endorsed, follow-up questions are asked that assess the severity (1 = not at all to 5 = extremely), frequency (1 to 5 or more times), timing (1 = ongoing to 7 = over 5 years), and duration (an open box where participants indicate years and/or months) of that stressor (Slavich & Shields, 2018). Stressors that are assessed with the Adult STRAIN span two time periods (early life vs. adulthood), and can be categorized into two stressor types (acute life events vs. chronic difficulties), 12 major life domains (housing, education, work, health, marital/partner, reproduction, financial, legal, other relationships, death, life-threatening situations, and possessions), and five social-psychological characteristics (interpersonal loss, physical danger, humiliation, entrapment, and role change/disruption). The two main variables used in this study were: (1) total count of lifetime stressors, which was calculated by summing the number of stressors encountered by participants (range = 0–166), and (2) total cumulative severity of lifetime stressors, which was calculated by summing the perceived severity of the stressors experienced by participants (range = 0–265). The Adult STRAIN has very good concurrent (rs = .15 – .62) and discriminant validity, with excellent test-retest reliability (rs = .90 –.95). Furthermore, the predictive validity of the Adult STRAIN has previously been demonstrated in relation to various outcomes, including mental and physical health complaints, sleep quality, and cognitive function among others (e.g., Cazassa, Oliveira, Spahr, Shields, & Slavich, 2020; Slavich & Shields, 2018; Sturmbauer et al., 2020).
1.4.2. Depression
The Patient Health Questionnaire (PHQ-9) was used to assess symptoms of depression over the past two weeks. The PHQ-9 consists of nine items (e.g., little interest or pleasure in doing things), with each item scored on a scale ranging from 0 (not at all) to 3 (nearly every day). Higher scores indicated greater symptoms (range = 0–27), with scores of 5, 10, 15, and 20 representing mild, moderate, moderately severe, and severe depression, respectively (Kroenke, Spitzer, & Williams, 2001). The PHQ-9 has good internal consistency (α = .86 – .89) and test-retest reliability (r = .84), as well as good construct and criterion validity (Kroenke et al., 2001).
1.4.3. Anxiety
The Generalized Anxiety Disorder (GAD-7) scale was used to assess symptoms of anxiety over the past two weeks. The GAD-7 consists of seven items (e.g., feeling nervous, anxious, or on edge), with each item scored on a scale ranging from 0 (not at all) to 3 (nearly every day). Higher scores indicated greater symptoms (range = 0–21), with scores of 5, 10, and 15 representing mild, moderate, and severe anxiety, respectively. The GAD-7 has good internal consistency (α = .89 – .92) and test-retest reliability (rs = .83), as well as convergent, construct, criterion, and factorial validity (Löwe et al., 2008; Spitzer, Kroenke, Williams, & Löwe, 2006).
1.4.4. Well-being
The Scales of General Well-Being (SGWB) was used to assess multiple indicators of well-being (e.g., happiness, vitality, self-acceptance; Longo, Coyne, & Joseph, 2018). The SGWB consists of 14 items (e.g., I have a purpose), with each item scored on a scale ranging from 1 (not at all true) to 5 (very true). Higher scores indicated better well-being (range = 14–70), with scores above 40 representing ‘good’ well-being. The SGWB has demonstrated good internal consistency (α = .86) and construct validity (rs = .67 – .88; Longo et al., 2018).
1.5. Data analysis
Quantitative data were analyzed using SPSS version 25.0. Prior to any analyses, outliers (z-scores greater or less than 3.29) were removed from the dataset (six values for total lifetime stressor count, seven values for total lifetime stressor severity, four values for PHQ-9, and three values for GAD-7). Following these outlier analyses, visual inspection confirmed that all data were normally distributed. First, to examine if total lifetime stressor count or severity predicted depression, anxiety, or well-being, a series of hierarchical linear regression analyses were conducted. Specifically, depression, anxiety, and well-being were entered into separate models as dependent variables, while in each model, independent variables were entered at step 1 (total lifetime stressor count or severity), and a priori covariates were entered at step 2 (age and gender).1 Next, a series of hierarchical linear regression analyses were conducted to examine if the different stressor types (acute life events vs. chronic difficulties), time periods (early-life vs. adulthood), life domains (e.g., work, health, death), and social-psychological characteristics (e.g., physical danger, humiliation, entrapment) significantly predicted depression, anxiety, and well-being, above and beyond age and gender. Three life domains (education, legal, and reproduction) were excluded from analyses, as very few participants in this sample reported experiencing these stressors.
Qualitative data were analyzed using a confirmatory approach to thematic analysis because the quantitative findings guided the ideas the researcher assessed using semi-structured interviews (Guest, MacQueen, & Namey, 2012). The six-step procedure described by Braun and Clarke (2006) was adopted. Analysis began by listening to interview recordings, and reading and re-reading each transcript, prior to the development of preliminary codes. The initial list of codes was then reduced through grouping to identify overarching themes that were relevant throughout the entire dataset. Themes were then refined, defined and named, before the results were written. As the qualitative component was subordinate to the quantitative element, themes were identified at a semantic level to help explain the quantitative results (Braun & Clarke, 2006).
1.6. Methodological integrity
Approaches were considered that sought to enhance the methodological integrity of the qualitative data via its two constituents: fidelity and utility (Levitt, Motulsky, Wertz, Morrow, & Ponterotto, 2017). Fidelity to the subject matter was established using perspective management in data collection. To elaborate, the researcher engaged in a process of bracketing to identify one’s implicit assumptions and biases (Morrow, 2005). Bracketing was achieved through the use of a reflexive journal where the researcher’s influence on the data collection process was identified. As a result, the use of a reflexive journal sought to limit the influence of the researcher’s implicit assumptions and biases to obtain a clearer representation of phenomena (Levitt et al., 2017). Furthermore, utility in achieving goals was achieved by collecting data that provided rich grounds for insightful analyses (Levitt et al., 2017). To elaborate, the methods adopted within the present study identified participants that had experienced the phenomena in question (i.e., lifetime stress exposure), resulting in enhanced insight to be derived from the data (Levitt et al., 2017).
2. Results
2.1. Quantitative findings
2.1.1. Descriptive statistics
Participants experienced an average of 13 stressors over their lifetime (range = 0–54), including an average of eight acute life events (range = 0–43), five chronic difficulties (range = 0–26), and three early life (range = 0–22) and ten adulthood (range = 0–48) adversities. The mean cumulative lifetime stressor severity was 31.38 (SD = 27.70). On average, participants reported relatively low symptoms of depression (M = 4.15, SD = 3.62) and anxiety (M = 3.49, SD = 3.04), and relatively high levels of well-being (M = 53.67, SD = 9.58). Overall, 1.3%, 2.6%, 3.8%, and 24% of participants met the criteria for severe, moderately severe, moderate, and mild depression, respectively. In addition, 1.2%, 3.8%, and 21.8% of participants met the criteria for severe, moderate and mild anxiety, respectively. No participants met the criteria for both severe depression and anxiety. Bivariate correlation analyses revealed that most of the STRAIN variables were moderately associated with poorer mental health and well-being (Table 1).
