

Abstract
Introduction:
Studies have shown that pneumococcal disease significantly increases morbidity and mortality rates in children 5 years old and under. These infections constitute the main cause of preventable deaths in the world, considering the availability of vaccination. Considering that Ecuador is in a high incidence region, despite the introduction of the vaccine, this study aims to describe the burden of hospitalized pneumococcal disease and related mortality in our country between 2005 and 2015, to help decision-making processes for the health authorities.
Methods:
This cross-sectional study analyzes morbidity, mortality, and the situation in Ecuador caused by pneumococcal disease in children 5 years old and under between 2005 and 2015 using national databases.
Results:
A total of 163,852 cases of children 5 years old and under were reported to have been hospitalized due to pneumococcal-related diseases. Males comprised 54.7% of the cases and females 45.3%. In 36% of the cases, the patients were 1 year old or under. The mortality rate due to pneumococcal disease in Ecuador in children aged 5 and under decreased in 48% during 2005–2015.
Conclusion:
The decrease in mortality can be related to the introduction of the vaccine and an increase in access to health care by the general population in the country. It is important to study the specific impact of the vaccine in the reduction of morbidity and mortality of children in Ecuador.
Keywords: Child health, infectious diseases, pneumococcal disease, public health, Streptococcus pneumoniae
INTRODUCTION
Streptococcus pneumoniae (S. pneumoniae) is a Gram-positive bacterium that causes a variety of clinical syndromes, including pneumonia, meningitis, bacteremia, acute otitis media, and sinusitis.[1]
There are 14.5 million cases reported of serious pneumococcal diseases in the world per year, leading to approximately 826,000 deaths.[2] In Latin America and the Caribbean, there is an estimated 12,000–28,000 deaths per year due to pneumococcal diseases, as well as 182,000 hospitalizations and 1.4 million outpatient appointments.[3] Studies have shown that pneumococcal disease significantly increases morbidity and mortality rates in children 5 years old and under. These infections constitute the main cause of preventable deaths in the world, considering the availability of vaccination.[4] Children under age 1 and older adults seem to be the most affected population.
Currently, all the countries in the Latin American region, including Ecuador, have introduced a pneumococcal conjugate vaccine in their immunization programs.[5] Considering that Ecuador is in a high incidence region, despite the introduction of the vaccine, this study aims to describe the burden of hospitalized pneumococcal disease and related mortality in our country between 2005 and 2015, to help decision-making processes for the health authorities.
METHODS
Study design
This cross-sectional study analyzes morbidity, mortality, and the situation in Ecuador caused by pneumococcal disease in children 5 years old and under between 2005 and 2015.
Data sources
The study uses secondary data from the National Registry of Hospital Discharges and the National Registry of Deaths.[6,7] These databases register all the hospital discharges and deaths in the country at both public and private health establishments. Every establishment that forms part of the National Health System reports the information on hospital discharges and deaths to the National Institute of Census and Statistics. This institution is responsible for the validation of the information and further publication.
The other source of data used in this study is SIREVA II database from the Pan American Health Organization.[8] They identified the need to collect data on pneumonia and bacterial meningitis in 1993 and created a regional program to gather information from sentinel hospitals in Latin American countries. Ecuador reported information starting in 2000, but with diverse forms of registration. Starting in 2009, uniform data reports are obtained from sentinel hospitals identifying the cases in children 5 years old and under.
Population
For this study, we selected all children between 0 and 5 years old in the National Registry of Hospital Discharges between 2005 and 2015, whose main cause of hospitalization was any of the ICD-10 codes related to pneumococcal infections (A40, G00–G03, and J12–J18). The selected ICD-10 codes are used in studies worldwide that evaluate the impact of pneumococcal disease based on secondary data.[9] We replicated this classification to make our study comparable to global results. Considering S. pneumoniae is the main cause of lower respiratory tract infections, we included all the codes related to such.[10] We excluded otitis media and sinusitis diagnoses, considering that these diseases are not registered in hospital databases due to their management in primary care. The variables included from this registry are age, sex, place of residence, type of health establishment, length of hospital stay, and year and code of diagnosis. These variables allow us to define the frequency and characteristics of pneumococcal infections in the country.
