

Key Points
Questions
Are there potential risk factors for the development of maculopathy after blood-brain barrier disruption (BBBD) therapy, and how does the maculopathy evolve after completion of systemic treatment?
Findings
In this case series of 68 patients, the number of BBBD treatment sessions, but not age, type of malignant central nervous system tumor, or systemic chemotherapy agent, was associated with maculopathy development. Some patients developed enlarging geographic atrophy in areas of prior pigmentation after completion of BBBD therapy.
Meaning
These findings suggest that patients treated with BBBD therapy can develop dose-dependent maculopathy, which may continue to evolve after completion of systemic therapy.
Abstract
Importance
Blood-brain barrier disruption (BBBD) is a systemic therapy for malignant central nervous system (CNS) tumors that has been linked to poorly understood pigmentary maculopathy.
Objectives
To examine the rate of and risk factors for the development of BBBD-associated maculopathy and to assess whether there can be visually significant progression after completion of systemic therapy.
Design, Setting, and Participants
In this retrospective case series, data from February 1, 2006, through December 31, 2019, were collected from patients treated with osmotic BBBD at a single tertiary referral center who had subsequent ophthalmic evaluation.
Exposures
Treatment with BBBD therapy for any malignant CNS tumor.
Main Outcomes and Measures
Rate and potential risk factors for developing BBBD-associated maculopathy and changes in visual acuity and retinal imaging characteristics after completion of BBBD therapy.
Results
Of 283 patients treated with BBBD and chemotherapy for a CNS malignant neoplasm, 68 (mean [SD] age, 46.0 [17.9] years; 25 [38.5%] female) had an ophthalmic examination after starting systemic therapy. After excluding 3 patients because of bilateral media opacities, pigmentary maculopathy was present in 32 of 65 patients (49.2%) treated with BBBD. The number of BBBD treatment sessions, but not age, CNS malignant cancer type, or systemic chemotherapy agent, was associated with maculopathy development (odds ratio, 1.30; 95% CI, 1.12-1.50; P = .001). After completion of BBBD therapy, progressive enlargement of geographic atrophy occurred in 5 eyes of 3 patients, and choroidal neovascularization developed in 1 eye.
Conclusions and Relevance
In this case series, an association was found between BBBD-related maculopathy and the number of BBBD treatment sessions, suggesting a dose-dependent effect. In some cases, maculopathy progression, including enlargement of geographic atrophy, occurred years after completion of systemic therapy. These findings may have important implications for patient education and ophthalmic monitoring.
This case series examines the rate of and risk factors for developing blood-brain barrier disruption–associated maculopathy.
Introduction
Osmotic blood-brain barrier disruption (BBBD) therapy was first introduced in the early 1980s as a method to increase the penetration of chemotherapeutics into the central nervous system (CNS).1,2 The procedure involves intra-arterial injection of a warmed, hypertonic mannitol solution to disrupt the tight junctions of vascular endothelial cells that form the blood-brain barrier followed by intra-arterial or intravenous chemotherapy. Pigmentary maculopathy was first described in patients with primary CNS lymphoma treated with BBBD and chemotherapy in 1986.3 Subsequent published series4,5,6 of patients with primary CNS lymphoma demonstrated that this particular maculopathy was indeed unique to patients who underwent BBBD therapy.
To our knowledge, there have been no reports of BBBD-associated maculopathy in patients with malignant CNS tumor other than primary CNS lymphoma. Furthermore, the natural history of this maculopathy, particularly after completion of BBBD therapy, is unknown. The current study evaluated the rate of and potential risk factors for maculopathy development in patients with a variety of malignant CNS tumors treated with BBBD therapy. In addition, we evaluated functional and structural changes in eyes with BBBD-associated maculopathy after the completion of systemic therapy.
Methods
Patient Cohort and Statistical Analysis
This case series was reviewed and approved by the institutional review board at Oregon Health & Science University and conducted in compliance with the Declaration of Helsinki.17 The informed consent requirement was waived by the review committee because of the retrospective and low-risk nature of this study. All data were deidentified. The study followed the reporting guideline for case series.
