

Abstract
Contrary to most theories of alcohol craving, which only consider desires to use, the Ambivalence Model of Craving (AMC) conceptualizes craving bi-dimensionally as the concurrent desires to consume (approach) and desires not to consume (avoid) alcohol. Consistent with the AMC, the Approach and Avoidance of Alcohol Questionnaire (AAAQ) is a 14-item self-reported measure designed to assess alcohol approach and avoidance inclinations. Scores on the AAAQ have been shown to have high reliability and validity in clinical and college student populations, with a two-factor solution emerging in clinical samples of patients with Alcohol Use Disorders (AUDs) and a three-factor solution in samples of college students. However, despite a number of studies examining the use of the AAAQ in clinical and college student samples, to the best of our knowledge there have not been any psychometric evaluations of the AAAQ in community samples. The current study examined the psychometric properties of the AAAQ by examining the factor structure in a community sample (N = 537). Consistent with the results of previous studies utilizing non-clinical samples, a three-factor solution fit the data best and was invariant across gender. Additionally, all three factors were significantly associated with variables of drinking behavior. These results suggest that the AAAQ provides valid and reliable scores that measure approach and avoidance inclinations in community populations.
Keywords: Approach, Avoidance, Craving, Alcohol, Psychometric, Community Sample
Alcohol Use Disorders (AUDs) are highly prevalent in the United States, with recent estimates suggesting that 14% of adults meet DSM-5 (American Psychiatric Association, 2013) criteria for diagnosis within a 12 month period and 29% at some point during their lifetime (Grant et al., 2015). With the reintroduction of craving as a criterion for AUD in the Diagnostic and Statistical Manual (DSM-5) there has been a renewed interest in the role of craving in the etiology and maintenance of problematic alcohol use. Although craving is commonly thought to be important in the transition from normal to problematic use, and in relapse to problematic use after treatment, findings have been inconsistent (Drummond, 2001; Lowman, Hunt, Litten, & Drummond, 2000; Michael A. Sayette, 2016). Additionally, while craving is generally considered to be the conscious experience of desiring alcohol (Drummond, 2001), even this simple definition is not agreed upon and it may be less contentious to state that craving is a subjective state associated with alcohol use (Drummond, 2001; Pickens & Johanson, 1992).
Craving is frequently assessed utilizing only a single binary item capturing a yes or no response. This is evident in both the International Classification of Diseases (ICD-10; World Health Organization, 2015) and DSM-5 (American Psychiatric Association, 2013), as well as large national surveys such as the National Epidemiological Survey on Alcohol and Related Conditions (NESARC; Grant et al., 2015) and the United States National Comorbidity Study (NCS; Kessler & Merikangas, 2004). Single item ratings are used often in both clinical and research applications as they are easy to understand and administer and are well suited for repeated assessments in laboratories, clinics, and naturalistic settings (Kavanagh et al., 2013). However, despite the convenience of measuring craving using a single binary item, the reliability and validity of these assessments is highly questionable (M. A. Sayette et al., 2000).
Traditionally, substance abuse researchers have measured craving as a unidimensional construct of urge intensity (Kozlowski & Wilkinson, 1987). With this conceptualization, only an individual’s desire to use alcohol is considered. However, along with the desire to use alcohol, most problematic substance users also express desires to avoid using alcohol, resulting in a state of ambivalence or conflicting motivations (e.g., Smith-Hoerter, Stasiewicz, & Bradizza, 2004). This conflicting nature of substance abuse is not effectively captured when only focusing on the traditional construct of craving, which only considers desires to use alcohol and ignores simultaneous and competing desires to avoid use. The Ambivalence Model of Craving (AMC; Breiner, Stritzke, & Lang, 1999) views craving as the “evaluative space” resulting from the co-activation of both desires to use (approach inclinations) and desires to avoid using alcohol (avoidance inclinations). These inclinations represent two motivational pathways that influence an individual’s decision to engage in alcohol use (Stritzke, McEvoy, Wheat, Dyer, & French, 2007). The AMC considers approach and avoidance inclinations to result from a combination of historical (e.g., biochemical reactivity, personality, environment, and past reinforcement) and current factors (e.g., positive and negative incentives and availability of alternative valued activities), including the reinforcing and negative consequences of use (see Breiner et al., 1999). Thus, people who experience and expect positive outcomes will be more inclined to approach alcohol and people who experience or expect negative outcomes will be more inclined to avoid alcohol. Importantly, individuals can be high on both approach and avoidance inclinations, which results in a conflicting state of ambivalence.
The AMC allows for a broader conceptualization of craving than had traditionally been considered. In order to assess approach and avoidance, the Approach and Avoidance to Alcohol Questionnaire (AAAQ; McEvoy, Stritzke, French, Lang, & Ketterman, 2004) was created. Additionally, this measure was developed largely in consideration of the AMC while also integrating broader theoretical considerations. Specifically, a neuroanatomical model of craving (Anton, 1999) suggests that there is a distinction between the desire to use alcohol and a stronger, pathological compulsion to drink. This compulsive drinking behavior results from changes in brain activity associated with prolonged exposure to alcohol. The simple desire to drink reflects a “mild approach”, which is observed among non-problematic drinkers. The obsessive compulsive dimension reflects a “strong approach” and can be seen in alcohol dependent individuals. With this in mind, items in the AAAQ were included to independently assess approach and avoidance inclinations as well as to reflect different intensities in desires to use. McEvoy et al. (2004) tested competing hypotheses that a three-factor structure would support the distinction between approach intensities suggested by the neuroanatomical model, while a two-factor structure would support a two-dimensional model consistent with the AMC.
