

Abstract
Purpose:
Relaxin is a polypeptide hormone produced by the corpus luteum and the decidua in females and by the prostate in males. It has vasodilatory and antifibrotic effects. In the past, it has been reported that injection of relaxin hormone has caused a reduction in the intraocular pressure although its mechanism has not yet been fully understood and the expression of relaxin receptors has not yet been evident in the human eye. Therefore, the purpose of this current study was to examine the presence of relaxin receptors in the human eye anterior segment.
Methods:
This is an interventional non-randomized study. Patients with primary open-angle glaucoma who underwent trabeculectomy were recruited. During the surgery, a punch biopsy (including the cornea, sclera, trabecular meshwork, and Schlemm's canal) was taken and stained with hematoxylin-eosin, and immunohistochemistry staining for relaxin/insulin-like family peptide receptor 1 (RXFP1).
Results:
A positive staining was noted for RXFP1 in the inner uveal, corneoscleral, and cribriform meshwork and Schlemm's canal's endothelium. Negative staining for RXFP1 was noted in the cornea and sclera.
Conclusion:
RXFP1 is present in the anterior segment drainage system of the human eye. Therefore, this receptor may have an active role in regulating the outflow facility and in the reduction of intraocular pressure.
Keywords: Drainage system, glaucoma, relaxin, Schlemm's canal
Relaxin is a protein hormone that was first discovered as a pregnancy hormone.[1] It was thought to be produced only by the corpus luteum in pregnant women causing cervical softening, pubic ligament elongation, and inhibition of spontaneous myometrial contractile activity.[2] Later, it was found to be produced also by the heart,[3] endometrium,[4] mammary gland,[5] placenta,[6] and prostate.[7] Moreover, the relaxin receptors have been detected in reproductive tissues,[8] brain,[9] kidney,[10] lung,[11] and blood cells.[12]
The relaxin hormone is known to have a vasodilatory effect.[11] Therefore, it is used as an experimental treatment in various diseases such as prostate cancer,[13] cerebral cavernoma,[14] osteosarcoma,[15] chronic heart failure,[16] and cancer.[17]
Primary open-angle glaucoma (POAG) is a complex, multifactorial neurodegenerative disease that leads to progressive damage to the optic nerve and irreversible visual field loss. It is the leading cause of irreversible blindness and the second leading cause of blindness worldwide.[18] The main risk factor for glaucoma evolution and progression (and the only one which can be treated) is the increase of intraocular pressure (IOP), caused by multiple mechanisms, such as dysfunction and/or increase resistance in the human eye drainage system or uncontrolled aqueous humor production.[19]
In the human eye, aqueous humor is leaving the anterior chamber through the “conventional” outflow system which includes the trabecular meshwork (TM), Schlemm's canal (SC) collector channels, and episcleral veins.[20]
There are few case reports that described relaxin as a hormone that decreases IOP in humans: Paterson et al. reported that after intramuscular injection of relaxin hormone, the IOP of the participants decreased and in the tonography an enhancement of the outflow facility was found.[21] Moreover, there are few reports about IOP reduction in the third trimester in healthy, pregnant women. This finding may indicate that there is a connection between relaxin secretion and IOP control.[22,23]
The purpose of this current study is to examine the presence of relaxin receptors in the anterior segment of the human eye in order to enhance further understanding of the relaxin induced IOP reduction mechanism.
Methods
Patient selection and data collection
This study is a non-randomized interventional study. Patients with POAG who underwent a trabeculectomy surgery during April- September 2015 were recruited. Inclusion and exclusion criteria are shown in Table 1. The study was approved by the local institutional review board. Written informed consent was obtained from all subjects and the study adhered to the tenets of the Declaration of Helsinki. All patients underwent a trabeculectomy surgery, as described below, by a single surgeon (SM). During the surgery, a block of tissue including cornea, sclera TM, and SC was taken and stained as described in the histology section. Peripheral iridectomy was also performed. The iris was processed for histology using the same methodology.
Table 1.
