

Abstract
Physical exercise can minimize dysfunction and optimize functional motor recovery after stroke by modulating cortical plasticity. However, the limitation of physical exercise is that large amounts of time and effort are necessary to significantly improve motor function, and even then, substantial exercise may not be sufficient to normalize the observed improvements. Thus, interventions that could be used to strengthen physical exercise-induced neuroplasticity may be valuable in treating hemiplegia after stroke. Repetitive transcranial magnetic stimulation seems to be a viable strategy for enhancing such plasticity. As a non-invasive cortical stimulation technique, repetitive transcranial magnetic stimulation is able to induce long-term plastic changes in the motor system. Recently, repetitive transcranial magnetic stimulation was found to optimize the plastic changes caused by motor training, thereby enhancing the long-term effects of physical exercise in stroke patients. Therefore, it is believed that the combination of repetitive transcranial magnetic stimulation and physical exercise may represent a superior method for restoring motor function after stroke.
Keywords: functional recovery, motor cortex, neuroplasticity, physical exercise, primary motor cortex, repetitive transcranial magnetic stimulation, stroke
Introduction
Stroke is a major cause of long-standing disability globally (Feigin et al., 2014). Hemiplegia of the upper extremities, which is the most prevalent form of stroke-induced dysfunction, has persistent and disabling consequences for stroke patients that affect quality of life and productivity (Winstein et al., 2016). Although the human brain has the spontaneous capacity to protect neurons and restore damaged neuronal function, this does not substantially improve survival quality or motor recovery.
Neural plasticity refers to the ability of the brain to adjust its function to adapt to new environments. From a neurophysiological point of view, neuroplasticity is primarily a stimulus-dependent synaptic phenomenon (Dayan and Cohen, 2011; Small et al., 2013). Plasticity is related to the balance between gamma-aminobutyric acid (GABA) inhibition and glutamatergic excitation in intracortical circuits (Benali et al., 2008). Regarding stroke, it includes the modulation of neural activation within the remaining motor network to maximize neural resources and resume function (Maldonado et al., 2008).
Functional recovery following stroke is associated with changes in the anatomy and function of the brain (Wang et al., 2010; Dijkhuizen et al., 2014; Wu et al., 2015). The changes in structure and function after stroke occur in the motor cortex and other brain areas (Chen and Schlaug, 2013; Fan et al., 2013; Cai et al., 2016; Tik et al., 2017). These structural changes include the restriction of dendritic and axonal branches, the formation of synapses, and the generation of new neuronal connections (Sampaio-Baptista et al., 2018). Structural plastic changes occur near the lesion, while anterograde or retrograde degeneration can occur in axons associated with the damaged area (Reitmeir et al., 2011). In the post-stroke rodent model, a large number of axonal fiber tracts recombine along the infarct edge, and pyramidal tract axons survive at the distal end of the ischemic brain injury area, with damaged axonal sprouting in the ipsilateral and contralateral pyramidal tract system. In addition, modification of the transcallosal projections between the two motor cortices has been observed (Hermann and Chopp, 2012).
Functional changes have been found to occur in response to learning and experience via the regulation of existing connections, for example, as the result of changes in presynaptic release levels of neurotransmitters, or the insertion or removal of presynaptic or postsynaptic receptors (Sampaio-Baptista et al., 2018). Practicing a particular movement is a process of motor learning (Wenger et al., 2017). Xu et al. (2009) found that practicing the reaching task caused output pyramidal neurons in the contralateral motor cortex to rapidly (within 1 hour) form a post-synaptic dendritic spine. They concluded that rapid synaptic reorganization is closely related to motor learning. Furthermore, different sets of synapses appear to encode different motor skills. Indeed, many studies have shown that stroke-induced changes in neural plasticity are an important foundation for the recovery of motor function (Andres et al., 2011; Reitmeir et al., 2011; Hermann and Chopp, 2012). With regard to brain plasticity after stroke, Van Meer et al. (2012) proposed the following four points: (1) Improved sensorimotor function is associated with the reorganization of functional connectivities between hemispheres and the normalization of the bilateral sensorimotor cortical network, (2) the gradual restoration of sensory motor function following stroke is related to increased structural integrity in the ipsilesional corticospinal tract (CST), (3) the recovery of functional connectivities between the bilateral sensorimotor cortices is associated with improved structural integrity in the unilateral CST, and (4) excellent functional outcomes are correlated with the retention or repair of structural integrity within the ipsilesional CST (van Meer et al., 2012). Indeed, the recovery of motor function following stroke is a complicated process in which both the integrity of the ipsilesional CST and remodeling of brain network connectivities appear to play a significant role.
Motor training has been recommended for stroke survivors to reduce limb paralysis (Billinger et al., 2014). Behavioral interventions, such as physical exercise, aim to improve motor function by shaping neural reorganization. As reported by some neurobehavioral studies with animals and humans, this exercise-dependent reorganization can occur at multiple levels of the central nervous system, ranging from molecular to synaptic levels, to cortical maps and broad-scale brain networks. The molecular pathways activated by behavioral interventions can induce remodeling of the damaged brain through angiogenesis, neurogenesis, axon plasticity, and dendritic plasticity (Zhang and Chopp, 2009). Stroke can deteriorate physiological brain maps in the cortex surrounding the infarct and then remap the motor and sensory functions in that area. The degree of functional remapping in the peri-infarct cortex is closely related to recovery (Carmichael, 2012). For instance, as a form of stroke rehabilitation therapy, constraint-induced movement therapy has been widely recognized as an effective treatment (Thrane et al., 2014). The theoretical basis of the treatment is the “learned non-use” of impaired limbs (Taub et al., 2006). With the goal of limiting the effects of the “learned non-use” phenomenon, constraint-induced movement therapy increases the patient’s use of their affected limb and thus alters certain neuronal changes driven by experience with the contralateral limb. The mechanisms of this treatment involve the remodeling of the structure and function of the central nervous system, and include processes such as angiogenesis, changes in brain metabolic intensity, neuronal renewal, brain activation, and protein expression (Kempf et al., 2014; Qu et al., 2014; Blicher et al., 2015; Ishida et al., 2015; Urushidani et al., 2018). However, exercise training alone is often not sufficient to resume normal function, although the outcome can be improved by combining exercise training with other treatments.
Transcranial magnetic stimulation (TMS), which is based on the principle of electromagnetic induction, a current generated by a magnetic stimulation coil placed on the surface of the head activates neurons in the cortical and subcortical regions, causing neuronal depolarization (Kobayashi and Pascual-Leone, 2003). A single TMS pulse can depolarize inhibitory or excitatory axons. This causes changes in the excitability and permeability of cells (Ridding and Rothwell, 2007), thus influencing cortical plasticity (Müller-Dahlhaus and Ziemann, 2015). When TMS pulses are repeatedly applied, they can up-regulate or down-regulate cortical excitability in accordance with the parameters of the stimulation. These changes can exceed the duration of the stimulation and even persist as long-term effects (Hsu et al., 2012; Chervyakov et al., 2015). Although the physiological bases of the long-term effects of repetitive TMS (rTMS) remain unclear, evidence from animal studies has indicated that the mechanisms may be relevant to long-term potentiation (LTP) and long-term depression (LTD) (Di Lazzaro et al., 2010). The duration of the after-effect is typically 30 to 60 minutes, and depends on the stimulus parameters, such as the number of applied pulses, stimulation frequency, number of sessions, and the intensity of each stimulus (Lefaucheur et al., 2014).
Through the mechanisms mentioned above, rTMS and physical exercise have been found to have synergistic effects on synaptic and network plasticity. Thus, a combination of rTMS and exercise training may enhance the functional changes that could be obtained by either therapy alone. Physical exercise can guide the activation of particular neural networks to correlate with target behaviors. After ischemic stroke, improved plasticity is often observed for 1 to 3 months, and both spontaneous and intervention-mediated recovery is maximal within this period (Zeiler and Krakauer, 2013). rTMS may help to prolong this time window, providing greater opportunities for appropriate behavioral therapy to enhance functional recovery. Therefore, in this review, we considered the mechanisms of recovery with respect to neural plasticity after stroke and proposed targets for future trials, as well as protocol design. We searched experimental studies and reviews on neural plasticity after stroke in the PubMed, GeenMedical, and Google Scholar search engines using the key words “neural plasticity”, “cortical plasticity”, “stroke”, “rTMS”, “motor training”, and “physical exercise”. The time range for the publications was set as 1990–2019.
