

Abstract
Background
Interns are vulnerable to emotional distress and burnout. Little is known about the extent to which interns’ well-being can be influenced by peer support provided by their senior residents.
Objective
To elucidate contributors to interns’ emotional distress and ways that peer support from senior residents may impact intern well-being.
Design
Qualitative study using semi-structured interviews conducted December 2017–March 2018.
Participants
Second year residents (n = 11) in internal medicine at a major academic medical center during the data collection period.
Approach
Constructivist grounded theory approach in which transcripts were analyzed in an iterative fashion using constant comparison to identify themes and to create a conceptual model.
Key Results
The investigators identified three themes around emotional distress and two themes around resident peer support. Distress was a pervasive experience among participants, caused by a combination of contextual factors that decreased emotional resilience (e.g., sleep deprivation) and acute triggers (e.g., patient death) that led to an abrupt increase in distress. Participants grappled with identity reconciliation throughout internship. Reaching clinical competency reinforced self-efficacy for participants. With regard to peer support, participants recalled that resident support was ad hoc, primarily involving task support and debriefing traumatic events. Participants reflected that their intern experiences shaped their supervisory support style once they became senior residents; they did not perceive any formalized, systematic approach to supporting interns.
Conclusions
We propose a model illustrating key points at which near-peers can make an impact in reducing interns’ distress and suggest strategies they can use. Given the substantial role peer learning plays in intern development, senior residents can impact their interns by normalizing emotions, allowing vulnerability, and highlighting the importance of self-care. A formalized peer support skill-building curriculum for senior residents may empower them to provide more effective support as part of their supervisory efforts.
Electronic supplementary material
The online version of this article (10.1007/s11606-020-05803-4) contains supplementary material, which is available to authorized users.
KEY WORDS: well-being, wellness, burnout, peer support, graduate medical education
INTRODUCTION
Resident physicians experience high levels of burnout in national studies1 and they are particularly vulnerable to emotional distress, burnout, and empathy erosion in their first year of training2. Given the immensity of the problem, there is a growing body of research around interventions to improve aspects of well-being and protect against burnout. Responding to emotional challenges has been highlighted as a key commitment that health care professionals must make to themselves and to each other3.
Resident well-being programs have traditionally been faculty-led and focused on interventions such as individual skill building (mindfulness4, mind-body interventions5, stress management6, or counseling7), group debriefing and facilitated discussion8, and positive psychology coaching9. On a faculty level, peer support has been shown to be beneficial to physicians in coping with emotional stressors10, sparking the creation of peer support programs at hospitals around the country11. Literature shows that interns rely heavily on the guidance, example, and support of senior residents who, as supervisory near-peers and teachers, play a significant role in their clinical learning and professional development 12, 13. However, little is known about the extent to which interns’ well-being can be influenced by support provided by their senior residents, and what peer support processes may be most effective for enhancing well-being. Promisingly, one recent study suggested that regular well-being check-ins with chief residents may normalize the intern experience and help interns manage stress14. To better understand the specific experience of interns, we conducted a qualitative study to elucidate contributors to emotional distress and ways that peer support from senior residents may impact intern well-being in our institution’s internal medicine residency program.
METHODS
Study Design
We used a constructivist grounded theory approach15 to understand emotional distress among interns and the role that support from senior residents played in coping with that distress.
Participants and Setting
One investigator (KM) invited all internal medicine postgraduate year (PGY)-2 residents at the University of California, San Francisco (UCSF), who had recently completed their PGY-1 year to participate in an interview. She sent invitations by email and scheduled interviews over the course of four months, with a plan to interview until the research team agreed that sufficient evidence existed to support themes (thematic saturation)16. As themes were identified, additional participants were recruited who might offer diverse perspectives and thereby contribute data to confirm, refute, and/or refine the themes. Participants did not receive any compensation for their participation.
Data Collection
From December 2017 to March 2018, one investigator (KM) conducted individual interviews using a semi-structured interview guide (Appendix), clustered in December, February, and March. The interview guide was developed through a review of the physician burnout/well-being and peer learning literature and was informed by the team’s experiences conducting well-being and burnout prevention programs at the residency level. After conducting a pilot interview, a question was added about how experiences as an intern impacted second year residents’ practices as near-peers. All interviews were audio-recorded and transcribed verbatim. Identifying information was removed from transcripts prior to analysis. Interviews ranged from 40 to 90 minutes.