Every case was defined by clinical diagnosis. Most cases are confirmed with image tests and only a few are confirmed by laboratory tests.
Inclusion criteria
Diagnosis of any of the following ICD-10 codes: A40, G00–G03, and J12–J18
Children up to 5 years of age.
Exclusion criteria
Any other ICD-10 code that is not A40, G00–G03, and J12–J18
People over 5 years of age.
From the National Registry of Deaths, we included all the children who died between 2005 and 2015 from age 0 to 5, whose main cause of death was coded as one of the ICD-10 categories related to pneumococcal disease described above. The variables included from these registries are cause of death, age, and sex.
From the SIREVA II database, we obtained the number of cases of S. pneumoniae in the sentinel hospitals included each year and the characteristics of the most frequently found serotypes in sentinel hospitals. All clinically diagnosed cases in the sentinel hospitals are further tested by laboratory to proceed to strain serotyping.
Statistical analysis
We performed a descriptive analysis of qualitative and quantitative variables related to morbidity and mortality. Quantitative and qualitative results are presented through frequency distributions, proportions, rates, and measures of central tendency and of dispersion. Mortality data allowed us to calculate the mortality rate due to pneumococcal infection of children in the country.
For the statistical analysis, we used Stata Version 14 from StataCorp LLC Texas-USA and Microsoft Excel version 16.32 (Product ID: 02954-015-045044).
Bioethical considerations
All the information came from secondary data. In Ecuador, the use of public databases with secondary data does not require approval by any ethics committee. The database is properly anonymized before its use.
RESULTS
In Ecuador, there was an average of 1,867,961 children of age 5 and under between 2005 and 2015. Out of these, around 918,301 (49.2%) were 1 year old or under.
Morbidity
During a 10-year study period, a total of 163,852 cases of children 5 and under were reported to have been hospitalized due to pneumococcal-related diseases. Males comprised 54.7% of the cases and females 45.3%. In 36% (67,288) of the cases, the patients were 1 year old or under, 20% (37,282) were 2 years old, 13.2% (24,742) were 3 years old, 10.2% (19,220) were 4 years old, and 8.2% (15,320) were 5 years old.
The patient's residence is registered according to the province the child comes from. In most cases, they come from Guayas and Pichincha, provinces that include the capital of the country and the biggest city. These are followed by Azuay, Chimborazo, and Cotopaxi which are part of the mountainous region and El Oro from the coastal region.
The child's diagnosis was classified using the ICD-10 codes [Table 1]. The most frequent reason reported for hospitalization corresponded to “diseases of the respiratory system” (J12–J18). In this category, the most relevant cause of morbidity in these children was due to unspecified pneumonia (J18) in 89.1% of the cases. This was followed by less frequent diseases such as bacterial pneumonia (7%) and viral pneumonia (2%). The remaining 1% adds up between the other “diseases of the respiratory system” (A40, G00–G03). The categories that represent “other diseases” and “inflammatory diseases of the central nervous system” only represent 1% of the cases.
Table 1.
Frequency of Pneumococcal Diseases. Original table
| Pneumococcal Diseases | Number of cases | Percentage |
|---|---|---|
| Pneumonia (J12-J18) | 162,481 | 99.16% |
| Meningitis (A40) | 44 | 0.02% |
| Sepsis (G00-G03) | 1327 | 0.82% |
The tendency of coding for ICD-10 diagnoses of pneumonia between 2005 and 2015 is shown in Figure 1.
Figure 1.
