

Key Points
Question
What is the effect of routine Global Registries of Acute Coronary Events risk score (GRS) implementation on guideline-indicated treatments and clinical outcomes of hospitalized patients with acute coronary syndrome?
Findings
In this cluster randomized clinical trial that included 2318 participants, routine GRS implementation was associated with an increase in early invasive treatment but not other aspects of care. With study cessation owing to futility, this influence on practice was not associated with a significant reduction in death and myocardial infarction over 12-month follow-up.
Meaning
The routine use of the GRS may increase the use of an early invasive strategy but not other aspects of care, and further larger studies are required to evaluate late clinical effect.
Abstract
Importance
Although international guidelines recommend use of the Global Registries of Acute Coronary Events (GRACE) risk score (GRS) to guide acute coronary syndrome (ACS) treatment decisions, the prospective utility of the GRS in improving care and outcomes is unproven.
Objective
To assess the effect of routine GRS implementation on guideline-indicated treatments and clinical outcomes of hospitalized patients with ACS.
Design, Setting, and Participants
Prospective cluster (hospital-level) randomized open-label blinded end point (PROBE) clinical trial using a multicenter ACS registry of acute care cardiology services. Fixed sampling of the first 10 patients within calendar month, with either ST-segment elevation or non–ST-segment elevation ACS. The study enrolled patients from June 2014 to March 2018, and data were analyzed between February 2020 and April 2020.
Interventions
Implementation of routine risk stratification using the GRS and guideline recommendations.
Main Outcomes and Measures
The primary outcome was a performance score based on receipt of early invasive treatment, discharge prescription of 4 of 5 guideline-recommended pharmacotherapies, and cardiac rehabilitation referral. Clinical outcomes included a composite of all-cause death and/or myocardial infarction (MI) within 1 year.
Results
This study enrolled 2318 patients from 24 hospitals and was stopped prematurely owing to futility. Of the patients enrolled, median age was 65 years (interquartile range, 56-74 years), 29.5% were women (n = 684), and 62.9% were considered high risk (n = 1433). Provision of all 3 measures among high-risk patients did not differ between the randomized arms (GRS: 424 of 717 [59.9%] vs control: 376 of 681 [55.2%]; odds ratio [OR], 1.04; 95% CI, 0.63-1.71; P = .88). The provision of early invasive treatment was increased compared with the control arm (GRS: 1042 of 1135 [91.8%] vs control: 989 of 1183 [83.6%]; OR, 2.26; 95% CI, 1.30-3.96; P = .004). Prescription of 4 of 5 guideline-recommended pharmacotherapies (GRS: 864 of 1135 [76.7%] vs control: 893 of 1183 [77.5%]; OR, 0.97; 95% CI, 0.68-1.38) and cardiac rehabilitation (GRS: 855 of 1135 [75.1%] vs control: 861 of 1183 [72.8%]; OR, 0.68; 95% CI, 0.32-1.44) were not different. By 12 months, GRS intervention was not associated with a significant reduction in death or MI compared with the control group (GRS: 96 of 1044 [9.2%] vs control: 146 of 1087 [13.4%]; OR, 0.66; 95% CI, 0.38-1.14).
Conclusions and Relevance
Routine GRS implementation in cardiology services with high levels of clinical care was associated with an increase in early invasive treatment but not other aspects of care. Low event rates and premature study discontinuation indicates the need for further, larger scale randomized studies.
Trial Registration
anzctr.org.au Identifier: ACTRN12614000550606
This randomized clinical trial assesses the effect of routine Global Registries of Acute Coronary Events risk score implementation on guideline-indicated treatments and clinical outcomes of hospitalized patients with acute coronary syndrome.
Introduction
The assessment of patient-specific risks provides a rational basis for the selective use of clinical therapies that are associated with both benefits and harms. Yet in the treatment of acute coronary syndromes (ACS), as with other areas of medicine, ample evidence indicates that risk stratification based on clinician intuition alone is imprecise when compared with objective risk scores.1,2,3,4,5,6 In ACS care, the discriminatory capacity of Global Registries of Acute Coronary Events (GRACE) risk scores (GRS) is superior to other risk models.5,7,8 However, there is limited prospective evidence assessing the effect of routine risk assessment in the treatment of ACS, contributing to varied implementation of risk scoring in clinical practice. Nevertheless, incorporating risk stratification into the planning of ACS treatment has been strongly advocated in clinical guidelines for several decades, albeit supported by a weak level of evidence.9,10
Few studies have prospectively assessed the effect of risk assessment in the treatment of ACS, contributing to the varied implementation of risk scoring in routine practice. Given the practice-level intervention, this provides the rationale for conducting a prospective cluster randomized clinical trial evaluating the effect of routine risk assessment using the GRS on use of guideline-recommended therapies and patient-level clinical events within ACS care.
Methods
Study Design
The Australian GRACE Risk Score Intervention Study (AGRIS) used a prospective cluster (hospital-level) randomized open-label blinded end point evaluation design to evaluate whether the GRS and associated treatment recommendations improved measures of hospital-level performance and clinical events over 12 months. Details of the protocol have been described previously.11 The trial was nested within the established Cooperative National Registry of Acute Coronary Care, Guideline Adherence and Clinical Events (CONCORDANCE) registry of patients with ACS, which was designed to evaluate the quality of care among representative Australian hospitals.12 The study was approved by the Sydney Local Health District Human Research Ethics Committee–Concord Repatriation General Hospital on March 19, 2014, and subsequently approved by the human research ethics committee and/or governance office of each participating institution. The study was conducted by the CONCORDANCE team at Concord Hospital, Sydney, New South Wales, Australia, and with independent clinical end point adjudication and data safety monitoring committees. Implementation of the GRS and treatment recommendation plan was provided by Flinders University Health Data Science Clinical Trials, Adelaide, South Australia. In March 2018, while the study was nearing completion, an unplanned interim analysis demonstrated likely futility in observing a difference in the primary end point. Consequently, the study was discontinued prematurely and the enrolled participants were followed up for a further 12 months. The formal trial protocols can be found in Supplement 1. Individual patient participation in the study used opt-out written consent.
