

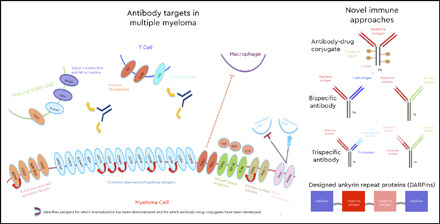
Visual Abstract
Abstract
Despite recent advances in treatment, relapses in multiple myeloma (MM) are inevitable. Off-the-shelf immunotherapeutics represent a promising avenue for research, with various classes of agents under development and several demonstrating deep and durable responses in patients who have exhausted all available therapies. Antibody-drug conjugates (ADCs) seek to improve on naked monoclonal antibodies by delivering a cytotoxic payload directly to tumor cells while largely limiting systemic effects. Belantamab mafodotin, a B-cell maturation antigen (BCMA)–targeted ADC, has shown response rates >30% in a phase 2 trial of highly refractory patients and is being investigated in a variety of settings and combinations. Several other ADCs are in earlier stages of development that target cell surface antigens that are internalized, including BCMA, CD38, CD46, CD56, CD74, and CD138. Bispecifics are designed to bring cytotoxic immune effector cells into proximity with tumor cells, and several agents have shown high response rates in early trials. Current targets include BCMA, CD38, GPRC5d, and FCRH5, and all of these seek to engage T cells through CD3. Bispecifics targeting natural killer (NK) cells through CD16 are still in preclinical development. Trispecific antibodies may represent an advance over bispecifics by providing a T-cell costimulatory signal such as CD28, or alternatively, dual MM antigens to increase specificity of NK or T-cell targeting. This is an area of active preclinical research at this time. Lastly, designed ankyrin repeat proteins, which are small antibody-mimetic proteins with high target-binding affinity, have the potential to block multiple pathways at once and provide stimulatory signals to the immune system.
Learning Objectives
Learn the myriad of targets under investigation for off-the-shelf immunotherapeutic approaches in the treatment of myeloma
Interpret the emerging clinical data from early-phase studies based on the differences in structure and function of classes of immunotherapeutic agents
Clinical case
A 75-year-old woman with IgA-κ relapsed refractory multiple myeloma (RRMM) was diagnosed with MM 15 years ago and underwent 7 lines of therapy, including 2 autologous stem cell transplants. She was refractory to 3 immunomodulatory (IMiD) drugs (thalidomide, lenalidomide, and pomalidomide), 2 proteasome inhibitors (PIs; bortezomib and carfilzomib), and an anti-CD38 monoclonal antibody (daratumumab) and had recently progressed through selinexor. What novel off-the-shelf immune therapies are available in clinical trials for this patient?
Introduction
Despite many recent drug approvals, relapses in multiple myeloma (MM) are inevitable. Patients who are pentarefractory (refractory to 2 IMiDs, 2 PIs, and an anti-CD38 monoclonal antibody) have particularly poor outcomes, with median overall survival (OS) of 5.6 months in 1 study.1 Several novel immunotherapeutic approaches are under development to harness the patient’s immune system to attack the malignant plasma cells. Although there are 3 naked monoclonal antibodies (mAbs) approved for treatment of MM targeting CD38 or SLAMF7, many other known myeloma antigens could serve as therapeutic targets (Figure 1). Several off-the-shelf novel immune approaches using these targets are under investigation for MM, including antibody-drug conjugates (ADCs), bispecific antibodies, trispecific antibodies, and designed ankyrin repeat proteins (DARPins). ADCs and bispecifics, in particular, have demonstrated single-agent activity in RRMM and belantamab mafodotin, an anti-BCMA ADC, was approved by the FDA in August 2020 for RRMM with 4 prior lines of therapy. We review the state of development of each class and the data presented to date.
Figure 1.

Antibody targets in multiple myeloma. There are numerous myeloma cell targets under investigation for immunotherapeutic approaches. The schematic is simplified, because not all of these targets are necessarily expressed on the cell surface, although those noted as undergoing internalization make ideal targets for ADCs. Other targets are expressed on cells comprising the immune microenvironment, including T cells, NK cells, and macrophages.
Antibody-drug conjugates
Antibody-drug conjugates (ADCs) enhance naked antibodies by attaching a potent cytotoxic agent to the mAb via a stable linker (Figure 2). After the antibody binds to a cell surface antigen and undergoes receptor-mediated endocytosis, the ADC is trafficked to the lysosome where the linker is cleaved and the cytotoxic agent is released intracellularly.2 The agent (the amount determined by the drug/antibody ratio [DAR]) accumulates in antigen-expressing cells while sparing other cells and limiting systemic toxicities. Belantamab mafodotin, an anti-BCMA ADC, was approved by the FDA in August 2020 for RRMM with at least 4 prior lines including an IMiD, PI, and anti-C38 mAb, while several other ADCs are in clinical trials for MM (Table 1).