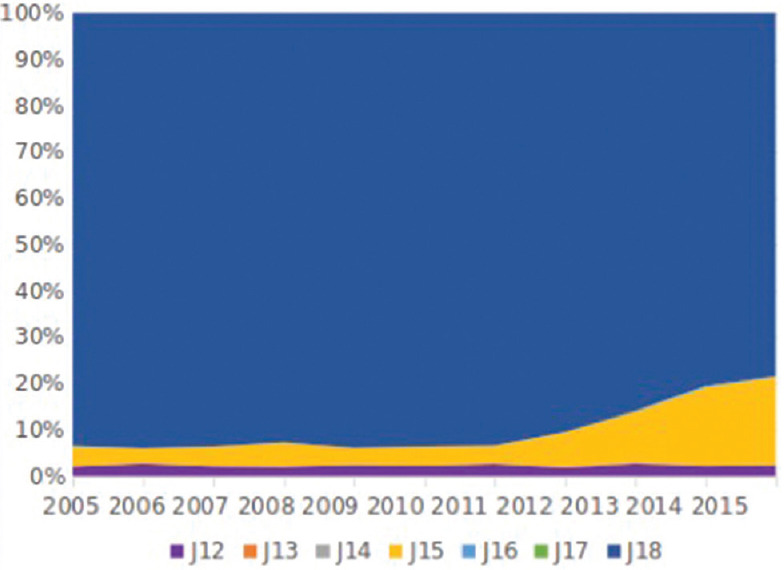
Tendency of ICD-10 coding for pneumonia
When analyzing the frequency of disease in the different years between 2005 and 2015, we can see a range that goes from as low as 9035 cases in 2005 (5.5% of total cases in the 10-year period) to 18,502 in 2013 (11.3% of total cases in the 10-year period) as seen in Figure 2.
Figure 2.
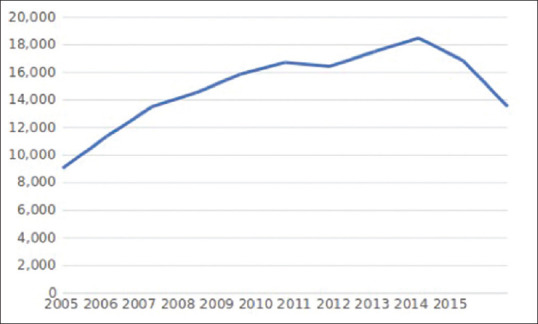
Number of cases of hospitalization due to pneumococcal disease per year
The median amount of days of stay in the hospital was 60.4 days. These hospitalizations were in health establishments classified into categories by the type of establishment. The public health system in Ecuador attends the health needs of 81.9% of the population. In this case, general hospitals (hospitals of reference with attention to multiple specialties) received 33.8% of cases, pediatric hospitals 24.6%, basic hospitals 23.5%, private clinics 10.5%, and the rest of the cases were distributed among other types of establishments. These health establishments were mostly in the provinces of Azuay, Guayas, and Pichincha, all of which contain the most populated cities in the country.
Mortality
The total amount of deaths due to pneumococcal-related infections among children five and under during the study period was 4874. The frequency per year has constantly decreased among the years [Figure 3]. From 2005 until 2015, there was a 48% decrease, going from 583 to 280 cases per year.
Figure 3.

Number of deaths due to pneumococcal disease per year
When analyzing deaths for all the children 5 and under, 54% happened in males and 46% in females [Table 2]. We can see that 2830 (58%) cases of death were among children under the age of 1 and 1915 (42%) cases between 1 and 5 years of age.
Table 2.
