

Abstract
To evaluate the qualitative fitting characteristics of FFRs on Iranian people. 62 participants were fit tested qualitatively by four brands of FFRs, including three imported (A, B, and C) and one domestic (D). The respirators were assigned to the participants randomly based on the Latin Square design (LSD) using the Moldex® Bitrex® Fit Test Kit. R 3.2.5.0 software was used to analyze the data. Among the respirators, A and C respirators had the lowest and highest fit test passing rates with 1.60% and 43.50%, respectively. The majority of the participants had medium face sizes (45.20%) and small and long/narrow shapes (32.20% and 32.30%). There was a significant difference between the passing rate of domestic (D) and imported (C) respirators (p value<0.001). Factors including respirator brand, style, and gender had significant effects on respirator fit (p value<0.01). There was a low fit test passing rate of the studied respirators among participants. Furthermore, 19.40% of the participants fell out of the NIOSH fit test panel. Therefore, it is required to develop a unique bivariate fit test panel and design the respirators based on the Iranian facial dimensions. Meantime, manufacturers need to provide various sizes and styles of the respirators to provide adequate respiratory protection for the users.
Keywords: Qualitative fit testing. Filtering face-piece respirators. Respirator features. Subject characteristics. NIOSH bivariate fit test panel
Introduction
The most common respiratory hazards consisted of airborne dusts, fumes, mists, gases, vapors, smoke, etc.
There are situations in which the same that could be exposed by the workforces are also a potential concern to the non-occupational users, for example, air pollution, wildfires, indoor mold growth after a flood, and bacteria and viruses. In addition to the workforces, it is vital to public users to wear respirators while occurring the epidemic or pandemic infectious disease transmission such as Tuberculosis (TB), Influenza (e.g., H1N1) or during air pollution. Specifically, when vaccines are not yet available, the respirator use would be required [1].
There are various studies were performed regarding the respirators’ performance [2–11]. For instance, Mueller et al. concluded that both filter efficiency and proper respirator fitting into the face are vital to provide the optimal protection [8, 12]. As mentioned, apart from the respirator’s performance, the fit of the respirator on the user’s face is also of great importance in respiratory protection [5, 13, 14].
Fitting characteristics of the respirators became a prominent issue in recent years. It plays a substantial role in the respiratory protection program (RPP) to verify the adequate fit of a particular make, model, style, and size of a respirator into the facial dimensions of the target users. In other means, it assures that the wearers could don the respirators correctly and achieve the expected protection during use. Fit testing is mandated as a substantial part of the RPP based on the respiratory protection standards of Occupational Safety and Health Administration (OSHA) regulation 29 CFR 1910.134 [15, 16], American National Standards Institute (ANSI Z88–10) [17], and International Organization for Standardization (ISO) 16,975–3 [18]. Since the subject face comes in different sizes and shapes, it is essential to select a respirator that properly accommodated the wearers’ anatomical features [19]. Therefore, it is required to conduct fit testing for all of the subjects included in the RPP in the process of respirator selection. As reported by some studies, wearers’ training on the proper donning and doffing of the respirators, remarkably increased the fit test passing rate [20–25].
It should be noted that OSHA included the annual fit test requirement in the final rule because fit testing not only determines the adequacy of the face-piece seal but also provides an opportunity to check the acceptability of respirator fit. Furthermore, fit testing permits the employee to reduce the unnecessary discomfort and irritation by selecting the most comfortable respirator and improves users’ training about the proper procedures of respirator donning and doffing, as well, providing the opportunity to detect poorly FFRs is another reason for fit testing [26].
A respirator fit defined as an ability of the respiratory protective equipment (RPE) to protect the users’ respiratory protection system from the hazardous inhalational exposure to chemical particles or gases [19, 27]. Under the traditional “hierarchy of controls”, RPE is used as the last measure when process/material substitution; engineering control; and administrative control have been adopted [19].
There are two general fit testing methods, qualitative (QLFT) and quantitative (QNFT). Quantitative fit testing decreases the test subjectivity and provides a numerical indicator of fit called “fit factor” using an instrument to measure the leakage into respirator (Cout/Cin) while carrying out a set of standardized exercises [28–30]. Noticeably, this method has some advantages such as documentation of numerical results, no chance of user deception [31], and applicable to various classes of RPE [32]. Nevertheless, it might be time-consuming, expensive and not be easily available [26, 31], required experienced assessors, probed respirator or sampling adaptor, and annual factory recalibration [15, 17, 18].
Qualitative fit testing examines the subject’s ability to taste or smell the challenge agent while conducting the same set of standardized exercises. Four common challenge agents were as follows: Bitrex™, saccharin, isoamyl acetate, and irritant smoke. Similarly to saccharin, Bitrex™ utilized as a challenge agent for fit testing of FFRs [33, 34]. Irritant smoke used for high-efficiency particulate air (HEPA) or P100 filters [15] and isoamyl acetate (IAA), is widely used for respirators equipped with organic vapor (OV) cartridges or filters [15, 28].
The quality of a respirator fit to wearers depends on two factors: The fitting characteristics of a respirator and accuracy of the proposed fit testing method in order to ensure the acceptability of the wearers’ fit. Each fit testing method has specific errors, which in turn, inherent errors could cause the user’s respirator erroneously considered as a failure. Also, as the fitting characteristics of a particular respirator improves, the chance of a user’s respirator considered as a failure and fit testing error reduces [35].
Various factors, including respirator features and subject characteristics, could affect the respirator fit. For instance, the study conducted by Zhuang et al., showed that the number of sizes available for a model significantly affect the respirator fit, otherwise, the unacceptable fit of the respirator might give mistakenly the wearer reassurance that he/she protected efficiently [36]. Another study by Zhuang et al., represented “as the time between the fit tests increases, so does the risk of acceptable fit” [37], confirmed the annual fit testing. Some researches obtained different results from the effects of the respirator style on the fit test passing rate [38–40].
Furthermore, some evidence determined that facial anthropometric dimensions differ among ethnics and nationalities [26, 41, 42].
