

Abstract
Background.
Valid assessment of adolescent substance use is important in both research and clinical applications. However, the optimal approach to assessing adolescent use remains controversial, particularly with regard to the use of parent-reported measures.
Methods.
Using a systematic review of existing literature, we sought to evaluate the utility of parent measures of adolescent alcohol and cannabis use by examining their correspondence with self-report measures. Furthermore, we investigated study-related variables that may be associated with differing levels of parent-child correspondence. Relevant articles were identified using a systematic search across multiple databases.
Results.
The review revealed generally poor agreement between parent and adolescent reports of alcohol and cannabis use. Parents consistently underestimated use and problems associated with use when compared to adolescents. Community-based (versus clinical) samples, reporting regarding alcohol (versus cannabis), and reporting problems associated with use (versus reports of use/nonuse) were each associated with lower levels of parent-child agreement.
Conclusions.
Recommendations for the optimal use of parent measures of adolescent substance use are provided.
Keywords: adolescence, alcohol use, cannabis use, assessment, self report, parent report, agreement
Introduction
The prevalence of adolescent substance use continues to be a public health concern. Among high school seniors in the United States, 39% report using an illicit drug in the past year, and 34% report having been drunk in the past year1. Despite numerous efforts to reduce problematic use, the trend of daily cannabis use in high school seniors has largely remained steady at around 6% for the past 20 years.1 In addition to a range of potential negative consequences of adolescent substance use involvement,2–4 the likelihood of developing a substance use disorder is significantly higher when use occurs during the teenage years.5,6
Because of the high prevalence and serious consequences of use, early detection of substance use behaviors among youth is critical. However, there remains considerable disagreement within the field about which approaches to assessing adolescent substance use may be optimal. Some researchers point to the value of biological measures, noting their objectivity and reliability.7 Others note that these tools are often not practical in clinical or research contexts and stress that self-report measures have maximal efficiency while retaining acceptable validity.8,9 The value of other collateral measures of substance use such as parent report is also controversial. There has long been general support for the collection of corroborative information from multiple reporters regarding adolescent psychopathology, including substance abuse.10,11 Whereas some studies support parent report as having strong convergent validity with youth report and biological measures,12 other studies note a relatively weak correspondence of parent report with other assessment strategies.10 The collection of parent-reported data is also associated with additional time and expense. Because of these mixed opinions within the field, we sought to evaluate further the utility of parent-reported data by examining its correspondence with self-report measures in existing literature.
Multi-informant Approaches
Existing literature is generally supportive of multi-informant approaches to evaluating children’s mental health.10,11 The collection of data from multiple reporters provides information about youth functioning across contexts and may help address concerns about under- or overreporting of symptoms.11 However, the level correspondence of reports from multiple informants is variable and appears to be influenced by several factors. Meta-analytic analyses reveal low to moderate correlations among youth and parent reports of psychopathology.11 Levels of agreement between youth and parents are found to be highest for those behaviors that are externally visible, such as oppositional behavior or aggression, and lowest for internal states like symptoms of depression and anxiety.13 Furthermore, levels of agreement between informants regarding socioemotional problems tends to be higher for younger children than older children and adolescents.13 Notably, the extent of the discrepancy present between parent and child informants may be in itself predictive of problems behaviors, including substance use.14,15
The literature examining cross-informant correspondence in child psychopathology has devoted considerably less attention to the assessment of substance use. Several features of adolescent substance use make it unique from other aspects of psychopathology in regards to correspondence. While some aspects of child and adolescent psychopathology are readily observable and may actively involve parents or other family members (e.g., oppositional behaviors), adolescents may take pains to hide or minimize their substance use from parents. The presence of such covert behaviors is associated with more limited parental knowledge and lower agreement with self-report measures.10,15 Furthermore, substance use and associated disorders typically have a later age of onset than externalizing disorders such as ADHD or Oppositional Defiant Disorder.16 Because adolescence is often associated with lower levels of correspondence between informants across a range of socioemotional problems when compared to childhood, substance use behaviors noted during adolescence may also be associated with lower correspondence when compared to other types of psychopathology that present earlier in development.
Assessment Techniques
Self-report is a nearly universal method in clinical practice and research studies to obtain substance use information from adolescents. Previous research generally supports the validity of adolescent self-report as an assessment strategy. Adolescent self-reports demonstrate good temporal stability and low rates of excessive response biases consistent with severely exaggerating or minimizing their use.9 Furthermore, a relatively high proportion of adolescents acknowledge drug use through self-report when a biological test was negative.7,17 However, some studies do raise questions about issues with relying exclusively on self-reported data. Of note is Magura’s analysis of the congruence between self-report and urinalysis, which suggests that data from self-report-based epidemiological surveys are producing erroneously low estimates of the prevalence rates of illicit drug use.18 Furthermore, the validity of self-reported data when compared to biological screening tools may vary depending on the substance, with drugs such as cocaine tending to be underreported more often than marijuana and opiates.7 These findings raise the question of whether it is necessary to corroborate self-report and how to best do so.
A common approach to corroborate self-report is via biological assays such as urine, blood, saliva, or hair.19,20 However, the use of biological assays is not without limitations. These tests can be expensive, and they are drug and time sensitive.7,19 It is often not practical to test for all potential drugs of abuse, and most drugs are not detectable through urine or saliva based-tests without relatively recent use. Thus, these tests may be most effective for frequent users of known drug types.
Another way to corroborate adolescent self-report is through collateral information from parents or caretakers (hereafter referred to as parents). The success of parent report as a source of valid data on adolescent substance use has received variable reviews in the research literature. Adolescents have reported more use than their parents’ reports in some studies, potentially reflecting a lack of parental knowledge, adolescent overreporting, or parental underreporting.21,22 Other researchers have found a relatively high degree of adolescent-parent congruence,17,23 even exceeding the level of agreement observed between self-report and bio-assays.7,12 Parent report may be a valuable component to the assessment process when an uncooperative adolescent is being clinically evaluated for a referral to treatment.24,25 Notably, there has been limited systematic evaluation of the corroborative value of parent-reported drug use data across studies.
There are a wide variety of parent-report assessment instruments that have been developed, including structured and semi-structured interviews and self-administered questionnaires. Yet evaluating the relative utility of these measures is challenging. For self-report data, there is evidence that the use of self-administered methods, such as paper-based questionnaires, may promote increased validity when compared to interview methods.26 However, there has been little investigation into this issue with parent-reported data.
Primary Aims
Using adolescent self-report as the most common standard of measurement in the field, we conducted a systematic review evaluating the extent to which parent-report measures generally corroborate adolescent self-report as well as variables that may impact the level of agreement with adolescent self-report. We first sought to evaluate study-level variables such as type of substance, assessment method (i.e., interview versus self-report), assessment type (i.e., assessment versus screening), sample (i.e., clinical versus community), and type of outcome (i.e., use or nonuse and frequency of use versus drug use problems and diagnostic status) for their association with parent-child agreement. Second, when available, we planned to examine the relative agreement of parent and adolescent self-report with biological measures in order to further evaluate the validity of each reporting strategy. Third, we planned to evaluate trends in other adolescent and parent variables (i.e., adolescent age and gender, adolescent and family risk factors) evaluated within studies for their association with variability in parent-adolescent agreement.
Methods
Search Strategy
We identified relevant articles by searching PubMed, PsycINFO, and Google Scholar without any year limit. Our search was last updated in December of 2018. Keywords used in the search included: parent report, child report, self report, agreement, multi-informant, concordance, parent awareness, parent knowledge, drug use, drug abuse, drug misuse, substance use, substance abuse, substance misuse, cannabis, alcohol, cannabis, assessment, and parent assessment tools. We also included the names of commonly used adolescent instruments. Reference sections of identified articles were searched for applicable citations as well. Figure 1 details the article search and review process using a PRISMA figure.27
Figure 1.