Mortality Rate Due to Pneumococcal Diseases Per Year. Original table
| Year | Mortality Rate ≤5 |
Mortality rate <1 |
Mortality rate 1-4 |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | Total | Male | Female | |
| 2005 | 34.6 | 38.0 | 31.2 | 113.0 | 123.7 | 102.2 | 20.8 | 22.8 | 18.7 |
| 2006 | 36.3 | 41.7 | 30.9 | 125.8 | 147.7 | 103.9 | 20.7 | 23.0 | 18.3 |
| 2007 | 30.8 | 31.9 | 29.6 | 111.8 | 116.7 | 106.9 | 15.9 | 16.3 | 15.5 |
| 2008 | 33.6 | 37.1 | 30.2 | 117.6 | 133.0 | 102.1 | 18.4 | 19.1 | 17.6 |
| 2009 | 28.9 | 31.2 | 26.5 | 97.5 | 113.4 | 81.5 | 16.5 | 15.9 | 17.1 |
| 2010 | 21.2 | 22.4 | 20.0 | 72.4 | 80.4 | 64.6 | 12.7 | 13.0 | 12.3 |
| 2011 | 18.0 | 18.9 | 17.2 | 58.2 | 62.3 | 54.2 | 11.4 | 11.6 | 11.3 |
| 2012 | 19.2 | 20.5 | 18.0 | 64.3 | 70.3 | 58.5 | 11.7 | 12.2 | 11.1 |
| 2013 | 16.0 | 16.9 | 15.1 | 53.3 | 53.2 | 53.4 | 10.3 | 11.6 | 8.9 |
| 2014 | 16.2 | 18.0 | 14.5 | 59.8 | 72.0 | 47.7 | 9.0 | 8.4 | 9.7 |
| 2015 | 13.9 | 14.8 | 12.9 | 48.3 | 51.8 | 44.9 | 8.1 | 8.5 | 7.7 |
| Average | 24.4 | 26.5 | 22.4 | 83.8 | 93.1 | 74.5 | 14.1 | 14.8 | 13.5 |
The crude mortality rate has significantly decreased through the years, being the highest in 2006 and the lowest in 2015, with a decreasing tendency since 2008 [Figure 4].
Figure 4.
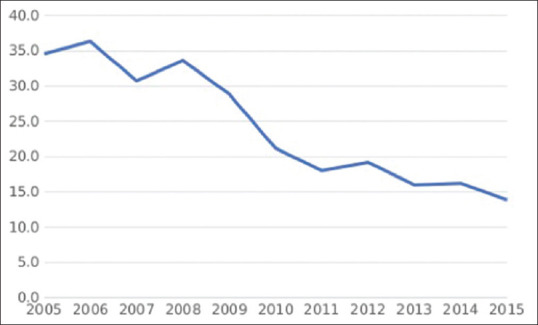
Mortality rate due to pneumococcal related infections in children 5 years old and under
Sentinel Data
The data from the SIREVA II database include the number of cases of pneumococcal diseases in sentinel hospitals in Ecuador [Table 3] and the most frequent serotypes of S. pneumoniae, which gives us an idea of the situation in our country [Table 4].
Table 3.
Number of cases of Streptococcus Pneumoniae per age group in sentinel hospitals in Ecuador. Original table
| Age Groups | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|---|---|---|
| < 12 months | 23 | 8 | 14 | 9 | 14 | 4 | 4 |
| 12-23 months | 5 | 16 | 12 | 1 | 0 | 7 | 1 |
| 24-59 months | 14 | 11 | 17 | 9 | 9 | 8 | 4 |
| Total < 5 years old | 42 | 35 | 43 | 19 | 23 | 19 | 9 |
Table 4.
