

Clinical trials have ruled out a role of hydroxychloroquine in the treatment of COVID-19, but it has been hypothesized that hydroxychloroquine's activity against SARS-CoV-2 in the laboratory suggests a role in prevention. This randomized controlled trial tests hydroxychloroquine as postexposure prophylaxis for SARS-CoV-2 infection.
Visual Abstract. Postexposure Hydroxychloroquine Prophylaxis to Prevent SARS-CoV-2 Infection.
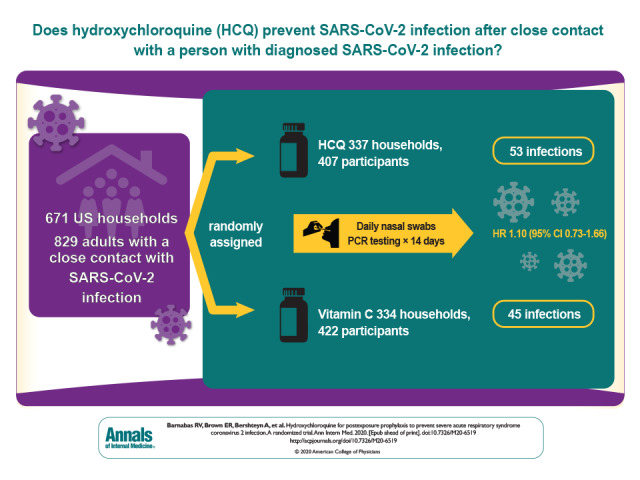
Clinical trials have ruled out a role of hydroxychloroquine in the treatment of COVID-19, but it has been hypothesized that hydroxychloroquine's activity against SARS-CoV-2 in the laboratory suggests a role in prevention. This randomized controlled trial tests hydroxychloroquine as postexposure prophylaxis for SARS-CoV-2 infection.
Abstract
Background:
Effective prevention against coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is currently limited to nonpharmaceutical strategies. Laboratory and observational data suggested that hydroxychloroquine had biological activity against SARS-CoV-2, potentially permitting its use for prevention.
Objective:
To test hydroxychloroquine as postexposure prophylaxis for SARS-CoV-2 infection.
Design:
Household-randomized, double-blind, controlled trial of hydroxychloroquine postexposure prophylaxis. (ClinicalTrials.gov: NCT04328961)
Setting:
National U.S. multicenter study.
Participants:
Close contacts recently exposed (<96 hours) to persons with diagnosed SARS-CoV-2 infection.
Intervention:
Hydroxychloroquine (400 mg/d for 3 days followed by 200 mg/d for 11 days) or ascorbic acid (500 mg/d followed by 250 mg/d) as a placebo-equivalent control.
Measurements:
Participants self-collected mid-turbinate swabs daily (days 1 to 14) for SARS-CoV-2 polymerase chain reaction (PCR) testing. The primary outcome was PCR-confirmed incident SARS-CoV-2 infection among persons who were SARS-CoV-2 negative at enrollment.
Results:
Between March and August 2020, 671 households were randomly assigned: 337 (407 participants) to the hydroxychloroquine group and 334 (422 participants) to the control group. Retention at day 14 was 91%, and 10 724 of 11 606 (92%) expected swabs were tested. Among the 689 (89%) participants who were SARS-CoV-2 negative at baseline, there was no difference between the hydroxychloroquine and control groups in SARS-CoV-2 acquisition by day 14 (53 versus 45 events; adjusted hazard ratio, 1.10 [95% CI, 0.73 to 1.66]; P > 0.20). The frequency of participants experiencing adverse events was higher in the hydroxychloroquine group than the control group (66 [16.2%] versus 46 [10.9%], respectively; P = 0.026).
Limitation:
The delay between exposure, and then baseline testing and the first dose of hydroxychloroquine or ascorbic acid, was a median of 2 days.
Conclusion:
This rigorous randomized controlled trial among persons with recent exposure excluded a clinically meaningful effect of hydroxychloroquine as postexposure prophylaxis to prevent SARS-CoV-2 infection.
Primary Funding Source:
Bill & Melinda Gates Foundation.
As of 3 December 2020, there have been 64 million reported cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), and 1 498 772 deaths globally (1), of which almost 14 million cases and 274 121 deaths were reported in the United States. A large proportion of people infected with SARS-CoV-2 are asymptomatic or experience only mild acute symptoms but may still transmit infection to close contacts (2, 3), thus contributing to epidemic growth (4). Within households, the incidence of SARS-CoV-2 is high: 10% to 30% of household contacts acquire infection (5). Although physical distancing, mask use, ventilation, and handwashing decrease SARS-CoV-2 transmission (6–8), identifying effective pharmaceutical interventions to prevent SARS-CoV-2 acquisition is an exigent public health priority (9). Postexposure prophylaxis (PEP) given to persons exposed to other viral infections, such as influenza and HIV, is effective and commonly used for prevention (10–12). Effective PEP for SARS-CoV-2 may decrease new infections and mitigate community transmission.
Hydroxychloroquine, a chloroquine analogue, has been used safely for over 6 decades as an antimalarial and to treat autoimmune conditions, with broad activity against intracellular organisms (13). With standard dosing, chloroquine inhibits SARS-CoV-2 replication in vitro (14, 15). Observational studies in health care settings supported the use of hydroxychloroquine to prevent SARS-CoV-2 (16, 17). Hydroxychloroquine and chloroquine are widely available globally; as such, they are ideal candidates for repurposed pharmaceutical interventions to prevent SARS-CoV-2 infection because they could be rapidly disseminated for new indications, including in resource-limited settings. We conducted a multicenter, double-blind, controlled, household-randomized trial of hydroxychloroquine PEP among close contacts of persons with diagnosed SARS-CoV-2 infection with the primary outcome of incident SARS-CoV-2 infection ascertained by polymerase chain reaction (PCR) assay.
