

Abstract
Background:
There are few estimates of vaccination-averted influenza-associated illnesses in China.
Methods:
We used a mathematical model and Monte Carlo algorithm to estimate numbers and 95% confidence intervals (CI) of influenza-associated outcomes (hospitalization, illness, and medically-attended (MA) illness) averted by vaccination among children aged 6–59 months in Suzhou from October 2011–September 2016. Influenza illnesses included non-hospitalized MA influenza illnesses and non-MA influenza illnesses. The numbers of influenza-associated outcomes averted by vaccination were the difference between the expected burden if there were no vaccination given and the observed burden with vaccination. The model incorporated the disease burden estimated based on surveillance data from Suzhou University Affiliated Children’s Hospital (SCH) and data from health utilization surveys conducted in the catchment area of SCH, age-specific estimates of influenza vaccination coverage in Suzhou from the Expanded Program on Immunization database, and influenza vaccine effectiveness estimates from previous publications. Averted influenza estimations were presented as absolute numbers and in terms of the prevented fraction (PF). A hypothetical scenario with 50% coverage (but identical vaccine effectiveness) over the study period was also modeled.
Results:
In ~250,000 children, influenza vaccination prevented an estimated 731 (CI: 549–960) influenza hospitalizations (PF: 6.2% of expected, CI: 5.8–6.6%) and 10,024 (7593–12,937) influenza illnesses (PF:6.5%, 6.4–6.7%), of which 8342 (6338–10,768) were MA (PF: 6.6%, 6.4–6.7%) from 2011 to 2016. The PFs declined each year along with decreasing influenza vaccination coverage. If 50% of the study population had been vaccinated over time, the estimated numbers of averted cases during the study period would have been 4059 (3120–5762) influenza hospitalizations (PF: 27.2%, 26.4–27.9%) and 56,215 (42,925–78,849) influenza illnesses (PF: 28.5%, 28.3–28.7%), of which 46,596 (35,662–65,234) would be MA (PF: 28.5%, 28.3–28.7%).
Conclusion:
Influenza vaccination is estimated to have averted influenza-associated illness outcomes even with low coverage in children aged 6–59 months in Suzhou. Increasing influenza vaccination coverage in this population could further reduce illnesses and hospitalizations.
Keywords: Influenza vaccination, Children, Averted outcomes, Hospitalization, Influenza illness, Medically attended
1. Introduction
Seasonal influenza causes an estimated 3–5 million severe illnesses and 290,000–650,000 deaths annually worldwide [1,2]. Young children, especially those <2 years, are at an increased risk of requiring outpatient and inpatient medical care due to influenza virus infection [3]. Studies conducted in Suzhou found that among children <5 years, influenza virus was detected in 17% of influenza-like illness (ILI) in 2011–2014 [4] and 16–19% of severe acute respiratory infections (SARI) in 2011–2016 [5]. Other studies from China have found annual influenza outpatient visit rates ranging from 15 to 21 per 100 children <5 years during 2011–2014 [6] and influenza hospitalization rates ranging from 20 to 23 per 1000 children <5 years during 2010–2012 [7]. Children infected with influenza can also spread the virus to their household contacts and peers in schools and daycare centers [8].
Annual influenza vaccination is the most effective way to prevent influenza [9]. Although the World Health Organization (WHO) and Chinese Center for Disease Control and Prevention (China CDC) recommend that children aged 6–59 months receive an annual seasonal influenza vaccination [9,10], vaccination coverage among children in China is sub-optimal. Studies evaluating influenza vaccination in children aged 6 months–7 years in China have found coverage estimates ranging from 12 to 32% during 2009–2016 [11,12]. Currently, seasonal influenza vaccine is a non-immunization program vaccine in China, which means it is not covered by the National Immunization Program and cost of vaccination is paid out-of-pocket [13].
Modeling has been used to evaluate the impact of influenza vaccination on averted influenza-associated illnesses. For example, one study showed that influenza vaccination was estimated to prevent an approximate annual average 7700–100,000 influenza hospitalizations, and 1.1–7.5 million influenza illnesses from 2005/06–2018/19 influenza seasons in the United States (U.S.) [14,15]. However, there are limited data to quantify the number of influenza-associated illnesses averted as a result of vaccination in China [16]. Addressing this knowledge gap could be beneficial for developing evidence to inform influenza vaccination policy in China. The objective of this study was to estimate the effect of influenza vaccination in averting influenza-associated hospitalizations, illnesses, and medically-attended (MA) illnesses from October 2011–September 2016 in children aged 6–59 months in Suzhou.
2. Methods
2.1. Study site and population
Suzhou is a major city located in eastern China with a population of approximately 10.7 million residents, of whom about 65% are registered residents, and a Gross Domestic Product (GDP) per capita up to 24,000 U.S. dollars in 2017 [17].