Electronic health records of patients who underwent BBBD therapy at the Oregon Health & Science University, Portland, from February 1, 2006, through December 31, 2019, were collected and reviewed, and those with a documented dilated eye examination or fundus imaging after their BBBD therapy start date were included for further analysis. Data collection included demographic information, CNS tumor diagnosis, and BBBD therapy characteristics, including total number of treatment sessions and associated chemotherapy agents. The CNS tumor diagnoses were categorized into (1) primary CNS lymphoma, (2) glioma, (3) pineal tumor, or (4) other. The presence of a maculopathy was defined as pigmentary changes or retinal pigment epithelium (RPE) atrophy in the macula documented on ophthalmoscopic examination or retinal imaging, including color fundus photographs, fluorescein angiography, or optical coherence tomography (OCT). Binary logistic regression was performed to test potential risk factors for the presence of a maculopathy using SPSS software, version 25.0 (IBM Corp). Two separate logistic regression models were reported because of high multicollinearity between systemic chemotherapy agent and CNS tumor category. Odds ratios (ORs) were reported with 95% CIs. Two-sided P < .05 was considered statistically significant.
Additional analysis to assess for maculopathy evolution after completion of BBBD therapy was performed. Patients who had multiple visits with fundus imaging after their last BBBD therapy date were included. Eyes with intraocular lymphoma were excluded from posttreatment progression analysis. For the purpose of this analysis, the first visit with retinal imaging after cessation of BBBD therapy was defined as the baseline visit. Duration of follow-up was defined as the time from this baseline visit to the last visit with retinal imaging that was available in the electronic health record. Data on visual acuity at baseline and last follow-up as well as all retinal imaging during the follow-up period were collected and analyzed. Of note, there is overlap between the primary CNS lymphoma subgroup and our group’s prior report6 on BBBD maculopathy in primary CNS lymphoma patients. Inclusion of these patients and their additional follow-up data in the present study allows for comparisons between CNS tumor categories and the most complete analysis of posttreatment progression.
BBBD Protocol
The BBBD procedure varied based on CNS tumor category and selected chemotherapeutics but followed a previously described general protocol.7 Briefly, patients received an intra-arterial hypertonic mannitol infusion followed by systemic chemotherapy. Mannitol infusions are typically rotated among 4 sites: the right internal carotid artery, left internal carotid artery, right vertebral artery, and left vertebral artery; however, infusion site was adjusted based on tumor location in some cases. Duration and number of treatments were variable and dependent on relevant study protocol, adverse effects, disease response, and tumor recurrences.
Results
Electronic medical records of 283 patients treated with osmotic BBBD and chemotherapy for a CNS tumor were identified and reviewed. Of these patients, 68 (mean [SD] age, 46.0 [17.9] years; 25 [38.5%] female) had a documented ophthalmoscopic examination and/or retinal imaging after their BBBD therapy start date. Three patients were excluded because the presence of maculopathy was unable to be determined because of dense bilateral vitritis or retinal disease attributable to intraocular lymphoma. Of the remaining 65 patients, 22 (33.8%) had at least 1 retinal imaging modality, 18 (27.7%) had color fundus photographs, 17 (26.2%) had OCT, and 4 (6.2%) had fluorescein angiography. Patients had a mean (SD) of 19.8 (10.9) BBBD treatment sessions. Diagnoses of CNS tumors included primary CNS lymphoma (33 [50.8%]); glioma (21 [32.3%]); pineal tumor (6 [9.2%]); and other (5 [7.7%]), including primitive neuroectodermal tumors and metastatic tumors. Macular pigmentary changes or RPE atrophy were present in 32 patients (49.2%) and occurred in all CNS tumor categories. Of these 32 patients, 19 (59.4%) had at least 1 retinal imaging modality, 16 (50.0%) had color fundus photographs, 15 (46.9%) had OCT, and 4 (13%) had fluorescein angiography. Maculopathy appearance was variable but predominantly involved the foveal and parafoveal regions (Figure 1). Morphologic patterns included (1) central RPE stippling, (2) reticular pigmentary changes, (3) parafoveal bull’s-eye, and (4) parafoveal or subfoveal geographic atrophy (eFigure 1 in the Supplement). Fourteen of the 15 patients (93.3%) with maculopathy and OCT imaging had evidence of focal ellipsoid zone (EZ) disruption.
Figure 1. Near-infrared Imaging in 4 Patients With Maculopathy After Blood-Brain Barrier Disruption Therapy.

Different morphologic appearances are represented: central retinal pigment epithelium (RPE) stippling (A), reticular pigmentary changes (B), parafoveal bull’s-eye (C), and parafoveal or subfoveal geographic atrophy (D).
Geographic atrophy was observed in 8 eyes of 5 patients. These patients had a mean (SD) age of 59.3 (4.4 years) at first BBBD treatment and a mean (SD) of 36.6 (13.2) BBBD treatment sessions. Four had primary CNS lymphoma and 1 had a glioma. The median time from first BBBD treatment to first identification of geographic atrophy was 90.9 months (range, 44.2-131.8 months). Four of the 5 patients had OCT, which showed complete RPE and outer retinal atrophy (cRORA) in all cases and outer retinal tubulations along the edge of RPE atrophy in 3 cases (Figure 2, Figure 3, and eFigure 2 in the Supplement).