Methods
Study Design
The trial was conducted by 7 institutions in the United States, as described elsewhere (18). The study was designed in March 2020, when comparably less was known about SARS-CoV-2 transmission. The initial sample size was based on an attack rate of 6%. At the first meeting, before review of end points, the Data Safety and Monitoring Board (DSMB) recommended that the sample size be end point–driven for ease of monitoring and to be more robust to incomplete evidence around household attack rates. Thus, the design was changed to an end point–driven trial and would stop when the prespecified number of end points were observed. Participants were enrolled between 31 March and 21 August 2020 and were followed for 2 weeks to determine SARS-CoV-2 infection. The Western Institutional Review Board approved this study, with reliance agreements with the collaborating institutions. The study was registered with ClinicalTrials.gov (NCT04328961).
Setting and Participants
The study was conducted across the United States, with outreach to additional states from the 7 centers: University of Washington, Seattle; New York University; University of Maryland, Baltimore; Boston Medical Center; Tulane University; University of California, Los Angeles; and State University of New York Upstate Medical University. Participants were recruited through online advertising, including social media; referral from hospitals, providers, health departments, or persons with known SARS-CoV-2 infection; and self-referral through the study website. Social media advertising allowed recruitment to shift geographic focus with changing COVID-19 incidence and move to “hot spots” of infection. Each state was assigned to a site to receive referrals. Potential participants signed up on the study Web site, and physicians were able to refer individuals through the Web site. Study team members contacted participants to discuss the study objectives and procedures.
Participants were eligible for randomization if they were able to provide informed consent, were 18 to 80 years of age, had close contact with a person (index) with recent known SARS-CoV-2 infection, had exposure within the prior 96 hours, were able to conduct study visits via telehealth, and were not planning to take hydroxychloroquine outside the study. Participants were excluded if they had symptoms consistent with SARS-CoV-2 infection, if they were hospitalized, or if hydroxychloroquine was medically contraindicated (Supplement). Close contacts were defined as either household contacts (residing in the same residence or prolonged exposure in a confined space) of an index person diagnosed within the past 14 days or health care workers who cared for an index case without appropriate personal protective equipment (19).
Study procedures were conducted remotely via Health Insurance Portability and Accountability Act–compliant telemedicine. Before screening, all participants provided electronic informed consent, which included counseling about randomization, risks and benefits of participation, study procedures, and their rights as research participants. Potential participants completed eligibility screening with a clinician via a telemedicine visit, including timing of SARS-CoV-2 exposure (0, 1, 2, 3, or 4 day/s since most recent contact and duration of contact), risk for transmission, current symptoms assessed through standardized questions (Supplement Figure 1), and a detailed medical history. During the enrollment visit, the study clinician reviewed the study box contents and technique for specimen collection. All questionnaires were conducted by using REDCap.
Randomizations and Interventions
The study analyst generated the randomization allocation stratified by site and contact type (household versus health care–associated exposure). The study staff did not have access to the randomization codes. Once eligibility was confirmed and the enrollment visit completed, a prescription was sent to the unblinded pharmacist who accessed the randomization allocation via REDCap and dispensed the study medication. Eligible participants in the same household were randomly assigned to the same group to prevent unblinding between study participants. Households were randomly assigned in a 1:1 ratio to receive either hydroxychloroquine (400 mg/d orally for 3 days, then 200 mg/d orally for an additional 11 days) or ascorbic acid (500 mg/d orally for 3 days, then 250 mg/d orally for 11 days) as a placebo equivalent. Both hydroxychloroquine and ascorbic acid tablets were round, pale, and had a bitter or sour taste. The labeling and packaging of the drug was identical in both groups. The pharmacist was unblinded, but the participants, investigators, laboratory technicians, and study team members were blinded to participant allocation.
The dose of hydroxychloroquine was chosen based on physiologically based pharmacokinetic modeling, which identified 200 mg of hydroxychloroquine (155 mg base) administered as 2 tablets daily for 3 days followed by 1 tablet daily for 11 days as the optimal dose to achieve levels above the lung half-maximal effective concentration of 242 ng/mL (18).
Outcomes and Follow-up
Within 48 hours of enrollment, a courier delivered a study box to the participant. The study box contained study medication, swabs, capped collection tubes with phosphate buffer solution transport medium, instructions, and packing and shipping materials. Each collection tube was labeled with the study day and had a unique, scannable identification number to facilitate tracking and linkage to the PCR result. Upon study box arrival, and daily for 14 days, participants were instructed by e-mail to collect their swab; take their study medication; and complete an online questionnaire to record medication adherence, swab collection, symptoms, adverse events, and social harms (defined as physical or verbal harm related to study participation). Participants were taught how to self-collect mid-turbinate swabs and pack them for return shipping or pick-up from a local courier. The study box contained written and illustrated instructions on how to collect study specimens and pack them for return shipment. In addition, videos were available to demonstrate good technique. Once participants received their study box, they had the option of an additional telemedicine visit to review study procedures.