Hospitals Randomization
Hospitals with continual onsite emergency and cardiology services willing to implement the GRS and treatment recommendation plan into their routine care, but without an existing risk stratification decision support system for patients with ACS, were approached to participate. Cluster randomization to either intervention or usual care was undertaken at the hospital level. Hospitals were block randomized by rural and metropolitan location using a centrally controlled numbered sequence. Randomized allocation was only revealed to each hospital after all ethics and governance documentation was complete and the local cluster custodian was ready to commence.
Participants
Patients with ACS presentation were eligible if they presented with 24 hours of onset, with symptoms consistent with acute cardiac ischemia for greater than 10 minutes and 1 of either electrocardiogram (ECG) changes consistent with coronary ischemia; an elevation in cardiac troponin T or I; or had a documented history of coronary artery disease. Furthermore, among patients without troponin elevation or ECG changes, at least 2 of the following characteristics were required: hemodynamic compromise (systolic blood pressure <90 mm Hg and heart rate [HR] >100 bpm); left ventricular ejection fraction less than 0.40; diabetes; or estimated glomerular filtration rate less than 60 mL/min per 1.73 m2. Patients were excluded if the clinical presentation was secondary to another concomitant illness (ie, type 2 MI), periprocedural or postoperative MI, or previously included in the study.12 Full details of the patient inclusion and exclusion criteria have been published.11 Each site included the first 10 patients presenting within each calendar month, regardless of acuity or survival as implemented in the GRACE registry.
Intervention and Control
For hospitals randomized to the intervention arm, the GRS and treatment recommendation plan was implemented into clinical care as a paper-based risk stratification worksheet with simple treatment recommendations aligned with clinical guidelines, which was incorporated into the patient record and available to all treating clinicians.9,10 Hospital services were required to undertake patient-level clinical assessment and then complete the GRS worksheet as part of the patient admission process. Management recommendations for early angiography with revascularization at clinical discretion, antithrombotic therapies, secondary prevention therapies, and referral to cardiac rehabilitation were provided. Four components of the intervention included calculation of the estimated risk of 6-month mortality and bleeding risk using the GRS and Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines (CRUSADE) registry risk score7,8,13; presentation of a nomogram classifying the individual patient as low, intermediate, or high risk of ischemic events and bleeding; treatment recommendations based on the degree of predicted ischemic risk; and a requirement for the admitting medical and nursing staff to document intended treatments (eFigure in Supplement 2).
The implementation team explored local care processes and facilitated the changes in the admission documentation to incorporate the study worksheet. Implementation of these changes occurred over 3 months with the engagement of local leading clinicians and structured meeting and information sessions. During this time, data collection by staff who were independent of those involved with intervention implementation continued, and uptake of the worksheet was confirmed by the embedded CONCORDANCE data collection process. Active participant inclusion commenced when the hospital assigned to the intervention demonstrated greater than 90% uptake of the GRS worksheet in a consecutive audit. Hospitals randomized to standard care continued the routine inclusion of patients with ACS into the registry, with participant inclusion commencing after local approvals were gained. No additional study-related education or training was provided, and individual clinician access to the GRS calculator was not precluded. Follow-up visits were performed via telephone, patient letter, and/or primary care physician contact.
Outcomes
The primary end point was receipt of all of the following quality indicators defined as (1) receipt of early invasive treatment during the index hospitalization; (2) prescription of at least 4 of 5 clinical guideline–recommended therapies at discharge (aspirin ≥100 mg/d, β-hydroxy β-methylglutaryl-CoA reductase inhibitor [statin], β-blocker, P2Y12 inhibitor, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker where there was a history of hypertension, diabetes, or known left ventricular impairment) if there is no stated contraindication (patients with a stated contraindication were coded as compliant); and (3) referral to cardiac rehabilitation.9,10,14 These criteria were also evaluated both separately and aggregated to a possible score of 3. In-hospital events reported included all-cause death, new or recurrent MI, recurrent ischemia, cardiac arrest, ventricular arrhythmias, and heart failure and stroke. All-cause mortality, new or recurrent MI, heart failure and stroke, the composite of all-cause death and/or MI, and death, MI, and/or stent thrombosis observed over 12-month follow-up in the entire population are also reported.
Determination of Sample Size
The study originally planned to engage 30 hospitals (15 per arm) and enroll at least 40 high-risk patients per hospital (ie, n = 1200 high-risk patients) but also anticipated that only 40% of patients with ACS within the registry would be considered high risk, thus requiring a total n = 3000.11 Previously observed rates in the registry of invasive treatment, 4 of 5 medications, and cardiac rehabilitation referral were 73%, 42%, and 51% respectively. However, challenges in site recruitment and a greater-than-expected rate of high-risk patients required a reestimation of sample size using more contemporaneous registry data. The data demonstrated mean performance score of high-risk patients (GRS >118) was 2.10. Hence, a sample size of 12 sites per study arm with 28 high-risk patients per site was calculated to achieve an 80% power to detect a difference in the total score of 0.5 between the group means when the standard deviation is 0.92 and the intracluster correlation is 0.176, using 2-sided t test with a significance level of .05.
Owing to slow site recruitment, the Study Executive Committee requested that the data safety monitoring board perform an assessment of the trial’s likelihood of detecting difference in the primary end point after 1237 high-risk patients had been enrolled. The data safety monitoring board deemed that based on current differences in the primary end point, continuation of the study would be futile, and enrollment ceased.