The NIOSH is responsible for certifying the respirators with good fitting characteristics to ensure that the users protected against the inhalational hazards [43]; to do so, NIOSH developed the bivariate fit test panel based on the face length and face width dimensions of the U.S. respirator user population. This panel determines the face size and shape of the users; more importantly, the correct size of the specific respirator [44].
Zhuang et al. pointed to the fact that the face length and face width would be as key facial dimensions for selecting the best respirator fitted into wearers’ face, besides, face size categories matched respirator sizing remarkably well [36]. Balkhyour et al. discussed that face shape played an important role in providing the optimal respirator fitted into the firefighters’ facial dimensions [45]. Oestenstad et al. reinforced that fit assessment of the different brands of respirators on the same subject resulted in significant differences in respirator fit [17]. According to the previous researches, age and gender have been considered as one of the important factors influencing the respirator fit [46]. The objective of this research is to determine the qualitatively fitting characteristics of the FFRs being tested on Iranian people’s faces.
Methods
Study design
We conducted an experimental study at Shiraz University of Medical Sciences, Iran in 2018.
Participants
Sixty-two students consisted of 37 females and 25 males with a mean age of 23.45 ± 4.66 years recruited in the study. The participants were participated randomly in the study, using proportional stratified sampling method based on educational level. The participants were tested in the Industrial Safety laboratory of the School of Health.
Ethical features
Ethical clearance was taken from the Research Ethics Committee of Shiraz University of Medical Sciences (approval code IR.SUMS.REC.1396.191). Before commencing the study, all participants were provided the verbal and written informed consent which included the approval code, consent statement, study purposes and procedures, and right to confidentiality and withdrawal. Before undertaking the investigation, we gave the participant a description of his/her responsibilities during the test procedure by playing two videos concerning the steps of QLFT procedure, including sensitivity test, user seal checks (USCs) and respirator fit testing procedures [35, 47].
Exclusion criteria
The exclusion criteria included the following: allergy to any substance; getting a cold; (3) nasal congestion; (4) cardiovascular or respiratory diseases (asthma, shortness of breath, dyspnea) [48]; stubble and beard; (6) facial deformity or scars; (7) facial surgery; (8) and plastic or rhinoplasty surgery. If the participants gave a wrong taste response to the test agent, Allegro saccharin fit test kit was used to perform the test.
Study procedure
All participants were prohibited from chewing gum, eating, and drinking (except for plain water) for at least 30 min before beginning the tests to ensure they could taste the sensitivity test solution. Meanwhile, the test conductor asked them to drink only plain water to obtain reliable results. All participants had a 5-min break to remove any taste’s residue of the challenge agent, too.
The participants were allocated randomly to the studied respirators based on the Latin Square Design (LSD). It aims to randomize the order of respirators being tested which was labeled randomly as A, B, C, and D, which were presented in Fig. 1. Totally, 248 qualitative fit tests were conducted on the participants (62 participants × 4 FFRs =248 qualitative fit tests).
Fig. 1.

Pictures of the studied FFRs
Measures
All participants were studied over four brands of FFRs which most widely used in Iran: one of the brands was domestic (D) and three of them were imported (A, B, and C). The commercial fit solutions were Moldex® Bitrex® Fit Test Kit Part number 0102 (Moldex Co., Culver, Calif.) contained 0.0135% denatonium benzoate, 94.9865% water, and 5% sodium chloride [49] and Allegro®.
saccharin Qualitative Fit test Kit Part Number 2040 (Allegro Industries, Paramount, Calif.) contained < 1% sodium saccharin and > 99% water [30].
The sensitivity test was conducted in accordance with the protocol contained in the OSHA respiratory protection standard, regulation 29 CFR 1910.134 [15], to assure that the participant being tested could detect the taste of aerosolized droplets of a dilute solution of Bitrex™ which involved placing an enclosure approximately 12 in. (30.5 cm) in diameter by 14 in. (35.6 cm) tall over a participant’s head, positioning the enclosure forward (a gap) about 6 in. (15.25 cm) between the participant’s face and enclosure window, and having a 0.75 in. (1.9 cm) hole in front of the participant’s nose and mouth area to help ensure the dispersion of the aerosol around the participant’s mouth and accommodate the nebulizer nozzle.
To start the intervention, the following steps were taken: Firstly, prior to conducting the sensitivity test, we instructed the participant to place the enclosure over the head without wearing a respirator, breathe only through their mouth slightly open with tongue extended, and report immediately when he/she could characterize the taste (not smell) of the challenge agent.
In the second step, the challenge agent was produced in the enclosure by firmly squeezing the nebulizer bulb. To do so, using the test solutions, we inserted the ten squeezes of the nebulizer bulb contained Bitrex™ aerosol into the hole in front of the enclosure by fully collapsing and expanding the bulb on each squeeze. In the third step, we asked the participant if he/she could detect the bitter taste of Bitrex™. Otherwise, we continued the procedure up to 30 squeezes. Also, the taste threshold was recorded as 10, 20 or 30 regardless of the numbers of squeezes actually completed. In other words, the threshold level per 1–10, 11–20, and 21–30 squeezes was high (L1), medium (L2), and low (L3), respectively. If the participant was unable to detect the bitter taste after 30 squeezes, the sensitivity test considered as a failure, therefore, we used the saccharin fit test kit. In the fourth step, the participant underwent the qualitative fit testing of the studied respirators. Thus, he/she conducted the USC procedures for at least 5 min before starting the fit test to ensure he/she properly adjusted those respirators. The features of the studied FFRs were presented in Table 1.
Table 1.
Features of studied Filtering Face-Piece Respirators (FFRS) used in the current study
| Respirator Code | Domestic or Imported | Filtering face-piece Level/type | Face-piece size(s) | Style | Valved Active Carbon pre-filter | Nose clip | Adjustable straps |
|---|---|---|---|---|---|---|---|
| A | Imported | FFP2 | OSFAa | Cup-shaped | Yes | Yes | No |
| B | N95/FFP2 | Flat-fold | Yes | ||||
| C | N95/FFP2 | Cup-shaped | No | ||||
| D | Domestic | N99/FFP3 | Flat-fold | Yes | Yes | Yes |
a One size fits all
If any participant consistently wore glasses, we asked him/her to do put on them during the test to assess whether they could interfere with respirator fit or not. The participant used the same enclosure as described in the first step while wearing the respirator. In the fifth step, a second nebulizer contained the Bitrex™ fit test solution was used to disperse the aerosol into the enclosure based on the number of squeezes reported by the participant during the sensitivity stage.