Medical advice and counseling were available 24 hours a day, 7 days a week from the study teams who responded daily to symptoms and social harms reported via the questionnaires. Participants were asked to complete their daily questionnaires by 2 p.m. local time each day, which included a symptom check list, open-ended questions, and an assessment of the severity of the symptom (Supplement Figure 2). If a concerning symptom or adverse event (grade 2 or worse) was reported, a flag was sent to the study team to follow up with the participant that day. Adverse events were managed and verified by the study clinician, and an adverse event form was completed and reviewed by the medical monitor. Potential causality was assessed by the study clinician and the medical monitor. Participants were followed for an additional 2 weeks and completed a day 28 exit questionnaire regarding symptoms and COVID-19 testing outside the study.
Study data were managed at the University of Washington International Clinical Research Center; site monitoring, including monitoring of randomization, was conducted by an external, independent clinical trials monitoring group.
The primary trial end point was reverse-transcription PCR (RT-PCR)–confirmed SARS-CoV-2 infection assessed via samples collected daily through day 14, among participants who were SARS-CoV-2 negative at baseline. To detect viable virus, a sensitivity end point was defined by using a lower PCR cycle threshold (Ct) cutoff of 38 (indicating higher viral load) if a target was positive to define a SARS-CoV-2–positive test. The Centers for Disease Control and Prevention (CDC) definition of symptomatic COVID-19 disease (20) assessed by using daily questionnaires through day 14 was a secondary end point. Safety was assessed through adverse event reporting.
Laboratory Methods
The RT-PCR testing was conducted by the University of Washington Virology Laboratory by using a Washington State emergency use authorized laboratory-developed test targeting the SARS-CoV-2 nucleocapsid genes N1 and N2 (21). A subset of specimens were tested for RNase P, a human DNA marker. The RT-PCR assays were performed on an ABI 7500 real-time PCR system (Applied Biosystems). An internal control amplification, either RNase P or EXO (RNA spike-in), was performed to monitor RNA extraction and RT-PCR quality. Specimens were considered positive if either or both the N1 and N2 targets were detected and the Ct, a semiquantitative measure of viral load, was 40 or less, consistent with the criteria for clinical diagnosis.
Statistical Analysis
Initial sample size calculations were based on a binary outcome of incident SARS-CoV-2 in the first 2 weeks after initiation of the intervention. Assuming 80% power to detect a 50% reduction in incident SARS-CoV-2, with a 2-sided α value of 0.05, a 10% loss to follow-up, and an attack rate of 6%, a sample size of 2000 was initially planned, which would have been expected to yield 81 infections. Before end point data were assessed, the sample size was recalculated by using an event-driven design to allow use of all observed data at interim analyses and not just data from participants who had completed follow-up. In addition, the event-driven design is more robust to assumptions about the overall event rate, preventing the need for redesign after observing end point data. In the redesign, power was increased to 90% and the design assumptions then anticipated 93 required end points. At that time, published data suggested household attack rates of 10% in the absence of intervention; therefore, we planned to enroll 1240 participants, acknowledging that the overall final number of enrolled participants could be much lower or much higher than 1240 depending on the overall attack rate.
We used a Cox proportional hazards model to estimate the adjusted hazard ratio (aHR) of the intervention versus control for the primary, secondary, and sensitivity efficacy end points. Models for all end points were stratified by study site and type of contact (household member versus health care worker) and, per U.S. Food and Drug Administration guidance on SARS-CoV-2 prevention studies, included adjustment for baseline variables (sex at birth, age, and quarantine status) to increase precision (22) (Supplement Table 1). The analysis for the secondary end point of symptomatic COVID-19 included additional covariates: metabolic disease and weight. The secondary analysis for day 28 outcomes included the day 28 SARS-CoV-2 PCR result and reported positive SARS-CoV-2 tests between day 1 and 28. End point time was set at the midpoint between the last negative and first positive assessments. Participants who did not reach the efficacy end points were censored at the last day when data were collected and did not meet the corresponding outcome definition. Corresponding 95% CIs and Wald test statistics were calculated by using robust SEs from the sandwich estimator to account for correlation (23) from multiple participants within a household. Cumulative incidence was calculated by using the Kaplan–Meier method, with 95% CIs computed by using robust SEs (23). Efficacy and sensitivity analyses were performed on a modified intention-to-treat (mITT) cohort of participants who were confirmed to be SARS-CoV-2 PCR-negative at baseline. Subgroup sensitivity analyses explored whether the efficacy of hydroxychloroquine varied with timing of exposure and starting PEP and household characteristics. Participants with missing covariate or subgroup defining data were excluded from the secondary analyses. The efficacy analysis was conducted on the intention-to-treat (ITT) cohort as a sensitivity analysis.
The safety analyses were conducted on the ITT cohort. Participants experiencing a safety event were compared between the 2 arms by using the Fisher exact test. We performed all analyses by using R, version 4.0.
An independent DSMB was constituted to review study progress, participant safety, and the primary outcome. Four interim analyses were planned. Stopping guidelines used O'Brien–Fleming boundaries for the primary outcome, with DSMB reviews for both efficacy and futility (24). The study was projected to reach the targeted number of end points before the second planned DSMB interim review on 21 August 2020, rendering an interim analysis unnecessary.
Role of the Funding Source
The study was funded by the Bill & Melinda Gates Foundation through the COVID-19 Therapeutics Accelerator and the University of Washington King K. Holmes Endowed Professorship in STDs and AIDS. Hydroxychloroquine for the study was donated by Sandoz. The funders had no role in study design; data collection, analysis, and interpretation; writing of the report; or in the decision to submit for publication. The corresponding author had full access to all study data and had final responsibility for the decision to submit for publication.
