

Abstract
Previous research has shown that as depressive symptomology increases, mothers tend to show withdrawn or harsh interaction patterns with their children, and the quality of these interaction patterns have subsequently been linked to child behavior problems. However, little research has examined bidirectional influences between mothers and their children, and how these moment-to-moment contingencies differ based on heritable and environmental characteristics. We used data from the Early Growth and Development Study a prospective adoption study to examine how adoptive mothers’ depressive symptoms and children’s heritable tendencies for negative affectivity interact to predict the quality of mother-child interactions at child age 27-months. Results detected two distinct dyadic interaction patterns. The first was a withdrawn interaction style and was observed in children with a high heritable tendency for negative affect. In that style, mother and child interactions were not contingent upon each other, suggesting a lack of joint engagement. The second was a volatile interaction style, observed in children with a low heritable tendency for negative affect. In these cases, mother and child interactions were highly contingent but negative. Our findings demonstrate essential differences in how dyadic interaction patterns vary according to level of depressive symptomology and heritable tendency for negative affect.
Keywords: parent-child interaction, depressive symptoms, temperamental negative affectivity, adoption, behavioral genetics, multivariate multilevel modeling
1. Introduction
Maternal depressive symptomology is associated with a range of important child outcomes including child externalizing behavior problems, lower intellectual functioning, and social exclusion by peers (Belsky, 1984; Goodman, 2007; Goodman et al., 2011; Kerr et al., 2013; Natsuaki et al., 2014). One of the mechanisms through which this is believed to occur is through the quality of maternal interactions with their children (Goodman & Gotlib, 1999; Goodman, 2007; Goodman et al., 2011). For example, mothers with depressive symptomology can be withdrawn from (Dix, Meunier, Lusk, & Perfect, 2012; Field, Healy, & LeBlanc, 1989; Leadbeater, Bishop, & Raver, 1996), or intrusive/negatively reactive towards their young children (Field, Healy, Goldstein, & Guthertz, 1990; Gelfand & Teti, 1990; Henderson & Jennings, 2003), but many also maintain high levels of responsivity and involvement despite challenges to their mental health (Cohn & Tronick, 1989; Shaw et al., 2006).
There is considerably less research on bi-directional influences of mother and infant influences on interaction quality (Pardini, Fite, & Burke, 2008; (Gross, Shaw, & Moilanen, 2008), although notable exceptions do exist of research on the coordination of and emotional regulation between depressed mothers and their children (e.g., Tronick & Reck, 2009; Riva Crugnola, Ierardi, Albizzati, & Downing, 2016). In this research tradition, contingency refers to the quality of the bidirectional, moment-to-moment, and mutually influential interactions within dyadic pairs. Contingent negativity refers to the degree to which a partner's negative behavior is dependent (or conditional on) the other's prior negative behavior (Roben et al., 2015). For example, contingent negativity would be demonstrated if a mother tries to force her toddler to place a puzzle piece where she wants it, and the child responds by forcibly resisting her grasp. It represents one approach to quantifying coercive cycles in which a negative behavior begets a negative response. Coercive cycles have been repeatedly shown to predict escalation in conflict and poor outcomes in children (Patterson et al., 2002).
In the reverse, positive behavior can of course follow positive behavior. Synchrony and mutuality are two approaches that have been widely used to determine the degree to which one partner’s affect or responsiveness temporally follows the other partner’s expression or behavior (Feldman, 2015; Kim & Kochanska, 2012). Synchrony and mutuality within dyads predict positive self-regulation outcomes in children (Blair et al., 2011; Feldman, Greenbaum, & Yirmiya, 1999; Deater-Deckard & Petrill, 2004). Theoretically, negative behavior followed by negative behavior, and positive behavior followed by positive behavior, would both be considered examples of synchrony or mutuality (see Feldman, 2007 for review). However, much of the empirical work in synchrony and mutuality is conducted using low-conflict tasks like free-play that are more likely to encourage positivity and less likely to elicit negativity (see Leclère et al., 2014 for review). In contrast, a conflictual task, like a cleanup task or a teaching task, tends to evoke higher contingent negativity (Rodriguez et al., 2005).
However, mothers and children tend to spend most of their time in mismatched states (e.g., the child is negative and the mother responds positively), rather than in matched states (Tronick & Cohn, 1989; Tronick, 1989). Thus, a method is needed to capture the degree to which one partner's behavior is dependent (or conditional on) the other's prior behavior, regardless of whether that behavior is positive or negative, and regardless of whether it is matched with the prior behavior. Here, we introduce the construct behavioral contingency which, like mutuality or synchrony, represents the overall contingency between partners. Critically, it captures congruent positive and negative responses, as well as mismatched responses. As this is the first study to measure mother-child behavioral contingency, it is not yet known if behavioral contingency will be moderated by mother and child characteristics.
In addition, research examining bidirectional mother-child interaction patterns tends to involve biologically-related mothers and children, where the influence of parenting is confounded with shared genetics. Sameroff’s (1975; 2009) seminal transactional model (which expanded on Bell’s (1968) theory on mother-child relationships) proposed that variations in children’s vulnerabilities to environmental stressors are the result of bidirectional, reciprocal influences between heritable child characteristics (e.g., temperament) and their environment (e.g., maternal depressive symptoms). Some children are more vulnerable to the effects of maternal depressive symptoms than others because of gene by environment (G x E) interactions (Goodman et al., 2011; Hammen, 2002; Rutter, 2007). Therefore, in studies of biologically related mother-child dyads, if an infant or toddler of a depressed mother shows high contingent negativity, it’s unclear whether this negative reactivity is due to the dyad’s shared heritable influences for temperamental negative affectivity, the effect of the mother’s style of parenting associated with her depressive symptoms, or the combination of the two.
The parent-offspring adoption design used in the current study included measurement of both adoptive and birth mothers, allowing us to disentangle how heritable and environmental influences work together to predict adoptive mother-child interaction patterns. Focusing only on contingent negativity, previous research using the same sample as the current study found that, as adoptive mother’s depressive symptoms increased, children’s contingent negativity increased, which subsequently predicted later adoptive mother’s increase depressive symptoms (Roben et al., 2015). Notably, this last finding was only present if the child’s birth mother was depressed, suggesting a G x E interaction. We aim to build on this prior work through modeling of contingent negativity and behavioral contingency. Our two-pronged approach can provide a more comprehensive analysis of two possible ways that maternal depressive symptoms negatively affect children, through mother-child mutual negativity and overall responsivity (either matched or mismatched).
Further, Roben et al. (2015) used one-second intervals in their analyses, but there are strong reasons to suggest that such a brief period of time may not provide a sufficiently long observation window for a young child to respond, limiting the ability to capture valid mother-child interaction patterns. For example, Tronick and Cohn (1989) used a data-driven approach for their observational coding and found that it took 3-5 seconds for mothers and their infants to repair disruptions in their interactions. There are of course substantive differences in construct between the repair of a disruption in a relationship, and behavioral contingency/contingent negativity, but the common concern is that there are currently no standardized rules for determining appropriate epoch length and lag for observation data. The length and lags chosen for any given study or group of studies could significantly impact results as they can be accounting for mere moments or up to a minute of interaction time.
