

Summary
Due to the significant spread of a new type of coronavirus (SARS-CoV-2) infection (COVID-19) in China, the Chinese government blockaded several cities in Hubei Province. Japanese citizens lost a means of transportation to return back to Japan. The National Center for Global Health and Medicine (NCGM) helped the operation of charter flights for evacuation of Japanese residents from Hubei Province, and this article outlines our experiences. A total of five charter flights were dispatched, and the majority of returnees (793/829 [95.7%]) were handled at NCGM. A large number of personnel from various departments participated in this operation; 107 physicians, 115 nurses, 110 clerical staff, and 45 laboratory technicians in total. Several medical translators were also involved. In this operation, we conducted airborne precautions in addition to contact precautions. Eye shields were also used. The doctors collecting the pharyngeal swab used a coverall to minimize the risk of body surface contamination from secretions and droplets. Enhanced hand hygiene using alcohol hand sanitizer was performed. Forty-eight persons were ultimately hospitalized after the triage at NCGM operation, which was more than the number of persons triaged at the airport (n = 34). Of those hospitalized after NCGM triage, 8.3% (4/48 patients) ultimately tested positive for SARS-CoV-2, significantly higher than the positive rate among subjects not triaged (4/48 [8.3%] vs. 9/745 [1.2%]: p = 0.0057). NCGM participated in a large-scale operation to evacuate Japanese nationals from the COVID-19 epidemic area. We were able to establish a scheme through this experience that can be used in the future.
Keywords: charter flight, Japan, airborne precautions, contact precautions, SARS-CoV-2, COVID-19
Introduction
Since the end of 2019, an accumulation of severe pneumonias of unknown cause was reported in Wuhan City, Hubei Province, China, which was subsequently found to be a new type of coronavirus (SARS-CoV-2) infection (COVID-19) (1). Due to the significant spread of the infection in China, especially in Wuhan City and Hubei Province, the Chinese government blockaded several cities in Hubei Province including Wuhan on January 23, 2020 (2). Due to the blockade, Japanese citizens lost a means of transportation to return back to Japan. The National Center for Global Health and Medicine (NCGM) helped the operation of charter flights for evacuation of Japanese residents from Hubei Province, and this article outlines our experiences.
Operational Methods and Results
Summary of the number of persons returning from charter flights
A total of five charter flights were dispatched, and the majority of returnees were handled at NCGM. The number of persons returning from charter flights are summarized in Table 1 (3-6). Among the returnees, 2~6.7% of the returnees on each flight were transported directly from the airport to other hospitals from the initial triage at the Haneda Airport. NCGM took care of the remaining returnees.
Table 1. Summary of the number of persons returning from charter flights.
| Flight | Date | Number of returnees | Symptomatic patients triaged at airport(a) | Returnees screened at NCGM | Numbers of patients admitted after NCGM triage(d,e) |
|---|---|---|---|---|---|
| No.1 | 29/Jan/2020 | 206 | 5 (2.4%) | 199(b) (96.6%) | 7 (3.4%) |
| No.2 | 30/Jan/2020 | 210 | 13 (6.2%) | 197 (93.8%) | 13 (6.2%) |
| No.3 | 31/Jan/2020 | 150 | 10 (6.7%) | 140 (93.3%) | 15 (10%) |
| No.4 | 7/Feb/2020 | 198 | 4 (2%) | 194(c) (98%) | 8(c) (4%) |
| No.5 | 17/Feb/2020 | 65 | 2 (3.1%) | 63 (96.9%) | 5 (7.7%) |
| Total | 829 | 34 (4.1%) | 793 (95.7%) | 48 (5.8%) |
(a)Transferred to other hospitals from Haneda airport; (b) Two persons rejected screening and were not screened at NCGM; (c) Including three family members for attending purpose; (d) People who were not admitted were quarantined for 14 days at public facilities; (e) % was calculated using the denominator of total numbers of returnees.
NCGM's response system
Under the direction of the Ministry of Health, Labour and Welfare, NCGM helped the screening of COVID-19 infection among returnees, in collaboration with the National Institute of Infectious Diseases. Because returnees had been having a hard time to come back to Japan during the emergent situation, we also provided care for the persons who felt sick as well as provided food and drinks for them. A large number of personnel from various departments participated in this operation; infectious disease doctors, support doctors from other departments, the nursing department, the medical professions division, the department of clinical laboratory, and the infection control team. The approximate number of staff members who participated in the operation at NCGM is summarized in Table 2.