Figure 2.

Antibody-drug conjugate. In addition to the antibody structure with antigen-binding domains, there are noncleavable linkers attaching the cytotoxic drugs to the Fc portion of the antibody. The drug-antibody ratio varies by agent and can affect cytotoxicity, stability in the circulation, and immunogenicity.
Table 1.
Clinical trials for antibody-drug conjugates in MM
| Agent | Target | Toxin | Phase | Clinical trial number | Status |
|---|---|---|---|---|---|
| Belantamab mafodotin (GSK2857916) | BCMA | MMAF | 1/2 | NCT03715478 | Ongoing |
| 1/2 | NCT03848845 | Ongoing | |||
| 1/2 | NCT03544281 | Ongoing | |||
| 1/2 | NCT04126200 | Ongoing | |||
| 1 | NCT04177823 | Ongoing | |||
| 1 | NCT03828292 | Ongoing | |||
| 1 | NCT04398680 | Not yet recruiting | |||
| 1 | NCT04398745 | Not yet recruiting | |||
| 2 | NCT03525678 | Completed | |||
| 1 | NCT02064387 | Completed | |||
| AMG224 | BCMA | Mertansine (DM1) | 1 | NCT02561962 | Completed |
| Medi2228 | BCMA | Pyrrolobenzodiazepine | 1 | NCT03489525 | Ongoing |
| CC99712 | BCMA | MMAE | 1 | NCT04036461 | Ongoing |
| TAK-573 | CD38 | Attenuated interferon-α | 1/21 | NCT03215030NCT03215030 | OngoingNot yet recruiting |
| TAK-169 | CD38 | Shiga-like toxin | 1 | NCT04017130 | Ongoing |
| FOR46 | CD46 | MMAE | 1 | NCT03650491 | Ongoing |
| Lorvotuzumab mertansine (1MGN901) | CD56 | Mertansine (DM1) | 11 | NCT00991562NCT00346255 | CompletedCompleted |
| STRO-001 | CD74 | Maytansinoid | 1 | NCT03424603 | Ongoing |
| Indatuximab ravtansine (BT062) | CD138 | Ravtansine (DM4) | 1/2a1/2a1 | NCT01638936NCT01001442NCT00723359 | CompletedCompletedCompleted |
PBD (DM1), pyrrolobenzodiazepine.
The most advanced ADC in development for MM is belantamab mafodotin (GSK2857916), which consists of a humanized IgG-1 anti-B-cell maturation antigen (BCMA) mAb linked to the microtubule inhibitor monomethyl auristatin F (MMAF) at a DAR of 4.3 The cysteine linker is not cleavable by proteases, making the ADC stable in the circulation. Belantamab mafodotin binds to BCMA, a member of the tumor necrosis factor superfamily expressed primarily on plasma cells, yet virtually absent on naive and memory B cells. Upon internalization, the ADC releases its payload, MMAF, to cause direct cytotoxicity. In addition, the Fc portion has been afucosylated to enhance antibody-dependent cellular cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis.
In DREAMM-1, a multicenter phase 1 trial,4 38 patients with RRMM were given belantamab mafodotin at 0.03 to 4.60 mg/kg in a 1-hour IV infusion every 3 weeks. No dose-limiting toxicities (DLTs) were observed, and the maximum tolerated dose (MTD) was not reached. Corneal events, thrombocytopenia, and anemia were the most common adverse events (AEs). In 35 heavily pretreated patients given 3.40 mg/kg,5 the overall response rate (ORR) was 60%, although in 13 patients with prior daratumumab exposure, the ORR was lower at 39%.
The multicenter phase 2 study, DREAMM-2, included 196 patients with RRMM with at least 3 prior lines of therapy and refractory to a PI, IMiD, and refractory to or intolerant of an anti-CD38 monoclonal antibody.6 Patients were randomized to receive either 2.5 or 3.4 mg/kg of belantamab mafodotin. After a 13-month follow-up, the ORRs were 31% and 35% in a population that underwent a median of 7 or 6 lines of therapy, respectively, including ∼5% complete response (CR). The median progression-free survival (PFS) was 2.8 and 3.9 months; however, the median duration of response (DOR) was encouraging at 11 and 6.2 months, and the median OS at 14.9 and 14.0 months. respectively. Efficacy outcomes were comparable for high-risk (∼45% of the population) and standard-risk patients.