In the current study, we use multivariate multilevel models to simultaneously model the associations between mother and child behaviors, and between broad characteristics of adoptive mothers and birth mothers. In this first study of behavioral contingency, we examined child and adoptive mother behavioral contingency, contingent negativity, and how these contingencies are associated with birth mother negative affect (as a heritable influence), current maternal depressive symptoms (as a proximal environmental influence), and the interaction between the two. We modeled adoptive mothers’ concurrent depressive symptoms and dyadic interaction patterns to capture the association of present depressive symptoms and dyadic interaction patterns because these dyadic interactions patterns have been associated with poor child outcomes (Goodman et al., 2011). While the timing of adoptive mother assessments is critical (given the risk for developing depression in the early days of adoption, see Mott, Schiller, Richards, O’Hara, & Stuart, 2011), the timing of birth mother assessments is less important because temperamental negative affect is a stable trait, whereas depressive symptoms change over time.
We note that birth mother negative affectivity was chosen as the heritable influence because it has moderate heritable associations with child negative affectivity, predicts young children’s externalizing behaviors, and evokes more harsh parenting (Goldsmith, Buss, & Lemery, 1997; Lipscomb et al., 2011, 2014). Difficult child temperament has also been shown to result in low behavioral contingency because mothers of difficult temperament children withdraw from their child, presumably due to the fact they are more stressful to parent (Koenig, Barry, & Kochanska, 2010).
1.1. Hypotheses
For adoptive mothers and their children engaged in a difficult teaching task, we hypothesized first that (1) dyads with children whose birth mothers show higher negative affectivity would show lower maternal (mother reacting to child) and child (child reacting to mother) behavioral contingency and higher contingent negativity. This would mean that the dyad shows less overall contingency, but when there is negative behavior, the partners respond with negative behavior.
Second, based on previous research on the environmental associations between maternal depressive symptoms and mother-child relationship quality (Goodman, 2007), we also hypothesized that (2) adoptive mothers with higher depressive symptomology would show lower maternal and child behavioral contingency and higher contingent negativity.
Finally, we hypothesized that there would be a moderating effect in which (3) dyads with children whose birth mothers showed higher negative affectivity and whose adoptive mothers had higher levels of depressive symptoms, would demonstrate the lowest maternal and child behavioral contingency and the highest contingent negativity. We presumed that the children whose birth mothers reported higher negative affectivity would be more difficult temperamentally, and this higher negative affectivity would be associated with lower behavioral contingency. Dyads with children whose birth mothers show lower negative affectivity and adoptive mothers with few depressive symptoms were expected to demonstrate the highest maternal and child behavioral contingency and the lowest contingent negativity.
2. Method
2.1. Participants
The data used in the current study were from the Early Growth and Development Study (EGDS), a prospective parent-offspring adoption study including data from birth parents, adoptive parents, and adopted children (Leve et al., 2019). Table 1 provides demographic information on birth and adoptive mothers who were included in this study (n = 393).
Table 1.
Birth and Adoptive Mother Demographics and Descriptives (n = 393).
| Birth Mother | Adoptive Mother | |
|---|---|---|
| Average age in years (SD) at first wave of data collection | 24.92 (6.0) | 38.19 (5.65) |
| Age range in years | 14.25 – 41.98 | 25.57 – 54.82 |
| Race (%) | ||
| Caucasian | 71.7 | 93.6 |
| African American | 13.3 | 3.1 |
| Hispanic/Latino | 5.6 | 1.8 |
| Multi-ethnic | 4.8 | 1.0 |
| Other (Asian, Native American/Pacific Islander, American Indian/Alaskan Native, and unknown) | 4.6 | 0.5 |
| Mean education levela(SD) | Completed 12th grade (1.55) | Bachelor’s degree |
| (1.84) | ||
| Median annual household incomeb (SD) | $25,000 (1.16) | $100,000 (1.19) |
| Annual household income range | < $15,000 – $125,000 | $15,001 – > $300,000 |
| Negative Affectivity score of the Adult Temperament Questionnaire | 4.01 (0.74) | N/A |
| Total Score on Beck Depression Inventory | N/A | 3.82 (4.10) |
Mothers’ education level was completed on a 11-point Likert scale, 1 (< eighth grade) to 11 (completed professional or graduate degree).
Household income range was completed on a 6-point Likert scale, 1 (< 15,000/yr) to 7 (> 125,000/yr).
The children in this study were 57.2% male, and 55.6% Caucasian, 19.3% multiracial, 13% African American, 10.9% Latino, < 1% Asian, < 1% American Indian, and < 1% ethnicity not reported. Families were recruited nationwide through various types of adoption agencies: public, private, religious, secular, open adoption, and closed adoption. All adoptions were to non-relative families; none of the children were adopted by parents who were genetically related to them. The median child age at placement was two days (SD = 12 days), and children had no significant medical conditions.
2.2. Procedure
The birth mother and adoptive family in-person assessments were conducted by interviewers who completed a minimum of 40 hours of training. Birth mother assessments were conducted in a location convenient to the birth mothers and occurred at 18-months post-partum. The adoptive family assessment occurred when the adopted child was 27-months of age. In-person assessments for birth mothers and the adoptive families lasted 2-3 hours and included self-report questionnaires, personal interview questions, and interviewer impressions, along with videotaped standardized tasks. In the current study, data from a microcoded dyadic interaction task, the Parent-Child Teaching Task, along with birth mother and adoptive mother questionnaire data were used for analyses.
2.3. Measures
2.3.1. Birth mother temperamental negative affectivity
The Adult Temperament Questionnaire(ATQ; Derryberry & Rothbart, 1988) was completed by the birth mother at 18-months postpartum. The Negative Affectivity factor of the ATQ consists of subscales measuring levels of fear, sadness, anger, frustration, and discomfort. Mothers reported on a 7-point scale that ranged from “extremely untrue” to “extremely true,” with higher scores representing higher levels of negative affectivity. Birth mother’s ratings were used to create factor scales with a minimum of 1 and a maximum of 7 (α = .81; See Table 1). This score was used to represent the heritable influences of temperamental negative affectivity on the child.
There was a large proportion of missing data (65% missing) for birth fathers, and therefore birth fathers’ temperamental negative affectivity scores were not included in the current analysis because of multivariate multilevel modeling’s limitation in its capacity to effectively handle such a high level of missing data.
2.3.2. Adoptive mother depressive symptoms
The Beck Depression Inventory(BDI; Beck, Steer, & Brown, 1996) was used to index the adoptive mother’s current depressive symptoms at the 27-month assessment. Adoptive mothers reported their depressive symptoms on a 3-point scale with higher scores representing the presence and severity of depressive symptoms. Items from the BDI assess multiple symptoms of depression, such as irritability, physical discomfort, guilt, and sadness. Adoptive mother depressive symptoms were calculated as the sum of the 20 BDI items (α = .71). For 65% of the sample the BDI did not include the suicidality item. As such, the suicidality item was removed from analyses. Scores from 0-13 are considered to be in the minimal range, 14-19 is considered mild, 20-28 is considered moderate, and 29-63 is severe (BDI; Beck et al., 1996). Table 1 provides means and standard deviations for adoptive mother depressive symptoms. Eleven of the adoptive mothers in this sample met criteria for mild depression (1.9% of the sample), one mother met criteria for severe depression (.3% of the sample), and no mothers met criteria for moderate depression in the sample.
2.3.3. The adoptive mother and child interaction
The Parent-Child Teaching Task was used to examine adoptive mother-child dyadic interaction patterns at the 27-months assessment. For this study, only the adoptive mothers and their adopted child observational data were included because we were interested in examining associations between maternal depressive symptoms and mother-child interactions. For same-sex adoptive couples, we included only the primary female caregiver because the analytic method used in this study was unable to model two adoptive parents of the same child. In the 5-minute Parent-Child Teaching Task, mothers were instructed to show their children a difficult puzzle to observe individual differences in mothers’ abilities to scaffold interaction, children’s responses, and how dyads negotiated a task above the children’s developmental ability (e.g., Forman & Kochanska, 2001; Belsky et al., 2006; Page, Wilhelm, Gamble, & Card, 2010). This task has been used in previous research to analyze global ratings of constructs such as children’s engagement, parents’ positive regard for children, maternal sensitivity, parents’ intrusiveness, and parents’ supportive presence (Egeland & Hiester, 1993).