Inclusion and exclusion criteria
| Inclusion criteria |
| Patients with primary open-angle glaucoma refractory to anti-glaucoma medications |
| Glaucoma patients’ who referred to their first trabeculectomy surgery in this eye |
| Patient without other intraocular diseases that may increase the IOP |
| Male or female of any race, at least 18 years of age |
| Has provided verbal and written informed consent |
| Exclusion Criteria |
| Patients with primary open-angle glaucoma which is end-stage disease |
| Patient who underwent trabeculectomy surgery in the same eye in the past |
| Patient who underwent laser trabeculoplasty |
| Patient with other intraocular disease that may increase the IOP |
| Patient with a history of ocular conditions that may affect the eye angle’s anatomic organs |
| Pregnant women |
| Male or female younger than 18 years of age |
Trabeculectomy surgery
The operated eye was prepped and draped in the usual sterile fashion for intraocular surgery. An eyelid speculum was placed into the right eye. Lidocaine eye drops 4% (DR. Fischer Ltd, Bnei Brak, Israel) was placed for topical anesthesia. Using conjunctival forceps and Vannas scissors, a superior limbal peritomy was performed. Preservative-free lidocaine 1% on a 30-gauge cannula was then injected into the subconjunctival area to achieve anesthesia. Westcott scissors were then used to perform posterior, nasal, and temporal Tenon's dissection. 0.12 mm forceps were used to grasp the sclera and the scleral bed was cleaned with a crescent blade. A trapezoidal scleral flap was then outlined using a diamond knife. The crescent blade was then used to dissect the scleral flap to the limbus. Sponges soaked in mitomycin C (Accord, North Carolina, United States) 0.4 mg/mL were then applied beneath the conjunctiva for the duration of 2 min. The sponges were then removed and the area was irrigated copiously with balanced salt solution (BSS). An MVR blade was then used to create a paracentesis at the 6 o'clock position. The scleral flap was then grasped with a 0.12 mm forceps and the anterior chamber was entered. A Kelly Descemet membrane punch was used to remove a portion of the TM, iris, and SC. Bonn forceps and Vannas scissors were then used to create a surgical iridectomy The scleral flap statured with 10-0 nylon sutured and adjusted for the appropriate flow. Once the appropriate flow was established, the sutures were tied and then buried. The conjunctiva and Tenon's fascia were then reapproximated to the limbus using interrupted 10-0 nylon sutures. The anterior chamber was noted to be deep with no leakage coming from the wound. At the end of the surgery, oflox (ofloxacin, Allergan, New Jersey, United States) and dexamycin (dexamethasone sodium phosphate, neomycin sulfate, Teva, Petach-Tikva, Israel) were applied to the operated eye and the eye was covered with eye shield.
Histology
Tissue samples were fixed in 4% paraformaldehyde. After dehydration with increasing ethanol concentrations, tissue pieces were cleared in chloroform and embedded in paraffin. Four micron sections were then prepared using a Leica RM2155 microtome. After removal of the paraffin by heating at 60 Celsius degree, sections were washed in toluene, rehydrated with decreasing ethanol concentrations, and were finally washed with water. Slides then stained with hematoxylin and eosin (H and E) for light microscopy assessment, three consecutive sections on each slide. A specialist ocular pathologist examined the tissues and decided which eye structures' are in each section.
Immunohistochemistry
Paraffin sections (4 μm) were deparaffinized and rehydrated. Following antigen retrieval (in citrate buffer pH 6.0), sections were incubated in 30% hydrogen peroxide solution for 10 min at RT, followed by blocking solution from Histostain®—Plus Kit (Invitrogen, Carlsbad, California, United States) for 30 min at RT. Then, sections were incubated with RXFP1 polyclonal antibody (Abnova, Taipei, Taiwan) for 20 h at 4°C followed by secondary antibody staining protocol following manufacturer's instruction (Histostain—Plus Kit Invitrogen, Carlsbad, California, United States). Skeletal muscle was used as a positive control according to the manufacturer's instructions.
Results
Six tissue samples with the cornea, TM and SC were taken from six patients (three males, three females) with POAG who underwent trabeculectomy due to uncontrolled glaucoma.