Importantly, McEvoy et al. (2004) developed the AAAQ using two large university samples, using both exploratory and confirmatory factor analysis. The results of these analyses supported a three-factor solution. These factors were labeled Resolved/Regulated (i.e., avoidance), Inclined/Indulgent (i.e., mild approach), and Obsessed/Compelled (i.e., strong approach). The authors concluded that their finding was consistent with the notion put forth by Anton (1999), which described the approach dimension as including a threshold where a simple desire to drink becomes an obsessive compulsive behavior. Further, responses to the AAAQ captured the variance in drinking behaviors, such that individuals higher on the Inclined/Indulgent subscale had the highest levels of drinking while those high on Resolved/Regulated items had the lowest levels of drinking. Notably, the Obsessed/Compelled items was only significantly associated with frequency, but not quantity, of drinking. Further, the association with frequency was stronger for the Inclined/Indulgent items (β = .46) than the Obsessed/Compelled (β = .24). However, both approach scales were significant predictors of alcohol-related problems, but again the association was stronger for the Inclined/Indulgent scale (β = 0.49) than the Obsessed/Compelled scale (β = .23).
Conversely, research using this measure with clinical samples has not supported the three-factor structure. Studies examining the factor structure of the AAAQ using samples of alcohol dependent individuals in treatment have derived a two-factor solution by which the two approach subscales are combined (e.g., Klein, Stasiewicz, Koutsky, Bradizza, & Coffey, 2007; Schlauch et al., 2013). Subsequently, Klein and Anker (2013) compared the two-factor structure and three-factor structure of the AAAQ in a sample of alcohol-dependent individuals in residential treatment. Their results demonstrated that the three-factor structure fit the data better than the two, however, the two approach factors were highly correlated (r = .82) and subsequent validity analyses combined the two approach subscales. As such, no meaningful differences were found between the two approach subscales, suggesting that such a distinction is not necessary in clinical samples.
Though the AAAQ has been evaluated in clinical and college student samples, it has yet to be evaluated in community samples. In a community sample, consumption and problem severity will vary much more widely than a clinical sample. In this way, the community may be more similar to a college student sample and the three-factor solution may be more appropriate as they are more likely to demonstrate a wide range of approach inclinations representing both the inclined/indulgent inclinations found in non-problem drinkers and the stronger obsessed/compelled inclinations that are more characteristic of problematic drinking. However, college students are often considered a distinct population in terms of drinking behaviors and this may be reflected in the functioning of the AAAQ. As such, the factor structure of the AAAQ in the community remains unknown. Additionally, though the factor structure of the AAAQ has been evaluated, currently no studies have explored whether the measure is invariant across gender. Although no research has suggested that approach and avoidance inclinations vary as a function of gender, it is possible that items of the AAAQ may perform differently for men and women due to several factors including, but not limited to, social desirability, gender norms, or differences in the consequences related to use. For example, a major underlying principle of the Ambivalence Model of Craving and AAAQ is that approach and avoidance develop as a result of both the positive and negative consequences of use. Research has demonstrated that such consequences are likely to vary by gender (e.g., Park & Grant, 2005), which may in turn affect item functioning.
The purpose of the current study was to evaluate the psychometric properties of the AAAQ in a community sample. Specifically, we conducted a confirmatory factor analysis to examine the factor structure of the AAAQ in a community sample, including testing for invariance across gender, followed by additional validity analyses examining the relationship between subscales of the AAAQ and drinking-related variables. Based on theory and previous research in both college and clinical samples, we hypothesized that the three-factor solution would best fit the data over a two-factor solution. Community samples are made up primarily of people who do not meet the criteria for AUD and have a wide range of drinking behaviors, and theoretically should demonstrate less intense approach inclinations than those characteristic of clinical samples. These compulsive urges (intense approach inclinations) are drastically different than the more benign mild urges to drink, and this distinction is posited to differentiate clinical from non-clinical samples (Anton, 1999). Therefore, although community samples may include heavy drinkers, they are less likely to include those who are alcohol dependent and fall into the “obsessed/compelled” category.
Method
Participants.
In total, 537 individuals recruited through Amazon’s Mechanical Turk (MTurk) completed the study. To be eligible for the study, participants were required to (a) be at least 18 years of age; (b) be English speaking; (c) report drinking alcohol at least once in the past month; (d) reside in the United States; and (e) have a 90% hit approval rate on MTurk (this indicates a majority of their work on MTurk has been approved). Approximately half of the sample was male (53.3%), with an average age of 33.0 (SD = 8.85) years. The majority of participants were Caucasian/White (78.4%; 6.9% African American, 7.3% Asian, 7.4% Multi-racial or Other) and employed full time (65.4%; 14.5% part time, 12.3% unemployed, 6.3% students, 1.5% other). Finally, the sample included a range of incomes with approximately 54% reporting annual income below $40,000 (10.6% $10,000 or below, 13.6% $10,000-20,000, 15.3% $20,000-30,000, 14.3% $30,000-40,000, 12.1% $40,000-50,000, 10.1% $50,000-60,000, 8.8% $60,000-70,000, 5.8% $70,000-80,000, 9.4% $80,000 or above), and approximately 40% indicating marital status as single (39.6%; 37.8% married, 16.8% cohabitating, 5.2% divorced, and 0.4% widowed).
