

Abstract
Objectives:
This prospective, observational, non-randomized multicentric study was conducted to compare efficiency and toxicity using different modalities of stereotactic body radiation therapy (SBRT) in early-stage peripheral non-small cell lung cancer (NSCLC).
Methods:
From 9 April to 11 December, 106 patients were treated according to the local equipment availability for peripheral NSCLC with SBRT: 68 by linear accelerator equipped for SBRT and 38 by Cyberknife®. Multivariate analysis and propensity score analysis using Inverse Probability Treatment Weighting (IPTW) were undertaken in an effort to adjust for potential bias due to non-randomization.
Results:
2-year local control rates were 97.0% (95% CI: [90.6%; 99.4%]) with SBRT by Linac vs 100% (95% CI: ([100%; 100%]) with Cyberknife® (p = 0.2839). 2-year PFS and 2-year OS rates were 52.7% (95% CI [39.9%;64.0%]) versus 54.1% (95% CI [36.8; 68.6%]) (p = 0.8582) and 65.1% (95% CI: [51.9%; 75.5%] versus 83.9% (95% CI: [67.5%; 92.4%] (p = 0.0831) using Linac and Cyberknife® respectively. Multivariate regression analysis indicates no significant effect of SBRT treatment type on PFS or OS. Local relapse could not be modeled due to the small number of events (n = 2). Acute and late toxicity rates were not significantly different. After IPTW adjustment, results were unchanged.
Conclusions:
No difference in efficiency or toxicity was shown after SBRT of peripheral NSCLC treatment using Linac or Cyberknife®.
Advances in knowledge:
This is the first large prospective non-randomized study focusing on peripheral localized NSCLC comparing SBRT using an appropriately equipped linac with Cyberknife®. No significant difference in efficiency or toxicity was shown in this situation.
Introduction
Stereotactic body radiation therapy (SBRT) is recognized as a standard-of-care treatment for inoperable patients with early peripheral stage non-small cell lung cancer (NSCLC). SBRT provides excellent local control up to 90% at 3 years with small rates of acute and late toxicity.1–4 SBRT can be delivered using either a conventional non-robotic linear-accelerator (Linac) equipped for SBRT or dedicated equipment such as the Cyberknife® (Accuray, Sunnyvale, CA). No randomized study has been published to compare these two approaches. Randomization between these technologies is not in practice feasible as the availability of equipment differs by institution and most institutions do not have both type of equipment. However, the study question remains interesting and relevant as many radiation departments are embarking on an SBRT program and have to choose between a conventional linear-accelerator equipped for SBRT or dedicated equipment. Data on prospective evaluations comparing both approaches in term of medical results are thus awaited. This study was conducted to evaluate and prospectively compare both efficiency and toxicity using two different modalities of SBRT in early-stage peripheral NSCLC in a large French multi-centric national study.
Methods and material
Study population
Patients >18 years, with a good WHO performance status (≤2), diagnosed with a non-metastatic peripheral NSCLC (T1 or T2), larger dimension <5 cm, without any node involvement on CT-scan and PET scan (N0) were eligible. Peripheral tumors were defined as further than 15 mm from large vessels, spinal cord and main bronchus. NSCLC was proven as often as possible. Non-proven lesions were eligible providing the following strict criteria were met: size progression on two successive scans, positive PET scan, negative bronchoscopy in term of bacteriology, and contra-indication for trans-thoracic biopsy assessed by a radiologist. A written multidisciplinary staff report was required to approve the exclusive SBRT treatment option. Surgery was not possible due to comorbidities or patient refusal. Patients with previously operated tumors, previous thoracic irradiation, previous or concurrent primary malignancies (except basocellular skin cancer or cervical cancer in situ or complete remission for more than 5 years), pregnant females and life expectancy <6 months were excluded. No chemotherapy was allowed during SBRT. All patients provided written informed consent.
Study design
A prospective, observational and multicentric national study (ClinicalTrials.gov; NCT00870116) was designed to provide a non-randomized clinical and economic evaluation of various SBRT modalities. Eligible patients were treated according to local equipment availability. The study design is presented on Figure 1. The study was opened in 16 departments but only 11 of them included at least one patient in the cohort. This study was funded by the French National Cancer Institute (INCa).
Figure 1.
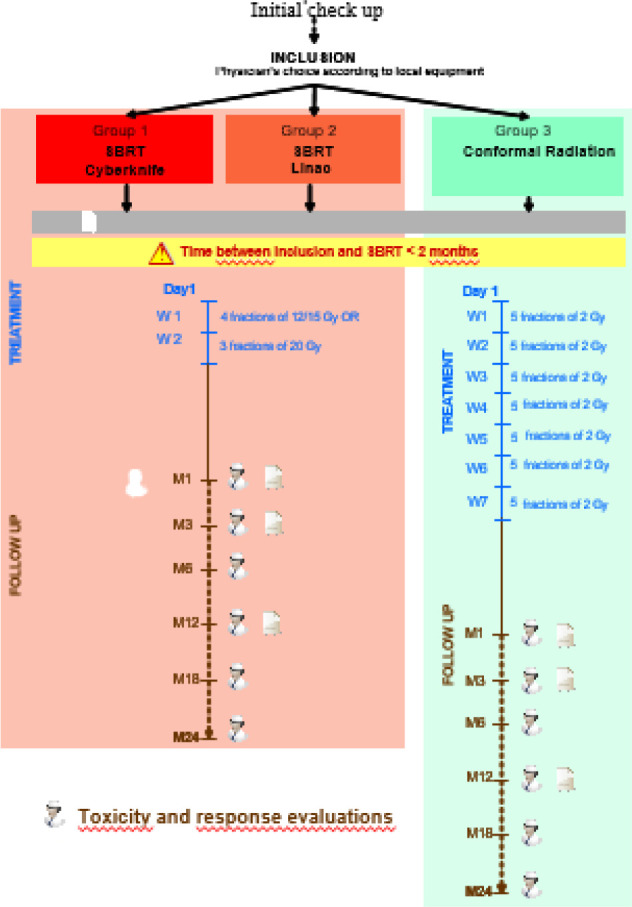
Study design. M: months ; W : week.
