

Abstract
Background
Vocal cord paralysis (VCP) is one of the most stressful experiences for patients undergoing general anesthesia. Moreover, it is a risk factor for aspiration pneumonia and may increase morbidity and mortality. We examined several clinical features of the condition by reviewing the medical records of patients who experienced VCP following general anesthesia.
Methods
We reviewed the medical records of 321 patients who consulted an otolaryngologist owing to hoarseness, sore throat, throat discomfort, or dysphagia after general anesthesia. Among these, we included in the present study 43 patients who were diagnosed with VCP by laryngoscopy, who did not have symptoms of suspected VCP before surgery, who had no past history of VCP, and for whom endotracheal intubation was not continued after surgery.
Results
The mean age of patients with VCP was 51.3 years. With respect to surgical site, the most common was upper limb surgery, performed in 12 cases (9 cases were performed in sitting posture. With respect to surgical duration, only 11 cases lasted less than 3 h, whereas 32 cases required a surgical duration longer than 3 h. The most common symptom of VCP was hoarseness. Nine of the patients with VCP recovered spontaneously, but VCP persisted in 13 cases until the final follow-up examination.
Conclusions
We hope that this study might call attention to the occurrence of VCP following general anesthesia. Moreover, it is necessary to further evaluate the reasons for the higher incidence of VCP in upper limb surgery performed in sitting posture.
Keywords: Endotracheal intubation, General anesthesia, Vocal cord paralysis
INTRODUCTION
Although vocal cord paralysis (VCP) is a rare complication associated with endotracheal intubation during surgery [1–3], it could be a stressful experience for patients following anesthesia [4,5]. Moreover, it is a risk factor for aspiration pneumonia and could increase morbidity and mortality [6–8].
VCP may be caused by neurogenic injury or by limitation of vocal cord movement. Neurogenic injuries are usually caused by damage to the vagal or recurrent laryngeal nerve resulting from surgery or neoplastic infiltration [5,9,10]. During surgery, the cuff pressure of the endotracheal tube may be related to nerve paralysis and neuropraxia [11]. Mechanical fixation of the vocal cords might result from arytenoid dislocation, edema or inflammation of the glottis, or neoplastic invasion [12–14]. The most common cause of postoperative VCP is iatrogenic recurrent laryngeal nerve injury following thyroid surgery [15]. Carotid endarterectomy for stenosis of the carotid artery, anterior cervical spine decompression, open-heart surgery, and thoracic surgery have also been revealed to cause postoperative VCP [5,8,13]. The most common cause of VCP in the absence of iatrogenic nerve injury is mechanical damage from endotracheal intubation [12,14]. Mechanical laryngeal injuries such as dislocation and subluxation of the cricothyroid or cricoarytenoid joints can occur after endotracheal intubation. In addition, if the endotracheal tube is placed in an improper position and maintained for an extended period, damage and dislocation of arytenoid cartilage and cricothyroid cartilage may result [16–18]. It is also known that ischemic nerve damage of the laryngeal nerve and vocal cords may be a cause of postoperative VCP owing to prolonged endotracheal tube placement [8].
In the present study, we analyzed 43 cases of VCP following general anesthesia that occurred in our hospital over a period of 10 years to investigate the clinical features (symptoms, progress, and prognosis) of VCP.
MATERIALS AND METHODS
We reviewed the medical record of 321 patients who consulted an otolaryngologist owing to sore throat, throat discomfort, difficulty in swallowing, or voice change following general anesthesia from January 2007 to October 2016. Among these, 43 patients were diagnosed with postoperative VCP and included in the current study. The inclusion criteria were as follows: (1) Patients diagnosed with VCP (partial or complete, unilateral or bilateral) by laryngoscopy (Fig. 1); (2) Patients who did not have symptoms of suspected VCP before surgery; (3) Patients without a past history of VCP prior to the surgery; (4) Patients in whom endotracheal intubation or ventilatory care was not maintained after surgery (for this reason, patients who underwent open-heart surgery were excluded from the current study). The analyzed factors were the following: otolaryngological medical factors (symptoms, time to receive consultation, and time to recovery); patient profiles (age, sex, height, weight, body mass index, and comorbidities); surgical factors (type of surgery, duration of surgery, surgical posture and whether the posture changed during the operation); and anesthetic factors (Cormack-Lehane grade, size of endotracheal tube, type of endotracheal tube, and whether nitrous oxide gas was used for anesthesia).