After that, the participant was trained to perform the fit tests exercises consisted sequence of normal breathing (NB), deep breathing (DB), turning head side to side (SS), moving head up and down (UD), talking (reading the “Rainbow Passage” loud), bending over (BO), and normal breathing for one minute each. The test conductor replenished the aerosol concentration every 30 s using one half of the initial number of squeezes used in the sensitivity test (e.g., 5, 10 or 15). If the participant didn’t report the taste of the fit test agent, the test was passed. If the taste of the agent was detected at any time during the fit test, the fit was deemed unsatisfactory [15].
Measurement of facial dimensions
To determine the participants’ face sizes and shapes, they were measured for two face dimensions based on the NIOSH bivariate fit test panel, including face length (Menton-sellion length) and face width (Bizygomatic breadth) using a calibrated Stainless Steel digital caliper (0–150-mm, accuracy: 0.01 mm, Model Number HB-101-111, Guanglu® Digital Caliper Manufacturer Co., Ltd., China). All measurements were made in millimeters to one decimal point, according to ISO ISO/TS 16976–2:2010 [36].To decrease the interpersonal variations, two key facial dimensions were measured three times by one investigator and mean values were recorded. The NIOSH bivariate panel consisted of 10 cells representing overall subjects’ face size. The mentioned cells were classified into three groups: small (cells 1–3), medium (cells 4–7), and large face size (cells 8–10). Also, the face shapes were categorized as follows: small (cells 1–3), medium (cells 4,7), long/narrow (cell 6), short/wide (cell 5), and large (cells 8–10) [50]. Eventually, if the overlapping percent between the subjects’ facial dimensions and fit test panel cells computed at least 90%; the NIOSH fit test panel would be considered appropriate for the Iranian people.
The demographic variables (age and gender, body weight, and height, facial dimensions), the results of sensitivity tests (threshold level, pass/fail), respirator features (make, model, and style), name of the challenge agent (Bitrex™ or saccharin), and results of fit tests (pass/fail) were recorded in the data sheet.
Statistical analysis
We took repeated measures on the participants and supposed that the observations were independent, so, Fixed Effect Logistic Regression (FELR) model was practiced. Moreover, the Mixed Effect Logistic Regression (MELR) model including random effects was proposed with the assumption that the repeated observations were correlated [51]. Meanwhile, these models were adjusted for age and gender, and BMI. Eventually, the results obtained from both FELR and MELR models were compared with each other.
Additionally, we calculated the Kappa statistics (k) to evaluate the significant agreement between the results of fit testing of the studied respirators [51] and the Chi-square test was used to assess the effects of respirator features and subject characteristics on respirator fit. Significant tests were set at an alpha value of 0.05 (α = 0.05). Data analysis were performed using R 3.2.5.0 software.
Results
Most of the study participants were female. The mean and standard deviation of the females’ facial dimensions were greater than those of males (Table 2).
Table 2.
Demographic characteristics of the study participants
| Subject characteristics | Gender | Total | |
|---|---|---|---|
| Male | Female | ||
| Age, mean ± SD (year) | 24.11 ± 5.85 | 22.94 ± 3.50 | 23.45 ± 4.66 |
| BMI, mean ± SD (kg/m2) | 23.10 ± 2.90 | 23.13 ± 3.71 | 23.12 ± 3.38 |
| Face length, mean ± SD (mm) | 117.16 ± 6.65 | 119.74 ± 6.60 | 118.70 ± 6.60 |
| Face width, mean ± SD (mm) | 120.16 ± 10.92 | 124.92 ± 10.32 | 123.0 ± 10.74 |
Of the study population, 57 participants characterized the bitter taste of Bitrex™ and 5 detected the sweet taste of saccharin at the threshold screening step.
In Table 3, descriptive statistics for fit test results obtained from the studied respirators were summarized. As can be seen, the majority of the fit tests were done on the participants, considered as a failure (84.27%). Interestingly, female participants had higher pass rates than males (10.48 vs. 5.24%).
Table 3.
Subjects with passing or failing fit test rates by respirator brand and gender
| Fit test result | Gender | Respirator brand | ∑N (%) | |||
|---|---|---|---|---|---|---|
| A N (%) |
B N (%) |
C N (%) |
D N (%) |
|||
| Passed | Male | 1 (0.40) | 0 | 11 (4.44) | 1 (0.40) | 13 (5.24) |
| Female | 0 | 6 (2.42) | 16 (6.45) | 4 (1.61) | 26 (10.48) | |
| Subtotal | 1 (0.40) | 6 (2.42) | 27 (10.89) | 5 (2.02) | 39 (15.73) | |
| Failed | Male | 24 (9.68) | 25 (10.08) | 14 (5.64) | 24 (9.68) | 87 (35.08) |
| Female | 37 (14.92) | 31 (12.5) | 21 (8.47) | 33 (13.30) | 122 (49.19( | |
| Subtotal | 61 (24.60) | 56 (22.58) | 35 (14.11) | 57 (22.98) | 209 (84.27) | |
As illustrated in Fig. 2a, A and C brands had the lowest and highest fit test passing rates, respectively (1.60 vs. 43.50%). Cup-shaped respirators had significantly higher pass rates than the flat-fold ones (71.80% vs. 28.20%) (Fig. 2b). The Chi-square test was utilized to determine if the proportions of the qualitative fit tests classified as a pass were different by the respirator features. Significant differences were observed between the respirator features and fit test passing rates (p value<0.003 for respirator brand; p value<0.001 for style).
Fig. 2.

Fit test passing rate by respirator brand (a) and style (b) among study participants
Table 4 compares the results of the QLFT of imported respirators against domestic one by FELR. As seen, a significant difference was revealed between the fit test results of the C and D brands (p value<0.001). On the other hand, the odds ratio (OR) for fit test passing rate of the C brand was 11.87 times the OR for the D one. Surprisingly, the male participants received a statistically lower proportion of passing qualitative fit tests than female participants (p value<0.01).