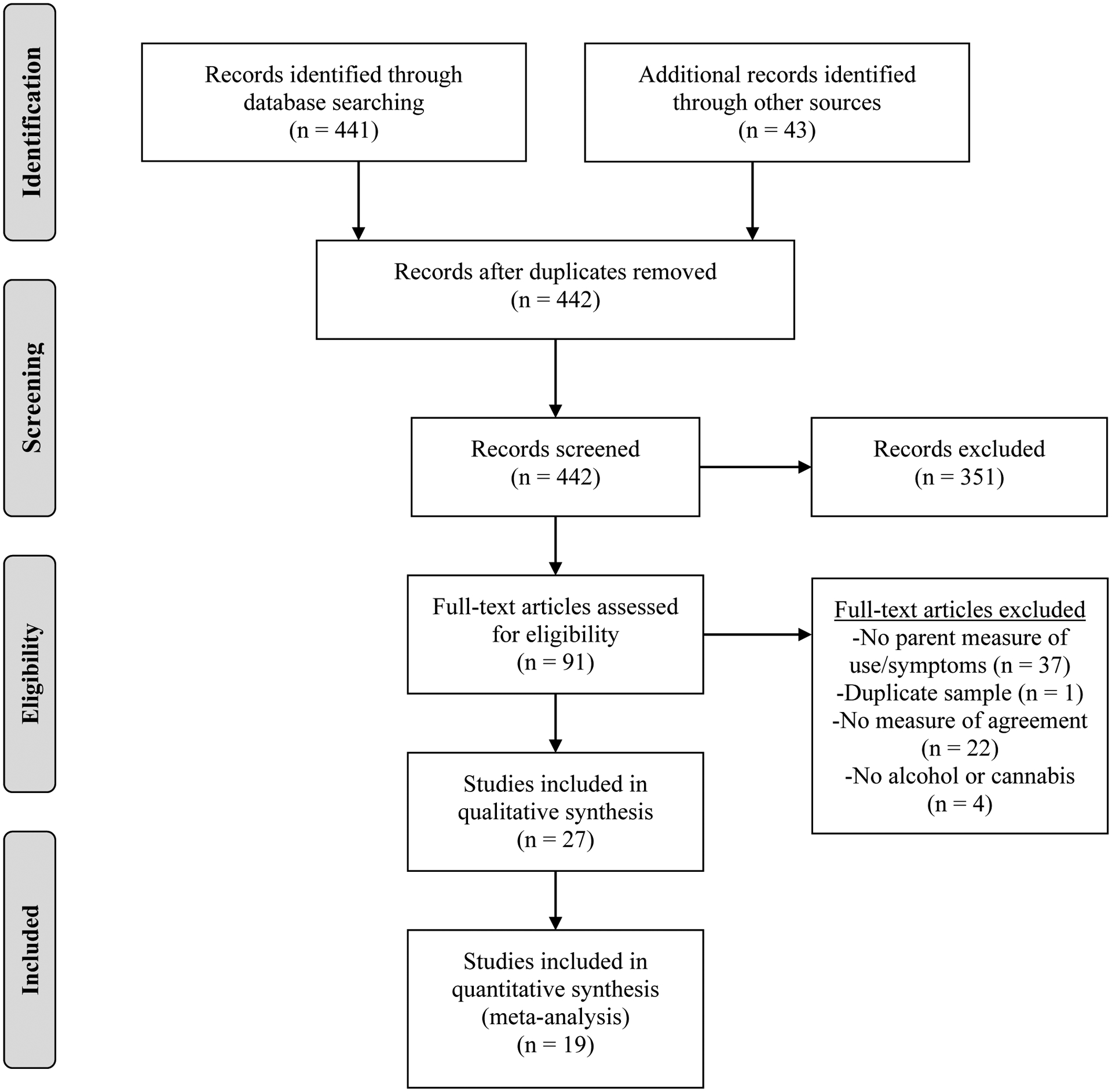
PRISMA systematic review flow diagram of literature search conducted in December of 2018.27
Inclusion and Exclusion Criteria
Published manuscripts were included in our review if they included empirical data directly pertaining to the agreement between parent and adolescent report concerning the adolescent’s substance use behaviors (e.g., onset, frequency, diagnostic symptoms, other problems). The focus of the present review was on alcohol and cannabis use due to these being the most commonly investigated in the identified articles. While the use of additional sources of information such as biological measures of drug use was not a requirement for inclusion in the review, we present these data when they are available. We excluded studies that 1) only examined reporter agreement regarding risk and protective factors, expectancies, and treatment utilization; 2) utilized the same samples as previously published manuscripts without additional data; 3) presented only descriptive statistics such as the percentage of adolescents or parents endorsing adolescent use without providing a statistical measure of concordance or agreement between reporters (i.e., percent agreement, sensitivity/specificity, intraclass correlation [ICC], kappa); and 4) only examined concordance for substances other than alcohol or cannabis. Whereas some studies presented data relevant to other substances (e.g., tobacco, opiates, hallucinogens, etc.), we considered space constraints in limiting our review to alcohol and cannabis. However, we do present data relevant to other drugs in several cases in which alcohol and/or cannabis use was combined with other drugs in a single variable.
Data Extraction and Analysis
Our search resulted in 27 articles published between 1987 and 2017. Table 1 provides detailed statistics for parent and child agreement regarding alcohol and cannabis. The table is organized by parent assessment instrument. Reporter agreement is presented using the statistics available in the published article and include percentage agreement, correlations (intraclass and Pearson), kappa scores, and sensitivity and specificity indices. While some caution is warranted in applying similar interpretive guidelines across all studies, we interpret kappa measures of interreporter agreement using Cicchetti and Sparrow’s criteria, which state that reliability coefficients below .40 may be considered poor agreement; between .40 and .59 fair agreement; between .60 and .74 good agreement; and between .75 and 1.00 excellent agreement.28 Intraclass correlation (ICC) coefficients were interpreted using guidelines from Koo and Li with values less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.90 reflecting poor, fair, good, and excellent agreement respectively.29
Table 1.
Studies on the Concordance of Parent and Adolescent Reports on Adolescent Alcohol and Cannabis Use
| Citation | N1 and Sample2 | Parent-Adolescent Concordance Data |
|---|---|---|
| Instrument: Diagnostic Interview Schedule for Children- Parent Version (DISC-P) | ||
| Chung, Colby, O’Leary, Barnett, & Monti (2003) | N: 272 Sample: Adolescents who presented to an emergency department for non-substance-related injury |
Kappa Scores of Parent and Adolescent Agreement on Substance Use Disorders Alcohol use disorder= 0.17 Cannabis use disorder= 0.26 |
| Dillon, Turner, Robbins, & Szapocznik (2005) | N: 190 Sample: Adolescents identified through involvement in juvenile justice or community-based services who met criteria for a substance use disorder |
Pearson’s Correlations Between Adolescent and Parent Report on Adolescent Abuse/Dependence Symptoms Baseline cannabis: r(181)= 0.32** 18 months cannabis: r(102)= 0.23* |
| Kramer, Robbins, Phillips, Miller, & Burns (2003) | N: 227 Sample: Adolescents who presented for outpatient mental health treatment |
Kappa Scores of Parent and Adolescent Agreement of Substance Abuse/Dependence Alcohol abuse/dependence= 0.36 Cannabis abuse/dependence= 0.45 |
| Instrument: Global Appraisal of Individual Needs (GAIN) | ||
| Dennis et al. (2002) | N: 600 Sample: Adolescents who presented for outpatient drug treatment |
Kappa Scores of Parent and Child Report of Use in Past 90 days at Intake, 3 Month, and 6 Month Intake Alcohol= 0.72 Intake Cannabis= 0.92 3 Month Alcohol= 0.86 3 Month Cannabis= 0.86 6 Month Alcohol= 0.89 6 Month Cannabis= 0.86 |
| Godley, Godley, Dennis, Funk, & Passetti (2002) | N: 114 Sample: Adolescents admitted to a residential drug treatment program |
Kappa Scores and Percent Agreement of Parent and Child Report of Use in Past 90 Days Intake Alcohol= 0.69, 89.7% Intake Cannabis= 0.92, 98.3% 3 Month Alcohol= 0.86, 93.1% 3 Month Cannabis= 0.86, 93.1% |
| Instrument: Semi-Structured Assessment for the Genetics of Alcoholism (C-SSAGA) | ||
| Fisher et al. (2006) | N: 591 Sample: Mix of adolescent community controls and adolescents with a family history of alcohol dependence |
Kappa Scores of Parent and Adolescent Report of Substance Use with Adolescent as Standard Alcohol use= 0.41 Cannabis use= 0.51 Alcohol intoxication= 0.38 Alcohol abuse or dependence= 0.37 Cannabis abuse or dependence= 0.35 |
| Instrument: Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS) | ||
| Cantwell, Lewinsohn, Rohde, & Seeley (1997) | N: 281 Sample: Community sample of adolescents |
Kappa Scores of Parent and Adolescent Diagnostic Agreement Alcohol Use Disorder= 0.19 Other Substance Use Disorders= 0.41 |
| Delaney-Black et al. (2010) | N: 432 Sample: High-risk community sample of adolescents |
Percentage Agreement between Adolescents and Parents With adolescent-reported marijuana use: 39% of parents reported adolescent use With parent-reported adolescent marijuana use: 69% of adolescents reported use |
| Gignac et al. (2005) | N: 22 Sample: Adolescents with ADHD diagnoses and community-based controls |
Sensitivity and Specificity of Self-Report of 30-day Cannabis Use with Urinalysis as Standard Sensitivity= 91% Specificity= 87% Sensitivity and Specificity of Parent Report of Child’s Cannabis Abuse or Dependence with Self-Report as Standard Sensitivity= 61% Specificity= 93% |
| Jones et al. (2017) | N: 5214 Sample: Community sample of adolescents |
Kappa Scores of Parent and Adolescent Report of Substance Use Alcohol= 0.30 Cannabis= 0.41 |
| O’Donnell et al. (1998) | N: 260 Sample: Youth with ADHD and community-based controls |
Kappa Scores of Parent and Adolescent Report of Substance Use Alcohol Abuse kappa= 0.22 Drug (including cannabis) abuse kappa= 0.26 Alcohol dependence kappa= 0.56 Drug (including cannabis) dependence kappa= 0.36 |
| Weissman et al. (1987) | N: 175 Sample: Children of depressed parents as well as community controls |
Kappa Scores of Parent and Child Diagnostic Agreement Alcohol Use Disorders= 0.10 Any Substance Use Disorder= 0.07 |
| Instrument: Teen Addiction Severity Index (T-ASI) | ||