The UCSF Institutional Review Board reviewed the study and approved it as exempt.
Data Analysis
Two investigators (KM and LT) coded all transcripts. After the first three interviews, we independently reviewed the transcripts and developed a preliminary set of codes. Initially, we planned to use peer learning theory to guide our analysis. However, after discussing the first three transcripts, we determined that the themes did not align with peer learning theory and used open coding to generate the codebook. Using constant comparative techniques15, we read each new interview and compared ideas conveyed in the new interviews with existing codes and themes. We added probes to some interview questions so we could explore preliminary themes in greater depth and also added new codes to our codebook to capture information that was not well-represented in existing codes. We met regularly to review and reconcile differences in coding. We used Dedoose software for coding and extracting data (Redondo Beach, CA).
After identifying a stable set of codes and completing open coding of all transcripts, the investigators (KM and LT) proceeded with axial coding to highlight relationships between coded excerpts. The third investigator (BO), a non-physician researcher with expertise in medical education and qualitative research, examined excerpts to check interpretations and identify connections to medical education literature. The final analytic step involved selective coding to develop a model of emotional distress during internship that integrated themes, then sharing this model and themes with groups of PGY-2 and PGY-3 internal medicine residents (including participants and non-participants) and residents and fellows from multiple specialties involved in education projects to check for resonance. These sessions confirmed the model and themes and resulted in no changes.
Reflexivity
The different perspectives of the members of our research team enabled robust discussion of themes and interpretations. KM was a peer PGY-2 resident at the time of the interviews and served as the sole interviewer— the team discussed the implications of this approach and felt that a peer interviewer was beneficial to encourage open, honest discussion in the interviews. LT and BO were blinded to all identities. Only KM knew the identity of participants and noted any ways in which relationships with study participants may have influenced her interactions and interpretations (e.g., personal knowledge of a situation described by a participant). The study team discussed these notes during open coding to ensure that these relationships did not influence KM’s coding of interview transcripts, and, in a few cases, codes were revised when it was determined that inferences based on external experiences had been made. The three perspectives of the research team (KM, a peer of participants; LT, a faculty member with well-being expertise; and BO, an education researcher external to the residency program) helped balance interpretations during analysis.
RESULTS
From interviews with 11 residents, we identified themes and a model of emotional distress during internship, as well as key ways in which peer support from senior residents impacted coping with distress.
Distress as a Pervasive Experience
All participants described significant emotional distress during internship and identified contextual factors and acute triggers as key sources of distress. Emotional distress included feelings of sadness, hopelessness, frustration, anxiety, and overwhelm. Distressing feelings varied by participant, and most described a combination of these feelings at different times during internship. They explained how contextual factors, such as volume of work, work hours, perceived expectation of perfection, isolation, and sleep deprivation, compounded to diminish their emotional reserve. Then acute triggers, primarily related to adverse patient care experiences, such as unexpected death, conflict around goals of care, and dealing with challenging or abusive patients caused an abrupt increase in distress. In some cases, distress was triggered by team dynamics. These triggers could push them over their coping threshold if their emotional reserve was low due to a high burden of contextual factors, causing enough distress to temporarily impact their ability to manage all of their responsibilities at work or at home. As one participant noted, “I can usually deal with a really sad patient case and breathe through it, and it’ll be okay. Or I can usually get a bunch of pages and just try to be calm and triage them, and it’ll all be okay... But they’re all happening at the same time. So, I think that’s the issue” (resident #10).
Participants recalled that lack of control over work schedule and flow, as well as a lack of control over aspects of patient outcomes such as social determinants of health, impacted their ability to cope with emotional distress as interns. They described a sense of self-doubt and sought external validation. These feelings were often compounded by feeling under-appreciated by superiors, patients, and families. One participant explained, “You want to prove that you belong here and that you can take care of someone and you’re not trying to kill them… I think that’s what drives a lot [of distress]… we all feel inadequate” (resident #3).