Mechanisms of Repetitive Transcranial Magnetic Stimulation Associated with Neuroplasticity
rTMS is a promising non-invasive brain stimulation technique that promotes functional recovery by modulating neural plasticity and reorganizing post-stroke motor network connectivity (Grefkes and Fink, 2012). The motor system comprises a complex network of cortical and subcortical regions that interact through excitatory and inhibitory circuits. Stroke impresses the interaction between motor areas, and then triggers changes in connectivity that are correlated with motor impairments (de Vico Fallani et al., 2009; Almeida et al., 2017). Inhibitory rTMS applied over the contralesional primary motor cortex (M1) was found to correlate with an clear reduction in pathological connectivity between the ipsilesional and contralesional M1 when compared with a control stimulation site (Grefkes et al., 2010). Furthermore, enhanced neural connectivity between the ipsilesional M1 and ipsilesional supplementary motor area was implicated in motor recovery (Grefkes et al., 2010). Hence, it appears that in addition to changing the connectivity of the targeted region, rTMS can also alter that of remote areas. This suggests that the stimulation-induced behavioral effects rely on the reorganization of the whole network rather than that of a certain motor region. Coinciding with this conclusion, other studies have indicated that rTMS can simultaneously regulate the excitability of the motor and non-motor cortex. The brain regions in the motor network mainly include the M1, premotor cortex, and supplementary motor area. Non-motor cortex regions, such as the cerebellum, thalamus, and dorsolateral prefrontal cortex, have also been implicated in motor recovery after stroke (Cramer, 2008). More thorough integration of the ipsilesional M1 into the motor network structure may be a key factor in improving motor function in stroke patients after rTMS (Grefkes et al., 2010). This conclusion is consistent with the observation via resting state functional magnetic resonance imaging analysis that spontaneous recovery over time is related to increased connectivity of the ipsilesional M1 (Wang et al., 2010).
The utilization of rTMS following stroke is largely based on interhemispheric inhibition. Interhemispheric inhibition refers to the neuronal excitability in each cerebral hemisphere that inhibits that in the contralateral hemisphere, allowing brain activity to be balanced between hemispheres (Nowak et al., 2009). However, a stroke-induced structural lesion may significantly disturb the complex hemispheric balance by reducing the inhibition effects in the non-lesioned hemisphere and increasing inhibition in the lesioned hemisphere. This can result in overactivation of the contralesional hemisphere compared with the lesioned hemisphere (Nowak et al., 2009). According to the rTMS parameters, LTD or LTP of cortical excitability can be induced: low-frequency rTMS (≤ 1 Hz) usually leads to a decrease in cortical excitability, and thus inhibitory effects, while high-frequency rTMS (> 1 Hz) results in an increase in cortical excitability, and therefore excitatory effects (Lefaucheur et al., 2014). The possible mechanisms involved in rTMS-induced LTP or LTD are discussed in the following sections:
Modulation of neurotransmitters and receptors
Niimi et al. (2020) found that levels of D-serine, which is a N-methyl-D-aspartic acid (NMDA) receptor-related amino acid, were lower in the rTMS group compared with a control group. This indicates that rTMS can regulate NMDA receptor-related amino acids, and that this regulation is associated with beneficial treatment effects (Niimi et al., 2020). Besides, an animal experiment found that 5 days of electromagnetic radiation exposure led to high levels of the neuromediators named as nitric oxide and cyclic guanosine monophosphate in the cerebral cortex, hippocampus, and gyri (Cho et al., 2012).
Effects on gene expression
Aydin-Abidin et al. (2008) examined the effects of low-frequency rTMS and high-frequency rTMS on the genetic expression of zif268 and c-Fos. Low-frequency rTMS and high-frequency rTMS both increased the expression of the c-Fos gene in all tested cortical regions, but 10-Hz rTMS had this effect only in the motor and sensory cortices. Although 1-Hz rTMS and sham stimulation did not affect the expression of zif268, sham stimulation increased c-Fos expression in the limbic zone (Aydin-Abidin et al., 2008). Furthermore, Funamizu et al. (2005) revealed that rTMS influences the expression of tyrosine hydroxylase and NeuN in the substantia nigra. Previous research has clearly demonstrated that TMS signaling stimulates and induces gene expression and increases the production of many enzymes. These effects may be the basis for the lasting effects of TMS (Simis et al., 2013).
Promotion of BDNF generation
Low-intensity stimulation (1.14 T, 1 Hz) was found to cause sudden axonal sprouting and growth, as well as increase the density of synaptic contacts in hippocampal cell cultures (Ma et al., 2013). In contrast, high-intensity stimulation (1.55 T, 1 Hz) had a devastating effect, decreasing the number of dendrites, synapses, and axons in the damaged neuronal areas. The authors revealed that these results were correlated with the brain-derived neurotrophic factor (BDNF)-tyrosine kinase B (TrkB) signaling system (Ma et al., 2013). Moreover, 5-Hz rTMS daily for 5 days significantly increased serum levels of BDNF (mature BDNF + proBDNF) in healthy participants, giving rise to the activation of BDNF-TrkB signaling (Wang et al., 2011). The Val66Met polymorphism of the BDNF gene has been found to have a negative impact on the effects of rTMS for upper limb hemiplegia after stroke (Chang et al., 2014). These findings indicate that the observed changes in peripheral blood flow are due to rTMS-induced regulation of BDNF-TrkB signaling (Wang et al., 2011).
The available data indicate that rTMS applied over the intact hemisphere in stroke patients does not merely remodel neural connectivity in the whole network, but can also lead to more adaptive plasticity.
Mechanisms of Physical Exercise Associated with Changes in Plasticity
Reorganization and repair of the injured brain is based on the regulation of experience-dependent plasticity (Sampaio-Baptista et al., 2018). In motor systems, plastic reorganization is primarily driven by physical practice. Reorganization of the brain involves a unique pattern of activity. Because axonal sprouting is a responsive process (Harms et al., 2008), the post-stroke emergence of adaptive and maladaptive activity patterns may influence the formation of new connections. One of the most important features of mammalian brain activity is that it can change with experience. At the organizational level, the adaptive benefits of experience-dependent change are the basis of our learning capacity. However, persistent experience-dependent maladaptive effects are of equal importance, including the formation of benign habits and adaptation to destructive conditions. In the aforementioned circumstances, these changes appear at the level of neural circuitry and individual neurons, and involve the reordering of gene expression, synaptic strength, and circuit connectivity (Allred and Jones, 2008b, a). Stroke induces unique gene expression in sprouting neurons or transcriptomes. Gene expression comprises a network of integrated signaling systems involving growth factors, cell surface receptors, intermediate cytoplasmic cascades, transcription factors, and epigenetic regulators (Li et al., 2010). Lee et al. (2013) found that in an animal model of stroke, functional recovery varied according to the rehabilitation time and lesion size. During the post-stroke recovery period, repetitive training of the affected forelimb reduced the size of motor representations in the intact hemisphere (Barbay et al., 2013). The underlying mechanism may involve contralesional CST plasticity and transcallosal axonal sprouting (Lee et al., 2013).
Behavioral experience can elicit the growth and regression of dendrites, changes in synaptic efficacy, modification of the vascular and glial systems, and can sometimes cause neurons to be added or lost (Kleim and Jones, 2008). Animal experiments have indicated that exercise training can not only up-regulate BDNF transcription and translation levels in healthy animals, but that it can also promote BDNF expression in the hippocampus, cortex, and cerebellum after ischemic stroke (Gomez-Pinilla et al., 2008). Furthermore, blocking BDNF via gene mutations or neutralization of antibodies can notably reduce the expression of cyclic adenosine monophosphate response-element-binding protein, and then eliminate exercise-induced recovery of motor learning memory (Ploughman et al., 2009). Exercise training has been found to promote plastic changes in the damaged motor network, specifically in M1, the premotor cortex, and the posterior parietal cortex (Youssofzadeh et al., 2016; De Vico Fallani et al., 2017). Physical exercise, particularly in paretic limbs, could reduce activity in the contralesional M1 and alter the activity of related brain regions (Barbay et al., 2013). Furthermore, physical activity training is able to facilitate changes in synaptic plasticity, including LTP and LTD (Citri and Malenka, 2008).
The evidence suggests that synaptic strength in the motor cortex is modifiable, and that synaptic strength could provide a basis for shifting the topography of motor cortical maps via rehabilitative interventions such as physical exercise.