Study endpoints
The primary clinical endpoint was the local control rate 2 years after SBRT on thoracic scan, defined as complete response, partial response or stable disease using RECIST criteria. Local progression was defined as both regrowth in PTV on thoracic scan and PET accumulation.
Secondary clinical endpoints were acute and late toxicities using National Cancer Institute (NCI) Common Toxicity Criteria (CTC) V3 classification, 2 year-progression-free survival (PFS) and overall survival (OS) after the time of registration. The study was conducted in accordance with the ethical principles for medical research involving human subjects developed in the Declaration of Helsinki by the World Medical Association. The study received approval in France from the National Ethics Committee (N° 00–1142) and the National Committee for Protection of Personal Data (N°09–016).
Statistics
Crude analysis
A preliminary analysis of the original dataset was performed as followed: OS and PFS functions were calculated using the Kaplan-Meier method5 and compared between the two arms using a log-rank test.6 Because there were possible competitive events to local relapse, the competing risk approach was used to estimate local relapse-free survival.7 The cumulative incidence function developed by Kalbfleisch and Prentice8 and non-parametric Gray’s test9 were used to estimate and compare cumulative incidence function between the two arms. Event-free survival probabilities were reported as (1 - [cumulative incidence probability]).
Adjustment for potential bias due to non-randomization
Both standard multivariate analyses and the Inverse Probability of Treatment Weighting (IPTW) method using the propensity score were also implemented in order to control the potential selection bias associated with non-randomization. Including those two complementary methods allows to improve the robustness of the results.10,11 The propensity score is the probability of treatment by Cyberknife® conditional on observed baseline characteristics. We determined the probability of receiving treatment with a Cyberknife® by fitting a logit model to age, gender, histology, tumor stage, history of thoracic surgery, use of corticotherapy, total radiation dose and comorbidities. The IPTW method balanced the covariates of the two groups by weighting all the patients by the inverse of the propensity score. The stabilized weighted of the Inverse Probability Weighting proposed by Robins12 was used in order to reduce the volatility of the weights and to preserve the sample size in pseudodatasets.13 The balance of covariate distribution checking after propensity score was achieved by comparing standardized differences of the treatment groups before and after IPTW. Standardized differences were reported in Figure 2. A standardized difference (d) >20% for a given covariate indicated a strong imbalance. The adjusted Kaplan–Meier Estimator (AKME), proposed by Xie and Liu was applied in order to compare survival distributions.14 The significant difference in survival curves for the two groups was tested to take into account the non-independence of the data after using IPTW using the Cox test.15 The adjustment of the treatment effect in standard multivariate regressions analyses was performed on the same set of co-variables included in the propensity score analysis.
Figure 2.

Dotplot of standardized differences for the covariates included in the propensity score before and after matching. Before matching, histology, sex, tumor stage, total radiation dose and antecedent of thoracic surgery appeared unbalanced between treatment groups (standardized difference ≥20%).
Radiation modalities
The inclusion period was supposed to be 2 years initially and was extended by one more year, due to a slower recruitment rate than expected. 80 patients treated with SBRT with a linac and 20 patients treated with a Cyberknife® were expected. In addition, 20 patients treated with conformal radiotherapy (66 Gy, 2 Gy / fraction) were expected for the clinical part of the study only, in case SBRT was not possible for any reason. Radiotherapy had to be delivered within two months after the inclusion in every arm.