Table 1.
Means, standard deviations, and intercorrelations for the main study variables.
| Mean | SD | 1 | 2 | 3 | |
|---|---|---|---|---|---|
| 1. Depression | 4.15 | 3.63 | – | ||
| 2. Anxiety | 3.49 | 2.30 | – | ||
| 3. Well-being | 53.67 | 9.58 | – | ||
| 4. Total count of lifetime stressors | 12.86 | 10.81 | .41*** | .33** | −.41*** |
| 5. Total severity of lifetime stressors | 31.48 | 27.70 | .43*** | .23 | −.26* |
| 6. Count of acute life events | 7.76 | 7.28 | .30* | .22 | .28* |
| 7. Count of chronic difficulties | 5.11 | 4.66 | .44*** | .24* | −.32** |
| 8. Count of early adversity | 2.77 | 3.25 | .30** | .29* | −.16 |
| 9. Count of adulthood adversity | 9.71 | 8.80 | .39*** | .27* | −.36** |
| 10. Severity of acute life events | 16.12 | 13.71 | .34** | .29* | −.24* |
| 11. Severity of chronic difficulties | 15.36 | 15.68 | .43*** | .21 | −.30** |
| 12. Severity of early adversity | 7.80 | 9.13 | .30* | .39*** | −.20 |
| 13. Severity of adulthood adversity | 23.68 | 22.41 | .42*** | .15 | −.31** |
p < .05;
p < .01;
p < .001.
2.1.2. Lifetime stressor count, mental health, and well-being
Cumulative lifetime stressor count significantly predicted symptoms of depression (β = .42, p < .001) and anxiety (β = .34, p = .003), and well-being (β = −.42, p < .001), above and beyond age and gender (Table 2). Examining stressor type revealed that chronic difficulties and acute life events both significantly predicted greater symptoms of depression (β = .44, p < .001; β = .30, p = .007) and anxiety (β = .24, p = .040; β = .24, p = .039), and well-being (β = −.35, p = .004; β = −.28, p = .018), above and beyond age and gender. With respect to stressor exposure timing, total count of early adversities significantly predicted symptoms of depression above and beyond age and gender (β = .25, p = .030), but did not significantly predict symptoms of anxiety (β = .22, p = .065) or well-being (β = −.16, p = .180). Total count of adulthood adversities, in contrast, significantly predicted symptoms of depression (β = .43, p < .001) and anxiety (β = .32, p = .006), as well as well-being (β = −.40, p = .001), above and beyond age and gender.
Table 2.
Hierarchical regression models examining if lifetime stress (LTS) count and severity predicted (a) symptoms of depression, (b) symptoms of anxiety, and (c) well-being (model 1), adjusting for age and gender (model 2).
| (a) | Depression | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | ||||||||||
| B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β | ||
| LTS Count | 0.17 (0.08 to 0.27) | 0.05 | 0.41*** | 0.18 (0.09 to 0.26) | 0.04 | 0.42*** | LTS Severity | 0.71 (0.04 to 0.11) | 0.02 | .043*** | 0.08 (0.04 to 0.11) | 0.02 | 0.46*** |
| Age | −0.02 (−0.06 to 0.03) | 0.02 | −0.08 | Age | −0.03 (−0.08 to 0.01) | 0.02 | −.0.16 | ||||||
| Gender | 1.67 (0.62 to 2.76) | 0.53 | 0.34** | Gender | 1.42 (0.38 to 2.46) | 0.52 | 0.30** | ||||||
| (b) | Anxiety | ||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | ||||||||||
| B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β | ||
| LTS Count | 0.14 (0.04 to 0.23) | 0.05 | 0.33** | 0.14 (0.05 to 0.24) | 0.05 | 0.34** | LTS Severity | 0.04 (0.00 to 0.07) | 0.02 | .23 | 0.04 (0.01 to 0.81) | 0.02 | 0.28* |
| Age | −0.03 (−0.08 to 0.02) | 0.02 | −0.16 | Age | −0.04 (−0.09 to 0.05) | 0.02 | −.0.22 | ||||||
| Gender | 1.10 (−0.04 to 2.21) | 0.56 | 0.23 | Gender | 0.90 (−0.20 to 2.00) | 0.55 | 0.20 | ||||||
| (C) | Well-Being | ||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | ||||||||||
| B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β | ||
| LTS Count | −0.65 (−0.10 to −0.31) | 0.17 | −0.41*** | −0.67 (−1.02 to −0.32) | 0.18 | −0.42*** | LTS Severity | −0.16 (−0.30 to −0.02) | 0.07 | −.26* | −0.18 (−0.33 to −0.04) | 0.74 | −0.30* |
| Age | 0.09 (−0.10 to 0.28) | 0.10 | 0.11 | Age | 0.13 (−0.06 to 0.32) | 0.10 | 0.17 | ||||||
| Gender | 0.55 (−3.96 to 5.05) | 2.26 | 0.03 | Gender | 1.60 (−2.85 to 6.03) | 2.23 | 0.09 | ||||||
p < .05;
p < .01,
p < .001, two-tailed
In terms of stressor characteristics, the total count of stressors that significantly predicted symptoms of depression across most of the life domains and social-psychological characteristics, while controlling for age and gender, including: work (β = .34, p = .002), marital/partner (β = .29, p = .010), financial (β = .28, p = .011), other relationships (β = .29, p = .007), entrapment (β = .40, p < .001), role change/disruption (β = .33, p = .002), humiliation (β = .30, p = .006), and interpersonal loss (β = .28, p = .011). Housing, health, death, life-threatening situations, possessions, and physical danger were not significantly associated with symptoms of depression (Fig. 1a). The stressor characteristics that significantly predicted symptoms of anxiety, while controlling for age and gender, included: role change/disruption (β = .26, p = .025), life-threatening situations (β = .26, p = .022), other relationships (β = .24, p = .034), and humiliation (β = .31, p = .005). Housing, work, health, marital/partner, financial, death, entrapment, possessions, interpersonal loss, and physical danger were not associated with symptoms of anxiety (Fig. 1b). Finally, the stressor characteristics that significantly predicted well-being, while controlling for age and gender, included: health (β = −.33, p = .005), role change (β = −.36, p = .002), marital/partner (β = −.26, p = .024), other relationships (β = −.25, p = .027), life-threatening situations (β = −.25, p = .032), entrapment (β = −.25, p = .034), and physical danger (β = −.35, p = .005). Housing, work, financial, death, possessions, interpersonal loss, and humiliation were not associated with well-being (Fig. 1c).
Fig. 1.