Combined Repetitive Transcranial Magnetic Stimulation and Physical Exercise to Enhance Neuroplasticity and Motor Function
As described above, both rTMS and exercise training can regulate neural plasticity, and both play a role in remodeling brain networks (Figure 1). Thus, combined rTMS and exercise training may have a synergistic effect, enabling maximization of their respective therapeutic effects. Some experimental studies have provided initial support for this hypothesis. In the following section, we review several studies examining the integration of motor training and rTMS.
Figure 1.
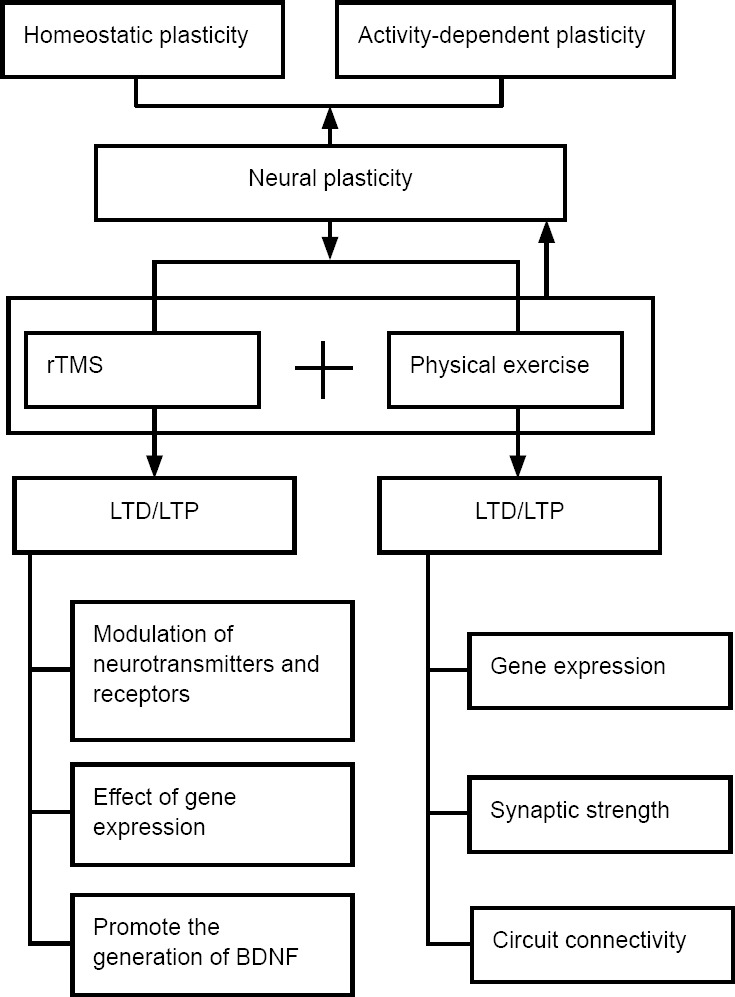
A schematic outline of the mechanisms by which rTMS and physical exercise induce plastic changes.
When rTMS is combined with physical exercise, two types of plasticity occur: homeostatic plasticity and activity-dependent plasticity. BDNF: Brain-derived neurotrophic factor; LTD: long-term depression; LTP: long-term potentiation; rTMS: repetitive transcranial magnetic stimulation.
Kim and Yim (2018) found that acute stroke patients who received high-frequency rTMS (20 Hz) and completed task-oriented mirror therapy showed more positive changes in motor evoked potential and hand function compared with those who underwent high-frequency rTMS only. This indicates that the combination of therapies had a more advantageous effects in terms of regulating cortical excitability and enhancing hand function (Kim and Yim, 2018).
A recent study of subacute stroke patients reported similar results. The researchers found that Manual Function Test subscores of hand motor function and grip power were distinctively improved in participants who completed both mirror therapy and high-frequency rTMS therapy rather than high-frequency rTMS alone. Thus, the combination of rTMS with action observation may be more helpful in improving upper limb function (Noh et al., 2019).
Studies of chronic post-stroke patients reached similar conclusions. Avenanti et al. (2012) divided 30 chronic stroke patients into rTMSreal-physical therapy, physical therapy-rTMSreal, rTMSsham-physical therapy, and physical therapy-rTMSsham groups. They found that physical therapy induced by inhibitory rTMS (1 Hz) most strongly promoted use-dependent plasticity and rebalanced the excitability of the two hemispheres. Thus, this combination mode of physical therapy and rTMS was advantageous in terms of motor function recovery and the restoration of cortical excitability. Chang et al. (2012) showed that in post-stroke patients, a 10-day high-frequency rTMS (10 Hz) treatment course in a combination with a finger-attack training task improved motion accuracy by modulating activity in the cortical-basal ganglia-thalamic cortex circuit. This suggests that rTMS combined with hand function training could affect the neuroplasticity of various brain networks.
The above evidence indicates that a combined intervention strategy is optimal for regulating cortical plasticity and enhancing motor function in post-stroke patients. In addition to rTMS and exercise training conducted sequentially, studies on the effect of rTMS applied during exercise training also found enhanced cortical excitability and clinical outcomes. The application of rTMS during exercise training is based on Hebbian theory (Hebb, 1949), which describes the basic principles of synaptic plasticity as the continuous repetitive stimulation of postsynaptic neurons by presynaptic neurons, inducing synaptic transmission and enhancing function.
A study based on Hebbian theory investigated the hypothesis that synchronous application of TMS and a motor training task might improve use-dependent plasticity. During physical exercise, repetitive practice of particular movements can build up motor memory, which is a form of use-dependent plasticity (Classen et al., 1998). The researchers found that motor memory encoded with use-dependent plasticity could be improved by synchronized Hebbian stimulation over the motor cortex (Bütefisch et al., 2004). This study opened the door to a new modality of non-invasive brain stimulation for post-stroke patients. Buetefisch and colleagues (Buetefisch et al., 2011) also tested whether motor training combined with Hebbian-type stimulation over M1 could improve M1 reorganization in stroke patients. They concluded that Hebbian-type stimulation over M1 was feasible in stroke patients and that it induced map recombination that was correlated with decreases in GABAergic inhibition (Buetefisch et al., 2011).
However, Todd et al. (2009) found that the relationship between voluntary movement and rTMS-induced plasticity in the motor cortex is complex. They applied high-frequency rTMS (6 Hz) for 5 seconds, repeated every 30 seconds for 10 minutes. The size of the resting motor evoked potential was inhibited for 15 minutes after the rTMS intervention. Surprisingly, rTMS applied during voluntary muscle contractions did not change the maximal finger tapping speed or motor performance, or behavior in a visuomotor tracking task. In contrast, Yin et al. (2015) concluded that both 5-Hz rTMS alone and 5-Hz rTMS integrated with maximum voluntary muscle contractions were able to improve excitability in the motor cortex of healthy subjects, although the synchronous combination produced a more apparent enhancement than that of rTMS alone, and had a longer-lasting effect. A study based on chronic stroke patients reached similar conclusion. A study randomly assigned 18 chronic stroke survivors into a functional rTMS (electromyogram-triggered rTMS, 10 Hz) group or passive rTMS (rTMS only; control) group. The results indicated that functional rTMS reduced short-interval intracortical inhibition and increased intracortical facilitation, while passive rTMS reduced abductor pollicis brevis muscle activity and the coefficient of variation of the force. However, no changes were observed in the relevant measurements (electromyogram, intracortical facilitation, short-interval intracortical inhibition) of the first dorsal interosseus. The authors concluded that compared with passive rTMS, functional rTMS promoted greater excitatory changes and selectively modulated agonistic muscle activity (Massie et al., 2013a). In the same year, the research team found enhanced cortical excitability and improved stability after both single and repeated functional rTMS, while passive stimulation tended to reduce excitability and did not improve stability (Massie et al., 2013b).
The aforementioned studies confirmed the effectiveness and feasibility of rTMS synchronized with exercise training, thus providing a new intervention mode for future research. However, the existing studies mainly examined healthy participants and chronic stroke patients. Future studies should investigate the effects of Hebbian-type stimulation on acute and subacute stroke patients and further attempt to detect the underlying mechanisms.
In addition to further clarifying the effectiveness of synchronous integration of the two interventions, exploring optimization of the two techniques is an important direction for future research.
