

Abstract
In the present study, malignant mesothelioma (MM) cases in Japan were investigated retrospectively. We extracted records for 6030 cases of death due to MM between 2003 and 2008 to clarify the clinical features of MM, including its association with asbestos exposure (AE). Of all these cases, a clinical diagnosis of MM was confirmed for 929. The origin of MM included the pleura in 794 cases (85.5%), the peritoneum in 123 cases (13.2%), the pericardium in seven cases (0.8%), and the testicular tunica vaginalis in five cases (0.5%). The histological subtypes of MM included 396 epithelioid (55.9%), 154 sarcomatoid (21.7%), 126 biphasic (17.8%), and 33 cases (4.7%) classified as “other types”. Of all the MM cases, AE was indicated in 76.8% and pleural plaques were detected in 34.2%. The number of asbestos particles was determined in 103 cases of MM. More than 1000 asbestos particles per gram dried lung tissue were detected in 74.8% of cases and more than 5000 particles were detected in 43.7% of cases. We compared patient characteristics and the diagnostic procedures for MM before and after the “Kubota shock”. Compared with the early phase of this study (2003–2005), the median age at diagnosis of MM was higher, the number of cases without definite diagnosis of MM was lower, the proportion of cases diagnosed by thoracoscopy was higher, and the percentage of cases in which the occupational history was described in the medical records was significantly higher in the later phase (2006–2008). Our study confirmed that more than 70% of MM cases in Japan are associated with AE. The “Kubota shock” may affect some features pertaining to MM. (Cancer Sci 2012; 103: 483–490)
Malignant mesothelioma (MM) is an aggressive tumor that develops from mesothelial cells of the pleura, peritoneum, pericardium, or testicular tunica vaginalis.( 1 ) A newspaper article published in June 2005 reported that five residents who lived near the now‐closed asbestos cement pipe plant in Amagasaki, Japan, developed pleural mesothelioma.( 2 ) The asbestos‐related problems that the article described caused considerable social concern, resulting in the so‐called “Kubota shock”. Asbestos has attracted increasing social attention, but no large‐scale studies have been conducted to date investigating the clinical features of MM in Japan. In Japan, patients who have a history of occupational asbestos exposure (AE) and have developed MM are receive worker’s compensation. However, of the 878 cases of death due to MM in 2003, only 85 cases were actually compensated (Ministry of Health, Labor and Welfare of Japan; http://www.mhlw.go.jp/houdou/2006/05/h0530‐1.html, accessed 30 May 2006). Based on these figures, there is an urgent need to clarify the association between MM and AE in Japan, so we initiated the present retrospective survey to address this serious issue. We planned to investigate all MM cases in Japan and analyzed more than 6000 MM cases registered in the Vital Statistics yearly survey carried out by the Ministry of Health, Labour and Welfare. We have already reported the preliminary results of the analyses of the cases between 2003 and 2005.( 3 ) In the present paper, we report the final results concerning the clinical features of MM in Japan between 2003 and 2008, with a particular focus on the association between MM and AE. The transition of some features of MM, such as patient characteristics and diagnostic procedures, before and after the Kubota shock is also discussed.
Materials and Methods
Study population. We requested and received authorization to view the death records in the Vital Statistics survey in Japan and extracted all the cases of death due to MM between 2003 and 2008. There were 6030 deaths due to MM (878 deaths in 2003, 953 in 2004, 911 in 2005, 1050 in 2006, 1068 in 2007, and 1170 in 2008), as shown in Figure 1. Based on the information in the death records, we contacted the closest living relatives by mail to obtain consent for our research. Consent was obtained in 2069 cases (34.3%). Based on authorization from the relatives, we applied to each medical institution to obtain medical information for the patients, including medical records, X‐ray films, and/or computed tomography (CT) images. Information was obtained in 1111 cases (53.7%). The institutes and hospitals that provided information for our study are listed in Appendix I. We reviewed the medical records and radiological images to confirm a clinical and pathological diagnosis of MM. As a result, a clinical diagnosis of MM was confirmed in 929 cases (Fig. 2). The classification of pathological subtypes was based on World Health Organization criteria.( 4 ) The clinical stage of MM was determined according to the criteria of the International Mesothelioma Interest Group (iMig).( 5 )
Figure 1.
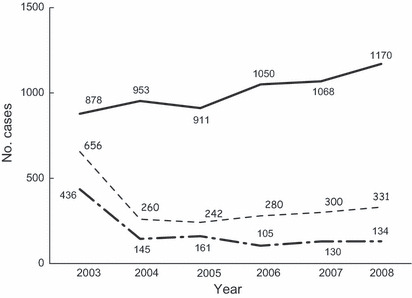
Changes in the number of subjects over the study period. The solid line indicates the number of deaths due to mesothelioma. The dashed line indicates the number of cases in which consent was obtained from the closest living relative. The dashed‐dotted line indicates the number of cases in which medical information was provided by the medical institution.
Figure 2.
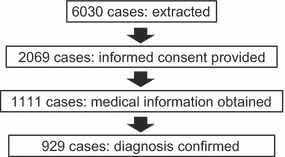
Diagram showing case collection in the present study.
Assessment of AE. The patients’ work histories, those of their family members, and residential histories for each case were investigated for AE. The residential histories of the patients covered the time period from their youth, which may suggest environmental exposure to asbestos based on information in their medical records. Questionnaires were also given to the patients’ family members. Pleural plaques were assessed based on chest X‐ray and/or CT images as the characteristic finding indicating AE.
Asbestos particle analysis. Asbestos particles were quantified based on lung tissues obtained from surgery or autopsy, which were provided from each medical institution, using the protocol modified by Kohyama and Suzuki.( 6 ) Briefly, normal lung tissues (1–2 g) without tumor involvement were dehydrated at 100°C, weighed precisely, and then microcut. The tissues were digested in an aqueous solution containing 5–20% sodium hypochlorite. Following digestion, samples were centrifuged at 1450g for 10 min and then resuspended in 50 mL distilled water. Samples were mixed well and suction filtered through a 0.45‐μm Millipore filter (Merck Millipore, Tokyo, Japan). The filter was dehydrated and dried with acetone vapor. Asbestos particles were then counted using phase contrast microscopy and the number of asbestos particles per gram dried lung tissue was calculated. This analysis was performed at the Okayama Rosai Hospital.