Statistical Analyses
Baseline descriptive statistics, aspects of ACS care, and clinical outcomes are reported as counts and percentages for dichotomous and categorical variables and were compared by the χ2 test adjusted for the clustered design (Rao-Scott test).15 Continuous variables were reported as medians (25th-75th percentile) compared by the Mann-Whitney U test. The discriminatory capacity of the GRS was reconfirmed using logistic regression and a receiver operating characteristic curve and reported as a C statistic. The primary analysis examined the efficacy of the GRS intervention vs standard care in improving the primary performance measure end point among patients with ACS with a GRS greater than 118 and alive at discharge. Exploratory analysis examined the provision of early invasive treatment among patients stratified by GRS greater than 140. Time to angiography between groups among patients with non–ST-segment elevation myocardial infarction was examined in a Cox proportional hazards model with shared frailty to account for clustering within hospitals. To assess for differences in provision of aspects of ACS care and clinical outcomes, generalized estimating equations with log link and binomial family were used to account for correlated outcomes within hospitals. Differences in performance measures was also assessed in all enrolled patients alive at discharge, while differences in mortality, MI, and the composite end point of death or MI over 12 months was assessed in the entire population using the same methods. Secondary analysis explored the interaction between key baseline characteristics (high-risk status [GRS >118], being older than 75 years, female, having diabetes, prior heart failure, and presentation to a rural hospital) and the association between use of the GRS and the complete provision of guideline-recommended therapies, as well as the provision of invasive treatment. However, given the study was powered to address clinical events and ceased for futility, inference regarding clinical events is subject to a greater type II error rate, and these results should be interpreted with caution. A P value of less than .05 (2-tailed) was considered statistically significant, and all analyses were undertaken using Stata, version 15.1 (StataCorp).
Results
Hospitals and Patient Characteristics
Of the 43 hospitals in the network, 17 declined to participate and 2 had already deployed risk scoring. Hence, this study enrolled 2318 patients from 24 hospitals (12 active and 12 control; median patients per hospital: 89; range, 56-142) (Figure 1). Of the hospitals, 16 were from metropolitan centers. All hospitals had cardiology services, cardiac catheterization laboratories, echocardiographic capability, and cardiology training programs. Among the patients enrolled, the median age was 65 years (range, 56-74 years), and 29.5% were female (n = 684), while 1433 (62.9%) were considered high risk using the trial definition, of whom 35 (2.4%) died in hospital (Table 1). Therefore, the high-risk population surviving to hospital discharge available for the assessment of performance measures consisted of 1398 patients (active arm, 681; control arm, 717). By 12 months, follow-up was available in 92% of the cohort (lost to follow-up was defined as not contactable and no prior events observed; 177 [8%]). Within this study, the GRS retained its discriminatory capacity for in-hospital death with a C statistic of 0.84.
Figure 1. CONSORT Figure.

CONCORDANCE indicates Cooperative National Registry of Acute Coronary Care, Guideline Adherence and Clinical Events; IQR, interquartile range.
Table 1. Hospital-Level and Patient-Level Characteristics Among All Patients With Acute Coronary Syndrome.
| Characteristic | No. (%) | P valuea | |
|---|---|---|---|
| Control | Intervention | ||
| Total No. | 1183 | 1135 | NA |
| Age, median (IQR), y | 64.0 (55.0-73.0) | 66.0 (57.0-74.0) | .30 |
| Female | 364 (30.8) | 320 (28.2) | .36 |
| Final diagnosis | |||
| STEMI | 323 (27.3) | 373 (32.9) | .18 |
| NSTEMI | 649 (54.9) | 634 (55.9) | |
| UA | 211 (17.8) | 138 (11.3) | |
| GRACE score | |||
| Median (IQR) | 127.0 (105.0-153.0) | 132.5 (109.0-158.0) | .35 |
| >118b | 699 (60.7) | 734 (65.2) | .32 |
| >140b | 450 (38.0) | 472 (41.6) | .42 |
| CRUSADE score | |||
| Median (IQR) | 26.0 (14.0-41.0) | 36.0 (18.0-49.0) | .16 |
| >40 | 342 (28.9) | 487 (42.9) | .19 |
| Diabetes, median (IQR) | 0.0 (0.0-1.0) | 0.0 (0.0-1.0) | .30 |
| Hypertension | 750 (63.4) | 687 (60.5) | .42 |
| Dyslipidemia | 684 (57.8) | 596 (52.5) | .06 |
| Current smoker | 352 (29.8) | 304 (26.8) | .36 |
| Known CHD | 276 (23.3) | 356 (31.4) | .16 |
| Height, median (IQR), cm | 170.0 (164.0-178.0) | 172.0 (165.0-178.0) | .33 |
| Weight, median (IQR), kg | 82.0 (71.5-95.0) | 84.0 (72.0-95.0) | .29 |
| SBP, median (IQR), mm Hg | 140.0 (123.0-158.0) | 140.0 (122.0-158.5) | .58 |
| DBP, median (IQR), mm Hg | 80.0 (70.0-90.0) | 80.0 (70.5-90.5) | .86 |
| HR, median (IQR), per min | 77.0 (66.0-90.0) | 78.0 (67.0-90.0) | .92 |
| Killip class | |||
| 1 | 1050 (88.8) | 989 (87.1) | .63 |
| 2 | 96 (8.1) | 116 (10.2) | |
| 3 | 29 (2.5) | 20 (1.8) | |
| 4 | 8 (0.7) | 10 (0.9) | |
| Cardiac arrest at admission | 27 (2.3) | 37 (3.3) | .31 |
| Previous myocardial infarction | 352 (29.8) | 306 (27.0) | .46 |
| Chronic heart failure | 75 (6.3) | 78 (6.9) | .71 |
| Previous angiogram | 418 (35.3) | 352 (31.0) | .24 |
| Previous PCI | 259 (21.9) | 216 (19.0) | .29 |
| Previous CABG | 126 (10.7) | 118 (10.4) | .88 |
| Previous AF | 113 (9.6) | 101 (8.9) | .73 |
| Permanent pacemaker | 27 (2.3) | 33 (2.9) | .46 |
| Previous valve surgery | 8 (0.7) | 7 (0.6) | .83 |
| Peripheral vascular disease | 68 (5.7) | 43 (3.8) | .12 |
| Chronic lung disease | 146 (12.3) | 133 (11.7) | .08 |
| Previous cancer | 7 (0.6) | 14 (1.2) | .29 |
| Dementia | 24 (2.0) | 28 (2.5) | .69 |
| LV function grade | |||
| Normal | 544 (62.6) | 550 (63.9) | .83 |
| Mild | 167 (19.2) | 172 (20.0) | |
| Moderate | 92 (10.6) | 87 (10.1) | |
| Severe | 66 (7.6) | 52 (6.0) | |
| Troponin peak value (within first 24 h), median (IQR), ng/L | 367.5 (47.0-3665.0) | 202.7 (35.0-2215.0) | .49 |
| Serum creatinine on admission, median (IQR), mg/dL | 84.0 (71.0-102.0) | 84.0 (71.0-101.0) | .10 |
Abbreviations: AF, atrial fibrillation; CABG, coronary artery bypass grafting; CHD, coronary heart disease; DBP, diastolic blood pressure; GRACE, Global Registries of Acute Coronary Events; HR, hazard ratio; IQR, interquartile range; LV, left ventricle; NA, not applicable; NSTEMI, non–ST-segment elevation myocardial infarction; SBP, systolic blood pressure; STEMI, ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; UA, unstable angina.