Fig. 1.
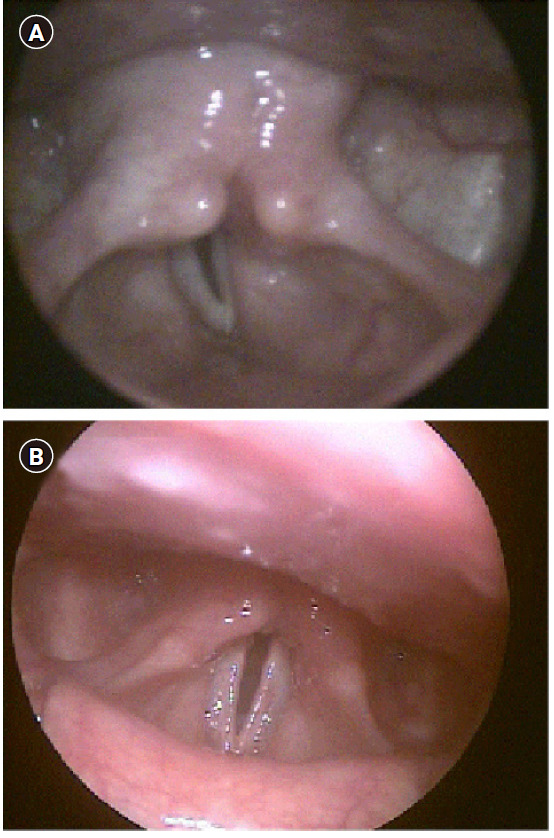
Laryngoscopic views of vocal cord paralysis (VCP). (A) Unilateral (right) VCP, (B) bilateral VCP. Above pictures are of VCP patients who occurred at our hospital.
This study protocol was reviewed and approved by the institutional review board of our hospital (no. 16-0249) and the protocol was registered at the clinical research information service (http://cris.nih.go.kr, no. KCT0002717).
RESULTS
Table 1 shows basic patient data. The number of surgeries performed from January 2007 to October 2016 was 100,921. Following surgery, 321 patients were referred to an otolaryngologist. Among these 321 patients, 43 were diagnosed with VCP. Among the 43 patients, unilateral VCP occurred in 40 (22 patients [55%] with left VCP and 18 patients [45%] with right VCP), and bilateral VCP occurred in 3 patients. All patients with bilateral VCP underwent total thyroidectomy with lymph node dissection, and one underwent nasotracheal intubation owing to difficulty in breathing 1 day after surgery.
Table 1.
Basic Data of Patients
| Variable | VCP (n = 43) |
|---|---|
| Age (yr) | 51.28 ± 14.90 |
| 20s | 3 (6.98) |
| 30s | 7 (16.28) |
| 40s | 6 (13.96) |
| 50s | 13 (30.23) |
| 60s | 10 (23.26) |
| 70s | 4 (9.30) |
| Gender | |
| Female | 18 (41.86) |
| Male | 25 (58.14) |
| Weight (kg) | 64.56 ± 12.68 |
| Height (cm) | 166.29 ± 9.04 |
| BMI (kg/m2) | 23.38 ± 3.30 |
| BMI < 18.5 | 2 (4.65) |
| 18.5 ≤ BMI < 23 | 18 (41.86) |
| 23 ≤ BMI < 25 | 10 (23.26) |
| 25 ≤ BMI < 30 | 10 (23.26) |
| 30 ≤ BMI < 40 | 1 (2.33) |
| Unmeasured | 2 (4.65) |
| Comorbidity | |
| Hypertension | 5 (11.63) |
| Diabetes mellitus | 6 (13.96) |
| CVA | 0 (0) |
| Cardiovascular | 1 (2.33) |
Values are presented as mean ± SD or number (%). VCP: vocal cord paralysis, BMI: body mass index (kg/m2), Classification of BMI according to Korean Society for the Study of Obesity; Underweight: BMI < 18.5, Normal: 18.5 ≤ BMI < 23, Overweight: 23 ≤ BMI < 25, Mild obesity: 25 ≤ BMI < 30, Severe obesity: 30 ≤ BMI < 40, Unmeasured: two patients were missing weight data, Comorbidity: patient accompanying the disease, CVA: cerebrovascular accident, Cardiovascular: cardiovascular disease.