Statistical analyses. Comparisons between independent groups were performed using the Chi‐squared test and non‐parametric analysis of the Mann–Whitney U‐test. Mean values were compared using t‐tests. Statistical calculations were performed with SPSS version 11.0 (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of patients with MM. Based on the description on the medical records and a review of the radiographs, a clinical diagnosis of MM was confirmed in 929 cases. These included 753 men (81.1%) and 176 women (18.9%). The median age at diagnosis was 67.0 years (range 16–94 years). The median age at the time of diagnosis of MM was significantly higher in the cases in which the patient had died between 2006 and 2008 (late phase) than in cases in which the patient had died between 2003 and 2005 (early phase; 69.4 vs 66.4 years, respectively; P < 0.001). In 101 cases (9.1%), a clinical diagnosis of MM was made on the basis of radiological or laboratory findings, such as hyaluronic acid in the pleural fluid, without pathological confirmation. We defined these cases as “suspected MM”. The number of cases of suspected MM decreased in the late phase compared with the early phase (26 [7.0%] vs 70 cases [9.4%], respectively; P < 0.001). The origin of MM included the pleura in 794 cases (85.5%) of MM and 96 cases of suspected MM, the peritoneum in 123 cases (13.2%) of MM and five cases of suspected MM, the pericardium in seven cases (0.8%) of MM, and the testicular tunica vaginalis in five cases (0.5%) of MM. Eighty‐one cases (7.3%) were excluded from further analysis because they were diagnosed as having other diseases based on their clinical and pathological records. These included 33 cases diagnosed as lung cancer, four cases diagnoses as ovarian cancer, three cases diagnosed as solitary fibrous tumor, and three cases diagnosed as carcinomatous pleuritis from unknown origin (Table 1).
Table 1.
Confirmed diagnoses
| Diagnoses | No. cases (%) |
|---|---|
| Malignant mesothelioma | 929 (83.6) |
| Pleura | 794 |
| Peritoneum | 123 |
| Pericardium | 7 |
| Testicular tunica vaginalis | 5 |
| Malignant mesothelioma (suspected) | 101 (9.1) |
| Pleura | 96 |
| Peritoneum | 5 |
| Lung cancer | 33 (3.0) |
| Lung cancer (suspected) | 24 (2.2) |
| Ovarian cancer | 4 (0.4) |
| Solitary fibrous tumor | 3 (0.2) |
| Carcinomatous pleuritis | 3 (0.2) |
| Others | 14 (1.3) |
| Total | 1111 (100) |
Diagnosis of MM. The histological subtype of MM was indicated in the medical records in 709 cases (76.3%). Subtypes included 396 (55.9%) epithelioid cases, 154 (21.7%) sarcomatoid cases, 126 (17.8%) biphasic cases, and 33 (4.7%) cases from other types (Table 2). The diagnostic procedure was described in 891 cases and histological diagnosis was confirmed in 776 of 891 cases (87.1%). Pathological specimens were obtained by thoracoscopic biopsy (46.1%), transcutaneous needle biopsy (32.4%), thoracotomy (18.4%), autopsy (1.8%), or other procedures in MM cases of the pleura. In cases of MM of the peritoneum, specimens were obtained by laparotomy (62.7%), laparoscopic biopsy (23.5%), transcutaneous needle biopsy (7.8%), or other procedures. Diagnoses were made on the basis of cytological analysis of the pleural fluid in 94 MM cases of the pleura, the ascites in 19 cases of MM of the peritoneum, and the pericardial fluid in two cases of MM of the pericardium.
Table 2.
Histological subtypes of malignant mesothelioma
| Pleura (n = 606) | Peritoneum (n = 95) | Others (n = 8) | Total (n = 709) | % | |
|---|---|---|---|---|---|
| Epithelioid | 325 | 68 | 3 | 396 | 55.9 |
| Sarcomatoid | 141 | 11 | 2 | 154 | 21.7 |
| Biphasic | 111 | 12 | 3 | 126 | 17.8 |
| Others | 29 | 4 | 0 | 33 | 4.7 |
We also investigated changes in diagnostic procedures. In the early phase, 150 cases (29.8%) were diagnosed by thoracotomy or laparotomy. This proportion decreased significantly decreased to 16.2% in the late phase (P < 0.001). Conversely, the proportion of cases diagnosed by thoracoscopy or laparoscopy increased significantly from 34.0% in the early phase to 58.8% in the late phase (P < 0.001). Immunohistochemical analysis was performed in 734 (97.0%) of cases diagnosed on the basis of histological findings, as well as in 55.4% of cases diagnosed on the basis of cytological analysis of the pleural fluid, ascites, or pericardial fluid. Immunohistochemical analysis was performed in 39.7% of cases diagnosed using body fluids in the early phase, and this percentage increased significantly to 82.4% in the late phase (P < 0.001).
History of AE. A history of AE was investigated in 929 cases that had a definite diagnosis of MM. Information regarding AE was obtained through the medical records and/or questionnaires administered to the patients’ families in 824 cases (88.7%). Among these, occupational AE was indicated in 607 cases (73.7%; Table 3). In 18 cases, AE was the result of an asbestos source in the neighborhood; nine of these cases had a history of residing in Amagasaki city, around the Kubota plant. In eight cases, AE in the home was indicated (i.e. the patient’s husband or another family member had a history of occupational AE). As a whole, AE was indicated in 633 cases (76.8%). Of the 584 patients who died between 2004 and 2008 in whom occupational AE was indicated, an occupational history was given in the medical record for 205 cases (47.7%). The questionnaire administered to family members revealed occupational AE in 363 cases (84.4%).
Table 3.
Detailed history of asbestos exposure in 824 mesothelioma cases
| No. cases (%) | |
|---|---|
| Occupational exposure | 607 (73.7) |
| Neighborhood exposure | 18 (2.2) |
| Home exposure | 8 (0.9) |
| Total | 633 (76.8) |
Occupational category of AE. Table 4 divides the 607 cases with a history of occupational AE into different occupational categories. In cases where the patient had multiple jobs that involved AE, the job with the longest work history was selected. On the basis of this analysis, 131 patients (21.6%) had worked in the construction industry, 91 patients (15.0%) had worked in the shipbuilding industry, 46 patients (7.6%) had worked in plumbing, 44 patients (7.2%) had performed electrical work, 41 patients (6.8%) had worked in steel mill production, 36 patients (5.9%) had worked in manufacturing asbestos products, 35 patients (5.8%) had worked in automobile manufacturing, and 33 patients (5.4%) had worked in demolition. The occupational history was provided in the medical records for 28.7% of patients in the early phase, with this percentage increasing significantly to 62.4% in the late phase.
Table 4.
