

To the Editor,
Italy has been recently involved in the outbreak of severe interstitial pneumonia associated with the previously unknown Coronavirus SARS-CoV-2 (1,2). Even before the notification of the first autochthonous cases, the SARS-CoV-2 associated syndrome (COVID-19) had raised an intense attention in the public opinion (3), with a counterproductive over-abundance of mixed quality information. As even Italian healthcare workers (HCWs) were not spared by subsequent misunderstandings and knowledge gaps during the previous influenza pandemic of 2009 (4), we performed a web-based survey (Google® Modules), specifically aimed to characterize knowledge status and risk perceptions in a sample from participating to 6 Facebook discussion groups (181,684 total unique members at the time of the study). The questionnaire was made available between February 1st and 7th, 2020, i.e. around 2 weeks before the first COVID-19 was officially diagnosed in Italian residents.
Overall, the sampled population included 2106 respondents (Table 1), and 39.3% were HCWs. Even though HCWs were more likely to exhibit a better understanding of SARS-CoV-2/COVID-19 related issues (aOR 2.195, 95%CI 1.809 to 2.664), they were not exempt for misunderstandings, particularly on actual incidence and lethality of COVID-19. Interestingly, most of respondents were aware of the main clinical features of COVID-19, with HCWs more frequently acknowledging that the COVID-19 may run pauci- or even asymptomatic (86.3% vs. 79.1%), resembling an Influenza-Like Illness (i.e. fever, cough, headache, etc; Figure 1), with a potential latency up to 14 days (85.9% vs. 80.3%), eventually spreading by droplets (98.5% vs. 92.7%) rather through running water (92.3% vs· 79.8%), or blood/body fluids (88.0% vs. 70.4%). As a matter of fact, very few among the respondents were aware that SARS-CoV-2 has non-respiratory involvement, particularly of conjunctiva, gastrointestinal tract, as well as neurological ones. In this regard, HCWs were more likely to recognize some of the non-respiratory symptoms than non-HCWs (more specifically: articular pain, headache and general malaise).
Table 1.
Knowledge and attitudes on COVID-19/SARS-CoV-2 infection in 2106 subjects participating to a web survey (Italy; February 2020) by occupational status, i.e. healthcare workers (HCW) vs. non-HCW. Comparisons were initially performed by means of chi squared test; variables that in univariate analysis were associated with HCW status with p value < 0.05 were included in a binary logistic regression model. The association was then reported as adjusted Odds Ratios (aOR) with their correspondent 95% confidence intervals (95%CI) (Notes: * = statement on the basis of the understanding of COVID-19/SARS-CoV-2 infection at January 30th, 2020)
|
TOTAL (No. 2106) |
HCW (No./827, %) |
Non HCW (No./1279, %) |
P value | aOR (95%CI) | |
| Age < 40 years | 1288, 61.2% | 479, 58.1% | 809, 63.3% | < 0.001 | 0.895 (0.736; 1.087) |
| Male Gender | 579, 27.2% | 185, 22.4% | 388, 30.3% | < 0.001 | 1.562 (1.259; 1.940) |
| Knowledge status (TRUE vs. FALSE) | 796, 37.8% | 413, 49.9% | 365, 28.5% | < 0.001 | 2.195 (1.809; 2.664) |
| 1. Worldwide official diagnoses of COVID-19 accounted to 1000 to 10000 cases (TRUE)* | 1062, 50.4% | 408, 49.3% | 654, 51.1% | 0.420 | - |
| 2. Lethality of COVID-19 is estimated to be 1 to 2 % of symptomatic cases (TRUE)* | 481, 22.8% | 201, 24.3% | 280, 21.9% | 0.198 | - |
| 3. All infected people become sick (FALSE) | 1486, 70.6% | 634, 76.7% | 852, 66.6% | < 0.001 | - |
| 4. Etiologic agent of COVID-19 is a virus somewhat similar to SARS virus (TRUE) | 1248, 59.3% | 565, 68.3% | 683, 53.4% | < 0.001 | - |
| 5. SARS-CoV-2is suspected to mainly spread through contaminated running water (FALSE) | 1784, 84.7% | 763, 92.3% | 1021, 79.8% | < 0.001 | - |
| 6. SARS-CoV-2is suspected to mainly spread through cough / droplets (TRUE) | 2000, 95.0% | 815, 98.5% | 1185, 92.7% | < 0.001 | - |