Grappling with Identity Reconciliation
Participants described feeling grief over the loss of their personal identity as this identity was subsumed by their professional role. This loss was a source of existential distress due to inability to maintain previous interests, relationships, and roles. As a result of intense, unique experiences, participants became alienated from those in their lives who could not relate to their professional experience and personal relationships suffered; they became isolated from former support. They also experienced grief as they reconciled expectations of what they thought they would be with who they became. One participant explained, “I think that part of that journey is reconciling with the death of your former self and the death of who you thought you were going to be. I think that there’s a mourning process there” (resident #7).
While participants mourned aspects of identity lost, they celebrated new aspects of their professional identity that emerged. Over time, participants learned to cope with difficult experiences of being a doctor such as patient deaths and saw their participation in these events as a privilege; they expressed gratitude for their unique role in patients’ lives. As their skills improved, participants gained confidence from patients identifying them as “my doctor” and becoming a doctor that patients choose. As one participant stated, “The days you feel like a really good doctor are the days where people are like, ‘You just told me I have stage IV cancer, but I want you to be my regular doctor. And you know what? When [I] die, I want my whole family to use you as [their] regular doctor.’” (resident #4).
Competency Reinforced Self-efficacy
Participants described a specific point during internship when they realized they had reached a threshold level of clinical competency. At this point, they could provide clinical care with more independence, which improved their sense of self-efficacy. One participant noted, “I think [I reached] a turning point. After that… I just didn’t feel scared as much anymore…I think it was a turning point in competency” (resident #3). During competency development, opportunities for autonomy contributed to feelings of self-efficacy when participants felt well-supported. However, autonomy could also contribute to distress if support was not available when needed.
Even before achieving clinical competency, developing experience and autonomy in non-clinical aspects of patient care, such as systems advocacy or providing emotional support to patients, reinforced self-efficacy.
“As an intern, I came to view deaths of patients as a very big privilege to be a part of. That time point in that patient’s life is so significant. And there are so few people in society that can guide a family and a patient through that process. And I found that to be almost rewarding in a sense that we can, kind of, like, get through this together” (resident #8).
Resident Support Was Ad Hoc
When reflecting on support by their senior residents, participants most commonly recalled seniors pitching in on tasks, such as navigating logistically complicated to-dos and holding their pagers in times of stress. One participant explained the value of this support, “I remember two or three times he held our pager during our morning report or during noon conference, so that we could go because he knew that was important to us. Just even little things where he recognized our personal goals or times when we were having emotional difficulties” (resident #5).
Ad hoc debriefing of traumatic events was the most common way in which senior residents provided explicit emotional support. Additionally, participants recalled few times when senior residents role-modeled showing or discussing their own emotions, but characterized it as a highly effective strategy when it occurred. One participant noted, “We had regular debriefs about where we both [were]… in our own emotional health with this very challenging case and [the senior resident] was open with how it was affecting her…which allowed me to do the same thing” (resident #1). How well people felt they could communicate and have a relationship with their team affected how supported they felt; this was sometimes challenging due to frequent team transitions.
Participants recognized that tailoring support to individual preferences is essential but extremely difficult to implement due to team discontinuity. Participants talked about the frustration of not receiving the right support as an intern, but then recognized how difficult it was to provide individualized support once they were themselves senior residents. This theme was more prominent in interviews conducted in the second half of the academic year. One participant discussed this challenge:
“Just thinking of how can I best support this person? Is it by taking away some of the busywork, so they can go home earlier? Or is it… this patient wants to have another goals conversation, for the third time today, with different family members, could I just do that for them?... But I think, it’s so hard. Because I think it does really vary based on the person” (resident #2).
Intern Experiences Shaped Supervisory Support Style
Once they became senior residents, participants reported replicating positive examples that they had experienced or seen role-modeled as interns. Participants also perceived that, as supervising residents, they used strategies that addressed gaps in support that they did not get as interns. For example, very few participants recalled being asked directly about self-care and coping during internship by a superior, but most highlighted checking in about self-care as a key strategy they employ as senior residents. One participant addressed this, “I use some of the things that I think I would have wanted [as an intern] with [my] interns, now. Like, ask my interns on a semi-regular basis how they’re doing outside the hospital…I didn’t know it at the time but I wished that someone had asked me those questions” (resident #1). They did not perceive any formalized, systematic approach to providing support to interns. They also did not recall receiving training in how to provide emotional support to interns once they became senior residents.