Figure 2. Maculopathy Progression After Completion of Blood-Brain Barrier Disruption Therapy in a Patient Treated for a Central Nervous System Glioma.
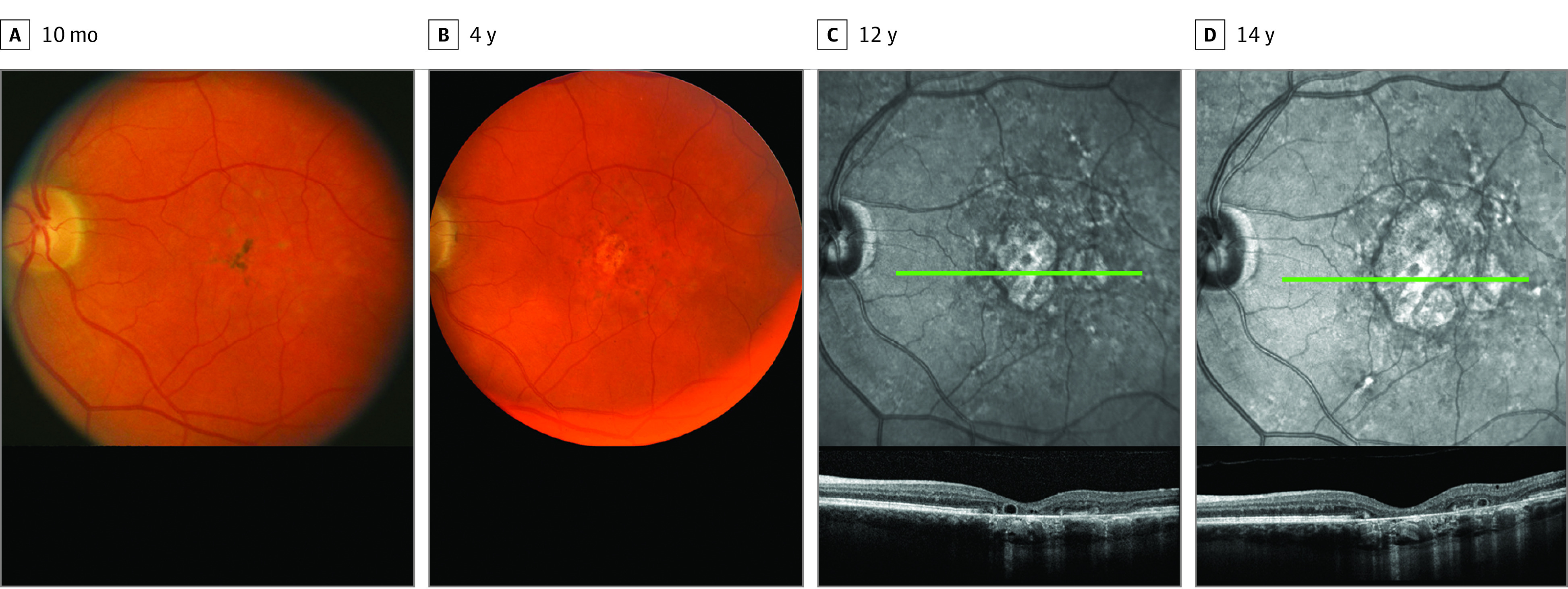
A and B, Progression of maculopathy shown by fundus photography at 10 months and 4 years. C and D, Near-infrared images in the same patient with corresponding optical coherence tomography (OCT) demonstrates expanding complete retinal pigment epithelium and outer retinal atrophy, as well as outer retinal tubulations (green lines designate the location of corresponding B-scan OCT images below) at 12 and 14 years.
Figure 3. Maculopathy Progression After Completion of Blood-Brain Barrier Disruption Therapy in a Patient Treated for Primary Central Nervous System Lymphoma Without Vitreoretinal Lymphoma.