| 7. SARS-CoV-2is suspected to mainly spread through contaminated blood (FALSE) | 1628, 77.3% | 728, 88.0% | 900, 70.4% | < 0.001 | - |
| 8. A vaccine against SARS-CoV-2is available and effective (FALSE) | 1931, 91.7% | 787, 95.2% | 1144, 89.4% | < 0.001 | - |
| 9. All people infected by SARS-CoV-2exhibit some symptoms (FALSE) | 1726, 82.0% | 714, 86.3% | 1012, 79.1% | < 0.001 | - |
| 10. A specific treatment for COVID-19 is available and effective (FALSE) | 1276, 60.6% | 585, 70.7% | 691, 54.0% | < 0.001 | - |
| 11. COVID-19 is causing an outbreak in mainland China (TRUE) | 1644, 78.1% | 687, 83.1% | 957, 74.8% | < 0.001 | - |
| 12. Around 80% of emerging infectious diseases are zoonoses (TRUE) | 910, 43.2% | 421, 50.9% | 489, 38.2% | < 0.001 | - |
| 13. SARS-CoV-2 is suspected to be transmitted to humans by animals (TRUE) | 968, 46.0% | 400, 48.4% | 568, 44.4% | 0.075 | - |
| 14. Meat of slaughtered animals may be associated with human transmission of SARS-CoV-2 (TRUE) | 494, 23.5% | 214, 25.9% | 280, 21.9% | 0.035 | - |
| 15. Latency of COVID-19 may reach 14 days (TRUE) | 1737, 82.5% | 710, 85.9% | 1027, 80.3% | < 0.001 | - |
| Acknowledging COVID-19 as a severe disease (yes vs. no) | 1305, 62.0% | 525, 63.5% | 780, 61.0% | 0.249 | - |
| Concern for being infected by SARS-CoV-2 in Italy (high vs. low) | 168, 8.0% | 72, 8.7% | 96, 7.5% | 0.321 | - |
| Concern for SARS-CoV-2 infection in international travelers (high vs. low) | 561, 26.7% | 222, 26.8% | 339, 26.5% | 0.864 | - |
| Acknowledged risk factors for emerging infectious diseases like SARS-CoV-2 | |||||
| … international travels | 1018, 48.4% | 413, 49.9% | 605, 47.3% | 0.237 | - |
| … climate change | 236, 11.2% | 108, 13.1% | 128, 10.0% | 0.030 | 1.413 (1.050; 1.901) |
| … migratory crisis | 567, 26.9% | 244, 29.5% | 323, 25.3% | 0.032 | 1.076 (0.869; 1.332) |
| … scarce foresight of competent authorities | 994, 47.2% | 379, 45.8% | 615, 48.1% | 0.311 | - |
| … inappropriate food hygiene standards in developing countries | 1389, 65.9% | 576, 69.6% | 813, 63.6% | 0.004 | 1.104 (0.884; 1.379) |
| … economic underdevelopment | 937, 44.5% | 410, 49.6% | 527, 41.2% | < 0.001 | 1.187 (0.962; 1.464) |
| Acknowledged preventive measures for emerging infectious diseases like SARS-CoV-2019 | |||||
| … regularly washing hands | 1938, 92.0% | 796, 96.3% | 1142, 89.3% | < 0.001 | 2.296 (1.507; 3.496) |
| … wearing a respiratory mask (i.e. surgical mask) | 154, 7.3% | 61, 7.4% | 93, 7.3% | 0.928 | - |
| … wearing a respiratory mask (i.e. filtering) | 1343, 63.8% | 623, 75.3% | 720, 56.3% | < 0.001 | 2.167 (1.768; 2.657) |
| … preventive use of antibiotics | 59, 2.8% | 23, 2.8% | 36, 2.8% | 1.000 | - |
| … preventive use of antiviral drugs | 167, 7.9% | 51, 6.2% | 116, 9.1% | 0.016 | 0.632 (0.439; 0.910) |
| Information sources | - | ||||
| Healthcare professionals | 1012, 48.1% | 405, 49.0% | 607, 47.5% | 0.497 | - |
| New Media (i.e. Social media, Wikis, blogs, web sites, etc.) | 1445, 68.6% | 550, 66.5% | 895, 70.0% | 0.094 | - |
| Conventional media (i.e. TV, radio, newspapers) | 1363, 64.7% | 514, 62.2% | 849, 66.4% | 0.047 | 0.685 (0.560; 0.839) |
Figure 1.
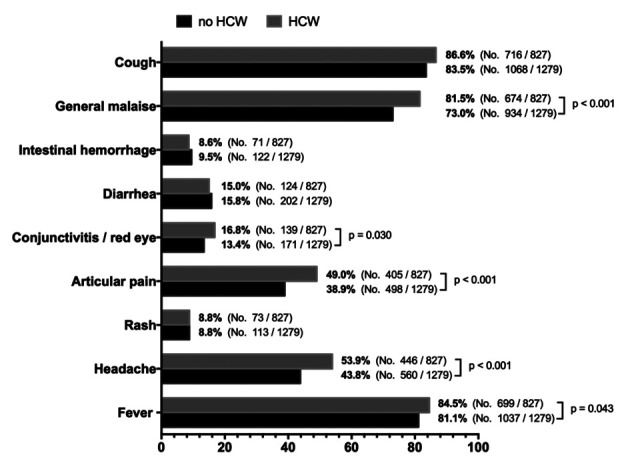
Recall of alleged symptoms for SARS-CoV-2 infection among study participants, broken down by being or not a healthcare worker (HCW). Univariate comparisons were performed by means of chi squared test (only p value < 0.05 are reported)
Retrospectively, the assessment of preventive measures and risk perception appears somewhat worrisome. For instance, while HCWs were more likely to acknowledge as an appropriate preventive measure wearing a filtering mask (i.e. N95/FFP2/3 mask; aOR 2.296, 95%CI 1.507 to 3.946), around ¼ of HCWs failed to recognize the importance of such personal protective equipment, while 7.4% felt as appropriate the wearing of a surgical mask.