SBRT delivered by cyberknife®
A vacuum pillow was recommended for all the patients. Four tracking strategies were available for lung tumors treated with Cyberknife®, according to local investigator protocols: (i) X-Sight Lung with which the tumor was tracked by both cameras, (ii) Spine Tracking when the tumor was not visible on both views, in which case tracking was based on the proximal vertebra, (iii) the one-view tracking when the tumor was seen by only one camera and (iiii) a fiducial tracking requiring a fiducial implantation before SBRT treatment. The gross tumor volume (GTV) was delineated on a CT scan. A 5- to 8-mm margin was added to the GTV to form the planning target volume (PTV) according to local investigator discretion. All treatment plans were performed on the exhale CT scan using a Ray-Tracing algorithm. Photon beam energy was 6 MV. A total dose of 60 Gy in four fractions, 15 Gy per fraction, was delivered to the 80% isodose 2 to 3 days per week over a 2-week period. Delivering a dose of 60 Gy in 3 fractions of 20 Gy each to the 80% isodose was also secondarily allowed as some Cyberknife® investigators wanted to follow another international study (STARS study) recommendations which required 3 fractions of treatment.16
SBRT delivered by linac
Patients were immobilized using custom devices (i.e., Stereotactic Body Frame, Bodyfix…) according to local preference. Breathing-adapted radiation therapy was required according to the local equipment availability (treating the entire track of tumor motion using four-dimensional computed tomography (4DCT), abdominal compression, gating, active breathing control, or tracking). Either CT-scans with 3 mm slice width (end of inhalation phase and expiration phase) or 4D CT-scans were required. The PTV was defined again as the GTV (=internal target volume (ITV) considering CT-scan modalities) with 5 to 8 mm margins according to local technique. A fiducial implantation before SBRT treatment could be necessary according to the local equipment used. A total dose of 60 Gy in four fractions, 15 Gy per fraction, was to be delivered to the 80% isodose, 2 to 3 days per week over a 2-week time period. Due to high doses to critical organs, the dose could be reduced to 48 Gy in 4 fractions of 12 Gy at the physician’s discretion. Photons beam energy was 4–10 MV.
Follow-up
Follow-up was performed using thoracic scans 1, 3, 6, 12, 18 and 24 months after the end of SBRT and PET-CT at 12 and 24 months (Figure 1). Pulmonary Function Tests were done 3, 12 and 24 months after SBRT. Median follow-up was 25.1 months. Since one institution has reported data more than 24 months after SBRT, a maximum follow-up of 26 months has been retained for the analysis for all patients to avoid a bias (potential negative impact of this center due to a longer reporting period). While the study was funded for a 2-year follow-up, no longer follow-up was prospectively recorded.
Results
Patients and tumors characteristics in the unweighted population
From April 2009 to December 2011, 113 patients were accrued: nine centers enrolled <10 patients, one center enrolled 12 patients, and one enrolled more than 20 patients. Three patients were not treated due to death (hypoxemic pulmonary infection, one patient), or treatment were not technically feasible (two patients). Two major deviations were noticed: one patient with lymph node involvement (N1) and one patient with previous thoracic irradiation. Four patients were treated using conformal radiotherapy and 106 patients were treated with SBRT: 68 by linear accelerator (7 Novalis True Beam®/ExacTrac® and 61 Linac with CBCT) and 38 patients with Cyberknife®. The small sample of patients treated with conformal radiotherapy was not generalizable and therefore excluded from the present analysis. Patient and tumor characteristics are summarized in Table 1.
Table 1.
Patient and treatments characteristics
| Number of patients (%) | ||||
|---|---|---|---|---|
| Cyberknife® n = 38 | CBCT n = 68 | Total n = 106 | p-value | |
| Age, years | ||||
| Mean ± SD | 74.2 (8.7) | 72.7 (8.1) | 73.2 (8.3) | 0.3433 |
| Median (min-max) | 74.9 (55.7–90.5) | 73.4 (54.5–84.1) | 74.8 (54.5–90.5) | |
| Sex | ||||
| Male | 34 (89.5%) | 55 (80.9%) | 89 (83.9%) | 0.2477 |
| Histology | ||||
| Not histologically proven | 11 (28.9%) | 27 (39.7%) | 38 (35.8%) | 0.2243 |
| Adenocarcinoma | 12 (31.6%) | 20 (29.4%) | 32 (30.2%) | |
| Epidermoïd carcinoma | 15 (39.5%) | 16 (23.5%) | 31 (29.2%) | |
| Other | 0 (0%) | 4.(5.9%) | 4 (3.8%) | |
| Tumor stagea | 0.2243 | |||
| Stage IA | 25 (65.8%) | 50 (74.6%) | 75 (71.4%) | |
| Stage IB | 13 (34.2%) | 16 (23.9%) | 29 (27.6%) | |
| Stage IIA | 0 (0%) | 1 (1.5%) | 1 (0.9%) | |
| History of thoracic surgery | 6 (15.8%) | 18 (26.5%) | 24 (22.6%) | 0.5293 |
| Cardiovascular disease | 26 (68.4%) | 42 (61.8%) | 68 (64.1%) | 0.4931 |
| Past-pulmonary disease | 33 (86.8%) | 57 (83.8%) | 90 (84.9%) | 0.6772 |
| Other comorbidities | 27 (71.1%) | 48 (70.6%) | 75 (70.7%) | 0.9598 |
| Corticotherapy during RT | 9 (23.7%) | 21 (30.9%) | 30 (28.3%) | 0.4301 |
| GTV in cm3 | ||||
| Median (min-max) | 10.5 (2.0–129.0) | 9.0 (0.0–89.0) | 9.0 (0.0–129.0) | 0.2486 |
| PTV in cm3 | ||||
| Median (min-max) | 34.00 (2.00–337.0) | 32.50 (5.00–130.0) | 33.5 (2.0–337.0) | 0.9869 |
| Number of fractions | ||||
| Median (min-max) | 3.0 (3.0–5.0) | 4.0 (3.0–9.0) | 4.0 (3.0–9.0) | <0.0001 |
| Total radiation dose on PTV in Gy Median (min-max) |
60 (37–60) | 48 (36–60) | 48 (36–60) | <0.0001 |
ECOG, Eastern Cooperative Oncology Group; GTV, Gross Tumor Volume; PTV, Planning Target Volume.