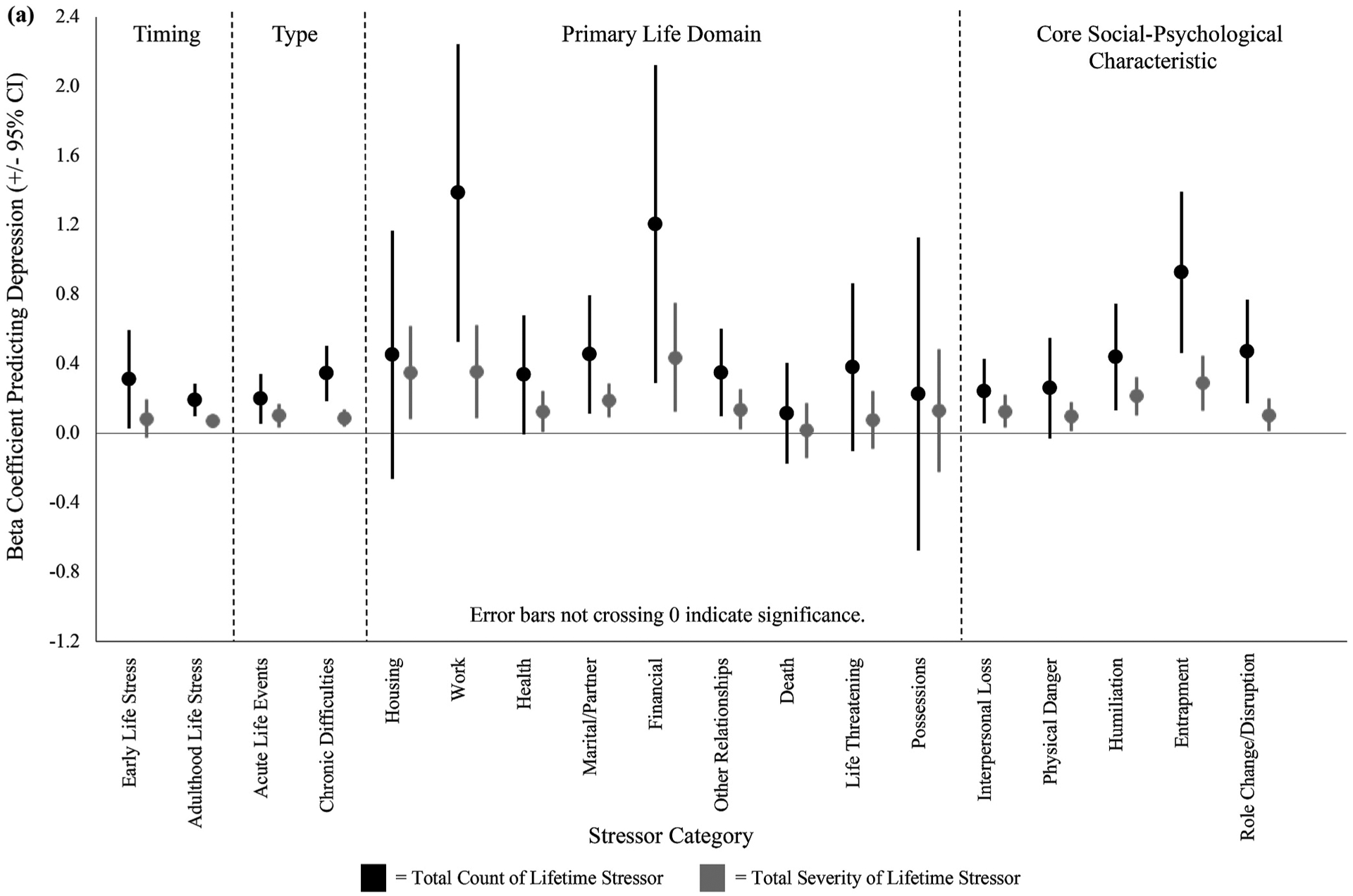
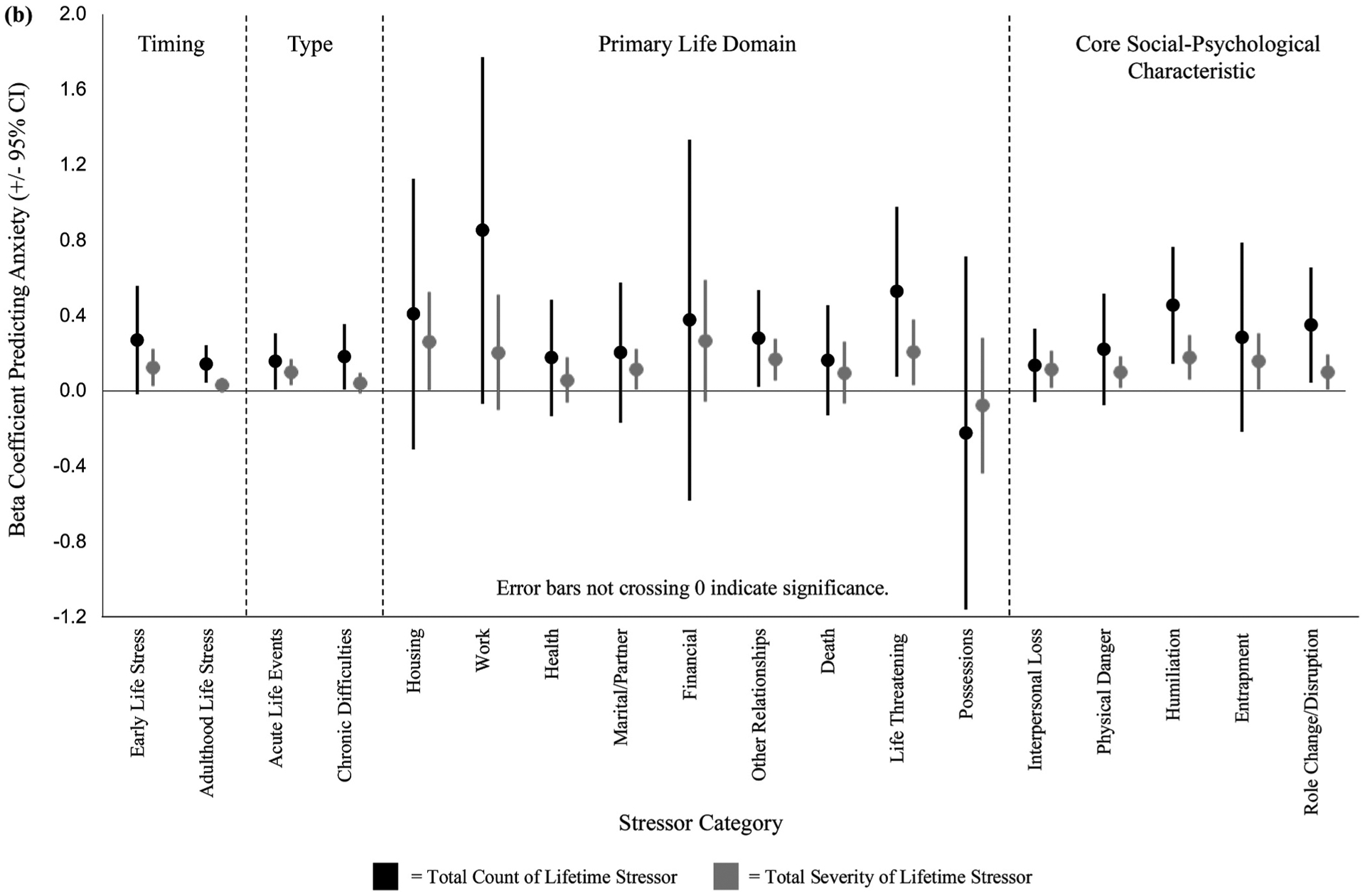
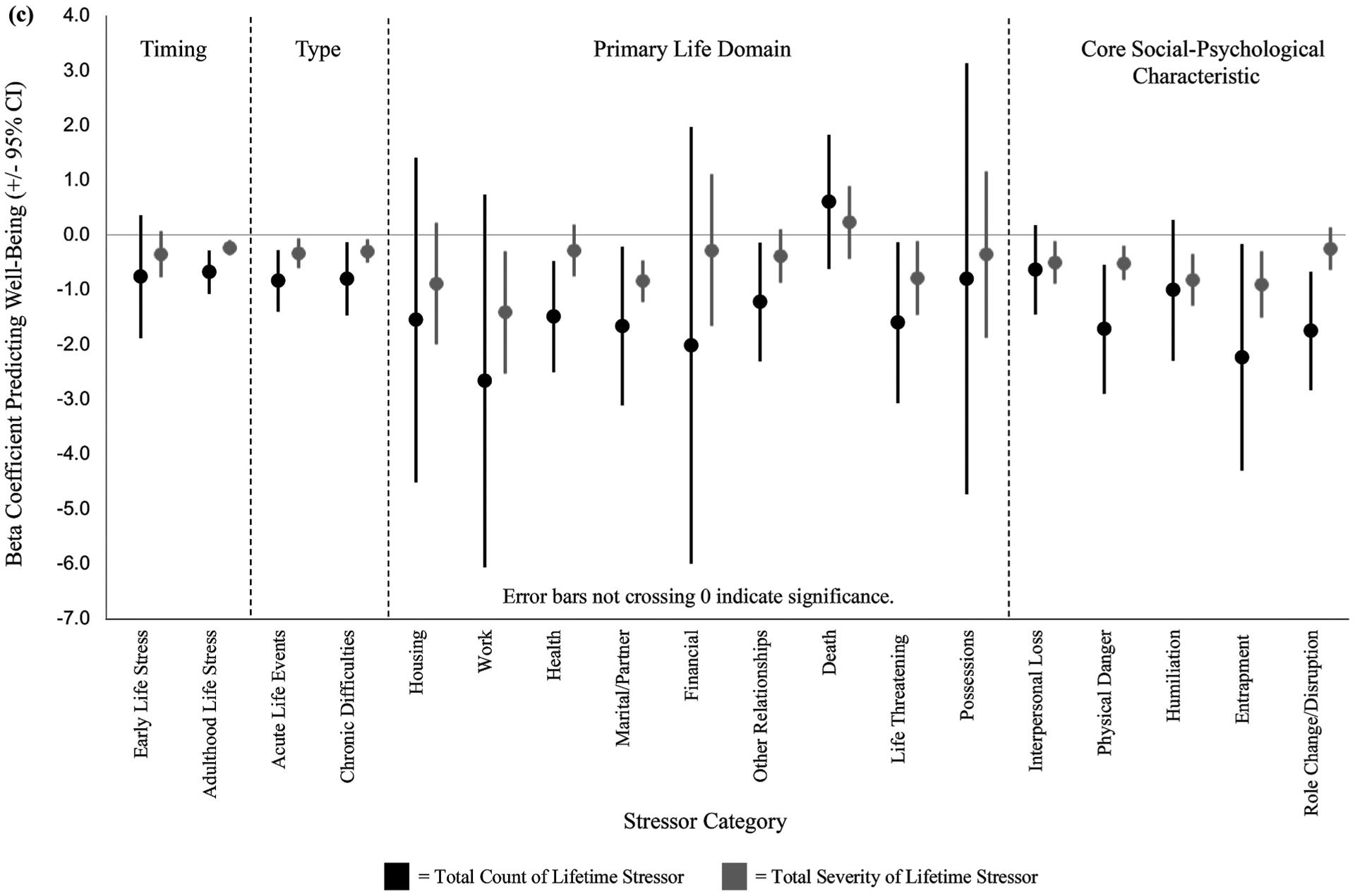
Associations between total count and severity of lifetime stressor exposure and (a) depression, (b) anxiety, and (c) well-being, categorized by stressor timing, type, primary life domain, and core social-psychological characteristic. Error bars represent 95% confidence intervals.
2.1.3. Lifetime stressor severity, mental health, and well-being
In terms of stressor severity, total severity of lifetime stressors significantly predicted symptoms of depression (β = .46, p < .001) and anxiety (β = .28, p = .018), as well as well-being (β = −.30, p = .015), above and beyond age and gender (Table 2). Examining stressors types revealed that severity of acute life events significantly predicted symptoms of depression (β = .39, p = .001) and anxiety (β = .36, p = .003), in addition to well-being (β = −.30, p = .019), above and beyond age and gender. In contrast, total severity of chronic difficulties significantly predicted symptoms of depression (β = .43, p < .001) and well-being (β = −.30, p = .010), above and beyond age and gender, but not symptoms of anxiety (β = .21, p = .063). With respect to stress exposure timing, total severity of early adversities significantly predicted symptoms of anxiety above and beyond age and gender (β = .32, p = .010), but not symptoms of depression (β = .21, p = .083) or well-being (β = −.20, p = .105). In contrast, total severity of adulthood adversities significantly predicted symptoms of depression (β = .52, p < .001) and anxiety (β = .24, p = .045), as well-being (β = 38, p = .002), above and beyond age and gender.