Suzhou University Affiliated Children’s Hospital (SCH) is a 1400-bed hospital that has an estimated 1.5 million outpatient and 42,000 inpatient visits annually [18]. SCH is the only tertiary hospital for children in Suzhou. We defined five municipal districts (Gusu, Wuzhong, Huqiu, Xiangcheng, Gongyeyuan) of Suzhou as SCH’s catchment area. From 1 October 2011–30 September 2016, we conducted year-round ILI and SARI surveillance among children in the outpatient clinics and the respiratory inpatient wards. We defined an influenza season as 1 October in one year to 30 September in the following year.
2.2. Outcome definitions
Three influenza-associated outcomes were included to estimate the impact of influenza vaccination in this study: hospitalization, illness, and MA illness. Influenza hospitalizations were defined as laboratory-confirmed influenza cases identified through SARI (hospitalized individual with ILI symptoms) surveillance. Influenza illnesses were defined as laboratory-confirmed influenza cases in any non-hospitalized individual with ILI symptoms (axillary temperature ≥38°C with fever and cough or sore throat/inflamed or red pharynx in the preceding 7 days), including MA influenza illnesses and individuals who did not seek medical care. MA influenza illnesses, a subset of all influenza illnesses, were defined as cases with laboratory-confirmed influenza cases with ILI who sought medical care in the outpatient department or emergency room.
2.3. Data sources
2.3.1. Rates of influenza hospitalizations, influenza illnesses, and MA influenza illnesses
Methods for estimating influenza burden among children <5 years in Suzhou using enhanced SARI and ILI surveillance at SCH and health utilization surveys (HUS) in SCH’s catchment area have been previously described [5,6]. In brief, we reviewed the residence records for enrolled SCH patients. For hospitalizations, this included records from 2011 to 2013, and for outpatient visits, this included records from 2011 to 2014. We found 67% of SARI cases and 85% of ILI cases who sought care at SCH resided in five municipal districts, which we defined as SCH’s catchment area. We then conducted HUS within this catchment area. In brief, we conducted 7 random telephone survey among community children <5 years within the catchment area from 2011 to 2014 [19] to understand whether and where they seek care after getting influenza-like illness. We further identified the proportion of SARI and ILI patients who sought care at SCH.
We extrapolated the total number of influenza hospitalizations and MA influenza illnesses in the catchment area based on the number of cases we observed in SCH and then calculated the population incidence of influenza hospitalization and MA influenza illness using the proportion of care seeking at SCH (67.7% of SARI cases and 43.6% of ILI) and the positive rates of laboratory-confirmed influenza test results. Suzhou Center for Disease Control and Prevention tested the respiratory samples from the ILI and SARI cases by using real time reverse-transcription polymerase chain reaction (RT-PCR) for influenza virus [20,21]. We divided the study population into three age groups: 6–23 months, 24–35 months and 36–59 months (m).
In addition, we used HUS results to determine the proportion of ILI that was medically attended at any health facility within the catchment area (86.0%, 79.5% and 81.6% for children aged 6–23 m, 24–35 m and 36–59 m respectively). We then calculated influenza illnesses as the number of MA influenza illnesses divided by the proportion of those seeking care at any health facility.
2.3.2. Influenza vaccination coverage and population size
We defined the vaccination coverage (VC) for influenza as the incident proportion of the starting population vaccinated during the month. Monthly VC estimates by age group and the age specific population size were both obtained from the Suzhou Expanded Program on Immunization (EPI) information system. The Suzhou EPI information system has complete electronic vaccination records for >99% of all children living in Suzhou, including non-permanent and permanent residents.
2.3.3. Influenza vaccine effectiveness (VE)
For 2011/12 influenza season, we used VE calculated in our previously published hospital-based test-negative case-control study conducted in Suzhou [22]. For the 2012/13 to 2014/15 influenza seasons, we used VE data from Guangzhou [23,24], since data from Suzhou were unavailable. For 2015/16 influenza season, we used VE from a Suzhou community-based quasi-experimental influenza vaccination evaluation study [25]. If age group specific VE estimates were unavailable from the literature, we assumed the VE estimation for that age group was equivalent to the reported VE for an age group that was inclusive of the population (Supplemental Table 1).
2.4. Averted outcome estimation model
We used the data described above to estimate the direct effect of influenza vaccination on the averted number of influenza-associated hospitalizations, illnesses, and MA illnesses using a month time-scale applying the method 2 model from Tokars et al. [26]. In general, we calculated the number of averted outcomes as the difference between the expected burden if there were no vaccination given and the observed burden with vaccination [14].
We started the model with the total population of children aged 6–59 months of Suzhou, who were unvaccinated and susceptible to influenza. Among the susceptible population during each month, we estimated how many became observed cases of the target influenza-associated hospitalizations, illnesses and MA illnesses for each age group using the surveillance and population data described above, how many were effectively vaccinated using vaccination coverage and effectiveness data described above, and how many remained susceptible to infection.
Each month we estimated the rates of each outcome in each age group by dividing the monthly number of cases in each outcome by the prior month’s susceptible population. Using these rates among the susceptible population, we estimated the expected number of outcomes that would have occurred in the same population in the absence of vaccination. To estimate the health outcomes averted by influenza vaccination, we calculated the difference between the expected number of outcomes without vaccination and the observed number of outcomes with vaccination.