(a) 14 missing data.
according to 6th TNM IASLC stage classification.
The median age was 75 years. Most of the patients were males (84%), active or former smokers (94%), with a NSCLC stage IA (71%). 25% of the patients had a Grade 3 dyspnea and higher at baseline and the median forced expiratory volume in 1 s (FEV1) was 1.37 L. Histology was unproven in 36% of the cases. GTVs and PTVs were not significantly different between SBRT by accelerator and Cyberknife®. The median energy used was 6 MV. Median prescription isodose was 80%. While total radiation dose was significantly different between the two groups, statistical methods were used to correct this observed bias (for details please see Methods: Statistics). 30 patients (27%) received corticosteroids, but only one had an initiation of this treatment during SBRT (inhaled corticosteroids). No patient received concomitant chemotherapy. Four premature discontinuations of SBRT were reported for undercurrent illness (n = 1), subject decision (n = 2), and physician decision (n = 1).
Recurrence and survival
Crude analysis
Within 26 months after inclusion, a local relapse was observed in two patients treated with SBRT by linac. A distant relapse occurred in 19 (27.9%) of the SBRT patients treated with a linear accelerator and 9 (23.7%) treated with a Cyberknife®. Figure 3 shows Kaplan–Meier curves. 2-year local control, progression-free survival and overall survival rates are reported in Table 2.
Figure 3.

Kaplan–Meier curves according to the arm of treatment (crude results) 3a: Local relapse-free survival 3b: Progression-Free Survival 3c: Overall Survival.
Table 2.
Recurrence and survival
| 2 year rates [95% CI] |
Crude analysis | After IPTW adjustment | ||||
|---|---|---|---|---|---|---|
| Linear accelerator | Cyberknife® | p | Linear accelerator | Cyberknife® | p | |
| Local control | 97.0% [90.6%;99.4%] | 100.0% [100%;100%] | 0.2839 | 95.6% [90.0%100.0%] | 100.0% [100%;100%] | 0.5703 |
| PFS rates | 52.7% [39.9%;64.0%] | 54.1% [36.8; 68.6%] | 0.8582 | 53.23% [40.3%;66.2%] | 36.9% [13.7%;60.1%] | 0.2875 |
| OS | 65.1% [51.9%;75.5%] | 83.9% [67.5%;92.4%] | 0.0831 | 65.9% [53.4% ;78.4%] | 83.5% [65.8% ;100.0%] | 0.2446 |
Adjustment for potential bias due to non-randomization
Multivariate regression analysis indicates no significant effect of treatment type on PFS (p = 0.1710) or on OS (p = 0.3041). Local relapse could not be modeled due to the small number of events (n = 2).
After IPTW adjustment, all standardized differences of weighted comparisons were <20%, indicating that the distributions of baseline patients and tumor characteristics were similar between treatment groups (Figure 2). Conclusions were unchanged after IPTW adjustment or multivariate analyses on local control (p = 0.5703), PFS (p = 0.2875), and OS (p = 0.2446).
Acute toxicity
Crude analysis
No difference was found between the rate of acute toxicity (grade ≥3) in the two groups (p = 0.1657). The details of acute grade ≥3 toxicities are presented in Table 3. Of the 29 patients who presented dyspnea (grade ≥3), it should be noted that it was already described at baseline in 20 of them. Similarly, cough (grade ≥3) was already reported at inclusion for all four patients who presented cough during the follow-up.
Table 3.
Acute toxicities (grade >3) and late toxicities (grade >2) using National Cancer Institute (NCI) Common Toxicity Criteria (CTC) V3 classification
| Cyberknife® n = 38 | Linac n = 68 | P-value | ||||
|---|---|---|---|---|---|---|
| ACUTE TOXICITY | 8 (21.1%) | 23 (33.8%) | 0.1657 (0.1849 after IPTW) | |||
| N | Maximum Grade | N | Maximum Grade | |||
| Cough | 1 | Grade 3 (1 pt already registered at baseline) | 3 | Grade 3 (including three pts already registered at baseline) | ||
| Dyspnea | 7 | Grade 3 (including six pts already registered at baseline) | 22 | 20 Grades 3 (including 13 pts already registered at baseline) 2 Grades 4 (including one pt already registered at baseline) |
||
| Respiratory Distress Syndrome (ARDS) | 0 | 1 | Grade 3 | |||
| Cutaneous toxicities | 0 | 1 | Grade 3 | |||
| Thoracic pain | 1 | Grade 3 | 0 | |||
| LATE TOXICITY | 20 (52.6%) | 38 (55.9%) | 0.7471 (0.4554 after IPTW) | |||
| N | Maximum Grade | N | Maximum Grade | |||
| Cough | 4 | Grade 2 (including one pt already registered at baseline) | 4 | 2 Grade 3 (including two pts already registered at baseline) | ||
| 2 Grade 2 (including two pts already registered at baseline) | ||||||
| Dyspnea | 16 | 8 Grade 2 (including six pts already registered at baseline) | 33 | 14 Grade 2 (including seven pts already registered at baseline) | ||
| 8 Grade 3 (including five pts already registered at baseline) | 16 Grade 3 | 10 already registered at baseline | ||||
| 3 Grade 4 | ||||||
| Respiratory Distress Syndrome (ARDS)a | 0 | 1 | 1 Grade 3 | |||
| Radiation fibrosis | 1 | 2 | 2 Grades 2 | |||
| Esophagitis*ab | 2 | 2 Grade 2 (both transitory) | 0 | |||
| Bone (rib) painc | 4 | 1 Grade 3 3 Grade 2 |
3 | 2 Grades 3 1 Grade 1 |
||
After IPTW, After Inverse Probability Weighting adjustment; N, number of patients; Pt/pts, patient, patients.