The types of surgery and characteristics of VCP are shown in Table 2. The most common type of surgery preceding VCP was upper limb surgery including the clavicle (n = 12, 27.91%). The next most common types of surgery were cervical spine surgery (n = 8, 18.60%) and abdominal surgery (n = 8, 18.60%). Thoracic surgery (n = 6, 13.95%) and thyroid surgery (n = 5, 11.63%) were next in frequency. Table 3 depicts the most common positions of patients during surgery. Nine of the 10 patients who underwent surgery in sitting position received orthopedic upper limb surgery and 1 underwent laparoscopic cholecystectomy.
Table 2.
The Types of Surgery and Characteristics of VCP
| Surgery | Unilateral (n = 40) |
Bilateral (n = 3) | |
|---|---|---|---|
| Right (n = 18) | Left (n = 22) | ||
| Brain | 1 | 3 | |
| Neck | |||
| Cervical spine (anterior approach) | 6 | 2 | |
| Total thyroidectomy | 1 | 3 | |
| Right parathyroidectomy | 1 | ||
| Thorax | |||
| Esophageal cancer | 1 | ||
| Right Mediastinal mass | 1 | ||
| Left Mediastinal mass | 1 | ||
| Left pneumothorax | 1 | ||
| Left pneumonectomy | 1 | ||
| Thoracic spine (posterior approach) | 1 | ||
| Upper limbs | |||
| Right clavicle | 3 | ||
| Left clavicle | 1 | ||
| Right upper arm | 3 | ||
| Left upper arm | 3 | 1 | |
| Right lower arm | 1 | ||
| Abdomen | |||
| Laparoscopic surgery | 1 | ||
| Open surgery | 4 | 3 | |
Values are presented as number. VCP: vocal cord paralysis, Unilateral: one-sided VCP, Bilateral: both sides VCP, Right: right sided VCP, Left: left sided VCP.
Table 3.
Main Position during Surgery and Characteristics of VCP
| Position | Unilateral (n = 40) | Bilateral (n = 3) | |
|---|---|---|---|
| Right (n = 18) | Left (n = 22) | ||
| Supine | 11 | 8 | 3 |
| Prone | 1 | ||
| Right lateral | 2 | 3 | |
| Left lateral | 2 | 1 | |
| Sitting | 2 | 8 | |
| Trandelenburg | 1 | 1 | |
Values are presented as number. VCP: vocal cord paralysis, Position: the main posture during the operation, Supine: including supine with lithotomy, Sitting: including reverse trandelenburg.
The surgical procedures varied in duration from 65 min to 11 h (Fig. 2). VCP occurred in 11 patients (25.58%) whose operation time was less than 3 h, in 22 patients (51.16%) whose operation time was between 3 h and 6 h, and in 10 patients (23.26%) whose operation time was 6 h or more.
Fig. 2.
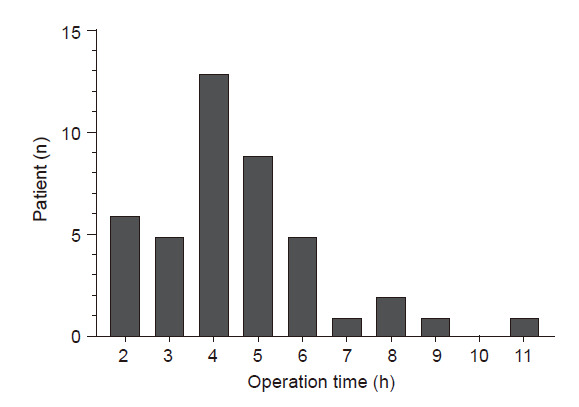
Distribution of vocal cord paralysis patients by operation time. Operation time: length of operation, “operation time = n” means that length of operation is ‘n – 1’ h or more and less than ‘n’ (e.g., 3: 2 h ≤ operation time < 3 h).
The number of patients with Cormack-Lehane grade 3 was 5. In two of these patients, we failed to perform intubation with a laryngoscope blade and reattempted the intubation using a fiberoptic bronchoscope. The types and sizes of endotracheal tubes and usage of nitrous oxide gas are shown in Table 4.
Table 4.