SI conversion factor: To convert creatinine to micromoles per liter, multiply by 88.4; troponin to micrograms per liter, multiply by 1.
P values account for clustered design.
Includes 35 patients who died in hospital (control arm, 18; intervention arm, 17).
Change in Clinical Performance Measures
There was a high use of guideline-recommended therapies in this study. Observed rates of cardiac investigations and therapies for the overall population and the high-risk group are presented in Table 2. After accounting for the clustered design, the provision of all 3 measures among high-risk patients did not differ between the 2 randomized arms (GRS: 424 of 717 [59.9%] vs control: 376 of 681 [55.2%; odds ratio [OR], 1.04; 95% CI, 0.63-1.71) as well as in the overall population (OR, 1.00; 95% CI, 0.59-1.70) (Table 2). The rates of prescription of 4 of 5 guideline-recommended pharmacotherapies and referral to cardiac rehabilitation were similar between the intervention and control groups within the overall population and the high-risk cohort and the entire population. The provision of invasive treatment was higher in the intervention group when assessed in the entire population (GRS: 1042 of 1135 [91.8%] vs control: 989 of 1183 [83.6%]; OR, 2.26; 95% CI, 1.30-3.96; P = .004) but not significantly different within the high-risk cohort (GRS: 652 of 717 [90.9%] vs control: 582 of 681 [85.5%]; OR, 1.74; 95% CI, 1.00-3.03; P = .05). The use of invasive treatment also did not differ among those patients with a GRS score of greater than 140 (GRS: 419 of 470 [89.2%] vs control: 373 of 451 [82.7%]; OR, 1.67; 95% CI, 0.88-3.18; P = .12). There was no difference in the median time to angiography between the treatment arms (GRS: 1.2 days; interquartile range [IQR], 0.2-2.7 days vs control: 1.2 days; IQR, 0.5-2.5 days; P = .13). Time to angiography was also similar among patients with non–ST-segment elevation myocardial infarction between GRS and control hospitals (GRS, 2.1 days; IQR, 1.2-3.5 days vs control, 1.8 days; IQR, 1.0-3.0 days; P = .45).
Table 2. Uptake of the GRACE Risk Score and Clinical Performance.
| Variable | No. (%) | OR (95% CI) | P valuea | |
|---|---|---|---|---|
| Control | Intervention | |||
| Overall population | ||||
| Total No. | 1183 | 1135 | NA | NA |
| Invasive angiography | 989 (83.6) | 1042 (91.8) | 2.17 (1.22-3.87) | .008 |
| PCI | 570 (48.2) | 608 (53.6) | 1.28 (0.76-2.19) | .35 |
| CABG | 108 (9.1) | 129 (11.4) | 1.23 (0.81-1.86) | .33 |
| Any revascularization | 672 (56.8) | 730 (64.3) | 1.41 (0.82-2.42) | .22 |
| Echocardiogram | 861 (72.8) | 753 (66.3) | 0.82 (0.47-1.41) | .47 |
| Functional studya | 50 (4.2) | 29 (2.6) | 0.55 (0.22-1.39) | .21 |
| Cardiac CT angiography | 11 (0.9) | 17 (1.5) | 1.34 (0.43-4.15) | .61 |
| Aspirin at discharge | 1054 (89.1) | 1038 (91.5) | 1.31 (0.86-2.00) | .21 |
| P2Y12 at discharge | 861 (72.8) | 821 (72.3) | 0.97 (0.66-1.44) | .90 |
| Statin at discharge | 1082 (91.5) | 1033 (91.0) | 0.96 (0.66-1.40) | .81 |
| ACE-I/ARB at discharge | 676 (73.1) | 599 (69.6) | 0.87 (0.65-1.16) | .35 |
| β-Blocker at discharge | 879 (74.3) | 843 (74.3) | 0.98 (0.73-1.31) | .87 |
| GP IIb/IIIa inhibition | 91 (7.7) | 94 (8.3) | 1.02 (0.50-2.10) | .97 |
| Medication compliance | 893 (77.5) | 864 (76.7) | 0.99 (0.70-1.40) | .95 |
| Rehabilitation compliance | 861 (72.8) | 852 (75.1) | 0.68 (0.33-1.41) | .32 |
| Performance score, median (IQR) | 2.0 (2.0-3.0) | 3.0 (2.0-3.0) | .50 | |
| Compliant 3 guideline recommendations | 639 (54.0) | 679 (59.8) | 0.99 (0.59-1.67) | .98 |
| High-risk cohort | ||||
| Total No. | 681 | 717 | NA | NA |
| Angiography | 582 (85.5) | 652 (90.9) | 1.74 (1.0-3.03) | .05 |
| PCI | 354 (52.0) | 395 (55.1) | 1.23 (0.72-2.10) | .45 |
| CABG | 68 (10.0) | 85 (11.9) | 1.20 (0.82-1.76) | .36 |
| Any revascularization | 418 (61.4) | 474 (66.1) | 1.32 (0.78-2.23) | .30 |
| Echocardiogram | 534 (78.4) | 517 (72.1) | 0.80 (0.43-1.47) | .47 |
| Functional studyb | 23 (3.4) | 11 (1.5) | 0.45 (0.18-1.11) | .08 |
| Cardiac CT angiography | 2 (0.3) | 6 (0.8) | 2.80 (0.54-14.50) | .22 |
| Aspirin at discharge | 614 (90.2) | 649 (90.5) | 1.09 (0.67-1.76) | .73 |
| P2Y12 at discharge | 520 (76.4) | 525 (73.2) | 0.89 (0.56-1.39) | .60 |
| Statin at discharge | 635 (93.2) | 654 (91.2) | 0.81 (0.48-1.40) | .45 |
| ACE-I/ARB at discharge | 410 (73.5) | 385 (66.6) | 0.81 (0.55-1.19) | .28 |
| β-Blocker at discharge | 523 (76.8) | 561 (78.2) | 1.09 (0.82-1.45) | .55 |
| GP IIb/IIIa inhibition | 56 (8.2) | 68 (9.5) | 1.11 (0.53-2.36) | .79 |
| Medication compliance | 520 (76.4) | 534 (74.5) | 1.00 (0.66-1.54) | .98 |
| Rehabilitation compliance | 520 (76.4) | 553 (77.1) | 0.68 (0.32-1.41) | .31 |
| Performance score, median (IQR) | 3.0 (2.0-3.0) | 3.0 (2.0-3.0) | NA | .70 |
| Compliant 3 guideline recommendations | 376 (55.2) | 424 (59.1) | 1.04 (0.63-1.71) | .88 |
Abbreviations: ACE-I, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CABG, coronary artery bypass grafting; CT, computed tomography; GP, glycoprotein; GRACE, Global Registries of Acute Coronary Events; IQR, interquartile range; NA, not applicable; OR, odds ratio; PCI, percutaneous coronary intervention.
