

Abstract
Background:
The relationships between sport specialization, physical activity, sleep, and illness in younger athletes are unknown. Therefore, the purpose of this study was to evaluate the independent effects of sport specialization, sleep, and physical activity on illness in middle school athletes.
Hypothesis:
Decreased sleep, decreased physical activity, and higher levels of sport specialization will be associated with an increased risk of illness among middle school athletes.
Study Design:
Prospective cohort study.
Level of Evidence:
Level 4.
Methods:
Parents of middle school–aged children reported baseline sport specialization (low, moderate, or high) as well as sleep duration, physical activity, and illnesses every week throughout the academic year. A mixed-effects logistic regression model was used to assess the association between illness and specialization while accounting for sleep and physical activity for the prior week as fixed effects and each individual as a random effect.
Results:
A total of 233 children (mean age, 12.1 ± 1.2 years; 61% male) participated, of whom 41%, 25%, and 34% were categorized as low, moderate, and high specialization, respectively. The proportion of individuals who experienced illness did not differ by specialization level (low, 76%; moderate, 70%; high, 59%; P = 0.064). In the multivariable model, the odds of illness compared with the low specialization group was not significantly different for moderate (odds ratio [OR], 0.93; 95% CI, 0.70-1.23; P = 0.61) or high specialization (OR, 0.76; 95% CI, 0.56-1.03; P = 0.073). A decreased risk of illness was associated with greater prior week sleep (OR, 0.79; 95% CI, 0.69-0.91; P < 0.001) and physical activity (OR, 0.94; 95% CI, 0.92-0.96; P < 0.001).
Conclusion:
Sport specialization is not associated with an increased risk of illness among middle school athletes, while increased sleep duration and physical activity appear to reduce the risk of illness.
Clinical Relevance:
Interventions to promote physical activity and improve sleep may reduce the risk of illness in early adolescent athletes.
Keywords: athletes, training load, specialization, sleep
A lthough numerous policy statements and guidelines suggest that specializing in a single sport at an early age may increase the risks of stress, overtraining, and burnout in young athletes,1,2,14,20 there is little primary evidence in this area. Stress and overtraining may be risk factors for illness,3,5,17 however, and a 2018 study showed that specialized female youth soccer athletes exhibited worse fatigue, stress, and mood quality during the season compared with their nonspecialized counterparts.29 Nonetheless, the increased prevalence of these risk factors may result in an increased incidence of illness in specialized youth athletes.
Specialized youth athletes may be subjected to higher training loads (TL) than nonspecialized athletes, but the relationship between TL or physical activity (PA) levels and illness in younger athletes is not understood. In adult athletes, higher volumes of exercise and overtraining appear to increase susceptibility to viral infections,10,25-27 and increased weekly TL is associated with an increased illness risk.7,8,11,27 A study of 15- to 18-year-old male soccer players found that longer training duration was predictive of in-season illness,3 and higher weekly and monthly TL preceded in-season illness among adolescent female soccer players.31 It is unclear whether this same relationship exists among younger athletes or whether sport specialization is associated with increased in-season illness after adjusting for PA level.
Poor sleep may also increase the risk of illness.4,22 Multiple prior studies have documented inadequate sleep among athletes, and young athletes may be at even greater risk for chronic sleep deprivation given their increased sleep needs in the face of competing academic, social, and athletic demands.6,9,15,16,24,32 Although moderate exercise is generally considered beneficial for sleep, the increased risk of illness in overtrained athletes may be due at least in part to sleep disturbances during periods of increased TL.10 Acute spikes in TL may negatively affect both sleep duration and quality among youth athletes,31 and specialized female soccer athletes have demonstrated worse sleep quality during the season than their nonspecialized counterparts, even after controlling for TL.30 Despite the importance of identifying the modifiable risk factors for illness in youth athletes, the interactions between specialization, sleep, TL, and illness in youth athletes is not understood.
The overwhelming majority of prior research regarding specialization has been conducted among older adolescent and high school–aged athletes, but little is known about the relationship with illness. In a single study of 16-year-old elite athletes over 6 months, sport specialization was not associated with an increased risk of illness.19 It is our hope that by identifying risks that could be associated with a pattern of youth sport participation, we can help inform the decision-making process. Although prior research in older athletes has evaluated the relationships between specialization, sleep, PA, and illness, we are not aware of prior research that has evaluated these relationships among younger athletes. Therefore, the purpose of this study was to determine the relationships between sport specialization, sleep, PA, and illness among middle school athletes.