Occupational category associated with asbestos exposure
| Occupation | Pleura (n = 540) | Peritoneum (n = 59) | Pericardium (n = 5) | TTV (n = 3) | Total (n = 607) |
|---|---|---|---|---|---|
| Construction | 120 | 9 | 1 | 1 | 131 |
| Shipbuilding | 81 | 8 | 1 | 1 | 91 |
| Plumbing | 43 | 2 | 1 | 0 | 46 |
| Electrical work | 40 | 4 | 0 | 0 | 44 |
| Steel production | 37 | 3 | 0 | 1 | 41 |
| Asbestos products industry | 25 | 11 | 0 | 0 | 36 |
| Automobile manufacturing | 32 | 3 | 0 | 0 | 35 |
| Demolition work | 31 | 2 | 0 | 0 | 33 |
| Manufacturing | 20 | 3 | 0 | 0 | 23 |
| Chemical manufacturing | 17 | 0 | 1 | 0 | 18 |
| Warehouse management | 13 | 4 | 0 | 0 | 17 |
| Cement manufacturing | 13 | 1 | 0 | 0 | 14 |
| Shipman* | 10 | 0 | 0 | 0 | 10 |
| Transportation | 10 | 0 | 0 | 0 | 10 |
| Metal manufacturing | 8 | 2 | 0 | 0 | 10 |
| Others | 33 | 7 | 1 | 0 | 41 |
*Shipman refers to someone who works on a boat in some capacity. TTV, testicular tunica vaginalis.
Duration of AE. The duration of AE and the period of latency for the onset of MM were investigated in MM cases with occupational AE (Table 5). The median duration of AE was 43 years and the median period of latency for disease onset of MM was 43.7 years. In MM of the pleura and peritoneum, the median duration of AE was 30 and 28 years, respectively. The median period of latency for disease onset for MM of the pleura and peritoneum was 43.5 and 42.5 years, respectively.
Table 5.
Duration of asbestos exposure and latency of mesothelioma
| Median | Range | |
|---|---|---|
| Mesothelioma of the pleura (n = 540) (years) | ||
| Duration | 30 | 0.25–58 |
| Age at diagnosis | 68 | 38–94 |
| Latency | 43.5 | 14–81 |
| Mesothelioma of the peritoneum (n = 59) (years) | ||
| Duration | 28 | 1.5–54 |
| Age at diagnosis | 68 | 25–89 |
| Latency | 42.5 | 19–73 |
| Total* (n = 607) (years) | ||
| Duration | 30 | 0.25–58 |
| Age at diagnosis | 68 | 25–94 |
| Latency | 43 | 13–81 |
*This includes five cases of pericardial mesothelioma and three cases of testicular tunica vaginalis mesothelioma.
Pleural plaques. The prevalence of pleural plaques was investigated based on chest X‐ray or CT images provided by each medical institution. Pleural plaques were detected in 280 of 818 cases (34.2%), including 242 of 703 cases (34.4%) of MM of the pleura, 36 of 106 cases (33.9%) of MM of the peritoneum, one of seven cases (14.3%) of MM of the pericardium, and one of two cases (50%) of MM of the testicular tunica vaginalis. Based on these figures, we investigated the prevalence of pleural plaques in each job category with AE. For those who worked in the manufacture of asbestos products and shipbuilding, the prevalence of pleural plaques was 75.8% and 58.6%, respectively (Fig. 3). Pleural plaques were also detected in 31 cases (13.5%) of MM cases without an obvious occupational history of AE, including two cases with a history of non‐occupational AE.
Figure 3.
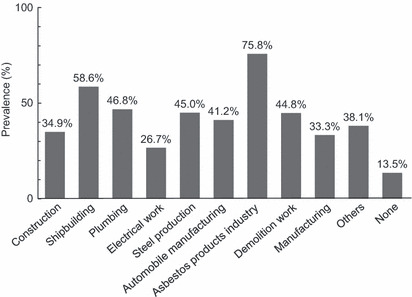
Prevalence of pleural plaques, as determined by chest X‐ray and/or computed tomography, for each occupational category.
Asbestos particles. The number of asbestos particles was determined in 103 MM cases (92 of the pleura and 11 of the peritoneum), in which lung tissue was provided by the medical institution. More than 1000 asbestos particles per gram dried lung tissue were detected in 77 cases (74.8%) and more than 5000 particles were detected in 45 cases (43.7%). Asbestos particles were more frequently detected in MM of the peritoneum than in MM of the pleura (P = 0.046), as shown in Figure 4. For patients with MM of the pleura, more than 1000 asbestos particles were detected in 67 cases (72.8%) and more than 5000 particles were detected in 37 cases (40.2%). For patients with MM of the peritoneum, more than 1000 particles were detected in 10 cases (90.9%) and more than 5000 particles were detected in eight cases (72.7%). The number of asbestos particles for each job category is shown in Figure 5. More than 5000 particles were detected in seven of eight patients (90.9%) who worked in the manufacture of asbestos products, in 16 of 21 patients (76.2%) who worked in shipbuilding, and in nine of 17 patients (52.9%) who worked in the construction industry. More than 1000 particles were detected in more than 90% of the patients who worked in the shipbuilding and construction industries. Asbestos particles were also detected in the cases without occupational AE. More than 5000 particles per gram dried lung were detected in one of 16 (6.3%) cases and more than 1000 particles were detected in eight of 16 (50%) cases. These included one case with a history of residence in Amagasaki city, near the Kubota plant (1042/g). We then analyzed the association between the prevalence of pleural plaques and asbestos particles in the lung and found an increased number of asbestos particles in cases of MM with pleural plaques (P < 0.001). It is of note that in more than half of the cases without pleural plaques (32/55; 58.2%) more than 1000 asbestos particles per gram dried lung were detected, with more than 5000 particles detected in 11 (25.0%) cases.
Figure 4.
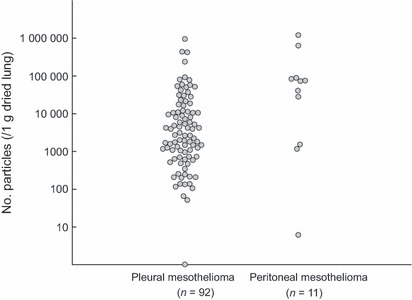
Distribution of the number of asbestos particles in the lung for cases of pleural and peritoneal mesothelioma.
Figure 5.
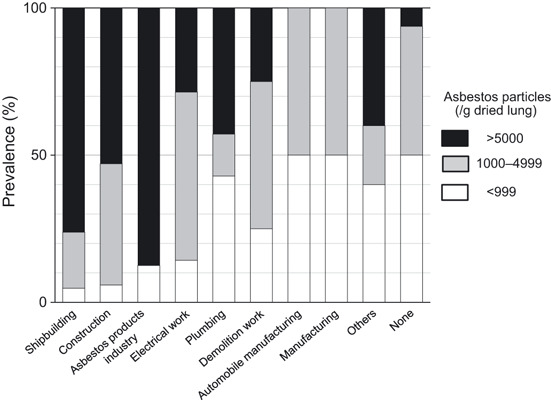
Prevalence of asbestos particles in the lung of mesothelioma cases for each occupational category.