Repetitive Transcranial Magnetic Stimulation in Combination with Physical Exercise: Methods for Optimizing Functional Enhancement
At present, few clinical trials have examined the combination of exercise training and rTMS, and there is a particular lack of large-sample and multi-center clinical studies. Thus, it is difficult to make predictions regarding the clinical utility of this intervention method.
rTMS alone does not lead to long-term behavioral changes in humans, but must be combined with physical exercise to enhance movement performance. When rTMS is applied for treatment of motor impairment following stroke, different types of plasticity should be considered to optimize the positive effects. There are three main types of plasticity: spontaneous plasticity, homeostatic plasticity, and activity-dependent plasticity (Hebbian plasticity; Schambra, 2018; Figure 1).
Spontaneous plasticity refers to the neuroplastic response to the damaged areas and remote interconnected regions. It is time-limited, and generally lasts for a period of weeks in stroke patients (Schambra, 2018). Rehme et al. (2011) examined interhemispheric and intrahemispheric connectivity during different courses of stroke. Their results showed that during the acute phase, positive coupling of the supplementary motor area and premotor cortex in the affected hemisphere decreased, and the negative impacts of damaged areas on M1 were reduced in the unaffected hemisphere. During the subacute stage, positive effects were expressed from the contralesional M1 to the ipsilesional M1. While the negative impact of activity in the affected area on the contralateral M1 subsequently returned to normal, patients with poor prognoses in the chronic phase showed increased negative coupling between the M1 in the two hemispheres (Rehme et al., 2011). This indicates that the course of disease should directly influence the selection of rTMS parameters, especially in terms of stimulation frequency. A meta-analysis indicated that the effectiveness of rTMS declined gradually according to the stroke stage: acute > subacute > chronic (Zhang et al., 2017). Therefore, to maximize the benefits, rTMS should be applied as early as possible to influence spontaneous plasticity.
The severity of stroke and the lesion site is also a factor influencing treatment efficiency. The standard approach to brain stimulation in stroke patients is based on the idea that the ipsilesional M1 is necessary for motor function of the paretic upper limb (Nudo and Milliken, 1996), while the contralesional M1 competes with the ipsilesional M1. As a result, facilitation of the ipsilesional M1 and/or inhibition of the contralesional M1 is typically advocated, and is widely applied among stroke patients to enhance motor performance (Lefaucheur et al., 2014). However, this approach fails to elicit substantial improvement in severely affected stroke patients, who may have highly damaged ipsilesional pathways. Thus, simulating the ipsilesional M1 may not be the optimal approach (Talelli et al., 2012; Levy et al., 2016). One study found that mildly affected stroke patients showed improved reaching task performance with standard inhibition of the contralesional M1, while severely affected patients showed improvements with a novel method involving facilitatory 5-Hz rTMS of the contralesional dorsal premotor cortex (Sankarasubramanian et al., 2017). An increasing number of clinical trials have reached similar conclusions (McCambridge et al., 2018; Harrington et al., 2020). The stroke severity illustrated here is important for selecting candidates for tailored stimulation in future studies, such that patients with different stroke severity levels may optimally benefit in terms of paretic upper extremity function. Hence, for patients with mild motor impairments, M1 may be the most appropriate stimulation site. For patients with serious impairments, the contralesional dorsal premotor cortex may be a better choice.
Stroke is usually classified as cortical stroke or subcortical stroke, according to the lesion site. Emara et al. (2009) showed that subcortical stroke patients benefited more from 1 Hz rTMS stimulation than cortical stroke patients. Ameli et al. (2009) investigated the effects of 10-Hz rTMS over the ipsilesional M1 on cortical and subcortical stroke patients. They found that 14 of 16 patients with subcortical stroke showed enhanced movement kinematics while no improvement was detected in cortical stroke patients (Ameli et al., 2009). Furthermore, a meta-analysis indicated that rTMS was more favorable for subcortical stroke survivors in terms of restoring upper limb motor dysfunction (Hsu et al., 2012; Zhang et al., 2017). Thus, both excitatory and inhibitory rTMS are beneficial for subcortical stroke patients in terms of recovering upper limb motor function.
rTMS can be used to “prime” patients in terms of homeostatic plasticity, preparing them for the subsequent interventions. One study provided Class I evidence that using low-frequency rTMS before physical therapy was more beneficial than applying physical therapy before low-frequency rTMS or a sham stimulation (Avenanti et al., 2012). Higgins et al. (2013) found that delivering low-frequency rTMS followed by motor training benefited more that 75% patients in the experimental group, who displayed increased excitability of the motor cortex at the end of the first stimulation session. Moreover, another study reported that compared with hand training performed 2 hours after low-frequency rTMS, hand training immediately after low-frequency rTMS led to more rapid enhancement in the motor power of hands (Park et al., 2018).
Further research is needed to determine the best options for optimizing the effects of rTMS with physical exercise. Relevant factors may include not only the severity of disease, stimulation sites, the course of disease, and the intervention time of physical exercise, but also the integrity of the ipsilesional CST and treatment parameters related to rTMS, such as stimulation frequency and stimulation interval.
Previous studies have indicated that the integrity of the CST is closely tied to motor function (Sterr et al., 2014). Yarossi et al. (2019) suggested that the patients presence of motor evoked potentials enhanced more apparent than those absence of motor evoked potentials compared with the change of the Wolf Motor Function Test, box and block test, and the active range of finger motion scores between baseline and post-intervention. This result illustrates that motor recovery likely relies on the integrity of the CST in the affected hemisphere.
As for the parameters of rTMS, frequency is always the most important parameter in a rTMS protocol. Both high-frequency rTMS and low-frequency rTMS have been widely used in stroke patients to restore motor impairments. The 2014 European Guideline on the therapeutic utilization of rTMS proposed a Level B recommendation for low-frequency rTMS of the contralesional M1 in chronic stroke patients and a Level C recommendation for high-frequency rTMS of the ipsilesional M1 in (post-)acute and chronic stroke patients (Lefaucheur et al., 2014). The Guideline added new data and proposed a level A recommendation for low-frequency rTMS used for hand function recovery in acute stroke patients and a level B recommendation for high-frequency rTMS for restoration of motor function in post-acute stroke patients (Lefaucheur et al., 2020). Recently, an animal study elucidated the impact of high-frequency rTMS and low-frequency rTMS in an acute-ischemic stroke model at a cellular and molecular level. The results illustrated that high-frequency rTMS (20 Hz) had more positive outcomes than low-frequency rTMS (1 Hz) in both acute and subacute mouse models of ischemic stroke. Specifically, high-frequency rTMS enhanced functional recovery by decreasing the infarct volume and rate of apoptosis, as well as activating neuronal survival, neurogenesis, neuronal plasticity, and regional cerebral blood flow (Caglayan et al., 2019). A meta-analysis also indicated that directly facilitating ipsilesional M1 excitability may be more effective than suppressing contralesional M1 excitability for enhancing post-stroke motor recovery (McDonnell and Stinear, 2017). With respect to the safety of different stimulation frequencies, published guidelines indicate that in individuals without known risk factors, high-frequency (> 1 Hz) rTMS is less likely to cause seizures (Lerner et al., 2019). Future studies are needed to identify the most favorable stimulation frequencies for different cases.
The stimulation interval is a crucial and easily adjusted parameter in terms of modulating cortical excitability. Previous studies have reported that low-frequency rTMS can inhibit the excitability of the unaffected hemisphere, while high-frequency rTMS can increase the excitability of the affected hemisphere. A study of 14 healthy participants found that continuous high-frequency rTMS (5 Hz) tended to have an inhibitory effect while stimulation with the traditional block design tended to have a facilitatory effect (Rothkegel et al., 2010). Further exploration is necessary to identify the most beneficial rTMS protocol.
Activity-dependent plasticity arises from interventions in which rTMS is applied during physical exercise. Previous studies have demonstrated the feasibility of activity-dependent rTMS for use with stroke patients (Bütefisch et al., 2004; Edwardson et al., 2013). However, in addition to the type of rTMS protocol, the form of physical exercise is also important. For patients with severe dysfunction, robot-assisted rehabilitation training represents a promising treatment strategy (Radder et al., 2019). Post-stroke patients with mild motor impairments can engage in various active movements, such as constraint-induced movement and task-oriented motor training. Individual differences in treatment response are also an important consideration for future research.
In summary, evidence to date suggests that patients with smaller lesions have greater potential for recovery and a stronger response to rehabilitation programs. Measures of cortical connectivity, such as electroencephalography, are useful, along with other biomarkers, for stratifying stroke patients, enabling the delivery of optimized personalized interventions. A future challenge is the development of a suite of rehabilitation approaches, with different programs optimized for different stroke patient groups, including those with severe damage (Sampaio-Baptista et al., 2018).