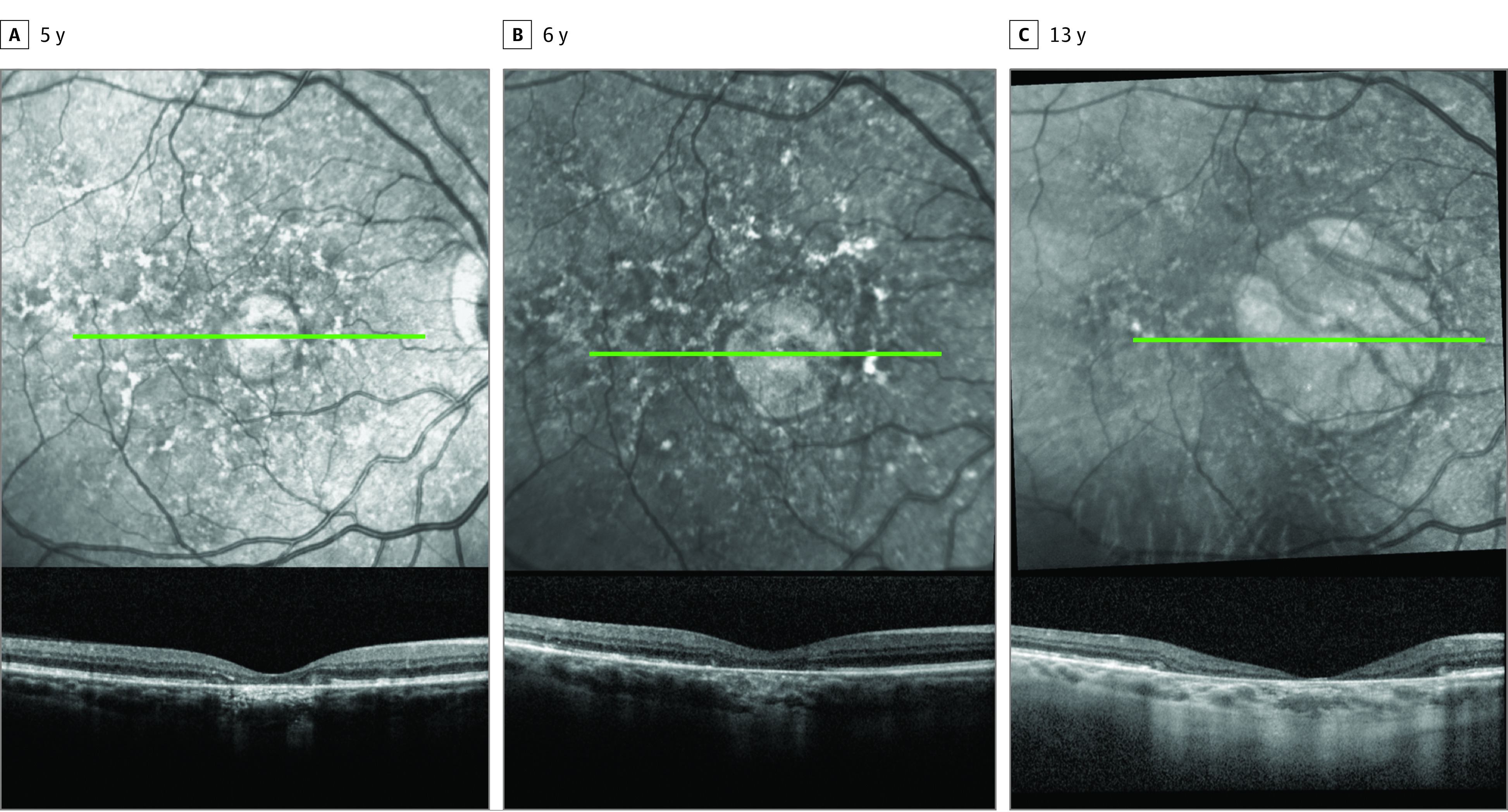
Near-infrared imaging and corresponding optical coherence tomography (OCT) demonstrating progression of complete retinal pigment epithelium and outer retinal atrophy over 13 years (green lines designate location of corresponding B-scan OCT images below).
Analysis of possible risk factors for maculopathy development are reported in Table 1. Because systemic methotrexate was used ubiquitously and exclusively in patients with primary CNS lymphoma, high multicollinearity was found between systemic chemotherapy agent and CNS tumor diagnosis; therefore, 2 separate logistic regression models were reported. The 2 most common systemic chemotherapy agents, methotrexate and carboplatin, were included. The number of BBBD treatment sessions, but not age, sex, presence of intraocular lymphoma (all patients with intraocular lymphoma received some degree of intraocular chemotherapy), systemic chemotherapy agent, or CNS tumor category, was associated with maculopathy development (OR, 1.30; 95% CI, 1.12-1.50; P = .001) (Table 1).