Table 2. The number of staff members who participated in the operation at NCGM.
| Flight | Date | Number of returnees | Physicians | Nurses | Clerical staff | Laboratory technicians | Total |
|---|---|---|---|---|---|---|---|
| No.1 | 29/Jan/2020 | 206 | 25 | 19 | 28 | 5 | 77 |
| No.2 | 30/Jan/2020 | 210 | 25 | 26 | 19 | 6 | 76 |
| No.3 | 31/Jan/2020 | 150 | 20 | 24 | 23 | 5 | 72 |
| No.4 | 7/Feb/2020 | 198 | 22 | 27 | 21 | 6 | 76 |
| No.5 | 17/Feb/2020 | 65 | 15 | 19 | 19 | 2 | 55 |
| Total | 829 | 107 | 115 | 110 | 24 | 356 |
After arrival of the buses, which carried returnees from Haneda Airport, we were divided into the following groups, with nurses and clerical staff guiding the returnees between each section. Large sightseeing buses were chartered to transport about 15 to 25 people per bus, with about 5 to 6 buses per flight.
1.Bus triage
ICNs (Certified Infection Control Nurses) and other nurses (3 to 5 nurses) triaged symptomatic patients in the bus. Returnees were also asked to fill out a questionnaire inside the bus as much as possible.
2.Guidance
Symptomatic persons who were triaged on the bus were directed by the clerical staff to the Infectious Diseases department, where a physician provided medical care to the patients thereafter. The remainder were directed by the clerk to a site for questioning and specimen collection.
3.Reception
Clerical staff assigned reception numbers and handed over specimen containers and performed other reception duties.
4.Interview
The doctors confirmed the contents of the questionnaire (Table 3). Those with additional symptoms or suspected unprotected exposure to COVID-19 confirmed patients identified at this stage were referred to the infectious disease outpatient clinic. Nurses and clerical staff guided the patient from the interview to blood collection and pharyngeal swab collection.
Table 3. Summary of the questionnaire.
| ● Age, sex and date of birth |
| ● Address (where you will be staying in Japan) and telephone number |
| ● Area of stay in Hubei Province of China within the past 14 days |
| ● History of contact with a person with fever or cough symptoms in the past 14 days |
| ● History of contact (or possible contact) with patients with COVID-19 infection within the past 14 days |
| ● The presence or absence of any abnormality in physical condition and its symptoms |
| ● Taking any antipyretic, cold medicine or pain medication. |
| ● Body temperature (measured by NCGM) |
5.Blood collection
The nurse and pediatrician drew blood samples to test for SARS-CoV-2 PCR testing as well as antibodies for SARS-CoV-2.
6.Pharyngeal swab specimen collection
Pharyngeal swab specimens were collected for SARS-CoV-2 PCR testing by a physician.
7.Specimen confirmation and collection
The specimens and medical questionnaires were collected. The average number of returnees per staff member in each occupation was as follows; 9-10 doctors, 5-8 nurses, 8-14 clerical staff, and 28-40 laboratory technicians (For flights 4 and 5, the percentage of children was particularly high, therefore, it is not included in the above average calculation because we needed more staff members than other flights). In the real operation, one doctor who collected pharyngeal swab samples handled about 40-50 specimens by himself. For nurses, the number of personnel needed could have been reduced if there was no need for blood draws. In addition, many Japanese families with Chinese nationality were included in the latter half of the flights (flights 4 and 5), and several Chinese interpreters were assigned from the International Health Care Center to assist with operations. Although there were children under six years old on each flight, the number of children was particularly high on the fourth and fifth flights, and pediatrician support was important throughout. In addition, although not included in the above, there was a need for personnel to timely communicate with airport quarantine and the Ministry of Health and Welfare.
In terms of response locations, it was necessary to choose locations that did not intersect with the hospital's patients. Triage was conducted in a room with a capacity of about 100 people, using a dedicated elevator from the backside parking lot. For the collection of pharyngeal swab specimens, a dedicated staff member was assigned to a separate room with an open window (a separate room was available for flights 4 and 5).
Infection control
In this operation, we conducted airborne precautions in addition to contact precautions (Figure 1). Eye shields were used according to the recommendations of the CDC and WHO (7,8).
Figure 1.