The task was coded with a microcoding system (Moore, Teti, & Roben, 2009) designed for the study based on existing parent-child interaction rating systems (Cohn & Tronick, 1988; Moore & Calkins, 2004; Moore, Cohn, & Campbell, 2001). Mothers’ and children’s behaviors during the Parent-Child Teaching Taskwere coded by trained research assistants naïve to the hypotheses of the current study. Coders were assigned to teams to code either mothers’ behaviors or children’s behaviors and used an observational coding software package (Interact with p.a.t.t.e.r.n. analysis module; Mangold International). The behaviors were coded in 1-second intervals, and most codes were not mutually exclusive so that coders could code all applicable behaviors. To establish inter-rater reliability, subsets of the cases were double-coded. For child codes, 18.9% of cases were double-coded (κ = .70). For mother codes, 22.2% of cases were double coded (κ = .70).
2.4. Data Analytic Strategy
2.4.1. Variable aggregation
Following prior research (Roben et al., 2015), the coded behaviors were collapsed into four theoretically derived composite variables: Positive Maternal Behavior (e.g., scaffold, positive touch, social bid), Negative Maternal Behavior (e.g., harsh touch, disengagement, off task, gaze away from toy and child), Positive Child Behavior (e.g., play with toy, approach toy, social bid, gaze at caregiver), and Negative Child Behavior (e.g., resist, move puzzle away, off task, proximity is outside of caregiver’s reach). The method for creating these composite variables was as follows: At each second, Positive Maternal Behavior was set to 1 if any of the coded behaviors that were positively focused on the child and task occurred (otherwise the variable was set to 0). Negative Maternal Behavior was set to 1 if any of the behaviors that were disengaged from the task or negatively focused on the child occurred. Positive Child Behavior was set to 1 if any of the behaviors that were positively focused on the task or parent occurred. Negative Child Behavior was set to 1 if any of the behaviors that were negatively focused on the parent and task or disengaged from the parent and task occurred. Mother Behavior was an aggregate of Positive Maternal Behavior and Negative Maternal Behavior. Child Behavior was an aggregate of Positive Child Behavior and Negative Child Behavior. The total number of mother and child positive and negative behaviors that were observed across the teaching task are reported in Table 2.
Table 2.
Average Number of Seconds of Coded Mother and Child Behaviors.
| Mean (SD) secs | Skew | Kurtosis | |
|---|---|---|---|
| Overall adoptive mother behavior | 135.89 (51.97) | .23 | −1.76 |
| Positive adoptive mother behavior | 84.44 (41.61) | .96 | −1.20 |
| Negative adoptive mother behavior | 51.45 (43.36) | 1.69 | −1.07 |
| Overall adopted child behavior | 193.46 (62.19) | .07 | −.81 |
| Positive adopted child behavior | 115.54 (65.10) | .48 | −1.77 |
| Negative child behavior | 77.92 (67.68) | 1.08 | −.83 |
To establish which length of time had the best model fit, mothers’ and children’s time-series data were then collapsed into 1-, 2-, 3-, 4-, and 5-second epochs, and the frequency of each composite variable within each epoch was aggregated (e.g., any 2 seconds of Positive Maternal Behavior in a 3-second epoch resulted in a value of 2 for that 3-second epoch). We used restricted maximum likelihood (REML) for these models because of its usefulness for fitting linear mixed models that include fixed and random effects (Raudenbush & Bryk, 2002; Searle, Casella, & McCulloch, 1992).
2.4.2. Multivariate Multilevel Modeling
This study used two multivariate multilevelmodels of time-series data (Hox, Moerbeek, & Van de Schoot, 2017; MacCallum, Kim, Malarkey, & Kiecolt-Glaser, 1997) to assess: (1) behavioral contingency and (2) contingent negativity, hereafter referred to as behavioral contingency for simplicity. Each multilevel model evaluated the degree to which mother and child behavior at epoch 2 was affected by the other’s behavior at epoch 1, over and above their own behavior at epoch 1 (i.e. autocorrelation).
We next asked whether heritable influences on children’s behavior (G; indexed by birth mother temperamental negative affectivity) and environment (E; indexed by adoptive mother’s depressive symptoms), moderated child and maternal behavioral contingency.
And finally, we created a G x E interaction term to determine whether the interaction of heritable and environmental factors influenced maternal and child behavioral contingency.
2.4.3. Data preparation
In the full sample, there were 561 linked sets of participants: 561 adopted children, 567 adoptive mothers, 552 adoptive fathers (this includes 41 same-sex adoptive parent families), 554 birth mothers, and 208 birth fathers. However, 17% of the dyads (n = 96) were not included in the models because they did not participate in the observation task, their task observations were missing because of audio/visual errors related to hardware malfunctions, or the dyad was not visible on the recording. There were other dyads who participated in the observation task but had missing adoptive mother report of depressive symptoms, biological mother report of negative temperament, or both (n = 72).
This missing data led to a final sample of 393 triads with sufficient data for the primary analyses. Of the dyads that were included in the model, their behavior was coded for a total of 48,083 of the 48,178 possible epochs (99.8% code rate). For data analysis, we used Little’s test for missing data used in this study, and the test statistic for data missing at random was not significant (χ2 = 1.79, p = .407). Therefore, the missing data were treated as missing (completely) at random.
To prepare the data, we person-centered the composite behaviors to independently test between- and within-person associations with the heritable influences and environmental influences (Bolger, Davis, & Rafaeli, 2003). This person-centered approach allows us to isolate and measure behavioral contingencies over and above the mother or child’s typical frequency of behavior during any 3-second epoch.
We also calculated individual-level residual deviations (i.e., random effects), which were not correlated with the residual error. Random effects parameters refer to deviations between each partner’s behavior at epoch 2 that varied between each dyad. We attempted random effects for autocorrelation effects and cross-lag effects, but the models did not converge because of the complexity of the model that could not accommodate more parameters. Similarly, we attempted to include covariates in the model, such as annual household income, adoptive mother’s education, and child gender, but those models did not converge because of the complexity of the model. We discuss the implications of the income/SES of our sample in the Discussion.
Finally, we ran behavioral contingency models with epoch lengths of 1-, 2-, 3-, 4-, and 5-seconds and with a lag of 1, 2, or 3 epochs. Model fit statistics (Akaike information criteria, AIC; Bayesian information criteria) were calculated to determine which model had the best fit. We determined best model fit as a combination of low AIC and BIC, along with interpretability. Therefore, a model with low model fit that was uninterpretable might be an example of overfitting the model, and, thus, would not be chosen as the best fitting model. We also used restricted maximum likelihood (REML) for these models because of its usefulness for fitting linear mixed models that include fixed and random effects (Raudenbush & Bryk, 2002; Searle et al., 1992).
Multivariate multilevel models were conducted by using nlme: Linear and Nonlinear Mixed Effects Models (nlme package version 3.1-137; Pinheiro, Bats, DebRoy, Sarkar, & R CORE TEAM, 2018) in R (Version 3.4.0; R Core Team, 2013). The multivariate multilevel models simultaneously calculate mother and child dyadic interaction patterns. The difference between the models is that the behavioral contingency model included positive and negative composite behavior, whereas the contingent negativity model only used negative composite behavior. Equations for these models can be found in the supplementary materials.