Results
Participants
Between 31 March 2020 and 21 August 2020, 943 participants were screened for study eligibility and 829 (88%) were enrolled (Figure 1) from 41 states (Supplement Figure 3). Of the 114 people who were ineligible for randomization, 18 (16%) had symptoms consistent with COVID-19; 14 (12%) had 96 or more hours since exposure; 11 (10%) had health conditions that excluded participation; and 71 (62%) met other exclusion criteria, including lack of consent. A total of 671 households (comprising 829 participants) were randomly assigned: 337 (407 participants) to the hydroxychloroquine group and 334 (422 participants) to the control group. When health care workers (n = 136) were excluded, the number of household contacts enrolled ranged from 1 to 11 per household, with 81% having 1 contact (Supplement Tables 2 and 3). Participants who tested SARS-CoV-2 positive at baseline (83 of 829 [10%]) or for whom a baseline result was not available (57 of 829 [7%]) were excluded from the mITT primary analysis (Supplement Table 4), which left 689 participants: 353 in the hydroxychloroquine group and 336 in the control group. RNase P was detected in more than 99% (1335 of 1347) of specimens tested.
Figure 1. Study flow diagram.
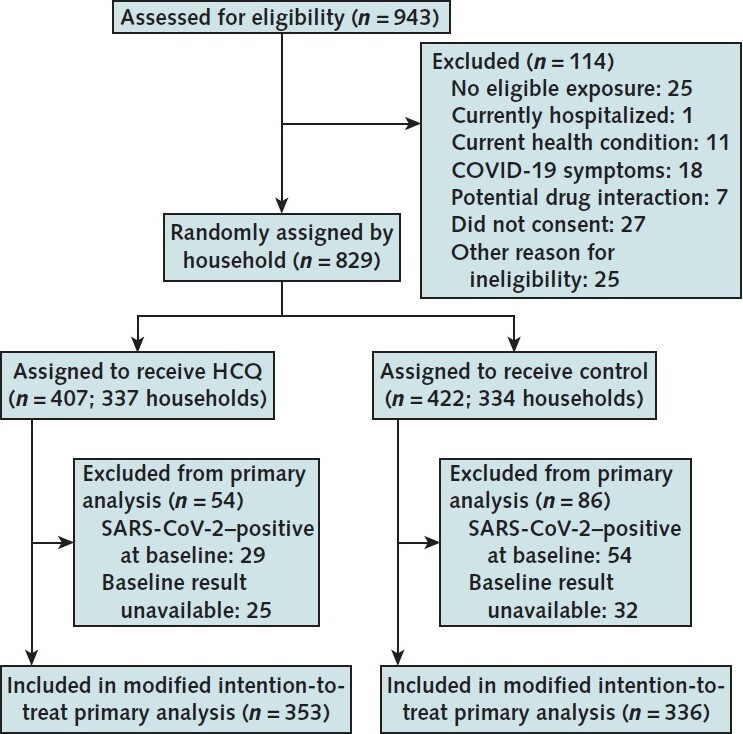
HCQ = hydroxychloroquine; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
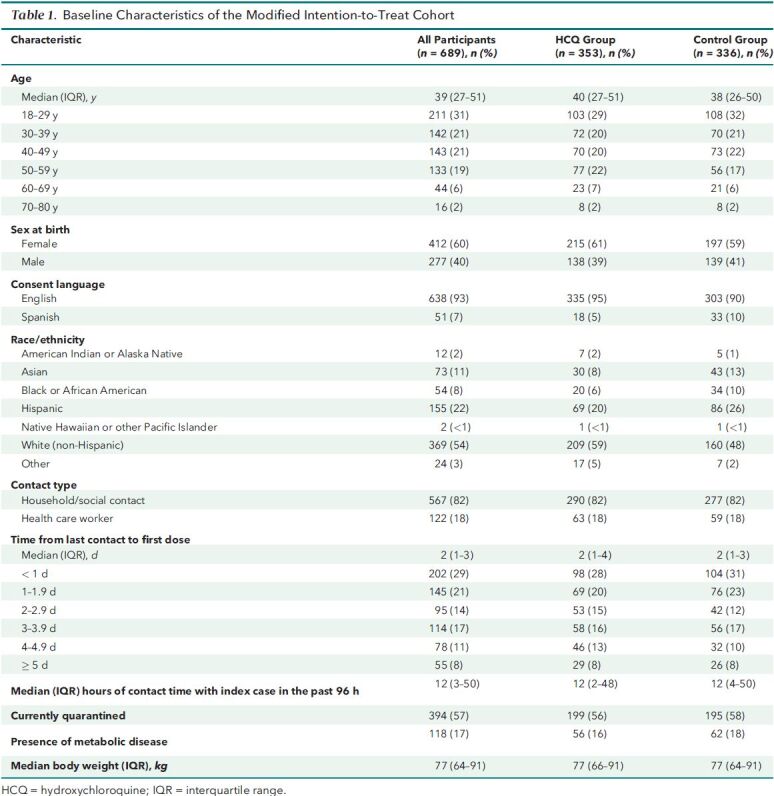
For the 689 participants in the primary mITT analysis, the median age was 39 years (interquartile range [IQR], 27 to 51 years) and 412 (60%) were female (Table 1). In addition, 567 (82%) were household or close contacts of an index case and 122 (18%) were exposed health care workers. The median number of self-reported hours of contact with the index case in the past 96 hours was 12 (IQR, 3 to 50 hours). The median time between the most recent exposure and first dose of study medication was 2 days (IQR, 1 to 3 days). Each day, over 90% of participants completed their symptom questionnaire surveys and collected follow-up swabs (Supplement Figures 4 to 7 and Supplement Tables 5 to 8). Self-reported adherence to study medication was 94% to 82% (day 1 to 14) (Supplement Figures 8 and 9 and Supplement Tables 9 and 10).