In terms of drinking behaviors, on average, participants reported consuming an average of 3.57 (SD = 2.28) drinks per drinking occasion and consumed alcohol approximately twice per week (M = 2.11, SD = 2.66). Participants reported consuming an average of 8.77 (SD = 14.65) drinks per week. Further, the sample was categorized by a relatively low number of alcohol-related problems (M =12. 23, SD = 17.46) as indicated on the Drinker’s Inventory of Consequences.
Measures.
Approach and Avoidance of Alcohol Questionnaire (AAAQ; McEvoy et al., 2004).
Approach and avoidance inclinations were assessed using the 14-item AAAQ. Participants responded to AAAQ items based on their attitudes toward alcohol over the last week. Answers ranged from Not at All (0) to Very Strongly (8). Approach inclinations include statements such as “I would like to have a drink or two” and “I am planning to drink alcohol.” Avoidance inclinations include statements such as “I am avoiding people who are likely to offer me a drink” and “I am deliberately occupying myself so I will not drink alcohol”.
Drinking History.
Alcohol use was assessed using the 10-item Drinking History Questionnaire (DHQ) based on the work of Cahalan, Cisin, and Crossley (1969). This questionnaire assesses a variety of drinking behaviors, such as length of time drinking at present rate, frequency of getting “somewhat intoxicated” and getting drunk, number of drinks it takes to get “somewhat intoxicated” and to get drunk, and preference for alcohol type. Frequency and quantity of alcohol use is also assessed. Frequency is assessed using a 10-point scale ranging from once a month or less to 21 or more times a week. Quantity is the number of standard drinks they typically consume per drinking occasion. The current study utilized frequency and quantity estimates from the DHQ to establish relationships to AAAQ subscales.
Drinker’s Inventory of Consequences (DrInC; Miller, Tonigan, & Longabaugh, 1995).
Alcohol-related consequences were assessed using the DrInC. Five different domains of problems are assessed including interpersonal (e.g., When drinking, I have said harsh or cruel things to someone), physical (e.g., I have been sick and vomited after drinking), social (e.g., The quality of my work has suffered because of my drinking), impulsive (e.g., I have taken foolish risks when I have been drinking), and intrapersonal consequences (e.g., I have felt guilty or ashamed because of my drinking). Participants are asked to respond to each item with how frequently the consequence has happened to them in the past 3 months with 0 (Never), 1 (Once or a few times), 2 (Once or twice a week), or 3 (Daily or almost daily).
Procedures.
Potential participants were recruited from Amazon Mechanical Turk (MTurk) as part of a larger study examining alcohol-related attitudes. Individuals were presented with a description of the study procedures and provided electronic informed consent if they volunteered to participate. Participants were then taken to the online survey, which in addition to the measures above, included measures of personality and other drinking related behaviors, and took approximately 45 minutes to complete. Participants were compensated $2.00 for their time.
Analytic Plan
Confirmatory factor analysis was conducted in Mplus 7.31 (Muthén & Muthén, 2007) using maximum likelihood with robust standard errors. For the three-factor solution, the items were specified to load onto their respective factor (Inclined/Indulgent, Obsessed/Compelled, or Resolved/Regulated). For the two-factor solution, the Inclined/Indulgent and Obsessed/Compelled items were specified to load onto a single approach scale. The variance of each latent factor was fixed to 1 for the model to be identified. Item distributions and correlations between items and factors were examined. We used multiple fit indices to examine model fit, including chi-square (χ2), comparative fit index (CFI), Tucker-Lewis index (TLI), standardized root mean residuals (SRMR), and the root mean square error of approximation (RMSEA). A non-significant chi-square represents a good fitting model. Importantly, the chi-square test is sensitive to large sample sizes, and as such is not typically a reliable estimate of model fit alone (Hooper, Coughlan, & R. Mullen, 2007). CFI and TFLI values ≥ .90 indicate adequate fit with values and ≥ .95 demonstrating excellent fit. SRMR values < .08 are preferred. Lastly, RMSEA values <.06 are preferred. After fitting a two-factor and three-factor model, we compared fit between models using a chi-square difference test.
We assessed composite reliability as well as Cronbach’s alpha of the AAAQ subscales to further establish the reliability of the measure. Unlike Cronbach’s alpha, calculating composite reliability has the advantage of not assuming equal loadings. Invariance testing was conducted using multiple group CFA in Mplus to look for configural, metric, and scalar invariance. Configural invariance means the same items load onto the same number of factors but the parameter estimates are free to vary across groups, metric invariance means factor loadings are constrained to be equal across groups, and scalar invariance means the intercepts are constrained to be equal across groups.
Lastly, multiple linear regressions were used to establish the concurrent validity of the AAAQ subscales. Specifically, these scales were examined in relation to drinking frequency, drinking quantity, drinks per week, and alcohol-related problems for the total sample and by gender.
Results
Confirmatory Factor Analysis
First, the three-factor model was examined. Overall, the results of this analysis indicate an adequate fitting model. The chi-square for the model was significant, X2 (74, N = 537) = 340.71, p < .01. The SRMR was .07, below the preferred cutoff of .08. The TLI was .89, just below the cut off for adequate fit. The CFI was .92, demonstrating good fit. The RMSEA was .08, 95% CI (.08, .09), just above the preferred value of .06. Together, results suggested that the three-factor model fit the data adequately.