Methods
Study Design
This was a prospective cohort study designed to examine the relationships between illness, sport specialization level, sleep, and PA. A convenience sample of youth sport clubs and governing bodies from multiple sports throughout the state of Wisconsin were approached regarding the study and asked to distribute information among their participant members. Interested participants who contacted the study team were screened for eligibility and deemed eligible if their child was 10 to 14 years of age at the start of the data collection period and planning to participate in at least 1 organized sport during the data collection period; the parent had to be able to read English at a minimum sixth-grade level and have access to email and/or SMS text. These individuals were asked to provide written informed consent, after which they reported baseline information regarding age, sex, and sport participation, as well as average weekly hours of organized and unorganized PA during the prior year. Based on the information reported, athletes were classified as low, moderate, or highly specialized using the 3-point sport specialization scale that has been described and widely utilized in previous research.1,12,13,18
During the subsequent 39-week academic year, participating families were sent a weekly electronic survey that asked them to report any illnesses suffered during the prior week, as well as the total number of hours of organized PA and the average hours of sleep during the prior week. If an illness was reported, further information was requested regarding the date of illness onset, whether a health care provider was seen, the number of days of school and athletics missed, and the duration of the illness. Based on symptoms provided, illnesses were classified as gastrointestinal, upper respiratory, lower respiratory, skin, or other. Patients and the public were not directly involved in the design, conduct, or reporting of the research. All procedures performed in this study were approved by the institutional review board of the University of Wisconsin–Madison.
Statistical Analysis
Individuals who provided complete data on the baseline survey and at least 80% of the weekly surveys during the academic year were included for analysis. Data were initially evaluated for normality using descriptive statistics and histogram analysis. Missing data were evaluated with respect to individual and time of year and felt to be missing at random. Based on this, missing values for weekly sleep and PA were imputed using a predictive mean matching approach, with additive regression fits on the complete data and simple bootstrapping to generate predicted values for the missing data (aregImpute function in R).23 Comparisons of baseline variables between specialization groups (low, moderate, high) were made using chi-square tests for categorical variables and Kruskal-Wallis tests with post hoc pairwise Wilcoxon tests for continuous variables. Comparisons of sleep duration and PA during the longitudinal data collection were made between specialization groups using least squares means from separate mixed-effects linear models including specialization and the variable of interest (sleep or PA) as fixed effects and each individual as a random effect. A mixed-effects logistic regression model was used to predict weekly illness (yes/no), including specialization, prior week average sleep duration (hours), prior week organized physical activity (hours), age (years), and sex as fixed effects and each individual as a random effect. The significance level was determined a priori at the 0.05 level, and all tests were 2-tailed. All statistical analyses were performed in R.23
Results
A total of 300 families initially agreed to participate, of whom 233 children provided baseline and at least 80% of the weekly surveys. Baseline characteristics of the 233 participants are shown in Table 1. A total of 434 illnesses were recorded in 162 participants (69%); 187 (43%) were evaluated by a health care provider. The majority of illnesses were classified as upper respiratory infections (313; 72%), followed by gastrointestinal infections (61; 14%), lower respiratory infections (7; 2%), skin infections (7; 2%), and other unclassified illnesses (46; 11%). The median days of school missed was 1 (range, 0-4 days), while the median days of sport missed was 0 (range, 0-5 days). The median time to recovery was 3 days (range, 1-12 days).
Table 1.
Baseline characteristics of participants (N = 233)
| Sex, male, n (%) | 142 (61) |
| Age, y, mean ± SD | 12.1 ± 1.2 |
| Total weekly PA, hours, mean ± SD | 19.5 ± 9.6 |
| Weekly organized PA, hours, mean ± SD | 13.0 ± 7.9 |
| Weekly unorganized PA, hours, mean ± SD | 6.44 ± 5.6 |
| Primary sport, n (%) | |
| Basketball | 81 (35) |
| Soccer | 27 (12) |
| Volleyball | 24 (10) |
| Tennis | 21 (9) |
| Baseball | 20 (9) |
| Football | 15 (6) |
| Cross-country | 12 (5) |
| Softball | 11 (5) |
| Swimming/diving | 11 (5) |
| Othera | 11 (5) |
PA, physical activity.
Includes sports in which 5 or fewer individuals participated: cheer/dance, gymnastics, wrestling, and ice hockey.