Distribution of VCP Patients by Factors associated with Anesthesia
| Factor | VCP (n = 43) | |
|---|---|---|
| Type of ETT | ||
| SLT | 38 (88.37) | |
| DLT | 5 (11.63) | |
| Size of ETT | ||
| DLT 37 fr | 4 (9.30) | |
| DLT 35 fr | 1 (2.33) | |
| SLT ID 7.5 mm | 19 (44.19) | |
| SLT ID 7.0 mm | 13 (30.23) | |
| SLT ID 6.5 mm | 1 (2.33) | |
| Cormack grade | ||
| 1 | 23 (53.49) | |
| 2 | 5 (11.63) | |
| 3 | 5 (11.63) | |
| 4 | 0 (0) | |
| Nitro | ||
| Yes | 21 (48.84) | |
| No | 22 (51.16) |
Values are presented as number (%). VCP: patient diagnosed with vocal cord paralysis, Type of ETT: types of endotracheal tubes used for intubation, SLT: single lumen cuffed endotracheal tube, DLT: double lumen endotracheal tube, Size of ETT: size of endotracheal tube used for intubation, ID: Inner diameter, Cormack grade: Cormack-Lehane grade, 10 patients were missing Cormack-Lehane grade data, Nitro: whether nitro oxide gas was used during general anesthesia.
The most frequent symptom of patients with VCP was hoarseness (Fig. 3). The number of patients who reported only sore throat, throat discomfort, or dyspnea without any other symptoms were 6, 2, and 1, respectively. The average time required for patients to see an otolaryngologist after surgery was 13 days.
Fig. 3.
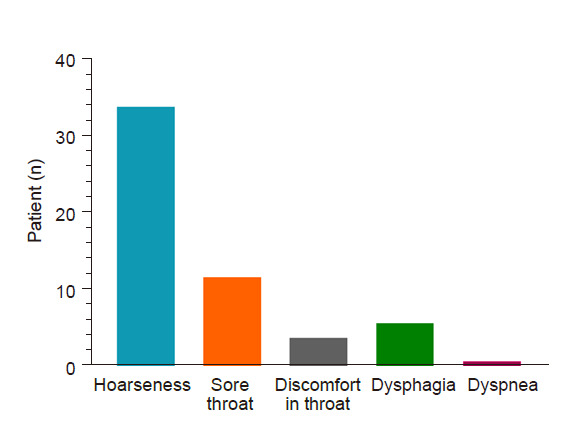
Symptoms complained by vocal cord paralysis patients. The complaining symptoms were counted in duplicate.
The course of VCP is shown in Fig. 4. Fifteen patients were lost to follow-up after a single visit to the Otolaryngology Department. Nine patients recovered spontaneously (with laryngoscopic confirmation of recovery from VCP), but 3 experienced continuing symptoms of voice change. The time to recover from VCP varied from between 20 to 113 days (average: 58 days). Six patients received vocal cord injection therapy, but 2 of these continued to report symptoms after treatment. Thirteen patients continued to experience VCP until the last laryngoscopic examination (the longest period from occurrence of VCP to the last exam was 449 days), while symptoms improved within 2–6 months in 4 of the patients. Additionally, one patient continued to report symptoms (voice change and throat discomfort) for more than 3 years, regardless of recovery from VCP.
Fig. 4.
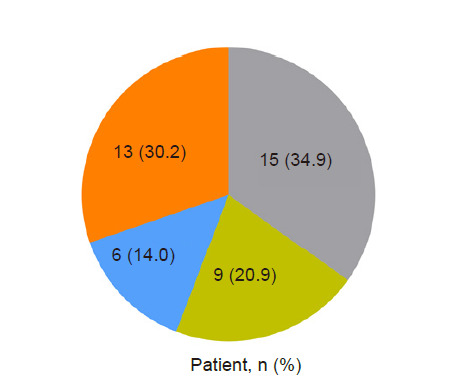
Distribution of vocal cord paralysis (VCP) patients by prognosis and progress. Grey: patients who did not have follow-up observation after seeing otolaryngology examination only once, Green: patients recovered spontaneously, Blue: patients had treatment with vocal cord injection, Orange: patients had VCP until the last laryngoscopic examination.
DISCUSSION
In this study, among 100,941 cases of general anesthesia, 43 patients experienced postoperative VCP (the incidence was 0.043%). Risk factors for VCP included long operation time, sitting posture during surgery, and whether the posture changed during surgery.
A previous study by Kikura et al. [8], which investigated risk factors for VCP with endotracheal intubation, reported that the incidence of VCP following general anesthesia was 0.077%. In their study, patients undergoing brain surgery, thyroid surgery, carotid endarterectomy, panendoscopy, laryngeal or pharyngeal surgery, anterior cervical surgery, thoracic surgery, or cardiac surgery were excluded to rule out iatrogenic VCP. In our study, however, we did not exclude types of surgery in which the vocal cords could be susceptible to iatrogenic damage. Moreover, we reviewed only the charts of patients who reported symptoms such as hoarseness, pain or discomfort in the throat, dysphagia, or dyspnea following surgery. Thus, asymptomatic patients with VCP may have been excluded in the present study.