Discussion
In the present study, we investigated the features of 1111 MM cases for which medical information was provided by medical institutions following consent from the patient’s closest living relative. We believe that the present study is the largest conducted in Japan into MM. There were 929 cases of confirmed MM and we regarded 101 cases (9.1%) as “suspected MM” because a pathological diagnosis had not been made. Compared with the early phase, the number of cases of suspected MM decreased significantly in the late phase. One possible explanation for this is that the propagation of immunohistochemical analysis may have contributed to definite diagnoses of MM. Immunohistochemical analysis was performed in most of the cases (97.0%) to obtain a diagnosis based on histological findings. An increased number of cases was diagnosed on the basis of cytological findings in the pleural fluid, ascites, or pericardial fluid in the late phase than in the early phase. Another possibility is the widespread dissemination of less‐invasive diagnostic procedures. The cases of suspected MM include more elderly patients (median age 80 years) in the early phase and we suppose that these cases may have been excluded from diagnostic procedures. During the study period, the proportion of cases diagnosed using thoracotomy or laparotomy decreased significantly, whereas the number of cases diagnosed using thoracoscopy or laparoscopy increased significantly. Thoracoscopic exploration can be performed under a local anesthetic and an increased number of cases were diagnosed using this procedure.( 7 ) Another possibility for the decrease in the number of cases of suspected MM is that patients with a pathologically confirmed diagnosis of MM could received Worker’s Compensation or compensation from the Act on Asbestos Health Damage Relief established following the “Kubota shock”. Dissemination of less‐invasive diagnostic procedures, accurate pathological analysis techniques, and widening of coverage by the compensation system may have contributed to definitive diagnostic confirmation of MM in Japan.
A history of AE could be revealed in interviews with the patients and confirmed medically by the presence of pleural plaques and/or asbestos particles. In the present study, occupational AE was evident in more than 70% of MM cases. This percentage is consistent with that reported in other countries.( 8 ) An association between MM and AE is well established worldwide.( 9 , 10 , 11 ) Thus far, there have been two reports based on a small number of cases that suggested this association between AE and MM in Japan,( 12 , 13 ) but no large‐scale study has been conducted concerning the clinical features of MM in Japan. The median latency of disease onset is 43 years. Within the period of the present study, the percentage of cases in which the occupational history of the patients was described in their medical records increased significantly. These results indicate the widespread dissemination of knowledge to physicians concerning the association between MM and AE.
Asbestos particle analysis is one of the most reliable methods to evaluate AE. A level exceeding 1000 particles per gram dry lung tissue is associated with occupational AE and levels of more than 5000 particles are consistent with a doubling of the risk of lung cancer.( 14 ) In the present study, these analyses revealed more than 1000 particles per gram dry lung tissue in 74% of cases examined. These results confirm that most of the MM cases in Japan are associated with AE. The number of asbestos particles was higher in cases in which the patients had an occupational history related to industries with a high level of AE, such as the asbestos products industry or shipbuilding. The friction materials used in automobiles or the asbestos plates used in manufacturing may contain chrysotile fibers, which are less likely to form asbestos particles than other types of asbestos. We think this may explain why automobile and manufacturing workers had comparatively low levels of asbestos particles in their lungs. Radiological examination detected pleural plaques in approximately 34% of cases (based on chest X‐ray or CT). The prevalence of plaques was higher in patients whose occupation was in an industry in which the number of asbestos particles was at a high level of AE, such as the asbestos products industry or shipbuilding. Cases with pleural plaques were found to have significantly higher asbestos particle counts than those without plaques, even though more than half of the cases without plaques were found to have 1000 particles per gram dry lung tissue, including 25% of cases with more than 5000 particles per gram dry lung tissue. These findings suggest that the presence of pleural plaques is not sufficient for an evaluation of a history of AE. Physicians should be aware that even in cases without pleural plaques, occupational or environmental AE is not improbable.
In conclusion, our study confirms that more than 70% of cases of MM in Japan are associated with AE. The “Kubota shock” may affect some features pertaining to MM.
Disclosure Statement
The authors declare that they have no conflicts of interest.
Acknowledgments
This research was supported mainly by grants from the research foundation of the Ministry of Health, Labour and Welfare of Japan (200500129A, 200635021A, 200733015A, 200733015B, 200836010A, 200938007A, and 201032004B). This research is a part of the research and development and dissemination projects related to the 13 fields of occupational injuries and illnesses of the Japan Labour, Health and Welfare Organization. The authors thank the living relatives of the mesothelioma patients who provided consent for our research. The authors also thank the medical institutions that provided the medical information for the mesothelioma cases. The authors thank Drs Yuko Akagi, Masaaki Fujiki, and Sumie Seno for asbestos particle analyses.
Appendix I: Medical institutions that provided medical information for the mesothelioma cases evaluated in the present study
Hokkaido. Family Clinic, Makita Hospital, Keiyukai Sapporo Hospital, Sapporo Minami Seisyu Hospital, Teine Keijinkai Hospital, Hokkaido Kin‐Ikyo Chuo Hospital, Hakodate Hospital, Toya Onsen Hospital, Steel Memorial Muroran Hospital, Muroran City General Hospital, Hokkaido Prefecture Tomakomai Hospital, Sapporo City General Hospital, Sapporo‐Kosei General Hospital, Sapporo Minami‐Ichijo Hospital, Sapporo Minami‐Sanjo Hospital, Hokkaido University Hospital, Hokkaido Social Insurance Hospital, KKR Sapporo Medical Center, NHO Hokkaido Medical Center, Hokkaido Ohno Hospital, Sapporo Higashi Tokushukai Hospital, Iwamizawa Hokusyokai Hospital, Asahikawa City Hospital, Fukagawa Municipal Hospital, Asahikawa‐Kosei General Hospital, Asahikawa Medical University Hospital, Obihiro‐Kosei General Hospital, Abashiri‐Kosei General Hospital, Shimokawa Town Hospital.
Aomori. Aomori Municipal Hospital, Aomori Prefectural Central Hospital, Mutsu General Hospital, Hirosaki Chuo Hospital, Hirosaki University School of Medicine & Hospital, Aomori Jikeikai Hospital, Tsugaru Seijinbyo Center.
Akita. Akita Red‐Cross Hospital, Yokote Municipal Hospital, Hiraka General Hospital, Senbokukumiai Hospital, Sasago Clinic, Koto General Hospital.