Finally, as a hypothetical scenario to model the effect of increased vaccination coverage, we used the methods described above to estimate the number of cases that would have been averted with 50% coverage (but identical vaccine effectiveness) among children aged 6–59 months in Suzhou.
2.5. Estimating the prevented fraction (PF)
Although the number of averted influenza-associated hospitalizations, illnesses and MA illnesses each season depends on that season’s vaccination coverage and vaccine effectiveness, it is also influenced by the influenza attack rate, which means that seasons with high attack rates will result in a higher number of averted outcomes assuming the same vaccination coverage and effectiveness. Therefore, averted influenza estimations were presented as absolute numbers and in terms of the PF. The prevented fraction was calculated as the proportion of averted outcomes out of the expected outcomes in the absence of vaccination.
We used a Monte Carlo method [27] with 5000 simulations to estimate the number of averted outcomes and 95% confidence intervals (CIs). We assumed normal distribution for vaccine effectiveness of each age group. VE was truncated at 0 if the lower limit of 95% CI was <0. We assumed Poisson distribution for the monthly count of reported hospitalizations, illnesses, MA illnesses for each age group. Population of children aged 6–59 m in Suzhou and vaccine coverage estimate considered constant. Considering that the VE in 2012/13–2014/15 influenza seasons used in this study came from other cities in China, we also performed a sensitivity analysis where VE was assumed to be 10% lower and 10% greater in each season to reflect the uncertainty of the estimated numbers. Data analysis was performed using R version 3.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
This study was approved by the Institutional Review Board (IRB) of the School of Public Health, Fudan University, and received a non-engaged determination from the U.S. Centers for Disease Control and Prevention (CDC).
3. Results
3.1. Observed numbers of three influenza-associated outcomes
During the study period, 11,065(CI: 10,859–11,269) influenza hospitalizations, 143,585(CI: 142,864–144,321) influenza illnesses, and 118,888(CI: 118,228–119,571) MA influenza illnesses were observed among children aged 6–59 months in Suzhou (Table 1).
Table 1.
The estimated number of influenza hospitalizations, illnesses, and medically-attended (MA) illnesses in children aged 6–59 months in Suzhou, China, by age and influenza season, 2011/12–2015/16.
| Average population size (N = 254,852) | Influenza hospitalization (N = 11,065) | Influenza illness (N = 143,585) | MA influenza illness (N = 118,888) | ||
|---|---|---|---|---|---|
| Age (month) | 6–23 | 89,011 | 5147 (5008, 5287) | 54,116 (53,663, 54,566) | 46,542 (46,115, 46,967) |
| 24–35 | 57,922 | 2064 (1975, 2154) | 31,505 (31,159, 31,845) | 25,053 (24,746, 25,358) | |
| 36–59 | 107,918 | 3852 (3739, 3973) | 57,963 (57,493, 58,434) | 47,298 (46,896, 47,717) | |
| Influenza season | 2011/12 | 197,913 | 4162 (4039, 4289) | 62,006 (61,519, 62,483) | 51,398 (50,958, 51,831) |
| 2012/13 | 236,342 | 1193 (1124, 1260) | 8293 (8112, 8478) | 6927 (6760, 7094) | |
| 2013/14 | 260,054 | 2657 (2558, 2757) | 38,815 (38,435, 39,191) | 32,118 (31,779, 32,475) | |
| 2014/15 | 283,656 | 1366 (1292, 1442) | 14,824 (14,579, 15,067) | 12,242 (12,022, 12,459) | |
| 2015/16 | 296,295 | 1687 (1607, 1767) | 19,649 (19,379, 19,917) | 16,206 (15,953, 16,458) |
Data are n (95% confidence interval), unless otherwise as indicated.
3.2. Influenza vaccination coverage and effectiveness
From the 2011/12–2015/16 influenza seasons, vaccination coverage declined from a high of 20.0% to 5.7%; the average coverage was 9.3% (Fig. 1). In the earlier study seasons, children aged 6–23 months had the highest influenza vaccination coverage, at22.8% in 2011/12, 14.9% in 2012/13 and 7.1% in 2013/14. In later years, children aged 36–59 months had the highest influenza vaccination coverage of all the age groups, at 7.5% in the 2014/15 season and 7.3% in the 2015/16 season (Fig. 1). VE estimates used in this study varied over the influenza seasons and differed by age group (Supplementary Table 1).
Fig. 1.