Table 1. Analysis of Risk Factors for Maculopathy in Patients Treated With BBBD Therapya.
| Risk factor | Maculopathy | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| Yes (n = 32) | No (n = 33) | OR (95% CI) | P value | OR (95% CI) | P value | |
| Female | 16 (50.0) | 9 (27.3) | 1.37 (0.30-6.31) | .68 | 1.74 (0.38-8.00) | .48 |
| Age at first treatment, mean (SD), y | 51.6 (16.7) | 40.2 (17.5) | 1.05 (0.99-1.11) | .09 | 1.03 (0.98-1.09) | .22 |
| No. of BBBD treatment sessions | 26.0 | 13.8 | 1.30 (1.12-1.50) | .001b | 1.27 (1.11-1.46) | .001b |
| Intraocular lymphoma | 6 (18.8) | 3 (9.1) | 3.00 (0.25-36.72) | .39 | 2.36 (0.21-27.10) | .49 |
| Systemic chemotherapy | ||||||
| Methotrexate | 21 (65.6) | 12 (36.4) | 1.28 (0.20-8.12) | .79 | NA | NA |
| Carboplatin | 17 (53.1) | 18 (54.5) | 0.21 (0.04-1.09) | .06 | NA | NA |
| Tumor diagnosis | ||||||
| PCNSL | 21 (65.6) | 12 (36.4) | NA | NA | 1 [Reference] | NA |
| CNS glioma | 8 (25.0) | 13 (39.4) | NA | NA | 0.99 (0.15-6.53) | .99 |
| Pineal tumor | 1 (3.1) | 5 (15.2) | NA | NA | 0.33 (0.02-6.67) | .47 |
| Other | 2 (6.3) | 3 (9.1) | NA | NA | 2.72 (0.12-62.87) | .53 |
Abbreviations: BBBD, blood-brain barrier disruption; CNS, central nervous system; NA, not applicable; OR, odds ratio; PCNSL, primary central nervous system lymphoma.
Data are presented as number (percentage) of patients unless otherwise indicated. Two logistic regression models are presented because of high multicollinearity between systemic chemotherapy agent and tumor diagnosis.
P < .05.
Eight patients had 2 or more visits with retinal imaging after their last BBBD therapy date and were included in posttherapy progression analysis (Table 2). Patients had a baseline visit at a median of 6.4 months (range, 0.9-64.2 months) after completion of BBBD therapy and had subsequent follow-up for a median of 54.2 months (range, 24.1-164.8 months). Geographic atrophy was present at the baseline visit in 1 eye, and new geographic atrophy was observed on subsequent follow-up visits in 4 eyes of 3 patients. After the initial appearance of RPE atrophy, definitive enlargement of the atrophy zone was seen on imaging in all 5 eyes (Figure 2, Figure 3, and eFigure 2 in the Supplement). There was a reduction of visual acuity of greater than 2 lines on the Snellen visual acuity chart at final follow-up compared with posttreatment baseline in 4 of 5 eyes with geographic atrophy. One patient developed choroidal neovascularization with subsequent submacular hemorrhage and bilateral geographic atrophy (eFigure 2 in the Supplement). Other findings included consolidation or partial resolution of pigment clumping and evolution of outer retinal or EZ irregularity (eFigure 3 in the Supplement).
Table 2. Maculopathy Disease Course After Completion of BBBD Therapya.
| Patient No. | Tumor diagnosis | Age at first BBBD treatment, y | No. of BBBD sessions | Time from last BBBD session to baseline imaging, mo | Duration of follow-up, mo | Structural analysis | Baseline vision | Final vision | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Right eye | Left eye | Right eye | Left eye | |||||||
| 1 | PCNSL | 60.2 | 48 | 64.2 | 85.3 | CNV with submacular hemorrhage in the left eye, enlarged area of GA in each eye | 20/80 | 20/25 | 20/150 | 20/60 |
| 2 | PCNSL | 58.2 | 39 | 2.6 | 24.1 | Partial pigment resolution | 20/40 | 20/60 | 20/40 | 20/40 |
| 3 | PCNSL | 56.2 | 24 | 0.9 | 41.6 | Partial pigment resolution, increased outer retinal atrophy | 20/20 | 20/20 | 20/25 | 20/25 |
| 4 | PCNSL | 64.4 | 22 | 1.6 | 23.3 | Consolidation of pigment clumping in bull’s-eye pattern, increased EZ disruption | 20/20 | 20/20 | 20/20 | 20/20 |
| 5 | PCNSL | 60.0 | 49 | 1.3 | 79.6 | Enlarged area of GA in the left eye | NA | 20/20 | NA | 20/25 |
| 6 | PCNSL | 62.0 | 24 | 13.1 | 66.7 | Consolidation of pigment clumping in the left eye | NA | 20/20 | NA | 20/25 |
| 7 | Oligodendroglioma grade 3 | 37.6 | 21 | 12.6 | 24.0 | Stable granular pigment clumping | 20/20 | 20/20 | 20/20 | 20/20 |
| 8 | Astrocytoma | 52.4 | 23 | 10.1 | 164.8 | Enlarged area of GA in each eye | 20/30 | 20/25 | 20/60 | 20/60 |
Abbreviations: BBBD, blood-brain barrier disruption; CNV, choroidal neovascularization; EZ, ellipsoid zone; GA, geographic atrophy; NA, not applicable; PCNSL, primary central nervous system lymphoma.