Keratopathy microcystlike epithelial changes in the 2 study arms occurred in 72% and 77% of patients, including grade 3 and 4 events in 46% and 42%, respectively. Corticosteroid eye drops were ineffective, and the changes were managed with artificial tears and dose delays (median, ∼80 days) or modifications. The keratopathy was attributed to MMAF, given that ocular toxicities had not occurred with other cytotoxic conjugates. Many patients experienced blurred vision, which may have significant implications for quality of life. Thrombocytopenia (38% and 57%) and anemia (21% and 27%) were the next most common grade 3 and 4 AEs, whereas primarily grade 1 and 2 infusion reactions occurred in 21% and 16%, respectively, mostly during the first infusion. In comparison with bispecific anti-BCMA agents, grade 3+ infections occurred infrequently in 6% and 11% of the 2 groups, respectively. AEs led to treatment discontinuation, dose reduction, and dose delays occurred in ∼10%, 40%, and 60% of patients.
Results of the addition of belantamab mafodotin 2.5 mg/kg to a bortezomib-dexamethasone backbone (DREAMM-6) in 18 patients were recently presented,7 and whereas the ORR of 78% was encouraging, grade 3 keratopathy occurred in 10 patients (55%) and grade 3+ thrombocytopenia in 11 (61%). Additional trials evaluating belantamab mafodotin in combination with both approved and investigational agents are ongoing.
To date, 2 other ADCs are in clinical development, with reports of early-phase clinical data. Preliminary phase 1 results of STRO-001, an anti-CD74 mAb linked to a maytansinoid payload in a 2:1 DAR, have been reported in 25 patients with B-cell malignancies.8 Of those, 14 were patients with MM, and 1 was reported to have SD. The main AEs included fatigue, pyrexia, cough, nausea, headache, and infusion reactions, with 2 DLTs (2 thromboembolic events). No ocular toxicity was reported.
AMG224, an anti-BCMA mAb linked to mertansine (DM1), showed a 23% ORR in RRMM. The main AEs included thrombocytopenia, anemia, neutropenia, aspartate aminotransferase elevation, myalgias, and ocular toxicities.9 Other ADCs targeting BCMA (MEDI2228,10 CC99712), CD46 (FOR4611), and CD38 (TAK-57312 and TAK-16913) are currently in phase 1 trials. Lorvotuzumab mertansine (IMGN901), an anti-CD56 mAb linked to mertansine, and indatuximab ravtansine (BT062), an anti-CD138 mAb linked to the microtubule inhibitor DM4, showed modest activity in early-phase trials, and their development has been discontinued.14-17
Bispecific antibodies
Bispecific antibodies are designed to bind a tumor antigen while binding cytotoxic immune effector cells, usually T cells and sometimes NK cells, which are then activated to kill the nearby tumor cells (Figure 3).18 Although there are many different bispecific constructs, the 2 major classes are those with an Fc region and those without. Bispecifics without an Fc region are small and easily penetrate tumor tissues.19 The main drawback is a short half-life, requiring frequent or continuous dosing. Various “half-life extenders” can be added, including polyethylene glycol, polyethylene glycol–mimetic polypeptides, or albumin-binding moieties. Fc-containing bispecific antibodies are larger and more stable in the circulation and have the added advantage of Fc-mediated effector functions including ADCC and complement fixation.20 At present, blinatumomab (a CD19xCD3 bispecific T-cell engager) is the only bispecific agent approved for use in cancer; however, the field is rapidly evolving, and many agents are in trials for MM (Table 2).
Figure 3.

Bispecific antibodies. (A) Bispecific T-cell engagers bring CD3+ T cells in proximity to cells expressing tumor antigen, to form an immunologic synapse and promote cell-mediated cytotoxicity. The Fc portion provides stability in the circulation, allowing for intermittent rather than continuous dosing, and can also promote antibody-dependent cellular cytotoxicity and complement activation. These constructs vary widely by agent, and the schematics shown are only representative. There can be variability in antigen-binding domains and dimerization (homodimers vs heterodimers), resulting in differences in antigen-binding sites (valency), geometry, size, and flexibility, all of which can result in different pharmacokinetic and pharmacodynamic properties. (B) Bispecific NK-cell engager, with 1 binding domain for the myeloma antigen and 1 for NK antigens leading to signal transduction and NK-cell activation.
Table 2.