Conclusion
Stroke patients may be responsive to a variety of external interventions, including behavioral training and neuromodulation methods such as rTMS. Our understanding of the underlying mechanisms of treatments involving rTMS and physical exercise is increasing along with our ability to regulate neuroplasticity. In this review, we presented the mechanisms by which rTMS combined with physical exercise induce changes in neuroplasticity. Both of these treatment approaches are able to regulate synaptic plasticity and further cause LTP or LTD. Furthermore, they can be used to remodel brain networks and reorganize the functional connections between brain regions, further promoting the recovery of motor function in stroke patients. Preliminary research has mainly focused on the combination of these approaches, and reported advantages in terms of regulating cortical excitability and improving motor performance. In recent years, an increasing number of experiments have examined the synchronous combination of these approaches in regulating activity-dependent plasticity. However, future work regarding the use of rTMS in combination with physical exercise is necessary, especially in terms of the disease course, lesion site, severity of stroke, and integrity of the CST. Moreover, large-sample and multi-center trials are needed to optimize rTMS protocols and produce more evidence to facilitate the development of individualized treatment programs.
Acknowledgments
We would like to thank the colleagues from Department of Rehabilitation Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China and Department of Rehabilitation Medicine, Shanghai Ruijin Rehabilitation Hospital for supporting our work and provide effective suggestions.
Footnotes
Conflicts of interest: The authors declare no conflicts of interest.
Financial support: This work was supported by the Shanghai Jiao Tong University School of Medicine-Institute of Neuroscience, Chinese Academy of Sciences, Leading Startup Project of Brain Diseases Clinical Research Center of China, No. 2017NKX002 (to QX).
Copyright license agreement: The Copyright License Agreement has been signed by all authors before publication.
Plagiarism check: Checked twice by iThenticate.
Peer review: Externally peer reviewed.
Funding: This work was supported by the Shanghai Jiao Tong University School of Medicine-Institute of Neuroscience, Chinese Academy of Sciences, Leading Startup Project of Brain Diseases Clinical Research Center of China, No. 2017NKX002 (to QX).
C-Editor: Zhao M; S-Editors: Yu J, Li CH; L-Editors: Yu J, Song LP; T-Editor: Jia Y
References
- 1.Allred RP, Jones TA. Maladaptive effects of learning with the less-affected forelimb after focal cortical infarcts in rats. Exp Neurol. 2008;210:172–181. doi: 10.1016/j.expneurol.2007.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Allred RP, Jones TA. Experience--a double edged sword for restorative neural plasticity after brain damage. Future Neurol. 2008b;3:189–198. doi: 10.2217/14796708.3.2.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Almeida SRM, Vicentini J, Bonilha L, De Campos BM, Casseb RF, Min LL. Brain connectivity and functional recovery in patients with ischemic stroke. J Neuroimaging. 2017;27:65–70. doi: 10.1111/jon.12362. [DOI] [PubMed] [Google Scholar]
- 4.Ameli M, Grefkes C, Kemper F, Riegg FP, Rehme AK, Karbe H, Fink GR, Nowak DA. Differential effects of high-frequency repetitive transcranial magnetic stimulation over ipsilesional primary motor cortex in cortical and subcortical middle cerebral artery stroke. Ann Neurol. 2009;66:298–309. doi: 10.1002/ana.21725. [DOI] [PubMed] [Google Scholar]
- 5.Andres RH, Horie N, Slikker W, Keren-Gill H, Zhan K, Sun G, Manley NC, Pereira MP, Sheikh LA, McMillan EL, Schaar BT, Svendsen CN, Bliss TM, Steinberg GK. Human neural stem cells enhance structural plasticity and axonal transport in the ischaemic brain. Brain. 2011;134:1777–1789. doi: 10.1093/brain/awr094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Avenanti A, Coccia M, Ladavas E, Provinciali L, Ceravolo MG. Low-frequency rTMS promotes use-dependent motor plasticity in chronic stroke: a randomized trial. Neurology. 2012;78:256–264. doi: 10.1212/WNL.0b013e3182436558. [DOI] [PubMed] [Google Scholar]
- 7.Aydin-Abidin S, Trippe J, Funke K, Eysel UT, Benali A. High- and low-frequency repetitive transcranial magnetic stimulation differentially activates c-Fos and zif268 protein expression in the rat brain. Exp Brain Res. 2008;188:249–261. doi: 10.1007/s00221-008-1356-2. [DOI] [PubMed] [Google Scholar]
- 8.Barbay S, Guggenmos DJ, Nishibe M, Nudo RJ. Motor representations in the intact hemisphere of the rat are reduced after repetitive training of the impaired forelimb. Neurorehab Neural Repair. 2013;27:381–384. doi: 10.1177/1545968312465193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Benali A, Weiler E, Benali Y, Dinse HR, Eysel UT. Excitation and inhibition jointly regulate cortical reorganization in adult rats. J Neurosci. 2008;28:12284–12293. doi: 10.1523/JNEUROSCI.1952-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Billinger SA, Arena R, Bernhardt J, Eng JJ, Franklin BA, Johnson CM, MacKay-Lyons M, Macko RF, Mead GE, Roth EJ, Shaughnessy M, Tang A, American Heart Association Stroke C, Council on C, Stroke N, Council on L, Cardiometabolic H, Council on E, Prevention, Council on Clinical C Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:2532–2553. doi: 10.1161/STR.0000000000000022. [DOI] [PubMed] [Google Scholar]
- 11.Blicher JU, Near J, Næss-Schmidt E, Stagg CJ, Johansen-Berg H, Nielsen JF, Østergaard L, Ho YCL. GABA levels are decreased after stroke and GABA changes during rehabilitation correlate with motor improvement. Neurorehab Neural Repair. 2015;29:278–286. doi: 10.1177/1545968314543652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Buetefisch C, Heger R, Schicks W, Seitz R, Netz J. Hebbian-type stimulation during robot-assisted training in patients with stroke. Neurorehab Neural Repair. 2011;25:645–655. doi: 10.1177/1545968311402507. [DOI] [PubMed] [Google Scholar]
- 13.Bütefisch CM, Khurana V, Kopylev L, Cohen LG. Enhancing encoding of a motor memory in the primary motor cortex by cortical stimulation. J Neurophysiol. 2004;91:2110–2116. doi: 10.1152/jn.01038.2003. [DOI] [PubMed] [Google Scholar]
- 14.Caglayan AB, Beker MC, Caglayan B, Yalcin E, Caglayan A, Yulug B, Hanoglu L, Kutlu S, Doeppner TR, Hermann DM, Kilic E. Acute and post-acute neuromodulation induces stroke recovery by promoting survival signaling, neurogenesis, and pyramidal tract plasticity. Front Cell Neurosci. 2019;13:144. doi: 10.3389/fncel.2019.00144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cai J, Ji Q, Xin R, Zhang D, Na X, Peng R, Li K. Contralesional cortical structural reorganization contributes to motor recovery after sub-cortical stroke: a longitudinal voxel-based morphometry study. Front Hum Neurosci. 2016;10:393. doi: 10.3389/fnhum.2016.00393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Carmichael ST. Brain excitability in stroke: the yin and yang of stroke progression. Arch Neurol. 2012;69:161–167. doi: 10.1001/archneurol.2011.1175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chang WH, Bang OY, Shin YI, Lee A, Pascual-Leone A, Kim YH. BDNF polymorphism and differential rTMS effects on motor recovery of stroke patients. Brain Stimul. 2014;7:553–558. doi: 10.1016/j.brs.2014.03.008. [DOI] [PubMed] [Google Scholar]