Iwate. Iwate Medical University Hospital, Iwate Prefectural Central Hospital, Iwate Prefectural Isawa Hospital, Tono Hospital, and Iwate Prefectural Takada Hospital.
Miyagi. Tohoku University Hospital, Sendai Kosei Hospital, Tohoku Rosai Hospital, Miyagi Cancer Center, Kurokawa Hospital, Tohoku Kosei Nenkin Hospital, NHO Sendai Medical Center, Saka General Hospital, Ishinomaki Red Cross Hospital, Tome City Hospital, Kesennuma City Hospital, Miyagi Cardiovascular & Respiratory Center, Furukawa Seiryo Hospital.
Niigata. Tachikawa Medical Center, Nagaoka Red Cross Hospital, Niigata Rosai Hospital, Niigata Prefectural Central Hospital, Keinan General Hospital, Kariwagun General Hospital, Niigata Prefectural Koide Hospital, Ojiya General Hospital, Tokamachi Hospital, Niigata Rinko Hospital, Kido Hospital, Niigata City General Hospital, Saiseikai Niigata Daini Hospital, Toyosaka Hospital, Niigata Cancer Center Hospital, Ryotsu Hospital, Sado General Hospital, Niitsu Medical Center Hospital, Kaetsu Hospital, Niigata Prefectural Shibata Hospital, Murakami Kinen Hospital, Suibaragou Hospital.
Fukushima. Iwase General Hospital, Tsuboi Cancer Center Hospital, Ohta Nishinouchi Hospital, Southern Tohoku Research Institute for Neuroscience Hospital, Takada Kosei Hospital, Kashima Hospital, Iwaki Kyouritsu Hospital.
Yamagata. Yamagata Saisei Hospital, Yamagata Prefectural Shinjo Hospital, Shonai Hospital, Saito Clinic, Tsuruoka Kyouritsu Hospital.
Ibaragi. Tsuchiura Kyodo General Hospital, JA Toride Medical Center, Tsukuba Medical Center Hospital, Johsai Hospital, The Prefecture West General Hospital, Ibaraki Prefectural Central Hospital, Hitachinaka General Hospital, Kashima Rosai Hospital, Hitachi General Hospital, NHO Ibarakihigashi National Hospital.
Tochigi. Tochigi Cancer Center, Dokkyo Medical University Hospital, Oyama Municipal Hospital, Ashikaga Hospital, Nogi Hospital, Hoshino Hospital.
Gunma. Komai Hospital, Maebashi Red Cross Hospital, Gunma University Hospital, Maebashi Kyouritsu Hospital, Saiseikai Maebashi Hospital, Isesaki Municipal Hospital, Gunma Prefectural Cancer Center, Tatebayashi Kosei Hospital, Fujioka General Hospital, Usui Hospital, Ohtashiyabuzukahonmachi Kokuho Clinic.
Saitama. Saitama Municipal Medical Center, Toda Chuo General Hospital, Saitama Red Cross Hospital, Maruyama Memorial General Hospital, Soka Municipal Hospital, Kuki General Hospital, Aida Hospital, Dokkyo Medical University Koshigaya Hospital, Higashisaitama General Hospital, Saiseikai Kurihashi Hospital, Saitama Medical University Hospital, Saitama Medical University Saitama Medical Center, Saitama Medical University International Medical Center, Higashimatsuyama Municipal Hospital, Musashi Ranzan Hospital, Japanese Red Cross Ogawa Hospital, Hanno Municipal Hospital, Toyooka‐daiichi Hospital, Saitama Prefectural Cardiovascular & Respiratory Medical Center, Ageo Kousei Hospital, Saitama Cancer Center, Kitasato University Kitasato Institute Medical Center Hospital, Chichibu Seikyo Hospital, Minano Hospital.
Chiba. Inoue Memorial Hospital, Chiba Cancer Center, NHO Chiba‐East‐Hospital, Chiba Kaihin Municipal Hospital, Sakusabesaka Street Clinic, Kasori Hospital, Shinmatsudo Central General Hospital, Shirai Seijinkai Hospital, Nippon Medical School Chiba Hokusoh Hospital, Matsudo City Hospital, Aozora Clinic, Funabashi Futawa Hospital, Saiseikai Narashino Hospital, St. Marguerite Hospital, Kashiwa City Hospital, National Cancer Center Hospital East, Kikkoman General Hospital, Seirei Sakura Citizen Hospital, Toho University Medical Center Sakura Hospital, Sanmu Medical Center, Asahi Hospital, Chiba Rosai Hospital, Yarita Hospital, Kimitsu Chuo Hospital, Hananotani Clinic, Kameda Medical Center, Yamanouchi Hospital, Mobara Chuo Hospital, Teikyo University Chiba Medical Center, Satsukidai Hospital.
Tokyo. Sanraku Hospital, Tokyo Teishin Hospital, Tokyo Metropolitan Police Hospital, Jikei University Hospital, Saiseikai Central Hospital, Eiju Hospital, Tokyo Kensei Hospital, Nippon Medical School Hospital, The University of Tokyo Hospital, Juntendo University Hospital, Higashijujo Hospital, Ouji Hospital, Towa Hospital, Jieikai Hospital, Kameari Hospital, Homecare Clinic Kawagoe, Edogawa Hospital, Jukoukai Hospital, Juntendo Tokyo Koto Geriatric Medical Center, NTT Medical Center Tokyo, Yutaka Hospital, Showa University Hospital, Tokyo Rosai Hospital, Toho University Medical Center Omori Hospital, Kimura Hospital, Ikegami General Hospital, Naito Hospital, NHO Tokyo Medical Center, Toho University Medical Center Ohashi Hospital, Tokyo Kyosai Hospital, Nissan Tamagawa Hospital, Kanto Central Hospital, Keio University Hospital, Tokyo Denryoku Hospital, Tokyo Medical University Hospital, National Center for Global Health and Medicine, Tokyo Women’s Medical University Hospital, Social Insurance Chuo General Hospital, Sekino Hospital, Toshima Hospital, Nihon University School of Medicine Itabashi Hospital, Tokiwadai Geka Hospital, Takashimadaira Clinic, Kyorin University Hospital, Nomura Hospital, Tokyo Metropolitan Tama Medical Center, NHO Disaster Medical Center, Tachikawa Sougo Hospital, Hinodegaoka Hospital, Tokai University Hachioji Hospital, Hachioji Sannou Hospital, Tokyo Medical University Hachioji Medical Center, Fukujuji Hospital, Tama‐nambu Chiiki Hospital.