Next, we examined a two-factor model (i.e., approach subscales combined). Results indicated a poor fitting model. Specifically, the chi-square for the model was significant X2 (76, N = 537) = 1009.04, p < .01), SRMR was .16, TLI and CFI were .70 and .64, respectively, and the RMSEA was .15. Finally, a chi-square difference test indicated that the three-factor model significantly fit the data better than a two-factor model (ΔX2 = 668.33, p = <.001). See Table 1. for a summary of the two-factor and three-factor results. See Figure 1 for an illustration of the final three-factor model including factor loadings, residuals, and inter-factor correlations. The correlations, standard deviations and correlations between items for the 14-item scale are presented in Table 2.
Table 1.
Results of confirmatory factor analysis of AAAQ in a community sample (N = 537)
| Model | X2 | df | p | SRMR | TLI | CFI | RMSEA |
|---|---|---|---|---|---|---|---|
| Two-Factor | 1009.04 | 76 | < .001 | .16 | .64 | .70 | .15 |
| Three-Factor | 340.71 | 74 | < .001 | .07 | .89 | .91 | .08 |
Note: df = Degrees of freedom, SRMR = Standardized root mean residual, TLI = Tucker-Lewis index, CFI = Comparative fit index, RMSEA = Root mean square error of approximations.
Figure 1.
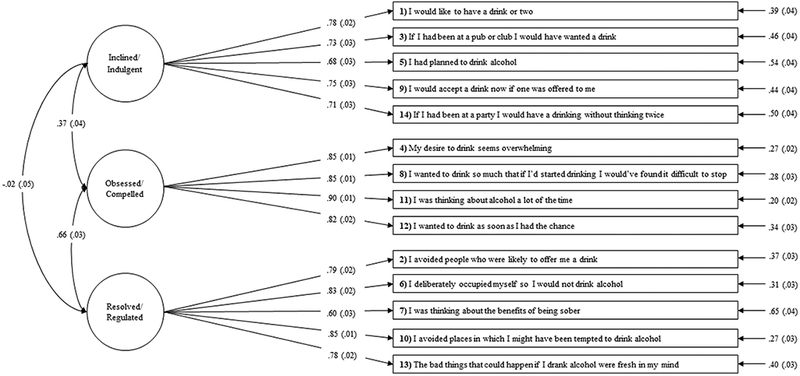
Factor structure of the AAAQ. Circles represent latent factors, rectangles represent observed variables. Factor loadings are associated with single-headed arrows from latent factors to observed variables. The error variance associated with each observed variable is indicated by single-headed arrows pointing to observed variables. Correlations are shown with double-headed arrows between the latent factors. Standardized values are shown.
Table 2.
Means, Standard Deviations and Correlations of Items in AAAQ (N = 537)
| Item number |
M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 5.91 | 2.47 | - | |||||||||||||
| 2 | 2.12 | 2.00 | .01 | - | ||||||||||||
| 3 | 6.45 | 2.40 | .61 | −.09 | - | |||||||||||
| 4 | 2.49 | 2.19 | .29 | .44 | .18 | - | ||||||||||
| 5 | 4.82 | 2.81 | .61 | .02 | .44 | .35 | - | |||||||||
| 6 | 2.13 | 1.94 | .12 | .67 | −.00 | .48 | .07 | - | ||||||||
| 7 | 3.71 | 2.43 | .00 | .44 | .04 | .26 | −.03 | .51 | - | |||||||
| 8 | 2.34 | 2.19 | .23 | .50 | .14 | .76 | .27 | .56 | .31 | - | ||||||
| 9 | 6.48 | 2.39 | .54 | −.18 | .55 | .14 | .46 | −.07 | −.07 | .08 | - | |||||
| 10 | 2.21 | 2.10 | .09 | .71 | .03 | .45 | .06 | .71 | .48 | .52 | −.09 | - | ||||
| 11 | 2.53 | 2.18 | .32 | .42 | .17 | .77 | .39 | .50 | .30 | .74 | .17 | .48 | - | |||
| 12 | 3.01 | 2.48 | .42 | .35 | .28 | .66 | .48 | .43 | .22 | .67 | .27 | .41 | .76 | - | ||
| 13 | 2.61 | 2.32 | .10 | .56 | .00 | .48 | .08 | .62 | .56 | .51 | −.10 | .67 | .55 | .46 | - | |
| 14 | 6.27 | 2.61 | .48 | −.15 | .55 | .12 | .12 | −.06 | −.11 | .09 | .64 | −.03 | .13 | .29 | −.06 | - |
Note. Items were scaled from 0 (Not at All) to 8 (Very Strongly).
Reliability
We calculated the composite reliability of each of the AAAQ subscales using factor loadings. Inclined/Indulgent, Obsessed/Compelled, and Resolved/Regulated all demonstrated high composite reliability (.85, .91, and .88, respectively). Interestingly, these values did not differ from Cronbach’s alpha (.85, .91, and .87, respectively), suggesting the assumption of equal loadings was not violated.
Invariance Testing
As a preliminary step in examining gender invariance in the three-factor model for AAAQ responses in our community sample we performed a separate confirmatory factor analysis for males and females. See Table 3 for model fit indices by gender and Table 4 for standardized factor loadings by gender. Although the model fit for males was slightly better than the model fit for females, overall the model fit was acceptable for both genders.
Table 3.