Table 4.
Results of fit testing of domestic (D) against imported (A, B, and C) respirators by FELR*
| Variable | Coefficient (β) | 95% CI for Coefficient | OR† | 95% CI for OR | |||
|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | ||||
| Respirator Brand | A | −0.12 | −4.71 | 0.16 | 0.18 | 0.009 | 1.18 |
| B | 0.74 | −1.08 | 1.54 | 1.24 | 0.34 | 4.68 | |
| C | 2.47* | 1.42 | 3.71 | 11.87 | 4.15 | 40.86 | |
| Subject characteristics | Face size | −0.005 | −0.8 | 0.17 | 0.99 | 0.83 | 1.19 |
|
Demographic variables |
Age | 0.03 | −0.05 | 0.12 | 1.03 | 0.95 | 1.12 |
| Gender | −1.64** | −2.62 | −0.74 | 0.19 | 0.07 | 0.48 | |
| BMI | −0.07 | −0.20 | 0.05 | 0.93 | 0.81 | 1.06 | |
*p value<0.001; **p value<0.01
However, the observed difference between the passing rate of the D brand and face size in this study was not significant. It means that there were no significant differences between the participants’ face sizes who passed or failed the fit test. Also, among the demographic variables, there was a statistically significant difference between the gender and fit test passing rate of the D brand.
The comparison of the QLFT results of studied respirators by MELR is set out in Table 5. As observed, there was a statistically significant difference between the brands of the C and D respirators by the fit test passing rates (p value<0.001). On the other hand, the OR for fit test passing rate of the C brand was 63.44 times the OR for the D brand. Moreover, there was no statistically significant difference between the D brand and face size.
Table 5.
Results of fit testing of domestic (D) against imported (A, B, and C) by MELR*
| Variable | Coefficient (β) | 95% CI for Coefficient | OR† | 95% CI for OR | |||
|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | ||||
| Respirator Brand | A | −2.49 | −5.15 | 0.18 | 0.08 | 0.006 | 1.19 |
| B | 0.34 | −1.28 | 1.96 | 1.40 | 0.28 | 7.12 | |
| C | 4.15* | 2.05 | 6.25 | 63.44 | 7.75 | 518.97 | |
| Subject characteristics | Face size | −0.01 | −0.38 | 0.35 | 1.18 | 0.69 | 1.42 |
| Demographic variables | Age | 0.08 | −0.10 | 0.26 | 1.08 | 0.90 | 1.29 |
| Gender | −2.77** | −4.97 | −0.56 | 0.06 | 0.007 | 0.57 | |
| BMI | −0.06 | −0.32 | 0.19 | 0.94 | 0.73 | 1.21 | |
*p value<0.001; **p value<0.01
In the present research, due to the existence of sparse data (low fit test passing rate), the MELR provided the wider bond than that of FELR for the proposed confidence interval (95% CI). The Kappa (k) statistics was examined the consistency between the results of qualitative fit testing of the imported and domestic respirators were as follow as: [A; 95% CI: 0.31(−0.16–0.79), B; 95% CI: 0.50 (0.12–0.88), C; 95% CI: 0.20 (.042 −0.37)].
Figure 3 points out that most of the participants’ facial dimensions fell within cells 4–7 of the NIOSH bivariate panel representing their medium face sizes.
Fig. 3.
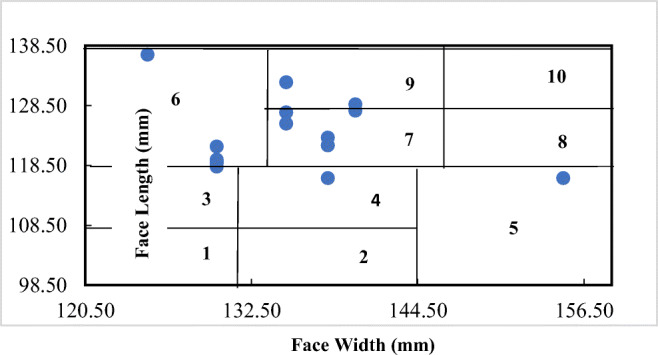
Distribution of study subjects in the NIOSH bivariate fit test panel
Based on the NIOSH bivariate fit test panel (Fig. 4), most of the study participants had medium face size (45.20%) and small and long/narrow shapes (32.20% and 32.30%). Besides, 12 (19.40%) of the study participants fell outside of the NIOSH bivariate fit test panel. The T-test showed no statistically significant differences between the mean values of the male and female participants’ facial dimensions.
Fig. 4.

Frequency of participants’ face size (a) and shape (b) based on the NIOSH bivariate fit test panel, respectively
The highest fit test passing rates corresponded to the participants with medium and small face sizes, respectively (38.50%) and participants with small and long/narrow shapes (38.50% and 30.80%, respectively) (Fig. 5).
Fig. 5.

Frequency of the respirator fit test passing rate by face size (a) and shape (b), respectively
Moreover, the Chi-square test showed no statistically significant differences between the participants’ face sizes and shapes by respirator fit.
Discussion
The major objective of this research was to investigate the qualitatively fitting characteristics of the FFRs on facial dimensions. The results showed a very low fit test passing rate (15.73%) among study participants. This result matches the results of some conducted studies [16, 18, 39, 52–56]. One of the possible explanations for this finding could be due to the size and style of the respirators being tested were not fitted the study subjects’ facial dimensions. In other words, “One size does not fit all” and it is necessary to provide more than one of the respirator models, styles, and sizes for the users to provide satisfactory protection. Most of the employers believe erroneously that respirator with one size will fit all employees, then, an inappropriately fitted or sized respirator may give the user a false sense of protection. In that case, it is necessary to promote the employers’ knowledge and attitudes regarding this fundamental problem [57].
Another explanation for the low fit test passing rate among study participants might be due to the failure performance of studied respirators’ filters and valves. On the other hand, there are no valid mechanisms or standards for respirators’ efficacy testing and certification like the NIOSH in the Iranian marketplaces in order to be tested and approved by the authorized bodies. Therefore, many users might be exposed to potential hazards while wearing respirators [58].