Clinical trials for bispecific antibodies in multiple myeloma
| Agent | Targets | Phase | Clinical trial number | Status |
|---|---|---|---|---|
| AMG420 | BCMAxCD3 | 1 | NCT03836053 | Completed |
| AMG701 | BCMAxCD3 | 1/2 | NCT03287908 | Ongoing |
| CC-93269 | BCMAxCD3 | 1 | NCT03486067 | Ongoing |
| PF-06863135 | BCMAxCD3 | 1 | NCT03269136 | Ongoing |
| REGN5458 | BCMAxCD3 | 1/2 | NCT03761108 | Ongoing |
| JNJ-64007957 | BCMAxCD3 | 1b1 | NCT04108195NCT03145181 | OngoingOngoing |
| TNB-383B | BCMAxCD3 | 1 | NCT03933735 | Ongoing |
| GBR1342 | CD38xCD3 | 1/2 | NCT03309111 | Ongoing |
| AMG424 | CD38xCD3 | 1 | NCT03445663 | Ongoing |
| JNJ-64407564 | GPRC5dxCD3 | 1b1 | NCT04108195NCT03399799 | OngoingOngoing |
| BFCR4350A | FCRH5xCD3 | 1 | NCT03275103 | Ongoing |
AMG420, targeting BCMAxCD3, was the first bispecific to have data reported on treatment of MM.21 In a phase 1 study, it was administered as a continuous IV infusion for 4 weeks followed by 2 weeks off (6-week cycles). Of the 42 patients enrolled, 16 (38%) experienced cytokine release syndrome (CRS), with 1 grade 3 toxicity. The most common serious AEs were infection (14; 33%), including 5 central line infections and 2 cases (5%) of polyneuropathy (PN). Because of a grade 3 CRS and a grade 3 PN at a dose of 800 μg/d, the MTD was 400 μg/d. Two AE- but nontreatment-related deaths were from influenza/aspergillosis and adenovirus-related hepatitis. Patients had a median of 5 lines of prior therapy, although only 38%, 48%, and 21% were refractory to PIs, IMiDs, and daratumumab, respectively. At the MTD, the ORR was 70% (7 of 10), including 5 minimal residual disease (MRD)–negative CRs (MRD measured at a sensitivity of 10−4 by flow cytometry), 1 very good PR (VGPR), and 1 PR. Median time to response was 1 month and median DOR was 9 months. Although the efficacy results are encouraging, given the impracticality of continuous IV dosing, AMG701, a BCMAxCD3 bispecific with a half-life–extending Fc domain that allows for weekly dosing, is currently in a phase 1/2a trial.22
The largest BCMAxCD3 study presented to date is teclistamab (JNJ-64007957),23 a humanized IgG-4 bispecific. In a phase 1 study of IV doses ranging from 0.3 to 720 μg/kg, predominantly with step-up dosing in 78 patients, 56% experienced CRS, none of which were grade 3+ and all of which were generally confined to initial doses. Two DLTs were grade 4 delirium (n = 1) and grade 4 thrombocytopenia (n = 1). Infections occurred in 65% of patients; 21% were grade 3+. Two deaths from AEs were grade 5 respiratory failure in the setting of pneumonia (deemed unrelated), and 1 death was caused by COVID-19. In a population with a median of 6 lines of prior therapy and 80% triple-class refractory, the ORR at weekly dosing of 38.4 to 180 μg/kg (n = 44) was 30%. At 270 μg/kg (n = 12) the ORR was 67% (50% ≥VGPR), including 4 of 5 evaluable patients who were MRD− at 10−6. Ongoing response was noted in 16 of 21 patients. Subcutaneous administration is also being studied.
A recent report of a phase 1 trial of CC-93269, an asymmetric 2+1 bispecific with bivalent BCMA binding, monovalent CD3 binding, and a half-life–extending Fc domain, showed early promising results.24 Nineteen patients were enrolled, with a median of 6 prior therapies and most refractory to a PI, IMiD, and daratumumab. Grade 3 or 4 neutropenia (53%), anemia (42%), infections (26%), and thrombocytopenia (21%) were common. CRS was seen in most (90%) patients, and all but 1 were grade 1 or 2. In the 12 patients who received at least 6 mg as the initial dose, ORR was 83%, including 4 (33%) stringent CRs and 9 (75%) MRD− at 10−5 by flow cytometry. All responses were ongoing at a short median follow-up of 2.1 to 4.7 months.
Several other BCMAxCD3 bispecifics are under development, but data are limited. PF-06863135 was tested in 17 heavily pretreated patients, with a median of 11 prior therapies, and 5 patients with prior anti-BCMA (bispecific antibody or chimeric antigen receptor T-cell [CAR-T]) therapy.25 There was only 1 MR and 5 SD, which may reflect the overall poor health of the T-cells of these heavily treated patients. Over 40 patients have now been treated, with dose-dependent responses and CRS as the main toxicity. Data on REGN5458 are available in just 3 elderly, heavily treated patients, showing a VGPR and an SD at the first dose level,26 and TNB-383B27 is in a phase 1 trial with no data reported yet.
There are limited data on the mechanisms of disease progression after BCMA-targeted treatments. However, recently, whereas the expression of BCMA on residual MM cells decreased more in patients responding to anti-BCMA CAR-T-cell therapy, BCMA expression increased at progression in most patients.28 Therefore, such patients could receive other anti-BCMA therapies, although the kinetics of T-cell recovery after fludarabine/cyclophosphamide lymphodepleting chemotherapy used before CAR-T may be important for the efficacy of bispecific antibodies. The sequencing of these therapies is an area of active investigation. For now, the choice of modality depends on the disease characteristics, side-effect profiles, and practical considerations outlined in Table 3.