As a positive control (according to manufacture instructions), a specimen of a skeletal muscle from the eyelid of a 72 years old patient who underwent blepharoplasty and agreed for pathological evaluation was taken. The muscle sample was sectioned and stained in H and E and then immunohistochemical analyses were performed to reveal the distribution of RXFP1. RXFP1 was identified in the endomysium layer of each individual myocyte in the sample [Fig. 1a and b]. Thereafter, all trabeculectomy samples were sectioned and stained with H and E [Fig. 2a]. Immunohistochemical analyses were performed to reveal the presence and distribution of RXFP1 in the TM and SC.
Figure 1.
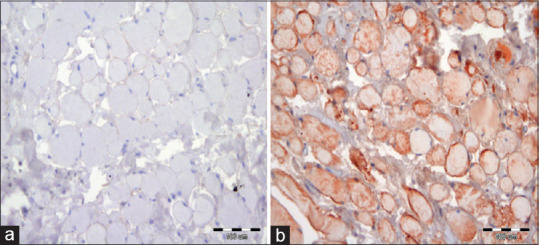
The histology of the orbicularis oculi muscle. (a) Negative-staining control -slide not incubated with primary antibody (magnification 200×), (b) immunohistochemistry red staining of the relaxin receptor (magnification 200×)
Figure 2.
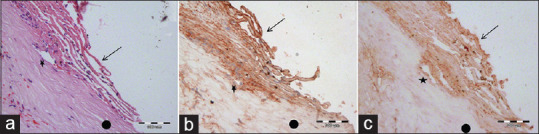
Slides of two different patients who underwent trabeculectomy. (a) H and E staining of a slide of a 68 years old female who underwent trabeculectomy—trabecular meshwork (Arrow), Schlemm's canal (Asterix), and sclera (Round) (magnification 200×). (b) An immunohistochemistry staining of relaxin receptors of the same patient—trabecular meshwork (Arrow), Schlemm's canal (Asterix), and sclera (Round) (magnification 200×). (c) An immunohistochemistry staining (red) of relaxin receptors of 70 years old male who underwent trabeculectomy—trabecular meshwork (Arrow), Schlemm's canal (Asterix), and sclera (Round) (magnification 200×)
Positive staining for RXFP1 was noted in the inner uveal, corneoscleral, and cribriform meshwork. RXFP1 was identified also in the endothelium of SC, but not in the part of the cornea and sclera that was observed in those sections [Fig. 2b and c]. Moreover, RXFP1 was found also in the iris that was taken from 68 years old female who underwent peripheral iridectomy during the trabeculectomy surgery [Fig. 3].
Figure 3.
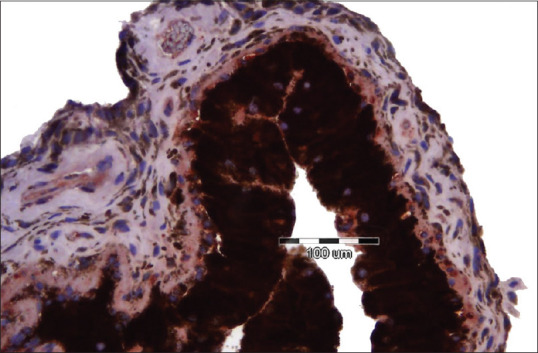
An immunohistochemistry staining of relaxin receptors in an iris
Discussion
Relaxin is a protein hormone of about 6000 Daltons. The hormone belongs to the relaxin peptide family within the insulin superfamily of hormones. The relaxin family peptides produce their physiological effects by activating a group of four G protein-coupled receptors (GPCRs) and RXFP1–4.[24] Human relaxins H1 and H2 can activate both RXFP1 and RXFP2 which are the two main relaxin receptor isoforms.[25] RXFP3 is thought to function primarily in the mouse brain[26] while the RXFP4 system stimulates appetite and activates colon motility to control food intake and glucose homeostasis in the mouse intestine.[27]
The relaxin hormone has vasodilatory effects and antifibrotic effects.[10] Relaxin has traditionally been associated with the genital tract prior to parturition during pregnancy in lower species. Contrary to lower species, human relaxin plasma levels are highest during the first trimester.[24] Relaxin was found to elongate the interpubic ligament, expand the vessels of the kidney, reduce systemic vascular resistance (SVR) and the consequent increase in cardiac output (CO).[12,28,29] RXFP1 and RXFP2 receptors have been identified in ligaments, cartilage, and synovium.[30,31] This may indicate that in those sites, relaxin may be involved with relaxing the fibrous tissue in these organs.