Another important finding was that the fit test passing rate of imported (C) respirator was higher than that of the other respirators including domestic (D) one. This finding is consistent with the findings of two studies conducted in South Korea [59, 60], stated that the performances of domestic respirators were inferior to those of imported ones; therefore, they considered the main reasons for this issue might be attributed to the inadequacy of the respirator certification program in Korea including specification of requirements for fit testing and establishment of fit test panel for face-seal leakage test. Moreover, Davies et al. supported this finding [61]. A possible explanation for this might be that each brand of respirator has specific fitting characteristics [17, 18, 30, 62]. Meanwhile, the C brand had the inner, soft and flexible layer which named sealing lip or nosepiece over the nose bridge; while the other brands had no such value. This lead to prevent from face seal leakage in the nasal area; thus, this respirator was fitted into face more efficiently. Also, the participants satisfied with wearing that. Moreover, it seems that the A respirator with cup style is more appropriate for the Korean, Chinese, or Japanese users who have short and wide faces than Iranian ones [26, 63].
Noticeably, the domestic (D) brand like the remained respirators designed based on the non-Iranian anthropometric databases. Other reasons for poor fitting characteristics of the studied respirators were related to the design, style of the respirators, and how to adjust to the subjects’ faces; not only face sizes. To do so, the quality features of the filter such as filter typology, the number of filter layers, and poor or well-fitting characteristics would be considered while using the respirator [6].
According to the obtained results from this study, females fitted to the studied respirators more significantly than males (p value<0.01). This finding confirmed the findings of previous works [37, 46]. Gross et al. reported that females’ fit was depended highly on the respirator’s brand [64]. However, some researches presented that the males fitted into the studied respirators than females, which seems that those respirators were more suitable for males than females [30, 46, 65–67]. The most important reason for the mentioned unconformity between the previous studies and current study would be that the selected respirators were more appropriate for females who usually have smaller faces than males. Although there are some contradicted findings regarding this issue, the researches conducted by Oestenstad et al. [17] and Spies et al. [16], showed no statistically significant differences between the males and females by respirator fit. Also, the study performed by Føreland et al., indicated that sex did not improve the fitting of the respirator model [68]. Accordingly, further works would be useful in order to assess the validity of this finding.
In this study, the cup-shaped respirators were significantly fitted into participants’ faces more than the flat-fold ones. Although this finding differs from some published studies conducted by Lin, et al. [38], Ciotti et al. [40], and Huh et al. [66] but this is consistent with the study of Jahangiri et al. [39]. Notably, Zhuang et al. found that the respirator style had no significant effect on respirator fit [36]. Among the evaluated respirators, the consistency between the fit test results of the B and D respirators was computed as the highest value (k = 0.50; moderate agreement); therefore, it stresses that the study participants fitted equally the mentioned respirators.
This study found no statistically significant differences between the demographic variables including age, BMI and respirator fit. This result supports the study of Danyluk et al. The reason considered due to the negligible change of people’s weight while increasing age [38]. In contrast, Zhuang et al. [42] and McMahon et al. [46] presented that age could affect the respirator fit. Zhuang et al. stated that the user’s physical changes while increasing age could have effects on the respirator fitting characteristics, therefore, it supports the OSHA requirement for annual fit testing [37]. Thereby, Føreland et al. [68] and Manganyi et al. [69] found that age had no significant effects on respirator fit. Because of the contradiction among the various studies concerning the effects of age and BMI on respirator fit, more studies are required to conduct.
Most of the participants had medium face sizes and small and long/narrow shapes (45.20%, 32.20%, respectively). Considerably, 19.40% of the study participants fell outside of the NIOSH bivariate fit test panel. This finding is consistent with the research of Jahangiri. et al. conducted on the Iranian people (22.50%, out of the panel) [39]. Additionally, some researches conducted in China, reported the higher proportions of the participants were out of the NIOSH fit test panel (12–35%, and 26.2%, respectively) [38, 41]. But the other Chinese study performed by Chen et al., noted that only 5.0% of the subjects were out of the NIOSH fit test panel boundaries [26].
It should be mentioned that according to the NIOSH study, the lowest overlapping percent between the subjects’ facial dimensions and fit test panel cells were considered 90%; as acceptable [50]. In the present study, the NIOSH fit test panel is not appropriate for the Iranian people and there is a crucial need to provide the comprehensive anthropometric database by measuring the facial dimensions of the Iranian users to develop a specific and optimal fit test panel.
The key limitation of this research was that due to the subjective nature of QLFT procedure, it is likely that the participants erroneously respond to the challenge agent in the steps of conducting QLFT, that’s why the fit test passing rate was too low. Another weakness of this study was that only four brands of OSFA respirators were evaluated, Thereby, it is possible that various results obtained from the larger groups of subjects of the different race with combinations of various make, model, style, and size of the respirators. Future studies of this issue would be of interest.
Conclusion
Taken together, the main finding from this paper was a low qualitative fit test passing rate of the respirators among studied subjects. Moreover, one of the imported respirators were fitted into face more efficiently than domestic one. Another implication, high proportions of the participants fell out of the NIOSH fit test panel cells. Therefore, it is required to not only the design of the respirators based on the Iranian facial dimensions, but also, develop exclusively the bivariate fit test panel for Iranian people. Meantime, it is confirmed the manufacturers required to prepare the various sizes and styles of the respirators to provide adequate respiratory protection for the target users.
Acknowledgements
We gratefully acknowledge all participants for their contribution to this research project.
Compliance with ethical standards
Conflict of interest
There is no conflict of interest.
Ethics approval and consent to participate
Informed consent forms were provided; Ethics approval IR.SUMS.REC.1396.191; Grant No. 1396-01-04-15,787.
Financial support
The present article was extracted from the thesis written by Anahita Fakherpour, MSc., a student of Occupational Health and was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran (Grant No. 1396-01-04-15,787).
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Ronald Shaffer JKC, Ginger Chew, LCDR Joy Hsu. Non-occupational Uses of Respiratory Protection – What Public Health Organizations and Users Need to Know. Centers for Disease Control and Prevention (CDC). 2018 Availabe from: https://blogs.cdc.gov/niosh-science-blog/2018/01/04/respirators-public-use/. Accessed 9 January 2020.