Table 3.
Comparison of anti-BCMA modalities
| CAR-T cells | Bispecific antibodies | ADCs | |
|---|---|---|---|
| Pros | Unprecedented response rates, including MRD negativity in heavily pretreated patients | Off the shelf | Off the shelf |
| One-time intervention; long chemotherapy holiday, resulting in median PFS ∼1 year | Deep responses | Encouraging response rates | |
| Limited severe CRS; ? elderly | 1-hour infusion every 3 weeks | ||
| Can be given in community settings | No CRS | ||
| Can be given in community settings | |||
| Cons | Manufacturing time makes it impractical for patients with aggressive or rapidly progressing disease | ? Need for admissions with initial doses until CRS risk is low | Ocular toxicity; requires close collaboration with ophthalmology and may negatively impact quality of life |
| Requires complex infrastructure, with a stem cell laboratory and nursing and ICU/ER training; thus restricted to accredited centers | Limited data in triple class/pentarefractory | Thrombocytopenia | |
| CRS; ? role in elderly and frail patients | Dosing/schedule to be determined | Need for continuous treatment until progression | |
| Impact of bridging chemotherapy on duration of remission | Need for continuous treatment until progression | Modest ORR and PFS in triple class/pentarefractory | |
| Cost, given relapses occur, even in MRD− patients | Toxicities require further study; neuropathy, infections | ||
| Low white cells and platelets after CAR-T requiring ongoing/frequent monitoring and treatment | |||
| Management of CAR-T relapses challenging, especially if soon after fludarabine/cyclophosphamide, given impact on T cells |
ICU/ER, intensive care unit/emergency room.
As BCMA-targeted therapies move closer to approval and widespread use, there will be an unmet need for BCMA-refractory patients. Bispecifics with several other antigen targets are currently in phase 1 trials. The orphan G protein–coupled receptor, class C group 5 member D (GPRC5D), is a 7-transmembrane G protein–coupled receptor whose ligand and signaling mechanisms are unknown. However, GPRC5D messenger RNA is primarily expressed in plasma cells and all neoplastic plasma cells. There is low expression in normal tissues, except in hair follicles, and in MM, overexpression correlates with worse OS.29 Results from a phase 1 trial of the humanized immunoglobulin IgG4 GPRC5dxCD3 talquetamab (JNJ-64407564) involving >100 patients (to be presented at the 2020 American Society of Hematology annual meeting) include typically low-grade CRS in initial doses, as with other bispecific antibodies. Although efficacy has been seen at a variety of doses, including stringent CRs and durable responses, dose escalation is ongoing.
FCRH5, a B-cell lineage marker present universally on malignant plasma cells,30 is the target (along with CD3) of BFCR4350A.31 BFCR4350A has been tested in >40 patients, with CRS as the expected toxicity and responses seen at multiple dose levels. Two bispecifics, GBR134232 and AMG424,33 target CD38xCD3; it will be interesting to see how efficacy and safety compare with currently available anti-CD38 naked mAbs. Although still in preclinical development, bispecific anti-BCMA NK-cell engagers (for example, AFM-26 targeting CD1634 and CTX-441935 or CTX-857336 targeting NKp30) may prove to have more efficient ADCC with potentially less CRS and may represent another promising avenue of research.
Trispecific antibodies
Although still in the preclinical stages of development, trispecific antibodies provide an intriguing future approach to the treatment of MM (Figure 4). Bispecifics typically target a tumor antigen and CD3 to bring cytotoxic T cells into proximity and form an immunologic synapse with malignant cells, leading to T-cell activation against the tumor. However, in the absence of costimulation, there is a higher likelihood of anergy,37 leading to a suboptimal antitumor response. Wu, et al. recently demonstrated that a trispecific antibody targeting CD38, CD3, and CD28, a well-known costimulatory protein on T cells, was feasible to produce and showed very potent killing of CD38+ myeloma cell lines, 3- to 4-log higher than daratumumab.38 The trispecific agent suppressed myeloma growth in mice and promoted proliferation of memory and effector T cells and downregulation of regulatory T cells in primates. Similarly, efforts are ongoing to create trispecific NK-cell engagers, targeting CD16A and the MM antigens BCMA and CD200. Clinical trials of trispecific antibodies are eagerly awaited.
Figure 4.

Trispecific antibodies. (A) Trispecific T-cell engagers, with 1 binding domain for the myeloma antigen and 2 for the T-cell antigens, which include CD3 and a costimulatory antigen. These schematics are representative of trispecifics and not the actual constructs. (B) Trispecific NK-cell engager with 2 myeloma antigen-binding domains and 1 NK-cell antigen domain.