Overall, 118 (41%), 72 (25%), and 99 (34%) participants were classified as low, moderate, and high specialization, respectively. The proportion of athletes categorized as specialized differed significantly across age groups, with the highest rates of high specialization being identified among 11- and 12-year-old athletes (Table 2 and Figure 1). Specialized athletes were younger, with a greater proportion of male participants and higher baseline weekly total and weekly organized PA but lower levels of weekly unorganized PA (Table 3).
Table 2.
Number of participants classified as low, moderate, or high specialization by age at the start of the study perioda
| Age, y | |||||
|---|---|---|---|---|---|
| 10 | 11 | 12 | 13 | 14 | |
| Total | 22 | 54 | 66 | 63 | 29 |
| Low | 12 (55) | 13 (24) | 29 (44) | 34 (54) | 13 (45) |
| Moderate | 8 (36) | 8 (15) | 13 (20) | 24 (38) | 11 (38) |
| High | 2 (9) | 33 (61) | 24 (36) | 5 (8) | 5 (17) |
Data are shown as n (%).
Figure 1.
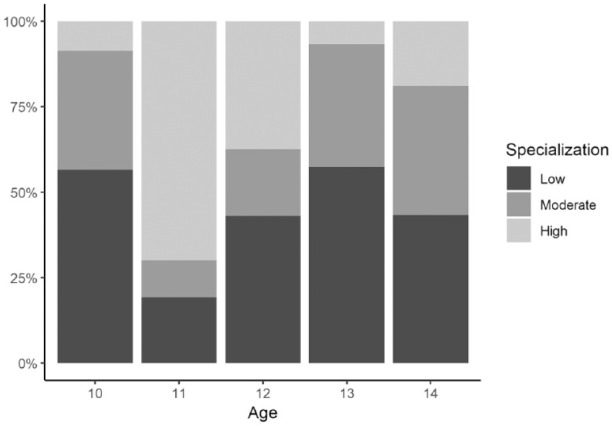
Frequency of low, moderate, and high specialization by age in middle school athletes.
Table 3.
Comparison of demographic and baseline physical activity variables by specialization group
| Variable | Low | Moderate | High | P |
|---|---|---|---|---|
| Sex, male, n (%) | 66, 55% | 43, 60% | 72, 73% | 0.028 |
| Age, y | 12.2 ± 1.2 | 12.3 ± 1.3 | 11.7 ± 0.91 | <0.001 |
| Total weekly PA, hours | 15.4 ± 7.5 | 20.4 ± 9.9 | 24.4 ± 9.6 | <0.001 |
| Weekly organized PA, hours | 9.41 ± 3.8 | 12.8 ± 6.7 | 18.5 ± 10 | <0.001 |
| Weekly unorganized PA, hours | 6.03 ± 5.4 | 7.62 ± 6.7 | 5.93 ± 4.6 | 0.23 |
| Ratio of organized:unorganized PA | 2.61 ± 2.2 | 2.91 ± 2.5 | 4.28 ± 4.6 | 0.007 |
PA, physical activity.
In the univariate analysis, we did not find a statistically significant difference in the proportion of individuals within each specialization group who suffered an illness during the study period (low, 76%; moderate, 70%; high, 59%; P = 0.064). Individuals in the high specialization group demonstrated lower average sleep duration during the year (low, 8.63 hours [95% CI, 8.5-8.8 hours]; moderate, 8.71 hours [95% CI, 8.6-8.9 hours]; high, 8.48 hours [95% CI, 8.3-8.6 hours]), while no significant differences were noted between groups with respect to PA (low, 9.32 hours [95% CI, 8.2-10 hours]; moderate, 9.43 hours [95% CI, 8.0-11 hours]; high, 10.8 hours [95% CI, 9.4-12 hours]) (Figure 2). In the multivariable logistic model, however, higher levels of sleep duration and PA were associated with a decreased risk of illness the subsequent week, while sport specialization level was not a significant predictor of in-season illness (Table 4).
Figure 2.

Weekly sleep duration and organized physical activity by specialization group among middle school athletes during the academic year. Data are shown as violin plots representing the distribution of the data, along with overlying mean and 95% CI from mixed-effects linear models.
Table 4.