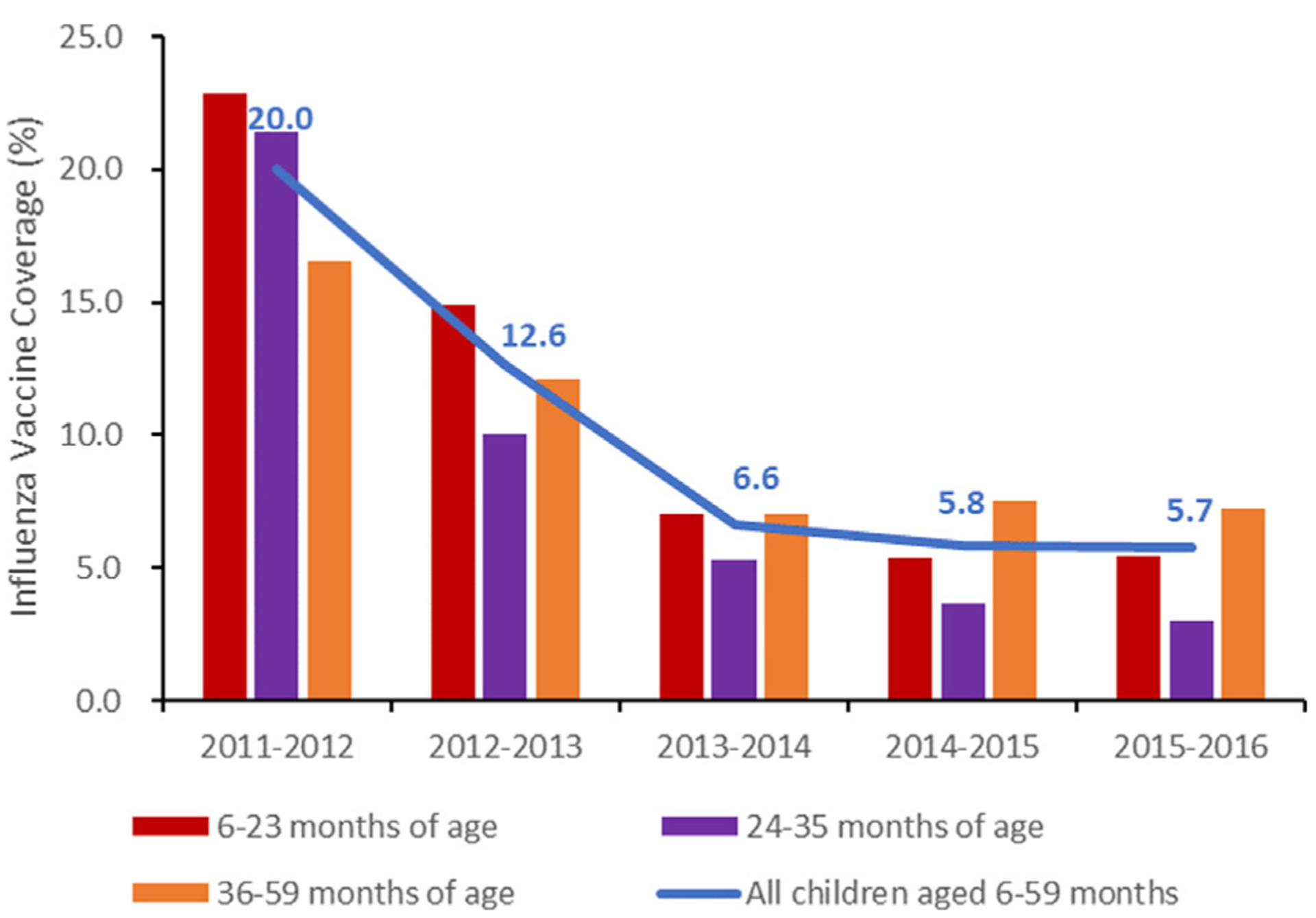
Influenza vaccine coverage of children aged 6–59 months in Suzhou, 2011/12–2015/16 influenza seasons (%).
3.3. Cases averted with existing vaccination coverage
From 2011 to 2016, influenza vaccination prevented an estimated 731 (CI: 549–960) influenza hospitalizations (PF: 6.2% of expected, CI: 5.8–6.6%) and 10,024 (7593–12,937) influenza illnesses (PF: 6.5%, 6.4–6.7%), of which 8342 (6338–10,768) were MA (PF: 6.6%, 6.4–6.7%) (Table 2).
Table 2.
The estimated number of influenza-associated outcomes among children aged 6–59 months averted by the current influenza vaccination program in Suzhou, China, 2011/12–2015/16 influenza seasons.