Table 1. Baseline Characteristics of the Modified Intention-to-Treat Cohort.
Primary Outcome
A total of 98 SARS-CoV-2 infections were detected in the first 14 days of follow-up among participants who were negative at baseline, for an overall cumulative incidence of 14.3% (95% CI, 11.5% to 17.0%). Overall, there were 53 SARS-CoV-2 acquisition events in the hydroxychloroquine group and 45 events the control group (aHR, 1.10 [CI, 0.73 to 1.66]; P > 0.20) (Table 2 and Figure 2). In preplanned analyses, aHRs were not significant within subgroup for type of contact, time between most recent contact and first dose of study medication, duration of contact, number of contacts enrolled within the household, quarantine status, index symptoms, and number of adults or children in the household (Supplement Figure 10). A sensitivity analysis using a PCR Ct value of 38 or less revealed 48 SARS-CoV-2 acquisition events in the hydroxychloroquine group and 36 events in the control group (aHR, 1.26 [CI, 0.81 to 1.95]; P > 0.20). In the preplanned secondary analysis including infections up to day 28, there were 58 cases in the hydroxychloroquine group and 48 cases in the control group (aHR, 1.16 [CI, 0.77 to 1.73]; P > 0.20) (Table 2). Among the 98 participants with incident PCR-confirmed SARS-CoV-2 infection, 63 (64%) met the CDC-defined criteria for symptomatic COVID-19, for a cumulative COVID-19 incidence of 9.2% (CI, 6.9% to 11.4%) at day 14. In that subset, there were 37 COVID-19 diagnoses in the hydroxychloroquine group and 26 in the control group (aHR, 1.38 [CI, 0.82 to 2.33]; P > 0.20). In the ITT analysis cohort, the overall cumulative incidence of SARS-CoV-2 was 23.3% (CI, 19.6 to 26.8). There were 82 SARS-CoV-2 acquisition events in the hydroxychloroquine group and 99 events in the control group (aHR, 0.81 [CI, 0.57 to 1.14]; P > 0.20) (Supplement Figure 11 and Supplement Table 11). In a post hoc sensitivity analysis that excluded participants in households where any contact tested SARS-CoV-2 positive at baseline, there were 50 SARS-CoV-2 acquisition events in the hydroxychloroquine group and 38 events in the control group (aHR, 1.20 [CI, 0.78 to 1.84]; P > 0.20) (Supplement Figure 12 and Supplement Table 12).
Table 2. Cumulative Incidence and Hazard Ratios of Reverse-Transcription Polymerase Chain Reaction–Confirmed SARS-CoV-2 Infection and COVID-19.
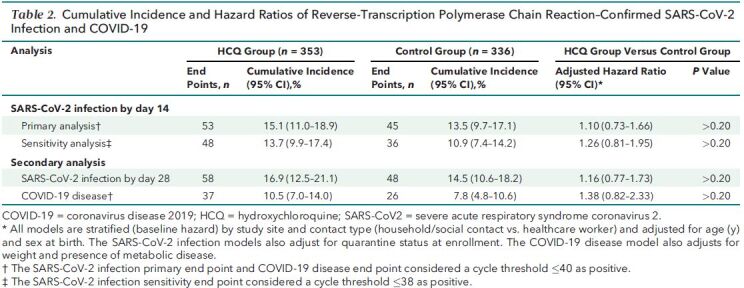
Figure 2. Cumulative incidence of SARS-CoV-2.