Kanagawa. St. Marianna University of Medicine Toyoko Hospital, Kanto Rosai Hospital, Inadanoborito Hospital, St. Marianna University of Medicine Hospital, Keiyu Hospital, Japanese Red Cross Tsukui Hospital, Kanagawaken Hospital, Yokohama Rosai Hospital, Showa University Northern Yokohama Hospital, Showa University Fujigaoka Hospital, Fuchinohe Hospital, Soai Hospital, Sagamihara Kyodo Hospital, Yokohama Central Hospital, Yokohama City University Medical Center, Byoubugaura Hospital, Yokohama City University Hospital, Yokohama Minami Kyousai Hospital, Kanazawabunko Hospital, Kanagawa Cardiovascular and Respiratory Center, Yokosuka Kyosai Hospital, Yokosuka General Hospital Uwamachi, Seirei Yokohama Hospital, Yokosuka City Hospital, Yokohama City Hospital, St. Marianna University School of Medicine Yokohama Seibu Hospital, Kanagawa Cancer Center, Yamato Municipal Hospital, Ebina General Hospital, Syonan Izumi Hospital, Yokohama Sakae Kyosai Hospital, Kiyokawa Hospital, Shonan Memorial Hospital, Odawara Municipal Hospital, Shonan Central Hospital, Chigasaki Municipal Hospital, Chigasaki Tokusyukai General Hospital, Hiratsuka Kyosai Hospital, Ashigarakami Hospital, Isehara Kyodo Hospital, Tokai University Hospital.
Yamanashi. Kofu Kyoritsu Hospital, Yamanashi Kosei Hospital, University of Yamanashi Hospital.
Shizuoka. Numazu City Hospital, Seirei Numazu Hospital, Susono Red Cross Hospital, Juntendo University Shizuoka Hospital, Shizuoka Cancer Center, Hattori Clinic, Ito Hospital, Fuji City General Hospital, Fujinomiya Municipal Hospital, Shizuoka General Hospital, Haibara General Hospital, Kanbara General Hospital, Shizuoka Saiseikai General Hospital, Yamanoue Hospital, Yaizu City Hospital, Fujieda Municipal General Hospital, Shimada Municipal Hospital, Hamamatsu Rosai Hospital, Seirei Hamamatsu General Hospital, Hamana Hospital, Hamamatsu University School of Medicine University Hospital, Hamamatsu Medical Center, Seirei Mikatahara General Hospital, Hamamatsu Red Cross Hospital, Kakegawa Municipal General Hospital, Omaezaki Municipal Hospital.
Nagano. Aiwa Hospital, Saku Central Hospital, NHO Shinsyu Ueda Medical Center, Hokushin General Hospital, Karuizawa Municipal Hospital, Tomi Civilian Hospital, Aizawa Hospital, Suwa Red Cross Hospital, Iida Municipal Hospital.
Aichi. Toyokawa City Hospital, Gamagori City Hospital, Aichi Cancer Center Aichi Hospital, Nishio Municipal Hospital, Anjo Kosei Hospital, Hekinan Municipal Hospital, Kariya Toyota General Hospital, Meitetsu Hospital, Aichi Saiseikai Hospital, Japanese Red Cross Nagoya Daiichi Hospital, Nagoya Ekisaikai Hospital, Sumitomo Kinen Hospital, Chubu Rosai Hospital, Rinko Hospital, Kyoritsu General Hospital, Daido Hospital, Minami Seikyo Hospital, Nagoya Municipal Seibu Medical Center Johoku Hospital, Nagoya University Hospital, Japanese Red Cross Nagoya Daini Hospital, Nagoya City University Hospital, Nagoya Memorial Hospital, Aichi Kokusai Hospital, Fujita Health University Hospital, Toyota Memorial Hospital, Chubu Hospital, Handa City Hospital, Tokai Municipal Hospital, Chita City Hospital, Tokoname City Hospital, Aichi Medical University Hospital, Konan Kosei Hospital, Komaki City Hospital, Kasugai Municipal Hospital, Asahi Rosai Hospital, Tosei General Hospital, Daiyukai General Hospital, Aichi Cardiovascular & Respiratory Medical Center, Yamashita Hospital, Bisai Hospital.
Gifu. Gifu Municipal Hospital, Kishimoto Hospital, Ogaki Municipal Hospital, Kumiai Kosei Hospital, Gifu Social Insurance Hospital, Kosaka Kokuho Clinic, Tohno Kosei Hospital, Ena Municipal Hospital.
Toyama. Toyama University Hospital, Toyama Red Cross Hospital, Toyama Prefectural Central Hospital, Toyama Kyoritsu Hospital, Nanto Municipal Hospital, Toyama Rosai Hospital, Shinseikai Toyama Hospital, NHO Toyama Hospital, Miwa Hospital, Toyama City Hospital.
Ishikawa. Kanazawa Social Insurance Hospital, Kanazawa Medical University Hospital, Saiseikai Kanazawa Hospital, NHO Kanazawa Medical Center, Tsurugi Hospital, Eijukai Mirai Hospital, Komatsu Municipal Hospital, Noto General Hospital, Keiju General Hospital.
Fukui. Nitta Gastrointestinal and Radiology Hospital, Fukui General Hospital, Municipal Tsuruga Hospital, Fukui Red Cross Hospital, Fukui Saiseikai Hospital.
Shiga. Otsu Municipal Hospital, Social Insurance Shiga Hospital, Shiga University of Medical Science Hospital, Hikone Municipal Hospital, Shiga Medical Center for Adults, Kusatsu General Hospital, NHO Shiga Hospital.
Mie. Yokkaichi Municipal Hospital, Mie Prefectural Medical Center, Yamamoto General Hospital, Kuze Gastrointestinal Clinic, Suzuka Chuo General Hospital, Mie University Hospital.
Kyoto. Takeda Hospital, Nishijin Hospital, Kyoto University Hospital, Yakushiyama Hospital, Kyoto Min‐Iren Chuo Hospital, Japanese Red Cross Kyoto Daiichi Hospital, The Japan Baptist Hospital, Aiseikai Yamashina Hospital, Shimizu Hospital, Rakusei Newtown Hospital, Daini Okamoto General Hospital, Kyoto Katsura Hospital, Saiseikai Kyoto Hospital, Nagaokakyo Hospital, Yamashiro Public Hospital, Fukuchiyama City Hospital, Maizuru Red Cross Hospital.
Nara. Hanna Central Hospital, Kura Hospital, Nara Prefectural Nara Hospital, Koseikai Takai Hospital, Tenri Hospital, Nara Medical University Hospital, Heisei Memorial Hospital, Mimuro Hospital, Nara Prefectural Gojo Hospital.