P values account for clustered design.
Functional study: exercise stress test, exercise or pharmacological stress echo, or nuclear medicine test.
Interactions Within Clinical Risk Subgroups
No interaction between the GRS and the provision of all hospital performance measures were demonstrated in any subgroup except for female sex (Figure 2A). The use of the GRS’s influence on early invasive treatment was greater among those younger than 75 years and patients not scored to be at high risk (Figure 2B).
Figure 2. Patient Subgroups Analysis for Compliance Measured as Compliance With All 3 Guideline Recommendations and Provision of Early Angiography.
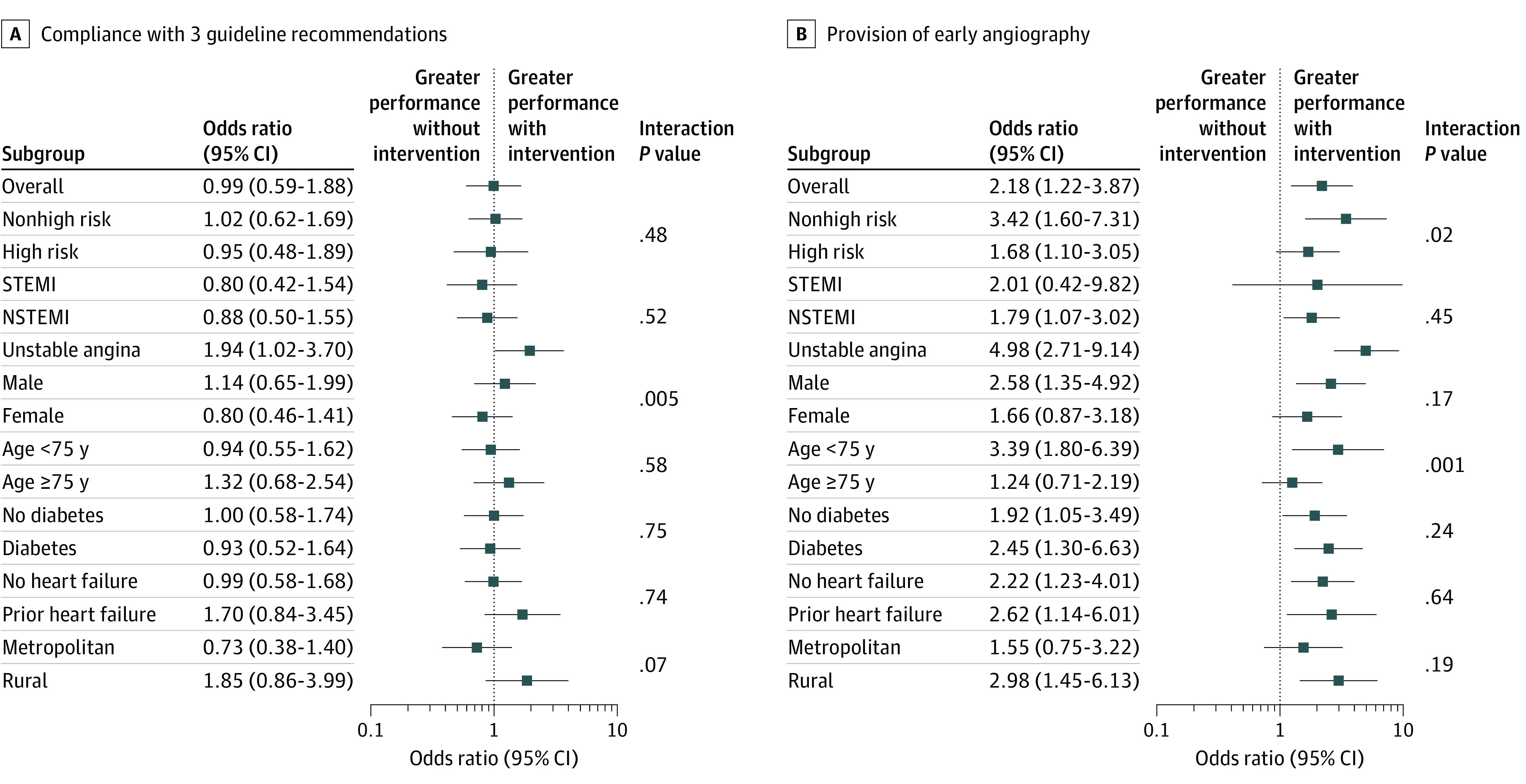
NSTEMI indicates non–ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Clinical Outcomes
Clinical events were infrequent (Table 3). In-hospital mortality and recurrent MI and major adverse cardiac events were observed in 41 of 2318 patients (1.8%) and 296 of 2318 patients (12.8%) within the overall cohort. There were only modest differences in in-hospital events with a lower rate of recurrent ischemia seen with use of the GRS.