Eyes with intraocular lymphoma were excluded from progression analysis.
Discussion
To our knowledge, this case series describes the first observation of BBBD-associated maculopathy in patients treated for malignant tumors other than primary CNS lymphoma. In addition, these results suggest that BBBD can be associated with late-onset and progressive RPE and outer retinal atrophy. Osmotic disruption of the blood-brain barrier, in combination with chemotherapy, has long been known to be associated with a pigmentary maculopathy in patients with primary CNS lymphoma. Little has been reported on the possible causative factors or the evolution of macular changes after completion of systemic therapy.
In this series, 49.2% of patients who underwent BBBD therapy and ophthalmoscopic examination were found to have macular RPE changes. This rate is similar to those reported in other retrospective studies4,5 that consist exclusively of patients with primary CNS lymphoma. Because BBBD therapy is combined with intra-arterial methotrexate for nearly all patients with primary CNS lymphoma, it has been difficult to determine which is responsible for the observed retinal changes. The findings of macular pigment changes and RPE atrophy in patients treated with BBBD coupled with other chemotherapy agents in different underlying malignant tumors suggest that intra-arterial methotrexate is not the sole culprit. A few findings suggest that direct disruption of the blood-retinal barrier likely plays a key role in the origin of this maculopathy. First, there are many similarities in the development and function of the blood-brain and blood-retinal barriers,8,9,10 and hypertonic mannitol may disrupt the cellular tight junctions of both in similar ways. Second, episodes of subretinal fluid observed shortly after BBBD therapy suggest that there is transient disruption of RPE tight junctions.6,11 Third, the predominant clinical findings in these patients, including pigmentary changes and geographic atrophy, localize to the RPE, which is the cell layer responsible for the outer blood-retinal barrier. Interestingly, outer retinal tubulations, which are tubular structures composed of surviving photoreceptors in areas of RPE and choriocapillaris atrophy, were seen in 3 patients.12 The presence of these structures also suggests that the RPE is the first cellular layer to degenerate. Whether recurrent disruption of the blood-retinal barrier alone or in combination with the local concentration of chemotherapeutics causes the observed maculopathy remains unknown.
On logistic regression analysis, the number of BBBD treatment sessions was the only statistically significant factor associated with maculopathy development. Although treatment plans varied by patient factors and CNS diagnosis, a common protocol included 2 BBBD treatment sessions per month for 12 months. Patients who underwent a higher number of treatment sessions typically have BBBD treatment restarted because of CNS malignant tumor recurrence. Overall, this finding suggests a dose-dependent association or toxicity threshold in regard to maculopathy development.
As seen in this study, the clinical appearance of BBBD-associated maculopathy can have significant variability. Patients may be initially diagnosed with age-related macular degeneration, medication-induced maculopathies, or hereditary macular dystrophies, depending on the appearance of the fundus. Different morphologic patterns, including stippled, reticular, or parafoveal bull’s-eye pigmentary changes, were seen and often best highlighted on near-infrared imaging. Geographic atrophy was also observed in 8 eyes of 5 patients and corresponded to cRORA on OCT. Although patients who developed RPE atrophy had a high number of BBBD treatment sessions (mean [SD], 36.6 [13.2]), this study was not powered to statistically assess this patient subgroup.
Posttreatment changes in patients with 2 or more retinal imaging visits after the completion of BBBD therapy were also analyzed. Of note, patients with intraocular lymphoma were excluded from posttreatment progression analysis to lessen the potential for confounding macular changes, and this analysis was not powered to assess risk factors for posttreatment progression. In some cases, these changes were mild and showed reduction of hyperpigmentation; however, OCT imaging often demonstrated that outer retinal and EZ irregularities persisted. Visual acuity generally remained near baseline in these cases. In other patients, posttherapy maculopathy changes were visually significant. Notably, all 5 patients with geographic RPE atrophy and available follow-up had enlargement of the RPE atrophy zone during the posttreatment period. This finding was best exemplified by the patient who developed new-onset RPE atrophy in areas of prior pigment clumping, first seen in the left eye 4 years after last BBBD therapy and in the right eye 8 years after last BBBD therapy (Figure 2 and eFigure 2 in the Supplement). Additional OCT and near-infrared imaging during the subsequent 10 years demonstrated enlargement of subfoveal cRORA in both eyes and formation of outer retinal tubulations along the expanding border of RPE atrophy in the left eye. For all patients, RPE atrophy was only observed years after the first BBBD therapy session (median, 90.9 months; range, 44.2-131.8 months). Therefore, the total proportion of eyes on a trajectory toward RPE atrophy may be higher than detected in our study because of limited follow-up in some cases.