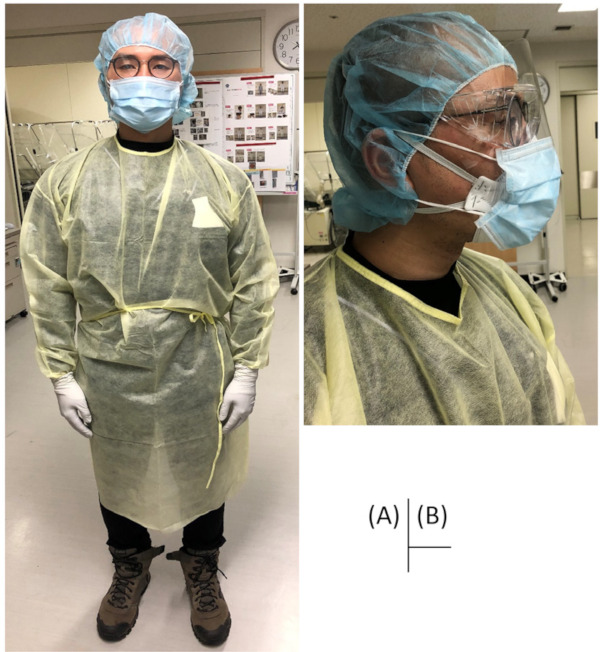
Personal protective equipment used in this operation.
In addition to the above, the doctor collecting the pharyngeal swab used a coverall to minimize the risk of body surface contamination by secretions and droplets (Figure 2). The doctor of the Department of Infectious Diseases instructed the staff of each section in the donning of personal protective equipment (PPE) prior to the start of the operation, and periodically checked for inappropriate use during the operation. Alcoholic hand sanitizers were placed in various locations for hand hygiene.
Figure 2.
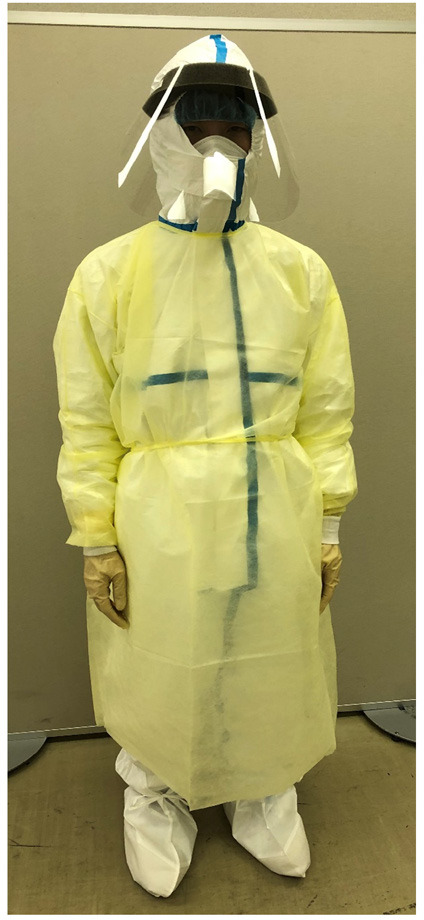
Personal protective equipment used in this operation to obtain pharyngeal swab samples.
Number of symptomatic patients and summary of SARS-CoV-2 test results
A summary of the number of NCGM cases that resulted in hospitalization is shown in Table 1. Although quarantine triage was conducted at the airport upon arrival of the charter flight (34 persons in total), 48 persons were ultimately hospitalized due to fever or symptoms (those with strong symptoms or relatively high probability of exposure) during the NCGM operation, which was more than the number of persons triaged at the airport. Of those hospitalized (NCGM or other hospital) after NCGM triage, 8.3% (4/48 patients) ultimately tested positive, which was significantly higher than the positive rate among subjects not triaged, and suggested the effectiveness of triage at NCGM (4/48 [8.3%] vs. 9/745 [1.2%]: p = 0.0057 [Fisher's exact test]).
Discussion
NCGM had an extremely valuable experience in operating a mass return from an emerging infectious disease epidemic area. Although this was the first time for such a large scale evacuation of Japanese people, we were able to complete the operation without any major problems.
With regard to the evacuation of its own citizens from China, where the spread of COVID-19 infection was initially recognized, the United States, Germany, and other countries, as well as Japan, had responded. Due to geographical proximity and economic ties, the number of Japanese staying in China was large (9), and indeed, it was much larger than Germany (126 people), with more than 800 evacuations, which was on a par with the United States (10,11).