Table 3. Final Diagnosis, In-Hospital, and 12-Month Clinical Events by Randomized Arm.
| Factor | Control | Intervention | Odds ratio (95% CI) | P valuea |
|---|---|---|---|---|
| No. | 1183 | 1135 | NA | NA |
| Final diagnosis | ||||
| NSTEMI | 323 (27.3) | 373 (32.9) | NA | .18 |
| STEMI | 649 (54.9) | 634 (55.9) | NA | |
| Unstable angina | 211 (17.8) | 128 (11.3) | NA | |
| In-hospital events | ||||
| In-hospital death | 22 (1.9) | 19 (1.7) | 0.95 (0.38-2.38) | .92 |
| New/recurrent MI | 24 (2.0) | 13 (1.1) | 0.54 (0.21-1.29) | .20 |
| Recurrent ischemia | 94 (7.9) | 18 (1.6) | 0.21 (0.07-0.68) | .009 |
| Cardiac arrest | 20 (1.7) | 34 (3.0) | 1.87 (0.87-4.04) | .10 |
| Congestive heart failure | 89 (7.5) | 101 (8.9) | 1.35 (0.66-2.76) | .41 |
| Ventricular arrhythmia | 14 (1.2) | 15 (1.3) | 1.16 (0.49-2.78) | .73 |
| Stroke/TIA | 7 (0.6) | 3 (0.3) | 0.49 (0.15-1.55) | .22 |
| TIMI major bleeding | 69 (5.8) | 70 (6.2) | 1.08 (0.64-1.81) | .76 |
| Events by 12 mo | ||||
| No. | 1087 | 1044 | NA | NA |
| Death | 87 (8.0) | 54 (5.2) | 0.60 (0.31-1.15) | .12 |
| MI | 73 (6.7) | 49 (4.7) | 0.73 (0.48-1.12) | .15 |
| Heart failure | 115 (10.6) | 120 (11.5) | 1.16 (0.58-2.30) | .68 |
| CVA | 9 (0.8) | 5 (0.5) | 0.60 (0.27-1.35) | .22 |
| Death or MI | 146 (13.4) | 96 (9.2) | 0.66 (0.38-1.14) | .13 |
| Death/MI/stent thrombosis | 149 (13.7) | 97 (9.3) | 0.65 (0.37-1.13) | .13 |
| Events by 12 mo (high-risk cohort) | ||||
| No. | 639 | 668 | ||
| Death | 56 (8.8) | 30 (4.5) | 0.44 (0.21-0.91) | .03 |
| MI | 50 (7.8) | 43 (6.4) | 0.88 (0.51-1.52) | .64 |
| Heart failure | 87 (13.6) | 105 (15.7) | 1.10 (0.54-2.27) | .79 |
| CVA | 5 (0.8) | 4 (0.6) | 1.10 (0.37-3.33) | .86 |
| Death or MI | 96 (15.0) | 66 (9.9) | 0.60 (0.32-1.14) | .12 |
| Death/MI/stent thrombosis | 98 (15.3) | 67 (10.0) | 0.60 (0.32-1.13) | .12 |
Abbreviations: CVA, cerebrovascular accident; MI, myocardial infarction; NA, not applicable; NSTEMI, non–ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; TIA, transient ischemic attack; TIMI, thrombolysis in myocardial infarction.
P values adjusted for clustered design.
By 12 months, the incidence of death or MI was not significantly lower among high-risk patients randomized to the intervention, but a lower rate of mortality alone was seen (GRS: 30 of 671 [4.5%] vs control: 57 of 641 [8.9%]; OR, 0.44; 95% CI, 0.21-0.91; P = .03). Within the overall population, mortality was not significantly lower among patients treated within the intervention hospitals (GRS: 54 of 1044 [5.2%] vs control: 87 of 1087 [8.0%]; OR, 0.60; 95% CI, 0.32-1.15; P = .12), as was the composite end point of death or MI (GRS: 96 of 1044 [9.2%] vs control: 146 of 1087 [13.4%]; OR, 0.66; 95% CI, 0.38-1.14; P = .11).
Discussion
While there has been a proliferation of risk scores guiding clinical treatment in cardiovascular care, to our knowledge, this study is the first to prospectively evaluate the effect of risk scoring on the use of guideline-recommended care and clinical outcomes in patients with ACS. In the context of a higher-than-expected rate of adherence with guideline recommendations, routine use of the GRS had no significant effect on the overall use of guideline-recommended care, either in the overall ACS population or those at high ischemic risk. However, it did increase the use of early invasive treatment, particularly in younger patients and those at lower predicted ischemic risk. No significant difference in invasive treatment was seen among high-risk patients, potentially owing to early study cessation and high overall performance at baseline. There were no specific hospital-level or patient-level characteristics that substantially influenced the effect of routine objective risk stratification on the provision of overall care, although there was a modest and unexplained interaction between the use of the GRS and poorer adherence to guideline-recommended care and female sex. In this cohort of high-performing hospitals and with only a 12-month follow-up, these differences in early invasive treatment were associated with nonsignificant differences in death and recurrent MI.16 Nevertheless, we observed that the GRS retains its discriminatory capacity for the prediction of short to intermediate-term mortality, and its use in estimating prognosis continues to be recommended in the 2020 European Society of Cardiology Guidelines for Non–ST-Segment Elevation ACS (class IIA; Level of Evidence B).17
The routine deployment of the GRS does appear to influence the decision for early invasive strategy. This influence appeared to be more striking among those of younger age and at lower ischemic risk in our study. The GRS’s greatest utility may reside in crystalizing the risk-benefit decisions for the near-term outcomes associated with early angiography. This is perhaps unsurprising because the decision for invasive vs conservative treatment among lower-risk patients is subject to the greatest variation in physician’s risk-benefit perception and practice.5,18 Further, most literature regarding the benefits of therapies based on the GRS has focused on invasive treatment.19,20,21,22
In contrast, the lack of effect of risk stratification on decisions to prescribe secondary prevention pharmacotherapies and referral to cardiac rehabilitation may be anticipated because therapeutic interventions are expected to improve long-term outcome regardless of baseline risk.22 Hence, the GRS does not offer a decision threshold advocating the use or withholding of these therapies. These may be more influenced by health service structure, workforce, and funding models than misperceptions of clinical risk.23,24,25 Systematic strategies, such as checklists and reminders as well as the configuration of secondary prevention services, may have a greater value in ensuring optimized care.