| Burleson & Kaminer (2006) | N: 88 Sample: Adolescents referred for outpatient treatment for substance use disorders |
Pearson Correlations between Parent-and Adolescent-Reported Measures and Urinalysis at 3- and 9-months Use/Nonuse Item: Adolescent and Parent Report Alcohol= 0.46** (3 Month); 0.42** (9 Month) Cannabis= 0.49** (3 Month); 0.55** (9 Month) T-ASI Scores: Adolescent and Parent Report Alcohol= 0.51*** (3 Month); 0.35** (9 Month) Other substances= 0.45** (3 Month); 0.57*** (9 Month) Use/Nonuse Item Adolescent Report and Urinalysis Cannabis= 0.49** (3 Month); 0.64*** (9 Month) Adolescent T-ASI score and Urinalysis 3 Month= 0.52***; 9 Month = 0.32* Use/Nonuse item Parent Report and Urinalysis 3 Month= 0.28*; 9 Month= 0.43** Parent T-ASI score and Urinalysis 3 Month= 0.33**; 9 Month= 0.31* |
| Instrument: Timeline Follow-back Interview (TLFB) | ||
| Donohue et al. (2004) | N = 188 Sample: Adolescents with both substance use disorder and conduct disorder diagnoses |
Intraclass Correlations Between Parent and Youth Reports of Youths’ Days of Using Per Month for the 6 Months Before Intake (Listed From 1 Month Prior to 6 Months Prior to Intake) Alcohol: 1 Month= 0.43; 2 Months= 0.45; 3 Months= 0.42; 4 Months= 0.45; 5 Months= 0.34; 6 Months= 0.25 Cannabis: 1 Month= 0.48; 2 Months= 0.39; 3 Months= 0.48; 4 Months= 0.38; 5 Months= 0.40; 6 Months = 0.40 |
| Donohue, Hill, Azrin, Cross, & Strada (2007) | N: 31 Sample: Marijuana-using adolescents with both substance use disorder and conduct disorder diagnoses who completed outpatient treatment |
Intraclass Correlations Between Parent and Adolescent Reports on Days of Use of Cannabis Over 6 Months of Treatment Month 1=0.69; Month 2=0.63; Month 3=0.63; Month 4 =0.74; Month 5 =0.85; Month 6 =0.75 Intraclass Correlations Between Parent Report on Days of Use of Cannabis Over 6 Months of Treatment and Urinalysis Results Month 1=0.49; Month 2=0.49; Month 3=0.34; Month 4 =0.58; Month 5 =0.53; Month 6 =0.44 Intraclass Correlations Between Adolescent Report on Days of Use of Cannabis Over 6 Months of Treatment and Urinalysis Results Month 1=0.41; Month 2=0.45; Month 3=0.39; Month 4 =0.49; Month 5 =0.62; Month 6 =0.54 |
| McGillicuddy, Rychtarik, Morsheimer, & Burke-Storer (2007) | N: 75 Sample: Adolescents with parents reporting concerns about the adolescents’ substance use |
Kappa Scores of Parent-Adolescent Agreement on Any Adolescent Substance Use in the Previous 180 Days Alcohol= 0.21 Cannabis= 0.43 Intraclass Correlation of Parent and Adolescent Reports on Quantity of Alcohol Used per Drinking Day ICC= 0.19 Intraclass Correlation of Parents and Adolescents for Days of Use in Past 180 Days Alcohol= 0.61 Cannabis= 0.52 |
| Waldron, Slesnick, Brody, Turner, & Peterson (2001) | N: 114 Sample: Adolescents referred for outpatient treatment for substance use disorders |
Pearson Correlations Between Adolescent and Parent Report of Adolescent Cannabis Use
r= 0.37*** |
| Instrument: Untitled Interview | ||
| Ciesla, Spear, & Skala, (1999) | N: 119 Sample: Adolescents who recently completed drug treatment (residential versus outpatient not specified) |
Kappa Scores of Parent and Adolescent Report on Adolescent Use of Any Substance at 3, 6, 9 and 12 months Post-Treatment
3 month= 0.41; 6 month= 0.45; 9 month= 0.76; 12 month= 0.18 |
| Instrument: CAGE-Adapted to Include Drugs (CAGE-AID) | ||
| Couwenbergh, Van Der Gaag, Koeter, De Ruiter, & Van den Brink (2009) | N: 143 Sample: Dutch adolescents referred for outpatient mental health services |
Percent Agreement and Kappa Scores of Parent and Adolescent Report of Substance Abuse Symptoms Above Clinical Cut-Off
Percent agreement= 94.7% Kappa= 0.74 |
| Instrument: Personal Experiences Inventory – Parent Version (PEI-PV) | ||
| Green, Bekman, Miller, Perrott, Brown, & Aarons (2011) | N: 985 Sample: Adolescents involved in services such as alcohol/drug treatment, child welfare, juvenile justice, mental health, or special education |
Kappa Scores of Parent-Child Agreement on Lifetime Adolescent Substance Use Alcohol= 0.50 Cannabis= 0.67 Kappa Scores of Parent-Child Agreement on Adolescent Substance Use Related Problems Alcohol= 0.34 Drugs (including cannabis)= 0.47 |
| Winters, Anderson, Bengston, Stinchfield, & Latimer (2000) | N: 205 Sample: Adolescents with a substance use disorder who presented for outpatient substance abuse treatment |
Pearson Correlations Between Parent and Adolescent Report on 3 Drug Involvement Scales on PEI Personal involvement with drugs= 0.27* Consequences of drug use= 0.30** Transituational drug use= 0.33** |
| Instrument: Drug Use Frequency (DUF) | ||
| Winters, Stinchfield, Latimer, & Lee (2007) | N: 315 Sample: Adolescents who met criteria for at least one substance dependence diagnosis (in treatment and waitlist groups) and community controls |
Overall Percent Agreement Rates Between Parent and Adolescent Reports on Adolescent Abstinence Versus Non-Abstinence for Any Substance
Agreement in treatment group= 85% Agreement in waitlist group= 89% Agreement in control group= 79% |
| Instrument: Personal Experience Screening Questionnaire (PESQ) | ||
| McGillicuddy & Eliseo-Arras (2012) | N: 50 Sample: Adolescents enrolled in a residential drug/alcohol treatment program |
Percent Agreement, Kappa Scores, and ICCs for Parent and Adolescent Report on Adolescent’s Use of Substances in the 90 Days Prior to Treatment Abstinence versus Non-Abstinence Alcohol percent agreement=76% Cannabis percent agreement=82% Alcohol kappa=0.45 Cannabis kappa=0.36 Days of Use Alcohol ICC=0.79 Cannabis ICC=0.57 |
| Untitled Questionnaires | ||
| Berge, Sundell, Ojehagen, Hoglund, & Hakansson (2015) | N: 1426 Sample: Community sample of Swedish adolescents |
Parent Sensitivity Regarding Adolescent-reported Substance Use and Kappas of Parent-Child Agreement Regarding Use Alcohol 7th grade= 5.6%; Kappa= 0.09 8th grade= 14.7%; Kappa= 0.19 9th grade= 26.1%; Kappa= 0.25 Illicit Drugs (including Cannabis) 7th grade= 7.1%; Kappa= 0.13 8th grade= 12.0%; Kappa= 0.20 9th grade = 4.9%; Kapp= 0.08 |
| Chang et al. (2013) | N: 1831 Sample: Community sample of Taiwanese adolescents) |
Percentages by Agreement Category of Parent and Adolescent Reports on Current Adolescent Alcohol Use Adolescent and Parent both “no”= 91.2% Adolescent and Parent both “yes”= 0.5% Adolescent “no”, Parent “yes”= 1.1% Adolescent “yes”, Parent “no”= 7.3% |
| Langhinrichsen et al. (1990) | N: 763 Sample: Community sample of adolescents |
Kappa Scores of Parent and Adolescent Report of Use Category Mother-child alcohol= 0.36 Father-child alcohol= 0.41 Mother-child cannabis= 0.61 Father-child cannabis= 0.56 |
| Williams, McDermitt, Bertrand, & Davis (2003) | N: 985 Sample: Community sample of adolescents |
Kappa Scores of Parent-Adolescent Agreement on Report of Adolescent Substance Use in Past Month
Alcohol=0.33 Other illicit drugs (including cannabis)= 0.20 |
Notes.