Not clearly related to SBRT but declared as adverse event by the local investigator.
1grade 2 at 18 months post SBRT and 1 gradeGrade 2 at 6 months post SBRT.
All transitory no rib fracture.
Adjustment for potential bias due to non-randomization
After IPTW adjustment, the occurrence of acute toxicities was also not significantly different between groups (p = 0.1849).
Long-term toxicity
Crude analysis
Thirty-eight patients (55.9%) reported at least one long-term Grade 2 or above toxicity in the Linac group, vs 20 (52.6%) in the Cyberknife® group (p = 0.7471) within the 2 years following SBRT. The detailed results are shown in Table 3. Dyspnea (grade ≥2) was reported in 49 patients but 31 of them had it at baseline. Similarly, 5 of the 13 patients with a cough (grade ≥2) had it already in the initial assessment.
Adjustment for potential bias due to non-randomization
After IPTW adjustment, the occurrence of long-term toxicities was also not significantly different between the two groups (p = 0.4554).
Discussion
To our knowledge, this study is the first prospective study comparing SBRT using an appropriately equipped linac with dedicated equipment such as Cyberknife® (Accuray, Sunnyvale, CA). Randomization is not easily achievable as the availability of equipment is different in the participating institutions and most of them do not have both types of equipment. Median total radiation dose was significantly different between the two groups (median dose 60 Gy in three fractions in Cyberknife® group versus 48 Gy in four fractions in Linac group) for historical reasons and physicians practices. However, the robustness of the results against bias, including this radiation dose difference, was assessed by two complementary methods to control selection bias in observational studies such as this, the regression adjustment and the propensity score analysis.17 Overall 2-year-local control is not significantly different in this situation of peripheral NSCLC between the Cyberknife® or SBRT linear-accelerator treated patients. These results confirm the high rate of local control, of above 90%, reported in the literature considering both techniques independently for T1–T2 peripheral localized NSCLC and providing high biological equivalent dose (>100–105 Gy - BED10), especially for T2 tumors.18 While the study was designed and funded only for a 2-year follow-up after SBRT, no results are available in term of long-term local control. This is regrettable as local recurrence may occur later. Of note, the radiation dose difference which was observed in this series did not lead to a significant difference in term of local control despite a higher dose in Cyberknife arm. The main studies reporting SBRT after Cyberknife® treatment are summarized in Table 4, together with the most recent prospective studies reporting SBRT using a Linac.19–26,28–33
Table 4.
Main studies reporting SBRT for NSCLC on Cyberknife® and Linac: efficiency and toxicities
| Author (year) (ref) | SBRT modality | Sample size | Follow-up (Months) | Dose scheme | Local control rate | Overall survival rate | Toxicity (Acute) |
Toxicity (late) |
|---|---|---|---|---|---|---|---|---|
| Nakamura19 | Retrospective Cyberknife® | 71 | 34 | 48–60 Gy in four fractions | 94% (2 y.) | 93% (2 y.) | NR | 1% gr 3 18% gr 2 (all) |
| Khadige20 | Retrospective Cyberknife® | 100 (71 primary NSCLC) | 24 | 60 Gy in three fractions | 93% (2 y.) peripheral lesions | NR | NR | NR |
| Tong21 | Retrospective Cyberknife® |
30 | 42–60 Gy in three fractions | 100% (1 y.) | NR | NR | NR | |
| Chen22 | Cyberknife® | 40 | 44 | 42–60 Gy in three fractions | 91% (3 y.) | 75% (3 y.) | NR | NR |
| Collins23 | Cyberknife® | 20 | 25 | 42–60 Gy in3 fractions | 100% (2 y.) | 87% (2 y.) | 25% PNO after fiducials 4% RP (gr 4) 66% rib pain if tumor close to pleura |
NR |
| Van Der Voort24 | Cyberknife® | 70 | 15 | 60 Gy in three fractions 45 Gy in three fractions |
96% (2 y.) 78% (2 y.) |
62% (2 y.) | 3% PNO after fiducials 10% gr 3 (all) 0% gr 4 (all) |
|
| Brown25 | Cyberknife® | 31 | 27 | 60 Gy in 3–5 fractions | 93% (1 y.) 86% (4 y.) |
86% (1 y.) 83% (4 y.) |
13% RP (Grade 2) 3% oesophagitis (gr 2) |
|
| Wang26 | Cyberknife® | 25 | 36 | 40–60 Gy in 2–5 days | 78% (3 years) | 70% (3 years) | 8% RP gr 3 8% RP gr 1–2 |
4% RP (gr 3) |
| Lischalt27 | Cyberknife® | 61 | 54–60 Gy in 3 to 5 fractions | 87% (5 y.) | 39% (5 y.) | 18% PNO after fiducials 0% PNO if fiducials using bronchoscopy |
21% rib fractures, median 2.9 y | |
| Nakamura28 | Cyberknife® | 56 | 12.5 | 48–56 Gy in four fractions | NR | NR | 10% RP >gr 2 | NR |
| Bahig29 | Cyberknife® | 150 | 22 | BED 180 | 96% (2 y.) | 95% (2 y.) | 1.3% RP gr 3 33% RP gr five if idiopathic fibrosis |
|
| Bauman30 | Linac | 57 | 35 | 45 Gy in three fractions | 92% (3 y.) | 65% (3 y.) | NR | NR |
| Timmerman31 | Linac | 34 | 55 | 54 Gy in three fractions | 97% (3 y.) | 56% (3 y.) | 12% RP (gr 3) 3.6% RP (gr 4) | |
| Ricardi32 | Linac | 62 | 28 | 45 Gy in three fractions | 88% (3 y.) | 57% (3 y.) | 10% mild symptoms (skin, fatigue…) | |
| Bral33 | Linac | 40 | 16 | 60 Gy in three fractions for peripheral lesions | 84% (2 y.) | 52% (2 y.) |
NR, not reported; PNO, pneumothorax; RP, radiation pneumonitis; gr, grade.