In terms of stressor characteristics, the total severity of stressors that significantly predicted symptoms of depression across the different life domains and social-psychological characteristics, while controlling for age and gender, included: housing (β = .30, p = .008), marital/partner (β = .42, p < .001), other relationships (β = .28, p = .012), work (β = .30, p = .008), health (β = .27, p = .020), financial (β = .30, p = .006), humiliation (β = .41, p < .001), entrapment (β = .40, p < .001), interpersonal loss (β = .32, p = .004), physical danger (β = .29, p = .010), and role change/disruption (β = .27, p = .015). Death, life-threatening situations, and possessions were not associated with symptoms of depression (Fig. 1a). The stressor characteristics that significantly predicted symptoms of anxiety, while controlling for age and gender, included: housing (β = .24, p = .043), marital/partner (β = .24, p = .029), other relationships (β = .34, p = .002), life-threatening situations (β = .28, p = .018), interpersonal loss (β = .28, p = .015), humiliation (β = .35, p = .002), physical danger (β = .30, p = .012), entrapment (β =.24, p = .033), and role change/disruption (β = .25, p = .027). Work, health, financial, death, and possessions were not associated with symptoms of anxiety (Fig. 1b). Finally, the stressor characteristics that significantly predicted well-being, while controlling for age and gender, included: work (β = −.30, p = .014), marital/partner (β = −.46, p < .001), life-threatening situations (β = −.27, p = .024), interpersonal loss (β = −.30, p = .011), physical danger (β = −.37, p = .002), humiliation (β = −.38, p = .001), and entrapment (β = −.34, p = .004). Housing, health, financial, other relationships, death, possessions, and role change/disruption were not associated with well-being (Fig. 1c).
2.2. Qualitative findings
The qualitative data collected in this study were used to help explain why cumulative lifetime stress exposure (count and severity) might have resulted in poor mental health and well-being among elite athletes. As discussed below, three themes were identified: (1) maladaptive long-term coping strategies, (2) increased susceptibility to future stress, and (3) interpersonal relationship difficulties. Pseudonyms are used throughout to protect participants identities.
2.2.1. Maladaptive long-term coping strategies
Three participants explained how experiencing negative childhood adversities led to the development of maladaptive coping styles. This notion was exemplified by Mary: “I lost my mother at 12 … I didn’t really deal with it very well; I threw myself into anything other than being at home. I trained intensely”. Despite participants attributing the success of their athletic career to the stressors and adversities they experienced, they also identified the long-standing mental health issues associated with their coping approach, as described by Elizabeth: “It got to a point where nothing was good enough and I was never satisfied. I was overtraining, I was at burnout, I was self-harming. I was damaging myself because I couldn’t cope”. As such, participants used sport as a short-term palliative coping strategy, which ultimately led to maladaptive coping in the longer term. This was supported by Sarah: “[sport] became the only thing I had … In the short term, [experiencing stress] had a fantastic effect on my sport but in the long-term, I was emotionally stunted and crippled”. As such, an exclusive focus on sport following adversity led to the development of a constrained identity, this was further supported by Elizabeth: “Running was all I had and all I focused on … It made me push myself and I don’t think I would’ve got to the level that I did if I hadn’t been through everything that I experienced”. Thus, this theme revealed how the elite athletes initially developed positively after experiencing stress and adversity, but, also, how their behavior led to maladaptive coping strategies that negatively impacted their mental health and well-being in the long-term.
2.2.2. Increased susceptibility to future stress
Three participants indicated that encountering adverse experiences in developmentally sensitive periods may have acted as a catalyst for experiencing subsequent stress. For example, Daniel stated: “They [the stressors] just fed off one another … If something was going on outside of sport, my sport performance would decrease, which meant I got deselected … The continuous and constant nature of stressors just fed into mental health problems … It was just this downward spiral that I couldn’t get out of”. As such, a history of high stressor exposure increased the likelihood of experiencing more frequent stressors, leading to the development of mental health disorders and reduced levels of well-being. This was further supported by Sophie: “It is that kind of helplessness feeling … I have never felt like I could fix it or make it better, [experiencing stress] just wears you down and you just cannot get away from it”. Consequently, the accumulation of stress and adversity was found to promote maladaptive stress responses (e.g., negative emotions such as anxiety or worry), which was further supported by Sophie: “I was a nightmare. I worried about everything. I was very, very insecure … Because so many other bad things had happened, I always thought the worst all the time. And even now, I catastrophize everything”. This notion was exemplified by Sarah: “What happened in childhood made me more susceptible to the stressors I experienced as an adult … It made me just shut down and I couldn’t cope”. Thus, this theme revealed that exposure to greater lifetime stressors led to an increased susceptibility to future stress, via the promotion of maladaptive stress responses, likely explaining the development of negative health-related outcomes (e.g., depression).
2.2.3. Interpersonal relationship difficulties
Finally, four participants demonstrated difficulty in establishing trusting and intimate relationships with others as a result of experiencing prior stress and adversity. This was demonstrated by Jessica, who said that: “When I moved up to seniors at 16, there was a lot of people who were making advances on me and being inappropriate … I ended up being in an abusive marriage and nearly losing my life … It totally warped my relationships”. Furthermore, the detrimental consequences associated with experiencing a high degree of lifetime stress without adequate support was illustrated by Mary: “I felt abandoned, I had to fend for myself … I shy away from intimate relationships and meaningful friendships … it has dramatically affected my life and my ability to be a mother”. Fragmented relationships with others resulted in participants reporting lower social support and increased distance from others. This was exemplified by Sophie, who noted that: “It is probably a feeling of insecurity and you just think, in particular with my husband, well he won’t stay because people don’t”. This notion was also illustrated by Elizabeth, who stated that: “I think the stressors that I have experienced made it very difficult for me to interact with other people … I can thank running for a lot of things, but I can’t cope in a normal environment”. Consequently, limited interpersonal relationships with others, coupled with the presence of major stressors and adversities over the life course, affected participants mental health and well-being. For example, Elizabeth stated: “My social circle was incredibly small, I had no friends outside of sport, I had no support structure … I felt abandoned … It resulted in a long-term anxiety problem and has took a long time to even start to recover from that”. Therefore, this theme revealed that the difficulties associated with establishing interpersonal relationships with others partly explained the link between cumulative lifetime stress exposure, mental health, and well-being.
3. Discussion
Despite considerable interest in stress, relatively little is known about how cumulative lifetime stress is associated with mental health and well-being in an elite sporting context. This study aimed to address this issue by collecting both quantitative and qualitative data from elite athletes and in doing so, provide the first insight into how lifetime stress exposure relates to mental health and well-being. The results revealed significant associations between cumulative lifetime stress exposure and symptoms of depression and anxiety, as well as well-being. These associations were similar for both lifetime stressor count and severity, and robust while controlling for age and gender, which are well-known predictors of poor mental health (Harkness et al., 2010). These findings are also consistent with the integrative model of lifespan stress and health (Epel et al., 2018), and suggest that greater lifetime stress is associated with poorer mental health and well-being but that these effects differ by the specific types of stressors experienced.