p<0.05;
p<0.01;
p<.001
The N provided represents the sample size used to calculate levels of agreement. This was often a subsample from a larger sample reported in the study.
All samples are North American unless otherwise noted
All studies were reviewed by the first two authors (TP and S-KL). All study characteristics and indices of agreement were coded and recorded independently by these authors. There were very few disagreements regarding the coding of study characteristics within specific categories, but those that arose were resolved through discussion. The second author involved in the coding was blind to study hypotheses. The categories evaluated across studies included substance (alcohol versus cannabis), assessment method (interview versus self-report), assessment type (assessment versus screening), sample (clinical versus community), and outcome type (use/nonuse or frequency versus problems or diagnoses associated with use). Samples were considered clinical when participants had established mental health or substance use diagnoses or were either seeking or had recently completed a mental health or substance use-related intervention. Samples not meeting these criteria but that were considered “at risk” (e.g., a family history of drug use problems) were included in the community category. When study samples included both clinical and community participants, they were excluded from comparisons of sample types. Screening measures (versus full assessments) were identified through the use of either an established screening measure or a brief assessments (i.e., less than three items) with community-based samples.
In order to evaluate the relationship between study-related variables and agreement, we calculated the average kappas across all studies fitting into different primary study categories. Kappas were selected because this was by far the most widely report agreement statistic across all studies. Because other indices of agreement (i.e., sensitivity/specificity, correlations, ICC, percent agreement) utilize distinct types of data (e.g., dichotomous, ordinal, continuous) and reflect distinct aspects of agreement, we did not feel it was appropriate to convert these other statistics into a common metric to evaluate agreement across all identified studies. However, when appropriate, we did calculate other indice-specific aggregations when reported by multiple studies.
When computing average kappas for all studies or for each study category, studies were weighted equally by averaging studies with multiple relevant kappas into a single study-level kappa prior to computing study category averages or overall averages across all studies. Thus, each summary kappa statistic included no more than one kappa from each study. However, a single study could contribute to multiple category averages provided relevant statistics were provided (e.g., alcohol and marijuana agreement). When agreement regarding the same outcome and substance was assessed longitudinally within a study, an average kappa value across each assessment point was calculated and utilized in creating average kappas by category. One study provided separate kappa values for mother-adolescent and father-adolescent agreement. These were averaged to form a single kappa value representing parent-child agreement. Given the high degree of heterogeneity across individual studies, no efforts were made to apply weights to the results of individual studies for evaluating average kappa values. Thus, average kappas and differences between kappas between categories should be interpreted only as approximation to aid in interpretation of overall levels of agreement and differences in agreement between study categories.
There were two studies identified in the current review that utilized an overlapping sample.12,30 Donohue, Hill, et al.12 examined a subsample of participants who completed an outpatient treatment study from the larger Donohue, Azrin, et al. study.30 We present both of these studies in the current review due to their unique sample characteristics (i.e., adolescents at treatment intake versus adolescents who complete outpatient treatment). However, neither study provided a kappa statistic reflecting agreement and therefore was not included in aggregated kappa agreement indices.
Results
Assessment Instruments
Table 1 details the measures used in each study. Eighteen out of the total 27 studies reviewed utilized an interview-based assessment of parental knowledge of adolescent substance use. Seventeen of the studies relied on established structured or semi-structured interviews. A single study relied upon an untitled semi-structured interview protocol developed for use in that study.31 Nine studies utilized self-administered questionnaires, with five studies utilizing established questionnaires and the remaining four utilizing untitled questionnaires created specifically for each study.
Structured Interviews
Diagnostic Interview Schedule for Children- Parent Version (DISC-P).
The DISC-P is a structured diagnostic interview designed to collect DSM-related diagnostic information for the most common mental health disorders found in children and adolescents.32 The questions pertaining to alcohol and other drug involvement ask about onset of use, diagnostic symptoms, and problems in multiple psychosocial areas (e.g., family functioning, peer affiliations, academic and occupational functioning, and school adjustment). If impairments are present, the interviewee is asked for additional information regarding severity and frequency of the problems. A parallel youth version of the DISC is also available that differs primarily in pronoun usage from the DISC-P. The DISC-P was utilized by three studies included in the review.21,33,34
Global Appraisal of Individual Needs - Collateral Assessment Form (GAIN –CAF).
The Global Appraisal of Individual Needs (GAIN) is a standardized psychosocial interview that covers a variety of areas of functioning that was designed to provide information regarding substance use as well as aid in treatment planning.35,36 A version of the GAIN, called the GAIN-CAF, was created for use by collaterals, including parents or guardians, to help validate participant self-reports and check for any areas of denial.36 The GAIN and GAIN-CAF both collect information about symptoms of substance use disorders and recency and frequency of using cannabis, alcohol, and other drugs. In the current review, the GAIN-CAF was used in two studies.36,37
Semi-Structured Interviews
Semi-Structured Assessment for the Genetics of Alcoholism (C-SSAGA).
The C-SSAGA is a polydiagnostic instrument that gathers a comprehensive, lifetime psychiatric history including substance use disorders.38 The interview also measures physical, social and psychological manifestations of psychiatric disorders and risk domains related to a substance use disorder. The C-SSAGA is available in both adolescent and parent versions. Fisher et al.39 was the only study in the current review to utilize the C-SSAGA.
Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS).
The K-SADS is a semi-structured diagnostic interview that gathers a comprehensive assessment of the child’s current and past psychiatric, behavioral, and social functioning.40 The K-SADS yields DSM diagnostic information, as well as use pattern behavior regarding a variety of substances. The K-SADS may be used to interview both adolescents and parents and is available in both an Epidemiologic version (K-SADS-E) that obtains lifetime symptoms and associated diagnoses and a Present Episode version (K-SADS-P) for current symptoms and diagnoses. Six studies in the current review utilized versions of the K-SADS.7,10,41–44
Teen Addiction Severity Index (T-ASI).
The T-ASI is a semi-structured diagnostic interview that was modified from the Addiction Severity Index.45 The T-ASI is available in both self- and parent-report versions and uses information about drug use history, frequency, quantity, problems associated with use, and impact of use on different areas of psychosocial functioning to calculate an overall severity index score across all substances. Burleson and Kaminer’s study24 was the only in the current review to utilize the T-ASI.
Timeline Follow-back Interview (TLFB).
This semi-structured interview provides a procedure to collect substance use information for a specific period of time such as 90 or 180 days.46 Although various adaptations have been made to this interview, most versions ask the respondents to retrospectively report on daily alcohol and substance use using a monthly calendar with interviewer prompts on such occasions as birthdays, holidays, etc. Scores obtained from the TLFB indicate the number of days a given substance was used, as well as the quantity (usually alcohol) on use days.46 The TLFB may also be administered to parents in order to assess the parents’ report of their child’s drug use. Four studies in the current review utilized the TLFB.12,30,47,48
Untitled Interview.
A single study used an untitled telephone interview of parents and adolescents to evaluate adolescent substance use during the previous 3 months.31
Self-Administered Questionnaires
CAGE-Adapted to Include Drugs (CAGE-AID).
The 4-item CAGE-AID is a screening measure that evaluates problematic use of drugs and alcohol.23 The CAGE-AID was modified from the original CAGE to include drug use in addition to alcohol.49 The questions evaluate common symptoms of drug and alcohol abuse during the previous six months. The CAGE-AID is available in both self-report and parent-report versions.23 A single study in the current review utilized the CAGE-AID.23 Notably, the CAGE-AID was developed for adults and has been previously found to have relatively poor psychometric properties with adolescents, including weaker sensitivity, when compared to other screening measures used with adolescents.50
Personal Experiences Inventory-Parent Version (PEI-PV).