As shown in Table 4, historical comparisons show small differences in local control rates considering both strategies. Of note, while patient immobilization for Cyberknife®, treatment is usually simpler and more comfortable for the patient as compared to those used for SBRT delivered by a Linac, the local control remains excellent thanks to an optimized tracking strategy. However, the feasibility and compliance of SBRT was excellent even in the Linac arm, despite more invasive respiratory breathing-adapted systems (e.g., diaphragmatic compression). Unfortunately, the quality of life study which was initially planned within this project was not feasible due to a poor rate of patient response.
Considering PFS and OS, no significant effect of treatment type was shown. More specifically, the 2-year PFS and OS rates are similar to those reported in the literature (Table 3), independent of the equipment used to deliver the treatment, while relapses are mainly due to distant metastases, and death to metastatic progression or comorbidities.30,34
The treatment tolerance was excellent in both arms, with no difference in terms of acute or late toxicity. As shown in the literature, acute toxicity is quite rare after SBRT in peripheral lung cancer.32 No skin toxicity over Grade 2 was reported in either arm. The most frequent acute symptoms were dyspnea and cough but most of the patients already had these symptoms at inclusion, due to frequent respiratory comorbidities. As for late toxicity, the most common events in the literature are radiation fibrosis (RF) in 4–8% of the cases32 and rib pain (incidence about 11–15%) or fractures in 2–3% of the patients (27,32 especially for tumors close to pleura23). In this series, we confirm that late RF over Grade 1 is reported in less than 3%, while late rib pain remains more frequent (5 to 11% in our series) but is usually transitory. Of note, no rib fracture was reported at 2 years in this series, but they often happen later, usually more than 2 years after SBRT.27 No significant difference was shown between the two strategies in term of toxicity. However, the study population included selected patients with only localized peripheral lesions. This point is crucial and it would be very interesting and helpful to mount a study comparing the different strategies of SBRT in other situations of lung cancers. For instance, proximal lesions or re-irradiation were not included in this study and can lead to additional treatment planning difficulties and toxicities as compared with peripheral tumors.33 Cyberknife® technology may be helpful in such situations dealing with doses to central critical organs, but a comparison, for example, with treatment using SBRT with Arctherapy may be relevant to discover the best option for these situations. Finally, economic data will be shortly reported in another paper.
Conclusion
In this large prospective non-randomized study focusing on peripheral localized NSCLC, no difference inefficiency or toxicity was shown after SBRT treatment using Linac equipped for SBRT or Cyberknife®.
Footnotes
Acknowledgements: This multicenter study involved 11 French centers who included at least one patient in the cohort. We would like to acknowledge them : Centre Oscar Lambret (Lille), Centre Antoine Lacassagne (Nice), Centre Alexis Vautrin (Vandoeuvre les Nancy), Centre Paul Papin (Angers), Centre Georges François Leclerc (Dijon), Centre Léon Bérard (Lyon), Centre Val d’Aurelle Paul Lamarque (Montpellier), Hôpital Tenon (Paris), Centre René Gauducheau (Saint-Herblain), Hôpital Henri Mondor (Créteil), CHR Orléans. Ms Sophie KING for English review.
Funding: This study was funded by the National Cancer Institute (INCa), 52 Avenue André Morizet, 92513 Boulogne Billancourt Cedex, for the collection of data.
Contributor Information
Line Claude, Email: line.claude@lyon.unicancer.fr.
Magali Morelle, Email: magali.morelle@lyon.unicancer.fr.
Marc-André Mahé, Email: marc-andre.mahe@ico.unicancer.fr.
David Pasquier, Email: d-pasquier.oscar-lambret@medical59.apicrypt.org.
Pierre Boisselier, Email: boisselier@icm.unicancer.fr.
Pierre Yves Bondiau, Email: bondiau@nice.unicancer.fr.
Emmanuel Touboul, Email: emmanuel.touboul@tnn.aphp.fr.
Karine Peignaux-Casasnovas, Email: peignaux@cgfl.fr.