3. Results
3.1. Preliminary Analyses
Descriptive statistics of the primary study variables were computed with SPSS 25.0. Correlations between the aggregated coded parent composite behaviors and aggregated child composite behaviors are presented in Supplemental Table 1. The correlations between positive and negative behaviors were low or negative, suggesting that behavioral contingency and contingent negativity were distinct from each other (rs .02 to −.56). More specifically, there was a moderate negative correlation between positive and negative behaviors for children but not for mothers. Model fit statistics of behavioral contingency models with epoch lengths of 1-, 2-, and 3-seconds and a lag of 1, 2, or 3 epochs are presented in Supplemental Table 2. Model fit statistics of models with epoch lengths of 4- and 5- seconds are not presented because of their lack of interpretability. That is, the models with 4- and 5-seconds epochs had nonsignificant autocorrelation of mother or child behavior at epoch 1 and epoch 2. This result is a sign of a poor-fitting model because autocorrelation of behavior typically accounts for the majority of variance when predicting the frequency of an individual’s behavior at epoch 2.
Chi-square tests for model fit could not be calculated because of the difference in dataset length between models. For example, a dataset of 1-second long epochs with a lag of 1 is considerably longer than a dataset of 5-second long epochs with a lag of 5. Therefore, based on our best model fit parameters, the behavioral contingency model with 3-second long epochs and a lag of 1 was determined to show best model fit. We used 3-second long epochs and a lag of 1 for the contingent negativity model as well. This result was in line with Tronick and Cohn (1989), who found that mothers and children tend to take 3-5 seconds to repair disruptions in the interaction.
3.2. 27-Month Behavioral Contingency Model
Note, that we report unstandardized coefficients throughout our model to aid in interpretation. As described in Table 3, we found a significant autocorrelation for mother behavior, such that mother behavior at epoch 1 was associated with a higher frequency of mother behavior at epoch 2(βA1i = .419, p < .001, with 95% CI = [.409, .428]). We also found a similar autocorrelation for child behavior (βB1i = .537, p < .001, with 95% CI = [.528, .545]). Maternal and child behavioral contingency was also significant, such that child behavior at epoch 1 was associated with a lower frequency of mother behavior at epoch 2 and mother behavior at epoch 1 was associated with a lower frequency of child behavior at epoch 2 (βA2i =−.134, p < .001, with 95% CI = [−.197, −.071]; βB2i = −.094, p < .01, with 95% CI = [−.165, −.023]).
Table 3.
Behavioral Contingency MLM Analyses.
| Fixed Effects | Estimate | Std. Error | p-value | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| AM Intercept, βA0 | 1.36 | 0.03 | < .01** | 1.31 | 1.41 |
| AC Intercept, βB0 | 1.93 | 0.03 | < .01** | 1.87 | 1.99 |
| Auto-correlation Parent βA1 | 0.42 | 0.005 | < .01** | .41 | .43 |
| Auto-correlation Child βB1 | 0.54 | 0.004 | < .01** | .53 | .55 |
| Crosslag Parent-reacts-to-Child (MC) βA2 | −0.13 | 0.03 | < .01** | −.19 | −.07 |
| Crosslag Child-reacts-to-Parent (CM) βB2 | −0.09 | 0.04 | .01* | −.17 | −.02 |
| AM Dep x MC γA21 | 0.02 | 0.01 | < .01* | .01 | .03 |
| AM Dep x CM γB21 | 0.01 | 0.01 | .45 | −.01 | .01 |
| BM NA x MC γA22 | 0.02 | 0.01 | .02* | .003 | .034 |
| BM NA x CM γB22 | 0.02 | 0.01 | .04* | .001 | .035 |
| AM Dep x BM NA x MC γA23 | −0.005 | 0.001 | < .01* | −.007 | −.002 |
| AM Dep x BM NA x CM γB23 | −0.001 | 0.002 | .42 | −.004 | .002 |
| Random Effects | |||||
| SD of AM Intercept uA0i | 0.50 | .46 | .54 | ||
| SD of AC Intercept uB0i | 0.60 | .56 | .65 | ||
| Correlation uA0iuB0i | −0.23 | −.29 | −.18 | ||
| −2LL | −116,896.7 |
Note. AM = Adoptive Mother. AC = Adoptive Child. AM Dep = Adoptive Mother number of depressive symptoms. BM NA = Birth Mother temperamental negative affectivity.
indicates p < .05
indicates p < .001.
Both birth mother’s negative affect and adoptive mother’s depressive symptoms were significantly associated with maternal behavioral contingency, and there was also a significant interaction between the two on maternal behavioral contingency (γA21 = .018, p < .01, with 95% CI = [−.197, −.071]; (γA22 = .019, p = .021 l, with 95% CI = [.003, .034]; γA23 = −.005, p = .001, with 95% CI = [−.007, −.002]). As seen in Fig. 1, adoptive mothers with higher depressive symptoms were less contingent to children whose birth mothers reported high vs. low negative affectivity. Interestingly, however, adoptive mothers with few depressive symptoms were more contingent to children whose birth mothers reported high negative affectivity than those whose birth mothers reported low negative affectivity.
Fig. 1. Adoptive mother behavioral contingency by adoptive mother depressive symptoms.
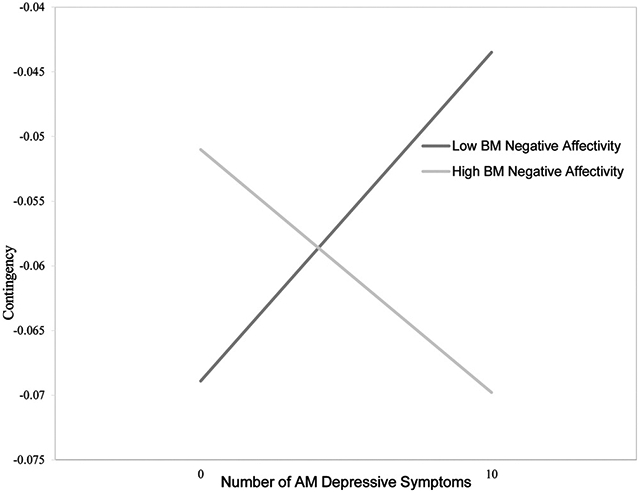
Note. “Number of AM Depressive Symptoms” refers to the number of depressive symptoms that were endorsed by adoptive mothers on the BDI at the 27-month assessment. BM Negative Affectivity refers to +/− 1 standard deviation from the mean level of children’s birth mother temperamental negative affectivity score.
The main effect of birth mother’s negative affectivity associated with child behavioral contingency was also significant (γB22 = .018, p = .046, with 95% CI = [.001, .035]). As negative affectivity increased, children showed a higher frequency of behavior following mother’s behavior.
3.3. 27-Month Negative Contingency Model
Again, note that we report unstandardized coefficients throughout our model to aid in interpretation. As described in Table 4, we found a significant autocorrelation for mother’s negative behavior, such that mother’s negative behavior at time 1 was associated with a higher frequency of mother’s negative behavior at time 2 (βA1i = .289, p < .001, with 95% CI = [.279, .299]). We also found a similar autocorrelation for child’s negative behavior (βB1i = .493, p < .001, with 95% CI = [.485, .502]). Maternal and child contingent negativity was not significant, such that child behavior at time 1 was not associated with frequency of mother behavior at time 2 and mother behavior at time 1 was not associated with frequency of child behavior at time 2 (βA2i = .029, p = .375, with 95% CI = [−.035, .093]; βB2i = −.044, p = .246, with 95% CI = [−.117, .030]).