Relaxin 3 peptide receptors were found in the eyes of zebra fish.[14] Recently, it was reported that Relaxin 2 fails to lower IOP and to dilate retinal vessels in rats.[32] In the human eye, Hampel et al. found that insulin-like peptide hormone relaxin 2, (RLN2) RXFP1, and RXFP2 are expressed at the ocular surface and in tears and, therefore, it may serve as a potential future therapeutic target during wound healing.[33]
The effect of the relaxin system on IOP has not been yet fully understood. Only one study mentioned IOP reduction after injection of relaxin.[21] Few reports found that there is a decrease in IOP in the third trimester of pregnant women compared to nonpregnant women or to the first or second trimester. The hypothesis in those reports was that this decrease is due to an increase in the secretion of relaxin and progesterone.[16,32] Quereshi et al. and Saylik et al. found that IOP is lower in the third trimester in multigravida than in primigravida.[17,34] They assumed that this decrease is most likely related to the presence of higher levels of hormones, particularly estrogen, progesterone and relaxin compared in multigravida than in primigravida. However, the presence of a relaxin receptor on the eyes' angle has never been examined. Therefore, to the best of our knowledge, our study is the first to examine the presence of relaxin receptors in the human eye angle.
In our study, RXFP1 was found in the TM and in the endothelium of SC, which is known to have a major role in the regulation of the eye drainage system resistance. RXFP1 was not detected in the sclera and cornea. The presence of relaxin receptors through the drainage system may indicate that relaxin has a role in IOP regulation. A clinical study that will examine if administration of systemic or topical relaxin cause to decrease in the ocular drainage system resistance, increase in the ocular outflow and decrease in IOP, should be done.
Our study has some limitations. First, a small number of patients were included in this study. Second, patients enrolled in this study were not naive to therapy. Thus, one may not rule out that anti-glaucoma medications used for long periods, or the duration of the disease have modified tissues and the expression of relaxin receptors. Third, this current study examined only one relaxin receptor through an indirect method and not through immunofluorescence or western blot. Moreover, only a punch biopsy was done. Larger biopsies may support our findings exclude the expression of the receptors in the cornea as a whole and also enable to capture the ciliary body. In addition, it would be interesting to examine the presence of the receptors in healthy patients in comparison to glaucoma patients. In addition, in further studies, maybe blood tests for systemic relaxin hormone that should be taken.
All of the patients in this current study were postmenopausal women and men. In accordance with the assumption that in the third trimester the level of relaxin hormone increases, it will be interesting to examine the level of relaxin receptors in the angle in pregnant women in the third trimester compared to men and postmenopausal women.
Conclusion
In conclusion, we found for the first time that relaxin receptor RXFP1 is present in the human drainage system (TM and SC). We suggest that relaxin may have an active role in regulating outflow facility and IOP in the human eye. Further larger studies are required in order to shed more light on its role in the human eye and his potential role in glaucoma therapy.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Dewar AD, Hall K, Newton WH. Potentiation of the vaginal response to oestrone by the relaxin fraction of pregnant rabbit serum. J Physiol. 1946;105:37. [PubMed] [Google Scholar]