| Influenza hospitalization | MA influenza illness | Influenza illness | |||||
|---|---|---|---|---|---|---|---|
| N (95% CI) | PF (%) (95% CI) | N (95% CI) | PF (%) (95% CI) | N (95% CI) | PF (%) (95% CI) | ||
| Age (month) | 6–23 | 367 (272, 477) | 6.7 (6.0, 7.3) | 4827 (3444, 6365) | 8.2 (8.0, 8.4) | 4149 (2970, 5471) | 8.2 (7.9, 8.4) |
| 24–35 | 158 (113, 214) | 7.1 (6.1, 8.2) | 2529 (1763, 3432) | 7.4 (7.1, 7.7) | 2011 (1396, 2726) | 7.4 (7.1, 7.7) | |
| 36–59 | 202 (69, 406) | 5.0 (4.3, 5.7) | 2609 (971, 5103) | 4.3 (4.1, 4.5) | 2135 (790, 4159) | 4.3 (4.1, 4.5) | |
| Influenza season | 2011/12 | 538 (361, 763) | 11.5 (10.5, 12.4) | 7931 (5560, 10,824) | 11.3 (11.1, 11.6) | 6604 (4636, 8990) | 11.4 (11.1, 11.7) |
| 2012/13 | 73 (60, 87) | 5.8 (4.5, 7.1) | 530 (429, 639) | 6.0 (5.5, 6.5) | 444 (360, 536) | 6.0 (5.5, 6.6) | |
| 2013/14 | 87 (69, 106) | 3.2 (2.5, 3.8) | 1150 (889, 1407) | 2.9 (2.7, 3.0) | 953 (738, 1163) | 2.9 (2.7, 3.1) | |
| 2014/15 | 17 (10, 25) | 1.2 (0.6, 1.8) | 217 (132, 305) | 1.4 (1.2, 1.6) | 178 (108, 249) | 1.4 (1.2, 1.6) | |
| 2015/16 | 16 (0, 44) | 0.9 (0.5, 1.4) | 175 (1, 508) | 0.9 (0.8, 1.0) | 145 (1, 420) | 0.9 (0.7, 1.0) | |
| Total | 731 (549, 960) | 6.2 (5.8, 6.6) | 10,024 (7593, 12,937) | 6.5 (6.4, 6.7) | 8342 (6338, 10,768) | 6.6 (6.4, 6.7) | |
MA: Medically Attended; CI: Confidence Interval; PF: Prevented Fraction.
Over the period, the highest number of cases were prevented in the 2011/12 influenza season when vaccination coverage was highest (20.0%) and VE was estimated at 71.9% for children 6–35 months and 50% for children 36–59 months. During the 2011/12 influenza season, 538 (361–763) cases of influenza hospitalizations were averted (PF: 11.5%, 10.5–12.4%) and 7931 (5560–10,824) cases of influenza illnesses were averted (PF: 11.3%,11.1–11.6%), of which 6604 (4636–8990) were MA (PF: 11.4%,11.1–11.7%) (Table 2). The fewest cases were prevented in the 2015/16 influenza season when vaccination coverage was lowest (5.7%) and VE was estimated at 16% for children 6–59 months. There were 16 (0–44) cases of influenza hospitalizations averted (PF: 0.9%, 0.5–1.4%) and 175 (1–508) cases of influenza illnesses averted (PF: 0.9%, 0.8–1.0%), of which 145 (1–420) were MA (PF:0.9%, 0.7–1.0%).
Among three age groups, the highest PF of influenza illnesses was in children aged 6–23 months (PF: 8.2%, 7.9–8.4%), and the lowest was children aged 36–59 months (PF: 4.3%, 4.1–4.5%). The prevented fractions of influenza hospitalization were similar for children aged 6–23 months and children aged 24–35 months, at6.7% (6.0–7.3%) and 7.1% (6.1–8.2%) respectively. And that children aged 36–59 months remained fewer than all other age groups, at5.0% (4.3–5.7%) (Table 2).
3.4. Cases averted with assumed vaccination coverage 50%
If 50% of children aged 6–59 months in Suzhou had been vaccinated for each season, the estimated numbers of averted cases during the study period would have been 4059 (3120–5762) influenza hospitalizations (PF: 27.2% of expected, 26.4–27.9%) and 56,215 (42,925–78,849) influenza illnesses (PF: 28.5%, 28.3–28.7%), of which 46,596 (35,662–65,234) would be MA (PF: 28.5%, 28.3–28.7%) (Table 3).
Table 3.
The estimated number of influenza-associated outcomes averted by influenza vaccination in Suzhou, China, assuming a hypothetical vaccine coverage of 50%, 2011/12–2015/16 influenza seasons.