Table 4.
Contingent Negativity MLM Analyses.
| Fixed Effects | Estimate | Std. Error | p-value | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| AM Intercept, βA0 | 0.52 | 0.02 | < .001** | .47 | .56 |
| AC Intercept, βB0 | 0.79 | 0.03 | < .001** | .72 | .85 |
| Auto-correlation Parent βA1 | 0.29 | 0.03 | < .001** | .28 | .29 |
| Auto-correlation Child βB1 | 0.49 | 0.004 | < .001** | .48 | .50 |
| Crosslag Parent-reacts-to-Child (MC) βA2 | 0.03 | 0.03 | .375 | −.04 | .09 |
| Crosslag Child-reacts-to-Parent (CM) βB2 | −0.04 | 0.04 | .246 | −.12 | .03 |
| AM Dep x MC γA21 | 0.009 | 0.01 | .137 | −.003 | .02 |
| AM Dep x CM γB21 | 0.012 | 0.006 | .048* | .0001 | .0246 |
| BM NA x MC γA22 | −0.002 | 0.008 | .857 | −.018 | .0146 |
| BM NA x CM γB22 | 0.016 | 0.009 | .092 | −.0026 | .0341 |
| AM Dep x BM NA x MC γA23 | −0.002 | 0.001 | .143 | −.0050 | .0007 |
| AM Dep x BM NA x CM γB23 | −0.003 | 0.002 | .025* | −.0063 | −.0004 |
| Random Effects | |||||
| SD of AM Intercept uA0i | .42 | .39 | .46 | ||
| SD of AC Intercept uB0i | .68 | .65 | .73 | ||
| Correlation uA0iuB0i | .04 | .04 | .06 | ||
| −2LL | −101,036.1 |
Note. AM = Adoptive Mother. AC = Adoptive Child. AM Dep = Adoptive Mother number of depressive symptoms. BM NA = Birth Mother temperamental negative affectivity.
indicates p < .05
indicates p < .001.
Adoptive mother’s depressive symptoms and birth mother’s negative affect were not associated with maternal contingent negativity, and the interaction between the two on maternal contingent negativity was also not significant. The main effect of adoptive mother’s depressive symptoms in the prediction of child contingent negativity was significant, and there was a significant interaction between adoptive mother’s depressive symptoms and birth mother’s negative affectivity on child contingent negativity (γB21 = .012, p = .048, with 95% CI = [.001, .025]; (γB23 = −.003, p = .025, with 95% CI = [−.006, −.001]). As seen in Fig. 2, and contrary to our expectations, for dyads of mothers with higher depressive symptoms, children with birth mothers who reported higher negative affectivity showed lower contingent negativity than those whose birth mothers reported lower negative affectivity. For dyads with mothers with fewer depressive symptoms, children with birth mothers with higher negative affectivity showed higher contingent negativity than other children with similar mothers.
Fig. 2. Adopted child contingent negativity by adoptive mother depressive symptoms.
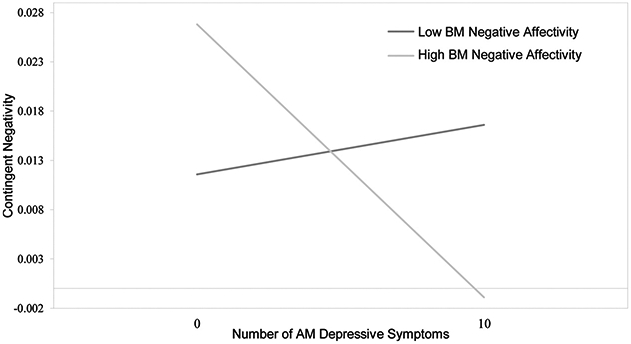
Note. “Number of AM Depressive Symptoms” refers to the number of depressive symptoms that were endorsed by adoptive mothers on the BDI at the 27-month assessment. BM Negative Affectivity refers to +/− 1 standard deviation from the mean level of children’s birth mother temperamental negative affectivity score.
4. Discussion
Goodman et al. (2011) identified a need for genetically informed research on mother-child interaction patterns that can clarify potential mechanisms of risk transmission of depressive symptoms from mothers to their young children. In this study we examined both behavioral contingency and contingent negativity to evaluate two theorized mechanisms of risk transmission. As maternal depressive symptoms increased, there were two distinct interaction patterns based on the dyad’s characteristics that matched previously theorized dyadic interactions (Goodman & Gotlib, 1999).
The first dyadic pattern resembled a withdrawn interaction style. Mothers showed low behavioral contingency and children showed low contingent negativity. This interaction style suggests a dyad where the mother and child are not as jointly engaged in the task as other dyads. The second dyadic pattern resembled a volatile interaction style. As maternal depressive symptomology increased, mothers showed higher behavioral contingency, and children showed higher contingent negativity. This would be a dyad where the mother and child are highly engaged in the task together, but when mothers acted negatively, their children responded more negatively than other children.
These dyadic interaction patterns are influenced by both heritable and environmental factors. Based on previous work, we had initially predicted that both adoptive and birth mother characteristics would be a risk factor for high contingent negativity (Goldsmith et al., 1997; Goodman, 2007; Lipscomb et al., 2011, 2014). However, in contrast to these expectations, children whose birth mothers had high negative affectivity showed the lowest contingent negativity. In these dyads, as adoptive mother’s depressive symptoms increased, children demonstrated a withdrawn interaction style. Conversely, as depressive symptoms increased, children whose birth mothers reported low negative affectivity showed a volatile interaction style. We found these patterns to be particularly interesting because even though few adoptive mothers in this sample reported clinical levels of depression, maternal depressive symptoms was still associated with differences in the parent-child interaction.
Prior research has shown that as maternal depressive symptomology increases, behavioral contingency decreases (Goodman & Gotlib, 1999). Notably, our study suggests that this is the case primarily for mothers of young children whose birth mothers self-report high negative affect. We speculate that such children may have a predisposition for more contingent negativity than other children. This in turn might lead to mothers becoming less behaviorally contingent because they have developed an expectation of unpleasant responses from their children. Similarly, children’s low contingent negativity may arise as an early form of learned helplessness. That is, they may show less contingent negativity in response to repeated maternal intrusive behavior. Low contingent negativity could also be linked with low maternal behavioral contingency, indicating that this dyad is not as jointly engaged as other dyads.
In contrast, the volatile mother-child interaction pattern occurred in dyads composed of children whose birth mothers reported low negative affectivity. As maternal depressive symptoms increased, these dyads showed higher maternal behavioral contingency paired with high child contingent negativity. Children who are less negatively reactive are better able to stay on task than other children (Goldsmith et al., 1997). These children may therefore experience their mothers’ level of contingency as intrusive because of their low heritable tendency for negative affectivity. This volatile interaction style may lead to a recurring cycle of negative mother-child interactions similar to Patterson’s (2002) coercive circle. Prior research had found similar patterns in young infants, such that mothers who were intrusive when their children were distressed showed more joint hostility in their interactions (Beebe et al., 2010).
Importantly, behavioral contingency is unique in its ability to capture both matched and mismatched responses. Previous contingency constructs have tended to focus on moments of matched affect, whereas behavioral contingency is better able to capture mismatched states which are most common in mother-child interactions (Tronick & Cohn, 1989). One example of a frequent mismatched response is structured parenting that is defined as moments when parents provide clear instructions and redirect children to the task at hand after they are off-task or disruptive. Previous work demonstrated that specific parent directives to children to stay on task is associated with better outcomes for children at high genetic risk for disruptive behavior (Leve et al., 2009). However, constructs like synchrony or mutuality would not be able to capture this adaptive parenting practice. Therefore, our construct of behavioral contingency expands on prior mother-child interaction research to allow researchers to capture these common mismatched responses between parents and children that other constructs could not.