Goodness of fit indexes for the baseline model by gender (males: n= 286, females: n =251)
| Group | X2 | df | p | SRMR | TLI | CFI | RMSEA |
|---|---|---|---|---|---|---|---|
| Male | 229.25 | 74 | < .001 | .08 | .90 | .92 | .09 |
| Female | 204.15 | 74 | < .001 | .07 | .87 | .90 | .08 |
Note: df = Degrees of freedom, SRMR = Standardized root mean residual, TLI = Tucker-Lewis index, CFI = Comparative fit index, RMSEA = Root mean square error of approximations.
Table 4.
Standardized factor loadings by gender (n = 537)
| Male | Female | |||
|---|---|---|---|---|
| Factor/Item | Estimate | S.E. | Estimate | S.E. |
| Inclined-Indulgent | ||||
| AAAQ1. I would like to have a drink or two | .82 | .03 | .73 | .04 |
| AAAQ3. If I had been at a pub or club I would have wanted a drink. | .79 | .03 | .68 | .04 |
| AAAQ5. I had planned to drink alcohol. | .71 | .04 | .63 | .05 |
| AAAQ9. I would have accepted a drink if one had been offered to me. | .74 | .03 | .76 | .04 |
| AAAQ14. If I had been at a party I would have a drink without thinking twice. | .72 | .04 | .70 | .04 |
| Obsessed-Compelled | ||||
| AAAQ4. My desire to drink seemed overwhelming. | .88 | .02 | .80 | .03 |
| AAAQ8. I wanted to drink alcohol so much that if I had started drinking I would have found it difficult to stop. | .85 | .02 | .82 | .02 |
| AAAQ11. I was thinking about alcohol a lot of the time. | .89 | .02 | .91 | .02 |
| AAAQ12. I wanted to drink as soon as I had the chance. | .79 | .03 | .83 | .02 |
| Resolved-Regulated | ||||
| AAAQ2. I avoided people who were likely to offer me a drink. | .87 | .02 | .69 | .04 |
| AAAQ6. I deliberately occupied myself so I would not drink alcohol. | .83 | .02 | .80 | .03 |
| AAAQ7. I was thinking about the benefits of being sober. | .57 | .04 | .62 | .04 |
| AAAQ10. I avoided places in which I might have been tempted to drink alcohol. | .89 | .02 | .83 | .03 |
| AAAQ13. The bad things that could happen if I drank alcohol are fresh in my mind. | .75 | .03 | .80 | .03 |
Note: S.E. = Standard Error. Males: n = 286; females: n = 251.
To further investigate gender invariance in our three-factor model of AAAQ results we conducted a multiple group CFA to analyze configural, metric, and scalar invariance between males and females. See Table 5 for the results. As with previous models the chi-square for the configural model was significant, however, the CFI, TLI, RMSEA, and SRMR all suggested an acceptably fitting model. Comparing the metric model with the configural model did not result in a significant chi-square increase (ΔX2 = 17.601, p = .09) indicating that constraining factor loadings to be equal for males and females resulted did not result in worse model fit. Further, comparing the scalar model with the metric model also did not result in a significant chi-square increase (ΔX2 = 19.71, p = .05), suggesting that constraining the intercepts to be equal for males and females did not result in a worse fit. In sum, males and females have the same items loading onto the same factors, and have equivalent factor loadings and intercepts.
Table 5.
Invariance tests for the approach and avoidance of alcohol questionnaire by gender
| Model | X2 | df | Model Comp. |
Δ X2 | Δdf | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|---|---|---|---|
| 1. Configural | 413.74 | 148 | .91 | .89 | .09 | .07 | |||
| 2. Metric | 447.70 | 159 | 2 vs.1 | 17.60 | 11 | .91 | .89 | .08 | .08 |
| 3. Scalar | 469.05 | 170 | 3 vs .2 | 19.71 | 11 | .90 | .90 | .08 | .08 |
Note: df = Degrees of freedom, SRMR = Standardized root mean residual, TLI = Tucker-Lewis index, CFI = Comparative fit index, RMSEA = Root mean square error of approximations. Δ X2 = change in X2. Δdf = change in df. Males: n = 286; females: n = 251.
Concurrent Validity
Results of the regression analyses are summarized in Table 6. The AAAQ subscales accounted for 16%, 12%, 18% and 53% of the variance of frequency, quantity, drinks per week, and alcohol-related consequences, respectively. All three subscales were significantly predictive of frequency, drinks per week and alcohol-related consequences. For quantity, only Inclined/ Indulgent and Obsessed/Compelled were significant. Obsessed/Compelled was the strongest predictor for frequency, drinks per week, and alcohol-related consequences. Resolved/Regulated demonstrated expected relationships with these variables in that it was negatively associated with frequency of drinking, drinks per week and alcohol-related consequences.
Table 6.