There are several known risk factors for VCP associated with endotracheal intubation. Gupta et al. [19] reported that the incidence of VCP increased with age and peaked in the fifth decade. Kikura et al. [8] reported that patient comorbidities (arterial hypertension, diabetes mellitus) and the duration of intubation, as well as age, were risk factors for VCP associated with endotracheal intubation. The authors reported that the risk of VCP increased three-fold in patients aged 50 or older, increased two-fold in patients with diabetes mellitus and hypertension, and also increased with duration of intubation (the risk doubled in patients with an intubation duration of more than 3 h and less than 6 h). The results of our study show a similar tendency. While VCP occurred in 27 patients (62.79%) more than 50 years old, it occurred in only 16 patients (37.21%) less than 50 years old. Moreover, VCP occurred in only 11 patients (25.58%) whose operation time was less than 3 h, whereas it occurred in 32 patients (74.42%) with operations lasting longer than 3 h.
The most common surgery associated with iatrogenic VCP is thyroid surgery. It is also known that iatrogenic VCP also occurs in head and neck surgery, thoracic surgery, cervical spine surgery, and open-heart surgery [5,8,13]. However, in our study, the most common surgery associated with VCP was upper limb surgery including the clavicle (12/43 patients, 27.91%). While upper limb surgery including the clavicle constituted 27.91% of all VCP cases in the present study, the proportion occupied by thyroid and parathyroid surgery was only 11.63% (5/43 patients). This finding seems to be the result of the decrease in iatrogenic nerve injury owing to developments in surgical techniques and nerve monitoring devices in thyroid surgery. In the above 5 patients, no device for monitoring laryngeal nerve damage was used, but in 4 patients the symptoms resolved spontaneously, and one patients was lost to follow-up without further evaluation. However, in the course of upper limb surgery, it is likely that the hyperextension of neck to obtain a better surgical view, as well as surgical manipulation such as pressing and pulling, resulted in more severe vocal cord damage. Moreover, most of the upper limb surgeries were performed in a sitting position. We expect that a sudden migration of the endotracheal tube followed by posture change caused damage to the vocal cords. In addition, Kikura et al. [8] hypothesized that ischemic neuronal damage to the recurrent laryngeal nerve and its peripheral branches in the larynx can be caused by a decrease in microcirculatory supply owing to cuff pressure. In upper limb surgery with posture change, the cuff may move to a place vulnerable to these injuries and cause VCP.
VCP with nerve injury has a low rate of spontaneous recovery, while idiopathic VCP without nerve injury has a spontaneously recovery rate from 13% to 85%. Most patients with idiopathic VCP spontaneously recover within one year. However, the cure rate of patients experiencing idiopathic VCP longer than one year is very low [20,21]. In our study, spontaneous recovery was observed in 20.93% (9/43) of patients with VCP following general anesthesia. The recovery time was about two months on average. Havas et al. [20] recommend early surgical treatment or re-innervation if aspiration or other symptoms are present or the possibility of nerve injury is high. Therefore, it is important to identify the exact cause and etiology of the VCP [20–22]. Radiological examination such as X-rays, and computed tomography with and/or without contrast, and laryngeal electromyography can be helpful to establish the prognosis of VCP [23,24].
There are potential limitations in our study.
First, because the incidence of postoperative VCP itself is very low, despite a review of the medical records of the past 10 years, we identified only 43 patients diagnosed with postoperative VCP in our hospital.
Secondly, during the time period covered in the present study, the medical records of patients diagnosed with VCP following general anesthesia frequently lacked details regarding the course of the VCP. Of the 43 patients with VCP identified in the present study, 15 saw an otolaryngologist only once and were subsequently lost to follow-up. In these cases, detailed evaluation of VCP was not performed. Moreover, only the laryngoscopic findings were described in the otolaryngology medical records, and this information was not sufficient to allow description of the degree of hoarseness and whether vocalization was possible, or physical findings such as the area of paralyzed vocal cord or the existence of paralyzed vocal cord atrophy, and whether there was dislocation of the arytenoid cartilage of the paralyzed vocal cord. Also, as mentioned above, radiological examination such as X-rays, computed tomography with and/or without contrast, and laryngeal electromyography should be performed to identify the exact cause of VCP [23,24]. In most cases, however, no further examination was performed and only symptomatic treatment was performed.