Number of cases of Streptococcus pneumoniae in sentinel hospitals in Ecuador categorized by serotype. Original table
| Serotypes | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 9 | 5 | 2 | 2 | 5 | 3 | 0 | 1 | 0 | 0 | 27 |
| 3 | 1 | 0 | 0 | 4 | 0 | 1 | 1 | 1 | 1 | 1 | 10 |
| 4 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 5 | 3 | 5 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| 6A | 1 | 2 | 1 | 2 | 0 | 3 | 1 | 2 | 6 | 0 | 18 |
| 6B | 3 | 8 | 0 | 3 | 5 | 3 | 3 | 1 | 0 | 1 | 27 |
| 6C | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 9V | 2 | 0 | 1 | 4 | 4 | 1 | 0 | 0 | 0 | 0 | 12 |
| 7F | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 3 |
| 23F | 1 | 0 | 0 | 4 | 1 | 0 | 0 | 0 | 0 | 0 | 6 |
| 14 | 6 | 12 | 12 | 15 | 9 | 13 | 5 | 1 | 2 | 0 | 75 |
| 18C | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 2 |
| 19A | 1 | 1 | 0 | 2 | 5 | 7 | 3 | 6 | 4 | 2 | 31 |
| 19F | 2 | 1 | 0 | 3 | 4 | 3 | 1 | 2 | 1 | 2 | 19 |
| 10A | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 2 |
| 9L | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| 11A | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 15A | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 2 | 4 |
| 15B | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| 15C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| 19B | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| 23B | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 3 |
| 24F | 0 | 0 | 0 | 0 | 0 | 2 | 1 | 4 | 0 | 0 | 7 |
| 34 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Grupo 28 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 2 |
| Grupo 15 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| Grupo 33 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Without typification | 8 | 6 | 18 | 1 | 2 | 0 | 0 | 2 | 0 | 0 | 37 |
| Total | 38 | 41 | 36 | 42 | 35 | 43 | 19 | 23 | 19 | 9 | 305 |
The most frequent serotypes found in the sentinel hospitals in Ecuador throughout the years have been serotypes 14, 19A, 1, and 6B.
DISCUSSION
Globally, there has been a tendency toward the reduction of pneumococcal disease. The 48% decrease in mortality due to pneumococcal disease in our country from 2005 to 2015 can be compared to the 51% decrease at the global level and a 58% compared to India that evaluated the change from 2000 to 2015.[2,11] This result endorses the importance of these data for the health authorities in the country, considering the vulnerability of the affected population.
The pneumococcal conjugate vaccine (PCV) was first introduced as part of a vaccine program in Ecuador in 2010 in its PCV-7 (including strains 4, 6B, 9V, 14, 18C, 19F, and 23F) format for a few months, when it was changed to the PCV-10 (including strains 1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, and 23F) and 23F format toward the end of the same year and remains until this day. The coverage increased significantly and can be the one responsible for the decrease in mortality rate due to pneumococcal-related diseases. A systematic review that includes six countries from the region compares morbidity and mortality rates before and after introduction of the vaccine shows a significant reduction in hospitalizations and mortality in children 5 years old and under due to pneumococcal diseases.[9]
The hospitalization due to pneumonia in children 5 years old and under increased in 187% from 2000 to 2015 in low- and middle-income countries around the world, according to McAllister et al.,[12] mostly due to an increase in access to health care and not to an increase in the number of actual cases. Our study shows similar results, with an increase of 149.5% from 2005 to 2015.
The most frequent serotypes in children under 6 years old in the region are 14 and 6A/6B according to a study by Valenzuela et al.[3] These are also the most frequent serotypes reported in our study.
The most important limitation in this study is that we are assuming that all the cases registered under the ICD-10 codes defined are due to pneumococcal diseases. Similar studies and health systems that report pneumococcal disease use the cases registered under these same codes, which is one of the reasons we used these codes for the present study, besides clinical deliberation, making our results comparable to other settings.[9,13,14] Nevertheless, it is important to take into account that a percentage of the reported cases may be due to other causes.
Another limitation could be the improvement in data registration in the country throughout the last decade, which can lead to an erroneous interpretation of what seems like a higher amount of cases in the first few years included in the study.
CONCLUSION
The mortality rate due to pneumococcal disease in Ecuador in children aged 5 and under decreased in 48% during 2005–2015. This decrease can be related to the introduction of the vaccine and an increase in access to health care by the general population in the country. It is important to study the specific impact of the vaccine in the reduction of morbidity and mortality of children in Ecuador.
Research quality and ethics statement
The authors of this manuscript declare that this scientific work complies with reporting quality, formatting, and reproducibility guidelines set forth by the EQUATOR Network. The authors also attest that this clinical investigation was determined to not require the institutional review board/ethics committee review, and the corresponding protocol/approval number is not applicable. We also certify that the contents in this submission are original and that we have done a plagiarism check.