Designed ankyrin repeat proteins
Designed ankyrin repeat proteins (DARPins) are a class of genetically engineered antibody-mimetic proteins derived from ankyrin proteins, which are among the most common binding proteins in nature. They have high binding affinity and specificity for their designated targets.39 They are typically much smaller (<20 kDa) than antibodies and can be linked to inhibit multiple pathways at once (Figure 5).40 MP0250 is the first DARPin product to be tested in MM and contains vascular endothelial growth factor A and hepatocyte growth factor–neutralizing DARPins, although without an immunostimulatory component.41 Preliminary results from a phase 2 trial combining MP0250 8 mg/kg IV every 21 days with bortezomib and dexamethasone were recently reported42; common grade 3+ events were hypertension (40%), thrombocytopenia (25%), proteinuria (20%), and anemia (20%). All 20 patients had been exposed to an IMiD and PI, and the ORR was 40% (67% in patients who had received a PI with the prior regimen). These results show that DARPins are a feasible technology in MM, and the addition of immunostimulatory components may further increase the effectiveness of this class of therapy.
Figure 5.

Designed ankyrin repeat proteins (DARPins), with 2 DARPins serving as stabilizers in the circulation and 2 targeting myeloma antigens. DARPins are much smaller than antibodies and can be linked in various numbers and combinations.
Clinical case and conclusions
The patient was enrolled in a clinical trial with the ADC belantamab mafodotin. She experienced progression of disease after 2 cycles and was then treated with 1 cycle each of bortezomib-dexamethasone-cyclophosphamide-etoposide-cisplatin (V-DCEP) infusional chemotherapy and daratumumab-carfilzomib-thalidomide-dexamethasone with no response. After 1 cycle of the GPRC5dxCD3 bispecific talquetamab clinical trial, she achieved a VGPR, and after 5 cycles, she achieved and maintained a stringent CR, amounting to 10+ months of deep, durable disease control.
The treatment landscape of MM is rapidly changing, with 8 drugs approved by the US Food and Drug Administration in the past 8 years. Despite this encouraging progress, relapses of MM remain inevitable, and novel treatment approaches are urgently needed. Through various distinct technologies and classes of agents, immunotherapy holds promise as the next wave of novel therapies for MM.
References
- 1.Gandhi UH, Cornell RF, Lakshman A, et al. . Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019;33(9):2266-2275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alley SC, Okeley NM, Senter PD. Antibody-drug conjugates: targeted drug delivery for cancer. Curr Opin Chem Biol. 2010;14(4):529-537. [DOI] [PubMed] [Google Scholar]
- 3.Tai YT, Mayes PA, Acharya C, et al. . Novel anti-B-cell maturation antigen antibody-drug conjugate (GSK2857916) selectively induces killing of multiple myeloma. Blood. 2014;123(20):3128-3138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Trudel S, Lendvai N, Popat R, et al. . Targeting B-cell maturation antigen with GSK2857916 antibody-drug conjugate in relapsed or refractory multiple myeloma (BMA117159): a dose escalation and expansion phase 1 trial. Lancet Oncol. 2018;19(12):1641-1653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Trudel S, Lendvai N, Popat R, et al. . Antibody-drug conjugate, GSK2857916, in relapsed/refractory multiple myeloma: an update on safety and efficacy from dose expansion phase I study. Blood Cancer J. 2019;9(4):37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lonial S, Lee HC, Badros A, et al. . Pivotal DREAMM-2 study: Single-agent belantamab mafodotin (GSK2857916) in patients with relapsed/refractory multiple myeloma (RRMM) refractory to proteasome inhibitors (PIs), immunomodulatory agents, and refractory and/or intolerant to anti-CD38 monoclonal antibodies (mAbs) [abstract]. J Clin Oncol. 2020:38(15). Abstract 8536. [Google Scholar]
- 7.Nooka A, Stockerl-Goldstein K, Quach H, et al. . DREAMM-6: Safety and tolerability of belantamab mafodotin in combination with bortezomib/dexamethasone in relapsed/refractory multiple myeloma (RRMM) [abstract]. J Clin Oncol. 2020:38(15). Abstract 8502. [Google Scholar]
- 8.Shah NN, Krishnan AY, Shah ND, et al. . Preliminary results of a phase 1 dose escalation study of the first-in-class anti-CD74 antibody drug conjugate (ADC), STRO-001, in patients with advanced B-cell malignancies [abstract]. Blood. 2019;134(suppl 1). Abstract 5329. [Google Scholar]