One patient, highlighted in a previous report,6 had geographic atrophy in one eye and choroidal neovascularization that resulted in submacular hemorrhage in the other eye. Additional follow-up in the present study showed resolution of the unilateral submacular hemorrhage after therapy with intravitreal anti–vascular endothelial growth factor and enlargement of geographic atrophy in both eyes.
In the case of BBBD-associated maculopathy, the underlying mechanism of which remains unknown, the cause of ongoing progression after completion of therapy is unclear. It is possible that there was persistence of a toxic compound, such as the chemotherapeutics used in conjunction with BBBD, after completion of therapy. Alternatively, and possibly more likely, affected eyes were set on a trajectory toward progressive degeneration after reaching some treatment threshold. Enlargement of RPE atrophy is seen in a number of other retinal conditions, such as geographic atrophy in age-related macular degeneration and atrophic creep after laser photocoagulation.13,14 As RPE cells degenerate, cellular signaling or an increased functional burden on neighboring RPE may lead to enlargement of the atrophic zone. Some similarities can also be drawn to retinal conditions in which pigmentary changes and late RPE atrophy develop in the setting of chronic subretinal fluid, such as central serous chorioretinopathy, where dysfunction of the blood-retinal barrier may also occur.15
Limitations
This retrospective study has limitations. Of importance, the lack of uniform follow-up makes it difficult to draw definite conclusions about the timeline of structural changes. The relatively high mortality rate of the conditions treated with BBBD therapy also limits follow-up. Because of the retrospective nature of this study, there was no standardized protocol in regard to retinal imaging. This lack of protocol may have led to missed cases of retinopathy, particularly if localized to the peripheral retina. Similarly, a standardized testing protocol for best-corrected visual acuity was not used. In addition, it is possible that some patients in this study have alternative causes of their maculopathy, including atypical age-related macular degeneration. However, this is unlikely to be the case for a large proportion given the high prevalence and unique retinal features seen in this population. Future studies with standardized imaging and follow-up intervals will be informative. Additional studies with OCT angiography as well as histopathologic correlation may better address the underlying maculopathy mechanism.
Conclusions
This study suggests that BBBD-associated maculopathy is not unique to primary CNS lymphoma; rather, it can be found in patients with a number of different malignant CNS tumors treated with BBBD therapy and chemotherapy. The number of BBBD treatment sessions was associated with maculopathy development, whereas age, systemic chemotherapy agent, and CNS tumor type were not. Evolution of macular changes after completion of BBBD therapy was common. Notably, geographic RPE atrophy was observed years after BBBD, which the present investigation suggests may progress after completion of systemic therapy. Of importance, BBBD can be a life- and function-saving therapy,7,16 and therefore we are not advocating changes to systemic treatment. Rather, these findings may have implications for patient education and ophthalmic monitoring. We propose that patients undergo a baseline ophthalmic examination before the start of BBBD therapy, as well as yearly ophthalmic examinations during and after systemic treatment with retinal imaging if a pigmentary maculopathy or RPE atrophy is detected.