In a paper on evacuation from Wuhan in Germany (11), of 126 people, 10 (7.9%) were triaged in an airplane (e.g., symptomatic or suspected exposure to COVID-19 cases) and an additional 1/116 (0.9%) were triaged in a subsequent physician's assessment at a medical assessment center. However, as a result, 2/114 (1.8%) PCR-positive individuals with SARS-CoV-2 were from people who were not triaged. The positive rate among asymptomatic patients was similar to that in Japan, where the rate was 1.2%, while the Japanese operation had a relatively high positive rate of 5.9% (2/34) among symptomatic patients at the airport and 8.3% (4/48) among those hospitalized after triage at NCGM. One of the reasons for this high rate of positive triage at our center, even though it was secondary triage, was the use of screening by experienced physicians, experienced nurses including ICNs, and Infectious Diseases physicians. The fact that the population of the Japanese cohort had a higher prevalence of symptoms than the German cohort may also have played a role.
Information on the number of staff members, location, means of transportation, and infection control in this operation is considered to be extremely important when conducting similar operations in the future. The hospital is a designated medical institution for specified infectious diseases, and many of the staff were more familiar with infection control measures even in ordinary times because the hospital routinely treats patients with infectious diseases and promotes infection control measures. However, the time to prepare for this operation was extremely limited, and we did not have enough time to train clerical staff for donning and doffing PPE in advance. We changed PPE to draw blood from pediatric patients from contact and droplet precautions (Figure 1) to coverall with N95 (Figure 2) for the latter half of the flights expecting that coverall might protect the staff members better in this circumstance. Although no positive results were reported this time from children, special care and preparation were considered necessary for infection control for this population. Although a few staff members visited the department of infectious diseases for respiratory tract symptoms within 2 weeks after participation in this operation, no one was confirmed to be infected with COVID-19; a detailed evaluation using serum antibodies is being planned in the future. In addition, central government officials, airline company employees, bus drivers, and others involved in this operation were screened for possible COVID-19 infection at the NCGM; none of them tested positive for SARS-CoV-2 by pharyngeal swab specimen PCR tests (data not shown).
Various studies are currently underway, and new evidence related to the pathogenesis of COVID-19 and effective infection control measures is awaited in the future from this operation cohort.
In conclusion, NCGM with a mission for infectious diseases, participated in a large-scale operation to evacuate Japanese nationals from the COVID-19 epidemic area. We were able to establish a scheme through this experience that can be used in the future.
Acknowledgements
We would like to express our heartfelt gratitude to all the NCGM staff who were involved in this operation, and to all the people at the other facilities involved in this operation for their support.
References
- 1. World Health Organization. WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed April 20, 2020).
- 2. BBC. China coronavirus: Lockdown measures rise across Hubei province. https://www.bbc.com/news/world-asia-china-51217455 (accessed April 20, 2020).
- 3. National Institute of Infectious Diseases. https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasr-news/9525-483p01.html (accessed April 20, 2020).
- 4. National Institute of Infectious Diseases. https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasr-news/9527-483p02.html (accessed April 20, 2020). (in Japanese) .
- 5. National Institute of Infectious Diseases. https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasr-news/9528-483p03.html (accessed April 20, 2020). (in Japanese) .
- 6. National Institute of Infectious Diseases. https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasr-news/9557-483p04.html (accessed April 20, 2020). (in Japanese) .
- 7. Centers for Disease Control and Prevention. Using Personal Protective Equipment (PPE). https://www.cdc.gov/coronavirus/2019-ncov/hcp/using-ppe.html (accessed April 20, 2020).
- 8. World Health Organization. Infection prevention and control during health care when novel coronavirus (nCoV) infection is suspected, Interim guidance. https://www.who.int/publications-detail/infection-prevention-and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125 (accessed April 20, 2020).
- 9. Qian Z, Elsinga S. "Nali Lai de?" - An Overview of Expat Demographics in China. https://www.china-briefing.com/news/nali-lai-de-overview-expats-china/ (accessed April 20, 2020).
- 10. Evacuation of Americans from Wuhan, China. https://china.usembassy-china.org.cn/evacuation-of-americans-from-wuhan-china/ (accessed April 20, 2020).
- 11. Hoehl S, Rabenau H, Berger A, et al. Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China. N Engl J Med. 2020; 382:1278-1280. [DOI] [PMC free article] [PubMed] [Google Scholar]