- 9.Lee HC, Raje NS, Landgren O, et al. . Phase 1 study of the anti-BCMA antibody-drug conjugate AMG 224 in patients with relapsed/refractory multiple myeloma [published online ahead of print 21 April 2020]. Leukemia. doi:10.1038/s41375-020-0834-9. [DOI] [PubMed] [Google Scholar]
- 10.Tai Y-T, Xing L, Lin L, et al. . MEDI2228, a novel BCMA pyrrolobenzodiazepine antibody drug conjugate, overcomes drug resistance and synergizes with bortezomib and DNA damage response inhibitors in multiple myeloma. Clin Lymphoma Myeloma Leuk. 2019;19(10 suppl):e154-e155. [Google Scholar]
- 11.Sherbenou DW, Aftab BT, Su Y, et al. . Antibody-drug conjugate targeting CD46 eliminates multiple myeloma cells. J Clin Invest. 2016;126(12):4640-4653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fatholahi M, Valencia M, Mark A, et al. . TAK-573, an anti-CD38-targeted attenuated interferon alpha (IFNα) fusion protein, showed anti-myeloma tumor responses in combination with standard of care (SOC) agents in multiple myeloma (MM) xenograft tumor models in vivo. Clin Lymphoma Myeloma Leuk. 2019;19(10 suppl):e116.30509780 [Google Scholar]
- 13.Willert EK, Robinson GL, Higgins JP, et al. . TAK-169, an exceptionally potent CD38 targeted engineered toxin body, as a novel direct cell kill approach for the treatment of multiple myeloma [abstract]. Cancer Res. 2019;79(13 suppl). Abstract 2384. [Google Scholar]
- 14.Ailawadhi S, Kelly KR, Vescio RA, et al. . A phase I study to assess the safety and pharmacokinetics of single-agent lorvotuzumab mertansine (IMGN901) in patients with relapsed and/or refractory CD-56-positive multiple myeloma. Clin Lymphoma Myeloma Leuk. 2019;19(1):29-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Berdeja JG, Hernandez-Ilizaliturri F, Chanan-Khan A, et al. . Phase I study of lorvotuzumab mertansine (LM, IMGN901) in combination with lenalidomide (Len) and dexamethasone (Dex) in patients with CD56-positive relapsed or relapsed/refractory multiple myeloma (MM) [abstract]. Blood. 2012;120(21). Abstract 728. [Google Scholar]
- 16.Jagannath S, Heffner LT Jr, Ailawadhi S, et al. . Indatuximab ravtansine (BT062) monotherapy in patients with relapsed and/or refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2019;19(6):372-380. [DOI] [PubMed] [Google Scholar]
- 17.Kelly KR, Chanan-Khan A, Heffner LT, et al. . Indatuximab ravtansine (BT062) in combination with lenalidomide and low-dose dexamethasone in patients with relapsed and/or refractory multiple myeloma: clinical activity in patients already exposed to lenalidomide and bortezomib [abstract]. Blood. 2014;124(21). Abstract 4736. [Google Scholar]
- 18.Kontermann RE, Brinkmann U. Bispecific antibodies [published correction appears in Drug Discov Today. 2019;24(7):1422]. Drug Discov Today. 2015;20(7):838-847. [DOI] [PubMed] [Google Scholar]
- 19.Ellerman D. Bispecific T-cell engagers: towards understanding variables influencing the in vitro potency and tumor selectivity and their modulation to enhance their efficacy and safety. Methods. 2019;154:102-117. [DOI] [PubMed] [Google Scholar]
- 20.Saxena A, Wu D. Advances in therapeutic Fc engineering - modulation of IgG-associated effector functions and serum half-life. Front Immunol. 2016;7:580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Topp MS, Duell J, Zugmaier G, et al. . Anti-B-cell maturation antigen BiTE molecule AMG 420 induces responses in multiple myeloma. J Clin Oncol. 2020;38(8):775-783. [DOI] [PubMed] [Google Scholar]
- 22.Cho S-F, Lin L, Xing L, et al. . AMG 701 potently induces anti-multiple myeloma (MM) functions of T cells and IMiDs further enhance its efficacy to prevent MM relapse in vivo [abstract]. Blood. 2019;134(suppl 1). Abstract 135. [Google Scholar]
- 23.Usmani S, Mateos M-V, Nahi H, et al. . Phase I study of teclistamab, a humanized B-cell maturation antigen (BCMA) x CD3 bispecific antibody, in relapsed/refractory multiple myeloma (R/R MM) [abstract]. J Clin Oncol. 2020;38(15). Abstract 100. [Google Scholar]
- 24.Costa LJ, Wong SW, Bermúdez A, et al. . First clinical study of the B-cell maturation antigen (BCMA) 2+1 T cell engager (TCE) CC-93269 in patients (pts) with relapsed/refractory multiple myeloma (RRMM): interim results of a phase 1 multicenter trial [abstract]. Blood. 2019;134(suppl 1). Abstract 143. [Google Scholar]