Results of multiple linear regression analyses for AAAQ subscales
| R2 | B | SE B | 95% CI | B | |
|---|---|---|---|---|---|
| Overall Sample | |||||
| Frequency | 0.16 | ||||
| Inclined/Indulgent | 0.23 | 0.06 | 0.11, 0.34 | 0.17*** | |
| Obsessed/Compelled | 0.46 | 0.07 | 0.32, 0.60 | 0.35*** | |
| Resolved Regulated | −0.15 | 0.08 | −0.30, 0.00 | −0.10* | |
| Quantity | 0.12 | ||||
| Inclined/Indulgent | 0.26 | 0.05 | 0.16, 0.36 | 0.23*** | |
| Obsessed/Compelled | 0.24 | 0.06 | 0.12, 0.36 | 0.21*** | |
| Resolved Regulated | −0.04 | 0.07 | −0.17, 0.09 | −0.03 | |
| Drinks per week | 0.18 | ||||
| Inclined/Indulgent | 1.10 | 0.32 | 0.47, 1.73 | 0.15*** | |
| Obsessed/Compelled | 2.91 | 0.10 | 2.14, 3.68 | 0.40*** | |
| Resolved Regulated | −1.09 | 0.41 | −1.90, −0.28 | −0.13** | |
| Consequences | 0.53 | ||||
| Inclined/Indulgent | 0.24 | 0.29 | −0.36, 0.81 | 0.10** | |
| Obsessed/Compelled | 5.03 | 0.36 | 4.33, 5.72 | 0.58*** | |
| Resolved Regulated | 1.99 | 0.37 | 1.26, 2.71 | 0.18*** | |
| Males | |||||
| Frequency | 0.18 | ||||
| Inclined/Indulgent | 0.04 | 0.03 | −1.15, 1.29 | 0.13* | |
| Obsessed/Compelled | 0.16 | 0.03 | 0.08, 0.19 | 0.39*** | |
| Resolved Regulated | −0.03 | 0.02 | −0.08, 0.10 | −0.11 | |
| Quantity | 0.11 | ||||
| Inclined/Indulgent | 0.05 | 0.02 | 0.02, 3.22 | 0.20** | |
| Obsessed/Compelled | 0.06 | 0.02 | 0.02, 0.11 | 0.23** | |
| Resolved Regulated | −0.04 | 0.02 | −0.07, 0.00 | −0.14 | |
| Drinks per week | 0.26 | ||||
| Inclined/Indulgent | 0.20 | 0.09 | 0.02, 0.37 | 0.13* | |
| Obsessed/Compelled | 0.90 | 0.12 | 066, 1.14 | 0.52*** | |
| Resolved Regulated | −0.36 | 0.10 | −0.57, −0.16 | −0.23** | |
| Consequences | 0.56 | ||||
| Inclined/Indulgent | 0.12 | 0.10 | −0.08, 0.31 | 0.05 | |
| Obsessed/Compelled | 1.43 | 0.14 | 1.16, 1.69 | 0.57*** | |
| Resolved Regulated | 0.54 | 0.12 | 0.32, 0.77 | 0.24*** | |
| Females | |||||
| Frequency | 0.12 | ||||
| Inclined/Indulgent | 0.13 | 0.46 | −0.78, 1.04 | 0.22** | |
| Obsessed/Compelled | 0.08 | 0.03 | 0.02, 0.08 | 0.24** | |
| Resolved Regulated | −0.02 | 0.02 | −0.07, 0.02 | −0.09 | |
| Quantity | 0.14 | ||||
| Inclined/Indulgent | 0.05 | 0.01 | 0.03, 0.08 | 0.25*** | |
| Obsessed/Compelled | 0.04 | 0.02 | 0.00, 0.09 | 0.15 | |
| Resolved Regulated | 0.03 | 0.02 | −0.01, 0.06 | 0.11 | |
| Drinks per week | 0.09 | ||||
| Inclined/Indulgent | 0.02 | 0.09 | 0.05, 0.42 | 0.16* | |
| Obsessed/Compelled | 0.45 | 0.17 | 0.12, 0.77 | 0.22** | |
| Resolved Regulated | −0.01 | 0.13 | −0.27, 0.25 | 0.000 | |
| Consequences | 0.47 | ||||
| Inclined/Indulgent | 0.25 | 0.07 | 0.11, 0.38 | 0.18*** | |
| Obsessed/Compelled | 1.12 | 0.12 | 0.88, 1.36 | 0.58*** | |
| Resolved Regulated | 0.10 | 0.10 | −0.09, 0.29 | 0.06 | |
Note: * p < .05, ** p < .01, *** p < .001
Discussion
This study examined the psychometric properties of the AAAQ in a community sample. Although the AAAQ has demonstrated different factor structures in clinical and student populations, the factor structure in community populations had yet to be examined. Thus, the main purpose of the current study was to evaluate the factor structure of the AAAQ in a community sample comparing the three-factor model (Resolved/Regulated, Inclined/Indulgent, and Obsessed/Compelled) observed in non-clinical student samples (McEvoy et al., 2004) to that of a the two-factor model (avoidance, approach) observed in clinical samples (Klein et al., 2007; Schlauch et al., 2013). Results from confirmatory factor analysis supported a three-factor structure of the AAAQ in community samples over the two-factor structure. Additionally, findings indicated that the three-factor AAAQ was invariant across gender. Specifically, multiple group confirmatory factor analyses was conducted to assess configural, metric and scalar invariance, with findings suggesting the AAAQ was invariant across males and females, with adequate fit among both genders.
The three subscales of the AAAQ also demonstrated high internal consistency and demonstrated high composite reliability. Further, we examined the associations of the subscales with drinking behaviors, as measured by quantity and frequency of drinking and alcohol-related problems. The subscales were significantly associated with frequency, quantity, drinks per week, and alcohol-related consequences, suggesting that all three subscales contribute significantly to drinking related outcomes. Of particular note, and consistent with the three factor model of the AAAQ, the Obsessed/Compelled was more strongly associated with frequency of drinking, drinks per week, and alcohol-related consequences than Inclined/Indulgent. Further, the correlation between Obsessed/Compelled and Inclined/Indulgent was significant, but only moderate (.37). Additionally, as expected, the Resolved/Regulated subscale (i.e., avoidance) was incrementally and negatively associated with frequency of use and total drinks per week, and positively associated with alcohol-related consequences (i.e., avoidance inclinations are posited to develop as a result of negative consequences of use).