Thirdly, as we reviewed charts of patients who received an otolaryngology consultation for symptoms such as hoarseness after surgery, cases of asymptomatic VCP were not included. However, according to Jung et al. [25], the incidence of asymptomatic VCP was reported to be twice the incidence of symptomatic VCP (8.3%), and we were unable to investigate these asymptomatic cases.
Fourthly, the exclusion criteria for this study included patients in whom endotracheal intubation was maintained after surgery. Previous studies have shown that the risk of VCP is high in patients undergoing open-heart surgery [6,26]. However, we excluded patients who were maintained on ventilator care, so patients who developed VCP following open-heart surgery were not investigated.
Finally, since our study performed only clinical review of VCP through analysis of 43 cases, we did not investigate the exact incidence according to the type of surgery through a complete enumeration survey, and failed to identify risk factors associated with type of surgery. Nevertheless, our discovery that a large proportion of cases of VCP occurred during a particular type of surgery (upper limb surgery) is meaningful. We believe that care should be taken to locate the endotracheal tube properly and maintain circulation in patients undergoing surgery under these conditions.
Particularly based on the results of this study, it is necessary to further explore the reasons for the higher incidence of VCP in upper limb surgery performed in sitting posture. Furthermore, we hope that the present study may provide greater awareness to anesthesiologists regarding VCP and the significant discomfort and danger it can cause in patients.
Footnotes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Seunghee Ki, Sehun Lim. Data acquisition: Kwangrae Cho, Myoung-hun Kim, Dong-chun Kim. Formal analysis: Sungho Moon, Seunghee Ki. Supervision: Sehun Lim. Writing-original draft: Hakmoo Cho, Dong-chun Kim. Writing-review&editing: Seunghee Ki.
REFERENCES
- 1.David DS, Shah M. Vocal cord paralysis following intubation. JAMA. 1971;216:1645–6. doi: 10.1001/jama.1971.03180360091022. [DOI] [PubMed] [Google Scholar]
- 2.Domino KB, Posner KL, Caplan RA, Cheney FW. Airway injury during anesthesia: a closed claims analysis. Anesthesiology. 1999;91:1703–11. doi: 10.1097/00000542-199912000-00023. [DOI] [PubMed] [Google Scholar]
- 3.Holley HS, Gildea JE. Vocal cord paralysis after tracheal intubation. JAMA. 1971;215:281–4. [PubMed] [Google Scholar]
- 4.Flint P, Haughey B, Lund V, Niparko J, Robbins K, Thomas JR, et al. Cummings otolaryngology: head and neck surgery. 6th ed. Philadelphia: Elsevier; 2015. [Google Scholar]
- 5.Takano S, Nito T, Tamaruya N, Kimura M, Tayama N. Single institutional analysis of trends over 45 years in etiology of vocal fold paralysis. Auris Nasus Larynx. 2012;39:597–600. doi: 10.1016/j.anl.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 6.Hamdan AL, Moukarbel RV, Farhat F, Obeid M. Vocal cord paralysis after open-heart surgery. Eur J Cardiothorac Surg. 2002;21:671–4. doi: 10.1016/s1010-7940(02)00019-2. [DOI] [PubMed] [Google Scholar]
- 7.Hulscher JB, van Sandick JW, Devriese PP, van Lanschot JJ, Obertop H. Vocal cord paralysis after subtotal oesophagectomy. Br J Surg. 1999;86:1583–7. doi: 10.1046/j.1365-2168.1999.01333.x. [DOI] [PubMed] [Google Scholar]
- 8.Kikura M, Suzuki K, Itagaki T, Takada T, Sato S. Age and comorbidity as risk factors for vocal cord paralysis associated with tracheal intubation. Br J Anaesth. 2007;98:524–30. doi: 10.1093/bja/aem005. [DOI] [PubMed] [Google Scholar]