- 2.Cherrie JW, Apsley A, Cowie H, Steinle S, Mueller W, Lin C, Horwell CJ, Sleeuwenhoek A, Loh M. Effectiveness of face masks used to protect Beijing residents against particulate air pollution. Occup Environ Med. 2018;75(6):446–452. doi: 10.1136/oemed-2017-104765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Guan T, Hu S, Han Y, Wang R, Zhu Q, Hu Y, Fan H, Zhu T. The effects of facemasks on airway inflammation and endothelial dysfunction in healthy young adults: a double-blind, randomized, controlled crossover study. Particle and fibre toxicology. 2018;15(1):30. doi: 10.1186/s12989-018-0266-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jung H, Kim J, Lee S, Lee J, Kim J, Tsai P, et al. Comparison of filtration efficiency and pressure drop in anti-yellow sand masks, quarantine masks, medical masks, general masks, and handkerchiefs. Aerosol Air Qual Res. 2014;14(14):991–1002. [Google Scholar]
- 5.Mueller W, Horwell CJ, Apsley A, Steinle S, McPherson S, Cherrie JW, Galea KS. The effectiveness of respiratory protection worn by communities to protect from volcanic ash inhalation. Part I: filtration efficiency tests. Int J Hyg Environ Health. 2018;221(6):967–976. doi: 10.1016/j.ijheh.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 6.Pacitto A, Amato F, Salmatonidis A, Moreno T, Alastuey A, Reche C, Buonanno G, Benito C, Querol X. Effectiveness of commercial face masks to reduce personal PM exposure. Sci Total Environ. 2019;650:1582–1590. doi: 10.1016/j.scitotenv.2018.09.109. [DOI] [PubMed] [Google Scholar]
- 7.Rengasamy S, Eimer BC. Total inward leakage of nanoparticles through filtering facepiece respirators. Ann Occup Hyg. 2011;55(3):253–263. doi: 10.1093/annhyg/meq096. [DOI] [PubMed] [Google Scholar]
- 8.Rengasamy S, Walbert GF, Newcomb WE, Faulkner K, Rengasamy MM, Brannen JJ, et al. Total inward leakage measurement of particulates for N95 filtering facepiece respirators—a comparison study. Ann Occup Hyg. 2014;58(2):206–216. doi: 10.1093/annhyg/met054. [DOI] [PubMed] [Google Scholar]
- 9.Rengasamy S, Zhuang Z, Niezgoda G, Walbert G, Lawrence R, Boutin B, Hudnall J, Monaghan WP, Bergman M, Miller C, Harris J, Coffey C. A comparison of total inward leakage measured using sodium chloride (NaCl) and corn oil aerosol methods for air-purifying respirators. J Occup Environ Hyg. 2018;15(8):616–627. doi: 10.1080/15459624.2018.1479064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shakya KM, Noyes A, Kallin R, Peltier RE. Evaluating the efficacy of cloth facemasks in reducing particulate matter exposure. Journal of exposure science & environmental epidemiology. 2017;27(3):352–357. doi: 10.1038/jes.2016.42. [DOI] [PubMed] [Google Scholar]
- 11.Steinle S, Sleeuwenhoek A, Mueller W, Horwell CJ, Apsley A, Davis A, Cherrie JW, Galea KS. The effectiveness of respiratory protection worn by communities to protect from volcanic ash inhalation. Part II: Total inward leakage tests. Int J Hyg Environ Health. 2018;221(6):977–984. doi: 10.1016/j.ijheh.2018.03.011. [DOI] [PubMed] [Google Scholar]
- 12.Program concept for total inward leakage (TIL) performance requirements and test methods NIOSH ,2004. Available from http://www.cdc.gov/niosh/npptl/standardsdev/til/. Accessed 14 April 2020.
- 13.Jahangiri M, Shahtaheri SJ, Adl J, Rashidi A, Kakooei H, Forushani AR, et al. Preparation of activated carbon from walnut shell and its utilization for manufacturing organic-vapour respirator cartridge. Fresenius Environ Bull. 2012;21(6a):1508–1514. [Google Scholar]
- 14.Jahangiri M, Adl J, Shahtaheri SJ, Rashidi A, Ghorbanali A, Kakooe H, Forushani AR, Ganjali MR. Preparation of a new adsorbent from activated carbon and carbon nanofiber (AC/CNF) for manufacturing organic-vacbpour respirator cartridge. Journal of environmental health science & engineering. 2013;10(1):15. doi: 10.1186/1735-2746-10-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.(OSHA) OSaHA. Title 29 CFR.1910.134 . Respiratory protection program Standards- Fit Testing Procedures (Mandatory). Washington, Occupational Safety & Health Administration (OSHA), Government Publishing Office. [Standard]. 2016.
- 16.Spies A, Wilson KS, Ferrie R. Respirator fit of a medium mask on a group of south Africans: a cross-sectional study. Environ Health. 2011;10(1):17. doi: 10.1186/1476-069X-10-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Oestenstad RK, Elliott LJ, Beasley TM. The effect of gender and respirator brand on the association of respirator fit with facial dimensions. J Occup Environ Hyg. 2007;4(12):923–930. doi: 10.1080/15459620701709619. [DOI] [PubMed] [Google Scholar]
- 18.Lawrence RB, Duling MG, Calvert CA, Coffey CC. Comparison of performance of three different types of respiratory protection devices. J Occup Environ Hyg. 2006;3(9):465–474. doi: 10.1080/15459620600829211. [DOI] [PubMed] [Google Scholar]
- 19.Racz L, Yamamoto DP. Eninger RM. Handbook of Respiratory Protection: Safeguarding Against Current and Emerging Hazards. CRC Press; 2017. [Google Scholar]
- 20.Jahangiri MMA, H. Assessment of factors influencing on fitting half-facepiece respirators in workers of a chemical industry 01st International Conference on Ergonomics.
- 21.Jahangiri MMA, H. Assessment of fitting half-facepiece respirators in IRANIAN workers of a petrochemical industry. Hormozgan Medical Journal. 1388(1).