The PEI-PV51 is the parent companion to the adolescent PEI.52 Both the PEI and PEI-PV are questionnaires that include three scales relevant to drug use severity, including drug involvement, consequences of drug use, and transituational drug use. The wordings of the parent PEI-PV items mirror those of the adolescent PEI. The PEI-PV was utilized by Winters et al.51 and Green et al.53 in this review.
Drug Use Frequency (DUF).
The DUF17 is a measure adapted from items used in the Monitoring the Future Study.54 The rating scale allows parents and youth to report on youth frequency of use of 12 major drug categories. A single study in the current review utilized the DUF.17
Personal Experiences Screening Questionnaire – Parent Version (PESQ).
The PESQ is a screening instrument for adolescent substance use problems.55 The measure includes a problem severity scale and several drug use frequency items. While the PESQ was developed as an adolescent self-report measure, a single study in the current review used an altered version to interview parents that mirrored the adolescent version.25
Untitled Questionnaires.
Several studies in the current review developed untitled questionnaires or items within larger questionnaires to assess parental knowledge of adolescent substance use. These assessments included Likert scales to assess frequency of use of difference substances,56 single dichotomous use/nonuse items,57,58 or substance-specific use items allowing for responses of yes, no, or unsure.22
Parent-Adolescent Agreement
Table 1 details indices of agreement reported for each study identified in the review. A variety of indices of agreement were utilized across the studies, with 17 studies including at least one Kappa in their results, four studies reporting only Pearson correlations,24,33,51,59 three studies reporting only percentage agreement,7,17,58 two studies reporting only intraclass correlations,12,30 and one study reporting only sensitivity/specificity information.41 The overall mean level of agreement across all studies reporting kappa scores for all outcomes was fair (n = 17; Mean k= 0.42; SD= 0.22). Studies reporting only Pearson correlations were consistent with an average low to moderate correlation between adolescent and parent report (n = 4; Mean r= .36, SD=.09).24,33,51,59 Of the three studies that provided only percent agreements,7,17,58 just two reported the statistic in a way that allowed for calculation of overall agreement rates. These two studies were consistent with generally high levels of agreement regarding use/non-use of substances (n = 2; Mean % Agreement= 88.01, SD=5.21).17,58 The two studies reporting only ICCs were consistent with a fair level of parent-adolescent agreement when averaged (n = 2; Mean ICC= .56, SD=.22).12,30
Agreement by Type of Substance
Out of 27 studies included in the review, 12 of those studies included in the review evaluated agreement regarding both alcohol and cannabis. Five studies evaluated only cannabis, and just one study evaluated only alcohol. Five studies examined alcohol along with a combined drug category that included cannabis. Finally, the remaining 4 studies evaluated agreement in only a combined substance category including alcohol, cannabis, and other drugs. Average kappas were calculated for each substance category for studies providing relevant kappas. Agreement rates for studies with alcohol-related measures (n = 15; Mean k= 0.37, SD = 0.21) and combined drug measures (n = 8; Mean k= 0.35, SD = 0.22) were lower than those observed for cannabis-related measures (n = 10; Mean k= 0.54, SD = 0.22). However, for the four studies that included any parent-child ICCs, alcohol-related ICCs were nearly equivalent (n = 3; Mean ICC = .6; SD = .20) to those ICCs reported for cannabis (n = 4; Mean ICC = .56, SD = .12).12,25,30,47
Agreement by Assessment Method
Eighteen studies utilized interview-based measures and 9 relied upon self-administered questionnaires to evaluate agreement. Among those studies providing kappas, interview-based measures (n = 11; Mean k= 0.42, SD = 0.23) displayed similar kappa scores to questionnaire-based measures (n = 6; M k= 0.43, SD = 0.20). There was insufficient representation of indices of agreement other than kappa that corresponded across both interview- and questionnaire-based methods to form meaningful comparisons.
Agreement by Assessment Type
A total of six studies utilized screening measures and the remaining 21 evaluated complete assessments. Among those studies providing kappas, screening measures (n = 5; Mean k= 0.42, SD = 0.22) displayed similar kappa scores to full assessments (n = 12; M k= 0.41, SD = 0.22). A single study that employed a screening measure did not provide a kappa measure of agreement;58 thus, comparisons on other indices were not examined.
Agreement by Sample Type
The study samples represented both clinical (n= 15) and community/at-risk populations (n= 10). Two studies provided agreement indices for samples comprised of a mix of community and clinical populations. Among those studies providing kappas, the clinical samples (n = 8; Mean k= 0.56, SD = 0.21) yielded higher rates of agreement than the community samples (n = 8; Mean k= 0.28, SD = 0.13). There were again inadequate corresponding indices of agreement other than kappa to form meaningful comparisons on those other indices.
Agreement by Type of Outcome
The reviewed studies evaluated several types of outcomes, including use/non-use, frequency, substance use diagnoses, and symptoms/problems associated with use. Several studies evaluated more than one type of outcome. Nineteen studies provided information regarding use/non-use or frequency of use, and twelve studies provided diagnostic outcomes or associated problems/symptoms associated with use. For studies reporting kappa agreements, within-study averages were calculated for each type of outcome. For these studies, use/non-use and frequency outcomes (n = 11; Mean k= 0.47, SD = 0.22) demonstrated slightly higher levels of agreement than diagnostic or symptom-related outcomes (n = 8; Mean k= 0.36, SD = 0.19). Beyond kappas, we were able to compare Pearson correlational agreement across outcome type. Two studies included parent-adolescent correlations of use/non-use and frequency outcomes,24,59 and three studies included correlations for diagnostic or symptom-related outcomes.24,33,51 The mean parent-adolescent correlation for use/non-use and frequency outcomes (n = 2; Mean r= .43, SD = .08) was similarly modestly higher than the mean correlation for diagnostic or symptom-related outcomes (n = 3; Mean r= .35, SD = .11).
Parent and Adolescent Agreement with Urinalysis
Several studies examined the level of concordance between adolescent urinalysis and parent and adolescent reports of adolescent substance use. Gignac and colleagues assessed cannabis use using urine toxicology screens and parental and adolescent report in adolescents with and without ADHD.41 From a larger sample including both adolescents and young adults, a subsample of participants under the age of 18 (n = 22) and their parents were interviewed using K-SADS-E. For those youth under the age of 18 with positive urine screens for cannabis, self-report exhibited a significantly higher level of agreement with urinalysis (91%) than parent report of use (64%). For those youth with a negative urine screen, there was not a significant difference in the level of agreement between the urinalysis result and self-report (87%) versus the urinalysis result and parent report (93%).
Burleson and Kaminer used adolescent report and parent report on the T-ASI along with urinalysis to assess substance use disorders in a sample of adolescents presenting for outpatient treatment.24 At 3- and 9-month assessments following treatment, the authors assessed youth use of alcohol and other substances using youth and parent report on the T-ASI, youth and parent report regarding single interview items reflecting use/nonuse, and substance use through urinalysis. Adolescent-reported information generally demonstrated stronger correlations with urinalysis (use/nonuse item: 0.49 – 0.64; adolescent T-ASI score: 0.52 – 0.32) when compared to parent-report/urinalysis correlations (use/nonuse item: 0.28 – 0.43; parent T-ASI score: 0.31 – 0.33). Using urinalysis as the standard, adolescent report also demonstrated generally higher specificity and sensitivity when compared to parent-report on the use/nonuse single item.
Donohue, Hill, et al. examined the concordance of urinalysis and parent and adolescent report of marijuana use in small sample of youth with co-occurring substance use and conduct disorders (n=31).12 These youth were a subsample from the Donohue et al. (2004) study who endorsed marijuana use and subsequently completed an outpatient substance use intervention. Both parents and youth completed the TLFB regarding the previous 6 months at the conclusion of treatment. Youth also completed urinalysis screening for cannabis at each intervention session. When compared to urinalysis results, the retrospective reports of parents and adolescents demonstrated similar levels of poor to fair agreement with urinalysis (parent-report/urinalysis ICCs: 0.34 – 0.58; adolescent-report/urinalysis ICCs: 0.39 – 0.62). Levels of agreement were generally consistent across each month of treatment.