- 2.Becker GJ, Hewitson TD. Relaxin and renal fibrosis. Kidney Int. 2001;59:1184–5. doi: 10.1046/j.1523-1755.2001.0590031184.x. [DOI] [PubMed] [Google Scholar]
- 3.Osheroff PL, Cronin MJ, Lofgren JA. Relaxin binding in the rat heart atrium. Proc Natl Acad Sci U S A. 1992;89:2384–8. doi: 10.1073/pnas.89.6.2384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schramm W, Einer-Jensen N, Brown MB, Mc Cracken JA. Effect of four primary prostaglandins and relaxin on blood flow in the ovine endometrium and myometrium. Biol Reprod. 1984;30:523–31. doi: 10.1095/biolreprod30.3.523. [DOI] [PubMed] [Google Scholar]
- 5.Bongers-Binder S, Burgardt A, Seeger H, Voelter W, Lippert TH. Distribution of immunoreactive relaxin in the genital tract and in the mammary gland of non-pregnant women. Clin Exp Obstet Gynecol. 1991;18:161–4. [PubMed] [Google Scholar]
- 6.Gautieri RF, Ciuchta HP. Effect of certain drugs on perfused human placenta I Narcotic analgesics, serotonin, and relaxin. J Pharm Sci. 1962;51:55–8. doi: 10.1002/jps.2600510109. [DOI] [PubMed] [Google Scholar]
- 7.Hansell DJ, Bryant-Greenwood GD, Greenwood FC. Expression of the human relaxin H1 gene in the decidua, trophoblast, and prostate. J Clin Endocrinol Metab. 1991;72:899–904. doi: 10.1210/jcem-72-4-899. [DOI] [PubMed] [Google Scholar]
- 8.MacLennan AH, Grant P, Borthwick AC. Relaxin and relaxin c-peptide levels in human reproductive tissues. Reprod Fertil Dev. 1991;3:577–83. doi: 10.1071/rd9910577. [DOI] [PubMed] [Google Scholar]
- 9.Ma S, Gundlach AL. Relaxin-family peptide and receptor systems in brain: Insights from recent anatomical and functional studies. Adv Exp Med Biol. 2007;612:119–37. doi: 10.1007/978-0-387-74672-2_9. [DOI] [PubMed] [Google Scholar]
- 10.Hsu SY. Cloning of two novel mammalian paralogs of relaxin/insulin family proteins and their expression in testis and kidney. Mol Endocrinol. 1999;13:2163–74. doi: 10.1210/mend.13.12.0388. [DOI] [PubMed] [Google Scholar]
- 11.Tang ML, Samuel CS, Royce SG. Role of relaxin in regulation of fibrosis in the lung. Ann N Y Acad Sci. 2009;1160:342–7. doi: 10.1111/j.1749-6632.2008.03825.x. [DOI] [PubMed] [Google Scholar]
- 12.Jeyabalan A, Shroff SG, Novak J, Conrad KP. The vascular actions of relaxin. Adv Exp Med Biol. 2007;612:65–87. doi: 10.1007/978-0-387-74672-2_6. [DOI] [PubMed] [Google Scholar]
- 13.Neschadim A, Summerlee AJ, Silvertown JD. Targeting the relaxin hormonal pathway in prostate cancer. Int J Cancer. 2015;137:2287–95. doi: 10.1002/ijc.29079. [DOI] [PubMed] [Google Scholar]
- 14.Gewiss C, Hagel C, Krajewski K. Cerebral cavernomas in adults and children express relaxin? J Neurosurg Pediatr. 2019:1–7. doi: 10.3171/2019.9.PEDS19333. doi: 10.3171/2019.9.PEDS19333. [DOI] [PubMed] [Google Scholar]
- 15.Huang H, Zheng HY, Liu ZL, Zhang L. Prognostic significance of relaxin-2 and S100A4 expression in osteosarcoma. Eur Rev Med Pharmacol Sci. 2014;18:2828–34. [PubMed] [Google Scholar]
- 16.Martins RC, Pintalhão M, Leite-Moreira A, Castro-Chaves P. Relaxin and the cardiovascular system: From basic science to clinical practice. Curr Mol Med. 2020;20:167–84. doi: 10.2174/1566524019666191023121607. [DOI] [PubMed] [Google Scholar]
- 17.Rizvi S, Gores GJ. The two faces of relaxin in cancer: Antitumor or protumor? Hepatology. 2020;71:1117–9. doi: 10.1002/hep.30998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–7. doi: 10.1136/bjo.2005.081224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130:429–40. doi: 10.1016/s0002-9394(00)00538-9. [DOI] [PubMed] [Google Scholar]