eFigure 1. Multimodal Retinal Imaging of Blood-Brain Barrier Disruption (BBBD) Associated Maculopathy
eFigure 2. Maculopathy Progression and Geographic Atrophy After Completion of Blood-Brain Barrier Disruption (BBBD) Therapy
eFigure 3. Maculopathy Evolution After Completion of Blood-Brain Barrier Disruption (BBBD) Therapy
References
- 1.Neuwelt EA, Frenkel EP, Diehl J, Vu LH, Rapoport S, Hill S. Reversible osmotic blood-brain barrier disruption in humans: implications for the chemotherapy of malignant brain tumors. Neurosurgery. 1980;7(1):44-52. doi: 10.1227/00006123-198007000-00007 [DOI] [PubMed] [Google Scholar]
- 2.Neuwelt EA, Diehl JT, Vu LH, Hill SA, Michael AJ, Frenkel EP. Monitoring of methotrexate delivery in patients with malignant brain tumors after osmotic blood-brain barrier disruption. Ann Intern Med. 1981;94(4 pt 1):449-454. doi: 10.7326/0003-4819-94-4-449 [DOI] [PubMed] [Google Scholar]
- 3.Millay RH, Klein ML, Shults WT, Dahlborg SA, Neuwelt EA. Maculopathy associated with combination chemotherapy and osmotic opening of the blood-brain barrier. Am J Ophthalmol. 1986;102(5):626-632. doi: 10.1016/0002-9394(86)90536-2 [DOI] [PubMed] [Google Scholar]
- 4.Galor A, Ference SJ, Singh AD, et al. Maculopathy as a complication of blood-brain barrier disruption in patients with central nervous system lymphoma. Am J Ophthalmol. 2007;144(1):45-49. doi: 10.1016/j.ajo.2007.03.057 [DOI] [PubMed] [Google Scholar]
- 5.Vicuna-Kojchen J, Frenkel S, Siegal T, Shalom E, Chowers I, Pe’er J. Maculopathy in patients with primary CNS lymphoma treated with chemotherapy in conjunction with blood-brain barrier disruption. Br J Ophthalmol. 2008;92(2):231-235. doi: 10.1136/bjo.2007.130062 [DOI] [PubMed] [Google Scholar]
- 6.Simonett JM, Ambady P, Neuwelt EA, Skalet AH, Lin P. Maculopathy associated with osmotic blood- brain barrier disruption and chemotherapy in patients with primary CNS lymphoma. Ophthalmic Surg Lasers Imaging Retina. 2020;51(5):S5-S12. doi: 10.3928/23258160-20200108-01 [DOI] [PubMed] [Google Scholar]
- 7.Angelov L, Doolittle ND, Kraemer DF, et al. Blood-brain barrier disruption and intra-arterial methotrexate-based therapy for newly diagnosed primary CNS lymphoma: a multi-institutional experience. J Clin Oncol. 2009;27(21):3503-3509. doi: 10.1200/JCO.2008.19.3789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang Y, Cho C, Williams J, et al. Interplay of the Norrin and Wnt7a/Wnt7b signaling systems in blood-brain barrier and blood-retina barrier development and maintenance. Proc Natl Acad Sci U S A. 2018;115(50):E11827-E11836. doi: 10.1073/pnas.1813217115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bosma EK, van Noorden CJF, Schlingemann RO, Klaassen I. The role of plasmalemma vesicle-associated protein in pathological breakdown of blood-brain and blood-retinal barriers: potential novel therapeutic target for cerebral edema and diabetic macular edema. Fluids Barriers CNS. 2018;15(1):24. doi: 10.1186/s12987-018-0109-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhou Y, Wang Y, Tischfield M, et al. Canonical WNT signaling components in vascular development and barrier formation. J Clin Invest. 2014;124(9):3825-3846. doi: 10.1172/JCI76431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pal BP, Palosaari T, Kivelä T. Multimodal imaging during the evolution of blood-brain barrier disruption maculopathy. Retin Cases Brief Rep. 2019;13(1):67-71. doi: 10.1097/ICB.0000000000000535 [DOI] [PubMed] [Google Scholar]
- 12.King BJ, Sapoznik KA, Elsner AE, et al. SD-OCT and adaptive optics imaging of outer retinal tubulation. Optom Vis Sci. 2017;94(3):411-422. doi: 10.1097/OPX.0000000000001031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Keenan TD, Agrón E, Domalpally A, et al. ; AREDS2 Research Group . Progression of geographic atrophy in age-related macular degeneration: AREDS2 report number 16. Ophthalmology. 2018;125(12):1913-1928. doi: 10.1016/j.ophtha.2018.05.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Morgan CM, Schatz H. Atrophic creep of the retinal pigment epithelium after focal macular photocoagulation. Ophthalmology. 1989;96(1):96-103. doi: 10.1016/S0161-6420(89)32924-1 [DOI] [PubMed] [Google Scholar]
- 15.Ferrara D, Mohler KJ, Waheed N, et al. En face enhanced-depth swept-source optical coherence tomography features of chronic central serous chorioretinopathy. Ophthalmology. 2014;121(3):719-726. doi: 10.1016/j.ophtha.2013.10.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McAllister LD, Doolittle ND, Guastadisegni PE, et al. Cognitive outcomes and long-term follow-up results after enhanced chemotherapy delivery for primary central nervous system lymphoma. Neurosurgery. 2000;46(1):51-60. doi: 10.1093/neurosurgery/46.1.51 [DOI] [PubMed] [Google Scholar]
- 17.World Medical Association World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Multimodal Retinal Imaging of Blood-Brain Barrier Disruption (BBBD) Associated Maculopathy
eFigure 2. Maculopathy Progression and Geographic Atrophy After Completion of Blood-Brain Barrier Disruption (BBBD) Therapy
eFigure 3. Maculopathy Evolution After Completion of Blood-Brain Barrier Disruption (BBBD) Therapy