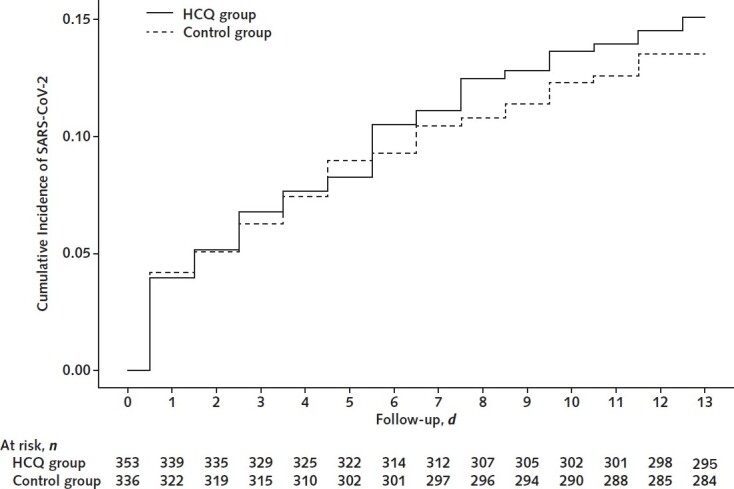
HCQ = hydroxychloroquine; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Safety
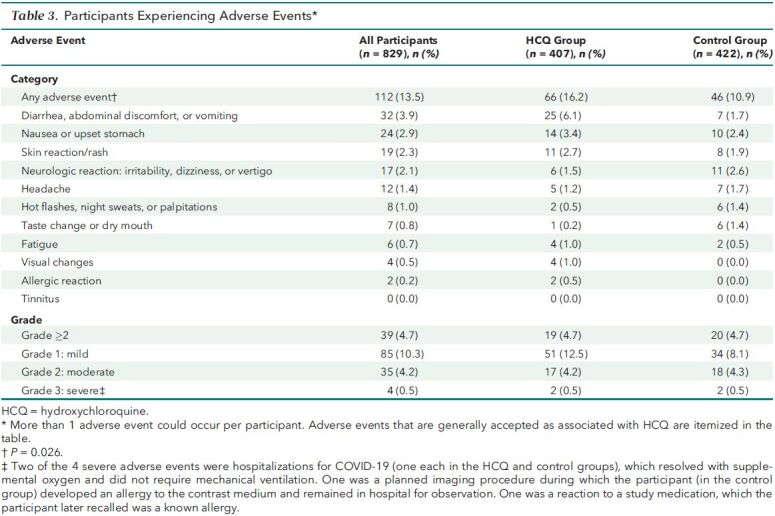
There were 112 participants in the ITT cohort who experienced adverse events consistent with known side effects of hydroxychloroquine, which included gastrointestinal symptoms and rash. Overall, the frequency was higher in the hydroxychloroquine group than in the control group (66 [16.2%] versus 46 [10.9%], respectively; P = 0.026) (Table 3). Three of 829 participants (0.4%) experienced serious adverse events that were assessed as not related to study medication, and 1 participant experienced a severe adverse event that was assessed as related to a study medication. Overall, 39 participants (4.7%) had grade 2 or higher adverse events: 4.7% (19 of 407) in the hydroxychloroquine group and 4.7% (20 of 422) in the control group. Social harms due to lack of social support for trial participation were reported by 18 participants (2.2%).
Table 3. Participants Experiencing Adverse Events*.
Discussion
In this randomized, double-blind, controlled trial conducted across multiple sites in the United States, SARS-CoV-2 incidence among close contacts of persons with confirmed SARS-CoV-2 infection was high—almost 15% over 14 days—and was similar between those receiving hydroxychloroquine and those receiving control medication. We used a rigorous design, assessed eligibility for PEP on the basis of exposure to recently diagnosed index cases, conducted baseline SARS-CoV-2 PCR testing of enrolled participants and daily PCR testing to ascertain the primary end point of incident SARS-CoV-2, and had high retention of participants, and the study was sufficiently powered to detect a clinically important prevention effect of hydroxychloroquine. The lack of effect shown in this study builds on other recent data (25, 26) and provides strong evidence against the use of hydroxychloroquine for SARS-CoV-2 PEP.
We hypothesized that hydroxychloroquine would decrease SARS-CoV-2 acquisition, on the basis of observational evidence (16, 17) and in vitro data in Vero cells (14, 15) that were not replicated later in human lung cells (27). Two other randomized trials recently tested hydroxychloroquine for PEP and also found no effect, but these trials had significant limitations. One study did not assess SARS-CoV-2 status at baseline and relied primarily on self-report of flulike illness for the primary trial end points, rather than an objective virologic end point (25). A second trial used an unblinded, uncontrolled design; did infrequent PCR testing for incident infection until day 14; and was underpowered to assess incident infection (26). Yet, frequent testing is needed to detect transient infections. We provide robust evidence based on a well-powered study with a biological end point among persons confirmed to be SARS-CoV-2 negative at baseline. In addition, a clinical trial assessing the efficacy of hydroxychloroquine as preexposure prophylaxis among health care workers did not find a clinical benefit of 8 weeks of study drug administration (28).
Household contacts and health care workers are a priority population for SARS-CoV-2 prevention. Although social distancing and use of personal protective equipment prevent some infections, it is challenging to follow these guidelines in many circumstances (for example, when providing emergency care). As we observed, even when the risk for exposure is known, SARS-CoV-2 incidence can be high—14% over 14 days in our study, on top of 10% who were infected at baseline, for a total cumulative incidence of over 23%. Once an efficacious intervention for PEP is identified, implementation science will need to evaluate strategies for timely delivery for prevention of SARS-CoV-2 infection and a suite of strategies will be needed, including PEP; potentially preexposure prophylaxis; early treatment; and, ideally, vaccination.
Strengths of our study include the household-randomized, double-blind, controlled design. Remote clinical trial infrastructure (including recruitment via social media, telemedicine visits, electronic consent, participant-collected specimens, and electronic questionnaires) allowed safe conduct of a clinical trial during a pandemic while limiting in-person visits and conserving space, personnel, and resources for necessary clinical care. In addition, the trial successfully identified and enrolled persons at risk for SARS-CoV-2 infection who subsequently demonstrated high incidence and were successfully retained in both randomized groups. This experience of remote clinical trial conduct provided lessons learned regarding the utility of telemedicine combined with participant-collected specimens which could be applied to other clinical investigations. Electronic consent and telemedicine were critical components of the study operations, and changes in guidance facilitating telemedicine across state lines were key for success. These changes would simplify clinical trials in the future and increase the geographic area covered as participants are not required to travel for study visits. The study primary aim was measured by detection of SARS-CoV-2 by RT-PCR, minimizing statistical noise from nonspecific respiratory symptoms that may be due to another cause.