- 22.Winter S, Thomas JH, Stephens DP, Davis JS. Particulate face masks for protection against airborne pathogens - one size does not fit all: an observational study. Critical care and resuscitation : journal of the Australasian Academy of Critical Care Medicine. 2010;12(1):24–27. [PubMed] [Google Scholar]
- 23.Hannum D, Cycan K, Jones L, Stewart M, Morris S, Markowitz SM, Wong ES. The effect of respirator training on the ability of healthcare workers to pass a qualitative fit test. Infection Control & Hospital Epidemiology. 1996;17(10):636–640. doi: 10.1086/647195. [DOI] [PubMed] [Google Scholar]
- 24.Lee M, Takaya S, Long R, Joffe A. Respirator-fit testing: does it ensure the protection of healthcare workers against respirable particles carrying pathogens? Infection Control & Hospital Epidemiology. 2008;29(12):1149–1156. doi: 10.1086/591860. [DOI] [PubMed] [Google Scholar]
- 25.Myong J-P, Byun J, Cho Y, Seo H-K, Baek J-E, Koo J-W, et al. The education and practice program for medical students with quantitative and qualitative fit-test for respiratory protective equipment. Ind Health. 2015. [DOI] [PMC free article] [PubMed]
- 26.Chen W, Zhuang Z, Benson S, Du L, Yu D, Landsittel D, et al. New respirator fit test panels representing the current Chinese civilian workers. Ann Occup Hyg. 2009;53(3):297–305. doi: 10.1093/annhyg/men089. [DOI] [PubMed] [Google Scholar]
- 27.Rajhans GS, Pathak BP. Practical guide to respirator usage in industry 2ed. Butterworth-Heinemann, Woburn: Respiratory Protection Program; 2002. [Google Scholar]
- 28.Mullins HE, Danisch SG, Johnston AR. Development of a new qualitative test for fit testing respirators. Am Ind Hyg Assoc J. 1995;56(11):1068–1073. doi: 10.1080/15428119591016278. [DOI] [PubMed] [Google Scholar]
- 29.Janssen LL, Luinenburg DM, Mullins HE, Nelson TJ. Comparison of three commercially available fit-test methods. AIHA journal : a journal for the science of occupational and environmental health and safety. 2002;63(6):762–767. doi: 10.1080/15428110208984767. [DOI] [PubMed] [Google Scholar]
- 30.Lam SC, Lee JK, Yau SY, Charm CY. Sensitivity and specificity of the user-seal-check in determining the fit of N95 respirators. The Journal of hospital infection. 2011;77(3):252–256. doi: 10.1016/j.jhin.2010.09.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.TSI. Introduction to Respirator Fit Testing. Available from www.tsi.com/uploadedFiles/_Site_Root/Products/Literature/...Notes/iti_070.pdf. Shoreview, MN USA 11/11/2015.
- 32.Coffey CC, Lawrence RB, Zhuang Z, Campbell DL, Jensen PA, Myers WR. Comparison of five methods for fit-testing N95 filtering-facepiece respirators. Appl Occup Environ Hyg. 2002;17(10):723–730. doi: 10.1080/10473220290107002. [DOI] [PubMed] [Google Scholar]
- 33.McKay RT, Davies E. Capability of respirator wearers to detect aerosolized qualitative fit test agents (sweetener and Bitrex) with known fixed leaks. Appl Occup Environ Hyg. 2000;15(6):479–484. doi: 10.1080/104732200301269. [DOI] [PubMed] [Google Scholar]
- 34.Liau Y-H, Bhattacharya A, Ayer H, Miller C. Determination of critical anthropometric parameters for design of respirators. The American Industrial Hygiene Association Journal. 1982;43(12):897–899. doi: 10.1080/15298668291410774. [DOI] [PubMed] [Google Scholar]
- 35.Campbell D, Coffey C, Lenhart S. Respiratory protection as a function of respirator fitting characteristics and fit-test accuracy. AIHAJ-American Industrial Hygiene Association. 2001;62(1):36–44. doi: 10.1080/15298660108984607. [DOI] [PubMed] [Google Scholar]
- 36.Zhuang Z, Coffey CC, Ann RB. The effect of subject characteristics and respirator features on respirator fit. J Occup Environ Hyg. 2005;2(12):641–649. doi: 10.1080/15459620500391668. [DOI] [PubMed] [Google Scholar]
- 37.Zhuang Z, Bergman M, Brochu E, Palmiero A, Niezgoda G, He X, Roberge R, Shaffer R. Temporal changes in filtering-facepiece respirator fit. J Occup Environ Hyg. 2016;13(4):265–274. doi: 10.1080/15459624.2015.1116692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lin YC, Chen CP. Characterization of small-to-medium head-and-face dimensions for developing respirator fit test panels and evaluating fit of filtering facepiece respirators with different faceseal design. PLoS One. 2017;12(11):e0188638. doi: 10.1371/journal.pone.0188638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Honarbakhsh M, Jahangiri M, Ghaem H, Ghorbani M, Omidvari F, Khorasani MA et al. Qualitative fit testing of medium-size N95/FFP2 respirators on iranian health care workers health scope 2018;7(4).
- 40.Ciotti C, Pellissier G, Rabaud C, Lucet JC, Abiteboul D, Bouvet E. Effectiveness of respirator masks for healthcare workers, in France. Med Mal Infect. 2012;42(6):264–269. doi: 10.1016/j.medmal.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 41.Yang L, Shen H, Wu G. Racial differences in respirator fit testing: a pilot study of whether American fit panels are representative of Chinese faces. Ann Occup Hyg. 2007;51(4):415–421. doi: 10.1093/annhyg/mem005. [DOI] [PubMed] [Google Scholar]
- 42.Zhuang Z, Landsittel D, Benson S, Roberge R, Shaffer R. Facial anthropometric differences among gender, ethnicity, and age groups. Ann Occup Hyg. 2010;54(4):391–402. doi: 10.1093/annhyg/meq007. [DOI] [PubMed] [Google Scholar]
- 43.NIOSH U. Particulates not Otherwise Regulated, Total. 0500. NMAM (NIOSH Manual of Analytical Methods). 1994;4.