Taken together results of the current study have both methodological and clinical/theoretical implications for the study of alcohol craving. First, this study offers furthering support for the need to assess both the desire to use (i.e., traditional craving) and the desire to avoid using alcohol. In the current study avoidance inclinations (Resolved/Regulated subscale) were significantly related to frequency, drinks per week and consequences while controlling for approach items, suggesting it contributes to the explanation of drinking outcomes. Further, while avoidance was negatively associated with frequency and drinks per week, it was positively associated with consequences, supporting the idea that problematic use may best be explained by the simultaneous desire to use and not to use. Indeed, avoidance inclinations are primarily thought to develop as a result of the negative consequences of use (e.g., Breiner et al., 1999).
Additionally, the Obsessed/Compelled subscale was more strongly predictive of drinking behaviors in the community sample, whereas the opposite pattern was seen in college student samples (McEvoy et al., 2004). Although college student samples often have a range of drinking experiences, including problematic use, they generally are beginning drinkers who have yet to establish patterns of problematic use over time seen in older clinical populations. As such, the Inclined/Indulgent scale (i.e., mild approach) may be more reflective of the typical, social drinking that takes place. This points to the possibility that the distinction in the Inclined/Indulgent scale and Obsessed/Compelled scale may reflect the development of riskier drinking over time. In contrast, in a community sample, we saw that the Obsessed/Compelled scale (i.e., intense approach) was more strongly related to drinking behaviors and problems. Overall, the distinction between mild approach and intense craving appears to be useful not only due to their relationship to drinking behavior, but because it may shed light on the developmental process of craving. Longitudinal research would aid in a better understanding of the development of and potential transition from mild to intense cravings as it relates to drinking behavior.
Although the current study provides support for the use of the AAAQ in community samples and continues to highlight the importance of multidimensional assessments of craving, the current study is not without limitations. First, the current study did not directly compare the performance of the AAAQ across different samples. As such, while the measure demonstrated gender invariance in a community sample, we cannot generalize this to a clinical or college student sample. Secondly, while we were able to show that the AAAQ subscales were associated with drinking behaviors, the current student was cross-sectional in nature which inhibits our ability to demonstrate the predictive validity of the AAAQ. Future longitudinal research is needed to establish how the AAAQ predicts drinking behaviors in community samples. Third, participants were recruiting using MTurk, and although widely used, the resulting sample characteristics may not be representative of a true community sample. However, MTurk samples have been found to be significantly more diverse than both college student samples and social media recruited samples in terms of age, geographic, ethnic and economic background (Buhrmester, Kwang, & Gosling, 2011; Casler, Bickel, & Hackett, 2013). Indeed, our sample demonstrates diversity among several important demographic variables, including gender, employment, and age.
In sum, the results of these analyses provide support for the reliability and validity of using the AAAQ to measure approach and avoidance inclinations in community samples. Further, these results demonstrate the different factor structure the AAAQ has depending on the sample in which it is used and the expected drinking behavior. The three-factor structure seems to be best in populations that exhibit a range of drinking. In contrast, the two-factor solution seems best in clinical samples as supported by previous research (e.g., Klein & Anker, 2013; Klein et al., 2007; Schlauch et al., 2012). However, further research is needed to examining the ways in which craving profiles change over the developmental trajectory of problematic alcohol use. Specifically, research of the AAAQ in other samples would further elucidate its varying factor structure, including multi-group comparisons of diverse samples (both clinically and demographically). As a step, this study provides demonstrates support for the three-factor structure of the AAAQ in community samples.