Limitations of the study include the average of a 2-day window between most recent exposure and initiation of study medication owing to remote recruitment and shipping times; PEP should be given as soon as possible after exposure to prevent infection. Delays in index testing and receipt of results meant that some index cases may have had infection for several days before the enrollment of their close contacts into this trial, during which time transmission could occur. Among all enrolled participants, 10% tested SARS-CoV-2 positive at baseline; however, the primary analysis was conducted only among persons who were SARS-CoV-2 negative at baseline.
Although we had biological confirmation of incident cases, we did not test the viability of SARS-CoV-2 via culture or subgenomic RNA analysis to assess markers of active replication and thus onward transmission (29). As techniques emerge to assess SARS-CoV-2 viability, characterizing viral and host factors related to infectiousness and susceptibility could help identify strategies to decrease SARS-CoV-2 transmission. With tests of viral viability new trials for PEP may be warranted.
Several reasons may explain why we found no efficacy of hydroxychloroquine for prevention of SARS-CoV-2 infection. First, the repurposed agent may have been the wrong choice of medication or used at an insufficient dose, even though pharmacokinetic modeling was used to choose the dose (18). In addition, self-reported adherence was uniformly high, but lack of adherence can always be a potential explanation for lack of effect in a clinical trial. Finally, the sample size may not have been adequate to exclude small but clinically meaningful decreases in infection, and, in all trials, chance may play a role in the outcome. However, on the basis of our data and that of others (25, 26), the conclusion that this drug is ineffective for SARS-CoV-2 prevention is most reasonable.
Even if highly effective and safe vaccines are identified (30), individuals exposed shortly before or after vaccination may not receive protection because of the time required to develop protective antibodies after immunization, making PEP a complementary intervention for COVID-19 prevention. Ongoing studies for SARS-CoV-2 PEP are evaluating repurposed biomedical interventions, including lopinavir–ritonavir and nitazoxanide (31–33), and passive immunization with anti-SARS-CoV-2 convalescent plasma (34) or SARS-CoV-2–specific antispike monoclonal antibodies (35–37). If safe and effective postexposure interventions are identified, they could decrease SARS-CoV-2 incidence, interrupt community transmission, and play a pivotal role in controlling the COVID-19 pandemic.
Supplementary Material
Footnotes
This article was published at Annals.org on 8 December 2020
* For members of the Hydroxychloroquine COVID-19 PEP Study Team, see the Supplement (available at Annals.org).
References
- 1. Dong E , Du H , Gardner L . An interactive web-based dashboard to track COVID-19 in real time [Letter]. Lancet Infect Dis. 2020;20:533-534. [PMID: ] doi: 10.1016/S1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wu Z , McGoogan JM . Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72?314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239-1242. [PMID: ] doi: 10.1001/jama.2020.2648 [DOI] [PubMed] [Google Scholar]
- 3. World Health Organization. Transmission of SARS-CoV-2: implications for infection prevention precautions. 9 July 2020. Accessed at www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions on 24 August 2020.
- 4. Oran DP , Topol EJ . Prevalence of asymptomatic SARS-CoV-2 infection. A narrative review. Ann Intern Med. 2020;173:362-367. doi: 10.7326/M20-3012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Madewell ZJ , Yang Y , Longini IM , et al. Household transmission of SARS-CoV-2: a systematic review and meta-analysis of secondary attack rate. med. Rxiv. 2020. [PMID: ] doi: 10.1101/2020.07.29.20164590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Drake TM , Docherty AB , Weiser TG , et al. The effects of physical distancing on population mobility during the COVID-19 pandemic in the UK. Lancet Digit Health. 2020;2:e385-e387. [PMID: ] doi: 10.1016/S2589-7500(20)30134-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Gudbjartsson DF , Helgason A , Jonsson H , et al. Spread of SARS-CoV-2 in the Icelandic population. N Engl J Med. 2020;382:2302-2315. [PMID: ] doi: 10.1056/NEJMoa2006100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19): how to protect yourself & others. Accessed at www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html on 24 August 2020.
- 9. Mitjà O , Clotet B . Use of antiviral drugs to reduce COVID-19 transmission [Letter]. Lancet Glob Health. 2020;8:e639-e640. [PMID: ] doi: 10.1016/S2214-109X(20)30114-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Gentile I , Maraolo AE , Piscitelli P , et al. COVID-19: time for post-exposure prophylaxis. Int J Environ Res Public Health. 2020;17. [PMID: ] doi: 10.3390/ijerph17113997 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Welliver R , Monto AS , Carewicz O , et al; Oseltamivir Post Exposure Prophylaxis Investigator Group. Effectiveness of oseltamivir in preventing influenza in household contacts: a randomized controlled trial. JAMA. 2001;285:748-54. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 12. Ikematsu H , Hayden FG , Kawaguchi K , et al. Baloxavir marboxil for prophylaxis against influenza in household contacts. N Engl J Med. 2020;383:309-320. [PMID: ] doi: 10.1056/NEJMoa1915341 [DOI] [PubMed] [Google Scholar]
- 13. Rolain JM , Colson P , Raoult D . Recycling of chloroquine and its hydroxyl analogue to face bacterial, fungal and viral infections in the 21st century. Int J Antimicrob Agents. 2007;30:297-308. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Wang M , Cao R , Zhang L , et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro [Letter]. Cell Res. 2020;30:269-271. [PMID: ] doi: 10.1038/s41422-020-0282-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Yao X , Ye F , Zhang M , et al. In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 2020;71:732-739. [PMID: ] doi: 10.1093/cid/ciaa237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Ferreira A , Oliveira-E-Silva A , Bettencourt P . Chronic treatment with hydroxychloroquine and SARS-CoV-2 infection. J Med Virol. 2020. [PMID: ] doi: 10.1002/jmv.26286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Lee SH , Son H , Peck KR . Can post-exposure prophylaxis for COVID-19 be considered as an outbreak response strategy in long-term care hospitals. Int J Antimicrob Agents. 2020;55:105988. [PMID: ] doi: 10.1016/j.ijantimicag.2020.105988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Barnabas RV , Brown E , Bershteyn A , et al; Hydroxychloroquine COVID-19 PEP Study Team. Efficacy of hydroxychloroquine for post-exposure prophylaxis to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among adults exposed to coronavirus disease (COVID-19): a structured summary of a study protocol for a randomised controlled trial [Letter]. Trials. 2020;21:475. [PMID: ] doi: 10.1186/s13063-020-04446-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Centers for Disease Control and Prevention. Using personal protective equipment (PPE). 9 June 2020. Accessed at www.cdc.gov/coronavirus/2019-ncov/hcp/using-ppe.html on 24 August 2020.