- 18.Chang WH, Kim YH, Yoo WK, Goo KH, Park CH, Kim ST, Pascual-Leone A. rTMS with motor training modulates cortico-basal ganglia-thalamocortical circuits in stroke patients. Restor Neurol Neurosci. 2012;30:179–189. doi: 10.3233/RNN-2012-110162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen JL, Schlaug G. Resting state interhemispheric motor connectivity and white matter integrity correlate with motor impairment in chronic stroke. Front Neurol. 2013;4:178. doi: 10.3389/fneur.2013.00178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chervyakov AV, Chernyavsky AY, Sinitsyn DO, Piradov MA. Possible Mechanisms Underlying the Therapeutic Effects of Transcranial Magnetic Stimulation. Front Hum Neurosci. 2015;9:303. doi: 10.3389/fnhum.2015.00303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cho SI, Nam YS, Chu LY, Lee JH, Bang JS, Kim HR, Kim HC, Lee YJ, Kim HD, Sul JD, Kim D, Chung YH, Jeong JH. Extremely low-frequency magnetic fields modulate nitric oxide signaling in rat brain. Bioelectromagnetics. 2012;33:568–574. doi: 10.1002/bem.21715. [DOI] [PubMed] [Google Scholar]
- 22.Citri A, Malenka RC. Synaptic plasticity: multiple forms, functions, and mechanisms. Neuropsychopharmacology. 2008;33:18–41. doi: 10.1038/sj.npp.1301559. [DOI] [PubMed] [Google Scholar]
- 23.Classen J, Liepert J, Wise SP, Hallett M, Cohen LG. Rapid plasticity of human cortical movement representation induced by practice. J Neurophysiol. 1998;79:1117–1123. doi: 10.1152/jn.1998.79.2.1117. [DOI] [PubMed] [Google Scholar]
- 24.Cramer SC. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Mechanisms of spontaneous recovery Ann Neurol. 2008;63:272–287. doi: 10.1002/ana.21393. [DOI] [PubMed] [Google Scholar]
- 25.Crystal GJ, Pagel PS. Right ventricular perfusion: physiology and clinical implications. Anesthesiology. 2018;128:202–218. doi: 10.1097/ALN.0000000000001891. [DOI] [PubMed] [Google Scholar]
- 26.Dayan E, Cohen LG. Neuroplasticity subserving motor skill learning. Neuron. 2011;72:443–454. doi: 10.1016/j.neuron.2011.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.De Vico Fallani F, Clausi S, Leggio M, Chavez M, Valencia M, Maglione AG, Babiloni F, Cincotti F, Mattia D, Molinari M. Interhemispheric connectivity characterizes cortical reorganization in motor-related networks after cerebellar lesions. Cerebellum. 2017;16:358–375. doi: 10.1007/s12311-016-0811-z. [DOI] [PubMed] [Google Scholar]
- 28.de Vico Fallani F, Astolfi L, Cincotti F, Mattia D, la Rocca D, Maksuti E, Salinari S, Babiloni F, Vegso B, Kozmann G, Nagy Z. Evaluation of the brain network organization from EEG signals: a preliminary evidence in stroke patient. Anat Rec (Hoboken) 2009;292:2023–2031. doi: 10.1002/ar.20965. [DOI] [PubMed] [Google Scholar]
- 29.Di Lazzaro V, Profice P, Pilato F, Dileone M, Oliviero A, Ziemann U. The effects of motor cortex rTMS on corticospinal descending activity. Clin Neurophysiol. 2010;121:464–473. doi: 10.1016/j.clinph.2009.11.007. [DOI] [PubMed] [Google Scholar]
- 30.Dijkhuizen RM, Zaharchuk G, Otte WM. Assessment and modulation of resting-state neural networks after stroke. Curr Opin Neurol. 2014;27:637–643. doi: 10.1097/WCO.0000000000000150. [DOI] [PubMed] [Google Scholar]
- 31.Edwardson MA, Lucas TH, Carey JR, Fetz EE. New modalities of brain stimulation for stroke rehabilitation. Exp Brain Res. 2013;224:335–358. doi: 10.1007/s00221-012-3315-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Emara T, El Nahas N, Elkader HA, Ashour S, El Etrebi A. MRI can predict the response to therapeutic repetitive transcranial magnetic stimulation (rTMS) in stroke patients. J Vasc Interv Neurol. 2009;2:163–168. [PMC free article] [PubMed] [Google Scholar]
- 33.Fan F, Zhu C, Chen H, Qin W, Ji X, Wang L, Zhang Y, Zhu L, Yu C. Dynamic brain structural changes after left hemisphere subcortical stroke. Hum Brain Mapp. 2013;34:1872–1881. doi: 10.1002/hbm.22034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson L, Truelsen T, O’Donnell M, Venketasubramanian N, Barker-Collo S, Lawes CMM, Wang W, Shinohara Y, Witt E, Ezzati M, Naghavi M, Murray C, et al. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. 2014;383:245–254. doi: 10.1016/s0140-6736(13)61953-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Funamizu H, Ogiue-Ikeda M, Mukai H, Kawato S, Ueno S. Acute repetitive transcranial magnetic stimulation reactivates dopaminergic system in lesion rats. Neurosci Lett. 2005;383:77–81. doi: 10.1016/j.neulet.2005.04.018. [DOI] [PubMed] [Google Scholar]
- 36.Gomez-Pinilla F, Vaynman S, Ying Z. Brain-derived neurotrophic factor functions as a metabotrophin to mediate the effects of exercise on cognition. Eur J Neurosci. 2008;28:2278–2287. doi: 10.1111/j.1460-9568.2008.06524.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Grefkes C, Fink GR. Disruption of motor network connectivity post-stroke and its noninvasive neuromodulation. Curr Opin Neurol. 2012;25:670–675. doi: 10.1097/WCO.0b013e3283598473. [DOI] [PubMed] [Google Scholar]
- 38.Grefkes C, Nowak DA, Wang LE, Dafotakis M, Eickhoff SB, Fink GR. Modulating cortical connectivity in stroke patients by rTMS assessed with fMRI and dynamic causal modeling. Neuroimage. 2010;50:233–242. doi: 10.1016/j.neuroimage.2009.12.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Harms KJ, Rioult-Pedotti MS, Carter DR, Dunaevsky A. Transient spine expansion and learning-induced plasticity in layer 1 primary motor cortex. J Neurosci. 2008;28:5686–5690. doi: 10.1523/JNEUROSCI.0584-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Harrington RM, Chan E, Rounds AK, Wutzke CJ, Dromerick AW, Turkeltaub PE, Harris-Love ML. Roles of lesioned and nonlesioned hemispheres in reaching performance poststroke. Neurorehab Neural Repair. 2020;34:61–71. doi: 10.1177/1545968319876253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hebb DO. Oxford, UK: Wiley; 1949. The organization of behavior: a neuropsychological theory. [Google Scholar]
- 42.Hermann DM, Chopp M. Promoting brain remodelling and plasticity for stroke recovery: therapeutic promise and potential pitfalls of clinical translation. Lancet Neurol. 2012;11:369–380. doi: 10.1016/S1474-4422(12)70039-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Higgins J, Koski L, Xie H. Combining rTMS and task-oriented training in the rehabilitation of the arm after stroke: a pilot randomized controlled trial. Stroke Res Treat. 2013;2013:539146. doi: 10.1155/2013/539146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012;43:1849–1857. doi: 10.1161/STROKEAHA.111.649756. [DOI] [PubMed] [Google Scholar]
- 45.Ishida A, Misumi S, Ueda Y, Shimizu Y, Cha-Gyun J, Tamakoshi K, Ishida K, Hida H. Early constraint-induced movement therapy promotes functional recovery and neuronal plasticity in a subcortical hemorrhage model rat. Behav Brain Res. 2015;284:158–166. doi: 10.1016/j.bbr.2015.02.022. [DOI] [PubMed] [Google Scholar]
- 46.Kempf A, Tews B, Arzt ME, Weinmann O, Obermair FJ, Pernet V, Zagrebelsky M, Delekate A, Iobbi C, Zemmar A, Ristic Z, Gullo M, Spies P, Dodd D, Gygax D, Korte M, Schwab ME. The sphingolipid receptor S1PR2 is a receptor for Nogo-a repressing synaptic plasticity. PLoS Biol. 2014;12:e1001763. doi: 10.1371/journal.pbio.1001763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kim J, Yim J. Effects of high-frequency repetitive transcranial magnetic stimulation combined with task-oriented mirror therapy training on hand rehabilitation of acute stroke patients. Med Sci Monit. 2018;24:743–750. doi: 10.12659/MSM.905636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. 2008;51:S225-239. doi: 10.1044/1092-4388(2008/018). [DOI] [PubMed] [Google Scholar]