Isabelle Martel-Lafay, Email: isabelle.martel-lafay@lyon.unicancer.fr.
Frederic Gassa, Email: frederic.Gassa@lyon.unicancer.fr.
Lionel Perrier, Email: Lionel.perrier@lyon.unicancer.fr.
Sophie Dussart, Email: sophie.dussard@lyon.unicancer.fr.
Veronique Beckendorf, Email: veronique.beckendorf@gmail.com.
REFERENCES
- 1.Falkson CB, Vella ET, Yu E, El-Mallah M, Mackenzie R, Ellis PM, et al. Radiotherapy with curative intent in patients with early-stage, medically inoperable, Non–Small-cell lung cancer: a systematic review. Clin Lung Cancer 2017; 18: 105–21. doi: 10.1016/j.cllc.2016.10.008 [DOI] [PubMed] [Google Scholar]
- 2.Louie AV, van Werkhoven E, Chen H, Smit EF, Paul MA, Widder J, et al. Patient reported outcomes following stereotactic ablative radiotherapy or surgery for stage Ia non-small-cell lung cancer: results from the ROSEL multicenter randomized trial. Radiother Oncol 2015; 117: 44–8. doi: 10.1016/j.radonc.2015.08.011 [DOI] [PubMed] [Google Scholar]
- 3.Nagata Y, Hiraoka M, Shibata T, Onishi H, Kokubo M, Karasawa K, et al. Prospective trial of stereotactic body radiation therapy for both operable and inoperable T1N0M0 non-small cell lung cancer: Japan clinical Oncology Group study JCOG0403. Int J Radiat Oncol Biol Phys 2015; 93: 989–96. doi: 10.1016/j.ijrobp.2015.07.2278 [DOI] [PubMed] [Google Scholar]
- 4.Shen Z-T, Wu X-H, Li B, Zhu X-X. Clinical outcomes of CyberKnife stereotactic body radiotherapy for peripheral stage I non-small cell lung cancer. Med Oncol 2015; 32: 55. doi: 10.1007/s12032-015-0506-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53: 457–81. doi: 10.1080/01621459.1958.10501452 [DOI] [Google Scholar]
- 6.Peto R, Pike MC, Armitage P, Breslow NE, Cox DR, Howard SV, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Br J Cancer 1977; 35: 1–39. doi: 10.1038/bjc.1977.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med 1999; 18: 695–706. doi: 10.1002/(SICI)1097-0258(19990330)18:6<695::AID-SIM60>3.0.CO;2-O [DOI] [PubMed] [Google Scholar]
- 8.Librairie Lavoisier. Statistical analysis of failure time data, 2nd ed [Internet]. 2020. Available from: https://www.lavoisier.fr/livre/mathematiques/statistical-analysis-of-failure-time-data-2nd-ed/kalbfleisch/descriptif_1366915 [2020 Mar 12].
- 9.Grey.pdf [Internet]. A Class of K-Sample Tests for Comparing the Cumulative Incidence of aCompeting Risk. 2020. Available from: http://www2.math.uu.se/~garmo/Grey.pdf.
- 10.Stuart EA. Matching methods for causal inference: a review and a look forward. Stat Sci 2010; 25: 1–21. doi: 10.1214/09-STS313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stürmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. J Clin Epidemiol 2006; 59: 437.e1–437.e24. doi: 10.1016/j.jclinepi.2005.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Robin JM. Proceedings the American Statistical Association, Section on Bayesian Statistical Science; 1998. [Google Scholar]
- 13.Xu S, Ross C, Raebel MA, Shetterly S, Blanchette C, Smith D. Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health 2010; 13: 273–7. doi: 10.1111/j.1524-4733.2009.00671.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Xie J, Liu C. Adjusted Kaplan-Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Stat Med 2005; 24: 3089–110. doi: 10.1002/sim.2174 [DOI] [PubMed] [Google Scholar]
- 15.Cole SR, Hernán MA. Adjusted survival curves with inverse probability weights. Comput Methods Programs Biomed 2004; 75: 45–9. doi: 10.1016/j.cmpb.2003.10.004 [DOI] [PubMed] [Google Scholar]
- 16.Samson P, Keogan K, Crabtree T, Colditz G, Broderick S, Puri V, et al. Interpreting survival data from clinical trials of surgery versus stereotactic body radiation therapy in operable stage I non-small cell lung cancer patients. Lung Cancer 2017; 103: 6–10. doi: 10.1016/j.lungcan.2016.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mistry H. Exploring two cost-adjustment methods for selection bias in a small sample: using a fetal cardiology dataset. Int J Technol Assess Health Care 2014; 30: 325–32. doi: 10.1017/S026646231400021X [DOI] [PubMed] [Google Scholar]