We note that contingency analyses lack an agreed-upon standard for epoch length. Previous research used epochs of various lengths of 1-,3-, 5- and even 30-seconds (Feldman, 2003; Lindsey, Cremeens, Colwell, & Caldera, 2009; Roben et al., 2015; Tronick & Cohn, 1989). This has resulted in some studies capturing mere moments up to a minute of interaction time. Epoch length would, of course, influence the patterning of results and their meaning. Because it takes more than a second for a partner to perceive the other’s behavior, interpret it, and engage in a motor response, an epoch of one second would be too brief a period of time to capture the back and forth dynamic of dyad partners. Conversely, an epoch of 30 seconds would be too long; within that time frame, multiple actions and reactions could have occurred, but that variance would be collapsed into a single measurement score of behavior. However, the theoretical difference between 3- and 5-seconds is hard to parse, and the data-driven approach may help to empirically ascertain optimal epoch length. Similarly, previous research used a lag of one epoch to measure contingencies, and our study adds to the evidence-base for using lag-1 in contingency research.
One of the strengths of the current study was the use of a data-driven strategy to identify the most appropriate epoch and lag lengths for analysis. Comparing model fit between models with 1-, 2-, 3-, 4-, and 5-second epochs and the effect of one epoch to the next of lag-1, lag-2, and lag-3, we found that a 3-second epoch with lag-1 had the best model fit based on fit statistics and interpretability. Thus, future work in contingency research should use a data-driven process and carefully consider the epoch length and lag that may vary based children’s developmental status.
Our findings suggest that clinicians working with mothers with depressive symptoms may wish to observe dyadic interactions before implementing treatment. Notably, our study is unable to suggest or describe an “ideal” level of behavioral contingency, which is likely to vary by the specific behavioral context as well as the developmental needs of the child. It might be appropriate to reduce some mothers’ level of contingency to their children so that the children can practice more autonomy. However, for other mothers, it might be appropriate to increase the mothers' level of contingency to their children to stimulate a more interactive mother-child dyadic interaction. Intervention programs, such as Attachment and Biobehavioral Catch-up (Bernard et al., 2012), Parent-Child Interaction Therapy (Eyberg, 1988), and other attachment-based intervention programs (e.g. PRERAYMI; Riva Crugnola et al., 2016) explicitly have clinicians focus on improving the quality of the parent-child relationship.The results of this study suggest that these interaction patterns should be closely monitored to guide recommendations for comparable treatment modalities. While this study was unable to examine how dyadic interaction patterns affected mother and child outcomes, it illuminates distinct differences in how dyads interact based on their characteristics.
5. Limitations and Future Directions
Adoptive families in this study were drawn from a predominantly White, higher SES, community sample with relatively low levels of depressive symptomology. It would therefore be important to replicate the findings of the study to see whether they are present in more racially, socioeconomically, and clinically diverse samples. Furthermore, we chose to focus on birth mother temperamental negative affectivity as a proxy influence on child negative emotionality. However, replications and extensions of these findings also should consider other indices of genetic influences on the child, such as birth parents’ general psychopathology, internalizing problems, or other characteristics. Although there were significant associations between the interaction of birth mother and adoptive mother characteristics with mother-child contingencies, it should be noted that the confidence intervals were close to zero. It is possible that other birth parent characteristics may show stronger links with mother-child contingencies than temperamental negative affectivity in birth mothers. That being said, to inform our understanding of how dyadic interaction patterns are associated with parental characteristics and behaviors, we also recommend future research examine birth fathers’ temperamental characteristics, adoptive father-child observation data, and the influence of child gender.
A strength of our study was in the inclusion of mismatched states in the evaluation of dyadic responsiveness in our behavioral contingency model. However, it may be that the directionality of mismatched responses may have differential effects on the mother-child relationship. For example, a mother responding negatively to a child’s positive behavior may likely predict outcomes that are distinct from a mother responding positively to a child’s negative behavior. However, an investigation of these mismatched responses was beyond the scope of this study, and we recommend that future work examine these mismatched responses using the same statistical approach as our contingent negativity model. Relatedly, we examined moment-to-moment dyadic interactions at age 27-months. To determine whether these associations persist into the early preschool and school entry periods, we recommend future studies also examine the predictive power of mother and child contingencies on child behavior problems and maternal well-being at these later ages. It may be that the lower maternal contingency of depressed mothers is a protective factor because it reduces children’s exposure to aversive characteristics of maternal depressive symptoms. Roben et al. (2015) had found that higher child contingent negativity at 18-months was related to greater maternal depressive symptoms at 27-months. Future studies are encouraged to determine whether mothers showed less contingency in response to countless negative interactions with more negative reactive adopted children, whereas other mothers showed more contingency with their less negative reactive adopted children.
6. Summary and Conclusions
Although an extensive literature exists that has documented the negative influence of maternal depressive symptoms on child outcome, the literature documenting bidirectional influences on interaction quality is substantially smaller, and the literature examining moderating influences on these transactions, smaller still. To help fill this relative gap in the literature, and using a data-driven approach to identify the most appropriate epoch length, this study examined the moderating influences of heritable child characteristics and maternal depressive symptoms on bidirectional transactions between mothers’ and children. This approach offered surprising findings. Even among mothers with generally normative levels of depressive symptoms, we found that as maternal depressive symptoms increased, dyads composed of children whose birth mothers reported high negative affectivity showed the lowest level of maternal behavioral contingency and child contingent negativity, in what we interpreted as an early form of learned helplessness. Also, as maternal depressive symptoms increased, dyads composed of children whose birth mothers reported low negative affectivity showed more maternal behavioral contingency and more child contingent negativity than other dyads. A more nuanced understanding of mother-child interaction patterns may help interventionists tailor their treatments to increase or decrease maternal behavioral contingency as an intervention target, thereby reducing the deleterious effects of maternal depressive symptoms.
Supplementary Material
Footnotes
Appendix A. Supplementary data
Supplementary material related to this article can be found, in the online version, at doi:https://doi.org/10.1016/j.infbeh.2020.101478.