Clinical care is complex, and for many patients with ACS, competing issues, such as comorbidities, personal preferences, and social demands, affect the ability to provide the complete evidence-based care. While the GRS describes the risk of death or recurrent MI associated with ACS, the provision of care is influenced by other competing risks within individual patients. Death or recurrent MI is only one dimension of the overall profile of outcomes patients may seek to optimize. Evidence that competing risks contribute to early hazard and attenuate the late benefits provided by early invasive treatment likely influence decisions to provide invasive treatment.26,27,28 These considerations may help explain the greater influence of the risk scoring on invasive treatment among the younger and not-high-risk groups within practice that already demonstrated high uptake.
Limitations
While these data provide only modest support for the routine GRS implementation, several limitations should be considered. First, while documentation of clinical interaction with the score was required during the implementation and enrollment phases, how well this clinical documentation was integrated with other processes of care could not be assessed. Similarly, we could not prevent individual clinicians accessing the GRS calculators independently, but our prior evidence suggests this is uncommon.2,5 Second, while the GRS demonstrates strong discriminatory performance, few studies have prospectively defined thresholds that serve as decision points in the continuous risk spectrum. Further, no studies have used these scores to demonstrate benefit or no benefit associated with ACS pharmacotherapies at various levels of predicted risk. Consequently, firm decision points, where recommendations transition from “do not treat” to “treat” have not been well defined. Potential, stratified randomization of future ACS clinical trials using the GRS may provide clearer guidance regarding the use or withholding of treatment strategies defining effectiveness or cost-effectiveness. Third, this study included a high proportion of patients with ST-segment elevation myocardial infarction, among whom care is more consistent, with a very high rate of invasive treatment, attenuating the ability to observe differences between treatment arms. Fourth, overall clinical performance in the study was higher than observed during the planning phase. Similarly, overall event rates were low, and clinical follow-up only extends to 12 months. In addition, this study was stopped early for futility. These factors contributed to a reduced power for detect a difference between the study arms in terms of performance measures and clinical outcomes.29,30 A greater ability to detect an effect on late clinical events may be achieved through a planned pooled analysis of this study, with another being conducted in different health care environment.31 The true test of routine risk stratification may require the conduct of similar trials in acute environments without ready access to cardiac clinical expertise.
Conclusions
Among an ACS cohort treated in high-performing hospitals, the routine use of the GRS appears to increase the use of an early invasive strategy but not other aspects of care. Routine GRS use did not reduce 12-month death or recurrent MI. These findings highlight the need for larger trials to determine the role of routine risk scoring.
Trial protocol
eFigure. AGRIS worksheet
Data sharing statement
References
- 1.Fox KA, Anderson FA Jr, Dabbous OH, et al. ; GRACE investigators . Intervention in acute coronary syndromes: do patients undergo intervention on the basis of their risk characteristics? the Global Registry of Acute Coronary Events (GRACE). Heart. 2007;93(2):177-182. doi: 10.1136/hrt.2005.084830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yan AT, Yan RT, Tan M, et al. ; Canadian Acute Coronary Syndromes 1 and 2 Registry Investigators . Management patterns in relation to risk stratification among patients with non-ST elevation acute coronary syndromes. Arch Intern Med. 2007;167(10):1009-1016. doi: 10.1001/archinte.167.10.1009 [DOI] [PubMed] [Google Scholar]
- 3.Yan RT, Yan AT, Tan M, et al. ; Canadian Acute Coronary Syndrome Registry Investigators . Underuse of evidence-based treatment partly explains the worse clinical outcome in diabetic patients with acute coronary syndromes. Am Heart J. 2006;152(4):676-683. doi: 10.1016/j.ahj.2006.04.002 [DOI] [PubMed] [Google Scholar]
- 4.Scott IA, Derhy PH, O’Kane D, Lindsay KA, Atherton JJ, Jones MA; CPIC Cardiac Collaborative . Discordance between level of risk and intensity of evidence-based treatment in patients with acute coronary syndromes. Med J Aust. 2007;187(3):153-159. doi: 10.5694/j.1326-5377.2007.tb01173.x [DOI] [PubMed] [Google Scholar]
- 5.Chew DP, Junbo G, Parsonage W, et al. ; Perceived Risk of Ischemic and Bleeding Events in Acute Coronary Syndrome Patients (PREDICT) Study Investigators . Perceived risk of ischemic and bleeding events in acute coronary syndromes. Circ Cardiovasc Qual Outcomes. 2013;6(3):299-308. doi: 10.1161/CIRCOUTCOMES.111.000072 [DOI] [PubMed] [Google Scholar]
- 6.Chew DP, Juergens C, French J, et al. ; Predict study Investigators . An examination of clinical intuition in risk assessment among acute coronary syndromes patients: observations from a prospective multi-center international observational registry. Int J Cardiol. 2014;171(2):209-216. doi: 10.1016/j.ijcard.2013.12.010 [DOI] [PubMed] [Google Scholar]
- 7.de Araújo Gonçalves P, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J. 2005;26(9):865-872. doi: 10.1093/eurheartj/ehi187 [DOI] [PubMed] [Google Scholar]
- 8.Fox KAA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ. 2006;333(7578):1091-1091. doi: 10.1136/bmj.38985.646481.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Roffi M, Patrono C, Collet J-P, et al. ; ESC Scientific Document Group . 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267-315. doi: 10.1093/eurheartj/ehv320 [DOI] [PubMed] [Google Scholar]