- 49.Kobayashi M, Pascual-Leone A. Transcranial magnetic stimulation in neurology. Lancet Neurol. 2003;2:145–156. doi: 10.1016/s1474-4422(03)00321-1. [DOI] [PubMed] [Google Scholar]
- 50.Lee KH, Kim JH, Choi DH, Lee J. Effect of task-specific training on functional recovery and corticospinal tract plasticity after stroke. Restor Neurol Neurosci. 2013;31:773–785. doi: 10.3233/RNN-130336. [DOI] [PubMed] [Google Scholar]
- 51.Lefaucheur JP, Aleman A, Baeken C, Benninger DH, Brunelin J, Di Lazzaro V, Filipović SR, Grefkes C, Hasan A, Hummel FC, Jääskeläinen SK, Langguth B, Leocani L, Londero A, Nardone R, Nguyen JP, Nyffeler T, Oliveira-Maia AJ, Oliviero A, Padberg F, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014-2018) Clin Neurophysiol. 2020;131:474–528. doi: 10.1016/j.clinph.2019.11.002. [DOI] [PubMed] [Google Scholar]
- 52.Lefaucheur JP, André-Obadia N, Antal A, Ayache SS, Baeken C, Benninger DH, Cantello RM, Cincotta M, de Carvalho M, De Ridder D, Devanne H, Di Lazzaro V, Filipović SR, Hummel FC, Jääskeläinen SK, Kimiskidis VK, Koch G, Langguth B, Nyffeler T, Oliviero A, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS) Clin Neurophysiol. 2014;125:2150–2206. doi: 10.1016/j.clinph.2014.05.021. [DOI] [PubMed] [Google Scholar]
- 53.Lerner AJ, Wassermann EM, Tamir DI. Seizures from transcranial magnetic stimulation 2012-2016: Results of a survey of active laboratories and clinics. Clin Neurophysiol. 2019;130:1409–1416. doi: 10.1016/j.clinph.2019.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Levy RM, Harvey RL, Kissela BM, Winstein CJ, Lutsep HL, Parrish TB, Cramer SC, Venkatesan L. Epidural electrical stimulation for stroke rehabilitation: results of the prospective, multicenter, randomized, single-blinded everest trial. Neurorehab Neural Repair. 2016;30:107–119. doi: 10.1177/1545968315575613. [DOI] [PubMed] [Google Scholar]
- 55.Li S, Overman JJ, Katsman D, Kozlov SV, Donnelly CJ, Twiss JL, Giger RJ, Coppola G, Geschwind DH, Carmichael ST. An age-related sprouting transcriptome provides molecular control of axonal sprouting after stroke. Nat Neurosci. 2010;13:1496–1504. doi: 10.1038/nn.2674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ma J, Zhang Z, Su Y, Kang L, Geng D, Wang Y, Luan F, Wang M, Cui H. Magnetic stimulation modulates structural synaptic plasticity and regulates BDNF-TrkB signal pathway in cultured hippocampal neurons. Neurochem Int. 2013;62:84–91. doi: 10.1016/j.neuint.2012.11.010. [DOI] [PubMed] [Google Scholar]
- 57.Maldonado MA, Allred RP, Felthauser EL, Jones TA. Motor skill training, but not voluntary exercise, improves skilled reaching after unilateral ischemic lesions of the sensorimotor cortex in rats. Neurorehab Neural Repair. 2008;22:250–261. doi: 10.1177/1545968307308551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Massie CL, Tracy BL, Malcolm MP. Functional repetitive transcranial magnetic stimulation increases motor cortex excitability in survivors of stroke. Clin Neurophysiol. 2013a;124:371–378. doi: 10.1016/j.clinph.2012.07.026. [DOI] [PubMed] [Google Scholar]
- 59.Massie CL, Tracy BL, Paxton RJ, Malcolm MP. Repeated sessions of functional repetitive transcranial magnetic stimulation increases motor cortex excitability and motor control in survivors of stroke. NeuroRehabilitation. 2013b;33:185–193. doi: 10.3233/NRE-130944. [DOI] [PubMed] [Google Scholar]
- 60.McCambridge AB, Stinear JW, Byblow WD. Revisiting interhemispheric imbalance in chronic stroke: A tDCS study. Clin Neurophysiol. 2018;129:42–50. doi: 10.1016/j.clinph.2017.10.016. [DOI] [PubMed] [Google Scholar]
- 61.McDonnell MN, Stinear CM. TMS measures of motor cortex function after stroke: A meta-analysis. Brain Stimul. 2017;10:721–734. doi: 10.1016/j.brs.2017.03.008. [DOI] [PubMed] [Google Scholar]
- 62.Müller-Dahlhaus F, Ziemann U. Metaplasticity in human cortex. Neuroscientist. 2015;21:185–202. doi: 10.1177/1073858414526645. [DOI] [PubMed] [Google Scholar]
- 63.Niimi M, Fujita Y, Ishima T, Hashimoto K, Sasaki N, Hara T, Yamada N, Abo M. Role of D-serine in the beneficial effects of repetitive transcranial magnetic stimulation in post-stroke patients. Acta Neuropsychiatr. 2020 doi: 10.1017/neu.2020.4. doi:101017/neu20204. [DOI] [PubMed] [Google Scholar]
- 64.Noh JS, Lim JH, Choi TW, Jang SG, Pyun SB. Effects and safety of combined rTMS and action observation for recovery of function in the upper extremities in stroke patients: A randomized controlled trial. Restor Neurol Neurosci. 2019;37:219–230. doi: 10.3233/RNN-180883. [DOI] [PubMed] [Google Scholar]
- 65.Nowak DA, Grefkes C, Ameli M, Fink GR. Interhemispheric competition after stroke: brain stimulation to enhance recovery of function of the affected hand. Neurorehab Neural Repair. 2009;23:641–656. doi: 10.1177/1545968309336661. [DOI] [PubMed] [Google Scholar]
- 66.Nudo RJ, Milliken GW. Reorganization of movement representations in primary motor cortex following focal ischemic infarcts in adult squirrel monkeys. J Neurophysiol. 1996;75:2144–2149. doi: 10.1152/jn.1996.75.5.2144. [DOI] [PubMed] [Google Scholar]
- 67.Park JW, Kim SB, Lee KW, Lee JH, Park JG, Lee SJ. Effects of hand training during the aftereffect period of low-frequency rTMS in subacute stroke patients. Ann Rehabil Med. 2018;42:521–527. doi: 10.5535/arm.2018.42.4.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Ploughman M, Windle V, MacLellan CL, White N, Doré JJ, Corbett D. Brain-derived neurotrophic factor contributes to recovery of skilled reaching after focal ischemia in rats. Stroke. 2009;40:1490–1495. doi: 10.1161/STROKEAHA.108.531806. [DOI] [PubMed] [Google Scholar]
- 69.Qu H, Zhao M, Zhao S, Xiao T, Tang X, Zhao D, Jolkkonen J, Zhao C. Forced limb-use enhances brain plasticity through the cAMP/PKA/CREB signal transduction pathway after stroke in adult rats. Restor Neurol Neurosci. 2014;32:597–609. doi: 10.3233/RNN-130374. [DOI] [PubMed] [Google Scholar]
- 70.Radder B, Prange-Lasonder GB, Kottink AIR, Holmberg J, Sletta K, van Dijk M, Meyer T, Melendez-Calderon A, Buurke JH, Rietman JS. Home rehabilitation supported by a wearable soft-robotic device for improving hand function in older adults: A pilot randomized controlled trial. PLoS One. 2019;14:e0220544. doi: 10.1371/journal.pone.0220544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Rehme AK, Eickhoff SB, Wang LE, Fink GR, Grefkes C. Dynamic causal modeling of cortical activity from the acute to the chronic stage after stroke. Neuroimage. 2011;55:1147–1158. doi: 10.1016/j.neuroimage.2011.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Reitmeir R, Kilic E, Kilic U, Bacigaluppi M, ElAli A, Salani G, Pluchino S, Gassmann M, Hermann DM. Post-acute delivery of erythropoietin induces stroke recovery by promoting perilesional tissue remodelling and contralesional pyramidal tract plasticity. Brain. 2011;134:84–99. doi: 10.1093/brain/awq344. [DOI] [PubMed] [Google Scholar]
- 73.Ridding MC, Rothwell JC. Is there a future for therapeutic use of transcranial magnetic stimulation. Nat Rev Neurosci. 2007;8:559–567. doi: 10.1038/nrn2169. [DOI] [PubMed] [Google Scholar]
- 74.Rothkegel H, Sommer M, Paulus W. Breaks during 5Hz rTMS are essential for facilitatory after effects. Clin Neurophysiol. 2010;121:426–430. doi: 10.1016/j.clinph.2009.11.016. [DOI] [PubMed] [Google Scholar]