Within-Study Variables Associated with Level of Parent-Adolescent Agreement
A number of the reviewed studies identified variables associated with variability in the level of agreement between parents and adolescents. Several studies examined adolescent age for its association with parent-child agreement. Jones et al. found that parent-adolescent agreement on the K-SADS was lower for older adolescents when compared to younger adolescents in a community sample.42 Also using the K-SADS, O’Donnell et al. similarly found that parents of older adolescents were less likely to be aware of adolescent-reported use when compared to parents of younger adolescents in a sample of adolescents with attention-deficit hyperactivity disorder and community control participants.43 McGillicuddy et al. also found that lower levels of agreement were present for younger adolescents when using the TLFB in a sample of youth identified due to parental concerns about substance use.47 In contrast, Fisher et al. found that the sensitivity of parent reports in detecting use when use was reported by adolescents increased with adolescent age in a sample of adolescents with a family history of alcohol use disorders as well as community controls.39 Williams et al. also found that parents of older adolescents were more likely to be aware of adolescent’s self-reported substance use in a community sample.22
Two studies produced contradictory results regarding adolescent gender as a predictor of parent-adolescent agreement. Using the PEI, Green et al. found that parents of males tended to be more aware of their adolescent’s self-reported drug use than did parents of females in a subsample of adolescents who met criteria for alcohol or drug abuse/dependence.53 However, Jones et al. found that parent-adolescent agreement on the K-SADS was lower for male adolescents when compared to females in a community sample.42
Several adolescent risk factors emerged as predictors of the level of parent-adolescent agreement. Using the PESQ in a sample of adolescents receiving drug treatment in residential programs, McGillicuddy and Eliseo-Arras found that greater adolescent involvement with parole or probation officers prior to treatment, fewer days of adolescent incarceration, and adolescents spending less time living at home were each associated with greater discrepancies between parent and adolescent report on any substance.25 O’Donnell et al. found that greater levels of social impairment, higher frequency of substance use, and the presence of multiple substance use disorders in the adolescent were each associated with a greater likelihood of parental awareness of adolescent use.43
A variety of parental and family-based risk factors were also found to have a relationship with parent-adolescent agreement. McGillicuddy et al. found lower levels of parent-adolescent agreement when parents demonstrated lower levels of monitoring of their adolescent’s behaviors, as well as when parents demonstrated higher levels of psychological distress and alcohol use.47 Green et al. similarly found that parental depression was associated with decreased parental awareness of adolescent problems with alcohol.53 Chang et al. found that low socioeconomic status and other family transitions (e.g., divorce) were positively associated with discrepancies in parent-adolescent report of adolescent alcohol use in a Taiwanese community sample.58 Langhinrichsen et al. found that for cannabis, single mothers were less likely to demonstrate congruence with adolescent report than those mothers in two-parent families in a community sample.56 In contrast, O’Donnell et al. reported that impairments in the family environment were associated with a greater likelihood of parental awareness of adolescent substance use.43 Interestingly, Williams et al. found that high adolescent ratings of family communication combined with low parental ratings of family communication were also associated with greater parental awareness of use in a community sample.22
Discussion
Our review of the literature on parent assessment of adolescent drug involvement provides a mixed picture. While many parents have some awareness of their adolescent’s use, our review indicates that parents’ report of a variety of features of their child’s drug use behaviors has several limitations. Parents and adolescents demonstrated generally modest levels of agreement. Furthermore, parents tended to report lower drug involvement rates and associated problems when compared to disclosures by the adolescent. We consistently found this pattern for all main drug involvement variables for both alcohol and cannabis involvement (i.e., use/nonuse, level/frequency of use, and drug related problems). Interview data was not superior to questionnaire data in this regard. Furthermore, when compared with biological measures, adolescent-reported data demonstrated a higher level of concordance than parent-reported data.
Poor corroboration between parent and adolescent reports does not necessarily mean that parental report is less valid than the child’s, but our review is suggestive that this might be the case. As noted above, parents tend to report lower rates of use and related problems when compared to the disclosure by their child. While this could reflect a pattern of overreporting use by adolescents, this seems less likely given the unclear motivation for adolescents to exaggerate use in an anonymous research context. Particularly for those studies conducted following completion of drug treatment, one might instead expect a reasonably high motivation for adolescents to deny or minimize drug use rather than exaggerate. Furthermore, examination of concordance with objective, biological measures does not generally support this possibility. In the studies that compared the parent’s and adolescent’s reports of drug use with biological measures such as urinalysis, the associations were nearly always higher in the adolescent-urinalysis agreement data when compared to parent-urinalysis agreement data.
There may be value in better understanding circumstances under which parental reports may be more likely to align with adolescent reporting. A number of study-level variables seemed to contribute to variability in the concordance between parent- and adolescent-reported data. Variables such as the type of substance, sample, and targeted outcome seemed to be associated with the level of concordance observed between adolescents and their parents. While the large number of study variables and the variety of methods used in assessing concordance across studies makes it difficult at times to draw clear, empirically-based comparisons relative to specific study variables, several general trends were evident in our review. First, there was generally higher parent-adolescent concordance regarding use of cannabis when compared to alcohol use. Because cannabis use was reported less frequently than alcohol use in most samples, it may be that cannabis has historically represented a deeper involvement in drug use that may be more likely to trigger parental awareness. However, recent national trends of decreasing alcohol use combined with steady to increasing numbers of adolescent cannabis users seem likely to impact this distinction.1 Both community and clinical samples (i.e., those with substance use disorder diagnoses or recent involvement in treatment programs) were commonly evaluated in the reviewed literature. Community samples tended to report lower levels of agreement when compared to clinical samples. There may be a few reasons for this. First, adolescents in clinical samples were very likely to be experiencing problems or impairment due to their drug use, increasing the likelihood of parental awareness of use. Furthermore, because clinical samples often had recent or ongoing contact with treating professionals, families in these samples may have been more likely to have open discussions about the adolescent’s drug use, increasing the likelihood of concordance between reporters. Finally, diagnostic outcomes produced generally lower levels of agreement when compared to use/nonuse outcomes. This is not surprising due to the relatively high level of complexity of evaluating diagnostic symptoms and the deeper level of knowledge of youth use and functioning required in order to evaluate diagnostic criteria.
Several study variables did not reveal any clear association with agreement when examined across studies. Our review did not support one assessment method as superior to another in producing strong parent-child agreement; interview-based assessments resulted in similar levels of agreement when compared to rating scales assessments. Similarly, screening measures did not produce notably different levels of agreement when compared to more complete assessment measures. The lack of differences for these study variables is reassuring that these key study methodological decisions are unlikely to make a large impact on parent-adolescent correspondence.
A variety of participant-related variables were examined within studies for their impact on parent-adolescent agreement. When examining developmental influences on parent-child agreement, there were mixed results. Some studies demonstrated greater agreement (and presumably greater awareness) of adolescent use for older adolescents while others found that parents tended to demonstrate higher levels of agreement for younger adolescents. Adolescent gender similarly produced mixed results with some studies showing higher agreement for male adolescents and others for female adolescents. Multiple studies also implemented repeated measures of agreement, including pre and post measures related to completing a treatment program and/or longitudinal follow-ups after completing treatment. Again, no clear pattern emerged among these multiple assessment points with regard to increasing or decreasing agreement.
An examination of study findings related to adolescent and parent risk factors as predictors of agreement revealed some trends. These within-study variables generally supported an association between higher risk and lower levels of agreement. In particular, parental and family-based risk factors such as impaired parental mental health, poor parental monitoring, or other family transitions such as divorce predicted greater discrepancies in most studies. These risk factors seem likely to negatively impact parental awareness of adolescent use. However, some studies found that increased risk in some areas was associated with increased awareness, including a greater frequency of adolescent use or problems associated with use. As the severity of adolescent use increases and associated problems become more difficult to conceal, it becomes less likely that the parent will remain unaware of this use.
Several limitations are important to consider when interpreting the results of our review. First, a number of the studies reviewed were conducted 20 or more years ago. As many aspects of adolescent substance use continually evolve (including norms surrounding acceptability of different substances and associated disclosure of use to parents), the results of these older studies may no longer reflect current realities for adolescents and their parents. Several studies included small sample sizes and/or measures with poor or undemonstrated psychometrics with adolescents. When summarizing agreement across different studies, we did not exclude studies due to these issues in order to provide the broadest perspective of parent-adolescent agreement across all measures and samples available. However, parent-adolescent agreement in some of these studies may have been reduced due to the use of poorly performing measures or may lack generalizability due to the use of small samples. Furthermore, our efforts to compare agreement across studies were hampered by the wide variety of indices of agreement utilized. While kappas were present in many studies, it could be that the impressions resulting from our review would be different if all studies utilized a common measure. Finally, as noted above, the wide variety of study-related variables that were often confounded lends additional caution to the interpretation of our conclusions about factors related to agreement.