- 25.Raje NS, Jakubowiak A, Gasparetto C, et al. . Safety, clinical activity, pharmacokinetics, and pharmacodynamics from a phase I study of PF-06863135, a B-cell maturation antigen (BCMA)-CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma (RRMM) [abstract]. Blood. 2019;134(suppl 1). Abstract 1869. [Google Scholar]
- 26.Cooper D, Madduri D, Lentzsch S, et al. . Safety and preliminary clinical activity of REGN5458, an anti-Bcma x anti-CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma [abstract]. Blood. 2019;134(suppl 1). Abstract 3176. [Google Scholar]
- 27.Buelow B, Choudry P, Clarke S, et al. . Pre-clinical development of TNB-383B, a fully human T-cell engaging bispecific antibody targeting BCMA for the treatment of multiple myeloma [abstract]. J Clin Oncol. 2018;36(15 suppl). Abstract 8034. [Google Scholar]
- 28.Cohen AD, Garfall AL, Stadtmauer EA, et al. . B cell maturation antigen-specific CAR T cells are clinically active in multiple myeloma. J Clin Invest. 2019;129(6):2210-2221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Atamaniuk J, Gleiss A, Porpaczy E, et al. . Overexpression of G protein-coupled receptor 5D in the bone marrow is associated with poor prognosis in patients with multiple myeloma. Eur J Clin Invest. 2012;42(9):953-960. [DOI] [PubMed] [Google Scholar]
- 30.Ise T, Nagata S, Kreitman RJ, et al. . Elevation of soluble CD307 (IRTA2/FcRH5) protein in the blood and expression on malignant cells of patients with multiple myeloma, chronic lymphocytic leukemia, and mantle cell lymphoma. Leukemia. 2007;21(1):169-174. [DOI] [PubMed] [Google Scholar]
- 31.Li J, Stagg N, Johnston J, et al. . Anti-FcRH5/CD3 T cell dependent bispecific antibody (TDB) for the treatment of multiple myeloma [abstract]. Blood. 2016;128(22). Abstract 4475. [Google Scholar]
- 32.Richter JR, Landgren CO, Kauh JS, et al. . Phase 1, multicenter, open-label study of single-agent bispecific antibody t-cell engager GBR 1342 in relapsed/refractory multiple myeloma [abstract]. J Clin Oncol. 2018;36(15 suppl). Abstract TPS3132. [Google Scholar]
- 33.Zuch de Zafra CL, Fajardo F, Zhong W, et al. . Targeting multiple myeloma with AMG 424, a novel anti-CD38/CD3 bispecific T cell-recruiting antibody optimized for cytotoxicity and cytokine release. Clin Cancer Res. 2019;25(13):3921-3933.2018. [DOI] [PubMed] [Google Scholar]
- 34.Ross T, Reusch U, Wingert S, et al. . Preclinical characterization of AFM26, a novel B cell maturation antigen (BCMA)-directed tetravalent bispecific antibody for high affinity retargeting of NK cells against myeloma [abstract]. Blood. 2018;132(suppl 1). Abstract 1927. [Google Scholar]
- 35.Draghi M, Schafer JL, Nelson A, et al. . Preclinical development of a first-in-class NKp30xBCMA NK cell engager for the treatment of multiple myeloma [abstract]. Cancer Res. 2019;79(13 suppl). Abstract 4972. [Google Scholar]
- 36.Watkins-Yoon J, Guzman W, Oliphant A, et al. . CTX-8573, an innate-cell engager targeting BCMA, is a highly potent multispecific antibody for the treatment of multiple myeloma [abstract]. Blood. 2019;134(suppl 1). Abstract 3182. [Google Scholar]
- 37.Esensten JH, Helou YA, Chopra G, Weiss A, Bluestone JA. CD28 Costimulation: from mechanism to therapy. Immunity. 2016;44(5):973-988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wu L, Seung E, Xu L, et al. . Trispecific antibodies enhance the therapeutic efficacy of tumor-directed T cells through T cell receptor co-stimulation. Nat Can. 2020;1(1):86-98. [DOI] [PubMed] [Google Scholar]
- 39.Plückthun A. Designed ankyrin repeat proteins (DARPins): binding proteins for research, diagnostics, and therapy. Annu Rev Pharmacol Toxicol. 2015;55(1):489-511. [DOI] [PubMed] [Google Scholar]
- 40.Hammill JA, VanSeggelen H, Helsen CW, et al. . Designed ankyrin repeat proteins are effective targeting elements for chimeric antigen receptors. J Immunother Cancer. 2015;3(1):55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Binz HK, Bakker TR, Phillips DJ, et al. . Design and characterization of MP0250, a tri-specific anti-HGF/anti-VEGF DARPin® drug candidate. MAbs. 2017;9(8):1262-1269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Grząśko N, Knop S, Goldschmidt H, et al. . The MP0250-CP201 mirror study: a phase 2 study update of MP0250 plus bortezomib and dexamethasone in relapse/refractory multiple myeloma (RRMM) patients previously exposed to proteasome inhibitors and immunomodulatory drugs [abstract]. Blood. 2019;134(suppl 1). Abstract 1899. [Google Scholar]