- 9.Feierabend RH, Shahram MN. Hoarseness in adults. Am Fam Physician. 2009;80:363–70. [PubMed] [Google Scholar]
- 10.Mau T. Diagnostic evaluation and management of hoarseness. Med Clin North Am. 2010;94:945–60. doi: 10.1016/j.mcna.2010.05.010. [DOI] [PubMed] [Google Scholar]
- 11.Tasar A, Yanturali S, Topacoglu H, Ersoy G, Unverir P, Sarikaya S. Clinical efficacy of dexamethasone for acute exudative pharyngitis. J Emerg Med. 2008;35:363–7. doi: 10.1016/j.jemermed.2007.11.029. [DOI] [PubMed] [Google Scholar]
- 12.Quick CA, Merwin GE. Arytenoid dislocation. Arch Otolaryngol. 1978;104:267–70. doi: 10.1001/archotol.1978.00790050033007. [DOI] [PubMed] [Google Scholar]
- 13.Rosenthal LH, Benninger MS, Deeb RH. Vocal fold immobility: a longitudinal analysis of etiology over 20 years. Laryngoscope. 2007;117:1864–70. doi: 10.1097/MLG.0b013e3180de4d49. [DOI] [PubMed] [Google Scholar]
- 14.Rudert H. [Uncommon injuries of the larynx following intubation. Recurrent paralysis, torsion and luxation of the cricoarytenoid joints] HNO. 1984;32:393–8. German. [PubMed] [Google Scholar]
- 15.Younes N, Robinson B, Delbridge L. The aetiology, investigation and management of surgical disorders of the thyroid gland. Aust N Z J Surg. 1996;66:481–90. doi: 10.1111/j.1445-2197.1996.tb00787.x. [DOI] [PubMed] [Google Scholar]
- 16.Colton House J, Noordzij JP, Murgia B, Langmore S. Laryngeal injury from prolonged intubation: a prospective analysis of contributing factors. Laryngoscope. 2011;121:596–600. doi: 10.1002/lary.21403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Santos PM, Afrassiabi A, Weymuller EA., Jr Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngol Head Neck Surg. 1994;111:453–9. doi: 10.1177/019459989411100411. [DOI] [PubMed] [Google Scholar]
- 18.Weymuller EA., Jr Laryngeal injury from prolonged endotracheal intubation. Laryngoscope. 1988;98(8 Pt 2 Suppl 45):1–15. doi: 10.1288/00005537-198808001-00001. [DOI] [PubMed] [Google Scholar]
- 19.Gupta J, Varshney S, Bist SS, Bhagat S. Clinico-etiolological study of vocal cord paralysis. Indian J Otolaryngol Head Neck Surg. 2013;65:16–9. doi: 10.1007/s12070-012-0574-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Havas T, Lowinger D, Priestley J. Unilateral vocal fold paralysis: causes, options and outcomes. Aust N Z J Surg. 1999;69:509–13. doi: 10.1046/j.1440-1622.1999.01613.x. [DOI] [PubMed] [Google Scholar]
- 21.Sulica L. The natural history of idiopathic unilateral vocal fold paralysis: evidence and problems. Laryngoscope. 2008;118:1303–7. doi: 10.1097/MLG.0b013e31816f27ee. [DOI] [PubMed] [Google Scholar]
- 22.Woodson GE, Miller RH. The timing of surgical intervention in vocal cord paralysis. Otolaryngol Head Neck Surg. 1981;89:264–7. doi: 10.1177/019459988108900223. [DOI] [PubMed] [Google Scholar]
- 23.Hoffman HT, McCulloch TM. Anatomic considerations in the surgical treatment of unilateral laryngeal paralysis. Head Neck. 1996;18:174–87. doi: 10.1002/(SICI)1097-0347(199603/04)18:2<174::AID-HED10>3.0.CO;2-F. [DOI] [PubMed] [Google Scholar]
- 24.Yin SS, Qiu WW, Stucker FJ. Major patterns of laryngeal electromyography and their clinical application. Laryngoscope. 1997;107:126–36. doi: 10.1097/00005537-199701000-00024. [DOI] [PubMed] [Google Scholar]
- 25.Jung A, Schramm J, Lehnerdt K, Herberhold C. Recurrent laryngeal nerve palsy during anterior cervical spine surgery: a prospective study. J Neurosurg Spine. 2005;2:123–7. doi: 10.3171/spi.2005.2.2.0123. [DOI] [PubMed] [Google Scholar]
- 26.Hahn FW, Jr, Martin JT, Lillie JC. Vocal-cord paralysis with endotracheal intubation. Arch Otolaryngol. 1970;92:226–9. doi: 10.1001/archotol.1970.04310030016005. [DOI] [PubMed] [Google Scholar]