In sum, efforts to assess parents about their adolescent’s possible drug use and resulting problems and symptoms should proceed cautiously. We do not recommend using parental report as a standalone method of assessing adolescent drug use. Parents may have limited ability to offer detailed and accurate information about their child’s drug use and resulting symptoms, and they may tend to underestimate their child’s use. We recommend that when parents are assessed by researchers in adolescent drug abuse studies or by clinicians in drug treatment programs, the focus be limited, including general use or non-use or drug use consequences (e.g., impairments in functioning) that realistically could come to the attention of the parent. Furthermore, the particularly low levels of agreement between parents and adolescents found in community samples is not encouraging of the use of parental reports as a primary screening tool for identifying adolescent use among lower risk samples.
While our findings do not generally highlight the concordance of parental and youth reports of adolescent substance use, it is important to note that parental assessments have research and clinical value. One promising body of research highlights the potential predictive utility of discrepancies between parent and youth reports of corresponding behaviors.60 Highly divergent reporting of adolescent problem behaviors between parents and youth may in fact signify risk associated with parenting practices or the parent-child relationship. Poor parental monitoring and limited parental knowledge of youth behaviors is associated with initiation of substance use in adolescence.14 Relatively large discrepancies in parental reports may signify risk associated with a lack of parental knowledge of their adolescent’s behavior.47 This developing research area is likely to yield further insights into the role of reporter discrepancies as a risk factor for adolescent substance use.
While potentially problematic as standalone assessments, we believe that parental reports have value as an adjunctive assessment tool to self-reported measures in certain clinical contexts. In settings such as primary care or in substance abuse treatment, both the adolescent and parent may be present and readily able to complete assessment measures. Particularly in situations when adolescents may be likely to inaccurately minimize or deny use due to potential negative consequences of acknowledging use, parents may more readily share any observed substance use behaviors. In settings such as primary care, the use of adjunctive parental screening measures may improve overall screening sensitivity for substance use with only minimal losses in specificity.
In clinical settings, parents are, of course, valuable reporters of other areas relevant to drug use and treatment outcomes, including the adolescent’s health history, family functioning, parenting practices, family history of drug use and treatment, and co-existing mental and behavioral problems and disorders (e.g., ADHD, depression) that may co-exist with drug involvement. Irrespective of the relative validity of parent reports of adolescent substance use, there may be general clinical value to involving parents in the assessment process. The value of parents being aware of their child’s use is heightened by the fact that many adolescent treatment programs involve parents. Clinicians may gain valuable information and perspectives from parents that are relevant to determining therapy strategies and establishing clinical goals. Previous research has shown how integral parents, parenting behaviors, and household rules can be in impacting adolescent substance use.53,61–63 Thus, irrespective of assessment processes, engaging parents in the treatment process is likely to hold benefits for youth.
Acknowledgements
This study was supported by grants P50DA027841 and K24-DA035882 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
References
- 1.Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future National Survey Results on Drug Use, 1975–2018: Overview, Key Findings on Adolescent Drug Use. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2019. [Google Scholar]
- 2.Ellickson PL, Tucker JS, Klein DJ. Ten-year prospective study of public health problems associated with early drinking. J Am Acad Child Adolesc Psychiatry. 2003;42(11):1318–1326. [DOI] [PubMed] [Google Scholar]
- 3.Fergusson DM, Boden JM. Cannabis use and later life outcomes. Addiction. 2008;103(6):969–976. [DOI] [PubMed] [Google Scholar]
- 4.National Institute on Drug Abuse. Principles of adolescent substance use disorder treatment: A research-based guide Vol NIH Publication No. 14–7953 Bethesda, MD: National Institute on Drug Abuse; 2014. [Google Scholar]
- 5.Substance Abuse and Mental Health Services Administration. Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013. [Google Scholar]
- 6.Kellam SG, Koretz D, Mościcki EK. Core elements of developmental epidemiologically based prevention research. Am J Community Psychol. 1999;27(4):463–482. [DOI] [PubMed] [Google Scholar]
- 7.Delaney-Black V, Chiodo LM, Hannigan JH, et al. Just say “I don’t”: Lack of concordance between teen report and biological measures of drug use. Pediatrics. 2010;126(5):887–893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Johnston LD, O’Malley PM. The recanting of earlier reported drug use by young adults. NIDA Res Monogr. 1997;167:59–80. [PubMed] [Google Scholar]
- 9.Winters KC, Stinchfield RD, Henly GA, Schwartz RH. Validity of adolescent self-report of alcohol and other drug involvement. Int J Addict. 1990;25(Supp. 11):1379–1395. [DOI] [PubMed] [Google Scholar]
- 10.Cantwell DP, Lewinsohn PM, Rohde P, Seeley JR. Correspondence between adolescent report and parent report of psychiatric diagnostic data. J Am Acad Child Adolesc Psychiatry. 1997;36(5):610–619. [DOI] [PubMed] [Google Scholar]
- 11.De Los Reyes A, Augenstein TM, Wang M, et al. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol Bull. 2015;141(4):858–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Donohue B, Hill HH, Azrin NH, Cross C, Strada MJ. Psychometric support for contemporaneous and retrospective youth and parent reports of adolescent marijuana use frequency in an adolescent outpatient treatment population. Addict Behav. 2007;32(9):1787–1797. [DOI] [PubMed] [Google Scholar]
- 13.Achenbach TM, McConaughy SH, Howell CT. Child/adolescent behavioral and emotional problems: implications of cross-informant correlations for situational specificity. Psychol Bull. 1987;101(2):213–232. [PubMed] [Google Scholar]
- 14.Lippold MA, Greenberg MT, Collins LM. Youths’ substance use and changes in parental knowledge-related behaviors during middle school: A person-oriented approach. J Youth Adolesc. 2014;43(5):729–744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Waters E, Stewart-Brown S, Fitzpatrick R. Agreement between adolescent self‐report and parent reports of health and well‐being: Results of an epidemiological study. Child Care Health Dev. 2003;29(6):501–509. [DOI] [PubMed] [Google Scholar]
- 16.Kessler CR, Amminger PG, Aguilar-Gaxiola BS, Alonso BJ, Lee BS, Üstün BT. Age of onset of mental disorders: A review of recent literature. Curr Opin Psychiatry. 2007;20(4):359–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Winters KC, Stinchfield R, Latimer WW, Lee S. Long-term outcome of substance-dependent youth following 12-step treatment. J Subst Abuse Treat. 2007;33(1):61–69. [DOI] [PubMed] [Google Scholar]
- 18.Magura S Validating self-reports of illegal drug use to evaluate National Drug Control Policy: A reanalysis and critique. Eval Program Plann. 2010;33(3):234–237. [DOI] [PubMed] [Google Scholar]
- 19.Dolan K, Rouen D, Kimber J. An overview of the use of urine, hair, sweat and saliva to detect drug use. Drug Alcohol Rev. 2004;23(2):213–217. [DOI] [PubMed] [Google Scholar]
- 20.Vearrier D, Curtis JA, Greenberg MI. Biological testing for drugs of abuse In: Luch A, ed. Molecular, Clinical and Environmental Toxicology. Volume 2: Clinical Toxicology Basel: Birkhäuser Basel; 2010:489–517. [DOI] [PubMed] [Google Scholar]
- 21.Chung T, Colby SM, Leary TA, Barnett NP, Monti PM. Screening for cannabis use disorders in an adolescent emergency department sample. Drug Alcohol Depend. 2003;70(2):177–186. [DOI] [PubMed] [Google Scholar]
- 22.Williams RJ, McDermitt DR, Bertrand LD, Davis RM. Parental awareness of adolescent substance use. Addict Behav. 2003;28(4):803–809. [DOI] [PubMed] [Google Scholar]