| Influenza hospitalization | MA influenza illness | Influenza illness | |||||
|---|---|---|---|---|---|---|---|
| N (95% CI) | PF (%) (95% CI) | N (95% CI) | PF (%) (95% CI) | N (95% CI) | PF (%) (95% CI) | ||
| Age (month) | 6–23 | 1888 (1380, 2598) | 27.1 (26.0, 28.1) | 22,654 (16,269, 31,270) | 29.7 (29.4, 30.0) | 19,497 (13,982, 26,848) | 29.7 (29.4, 30.1) |
| 24–35 | 816 (588, 1111) | 28.5 (26.9, 30.2) | 12,634 (8567, 17,809) | 28.8 (28.4, 29.2) | 10,057 (6819, 14,177) | 28.8 (28.4, 29.3) | |
| 36–59 | 1305 (654, 2925) | 25.5 (24.3, 26.7) | 20,153 (10,526, 41,675) | 26.1 (25.8, 26.4) | 16,451 (8579, 34,029) | 26.1 (25.8, 26.4) | |
| Influenza season | 2011/12 | 2026 (1243, 3694) | 33.0 (31.8, 34.2) | 30,830 (19,473, 53,464) | 33.5 (33.2, 33.8) | 25,620 (16,269, 44,222) | 33.6 (33.2, 33.9) |
| 2012/13 | 458 (362, 576) | 27.8 (25.6, 30.0) | 3207 (2448, 4161) | 27.9 (27.1, 28.7) | 2679 (2048, 3458) | 27.9 (27.0, 28.8) | |
| 2013/14 | 1123 (832, 1460) | 29.8 (28.3, 31.2) | 16,530 (11,749, 22,445) | 29.9 (29.5, 30.3) | 13,668 (9730, 18,574) | 29.9 (29.5, 30.3) | |
| 2014/15 | 197 (101, 320) | 12.7 (11.0, 14.3) | 2512 (1401,3851) | 14.6 (14.0, 15.1) | 2065 (1154, 3168) | 14.5 (13.9, 15.1) | |
| 2015/16 | 199 (0, 697) | 10.8 (9.4, 12.3) | 2382 (0, 7316) | 11.2 (10.7, 11.6) | 1960 (0, 6051) | 11.1 (10.7, 11.6) | |
| Total | 4059 (3120, 5762) | 27.2 (26.4, 27.9) | 56,215 (42,925, 78,849) | 28.5 (28.3, 28.7) | 46,596 (35,662, 65,234) | 28.5 (28.3, 28.7) | |
MA: Medically Attended; CI: Confidence Interval; PF: Prevented Fraction.
3.5. Sensitivity analysis
Under the current influenza vaccination program in Suzhou, when VE decreased by 10% compared with the current VE, the PF decrease varied from 0.3–1.8% depending on the influenza season. When VE increased by 10% compared with the current VE, the PF increase varied from 0.4–1.8% depending on the influenza season. When the influenza vaccination coverage was assumed to be 50% and the VE was 10% higher than the current VE, the PF increase varied from 4.3–5.2% depending on the influenza season (Supplemental Table 2 and Supplemental Table 3).
4. Discussion
From 2011 to 2016, influenza vaccination averted an estimated ~6% of expected hospitalizations and ~7% of influenza illnesses in children 6–59 months in Suzhou when influenza vaccination coverage averaged ~9%. Over the course of the study period influenza vaccination coverage declined in this population. This led to a decline in the estimated prevented fraction of influenza hospitalization and influenza illnesses over the study period, from around 12% in the 2011/12 influenza season to around 1% in 2015/16.
Unlike other studies on averted outcomes in settings where influenza vaccination coverage is higher [14,16,27–29], we describe estimates of averted outcomes in a low coverage setting. Despite the comparatively low coverage, we demonstrated that influenza vaccination can still be beneficial in preventing hospitalizations and influenza illnesses. Our findings from a setting with an average vaccination coverage of ~9% underscore a meaningful population level impact on averting influenza hospitalizations and influenza illnesses. Since our vaccine effectiveness estimates were similar to those of other studies, the difference in observed prevented fractions was likely associated with differences in the vaccination coverage [29]. This finding was observed in our own data when comparing the 2011/12 influenza season to 2012/13 and 2013/14 influenza seasons.
Influenza vaccination coverage in China is generally low, estimated at around 2% for the general population [30]. The reasons for the low coverage rate are multifactorial, including issues related to lack of confidence in the overall vaccination system and influenza vaccination’s designation as a non-immunization program [30,31]. However, compared to the general population, influenza vaccination coverage in younger children in China is higher [11,12,32]. In the 2011/12 influenza season, we found that the coverage for children 6–59 months was 20%. Despite a higher coverage in 2011/12, influenza vaccination coverage declined every year through 2015/16 in children 6–59 months in Suzhou. Although factors such as waning interest for influenza vaccine following the 2009 pandemic may have contributed to reduced vaccination, this decline likely occurred because after the 2011/12 influenza season, a policy was enacted which disallowed points of vaccination from setting prices for non-immunization program vaccination services [13]. This policy reduced the amount of service fees collected by vaccination sites and likely disincentivized vaccination sites from providing certain services such as influenza vaccination. Thus, influenza vaccination coverage levels can be particularly sensitive to policies related to the management of non-immunization program vaccinations since the government is not a guaranteed purchaser of services for these vaccinations. Any increase of influenza vaccination coverage in China will require an understanding of the incentives of vaccine purchase and distribution stakeholders.
In our hypothetical scenario where 50% influenza vaccination coverage was achieved for each year within our study period, vaccination would have averted an estimated ~27% of expected influenza hospitalizations and ~29% of influenza illnesses compared to ~6% of hospitalizations and ~7% of influenza illnesses. This finding is comparable to the median prevented fraction of 31% (median vaccination coverage: 55.0%) of expected influenza cases from 2010/11 to 2016/17 influenza seasons in the United States [26]. Thus, improving influenza vaccination coverage in Suzhou could have substantial impact in reducing influenza-associated morbidity in children 6–59 months each influenza season.