Acknowledgments
The development of this report was supported in part by NIH-NIAAA K23-AA021768 (Schlauch). The content is solely the responsibility of the authors and does not represent the official views of National Institutes of Health.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, D.C.: American Psychiatric Association. [Google Scholar]
- Anton RF (1999). What is craving? Models and implications for treatment. Alcohol Research and Health, 23(3), 165–173. [PMC free article] [PubMed] [Google Scholar]
- Breiner MJ, Stritzke WG, & Lang AR (1999). Approaching avoidance. A step essential to the understanding of craving. Alcohol Research and Health, 23(3), 197–206. [PMC free article] [PubMed] [Google Scholar]
- Buhrmester M, Kwang T, & Gosling SD (2011). Amazon’s Mechanical Turk: A New Source of Inexpensive, Yet High-Quality, Data? Perspectives on Psychological Science, 6(1), 3–5. doi: 10.1177/1745691610393980 [DOI] [PubMed] [Google Scholar]
- Cahalan D, Cisin I, & Crossley H (1969). American drinking practices: A national study of drinking behavior and attitudes . (Monograph No. 6.). New Haven, Connecticut: College & University Press, Rutgers Center of Alcohol Studies. [Google Scholar]
- Casler K, Bickel L, & Hackett E (2013). Separate but equal? A comparison of participants and data gathered via Amazon’s MTurk, social media, and face-to-face behavioral testing. Computers in Human Behavior, 29(6), 2156–2160. doi: 10.1016/j.chb.2013.05.009 [DOI] [Google Scholar]
- Drummond DC (2001). Theories of drug craving, ancient and modern. Addiction, 96(1), 33–46. doi: 10.1080/09652140020016941 [DOI] [PubMed] [Google Scholar]
- Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, … Hasin DS (2015). Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry, 72(8), 757–766. doi: 10.1001/jamapsychiatry.2015.0584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooper D, Coughlan J, & Mullen RM, (2007). Structural Equation Modeling: Guidelines for Determining Model Fit (Vol. 6). [Google Scholar]
- Kavanagh DJ, Statham DJ, Feeney GF, Young RM, May J, Andrade J, & Connor JP (2013). Measurement of alcohol craving. Addictive Behaviors, 38(2), 1572–1584. doi: 10.1016/j.addbeh.2012.08.004 [DOI] [PubMed] [Google Scholar]
- Kessler RC, & Merikangas KR (2004). The National Comorbidity Survey Replication (NCS-R): background and aims. International Journal of Methods in Psychiatric Research, 13(2), 60–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein AA, & Anker JJ (2013). A Psychometric Evaluation of the Approach and Avoidance of Alcohol Questionnaire Among Alcohol-Dependent Patients Attending Residential Treatment. Journal of Psychopathology and Behavioral Assessment, 35(2), 205–214. doi: 10.1007/s10862-012-9322-5 [DOI] [Google Scholar]
- Klein AA, Stasiewicz PR, Koutsky JR, Bradizza CM, & Coffey SF (2007). A Psychometric Evaluation of the Approach and Avoidance of Alcohol Questionnaire (AAAQ) in Alcohol Dependent Outpatients. Journal of Psychopathology and Behavioral Assessment, 29(4), 231–240. doi: 10.1007/s10862-007-9044-2 [DOI] [Google Scholar]
- Kozlowski LT, & Wilkinson DA (1987). Use and Misuse of the Concept of Craving by Alcohol, Tobacco, and Drug Researchers. British Journal of Addiction, 82(1), 31–45. doi: 10.1111/j.1360-0443.1987.tb01430.x [DOI] [PubMed] [Google Scholar]
- Lowman C, Hunt WA, Litten RZ, & Drummond DC (2000). Research perspectives on alcohol craving: an overview. Addiction, 95 Suppl 2, S45–54. [DOI] [PubMed] [Google Scholar]
- McEvoy PM, Stritzke WGK, French DJ, Lang AR, & Ketterman R (2004). Comparison of three models of alcohol craving in young adults: a cross-validation. Addiction, 99(4), 482–497. doi: 10.1111/j.1360-0443.2004.00714.x [DOI] [PubMed] [Google Scholar]
- Miller WR, Tonigan JS, & Longabaugh R (1995). The Drinker Inventory of Consequences (DrInC): An Instrument for Assessing Averse Consequence of Alcohol Abuse Project MATCH Monograph Series: Rockville, MD. [Google Scholar]
- Muthén LK, & Muthén BO (2007). Mplus User’s Guide (Sixth Edition). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Park CL & Grant C (2005). Determinants of positive and negative consequences of alcohol consumption in college students: alcohol use, gender, and psychological characteristics. Addictive Behaviors, 30, 755–765. [DOI] [PubMed] [Google Scholar]
- Pickens RW, & Johanson CE (1992). Craving: consensus of status and agenda for future research. Drug & Alcohol Dependence, 30(2), 127–131. [DOI] [PubMed] [Google Scholar]
- Sayette MA (2016). The Role of Craving in Substance Use Disorders: Theoretical and Methodological Issues. Annual Review of Clinical Psychology, 12(1), 407–433. doi: 10.1146/annurev-clinpsy-021815-093351 [DOI] [PubMed] [Google Scholar]
- Sayette MA, Shiffman S, Tiffany ST, Niaura RS, Martin CS, & Shadel WG (2000). The measurement of drug craving. Addiction, 95 Suppl 2, S189–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlauch RC, Levitt A, Bradizza CM, Stasiewicz PR, Lucke JF, Maisto SA, … Connors GJ (2013). Alcohol craving in patients diagnosed with a severe mental illness and alcohol use disorder: bidirectional relationships between approach and avoidance inclinations and drinking. Journal of Consulting and Clinical Psychology, 81(6), 1087–1099. doi: 10.1037/a0033914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlauch RC, Stasiewicz PR, Bradizza CM, Coffey SF, Gulliver SB, & Gudleski GD (2012). Relationship between approach and avoidance inclinations to use alcohol and treatment outcomes. Addictive Behaviors, 37(7), 824–830. doi: 10.1016/j.addbeh.2012.03.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith-Hoerter K, Stasiewicz PR, & Bradizza CM (2004). Subjective reactions to alcohol cue exposure: a qualitative analysis of patients’ self-reports. Psychology of Addictive Behaviors, 18(4), 402–406. doi: 10.1037/0893-164X.18.4.402 [DOI] [PubMed] [Google Scholar]
- Stritzke WG, McEvoy PM, Wheat LR, Dyer KR, & French DJ (2007). The yin and yang of indulgence and restraint: The ambivalence model of craving In O’Neal PW (Ed.), Motivation of health behavior (pp. 31–47). New York: Nova Science Publishers. [Google Scholar]
- World Health Organization. (2015). ICD-10 Version: 2016. Geneva: World Health Organization. [Google Scholar]