- 23.Couwenbergh C, Van Der Gaag RJ, Koeter M, De Ruiter C, Van Den Brink W. Screening for substance abuse among adolescents validity of the CAGE-AID in youth mental health care. Subst Use Misuse. 2009;44(6):823–834. [DOI] [PubMed] [Google Scholar]
- 24.Burleson JA, Kaminer Y. Adolescent alcohol and marijuana use: Concordance among objective-, self-, and collateral-reports. J Child Adolesc Subst Abuse. 2006;16(1):53–68. [Google Scholar]
- 25.McGillicuddy NB, Eliseo-Arras RK. Parent-adolescent report correspondence on adolescent substance abuse among teens in residential rehabilitation. Addict Behav. 2012;37(4):456–462. [DOI] [PubMed] [Google Scholar]
- 26.Knight JR, Harris SK, Sherritt L, et al. Adolescents’ preferences for substance abuse screening in primary care practice. Subst Abus. 2007;28(4):107–117. [DOI] [PubMed] [Google Scholar]
- 27.Moher D, Liberati A, Tetzlaff J, Altman DG, and the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151(4):264–269. [DOI] [PubMed] [Google Scholar]
- 28.Cicchetti DV, Sparrow SA. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am J Ment Defic. 1981;86(2):127–137. [PubMed] [Google Scholar]
- 29.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Donohue B, Azrin NH, Strada MJ, Silver NC, Teichner G, Murphy H. Psychometric evaluation of self- and collateral timeline follow-back reports of drug and alcohol use in a sample of drug-abusing and conduct-disordered adolescents and their parents. Psychol Addict Behav. 2004;18(2):184–189. [DOI] [PubMed] [Google Scholar]
- 31.Ciesla JR, Spear SF, Skala SY. Reliability over time of self-reports given by adolescents and their parents in substance abuse outcome research. J Child Adolesc Subst Abuse. 2000;9(2):57–73. [Google Scholar]
- 32.Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry. 2000;39(1):28–38. [DOI] [PubMed] [Google Scholar]
- 33.Dillon FR, Turner CW, Robbins MS, Szapocznik J. Concordance among biological, interview, and self-report measures of drug use among African American and Hispanic adolescents referred for drug abuse treatment. Psychol Addict Behav. 2005;19(4):404–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kramer TL, Robbins JM, Phillips SD, Miller TL, Burns BJ. Detection and outcomes of substance use disorders in adolescents seeking mental health treatment. J Am Acad Child Adolesc Psychiatry. 2003;42(11):1318–1326. [DOI] [PubMed] [Google Scholar]
- 35.Dennis ML. Global Appraisal of Individual Needs (GAIN): Administration guide for the GAIN and related measures, Version 1299. Bloomington, IL: Chestnut Health Systems; 1999. [Google Scholar]
- 36.Dennis M, Titus JC, Diamond G, et al. The Cannabis Youth Treatment (CYT) experiment: Rationale, study design and analysis plans. Addiction. 2002;97(1):16–34. [DOI] [PubMed] [Google Scholar]
- 37.Godley MD, Godley SH, Dennis ML, Funk R, Passetti LL. Preliminary outcomes from the assertive continuing care experiment for adolescents discharged from residential treatment. J Subst Abuse Treat. 2002;23(1):21–32. [DOI] [PubMed] [Google Scholar]
- 38.Kuperman S, Schlosser SS, Kramer JR, et al. Risk domains associated with an adolescent alcohol dependence diagnosis. Addiction. 2001;96(4):629–636. [DOI] [PubMed] [Google Scholar]
- 39.Fisher SL, Bucholz KK, Reich W, et al. Teenagers are right—parents do not know much: An analysis of adolescent–parent agreement on reports of adolescent substance use, abuse, and dependence. Alcohol Clin Exp Res. 2006;30(10):1699–1710. [DOI] [PubMed] [Google Scholar]
- 40.Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980–988. [DOI] [PubMed] [Google Scholar]
- 41.Gignac M, Wilens TE, Biederman J, Kwon A, Mick E, Swezey A. Assessing cannabis use in adolescents and young adults: What do urine screen and parental report tell you? J Child Adolesc Psychopharmacol. 2005;15(5):742–750. [DOI] [PubMed] [Google Scholar]
- 42.Jones JD, Scott JC, Calkins ME, et al. Correspondence between adolescent and informant reports of substance use: Findings from the Philadelphia Neurodevelopmental Cohort. Addict Behav. 2017;65:13–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.O’Donnell D, Biederman J, Jones J, et al. Informativeness of child and parent reports on Substance Use Disorders in a sample of ADHD probands, control probands, and their siblings. J Am Acad Child Adolesc Psychiatry. 1998;37(7):752–758. [DOI] [PubMed] [Google Scholar]
- 44.Weissman MM, Wickramaratne P, Warner V, et al. Assessing psychiatric disorders in children. Discrepancies between mothers’ and children’s reports. Arch Gen Psychiatry. 1987;44(8):747–753. [DOI] [PubMed] [Google Scholar]
- 45.McLellan EAT, Luborsky PL, Woody PG, Oʼbrien PC. An improved diagnostic evaluation instrument for substance abuse patients: The Addiction Severity Index. J Nerv Ment Dis. 1980;168(1):26–33. [DOI] [PubMed] [Google Scholar]
- 46.Sobell LC, Sobell MB. Timeline followback: A technique for assessing self-reported alcohol consumption Measuring Alcohol Consumption: Psychosocial and Biochemical Methods. Totowa, NJ: Humana Press; 1992. [Google Scholar]
- 47.McGillicuddy NB, Rychtarik RG, Morsheimer ET, Burke-Storer MR. Agreement between parent and adolescent reports of adolescent substance use. J Child Adolesc Subst Abuse. 2007;16(4):59–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Waldron HB, Turner CW. Evidence-based psychosocial treatments for adolescent substance abuse. J Clin Child Adolesc Psychol. 2008;37(1):238–261. [DOI] [PubMed] [Google Scholar]
- 49.Ewing JA. Detecting alcoholism: The CAGE questionnaire. JAMA. 1984;252(14):1905–1907. [DOI] [PubMed] [Google Scholar]
- 50.Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alcohol screening tests among adolescents: A comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res. 2003;27(1):67–73. [DOI] [PubMed] [Google Scholar]
- 51.Winters KC, Anderson N, Bengston P, Stinchfield RD, Latimer WW. Development of a parent questionnaire for use in assessing adolescent drug abuse. J Psychoactive Drugs. 2000;32(1):3–13. [DOI] [PubMed] [Google Scholar]
- 52.Winters KC, Henly GA. Personal Experience Inventory and manual. Los Angeles: Western Psychological Services; 1989. [Google Scholar]
- 53.Green AE, Bekman NM, Miller EA, Perrott JA, Brown SA, Aarons GA. Parental awareness of substance use among youths in public service sectors. J Stud Alcohol Drugs. 2011;72(1):44–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bachman JG, Johnston LD, O’Malley PM. Monitoring the Future: Questionnaire responses from the nation’s high school seniors, 1984. Ann Arbor, MI: Institute for Social Research; 1985. [Google Scholar]
- 55.Winters KC. Development of an adolescent alcohol and other drug abuse screening scale: Personal Experience Screening Questionnaire. Addict Behav. 1992;17(5):479–490. [DOI] [PubMed] [Google Scholar]
- 56.Langhinrichsen J, Lichtenstein E, Seeley J, et al. Parent-adolescent congruence for adolescent substance use. J Youth Adolesc. 1990;19(6):623–635. [DOI] [PubMed] [Google Scholar]
- 57.Berge J, Sundell K, Öjehagen A, Höglund P, Håkansson A. Parental awareness of substance use among adolescents in a junior high school sample. J Drug Issues. 2015;45(3):263–278. [Google Scholar]
- 58.Chang F-C, Lee C-M, Miao N-F, et al. Parent-adolescent discrepancies in reports of adolescent tobacco and alcohol use associated with family relationships in Taiwan. J Subst Use. 2013;18(4):288–301. [Google Scholar]
- 59.Waldron HB, Slesnick N, Brody JL, Turner CW, Peterson TR. Treatment outcomes for adolescent substance abuse at 4- and 7-month assessments. J Consult Clin Psychol. 2001;69(5):802–813. [PubMed] [Google Scholar]
- 60.De Los Reyes A, Ohannessian CM, Racz SJ. Discrepancies between adolescent and parent reports about family relationships. Child Dev Perspect. 2019;13(1):53–58. [Google Scholar]
- 61.Latendresse SJ, Rose RJ, Viken RJ, Pulkkinen L, Kaprio J, Dick DM. Parenting mechanisms in links between parents’ and adolescents’ alcohol use behaviors. Alcohol Clin Exp Res. 2008;32(2):322–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Piehler TF, Winters KC. Parental involvement in brief interventions for adolescent marijuana use. Psychol Addict Behav. 2015;29(3):512–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.van den Eijnden R, van de Mheen D, Vet R, Vermulst A. Alcohol-specific parenting and adolescents’ alcohol-related problems: The interacting role of alcohol availability at home and parental rules. J Stud Alcohol Drugs. 2011;72(3):408–417. [DOI] [PubMed] [Google Scholar]