A Model of Distress
We developed a model (Fig. 1) integrating the themes related to emotional distress and the role of peer support during internship. The model shows that interns’ level of emotional distress fluctuates over time. Throughout internship, identity stress and contextual factors (e.g., lack of control, work intensity, schedule, isolation) contribute to some level of distress that interns tolerate throughout the course of the year. Interns also encounter acute triggers of distress, such as patient deaths, challenging patients, or difficult goals of care conversations. When these triggers occur during a period with a particularly high burden of contextual factors, distress may escalate beyond an intern’s coping threshold to temporarily affect perceived ability to optimally manage professional or personal responsibilities. Interventions by senior residents generally aim to reduce distress by providing logistical support (to decrease the contribution of workload as a contextual factor) and debriefing traumatic events.]-->
Figure 1.
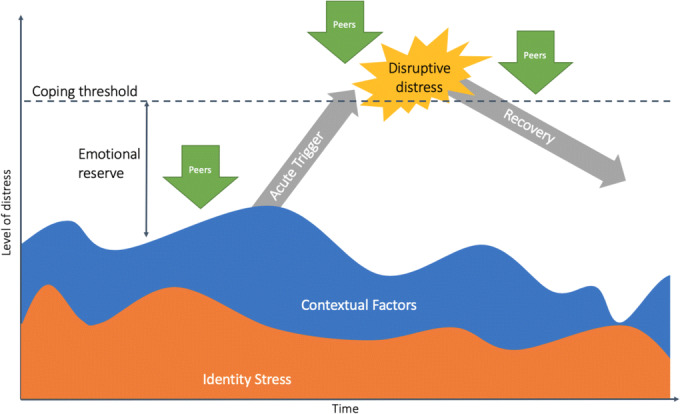
A model of emotional distress and opportunities for peer support during internship.
DISCUSSION
Our research confirms that emotional distress is common during internship, and suggests that senior residents provide ad hoc emotional support for their interns. Our findings also reveal a perceived absence of formal strategies that prepare residents to provide emotional support to interns.
In our study, interns describe many of the same factors known to contribute to physicians’ emotional distress and burnout17. The life of an intern is a barrage of contextual factors such as long hours, sleep deprivation, poor work-life integration18, isolation19, and challenging work environments20. These contextual factors are layered on top of identity stress21 that contributed to significant self-doubt among participants in our study. When acute triggers of emotional distress such as patient death, challenging patient/family interactions, or disagreement regarding goals of care are superimposed on the burden of preexisting contextual factors, an intern’s distress can exceed their coping threshold such that they feel temporarily unable to optimally fulfill their responsibilities. These findings complement work by Abedini and colleagues, who found that residents experience both existential and circumstantial aspects of burnout, which require different strategies for recovery22. Our model of distress also builds on prior knowledge to suggest potential intervention points for effective peer support that could reduce intern distress.
Work by Hu and colleagues indicates that physicians gravitate towards peer support as a strategy for coping with stressors10. Similarly, we found that the interns in our study tended to look first to their near-peer senior residents for support after distressing events, and that senior residents attempted to provide that support. Without a roadmap or specific training, senior residents primarily focused on logistical support (i.e., helping interns with tasks); deliberate emotional support generally occurred on an ad hoc basis in response to traumatic clinical situations, sometimes at a point when an emotional reaction from the intern or the team could no longer be ignored. Perceived quality of support varied widely, and participants perceived that their supervisory residents lacked a framework or formal training to guide them. When reflecting on their transition to being a senior resident, the same participants recognized that their own strategies for support were primarily based on informal learning from role modeling and perceived gaps, rather than from formal instruction.
Our study therefore suggests that creating a learning environment that acknowledges emotion by training senior residents to understand contributors to interns’ emotional distress and to provide emotional support can potentially impact interns’ well-being. We suspect peers can be particularly impactful in three areas: (1) improving coping with contextual factors, (2) addressing triggers of acute distress, and (3) promoting recovery after distress (see Fig. 1).