Financial support and sponsorship
The researchers did not receive additional funding for this analysis. The publication fee was financed by the Pontifical Catholic University of Ecuador.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Pneumococcal Disease | Clinical | Features | CDC. [Last accessed on 2019 Feb 21]. https://www.cdc.gov/pneumococcal/clinicians/clinical-features.html .
- 2.O'Brien KL, Wolfson LJ, Watt JP, Henkle E, Deloria-Knoll M, McCall N, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet Lond Engl. 2009;374:893–902. doi: 10.1016/S0140-6736(09)61204-6. [DOI] [PubMed] [Google Scholar]
- 3.Valenzuela MT, O'Loughlin R, De La Hoz F, Gomez E, Constenla D, Sinha A, et al. The burden of pneumococcal disease among Latin American and Caribbean children: Review of the evidence. Rev Panam Salud Publ Pan Am J Public Health. 2009;25:270–9. doi: 10.1590/s1020-49892009000300011. [DOI] [PubMed] [Google Scholar]
- 4.Chen C, Cervero Liceras F, Flasche S, Sidharta S, Yoong J, Sundaram N, et al. Effect and cost-effectiveness of pneumococcal conjugate vaccination: A global modelling analysis. Lancet Glob Health. 2019;7:e58–67. doi: 10.1016/S2214-109X(18)30422-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. [Last accessed on 2019 Jun 25];World Health Organization | Vaccine Position Papers. Available from: https://www.who.int/immunization/documents/positionpapers/en . [Google Scholar]
- 6.Censos IN de E y. Camas y Egresos Hospitalarios. Instituto Nacional de EstadÍstica y Censos. [Last accessed on 2019 Mar 28]. Available from: http://www.ecuadorencifras.gob.ec/camas-y-egresos-hospitalarios .
- 7.Censos IN de Ey. Nacimientosy Defunciones. Instituto Nacional de EstadÍstica y Censos. [Last accessed 2019 Jun 25]. Available from: http://www.ecuadorencifras.gob.ec/nacimientos_y_defunciones .
- 8.Revilla F. PAHO/WHO | SIREVA II (Spanish only) [Last accessed on 2019 Jun 25]. Available from: https://www.facebook.com/pahowho. Pan American Health Organization/World Health Organization. Available from: https://www.paho.org/hq/index.php?option=com_content&view=article&id=5536:2011-sireva-ii and Itemid=3966&lang=en .
- 9.Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016 the Lancet Infectious Diseases. [Last accessed on 2019 Jun 25]. Available from: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099 (18)30310-4/fulltext . [DOI] [PMC free article] [PubMed]
- 10.National, Regional, and State-level Burden of Streptococcus pneumoniae and Haemophilus influenzae Type B Disease in Children in India: Modelled Estimates for 2000-15. [Last accessed on 2019 Jun 25]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6527518 . [DOI] [PMC free article] [PubMed]
- 11.de Oliveira LH, Camacho LA, Coutinho ES, Martinez-Silveira MS, Carvalho AF, Ruiz-Matus C, et al. Impact and effectiveness of 10 and 13-valent pneumococcal conjugate vaccines on hospitalization and mortality in children aged less than 5 years in Latin American countries: A systematic review. PLoS One. 2016;11:e0166736. doi: 10.1371/journal.pone.0166736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McAllister DA, Liu L, Shi T, Chu Y, Reed C, Burrows J, et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: A systematic analysis. Lancet Glob Health. 2019;7:e47–57. doi: 10.1016/S2214-109X(18)30408-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Clothier HJ, Vu T, Sundararajan V, Andrews RM, Counahan M, Tallis GF, et al. Invasive pneumococcal disease in Victoria: A better measurement of the true incidence. Epidemiol Infect. 2008;136:225–31. doi: 10.1017/S0950268807008187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Department of Health | 3.10 Pneumococcal Disease. [Last accessed on 2019 Jun 25]. Available from: https://www.health.gov.au/internet/publications/publishing.nsf/Content/cda-cdi34suppl.htm ~ cda-cdi34 suppl-3-vpd.htm ~ cda-cdi34 suppl-3-vpd10.htm .