- 10.Chew DP, Scott IA, Cullen L, et al. ; NHFA/CSANZ ACS Guideline 2016 Executive Working Group . National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Management of Acute Coronary Syndromes 2016. Heart Lung Circ. 2016;25(9):895-951. doi: 10.1016/j.hlc.2016.06.789 [DOI] [PubMed] [Google Scholar]
- 11.Chew DP, Astley CM, Luker H, et al. A cluster randomized trial of objective risk assessment versus standard care for acute coronary syndromes: rationale and design of the Australian GRACE Risk Score Intervention Study (AGRIS). Am Heart J. 2015;170(5):995-1004.e1. doi: 10.1016/j.ahj.2015.07.032 [DOI] [PubMed] [Google Scholar]
- 12.Aliprandi-Costa B, Ranasinghe I, Turnbull F, et al. The design and rationale of the Australian Cooperative National Registry of Acute Coronary Care, Guideline Adherence and Clinical Events (CONCORDANCE). Heart Lung Circ. 2013;22(7):533-541. doi: 10.1016/j.hlc.2012.12.013 [DOI] [PubMed] [Google Scholar]
- 13.Subherwal S, Bach RG, Chen AY, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the ACC/AHA guidelines) Bleeding Score. Circulation. 2009;119(14):1873-1882. doi: 10.1161/CIRCULATIONAHA.108.828541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ibanez B, James S, Agewall S, et al. ; ESC Scientific Document Group . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. doi: 10.1093/eurheartj/ehx393 [DOI] [PubMed] [Google Scholar]
- 15.Rao JN, Scott AJ. A simple method for the analysis of clustered binary data. Biometrics. 1992;48(2):577-585. doi: 10.2307/2532311 [DOI] [PubMed] [Google Scholar]
- 16.Fox KAA, Clayton TC, Damman P, et al. ; FIR Collaboration . Long-term outcome of a routine versus selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome a meta-analysis of individual patient data. J Am Coll Cardiol. 2010;55(22):2435-2445. doi: 10.1016/j.jacc.2010.03.007 [DOI] [PubMed] [Google Scholar]
- 17.Collet J-P, Thiele H, Barbato E, et al. ; ESC Scientific Document Group . 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2020;37:267. doi: 10.1093/eurheartj/ehaa575 [DOI] [PubMed] [Google Scholar]
- 18.Chew DP, Bhatt DL. Predicting risk in ACS: taking the long-term view. J Am Coll Cardiol. 2017;70(15):1858-1860. doi: 10.1016/j.jacc.2017.08.035 [DOI] [PubMed] [Google Scholar]
- 19.Fox KA, Poole-Wilson P, Clayton TC, et al. 5-Year outcome of an interventional strategy in non-ST-elevation acute coronary syndrome: the British Heart Foundation RITA 3 randomised trial. Lancet. 2005;366(9489):914-920. doi: 10.1016/S0140-6736(05)67222-4 [DOI] [PubMed] [Google Scholar]
- 20.Mehta SR, Granger CB, Boden WE, et al. ; TIMACS Investigators . Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360(21):2165-2175. doi: 10.1056/NEJMoa0807986 [DOI] [PubMed] [Google Scholar]
- 21.Hall M, Dondo TB, Yan AT, et al. Association of clinical factors and therapeutic strategies with improvements in survival following non-ST-elevation myocardial infarction, 2003-2013. JAMA. 2016;316(10):1073-1082. doi: 10.1001/jama.2016.10766 [DOI] [PubMed] [Google Scholar]
- 22.Hall M, Bebb OJ, Dondo TB, et al. Guideline-indicated treatments and diagnostics, GRACE risk score, and survival for non-ST elevation myocardial infarction. Eur Heart J. 2018;39(42):3798-3806. doi: 10.1093/eurheartj/ehy517 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Astley CM, Macdougall CJ, Davidson PM, Chew DP. Lost in translation: health resource variability in the achievement of optimal performance and clinical outcome. Circ Cardiovasc Qual Outcomes. 2011;4(5):512-520. doi: 10.1161/CIRCOUTCOMES.110.960229 [DOI] [PubMed] [Google Scholar]
- 24.Briffa TG, Hammett CJ, Cross DB, et al. Should fee-for-service be for all guideline-advocated acute coronary syndrome (ACS) care? Observations from the Snapshot ACS study. Aust Health Rev. 2015;39(4):379-386. doi: 10.1071/AH14153 [DOI] [PubMed] [Google Scholar]
- 25.Joynt KE, Harris Y, Orav EJ, Jha AK. Quality of care and patient outcomes in critical access rural hospitals. JAMA. 2011;306(1):45-52. doi: 10.1001/jama.2011.902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chuang AM-Y, Hancock DG, Halabi A, et al. Invasive management of acute coronary syndrome: interaction with competing risks. Int J Cardiol. 2018;269:13-18. doi: 10.1016/j.ijcard.2018.07.078 [DOI] [PubMed] [Google Scholar]
- 27.Tegn N, Abdelnoor M, Aaberge L, et al. ; After Eighty study investigators . Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study): an open-label randomised controlled trial. Lancet. 2016;387(10023):1057-1065. doi: 10.1016/S0140-6736(15)01166-6 [DOI] [PubMed] [Google Scholar]
- 28.Joynt KE, Huynh L, Amerena JV, et al. Impact of acute and chronic risk factors on use of evidence-based treatments in patients in Australia with acute coronary syndromes. Heart. 2009;95(17):1442-1448. doi: 10.1136/hrt.2008.154781 [DOI] [PubMed] [Google Scholar]
- 29.Berwanger O, Guimarães HP, Laranjeira LN, et al. ; Bridge-Acs Investigators . Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012;307(19):2041-2049. doi: 10.1001/jama.2012.413 [DOI] [PubMed] [Google Scholar]
- 30.Tu JV, Donovan LR, Lee DS, et al. Effectiveness of public report cards for improving the quality of cardiac care: the EFFECT study: a randomized trial. JAMA. 2009;302(21):2330-2337. doi: 10.1001/jama.2009.1731 [DOI] [PubMed] [Google Scholar]
- 31.Everett CC, Fox KA, Reynolds C, et al. Evaluation of the impact of the GRACE risk score on the management and outcome of patients hospitalised with non-ST elevation acute coronary syndrome in the UK: protocol of the UKGRIS cluster-randomised registry-based trial. BMJ Open. 2019;9(9):e032165. doi: 10.1136/bmjopen-2019-032165 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial protocol
eFigure. AGRIS worksheet
Data sharing statement