A longitudinal peer support curriculum during residency training would allow senior residents to deliberately build these skills, rather than developing them ad hoc through trial and error, and could be geared to address these three potential areas of impact. First, educating residents about our model for emotional distress during internship and training them to understand the layers that contribute to distress may allow them to recognize distress earlier and to address contextual factors as they build. Second, in order to address acute triggers of distress, senior residents could be armed with a communication framework to guide them in proactively reaching out to their interns when traumatic experiences occur. Structured frameworks are effective in other areas of communication in medicine, such as breaking bad news23. Like breaking bad news, providing peer support between residents is a complex communication task that often must take place in busy clinical environments, in the midst of many competing bids for attention, while senior residents are stressed themselves. A framework for peer support could build on the principles of an effective peer support encounter proposed by Shapiro and colleagues, including listening, reflecting, and making referrals11. Third, to promote recovery after distress, a curriculum could provide opportunities to practice effective communication skills and incorporate positive psychology techniques that foster resilience in a low-stakes environment where feedback is provided. Lastly, a curriculum would need to educate residents about the limitations of peer support and parameters for escalation when additional support is needed. This multi-pronged approach to a resident curriculum would allow for longitudinal development tied to the progression of their leadership roles in their clinical work.
While we believe resident peer support could be effective, we acknowledge that senior residents are vulnerable to burnout themselves, and we are wary of framing peer support as a complete solution to intern distress—it is only one piece of the puzzle. Support and allyship of faculty and program leaders who have power to make larger scale system change is essential. Additionally, residents need protected time for this curriculum, rather than adding it on top of existing responsibilities.
Our findings must be interpreted in light of study limitations. All participants were in the same year of training in one specialty at one institution and thus represent perspectives shaped by a particular context and culture. Two of three of our investigators are involved in the residency program and inevitably view the data through this lens. As with any retrospective interviews, there is also risk that participants inaccurately recalled the events of their intern year. Additionally, we focused our interviews on the participants’ intern experiences, and did not interview their supervising senior residents, though we did include some questions about the participants’ own PGY2 supervisory experience. Discussions among the full research team and member checking both with residents who were part of the study and with resident peers who did not participate in the study provided some ways of ensuring the credibility of interpretations.
CONCLUSION
We propose a model illustrating key points at which near-peers can make an impact in reducing interns’ distress and suggest strategies they can use. Currently, senior residents primarily provide support by accomplishing tasks or navigating logistics, as well as debriefing traumatic events. Our findings highlight opportunities to address the contributors to distress more holistically; reducing the burden of contextual factors by implementing multilevel solutions at the personal, cultural, and systems level is necessary. While systems-level reform is beyond the scope of the resident role, senior residents still have an opportunity to support interns’ well-being. Given the substantial role that peer learning plays in intern development, senior residents can impact their interns by normalizing emotions, allowing vulnerability, and highlighting the importance of self-care. Since senior residents are already providing ad hoc support, a formalized peer support skill-building curriculum for senior residents may empower them to provide more effective support as part of their supervisory efforts.
Electronic supplementary material
(DOCX 59 kb)
Funding Information
This study was funded by a Pathways Grant, UCSF School of Medicine Resource Allocation Program for Trainees.