Associations between different stressor types and athletes’ mental health status revealed that the total count and severity of chronic difficulties was a marginally stronger predictor of depression, when compared with the total count and severity of acute life events. Contextualized within extant literature and theory, these findings are consistent with the integrative model (Epel et al., 2018), suggesting that chronic stress may be a stronger predictor of depression than acute stress (Slavich et al., 2019). In contrast, when comparing these associations with symptoms of anxiety and well-being, results for the total count and severity of chronic difficulties were nearly identical to those observed for the count and severity of acute life events. An interesting lack of association, however, was observed between the total severity of chronic difficulties and symptoms of anxiety. This is in contrast to prior research, which has demonstrated that chronic difficulties are a marginally stronger predictor of psychiatric disorders (i.e., depression and anxiety) than acute life events (e.g., Slavich et al., 2019). One potential explanation for these disparate findings could involve the low levels of anxiety reported by participants in the present study. Alternatively, chronic stress may act as a motivator for success, rather than as an anxiety-producing barrier, in elite athletes.
The present study revealed significant relationships between recent adulthood life events and symptoms of depression and anxiety, as well as well-being. Consistent with prior research (e.g., Lam et al., 2019), associations between lifetime stress exposure and health-related outcomes were consistent and strongest for stressors occurring in adulthood. This finding suggests that experiencing greater and more severe recent life events are predictive of mental ill-health and lower levels of well-being among elite athletes. In contrast, exposure to early adversity was found to be predictive of symptoms of depression and anxiety; however, these associations were not as consistent or as strongly related to mental health problems and levels of well-being. This finding was interesting as the association between childhood adversity and poor mental health is nearly ubiquitous in the psychology literature (e.g., Hughes et al., 2017). One possible explanation for this finding may be that exposure to early adversity may interact and exacerbate the effects of recent stressors, leading to the development of mental ill-health among elite athletes (Turney, 2014).
Consistent with the stressor characteristic perspective (e.g., Slavich et al., 2019), stressors categorized by primary life domains and social-psychological characteristics were found to be differentially associated with symptoms of depression and anxiety, as well as well-being. Most notably, the stressor count indices that most consistently and significantly predicted mental health and well-being were role change (e.g., starting a new job) and other relationships (e.g., parental or non-intimate relationship problems). In contrast, the stressor severity indices that most consistently and significantly predicted mental health and well-being were interpersonal loss (e.g., close friend moves away), physical danger (e.g., being robbed at gun point), entrapment (e.g., having to care for a disabled parent), humiliation (e.g., being cheated on by a romantic partner) and marital/partner (e.g., ongoing marital discord). A growing body of work suggests that major life stressors that include interpersonal loss and humiliation are particularly harmful for health (e.g., Kendler, Hettema, Butera, Gardner, & Prescott, 2003; Slavich, 2020). As such, this study extends existing work by highlighting the specific life domains and social-psychological characteristics that might make athletes more susceptible to poor mental health and well-being.
This study also used qualitative methods to help explain why cumulative lifetime stress exposure might have resulted in poor mental health and well-being, which added meaning to the quantitative results. First, participants revealed how adversity-related experiences led to improved sporting performance in the short-term, but, also to some maladaptive coping strategies in the long-term. For example, the qualitative data suggested that the exclusive focus on sport following adversity led to the development of a constrained identity. Although intuitively appealing for sporting performance, research has shown that athletic identity foreclosure can limit adaptive responses to stress, resulting in psychological difficulties (e.g., Giannone, Haney, Kealy, & Ogrodniczuk, 2017). The data, therefore, offer some support to the potential antithetical relationship between well-being and performance among athletes at the highest level (Fletcher, 2019). Second, consistent with prior research, the accumulation of stressors during childhood was found to render participants more susceptible to stress throughout adulthood (e.g., Pearlin, Schieman, Fazio, & Meersman, 2005). This finding suggests that the accumulation of stressors over the life course may limit coping resources to deal with the demands of a stressful situation. One theoretical framework that offers a possible explanation for this result is the biopsychosocial model of challenge and threat (Blascovich, 2008a), which suggests that when coping resources are limited, individuals will typically appraise a stressful situation as more of a threat. When frequently experienced, repeated threat appraisals have been linked to deleterious health consequences (e.g., depression; Blascovich, 2008b). Finally, this study found that participants who experienced greater and more severe lifetime stressors demonstrated difficulty in establishing and maintaining interpersonal relationships. Congruent with the interpersonal theory of psychopathology, the presence of stressors can have detrimental effects on health through the disruption of interpersonal relationships (Hammen & Rudolph, 1996). Thus, limited interpersonal relationships with others can increase the cumulative effects of stress (McEwen & Gianaros, 2010).
Several strengths and weaknesses of this study should be noted. In terms of strengths, this is the first mixed methods study to examine cumulative lifetime stress exposure and mental health and well-being in elite athletes. Indeed, the adoption of both quantitative and qualitative methodologies provided a more comprehensive understanding of phenomena. Furthermore, this study examined stress-health links in elite athletes, which is noteworthy considering the increasing risk of mental ill-health in this population (Gorczynski et al., 2017). Finally, this study assessed participants’ exposure to different types of stressors over the entire lifespan, which has rarely been done (Slavich & Shields, 2018). Consequently, the results provide meaningful information to researchers and practitioners who are interested in better understanding the risk factors that are associated with the mental health and well-being of the athletes they work with.
With regard to limitations, first, the exclusive focus on non-sporting stressors and adversities (e.g., bereavement), and the absence of sport-related stressors and adversities (e.g., injury), could be seen as a potential limitation. Indeed, it is possible that stressors unique to the elite sporting environment could have different effects on athletes’ mental health (Rice et al., 2016). Therefore, future research should examine the role of both sporting and non-sporting stressors to garner a more comprehensive understanding of cumulative lifetime stress exposure on athlete mental health and well-being. Second, a cross-sectional study design was used, which prevents causal inferences from being drawn from the data. Future research should therefore assess lifetime stress and mental health using longitudinal study designs. Third, although adequately powered, the study used a sample size that is relatively small owing to challenges associated with collecting data from elite athletes. Consequently, future research should attempt to gather data from larger samples.
From an applied perspective, the results of this study have important implications for practitioners and organizations that are committed to better supporting mental health and well-being. Based on these findings, it is suggested that practitioners working with sport performers should be aware of the competing demands placed on elite athletes and begin assessing their stress levels (i.e., historical and current stress exposure) to help identify athletes who may be most susceptible to developing mental health problems (Fletcher et al., 2006). Notably, the quantitative findings emphasize the importance of identifying athletes who have been exposed to stressors that are either chronic in nature or that have occurred in adulthood. As a result, the implementation of a stress audit within elite sport could provide practitioners with important information and enable coaches to address stressors that increases individuals’ risk for mental health problems and diminished well-being (Reardon et al., 2019). With regard to the qualitative findings, coaches should promote effective coping by improving athletes’ self-awareness using systematic self-reflection (Tamminen & Holt, 2012). In doing so, athletes could become better able to assess the demands of stressful situations and identify the resources that they have to effectively cope (Blascovich, 2008a). Furthermore, the ability to cope with stressful situations can be bolstered by developing strong interpersonal relationships with others. Specifically, sport psychologists should help athletes identify various sources of social support and facilitate the development of a supportive environment (e.g., improved communication and empathy with others in the sporting organization; Freeman, 2021). Finally, sporting organizations must support elite athletes by viewing mental health as an organizational priority (Reardon et al., 2019).