Results of a multivariable mixed-effects logistic regression model to predict the individual risk of weekly illness during the academic year among middle school athletes
| 95% CI | ||||
|---|---|---|---|---|
| Variable | Estimate | Lower Limit | Upper Limit | P |
| Specialization—Moderate | 0.93 | 0.70 | 1.23 | 0.61 |
| Specialization—High | 0.76 | 0.56 | 1.03 | 0.073 |
| Prior week PA, hours | 0.94 | 0.92 | 0.96 | <0.001 |
| Prior week sleep, hours | 0.79 | 0.69 | 0.91 | <0.001 |
| Age, y | 1.06 | 0.95 | 1.18 | 0.28 |
| Sex, male | 0.79 | 0.62 | 1.01 | 0.055 |
PA, physical activity.
Discussion
The primary finding of this study is that in middle school athletes, there was no increased risk of illness associated with higher degrees of sport specialization. These findings are consistent with a recent study of adolescent elite athletes over a 6-month period that did not identify any increased risk of illness among single-sport athletes or those who reported previously specializing in their sport before the age of 12 years.19 The participants in this study demonstrated higher rates of specialization at younger ages, which is in contrast to studies of high school–aged athletes who typically exhibit increasing levels of specialization as they get older. The reason for this is not clear from the available data, but even after adjusting for age in the multivariable model, we did not find an increased risk of illness with higher levels of specialization.
Prior research has suggested that specialized youth athletes exhibit several characteristics that could put them at increased risk for illness compared with their nonspecialized counterparts.30 For example, specialization was associated with worse mood, stress, fatigue, and sleep quality among adolescent female soccer athletes—all of which could be considered risk factors for illness.30 Among a group of elite adolescent male soccer players, psychosocial stress was a risk factor for illness over 2 seasons of competitive play.3 In addition, early sport specialization includes high training loads and an increased risk of overtraining,2 which is related to illness incidence in adult athletes.10 In the present study, we found that highly specialized athletes had lower sleep duration during the study, which is consistent with a prior study of adolescent athletes that found higher levels of daytime sleepiness among specialized individuals.21 It is unclear, however, whether this represents a clinically meaningful difference. Nonetheless, in the current study of middle school athletes from a wide variety of sports, we did not find that the proportion of individuals who suffered an illness differed between specialization groups, and in the multivariable model, there was no association between specialization and illness risk during a 9-month academic year.
On the other hand, we did find that individuals with greater sleep duration were less likely to report an illness the following week, even after adjusting for age, sex, and physical activity. This is consistent with prior research in adults that has suggested that decreased sleep duration results in an increased susceptibility to upper respiratory infections.4,22 Similarly, in a study of elite cyclists randomized to 3 weeks of either habitual training or overload (130% habitual volume), those individuals in the overload group who demonstrated signs of overreaching not only experienced impaired sleep but also had an increased incidence of illnesses during the study period.10 In the current study, we found that an increase of 1 hour of sleep per week was associated with a 6% decrease in illness risk the following week. While this increase may seem small, individual increases of an hour per night could have much larger effects, and efforts to promote proper sleep in middle school athletes in general could have a significant effect on the overall burden of illness during the school year.
We also found that greater amounts of PA appeared to be protective against illness the following week. Although there was some evidence that specialized athletes had higher average PA levels before and during the study period, the effect of PA on illness risk persisted after adjusting for specialization, age, sex, and sleep duration. Overtraining may be immunosuppressive and increase the risk of illness in athletes, but it has generally been accepted that appropriate levels of PA promote immune system function and may reduce the risk of infection.10,28,31 During the study period participants typically reported moderate amounts of 8 to 10 hours of weekly organized PA, with higher weekly volumes associated with a decreased risk of illness the subsequent week. It is possible that the higher baseline PA levels represent an overestimation when reported retrospectively for the prior year, or it could mean that levels of PA were higher during the summer months immediately prior to the start of the study period. Nonetheless, the prospective data suggest that among middle school athletes, the promotion of appropriate levels of PA may reduce the risk of illness during the school year.
Limitations
This study has several limitations. Given the recruitment methodology, we cannot determine the number of individuals initially contacted and therefore do not know the overall response rate. We also cannot account for factors that may influence the decision to participate in or drop out of the study that may influence the results. For example, current perceptions about sport specialization may make families less likely to participate if they are highly specialized or more likely to drop out if they are experiencing multiple illnesses. This study relies on self-reported information from the parents of the youth athletes being studied. This was the best way to obtain information from a larger group of participants in a cost-effective manner; however, it is possible that there could be inaccuracies in the reported data. Parents were asked to report whether their child had experienced an illness, and a nonuniform understanding of the definition of “illness” among the study participants could influence the data. Given the recruitment methods, this sample of middle school athletes likely includes predominantly club sport participants and may not represent a diverse group from a socioeconomic standpoint.