Compliance with Ethical Standards
The UCSF Institutional Review Board reviewed the study and approved it as exempt.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Footnotes
Prior Presentations
UCSF Education Showcase, April 30, 2018.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443–451. doi: 10.1097/ACM.0000000000000134. [DOI] [PubMed] [Google Scholar]
- 2.Bellini LM, Baime M, Shea JA. Variation of mood and empathy during internship. JAMA. 2002;287(23):3143. doi: 10.1001/jama.287.23.3143. [DOI] [PubMed] [Google Scholar]
- 3.Thomas LR, Ripp JA, West CP. Charter on physician well-being. JAMA. 2018;319(15):1541. doi: 10.1001/jama.2018.1331. [DOI] [PubMed] [Google Scholar]
- 4.Goldhagen BE, Kingsolver K, Stinnett SS, Rosdahl JA. Stress and burnout in residents: impact of mindfulness-based resilience training. Adv Med Educ Pract. 2015;6:525–532. doi: 10.2147/AMEP.S88580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kemper KJ, Khirallah M. Acute effects of online mind–body skills training on resilience, mindfulness, and empathy. J Evid Based Complement Alternat Med. 2015;20(4):247–253. doi: 10.1177/2156587215575816. [DOI] [PubMed] [Google Scholar]
- 6.Milstein JM, Raingruber BJ, Bennett SH, Kon AA, Winn CA, Paterniti DA. Burnout assessment in house officers: evaluation of an intervention to reduce stress. Med Teach. 2009;31(4):338–341. doi: 10.1080/01421590802208552. [DOI] [PubMed] [Google Scholar]
- 7.Guille C, Zhao Z, Krystal J, Nichols B, Brady K, Sen S. Web-based cognitive behavioral therapy intervention for the prevention of suicidal ideation in medical interns. JAMA Psychiatry. 2015;72(12):1192. doi: 10.1001/jamapsychiatry.2015.1880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abrams MP. Improving resident well-being and burnout: the role of peer support. J Grad Med Educ. 2017;9(2):264. doi: 10.4300/JGME-D-16-00805.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Palamara K, Kauffman C, Chang Y, et al. Professional development coaching for residents: results of a 3-year positive psychology coaching intervention. J Gen Intern Med. 2018;33(11):1842–1844. doi: 10.1007/s11606-018-4589-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hu Y-Y, Fix ML, Hevelone ND, et al. Physicians’ needs in coping with emotional stressors. Arch Surg. 2012;147(3):212. doi: 10.1001/archsurg.2011.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shapiro J, Galowitz P. Peer support for clinicians. Acad Med. 2016;91(9):1200–1204. doi: 10.1097/ACM.0000000000001297. [DOI] [PubMed] [Google Scholar]
- 12.Baldwin DC, Daugherty SR. How residents say they learn: a national, multi-specialty survey of first- and second-year residents. J Grad Med Educ. 2016;8(4):631–639. doi: 10.4300/JGME-D-16-00182.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Seltz LB, Preloger E, Hanson JL, Lane L. Ward rounds with or without an attending physician: how interns learn most successfully. Acad Pediatr. 2016;16(7):638–644. doi: 10.1016/j.acap.2016.05.149. [DOI] [PubMed] [Google Scholar]
- 14.Fischer J, Alpert A, Rao P. Promoting intern resilience: individual chief wellness check-ins. MedEdPORTAL. 2019;15:10848. doi: 10.15766/mep_2374-8265.10848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Charmaz K. Constructionism and the grounded theory method. In: Holstein JA, Gubrium JF, editors. Handbook of Constructionist Research. New York: The Guilford Press; 2008. pp. 397–412. [Google Scholar]
- 16.Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies. Qual Health Res. 2016;26(13):1753–1760. doi: 10.1177/1049732315617444. [DOI] [PubMed] [Google Scholar]
- 17.O’Dowd E, O’Connor P, Lydon S, et al. Stress, coping, and psychological resilience among physicians. BMC Health Serv Res. 2018;18(1):730. doi: 10.1186/s12913-018-3541-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Guille C, Frank E, Zhao Z, et al. Work-family conflict and the sex difference in depression among training physicians. JAMA Intern Med. 2017. 10.1001/jamainternmed.2017.5138. [DOI] [PMC free article] [PubMed]
- 19.Rogers E, Polonijo AN, Carpiano RM. Getting by with a little help from friends and colleagues: testing how residents’ social support networks affect loneliness and burnout. Can Fam Phys Med. 2016;62(11):e677–e683. [PMC free article] [PubMed] [Google Scholar]
- 20.Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377. doi: 10.1001/archinternmed.2012.3199. [DOI] [PubMed] [Google Scholar]
- 21.Law M, Lam M, Wu D, Veinot P, Mylopoulos M. Changes in personal relationships during residency and their effects on resident wellness. Acad Med. 2017;92(11):1601–1606. doi: 10.1097/ACM.0000000000001711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Abedini NC, Stack SW, Goodman JL, Steinberg KP. “It’s Not Just Time Off”: a framework for understanding factors promoting recovery from burnout among internal medicine residents. J Grad Med Educ. 2018;10(1):26–32. doi: 10.4300/JGME-D-17-00440.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302–311. doi: 10.1634/theoncologist.5-4-302. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX 59 kb)