- 44.Zhuang Z, Groce D, Ahlers HW, Iskander W, Landsittel D, Guffey S, Benson S, Viscusi D, Shaffer RE. Correlation between respirator fit and respirator fit test panel cells by respirator size. J Occup Environ Hyg. 2008;5(10):617–628. doi: 10.1080/15459620802293810. [DOI] [PubMed] [Google Scholar]
- 45.Balkhyour MA. Evaluation of full-facepiece respirator fit on fire fighters in the municipality of Jeddah, Saudi Arabia. Int J Environ Res Public Health. 2013;10(1):347–360. doi: 10.3390/ijerph10010347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.McMahon E, Wada K, Dufresne A. Implementing fit testing for N95 filtering facepiece respirators: practical information from a large cohort of hospital workers. Am J Infect Control. 2008;36(4):298–300. doi: 10.1016/j.ajic.2007.10.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zhuang Z, Bradtmiller B, Shaffer RE. New respirator fit test panels representing the current US civilian work force. J Occup Environ Hyg. 2007;4(9):647–659. doi: 10.1080/15459620701497538. [DOI] [PubMed] [Google Scholar]
- 48.3M and the science of fit testing available from: https://workersafety.3m.com/3m-and-the-science-of-fit-testing/.Accessed 2 January 2020., 3M United States September 6, 2016.
- 49.Coffey CC, Lawrence RB, Campbell DL, Zhuang Z, Calvert CA, Jensen PA. Fitting characteristics of eighteen N95 filtering-facepiece respirators. J Occup Environ Hyg. 2004;1(4):262–271. doi: 10.1080/15459620490433799. [DOI] [PubMed] [Google Scholar]
- 50.Zhuang Z, Bradtmiller B, Shaffer RE. New respirator fit test panels representing the current U.S. civilian work force. J Occup Environ Hyg. 2007;4(9):647–659. doi: 10.1080/15459620701497538. [DOI] [PubMed] [Google Scholar]
- 51.Agresti A. Categorical data analysis. 2nd ed. Gainesville: University of Florida; 2002.
- 52.Cho T-L, Li K-C, Huang C-C, Chuang L-L, Chiang C-Y, Tsai C-C et al. Qualitative fit test of N95 facial masks for medical staff. Journal of Microbiology, Immunology and Infection. 2015;48(2):S76.
- 53.Clapham SJ. Comparison of N95 disposable filtering facepiece fits using bitrex qualitative and TSI Portacount quantitative fit testing. Int J Occup Environ Health. 2000;6(1):50–55. doi: 10.1179/oeh.2000.6.1.50. [DOI] [PubMed] [Google Scholar]
- 54.Coffey C, Zhuang Z, Campbell D. Evaluation of the Bitrix™ qualitative fit test method using N95 filtering-Facepiece respirators. J Int Soc Respir Prot. 1998;16(1/4):48–55. [Google Scholar]
- 55.Niemandt M. Use and fit of filtering facepiece respirators in a department of anaesthesiology. 2018. [Google Scholar]
- 56.Ann RB. NIOSH investigation of 3M model 8000 filtering facepiece respirators as requested by the California Occupational Safety and Health Administration, Division of Occupational Safety and Health. US Department of Health and Human Services, Centers for Disease Control and …; 2010.
- 57.Manganyi MJ. A study of respirator fit and face sizes of National Health Laboratory Service (NHLS) respirator users during 2013–2014. 2015. [Google Scholar]
- 58.Respirator Certification Fees Final Rule. The National Personal Protective Technology Laboratory (NPPTL), USA,Available from https://www.cdc.gov/niosh/npptl/respcertfee.htm. 2018.
- 59.Han DH. Correlation of fit factors for respirators and anthropometric dimension. Korean J Prev Med. 1998;31(3):440–448. [Google Scholar]
- 60.Hyunwook K, Don-Hee H, Young-Man R, Kangyoon K, Yong-Gyu P. Facial anthropometric dimensions of Koreans and their associations with fit of quarter-mask respirators. Ind Health. 2003;41(1):8–18. doi: 10.2486/indhealth.41.8. [DOI] [PubMed] [Google Scholar]
- 61.Davies A, Thompson K-A, Giri K, Kafatos G, Walker J, Bennett A. Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster medicine and public health preparedness. 2013;7(4):413–418. doi: 10.1017/dmp.2013.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Earle-Richardson G, Fiske T, Wyckoff S, Shuford J, May J. Respiratory fit testing for farmworkers in the black dirt region of Hudson Valley. New York Journal of agromedicine. 2014;19(4):346–353. doi: 10.1080/1059924X.2014.945711. [DOI] [PubMed] [Google Scholar]
- 63.Du L, Zhuang Z, Guan H, Xing J, Tang X, Wang L, et al. Head-and-face anthropometric survey of Chinese workers. Ann Occup Hyg. 2008;52(8):773–782. doi: 10.1093/annhyg/men056. [DOI] [PubMed] [Google Scholar]
- 64.Gross SF, Horstman SW. Half-mask respirator selection for a mixed worker group. Appl Occup Environ Hyg. 1990;5(4):229–235. [Google Scholar]
- 65.Kim H, Han DH, Roh YM, Kim K, Park YG. Facial anthropometric dimensions of Koreans and their associations with fit of quarter-mask respirators. Ind Health. 2003;41(1):8–18. doi: 10.2486/indhealth.41.8. [DOI] [PubMed] [Google Scholar]
- 66.Huh YJ, Jeong HM, Lim J, Park HY, Kim MY, Oh HS et al. Fit characteristics of N95 filtering facepiece respirators and the accuracy of the user seal check among Koreans. infection control & hospital epidemiology. 2018;39(1):104–7. [DOI] [PubMed]
- 67.Han D-H. Fit factors for quarter masks and facial size categories. Ann Occup Hyg. 2000;44(3):227–234. [PubMed] [Google Scholar]
- 68.Føreland S, Robertsen Ø, Hegseth MN. Do various respirator models fit the workers in the Norwegian smelting industry? Safety and health at work. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Manganyi J, Wilson KS, Rees D. Quantitative respirator fit, face sizes, and determinants of fit in south African diagnostic laboratory respirator users. Annals of work exposures and health. 2017;61(9):1154–1162. doi: 10.1093/annweh/wxx077. [DOI] [PubMed] [Google Scholar]