- 18.Davis JN, Medbery C, Sharma S, Perry D, Pablo J, D'Ambrosio DJ, et al. Stereotactic body radiotherapy for early-stage non-small cell lung cancer: clinical outcomes from a national patient registry. J Radiat Oncol 2015; 4: 55–63. doi: 10.1007/s13566-014-0177-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nakamura M, Nishikawa R, Mayahara H, Uezono H, Harada A, Hashimoto N, et al. Pattern of recurrence after CyberKnife stereotactic body radiotherapy for peripheral early non-small cell lung cancer. J Thorac Dis 2019; 11: 214–21. doi: 10.21037/jtd.2018.12.115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Khadige M, Salleron J, Marchesi V, Oldrini G, Peiffert D, Beckendorf V. Cyberknife® stereotactic radiation therapy for stage I lung cancer and pulmonary metastases: evaluation of local control at 24 months. J Thorac Dis 2018; 10: 4976–84. doi: 10.21037/jtd.2018.07.26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tong A-N, Yan P, Yuan G-H, Lv X-Y, Gong H, Zhao H, et al. Advantages of CyberKnife for inoperable stage I peripheral non-small-cell lung cancer compared to three-dimensional conformal radiotherapy. Mol Clin Oncol 2015; 3: 442–8. doi: 10.3892/mco.2014.475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chen VJ, Oermann E, Vahdat S, Rabin J, Suy S, Yu X, et al. CyberKnife with tumor tracking: an effective treatment for high-risk surgical patients with stage I non-small cell lung cancer. Front Oncol 2012; 2: 9. doi: 10.3389/fonc.2012.00009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Collins BT, Vahdat S, Erickson K, Collins SP, Suy S, Yu X, et al. Radical cyberknife radiosurgery with tumor tracking: an effective treatment for inoperable small peripheral stage I non-small cell lung cancer. J Hematol Oncol 2009; 2: 1. doi: 10.1186/1756-8722-2-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.van der Voort van Zyp NC, Prévost J-B, Hoogeman MS, Praag J, van der Holt B, Levendag PC, et al. Stereotactic radiotherapy with real-time tumor tracking for non-small cell lung cancer: clinical outcome. Radiother Oncol 2009; 91: 296–300. doi: 10.1016/j.radonc.2009.02.011 [DOI] [PubMed] [Google Scholar]
- 25.Brown WT, Wu X, Fayad F, Fowler JF, García S, Monterroso MI, et al. Application of robotic stereotactic radiotherapy to peripheral stage I non-small cell lung cancer with curative intent. Clin Oncol 2009; 21: 623–31. doi: 10.1016/j.clon.2009.06.006 [DOI] [PubMed] [Google Scholar]
- 26.Wang Z, Li A-M, Gao J, Li J, Li B, Lee P, et al. Clinical outcomes of CyberKnife stereotactic radiosurgery for elderly patients with presumed primary stage I lung cancer. Transl Lung Cancer Res 2017; 6: 6–13. doi: 10.21037/tlcr.2017.02.04 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lischalk JW, Woo SM, Kataria S, Aghdam N, Paydar I, Repka MC, et al. Long-Term outcomes of stereotactic body radiation therapy (SBRT) with fiducial tracking for inoperable stage I non-small cell lung cancer (NSCLC. J Radiat Oncol 2016; 5: 379–87. doi: 10.1007/s13566-016-0273-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nakamura M, Nishimura H, Nakayama M, Mayahara H, Uezono H, Harada A, et al. Dosimetric factors predicting radiation pneumonitis after CyberKnife stereotactic body radiotherapy for peripheral lung cancer. Br J Radiol 2016; 89: 20160560. doi: 10.1259/bjr.20160560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bahig H, Filion E, Vu T, Roberge D, Lambert L, Bouchard M, et al. Excellent cancer outcomes following Patient-adapted robotic lung SBRT but a case for caution in idiopathic pulmonary fibrosis. Technol Cancer Res Treat 2015; 14: 667–76. doi: 10.7785/tcrt.2012.500445 [DOI] [PubMed] [Google Scholar]
- 30.Baumann P, Nyman J, Hoyer M, Wennberg B, Gagliardi G, Lax I, et al. Outcome in a prospective phase II trial of medically inoperable stage I Non–Small-Cell lung cancer patients treated with stereotactic body radiotherapy. Journal of Clinical Oncology 2009; 27: 3290–6. doi: 10.1200/JCO.2008.21.5681 [DOI] [PubMed] [Google Scholar]
- 31.Timmerman R, Papiez L, McGarry R, Likes L, DesRosiers C, Frost S, et al. Extracranial stereotactic radioablation: results of a phase I study in medically inoperable stage I non-small cell lung cancer. Chest 2003; 124: 1946–55. doi: 10.1378/chest.124.5.1946 [DOI] [PubMed] [Google Scholar]
- 32.Ricardi U, Badellino S, Filippi AR. Stereotactic body radiotherapy for early stage lung cancer: history and updated role. Lung Cancer 2015; 90: 388–96. doi: 10.1016/j.lungcan.2015.10.016 [DOI] [PubMed] [Google Scholar]
- 33.Bral S, Gevaert T, Linthout N, Versmessen H, Collen C, Engels B, et al. Prospective, risk-adapted strategy of stereotactic body radiotherapy for early-stage non-small-cell lung cancer: results of a phase II trial. Int J Radiat Oncol Biol Phys 2011; 80: 1343–9. doi: 10.1016/j.ijrobp.2010.04.056 [DOI] [PubMed] [Google Scholar]
- 34.Timmerman R, Paulus R, Galvin J, Michalski J, Straube W, Bradley J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 2010; 303: 1070–6. doi: 10.1001/jama.2010.261 [DOI] [PMC free article] [PubMed] [Google Scholar]