- 75.Sampaio-Baptista C, Sanders ZB, Johansen-Berg H. Structural plasticity in adulthood with motor learning and stroke rehabilitation. Annu Rev Neurosci. 2018;41:25–40. doi: 10.1146/annurev-neuro-080317-062015. [DOI] [PubMed] [Google Scholar]
- 76.Sankarasubramanian V, Machado AG, Conforto AB, Potter-Baker KA, Cunningham DA, Varnerin NM, Wang X, Sakaie K, Plow EB. Inhibition versus facilitation of contralesional motor cortices in stroke: Deriving a model to tailor brain stimulation. Clin Neurophysiol. 2017;128:892–902. doi: 10.1016/j.clinph.2017.03.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Schambra HM. Repetitive transcranial magnetic stimulation for upper extremity motor recovery: does it help. Curr Neurol Neurosci Rep. 2018;18:97. doi: 10.1007/s11910-018-0913-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Simis M, Adeyemo BO, Medeiros LF, Miraval F, Gagliardi RJ, Fregni F. Motor cortex-induced plasticity by noninvasive brain stimulation: a comparison between transcranial direct current stimulation and transcranial magnetic stimulation. Neuroreport. 2013;24:973–975. doi: 10.1097/WNR.0000000000000021. [DOI] [PubMed] [Google Scholar]
- 79.Small SL, Buccino G, Solodkin A. Brain repair after stroke--a novel neurological model. Nat Rev Neurol. 2013;9:698–707. doi: 10.1038/nrneurol.2013.222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Sterr A, Dean PJA, Szameitat AJ, Conforto AB, Shen S. Corticospinal tract integrity and lesion volume play different roles in chronic hemiparesis and its improvement through motor practice. Neurorehab Neural Repair. 2014;28:335–343. doi: 10.1177/1545968313510972. [DOI] [PubMed] [Google Scholar]
- 81.Talelli P, Wallace A, Dileone M, Hoad D, Cheeran B, Oliver R, VandenBos M, Hammerbeck U, Barratt K, Gillini C, Musumeci G, Boudrias MH, Cloud GC, Ball J, Marsden JF, Ward NS, Di Lazzaro V, Greenwood RG, Rothwell JC. Theta burst stimulation in the rehabilitation of the upper limb: a semirandomized, placebo-controlled trial in chronic stroke patients. Neurorehab Neural Repair. 2012;26:976–987. doi: 10.1177/1545968312437940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Taub E, Uswatte G, Mark VW, Morris DMM. The learned nonuse phenomenon: implications for rehabilitation. Eura Medicophys. 2006;42:241–256. [PubMed] [Google Scholar]
- 83.Thrane G, Friborg O, Anke A, Indredavik B. A meta-analysis of constraint-induced movement therapy after stroke. J Rehabil Med. 2014;46:833–842. doi: 10.2340/16501977-1859. [DOI] [PubMed] [Google Scholar]
- 84.Tik M, Hoffmann A, Sladky R, Tomova L, Hummer A, Navarro de Lara L, Bukowski H, Pripfl J, Biswal B, Lamm C, Windischberger C. Towards understanding rTMS mechanism of action: Stimulation of the DLPFC causes network-specific increase in functional connectivity. Neuroimage. 2017;162:289–296. doi: 10.1016/j.neuroimage.2017.09.022. [DOI] [PubMed] [Google Scholar]
- 85.Todd G, Rogasch NC, Flavel SC, Ridding MC. Voluntary movement and repetitive transcranial magnetic stimulation over human motor cortex. J Appl Physiol (1985) 2009;106:1593–1603. doi: 10.1152/japplphysiol.91364.2008. [DOI] [PubMed] [Google Scholar]
- 86.Urushidani N, Kinoshita S, Okamoto T, Tamashiro H, Abo M. Low-frequency rTMS and intensive occupational therapy improve upper limb motor function and cortical reorganization assessed by functional near-infrared spectroscopy in a subacute stroke patient. Case Rep Neurol. 2018;10:223–231. doi: 10.1159/000492381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.van Meer MPA, Otte WM, van der Marel K, Nijboer CH, Kavelaars A, van der Sprenkel JWB, Viergever MA, Dijkhuizen RM. Extent of bilateral neuronal network reorganization and functional recovery in relation to stroke severity. J Neurosci. 2012;32:4495–4507. doi: 10.1523/JNEUROSCI.3662-11.2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Wang HY, Crupi D, Liu J, Stucky A, Cruciata G, Di Rocco A, Friedman E, Quartarone A, Ghilardi MF. Repetitive transcranial magnetic stimulation enhances BDNF-TrkB signaling in both brain and lymphocyte. J Neurosci. 2011;31:11044–11054. doi: 10.1523/JNEUROSCI.2125-11.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Wang L, Yu C, Chen H, Qin W, He Y, Fan F, Zhang Y, Wang M, Li K, Zang Y, Woodward TS, Zhu C. Dynamic functional reorganization of the motor execution network after stroke. Brain. 2010;133:1224–1238. doi: 10.1093/brain/awq043. [DOI] [PubMed] [Google Scholar]
- 90.Wenger E, Kühn S, Verrel J, Mårtensson J, Bodammer NC, Lindenberger U, Lövdén M. Repeated structural imaging reveals nonlinear progression of experience-dependent volume changes in human motor cortex. Cereb Cortex. 2017;27:2911–2925. doi: 10.1093/cercor/bhw141. [DOI] [PubMed] [Google Scholar]
- 91.Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, Deruyter F, Eng JJ, Fisher B, Harvey RL, Lang CE, MacKay-Lyons M, Ottenbacher KJ, Pugh S, Reeves MJ, Richards LG, Stiers W, Zorowitz RD. Guidelines for Adult Stroke Rehabilitation and Recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47:e98-e169. doi: 10.1161/STR.0000000000000098. [DOI] [PubMed] [Google Scholar]
- 92.Wu J, Quinlan EB, Dodakian L, McKenzie A, Kathuria N, Zhou RJ, Augsburger R, See J, Le VH, Srinivasan R, Cramer SC. Connectivity measures are robust biomarkers of cortical function and plasticity after stroke. Brain. 2015;138:2359–2369. doi: 10.1093/brain/awv156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Xu T, Yu X, Perlik AJ, Tobin WF, Zweig JA, Tennant K, Jones T, Zuo Y. Rapid formation and selective stabilization of synapses for enduring motor memories. Nature. 2009;462:915–919. doi: 10.1038/nature08389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Yarossi M, Patel J, Qiu Q, Massood S, Fluet G, Merians A, Adamovich S, Tunik E. The association between reorganization of bilateral M1 topography and function in response to early intensive hand focused upper limb rehabilitation following stroke is dependent on ipsilesional corticospinal tract integrity. Front Neurol. 2019;10:258. doi: 10.3389/fneur.2019.00258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Yin Z, Shen Y, Reinhardt JD, Chen CF, Jiang X, Dai W, Zhang W, Machado S, Arias-Carrion O, Yuan TF, Shan C. 5 Hz repetitive transcranial magnetic stimulation with maximum voluntary muscle contraction facilitates cerebral cortex excitability of normal subjects. CNS Neurol Disord Drug Targets. 2015;14:1298–1303. doi: 10.2174/1871527315666151111124216. [DOI] [PubMed] [Google Scholar]
- 96.Youssofzadeh V, Zanotto D, Wong-Lin K, Agrawal SK, Prasad G. Directed functional connectivity in fronto-centroparietal circuit correlates with motor adaptation in gait training. IEEE Trans Neural Syst Rehabil Eng. 2016;24:1265–1275. doi: 10.1109/TNSRE.2016.2551642. [DOI] [PubMed] [Google Scholar]
- 97.Zeiler SR, Krakauer JW. The interaction between training and plasticity in the poststroke brain. Curr Opin Neurol. 2013;26:609–616. doi: 10.1097/WCO.0000000000000025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Zhang L, Xing G, Fan Y, Guo Z, Chen H, Mu Q. Short- and long-term effects of repetitive transcranial magnetic stimulation on upper limb motor function after stroke: a systematic review and meta-analysis. Clin Rehabil. 2017;31:1137–1153. doi: 10.1177/0269215517692386. [DOI] [PubMed] [Google Scholar]
- 99.Zhang ZG, Chopp M. Neurorestorative therapies for stroke: underlying mechanisms and translation to the clinic. Lancet Neurol. 2009;8:491–500. doi: 10.1016/S1474-4422(09)70061-4. [DOI] [PMC free article] [PubMed] [Google Scholar]