Wakayama. Wakayama Red Cross Medical Center, Wakayama Rosai Hospital, Wakayama Medical University Hospital, Wakayama National Hospital, Social Insurance Kinan Hospital, Naga Hospital.
Osaka. Sumitomo Hospital, Osaka Saiseikai Nakatsu Hospital, Osaka Kaisei Hospital, Kitaosaka Hospital, Iseikai Hospital, Yodogawa Christian Hospital, Sumire Hospital, Noe Hospital, Otemae Hospital, Osaka Red Cross Hospital, NTT Osaka Hospital, Ikuwakai Memorial Hospital, Imazato Gastroenteric Hospital, Ryokufukai Hospital, Osaka Seninhoken Hospital, Matsumoto Hospital, Kansai Denryoku Hospital, Osaka Koseinenkin Hospital, Osakakitashimin Hospital, Yamamoto Daisan Hospital, Osaka General Medical Center, Toyonaka Municipal Hospital, Senri Pain Clinic, Galacia Hospital, Minoh City Hospital, Saiseikai Suita Hospital, Suita Municipal Hospital, Osaka Medical College Hospital, Takatsuki Red Cross Hospital, Takatsuki General Hospital, Kansai Medical University Hospital, Sousei Hospital, Hoshigaoka Soseinenkin Hospital, Nozaki Tokusyukai Hospital, Katano Hospital, Kawachi General Hospital, Wakakusa Daiichi Hospital, Yao General Hospital, Fujiidera Municipal Hospital, Tondabayashi Saiseikai Hospital, Okakinen Hospital, Kinki University Hospital, Sakai Municipal Hospital, Nogami Hospital, Ueki Hospital, Osaka Rosai Hospital, NHO Kinki‐Chuo Chest Medical Center, Izumi Municipal Hospital, Kishiwada Tokusyukai Hospital, Kishiwada City Hospital, Kaizuka City Hospital, Aomatsu Hospital, Izumisano Yujinkai Hospital, Higashisano Hospital, Rinku General Medical Center, Bell land General Hospital, Hanwadaini Senhoku Hospital.
Hyogo. Kobe University Hospital, Kobe City Medical Center General Hospital, Kobe Rosai Hospital, Shinko Hospital, Shakaihoken Kobe Central Hospital, Saiseikai Hyogoken Hospital, Adachi Hospital, Kaisei Hospital, Midori Hospital, Nishikobe Medical Center, Mitsubishi Kobe Hospital, Kobe City Medical Center West Hospital, Nomura Kaihin Hospital, Hayashiyama Clinic, Rokko Hospital, Rokko Island Hospital, Higashi‐Kobe Hospital, Ashiya Municipal Hospital, Kansai Rosai Hospital, Okuma Hospital, Hyogo Prefectural Amagasaki Hospital, Ando Hospital, Okada Hospital, Hyogo Prefectural Tsukagoshi Hospital, Tachibana Hospital, Amagasaki Iryoseikyo Hospital, Itami City Hospital, Takarazuka City Hospital, The Veritas Hospital, Imai Hospital, Yoka Hospital, Hyogo‐chuo National Hospital, Hirashima Hospital, Otsuka Hospital, NHO Himeji Medical Center, Tsukazaki Memorial Hospital, Meimai Central Hospital, Akashi Medical Center, Nishieigashima Hospital, Kakogawa West City Hospital, Kasai City Hospital, Harima Hospital, Ako City Hospital.
Tottori. Tottori Municipal Hospital, Sanin Rosai Hospital.
Shimane. Matsue Seikyo General Hospital.
Okayama. Okayama Saiseikai General Hospital, Okayama Chuo Hokancho Hospital, Tanaka Clinic, Okayama University Hospital, Japanese Red Cross Okayama Hospital, Kawasaki Medical University Kawasaki Hospital, Shigei Medical Institution Hospital, Bizen City Hinase Hospital, Okayama Rosai Hospital, Fujita Hospital, Onishi Hospital, Tamano City Hospital, Yoshino Hospital, Tsuyama Chuo Hospital, Akaiwa City Kumayama Hospital, Satou Memorial Hospital, Asano Hospital, Shigei Hospital, Kurashiki Central Hospital, Kurashiki Medical Center, Kenju Kyodo Hospital, Kasaoka City Hospital, Sakumoto Clinic, Ochiai Hospital.
Hiroshima. Chugoku Central Hospital, NHO Fukuyama Medical Center, Kobatake Hospital, Fukuyama Daiichi Hospital, JA Onomichi General Hospital, Murakami Kinen Hospital, Onomichi Municipal Hospital, Mitsugi General Hospital, Innnoshima Ishikai Hospital, Innoshima General Hospital, Mihara Medical Associations Hospital, Miyoshi Medical Association Hospital, Miyoshi Central Hospital, Nishida Clinic, Hiroshima City Hospital, Hiroshima Red Cross Hospital & Atomic‐bomb Survivors Hospital, Yoshijima Hospital, Shimura Hospital, Funaki Hospital, Hiroshima City Asa Hospital, Yoshida General Hospital, Saiseikai Hiroshima Hospital, Hiroshima Park Hill Hospital, Hiroshima Prefectural Hospital, Hiroshima University Hospital, Aki City Hospital, NHO Kure Medical Center, Hakuai Clinic, Goto Hospital, Chugoku Rosai Hospital, Kure Kyosai Hospital, Kajikawa Clinic, JA Hiroshima General Hospital.
Yamaguchi. Hikari Municipal Hikari General Hospital, Hitachi Hospital, Shunan Memorial Hospital, Tokuyama Central Hospital, Hofu Gastroenteric Hospital, Hofu Onsen Hospital, Shimonoseki Kosei Hospital, Saiseikai Shimonoseki General Hospital, Yamaguchi Wakamiya Hospital, NHO Yamaguchi–Ube Medical Center, Yamaguchi Rosai Hospital, Shigeoka Hospital.
Kagawa. Kagawa Prefectural Central Hospital, Yashima General Hospital, Kagawa University Hospital, Takinomiya General Hospital, Kagawa Rosai Hospital, Miyano Hospital, Asada General Hospital, NHO Zentsuji National Hospital.
Tokushima. Tokushima Prefectural Central Hospital, Kondo Hospital, Kondo Clinic, Fujino Clinic.
Kochi. Kochi Health Sciences Center, Kochi Seikyo Hospital, NHO Kochi National Hospital, JA Kochi Hospital, Kochi Medical School Hospital, Kouhoku Hospital.