As with virtually any survey-based study, there were missing data. During the design of the study, we assumed it would be reasonable to include those individuals with 80% compliance or higher with the weekly surveys. We also evaluated the sensitivity of the imputation method utilized by comparing the results with those generated without imputation, with crude imputation methods including the use of mean, median, and last value carried forward, and with variable numbers of knots and multiple imputations within the imputation method used. The results of each analysis were virtually identical, suggesting that the imputation method is reliable and that the missing data had little influence on the overall results. Finally, it may be difficult to generalize the results to other specific populations of athletes.
Conclusion
This study demonstrates that greater amounts of sleep and PA are independently associated with a decreased risk of illness the following week. We did not, however, identify any relationship between illness risk and sport specialization, age, or sex among this group of middle school athletes. While prior research has found that specialized athletes report higher levels of risk factors for illness such as stress and sleep impairment, this does not appear to translate into an increased risk of illness during the academic year in middle school athletes.
Footnotes
The following authors declared potential conflicts of interest: A.W. and D.B. have received grants from the American Medical Society for Sports Medicine. M.A.B. has grants pending from NCAA-DOD CARE Consortium Concussion study and has received reimbursements from American Medical Society for Sports Medicine and American Academy of Pediatrics Council on Sports Medicine and Fitness.
References
- 1. Bell DR, Post EG, Trigsted SM, Hetzel S, McGuine TA, Brooks MA. Prevalence of sport specialization in high school athletics: a 1-year observational study. Am J Sports Med. 2016;44:1469-1474. [DOI] [PubMed] [Google Scholar]
- 2. Brenner JS. Overuse injuries, overtraining, and burnout in child and adolescent athletes. Pediatrics. 2007;119:1242-1245. [DOI] [PubMed] [Google Scholar]
- 3. Brink MS, Visscher C, Arends S, Zwerver J, Post WJ, Lemmink KA. Monitoring stress and recovery: new insights for the prevention of injuries and illnesses in elite youth soccer players. Br J Sports Med. 2010;44:809-815. [DOI] [PubMed] [Google Scholar]
- 4. Cohen S, Doyle WJ, Alper CM, Janicki-Deverts D, Turner RB. Sleep habits and susceptibility to the common cold. Arch Intern Med. 2009;169:62-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Drew MK, Vlahovich N, Hughes D, et al. A multifactorial evaluation of illness risk factors in athletes preparing for the Summer Olympic Games. J Sci Med Sport. 2017;20:745-750. [DOI] [PubMed] [Google Scholar]
- 6. Erlacher D, Ehrlenspiel F, Adegbesan OA, El-Din HG. Sleep habits in German athletes before important competitions or games. J Sports Sci. 2011;29:859-866. [DOI] [PubMed] [Google Scholar]
- 7. Foster C. Monitoring training in athletes with reference to overtraining syndrome. Med Sci Sports Exerc. 1998;30:1164-1168. [DOI] [PubMed] [Google Scholar]
- 8. Gleeson M, Bishop N, Oliveira M, Tauler P. Influence of training load on upper respiratory tract infection incidence and antigen-stimulated cytokine production. Scand J Med Sci Sports. 2013;23:451-457. [DOI] [PubMed] [Google Scholar]
- 9. Gupta L, Morgan K, Gilchrist S. Does elite sport degrade sleep quality? A systematic review. Sports Med. 2017;47:1317-1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hausswirth C, Louis J, Aubry A, Bonnet G, Duffield R, Le Meur Y. Evidence of disturbed sleep and increased illness in overreached endurance athletes. Med Sci Sports Exerc. 2014;46:1036-1045. [DOI] [PubMed] [Google Scholar]
- 11. Hellard P, Avalos M, Guimaraes F, Toussaint JF, Pyne DB. Training-related risk of common illnesses in elite swimmers over a 4-yr period. Med Sci Sports Exerc. 2015;47:698-707. [DOI] [PubMed] [Google Scholar]