The methods used in this study have been used routinely in the United States to evaluate the impact of influenza vaccination on averted outcomes [14,15,26–28,33]; however, this is the first study to apply these methods to estimating the impact of influenza vaccination in China. Results from this study can be particularly useful in a country such as China that is currently developing influenza vaccination policy. Despite China CDC recommendations since 2014 for vaccinating children 6–59 months [10], we found that vaccination coverage in Suzhou decreased continuously even after the recommendations were issued. Providing easily interpretable evidence on the benefits of public health recommendations can be helpful for increasing support and compliance among policy makers and the general public. Our results demonstrate how multiple data sources can be applied to produce an easily interpretable result using local evidence that highlight the benefits of increasing influenza vaccination coverage to reduce influenza-associated morbidity.
Our study is subject to several limitations. First, we could not stratify VE estimates by clinical severity (e.g., ILI, SARI) given the declining influenza vaccination coverage over the study period. Second, although we selected Suzhou’s only tertiary care children’s hospital as our surveillance site to estimate influenza hospitalizations and MA influenza illnesses, there are other general hospitals in Suzhou which provide inpatient and outpatient care to pediatric patients. We also assumed that the positive rate of influenza in persons with influenza ILI who do not seek care was the same as that in MA influenza illnesses, which may overestimate the number of influenza illnesses. It is possible that the health seeking behaviors, baseline risk of influenza, vaccination coverage, and outcomes may vary among children seeking care at these hospitals from those at our study site and vary between children seeking care and not seeking care, which would limit the generalizability of our findings. Third, our Monte Carlo method did not account for uncertainty in the point estimate of the number of cases. Fourth, we did not have VE data by month and we did not have VE data specifically for Suzhou for all seasons. VE data from other locations in China were applied for certain seasons. Finally, although we considered average influenza activity level, vaccine effectiveness and vaccine coverage in the model, we have no individual level confounding factors which might influence the averted number estimation.
5. Conclusion
Even with low and decreasing coverage, influenza vaccination is estimated to have averted influenza-associated illness outcomes in children 6–59 months in Suzhou. Finding solutions to increase influenza vaccination coverage in children could substantially reduce influenza-associated illness.
Supplementary Material
Acknowledgements
We thank all children and their parents or guardians who have participated in this study, as well as the members of the Influenza Research Group. The authors are grateful to the US Centers for Disease Control and Prevention in Atlanta for its financial support.
Funding
The work was funded by a US CDC cooperative agreement (5U2GGH000018) and supported by the China-US Collaborative Program on Emerging and Re-emerging Infectious Diseases.
Footnotes
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Publisher's Disclaimer: Disclaimer
Publisher's Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention.
Appendix A. Supplementary material
Supplementary data to this article can be found online at https://doi.org/10.1016/j.vaccine.2020.10.069.
References
- [1].Iuliano AD, Roguski KM, Chang HH, Muscatello DJ, Palekar R, Tempia S, et al. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet 2018;391(10127):1285–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].World Health Organization Influenza (Seasonal); 2020
- [3].Neuzil KM, Mellen BG, Wright PF, Mitchel EJ, Griffin MR. The effect of influenza on hospitalizations, outpatient visits, and courses of antibiotics in children. N Engl J Med 2000;342(4):225–31. [DOI] [PubMed] [Google Scholar]
- [4].Wang D, Chen L, Ding Y, Zhang J, Hua J, Geng Q, et al. Viral etiology of medically attended influenza-like illnesses in children less than five years old in 2011–2014 Suzhou, China. J Med Virol 2016;88(8):1334–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Yu J, Zhang X, Shan W, Gao J, Hua J, Tian J, et al. Influenza-associated hospitalization in children younger than 5 years of age in Suzhou, China. Pediatr Infect Dis J 2019;38(5):445–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Zhang T, Zhang J, Hua J, Wang D, Chen L, Ding Y, et al. Influenza-associated outpatient visits among children less than 5 years of age in eastern China, 2011–2014. BMC Infect Dis 2016;16:267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Yu H, Huang J, Huai Y, Guan X, Klena J, Liu S, et al. The substantial hospitalization burden of influenza in central China: surveillance for severe, acute respiratory infection, and influenza viruses, 2010–2012. Influenza Other Respir Viruses 2014;8(1):53–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Neuzil KM, Hohlbein C, Zhu Y. Illness among schoolchildren during influenza season: effect on school absenteeism, parental absenteeism from work, and secondary illness in families. Arch Pediatr Adolesc Med 2002;156(10):986–91. [DOI] [PubMed] [Google Scholar]
- [9].World Health Organization. Vaccines against influenza WHO position paper - November 2012. Wkly Epidemiol Rec 2012;87(47):461–76. [PubMed] [Google Scholar]
- [10].Feng L, Yang P, Zhang T, Yang J, Fu C, Qin Y, et al. Technical guidelines for the application of seasonal influenza vaccine in China (2014–2015). Hum Vaccin Immunother 2015;11(8):2077–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Lau J, Ng C, Wu A, Ma YL, Lau M. Low coverage of influenza vaccination among Chinese children aged 12–23 months: Prevalence and associated factors. PLoS ONE 2018;13(10):e205561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Zhou L, Su Q, Xu Z, Feng A, Jin H, Wang S, et al. Seasonal influenza vaccination coverage rate of target groups in selected cities and provinces in China by season (2009/10 to 2011/12). PLoS ONE 2013;8(9):e73724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Zheng Y, Rodewald L, Yang J, Qin Y, Pang M, Feng L, et al. The landscape of vaccines in China: history, classification, supply, and price. BMC Infect Dis 2018;18(1):502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Kostova D, Reed C, Finelli L, Cheng PY, Gargiullo PM, Shay DK, et al. Influenza Illness and Hospitalizations Averted by Influenza Vaccination in the United States, 2005–2011. PLoS ONE 2013;8(6):e66312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Centers for Disease Control and Prevention. Past Seasons Estimated Influenza Disease Burden Averted by Vaccination; 2020. [Google Scholar]
- [16].Zhang Y, Cao Z, Costantino V, Muscatello DJ, Chughtai AA, Yang P, et al. Influenza illness averted by influenza vaccination among school year children in Beijing, 2013–2016. Influenza Other Respir Viruses 2018;12(6):687–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Suzhou Statistics Bureau. Suzhou statistical yearbook 2018. China Statistics Press; 2018. [Google Scholar]
- [18].Suzhou University Affiliated Children’s Hospital; 2020.