To conclude, this study examined cumulative lifetime stress exposure and mental health and well-being in elite athletes, using a mixed-method approach. The findings demonstrated that greater and more severe lifetime stress exposure was associated with poorer mental health and well-being, but that these effects differed by the specific types of stress experienced. Moreover, follow-up qualitative data suggested that maladaptive long-term coping strategies, increased susceptibility to future stress, and difficulties establishing interpersonal relationships, may help explain the link between lifetime stress and poorer mental health and well-being in athletes.
Footnotes
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper.
Curvilinear or quadratic relationships between lifetime stress exposure (i.e., total count and severity of lifetime stress) and outcomes (i.e., depression, anxiety, and well-being) were also assessed via curve estimation regression analyses. The results revealed no significant curvilinear or quadratic relationships between any of the lifetime stress exposure and outcome variables.
References
- Arnold R, Fletcher D, & Daniels K (2016). Demographic differences in sport performers’ experiences of organizational stressors. Scandinavian Journal of Medicine & Science in Sports, 26(3), 348–358. 10.1111/sms.12439 [DOI] [PubMed] [Google Scholar]
- Blascovich J (2008a). Challenge and threat In Elliot AJ (Ed.), Handbook of approach and avoidance motivation (pp. 431–445). New York, NY: Psychology Press. [Google Scholar]
- Blascovich J (2008b). Challenge, threat, and health In Shah JY, & Gardner WL (Eds.), Handbook of motivation science (pp. 481–493). New York, NY: The Guilford Press. [Google Scholar]
- Braun V, & Clarke V (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. 10.1191/1478088706qp063oa [DOI] [Google Scholar]
- Cazassa M, Oliveira M, Spahr C, Shields G, & Slavich G (2020). The Stress and Adversity Inventory for Adults (Adult STRAIN) in Brazilian Portuguese: Initial validation and links with executive function, sleep, and mental and physical health. Frontiers in Psychology, 10, 30383 10.3389/fpsyg.2019.03083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creswell J, & Plano-Clark V (2011). Designing and conducting mixed method research (2nd ed.). Thousand Oaks, CA: Sage. [Google Scholar]
- Epel ES, Crosswell AD, Mayer SE, Prather AA, Slavich GM, Puterman E, et al. (2018). More than a feeling: A unified view of stress measurement for population science. Frontiers in Neuroendocrinology, 49, 146–169. 10.1016/j.yfrne.2018.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher D (2019). Psychological resilience and adversarial growth in sport and performance In Acevedo EO (Ed.), The Oxford encyclopedia of sport, exercise, and performance psychology (pp. 731–756). New York, NY: Oxford University Press. [Google Scholar]
- Fletcher D, Hanton S, & Mellalieu SD (2006). An organizational stress review: Conceptual and theoretical issues in competitive sport In Hanton S, & D Mellalieu S (Eds.), Literature reviews in sport psychology (pp. 321–374). Hauppauge, NY: Nova Science Publishers. [Google Scholar]
- Fletcher D, & Sarkar M (2012). A grounded theory of psychological resilience in Olympic champions. Psychology of Sport and Exercise, 13(5), 669–678. 10.1016/j.psychsport.2012.04.007 [DOI] [Google Scholar]
- Foskett R, & Longstaff F (2018). The mental health of elite athletes in the United Kingdom. Journal of Science and Medicine in Sport, 21(8), 765–770. 10.1016/j.jsams.2017.11.016 [DOI] [PubMed] [Google Scholar]
- Freeman P (2021). Social support In Arnold R, & Fletcher D (Eds.), Stress, well-being, and performance in sport. Oxford, UK: Taylor & Francis. [Google Scholar]
- Giannone Z, Haney C, Kealy D, & Ogrodniczuk J (2017). Athletic identity and psychiatric symptoms following retirement from varsity sports. International Journal of Social Psychiatry, 63(7), 598–601. 10.1177/0020764017724184 [DOI] [PubMed] [Google Scholar]
- Gorczynski P, Coyle M, & Gibson K (2017). Depressive symptoms in high-performance athletes and non-athletes: A comparative meta-analysis. British Journal of Sports Medicine, 51(18), 1348–1354. 10.1136/bjsports-2016-096455 [DOI] [PubMed] [Google Scholar]
- Greene J, Caracelli V, & Graham W (1989). Toward a conceptual framework for mixed method evaluation designs. Educational Evaluation and Policy Analysis, 11(3), 255–274. 10.3102/01623737011003255 [DOI] [Google Scholar]
- Guest G, MacQueen K, & Namey E (2012). Applied thematic analysis. Los Angeles, LA: Sage Publications. [Google Scholar]
- Hammen C, & Rudolph KD (1996). Childhood depression In Mash EJ, & Barkley RA (Eds.), Child psychopathology (pp. 153–195). New York, NY: Guilford Press. [Google Scholar]
- Hardy L, Barlow M, Evans L, Rees T, Woodman T, & Warr C (2017). Great British medalists: Psychosocial biographies of super-elite and elite athletes from Olympic sports In Walsh V, Wilson M, & Parkin B (Eds.), Sport and the brain: The science of preparing, enduring and winning Part A (pp. 1–119). London, UK: Academic Press. [DOI] [PubMed] [Google Scholar]
- Harkness K, Alavi N, Monroe S, Slavich G, Gotlib I, & Bagby R (2010). Gender differences in life events prior to onset of major depressive disorder: The moderating effect of age. Journal of Abnormal Psychology, 119(4), 791–803. 10.1037/a0020629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howells K, & Fletcher D (2015). Sink or swim: Adversity- and growth-related experiences in Olympic swimming champions. Psychology of Sport and Exercise, 16, 37–48. 10.1016/j.psychsport.2014.08.004 [DOI] [Google Scholar]
- Hughes K, Bellis M, Hardcastle K, Sethi D, Butchart A, Mikton C, et al. (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), 356–366. 10.1016/s2468-2667(17)30118-4 [DOI] [PubMed] [Google Scholar]
- Johnson R, & Onwuegbuzie A (2004). Mixed methods research: A research paradigm whose time has come. Educational Researcher, 33(7), 14–26. 10.3102/0013189×033007014 [DOI] [Google Scholar]
- Kendler K, Hettema J, Butera F, Gardner C, & Prescott C (2003). Life event dimensions of loss, humiliation, entrapment, and danger in the prediction of onsets of major depression and generalized anxiety. Archives of General Psychiatry, 60(8), 789–796. 10.1001/archpsyc.60.8.789 [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, & Williams JB (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kvale S, & Brinkmann S (Eds.). (2009). InterViews: Learning the craft of qualitative research interviewing. Los Angeles, CA: Sage. [Google Scholar]