References
- Beck AT, Steer RA, & Brown GK (1996). Beck depression inventory-II. San Antonio, 78(2), 490–498. [Google Scholar]
- Beebe B, Jaffe J, Markese S, Buck K, Chen H, Cohen P, … Feldstein S (2010). The origins of 12-month attachment: a microanalysis of 4-month mother-infant interaction. Attachment & human development, 12(1-2), 3–141. 10.1080/14616730903338985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bell RQ, & Bell RQ (1968). Effects in Studies of Socialization. Psychological Review, 75(2), 81–95. 10.1037/h0025583. [DOI] [PubMed] [Google Scholar]
- Belsky J (1984). The determinants of parenting: A process model. Child Development, 83–96. 10.2307/1129836. [DOI] [PubMed] [Google Scholar]
- Belsky J, Booth-LaForce CL, Bradley R, Brownell CA, Burchinal M, Campbell SB, … Kelly JF (2006). Infant-mother attachment classification: Risk and protection in relation to changing maternal caregiving quality. Developmental Psychology, 42(1), 38–58. 10.1037/0012-1649.42.1.38. [DOI] [PubMed] [Google Scholar]
- Bernard K, Dozier M, Bick J, Lewis-Morrarty E, Lindhiem O, & Carlson E (2012). Enhancing attachment organization among maltreated children: Results of a randomized clinical trial. Child Development, 83(2), 623 10.1111/j.1467-8624.2011.01712.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blair C, Granger DA, Willoughby M, Mills-Koonce R, Cox M, Greenberg MT, … FLP Investigators (2011). Salivary cortisol mediates effects of poverty and parenting on executive functions in early childhood. Child development, 82(6), 1970–1984. 10.1111/j.1467-8624.2011.01643.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bolger N, Davis A, & Rafaeli E (2003). Diary methods: Capturing life as it is lived. Annual Review of Psychology, 54(1), 579–616. 10.1146/annurev.psych.54.10160. [DOI] [PubMed] [Google Scholar]
- Cohn JF, & Tronick EZ (1988). Mother-infant face-to-face interaction: Influence is bidirectional and unrelated to periodic cycles in either partner’s behavior. Developmental Psychopathology, 24, 386–392. 10.1037/0012-1649.24.3.386. [DOI] [Google Scholar]
- Cohn JF, & Tronick E (1989). Specificity of infants’ response to mothers’ affective behavior. Journal of the American Academy of Child & Adolescent Psychiatry, 28(2), 242–248. 10.1097/00004583-198903000-00016. [DOI] [PubMed] [Google Scholar]
- Dix T, Meunier L, Lusk K, & Perfect M (2012). Mothers’ depressive symptoms and children’s facial emotions: Examining the depression–inhibition hypothesis. Development and Psychopathology, 24(1), 195–210. 10.1017/S0954579411000770. [DOI] [PubMed] [Google Scholar]
- Deater-Deckard K, & Petrill SA (2004). Parent–child dyadic mutuality and child behavior problems: An investigation of gene–environment processes. Journal of Child Psychology and Psychiatry, 45(6), 1171–1179. 10.1111/j.1469-7610.2004.00309.x. [DOI] [PubMed] [Google Scholar]
- Derryberry D, & Rothbart MK (1988). Arousal, affect, and attention as components of temperament. Journal of Personality and Social Psychology, 55(6), 958 10.1037/0022-3514.55.6.958. [DOI] [PubMed] [Google Scholar]
- Egeland B, & Hiester M (1993). Teaching task rating scales. Institute of Child Development, University of Minnesota. [Google Scholar]
- Eyberg S (1988). Parent-child interaction therapy: Integration of traditional and behavioral concerns. Child & Family Behavior Therapy, 10(1), 33–46. 10.1300/J019vl0n01_04. [DOI] [Google Scholar]
- Feldman R (2003). Infant-mother and infant-father synchrony: The coregulation of positive arousal. Infant Mental Health Journal, 24(1), 1–23. 10.1002/imhj.10041. [DOI] [Google Scholar]
- Feldman R (2007). Parent-infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. Journal of Child Psychology and Psychiatry and Allied Disciplines, 48(3-4), 329–354. 10.1111/j.1469-7610.2006.01701.x. [DOI] [PubMed] [Google Scholar]
- Feldman R (2015). Mutual influences between child emotion regulation and parent-child reciprocity support development across the first 10 years of life: Implications for developmental psychopathology. Development and Psychopathology, 27(4), 1007–1023. 10.1017/S0954579415000656. [DOI] [PubMed] [Google Scholar]
- Feldman R, Greenbaum CW, & Yirmiya N (1999). Mother-infant affect synchrony as an antecedent of the emergence of self-control. Developmental Psychology, 35(1), 223–231. 10.1037/0012-1649.35.1.223. [DOI] [PubMed] [Google Scholar]
- Field T, Healy BT, Goldstein S, & Guthertz M (1990). Behavior-state matching and synchrony in mother-infant interactions of nondepressed versus depressed dyads. Developmental Psychology, 26(1), 7–14. 10.1037/0012-1649.26.1.7. [DOI] [Google Scholar]
- Field T, Healy B, & LeBlanc WG (1989). Sharing and synchrony of behavior states and heart rate in nondepressed versus depressed mother-infant interactions. Infant Behavior and Development, 12(3), 357–376. 10.1016/0163-6383(89)90044-1. [DOI] [Google Scholar]
- Forman DR, & Kochanska G (2001). Viewing imitation as child responsiveness: A link between teaching and discipline domains of socialization. Developmental Psychology, 37(2), 198 10.1037/0012-1649.37.2.198. [DOI] [PubMed] [Google Scholar]
- Gelfand DM, & Teti DM (1990). The effects of maternal depression on children. Clinical Psychology Review, 10(3), 329–353. 10.1016/0272-7358(90)90065-1. [DOI] [Google Scholar]
- Goldsmith HH, Buss KA, & Lemery KS (1997). Toddler and childhood temperament: Expanded content, stronger genetic evidence, new evidence for the importance of environment. Developmental Psychology, 33(6), 891 10.1037/0012-1649.33.6.891. [DOI] [PubMed] [Google Scholar]
- Goodman SH (2007). Depression in mothers. Annual Review of Clinical Psychology, 3, 107–135. 10.1146/annurev.clinpsy.3.02280. [DOI] [PubMed] [Google Scholar]
- Goodman SH, & Gotlib IH (1999). Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission. Psychological Review, 106(3), 458 10.1037/0033-295X.106.3.458. [DOI] [PubMed] [Google Scholar]
- Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, & Heyward D (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. 10.1007/s10567-010-0080-1. [DOI] [PubMed] [Google Scholar]
- Gross HE, Shaw DS, & Moilanen KL (2008). Reciprocal associations between boys’ externalizing problems and mothers’ depressive symptoms. Journal of Abnormal Child Psychology, 36(5), 693–709. 10.1007/s10802-008-9224-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammen C (2002). Context of stress in families of children with depressed parents In Goodman SH, & Gotlib IH (Eds.). Children of depressed parents: Mechanisms of risk and implications for treatment (pp. 175–202). Washington, DC: American Psychological Association. [Google Scholar]
- Henderson EN, & Jennings KD (2003). Maternal depression and the ability to facilitate joint attention with 18-month-olds. Infancy, 4(1), 27–46. 10.1207/s15327078in0401_2. [DOI] [Google Scholar]
- Hox JJ, Moerbeek M, & Van de Schoot R (2017). Multilevel analysis: Techniques and applications. Routledge; https://doi.org/l0.1007/s10802-013-9711-6. [Google Scholar]
- Kerr DC, Leve LD, Harold GT, Natsuaki MN, Neiderhiser JM, Shaw DS, … Reiss D (2013). Influences of biological and adoptive mothers’ depression and antisocial behavior on adoptees’ early behavior trajectories. Journal of Abnormal Child Psychology, 41(5), 723–734. 10.1007/s10802-013-9711-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim S, & Kochanska G (2012). Child temperament moderates effects of parent–child mutuality on self-regulation: A relationship-based path for emotionally negative infants. Child Development, 83(4), 1275–1289. 10.1111/j.1467-8624.2012.01778.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenig JL, Barry RA, & Kochanska G (2010). Rearing difficult children: Parents’ personality and children’s proneness to anger as predictors of future parenting. Parenting 10(4), 258–273. 10.1080/15295192.2010.492038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leadbeater BJ, Bishop SJ, & Raver CC (1996). Quality of mother-toddler interactions, maternal depressive symptoms, and behavior problems in preschoolers of adolescent mothers. Developmental Psychology, 32(2), 280 10.1037/0012-1649.32.2.280. [DOI] [Google Scholar]