Ehime. Ehime Prefectural Central Hospital, Matsuyama Shimin Hospital, Matsuyama Red Cross Hospital, NHO Ehime National Hospital, NHO Shikoku Cancer Center, Uchiyama Hospital, Jyuzen General Hospital, Sumitomo Besshi Hospital, Ehime Rosai Hospital, Saijo Central Hospital, Manabe Hospital, Ehime Prefectural Imabari Hospital.
Fukuoka. Moji Hospital, Kyusyu Rosai Hospital, Obase Hospital, Ekiseikai Moji Hospital, Moji Rosai Hospital, Shin‐Kokura Hospital, Saiseikai Yahata General Hospital, Kitakyusyu Yahata Higashi Hospital, Kyusyu Kosei Nekin Hospital, Fukuoka Shin Mizumaki Hospital, Aobadai Hospital, Shinnakama Hospital, Akimoto Hospital, NHO Kyusyu Medical Center, Hamanomachi Hospital, Nagano Clinic, Eikoh Hospital, Fukuoka Seisyukai Hospital, NHO Fukuoka Higashi Medical Center, Togo Clinic, Chidoribashi Hospital, Fukuoka City Hospital, Yagi Hospital, Kyusyu University Hospital, Fukuoka University Hospital, Muta Hospital, Fukuseikai Hospital, Fukuoka Tokusyukai Medical Center, Hakujuji Hospital, Murakami Karindou Hospital, IIzuka Hospital, Nogata Chuo Hospital, Social Insurance Tagawa Hospital, Shinkoga Hospital, St. Mary’s Hospital, Yame General Hospital, Koga Hospital 21.
Saga. NHO Ureshino Medical Center, Karatsu Red Cross Hospital, Saga University Hospital, Oda Hospital, Omachi Town Hospital, Arita Kyoritsu Hospital.
Nagasaki. Iki Hospital, Saiseikai Nagasaki Hospital, Nagasaki Municipal Hospital, Uetomachi Hospital, Wajinkai Hospital, Nagasaki Memorial Hospital, Nagasaki Municipal Medical Center, Nijigaoka Hospital, Nagasaki University Hospital, St. Francis Hospital, Isahaya Health Insurance General Hospital, Omura City Municipal Hospital, Sasebo City General Hospital, Nagasaki Rosai Hospital, Sasebo Kyosai Hospital, Sasebo Chuo Hospital, Kurihara Clinic, Akagaki Naikajunkankika Clinic, NHO Nagasaki Kawatana Medical Center, Sekisyukai Hospital.
Kumamoto. Tajima Clinic, Otsuka Hospital, Yamaga Chuo Hospital, Japanese Red Cross Kumamoto Hospital, Kumamoto Chuo Hospital, Konan Hospital, Amakusa Daiichi Hospital, Amakusa Area Medical Center, Tamana Central Hospital, Kumamoto Rosai Hospital, Minamata City General Hospital and Medical Center, Taragi Hospital, Saiseikai Misumi Hospital.
Oita. Oita Cardiovascular Hospital, Oita Oka Hospital, Oita Prefectural Hospital, Usuki Cosmos Hospital, Tomachidai Surgical Hospital, Saiki Central Hospital, Nankai Hospital.
Miyazaki. Miyazaki Seikyo Hospital, Hinokage Kokuminkenkohoken Hospital, Miyazaki Prefectural Nobeoka Hospital, Nobeoka Medical Association Hospital.
Kagoshima. Yoshida Onsen Hospital, Imakiire General Hospital, Ogura Kinen Hospital, Oshima Hospital, Southern Region Hospital, Akune Citizen Hospital, Honjo Hospital, Ariake Hospital.
Okinawa. NHO Okinawa National Hospital, Adventist Medical Center, Hokubu Hospital, Okinawa Miyako Hospital.
References
- 1. Ismail‐Khan R, Robinson LA, Williams CC Jr, Garrett CR, Bepler G, Simon GR. Malignant pleural mesothelioma: a comprehensive review. Cancer Control 2006; 13: 255–63. [DOI] [PubMed] [Google Scholar]
- 2. Ohshima H. Five cases with mesothelioma living near a now‐defunct asbestos cement plant in Amagasaki city. Osaka: Mainichi Newspaper, 2005, p.1. (in Japanese) [Google Scholar]
- 3. Kishimoto T, Gemba K, Fujimoto N et al. Clinical study on mesothelioma in Japan: relevance to occupational asbestos exposure. Am J Ind Med 2010; 53: 1081–7. [DOI] [PubMed] [Google Scholar]
- 4. Churg A, Inai K, Samet J. Tumours of the Pleura. Lyon: IARC Press, 2004. [Google Scholar]
- 5. Rusch VW. A proposed new international TNM staging system for malignant pleural mesothelioma. From the International Mesothelioma Interest Group. Chest 1995; 108: 1122–8. [DOI] [PubMed] [Google Scholar]
- 6. Kohyama N, Suzuki Y. Analysis of asbestos fibers in lung parenchyma, pleural plaques, and mesothelioma tissues of North American insulation workers. Ann N Y Acad Sci 1991; 643: 27–52. [DOI] [PubMed] [Google Scholar]
- 7. Walters J, Maskell NA. Biopsy techniques for the diagnosis of mesothelioma. Recent Results Cancer Res 2011; 189: 45–55. [DOI] [PubMed] [Google Scholar]
- 8. Yates DH, Corrin B, Stidolph PN, Browne K. Malignant mesothelioma in south east England: clinicopathological experience of 272 cases. Thorax 1997; 52: 507–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Magnani C, Agudo A, Gonzalez CA et al. Multicentric study on malignant pleural mesothelioma and non‐occupational exposure to asbestos. Br J Cancer 2000; 83: 104–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Newhouse ML, Thompson H. Mesothelioma of pleura and peritoneum following exposure to asbestos in the London area. Br J Ind Med 1965; 22: 261–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rees D, Goodman K, Fourie E et al. Asbestos exposure and mesothelioma in South Africa. S Afr Med J 1999; 89: 627–34. [PubMed] [Google Scholar]
- 12. Kishimoto T, Ozaki S, Kato K, Nishi H, Genba K. Malignant pleural mesothelioma in parts of Japan in relationship to asbestos exposure. Ind Health 2004; 42: 435–9. [DOI] [PubMed] [Google Scholar]
- 13. Fujimoto N, Aoe K, Gemba K, Kato K, Yamazaki K, Kishimoto T. Clinical investigation of malignant mesothelioma in Japan. J Cancer Res Clin Oncol 2010; 136: 1755–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Asbestos, asbestosis, and cancer: the Helsinki criteria for diagnosis and attribution (Consensus Report). Scand J Work Environ Health 1997; 23: 311–6. [PubMed] [Google Scholar]