- Lam JCW, Shields GS, Trainor BC, Slavich GM, & Yonelinas AP (2019). Greater lifetime stress exposure predicts blunted cortisol but heightened DHEA responses to acute stress. Stress and Health, 35(1), 15–26. 10.1002/smi.2835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levitt H, Motulsky S, Wertz F, Morrow S, & Ponterotto J (2017). Recommendations for designing and reviewing qualitative research in psychology: Promoting methodological integrity. Qualitative Psychology, 4(1), 2–22. 10.1037/qup0000082 [DOI] [Google Scholar]
- Longo Y, Coyne I, & Joseph S (2018). Development of the short version of the scales of general well-being: The 14-item SGWB. Personality and Individual Differences, 124, 31–34. 10.1016/j.paid.2017.11.042 [DOI] [Google Scholar]
- Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Medical Care, 46(3), 266–274. 10.1097/mlr.0b013e318160d093 [DOI] [PubMed] [Google Scholar]
- Malterud K, Siersma V, & Guassora A (2016). Sample size in qualitative interview studies. Qualitative Health Research, 26(13), 1753–1760. 10.1177/1049732315617444 [DOI] [PubMed] [Google Scholar]
- McEwen BS, & Gianaros P (2010). Central role of the brain in stress and adaptation. Annals of the New York Academy of Sciences, 1186(1), 190–222. 10.1111/j.1749-6632.2009.05331.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moesch K, Kenttä G, Kleinert J, Quignon-Fleuret C, Cecil S, & Bertollo M (2018). FEPSAC position statement: Mental health disorders in elite athletes and models of service provision. Psychology of Sport and Exercise, 38, 61–71. 10.1016/j.psychsport.2018.05.013 [DOI] [Google Scholar]
- Moore L, Young T, Freeman P, & Sarkar M (2017). Adverse life events, cardiovascular responses, and sports performance under pressure. Scandinavian Journal of Medicine & Science in Sports, 28(1), 340–347. 10.1111/sms.12928 [DOI] [PubMed] [Google Scholar]
- Morrow SL (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52(2), 250–260. 10.1037/0022-0167.52.2.250 [DOI] [Google Scholar]
- Neil R, McFarlane HM, & Smith AP (2017). Well-being in sport organizations In Wagstaff CRD (Ed.), The organizational psychology of sport: Key issues and practical applications (pp. 101–119). New York, NY: Routledge. [Google Scholar]
- Olvera Alvarez H, Provencio-Vasquez E, Slavich G, Laurent J, Browning M, McKee-Lopez G, et al. (2019). Stress and health in nursing students. Nursing Research, 68 (6), 453–463. 10.1097/nnr.0000000000000383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onwuegbuzie A, & Leech N (2005). Taking the “Q” out of research: Teaching research methodology courses without the divide between quantitative and qualitative paradigms. Quality and Quantity, 39(3), 267–295. 10.1007/s11135-004-1670-0 [DOI] [Google Scholar]
- Pearlin L, Schieman S, Fazio E, & Meersman S (2005). Stress, health, and the life course: Some conceptual perspectives. Journal of Health and Social Behavior, 46(2), 205–219. 10.1177/002214650504600206 [DOI] [PubMed] [Google Scholar]
- Pegg S, Ethridge P, Shields GS, Slavich GM, Weinberg A, & Kujawa A (2019). Blunted social reward responsiveness moderates the effect of lifetime social stress exposure on depressive symptoms. Frontiers in Behavioral Neuroscience, 13, 178 10.3389/fnbeh.2019.00178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reardon C, Hainline B, Aron C, Baron D, Baum A, Bindra A, et al. (2019). Mental health in elite athletes: International Olympic Committee consensus statement (2019). British Journal of Sports Medicine, 53(11), 667–699. 10.1136/bjsports-2019-100715 [DOI] [PubMed] [Google Scholar]
- Rice SM, Purcell R, De Silva S, Mawren D, McGorry PD, & Parker AG (2016). The mental health of elite athletes: A narrative systematic review. Sports Medicine, 46 (9), 1333–1353. 10.1007/s40279-016-0492-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan RM, & Deci EL (2001). On happiness and human potential: A review of research on hedonic and eudaimonic well-being. Annual Review of Psychology, 52(1), 141–166. 10.1146/annurev.psych.52.1.141 [DOI] [PubMed] [Google Scholar]
- Slavich GM (2020). Social safety theory: A biologically based evolutionary perspective on life stress, health, and behavior. Annual Review of Clinical Psychology, 16(1), 265–295. 10.1146/annurev-clinpsy-032816-045159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slavich GM, & Shields GS (2018). Assessing lifetime stress exposure using the stress and adversity inventory for adults (adult STRAIN). Psychosomatic Medicine, 80(1), 17–27. 10.1097/psy.0000000000000534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slavich GM, Stewart JG, Esposito EC, Shields GS, & Auerbach RP (2019). The Stress and Adversity Inventory for Adolescents (Adolescent STRAIN): Associations with mental and physical health, risky behaviors, and psychiatric diagnoses in youth seeking treatment. Journal of Child Psychology and Psychiatry, 60(9), 998–1009. 10.1111/jcpp.13038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer R, Kroenke K, Williams J, & Löwe B (2006). A brief measure for assessing generalized anxiety disorder. Archives of Internal Medicine, 166(10), 1092 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Sturmbauer S, Shields G, Hetzel E, Rohleder N, & Slavich G (2019). The stress and adversity inventory for adults (adult STRAIN) in German: An overview and initial validation. PloS One, 14(5), Article e0216419 10.1371/journal.pone.0216419 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swann C, Moran A, & Piggott D (2015). Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychology of Sport and Exercise, 16, 3–14. 10.1016/j.psychsport.2014.07.004 [DOI] [Google Scholar]
- Tamminen KA, & Holt NL (2012). Adolescent athletes’ learning about coping and the roles of parents and coaches. Psychology of Sport and Exercise, 13(1), 69–79. 10.1016/j.psychsport.2011.07.006 [DOI] [Google Scholar]
- Teddlie C, & Tashakkori A (2011). Mixed methods research: Contemporary issues in an emerging field In Denzin N, & Lincoln Y (Eds.), The SAGE handbook of qualitative research (pp. 285–299). London: Sage. [Google Scholar]
- Toussaint L, Shields GS, Dorn G, & Slavich GM (2016). Effects of lifetime stress exposure on mental and physical health in young adulthood: How stress degrades and forgiveness protects health. Journal of Health Psychology, 21(6), 1004–1014. 10.1177/1359105314544132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turney K (2014). Stress proliferation across generations? Examining the relationship between parental incarceration and childhood health. Journal of Health and Social Behavior, 55(3), 302–319. 10.1177/0022146514544173 [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2004). Promoting mental health: Concepts, emerging evidence, practice: Summary report. Geneva: World Health Organization. [Google Scholar]