- 12. Jayanthi N, Pinkham C, Dugas L, Patrick B, Labella C. Sports specialization in young athletes: evidence-based recommendations. Sports Health. 2013;5:251-257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Jayanthi NA, LaBella CR, Fischer D, Pasulka J, Dugas LR. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med. 2015;43:794-801. [DOI] [PubMed] [Google Scholar]
- 14. LaPrade RF, Agel J, Baker J, et al. AOSSM early sport specialization consensus statement. Orthop J Sports Med. 2016;4:2325967116644241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lastella M, Lovell GP, Sargent C. Athletes’ precompetitive sleep behaviour and its relationship with subsequent precompetitive mood and performance. Eur J Sport Sci. 2014;14(suppl 1):S123-S130. [DOI] [PubMed] [Google Scholar]
- 16. Leeder J, Glaister M, Pizzoferro K, Dawson J, Pedlar C. Sleep duration and quality in elite athletes measured using wristwatch actigraphy. J Sport Sci. 2012;30:541-545. [DOI] [PubMed] [Google Scholar]
- 17. Mann JB, Bryant KR, Johnstone B, Ivey PA, Sayers SP. Effect of physical and academic stress on illness and injury in Division 1 college football players.J Strength Cond Res. 2016;30:20-25. [DOI] [PubMed] [Google Scholar]
- 18. McGuine TA, Post EG, Hetzel SJ, Brooks MA, Trigsted S, Bell DR. A prospective study on the effect of sport specialization on lower extremity injury rates in high school athletes. Am J Sports Med. 2017;45:2706-2712. [DOI] [PubMed] [Google Scholar]
- 19. Moseid CH, Myklebust G, Fagerland MW, Bahr R. The association between early specialization and performance level with injury and illness risk in youth elite athletes. Scand J Med Sci Sports. 2019;29:460-468. [DOI] [PubMed] [Google Scholar]
- 20. Myer GD, Jayanthi N, Difiori JP, et al. Sport specialization, part I: does early sports specialization increase negative outcomes and reduce the opportunity for success in young athletes? Sports Health. 2015;7:437-442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Post EG, Trigsted S, Schaefer DA, et al. The association of sport specialization, overuse injury, and travel with daytime sleepiness in youth athletes. Athl Train Sports Health Care. 2020;12:59-66. [Google Scholar]
- 22. Prather AA, Janicki-Deverts D, Hall MH, Cohen S. Behaviorally assessed sleep and susceptibility to the common cold. Sleep. 2015;38:1353-1359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. R Development Core Team. R: A Language and Environment for Statistical Computing [computer program]. R Foundation for Statistical Computing; 2015. [Google Scholar]
- 24. Robey E, Dawson B, Halson S, Gregson W, Goodman C, Eastwood P. Sleep quantity and quality in elite youth soccer players: a pilot study. Eur J Sport Sci. 2014;14:410-417. [DOI] [PubMed] [Google Scholar]
- 25. Spence L, Brown WJ, Pyne DB, et al. Incidence, etiology, and symptomatology of upper respiratory illness in elite athletes. Med Sci Sports Exerc. 2007;39:577-586. [DOI] [PubMed] [Google Scholar]
- 26. Svendsen IS, Gleeson M, Haugen TA, Tonnessen E. Effect of an intense period of competition on race performance and self-reported illness in elite cross-country skiers. Scand J Med Sci Sports. 2015;25:846-853. [DOI] [PubMed] [Google Scholar]
- 27. Thornton HR, Delaney JA, Duthie GM, et al. Predicting self-reported illness for professional team-sport athletes. Int J Sports Physiol Perform. 2016;11:543-550. [DOI] [PubMed] [Google Scholar]
- 28. Walsh NP. Recommendations to maintain immune health in athletes. Eur J Sport Sci. 2018;18:820-831. [DOI] [PubMed] [Google Scholar]
- 29. Watson A, Brickson S. Impaired sleep mediates the negative effects of training load on subjective well-being in female youth athletes. Sports Health. 2018;10:244-249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Watson A, Brickson S. Relationships between sport specialization, sleep, and subjective well-being in female adolescent athletes. Clin J Sport Med. 2019;29:384-390. [DOI] [PubMed] [Google Scholar]
- 31. Watson A, Brickson S, Brooks A, Dunn W. Subjective well-being and training load predict in-season injury and illness risk in female youth soccer players. Br J Sports Med. 2017;51:194-199. [DOI] [PubMed] [Google Scholar]
- 32. Watson AM. Sleep and athletic performance. Curr Sports Med Rep. 2017;16:413-418. [DOI] [PubMed] [Google Scholar]