- 20.Swaminathan SS, Oh DJ, Kang MH, Rhee DJ. Aqueous outflow: Segmental and distal flow. J Cataract Refract Surg. 2014;40:1263–72. doi: 10.1016/j.jcrs.2014.06.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Paterson GD, Miller SJ. Hormonal influence in simple glaucoma. A preliminary report. Br J Ophthalmol. 1963;47:129–37. doi: 10.1136/bjo.47.3.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Atas M, Duru N, Ulusoy DM, Altınkaynak H, Duru Z, Açmaz G, et al. Evaluation of anterior segment parameters during and after pregnancy. Cont Lens Anterior Eye. 2014;37:447–50. doi: 10.1016/j.clae.2014.07.013. [DOI] [PubMed] [Google Scholar]
- 23.Efe YK, Ugurbas SC, Alpay A, Ugurbas SH. The course of corneal and intraocular pressure changes during pregnancy. Can J Ophthalmol. 2012;47:150–4. doi: 10.1016/j.jcjo.2012.01.004. [DOI] [PubMed] [Google Scholar]
- 24.Bathgate RA, Halls ML, van der Westhuizen ET, Callander GE, Kocan M, Summers RJ. Relaxin family peptides and their receptors. Physiol Rev. 2013;93:405–80. doi: 10.1152/physrev.00001.2012. [DOI] [PubMed] [Google Scholar]
- 25.Scott DJ, Rosengren KJ, Bathgate RA. The different ligand-binding modes of relaxin family peptide receptors RXFP1 and RXFP2. Mol Endocrinol. 2012;26:1896–906. doi: 10.1210/me.2012-1188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Scott DJ, Layfield S, Riesewijk A, Morita H, Tregear GW, Bathgate RA. Characterization of the mouse and rat relaxin receptors. Ann N Y Acad Sci. 2005;1041:8–12. doi: 10.1196/annals.1282.002. [DOI] [PubMed] [Google Scholar]
- 27.McGowan BM, Stanley SA, Donovan J, Thompson EL, Patterson M, Semjonous NM, et al. Relaxin-3 stimulates the hypothalamic-pituitary-gonadal axis. Am J Physiol Endocrinol Metab. 2008;295:E278–86. doi: 10.1152/ajpendo.00028.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Conrad KP. Renal hemodynamics during pregnancy in chronically catheterized, conscious rats. Kidney Int. 1984;26:24–9. doi: 10.1038/ki.1984.129. [DOI] [PubMed] [Google Scholar]
- 29.Conrad KP, Gandley RE, Ogawa T, Nakanishi S, Danielson LA. Endothelin mediates renal vasodilation and hyperfiltration during pregnancy in chronically instrumented conscious rats. Am J Physiol. 1999;276:F767–76. doi: 10.1152/ajprenal.1999.276.5.F767. [DOI] [PubMed] [Google Scholar]
- 30.Lubahn J, Ivance D, Konieczko E, Cooney T. Immunohistochemical detection of relaxin binding to the volar oblique ligament. J Hand Surg Am. 2006;31:80–4. doi: 10.1016/j.jhsa.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 31.Clifton KB, Rodner C, Wolf JM. Detection of relaxin receptor in the dorsoradial ligament, synovium, and articular cartilage of the trapeziometacarpal joint. J Orthop Res. 2014;32:1061–7. doi: 10.1002/jor.22640. [DOI] [PubMed] [Google Scholar]
- 32.Hampel U, Träger K, Liu H, Teister J, Grus F, Prokosch-Willing V. Relaxin 2 fails to lower intraocular pressure and to dilate retinal vessels in rats. Int Ophthalmol. 2019;39:847–51. doi: 10.1007/s10792-018-0884-4. [DOI] [PubMed] [Google Scholar]
- 33.Hampel U, Klonisch T, Makrantonaki E, Sel S, Schulze U, Garreis F, et al. Relaxin 2 is functional at the ocular surface and promotes corneal wound healing. Invest Ophthalmol Vis Sci. 2012;53:7780–90. doi: 10.1167/iovs.12-10714. [DOI] [PubMed] [Google Scholar]
- 34.Saylik M, Saylik SA. Not only pregnancy but also the number of fetuses in the uterus affects intraocular pressure. Indian J Ophthalmol. 2014;62:680–2. doi: 10.4103/0301-4738.120208. [DOI] [PMC free article] [PubMed] [Google Scholar]