- 20. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19) 2020 interim case definition, approved April 5, 2020. Accessed at wwwn.cdc.gov/nndss/conditions/coronavirus-disease-2019-covid-19/case-definition/2020 on 26 August 2020.
- 21. Lieberman JA , Pepper G , Naccache SN , et al. Comparison of commercially available and laboratory-developed assays for in vitro detection of SARS-CoV-2 in clinical laboratories. J Clin Microbiol. 2020;58. [PMID: ] doi: 10.1128/JCM.00821-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. U.S. Department of Health and Human Services; Food and Drug Administration; Center for Drug Evaluation and Research (CDER); Center for Biologics Evaluation and Research (CBER). COVID-19: developing drugs and biological products for treatment or prevention: guidance for industry. May 2020. Accessed at www.fda.gov/media/137926/download on 27 August 2020.
- 23. Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. Springer; 2000.
- 24. O'Brien PC , Fleming TR . A multiple testing procedure for clinical trials. Biometrics. 1979;35:549-56. [PMID: ] [PubMed] [Google Scholar]
- 25. Boulware DR , Pullen MF , Bangdiwala AS , et al. A randomized trial of hydroxychloroquine as postexposure prophylaxis for covid-19. N Engl J Med. 2020;383:517-525. [PMID: ] doi: 10.1056/NEJMoa2016638 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Mitja O, Ubals M, Corbacho M, et al. A cluster-randomized trial of hydroxychloroquine as prevention of Covid-19 transmission and disease. medRxiv. Preprint posted online 26 July 2020. doi:10.1101/2020.07.20.20157651
- 27. Hoffmann M , Mösbauer K , Hofmann-Winkler H , et al. Chloroquine does not inhibit infection of human lung cells with SARS-CoV-2. Nature. 2020;585:588-590. [PMID: ] doi: 10.1038/s41586-020-2575-3 [DOI] [PubMed] [Google Scholar]
- 28. Abella BS , Jolkovsky EL , Biney BT , et al; and the Prevention and Treatment of COVID-19 With Hydroxychloroquine (PATCH) Investigators. Efficacy and safety of hydroxychloroquine vs placebo for pre-exposure SARS-CoV-2 prophylaxis among health care workers: a randomized clinical trial. JAMA Intern Med. 2020. [PMID: ] doi: 10.1001/jamainternmed.2020.6319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Perera RAPM , Tso E , Tsang OTY , et al. SARS-CoV-2 virus culture and subgenomic RNA for respiratory specimens from patients with mild coronavirus disease. Emerg Infect Dis. 2020;26:2701-2704. [PMID: ] doi: 10.3201/eid2611.203219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Bar-Zeev N , Moss WJ . Encouraging results from phase 1/2 COVID-19 vaccine trials. Lancet. 2020;396:448-449. [PMID: ] doi: 10.1016/S0140-6736(20)31611-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.COVID-19 ring-based prevention trial with lopinavir/ritonavir (CORIPREV-LR). ClinicalTrials.gov. Accessed at https://clinicaltrials.gov/ct2/show/NCT04321174 on 26 August 2020.
- 32.Efficacy and safety of nitazoxanide for post exposure prophylaxis of COVID-19. ClinicalTrials.gov. Accessed at https://clinicaltrials.gov/ct2/show/NCT04435314 on 26 August 2020.
- 33.Measles vaccine in HCW (MV-COVID19). ClinicalTrials.gov. Accessed at https://clinicaltrials.gov/ct2/show/NCT04357028 on 30 August 2020.
- 34.Convalescent plasma for COVID-19 close contacts. ClinicalTrials.gov. Accessed at https://clinicaltrials.gov/ct2/show/NCT04390503 on 30 August 2020.
- 35. Baum A , Fulton BO , Wloga E , et al. Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies. Science. 2020;369:1014-1018. [PMID: ] doi: 10.1126/science.abd0831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Hansen J , Baum A , Pascal KE , et al. Studies in humanized mice and convalescent humans yield a SARS-CoV-2 antibody cocktail. Science. 2020;369:1010-1014. [PMID: ] doi: 10.1126/science.abd0827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Study assessing the efficacy and safety of anti-spike SARS CoV-2 monoclonal antibodies for prevention of SARS CoV-2 infection asymptomatic in healthy adults who are household contacts to an individual with a positive SARS-CoV-2 RT-PCR assay. ClinicalTrials.gov. Accessed at https://clinicaltrials.gov/ct2/show/NCT04452318 on 30 August 2020.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.