Moreover, not only COVID-19 was appropriately acknowledged as a severe disease by only 62.0% of respondents, with no differences between HCWs and non-HCWs, but an even smaller share (i.e. 8.0%) reported any concern for being infected by SARS-CoV-2 in Italy. In fact, at the time of the survey SARS-CoV-2 was more properly associated with international travelers (26.7%).
Our results are therefore of certain interests for several reasons. First at all, early epidemiological reports on the Italian cases of COVID-19 hint towards some failures in the initial management of incident cases (5-6). In fact, in our survey a large share of respondents substantially overlooked the risk to interact with SARS-CoV-2 positive subjects, that was otherwise perceived as a not-so-severe disease (i.e. “nothing more than a seasonal flu”, as often described in some social media) (7). Moreover, around a 1/3 of HCWs participating to the study presumptively did not use proper personal protective equipment for the airways interacting with possible COVID-19 cases, either underestimating the infection risk or being unable to recognize early symptoms. Actually, the base of evidence shared by participants at the time of the study substantially ignored that COVID-19 may be characterized by dermatologic and gastro-intestinal symptoms (8-9). As most of infections may be actually pauci- or asymptomatic, such early exposure in the healthcare settings may have contributed to the quick spreading of SARS-CoV-2 epidemic in Northern Italy.
Therefore, despite the intrinsic limits of a convenience sampling, web-based survey (10), our study stresses the importance to improve the overall quality of information on COVID-19 conveyed not only in HCWs, but also in the general population. Moreover, our data may contribute to clarify the early stages of SARS-CoV-2 pandemic in Italy.
The facts, conclusions, and opinions stated in the article represent the authors’ research, conclusions, and opinions and are believed to be substantiated, accurate, valid, and reliable. However, as this article includes the results of personal researches of the Authors, presenting correspondent, personal conclusions and opinions, parent employers are not forced in any way to endorse or share its content and its potential implications.
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. Jama. 2020;323(11):1061–1069. doi: 10.1001/jama.2020.1585. doi: 10.1001/jama.2020.1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020 doi: 10.1056/NEJMoa2001017. NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi: 10.1016/S0140-6736(20)30185-9. doi: 10.1016/S0140-6736(20)30185-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Prati G, Pietrantoni L, Zani B. Compliance with recommendations for pandemic influenza H1N1 2009: The role of trust and personal beliefs. Health Educ Res. 2011;26:761–9. doi: 10.1093/her/cyr035. doi: 10.1093/her/cyr035. [DOI] [PubMed] [Google Scholar]
- 5.Guzzetta G, Poletti P, Ajelli M, Trentini F, Marziano V, Cereda D, Tirani M, Diurno G, Bodina A, Barone A, Crottogini L, Gramegna M, Melegaro A, Merler S. Potential Short-Term Outcome of an Uncontrolled COVID-19 Epidemic in Lombardy, Italy, February to March 2020. Euro Surveill. 2020;25(12):2000293. doi: 10.2807/1560-7917.ES.2020.25.12.2000293. doi: 10.2807/1560-7917.ES.2020.25.12.2000293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Signorelli C, Odone A, Gianfredi V, et al. The spread of COVID-19 in six western metropolitan regions: a false myth on the excess of mortality in Lombardy and the defense of the city of Milan. Acta Biomed. 2020;91 doi: 10.23750/abm.v91i2.9600. epub ahead of print https://doi.org/10.23750/abm.v91i2.9579 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Motta Zanin G, Gentile E, Parisi A, Spasiano D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Health. 2020;17:3024. doi: 10.3390/ijerph17093024. doi:10.3390/ijerph17093024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Riccò M, Ferraro P, Gualerzi G, et al. Point-of-Care diagnostic of SARS-CoV-2: knowledge, attitudes, and perceptions (KAP) of medical workforce in Italy. Acta Biomed. 2020;91 doi: 10.23750/abm.v91i2.9573. epub ahead of print https://doi.org/10.23750/abm.v91i2.9573 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stratton SJ. Data sampling strategies for disaster and emergency health research. Prehosp Disaster Med. 2019;34:227–9. doi: 10.1017/S1049023X19004412. doi: 10.1017/S1049023X19004412. [DOI] [PubMed] [Google Scholar]