- [19].Wang D Analysis of influenza epidemiology and disease burden in outpatients under 5 years of age in Suzhou [Doctor]. Fudan University; 2014. [Google Scholar]
- [20].Wang Y, Chen L, Yu J, Pang Y, Zhang J, Zhang T, et al. The effectiveness of influenza vaccination among nursery school children in China during the 2016/17 influenza season. Vaccine 2018;36(18):2456–61. [DOI] [PubMed] [Google Scholar]
- [21].National Health Commission National influenza surveillance protocol. 2017; 2020.
- [22].Wang Y, Zhang T, Chen L, Greene C, Ding Y, Cheng Y, et al. Seasonal influenza vaccine effectiveness against medically attended influenza illness among children aged 6–59 months, October 2011–September 2012: A matched test-negative case-control study in Suzhou, China. Vaccine 2016;34(21):2460–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Fu C, Greene CM, He Q, Liao Y, Wan Y, Shen J, et al. Dose effect of influenza vaccine on protection against laboratory-confirmed influenza illness among children aged 6 months to 8 years of age in southern China, 2013/14–2015/16 seasons: a matched case-control study. Hum Vaccin Immunother 2020;16(3):595–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].He Q Effectiveness of seasonal influenza vaccine in children aged 6 to 59 months [Master]. Southern Medical University; 2014. [Google Scholar]
- [25].Wang Y, Chen L, Cheng Y, Zhou S, Pang Y, Zhang J, et al. Potential impact of B lineage mismatch on trivalent influenza vaccine effectiveness during the 2015–2016 influenza season among nursery school children in Suzhou, China. Hum Vaccin Immunother 2018;14(3):630–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Tokars JI, Rolfes MA, Foppa IM, Reed C. An evaluation and update of methods for estimating the number of influenza cases averted by vaccination in the United States. Vaccine 2018;36(48):7331–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Rolfes MA, Flannery B, Chung JR, O’Halloran A, Garg S, Belongia EA, et al. Effects of influenza vaccination in the United States during the 2017–2018 influenza season. Clin Infect Dis 2019;69(11):1845–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Reed C, Kim IK, Singleton JA, Chaves SS, Flannery B, Finelli L, et al. Estimated influenza illnesses and hospitalizations averted by vaccination–United States, 2013–14 influenza season. MMWR Morb Mortal Wkly Rep 2014;63(49):1151–4. [PMC free article] [PubMed] [Google Scholar]
- [29].Backer JA, Wallinga J, Meijer A, Donker GA, van der Hoek W, van Boven M. The impact of influenza vaccination on infection, hospitalisation and mortality in the Netherlands between 2003 and 2015. Epidemics-Neth 2019;26:77–85. [DOI] [PubMed] [Google Scholar]
- [30].Wang Q, Yue N, Zheng M, Wang D, Duan C, Yu X, et al. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: A meta-analysis. Vaccine 2018;36(48):7262–9. [DOI] [PubMed] [Google Scholar]
- [31].Cao L, Zheng J, Cao L, Cui J, Xiao Q. Evaluation of the impact of Shandong illegal vaccine sales incident on immunizations in China. Hum Vaccin Immunother 2018;14(7):1672–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Yang J, Atkins KE, Feng L, Pang M, Zheng Y, Liu X, et al. Seasonal influenza vaccination in China: Landscape of diverse regional reimbursement policy, and budget impact analysis. Vaccine 2016;34(47):5724–35. [DOI] [PubMed] [Google Scholar]
- [33].Jackson ML, Phillips CH, Benoit J, Jackson LA, Gaglani M, Murthy K, et al. Burden of medically attended influenza infection and cases averted by vaccination - United States, 2013/14 through 2015/16 influenza seasons. Vaccine 2018;36(4):467–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.