- Leelère C, Viaux S, Avril M, Achard C, Chetouani M, Missonnier S, … Cohen D (2014). Why synchrony matters during mother-child interactions: a systematic review. PLoS one, 9(12), 1–34. 10.1371/journal.pone.0113571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Harold GT, Ge X, Neiderhiser JM, Shaw D, Scaramella LV, … Reiss D (2009). Structured parenting of toddlers at high versus low genetic risk: Two pathways to child problems. Journal of the American Academy of Child and Adolescent Psychiatry, 48(11), 1102–1109. 10.1097/CHI.0b013e3181b8bfc0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Neiderhiser JM, Ganiban JM, Natsuaki MN, Shaw DS, & Reiss D (2019). The early growth and development study: A dual-family adoption study from birth through adolescence. Twin Research and Human Genetics, 1–12. 10.1017/thg.2019.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsey EW, Cremeens PR, Colwell MJ, & Caldera YM (2009). The structure of parent-child dyadic synchrony in toddlerhood and children’s communication competence and self-control. Social Development, 18(2), 375–396. 10.1111/j.1467-9507.2008.00489.x. [DOI] [Google Scholar]
- Lipscomb ST, Leve LD, Harold GT, Neiderhiser JM, Shaw DS, Ge X, … Reiss D (2011). Trajectories of parenting and child negative emotionality during infancy and toddlerhood: A longitudinal analysis. Child Development, 82(5), 1661–1675. 10.1111/j.1467-8624.2011.01639.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipscomb ST, Laurent H, Neiderhiser JM, Shaw DS, Natsuaki MN, Reiss D, … Leve LD (2014). Genetic vulnerability interacts with parenting and early care education to predict increasing externalizing behavior. International Journal of Behavioral Development, 38(1), 70–80. 10.1177/0165025413508708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacCallum RC, Kim C, Malarkey WB, & Kiecolt-Glaser JK (1997). Studying multivariate change using multilevel models and latent curve models. Multivariate Behavioral Research, 32(3), 215–253. 10.1207/s15327906mbr3203_1. [DOI] [PubMed] [Google Scholar]
- Moore GA, & Calkins SD (2004). Infants’ vagal regulation in the still-face paradigm is related to dyadic coordination of mother-infant interaction. Developmental Psychology, 40, 1068–1080. 10.1037/0012-1649.40.6.1068. [DOI] [PubMed] [Google Scholar]
- Moore GA, Cohn JF, & Campbell SB (2001). Infant affective responses to mother’s still face at 6 months differentially predict externalizing and internalizing behaviors at 18 months. Developmental Psychology, 37, 706–714. 10.1037/0012-1649.37.5.706. [DOI] [PubMed] [Google Scholar]
- Moore GA, Teti LO, & Roben CKP (2009). Early Growth and Development Study (EGDS) microcoding manual for the Parent–Child Teaching Task. Unpublished manuscriptUniversity Park, PA: The Pennsylvania State University. [Google Scholar]
- Mott SL, Schiller CE, Richards JG, O’Hara MW, & Stuart S (2011). Depression and anxiety among postpartum and adoptive mothers. Archives of Women’s Mental Health, 14(4), 335–343. 10.1007/s00737-011-0227-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Natsuaki MN, Shaw DS, Neiderhiser JM, Ganiban JM, Harold GT, Reiss D, … Leve LD (2014). Raised by depressed parents: is it an environmental risk? Clinical Child and Family Psychology Review, 17(4), 357–367. 10.1007/s10567-014-0169-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Page M, Wilhelm MS, Gamble WC, & Card NA (2010). A comparison of maternal sensitivity and verbal stimulation as unique predictors of infant social-emotional and cognitive development. Infant Behavior and Development, 33(1), 101–110. 10.1016/j.infbeh.2009.12.001. [DOI] [PubMed] [Google Scholar]
- Pardini D, Fite PJ, & Burke JD (2008). Bidirectional associations between parenting practices and conduct problems in boys from childhood to adolescence: The moderating effect of age and African-American ethnicity. Journal of Abnormal Child Psychology, 36(5), 647–662. 10.1007/s10802-007-9162-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR (2002). The early development of coercive family process In Reid JB, Patterson GR, & Snyder J (Eds.). Antisocial behavior in children and adolescents: A developmental analysis and model for intervention; antisocial behavior in children and adolescents: A developmental analysis and model for intervention (pp. 25–44). Washington, DC: American Psychological Association Chapter xi, 337 Pages. [Google Scholar]
- Pinheiro J, Bats D, DebRoy S, Sarkar DRCT, & R CORE TEAM (2018). nmle: Linear and nonlinear mixed effects models. [Google Scholar]
- R Core Team (2013). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. [Google Scholar]
- Raudenbush SW, & Bryk AS (2002). Hierarchical linear models: Applications and data analysis methods, Vol. 1 Sage. [Google Scholar]
- Riva Crugnola C, Ierardi E, Albizzati A, & Downing G (2016). Effectiveness of an Attachment-Based Intervention Program in Promoting Emotion Regulation and Attachment in Adolescent Mothers and their Infants: A Pilot Study. Frontiers in Psychology, 7(195), 1–17. 10.1002/icd.1906 doi:. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roben CK, Moore GA, Cole PM, Molenaar P, Leve LD, Shaw DS, … Neiderhiser JM (2015). Transactional patterns of maternal depressive symptoms and mother–child mutual negativity in an adoption sample. Infant and Child Development, 24(3), 322–342. 10.1002/icd.1906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodriguez ML, Ayduk O, Aber JL, Mischel W, Sethi A, & Shoda Y (2005). Contextual Approach to the Development of Self-regulatory Competencies: The Role of Maternal Unresponsivity and Toddlers’ Negative Affect in Stressful Situations. SocialDevelopment, 14(1), 136–157. 10.1111/j.1467-9507.2005.00294.x. [DOI] [Google Scholar]
- Rutter M (2007). Gene-environment interdependence. Developmental Science, 10(1), 12–18. [DOI] [PubMed] [Google Scholar]
- Sameroff A (1975). Transactional models in early social relations. Human Development, 18(1–2), 65–79. 10.1159/000271476. [DOI] [Google Scholar]
- Sameroff A (2009). The transactional model In Sameroff A (Ed.). The transactional model of development: How children and contexts shape each other (pp. 3–21). Washington, DC, US: American Psychological Association, 10.1037/11877-001. [DOI] [Google Scholar]
- Searle SR, Casella G, & McCulloch CE (1992). Variance components. Hoboken: John Wiley & Sons. [Google Scholar]
- Shaw DS, Schonberg M, Sherrill J, Huffman D, Lukon J, Obrosky D, … Kovacs M (2006). Responsivity to offspring’s expression of emotion among childhood-onset depressed mothers. Journal of Clinical Child & Adolescent Psychology, 35(4), 490–503. 10.1207/s15374424jccp3504_1. [DOI] [PubMed] [Google Scholar]
- Tronick EZ (1989). Emotions and Emotional Communication in Infants. American Psychologist, 44(2), 112–119. 10.1037/0003-066X.44.2.112. [DOI] [PubMed] [Google Scholar]
- Tronick EZ, & Cohn JF (1989). Infant-mother face-to-face interaction: age and gender differences in coordination and the occurrence of miscoordination. Child Development, 60(1), 85–92. 10.2307/1131074. [DOI] [PubMed] [Google Scholar]
- Tronick E, & Reck C (2009). Infants of depressed mothers. Harvard Review of Psychiatry, 17(2), 147–156. 10.1080/10673220902899714. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.