

This cross-sectional study assesses potential opportunities for genotype-guided prescribing in pediatric populations among multiple health systems by examining the prevalence of prescriptions for each drug with the highest level of evidence and estimating the prevalence of potentially actionable prescribing decisions.
Key Points
Question
What is the opportunity for genotype-guided prescribing among pediatric patients in the US?
Findings
In this serial cross-sectional study of annual prescribing data at 16 health systems representing approximately 2.9 million pediatric patients per year from 2011 to 2017, the annual prevalence of exposure to at least 1 Clinical Pharmacogenetics Implementation Consortium level A drug ranged from 7987 to 10 629 per 100 000 pediatric patients, with increasing prevalence before reaching a plateau in 2014. The medications with the highest potential for actionability were analgesics (oxycodone, codeine, and tramadol), the antiemetic ondansetron, and antidepressants (citalopram, escitalopram, and amitriptyline).
Meaning
These findings suggest that ample opportunity exists for genotype-guided prescribing among pediatric patients in the US, especially for drugs metabolized by CYP2D6 or CYP2C19.
Abstract
Importance
Genotype-guided prescribing in pediatrics could prevent adverse drug reactions and improve therapeutic response. Clinical pharmacogenetic implementation guidelines are available for many medications commonly prescribed to children. Frequencies of medication prescription and actionable genotypes (genotypes where a prescribing change may be indicated) inform the potential value of pharmacogenetic implementation.
Objective
To assess potential opportunities for genotype-guided prescribing in pediatric populations among multiple health systems by examining the prevalence of prescriptions for each drug with the highest level of evidence (Clinical Pharmacogenetics Implementation Consortium level A) and estimating the prevalence of potential actionable prescribing decisions.
Design, Setting, and Participants
This serial cross-sectional study of prescribing prevalences in 16 health systems included electronic health records data from pediatric inpatient and outpatient encounters from January 1, 2011, to December 31, 2017. The health systems included academic medical centers with free-standing children’s hospitals and community hospitals that were part of an adult health care system. Participants included approximately 2.9 million patients younger than 21 years observed per year. Data were analyzed from June 5, 2018, to April 14, 2020.
Exposures
Prescription of 38 level A medications based on electronic health records.
Main Outcomes and Measures
Annual prevalence of level A medication prescribing and estimated actionable exposures, calculated by combining estimated site-year prevalences across sites with each site weighted equally.
Results
Data from approximately 2.9 million pediatric patients (median age, 8 [interquartile range, 2-16] years; 50.7% female, 62.3% White) were analyzed for a typical calendar year. The annual prescribing prevalence of at least 1 level A drug ranged from 7987 to 10 629 per 100 000 patients with increasing trends from 2011 to 2014. The most prescribed level A drug was the antiemetic ondansetron (annual prevalence of exposure, 8107 [95% CI, 8077-8137] per 100 000 children). Among commonly prescribed opioids, annual prevalence per 100 000 patients was 295 (95% CI, 273-317) for tramadol, 571 (95% CI, 557-586) for codeine, and 2116 (95% CI, 2097-2135) for oxycodone. The antidepressants citalopram, escitalopram, and amitriptyline were also commonly prescribed (annual prevalence, approximately 250 per 100 000 patients for each). Estimated prevalences of actionable exposures were highest for oxycodone and ondansetron (>300 per 100 000 patients annually). CYP2D6 and CYP2C19 substrates were more frequently prescribed than medications influenced by other genes.
Conclusions and Relevance
These findings suggest that opportunities for pharmacogenetic implementation among pediatric patients in the US are abundant. As expected, the greatest opportunity exists with implementing CYP2D6 and CYP2C19 pharmacogenetic guidance for commonly prescribed antiemetics, analgesics, and antidepressants.
Introduction
Pharmacogenetics is a key component of precision medicine that uses genetic information to guide drug selection and dosing decisions.1 More than 100 commercially available drugs in the US contain pharmacogenetic information in the US Food and Drug Administration (FDA) label, including therapeutic management recommendations and warnings about the potential effects on drug safety, response, or potential alterations in pharmacokinetic parameters.2,3 The Clinical Pharmacogenetics Implementation Consortium (CPIC) publishes evidence-based, drug-centric, peer-reviewed guidelines for how to translate genetic test results into actionable prescribing decisions.4,5,6 During the last decade, CPIC has published guidelines on more than 35 gene-drug pairs as CPIC level A, indicating that a prescribing action is recommended when genotype information is available and that the preponderance of evidence is high or moderate in favor of changing prescribing.7
Although most pharmacogenetic research to date has focused on adults, the potential benefits of genotype-guided therapy in children are increasingly recognized.8,9,10 Many CPIC guidelines suggest application of genotype-guided therapy in both adults and children, whereas some CPIC guidelines contain unique recommendations for children (eg, voriconazole, atomoxetine, and warfarin), owing to ontogeny or other pediatric considerations.11,12,13 There is at least 1 example of a greater effect of a pharmacogenetic variant in children than adults that involves the drug transporter SLCO1B1 and simvastatin.14 Thus, the opportunity exists for more personalized pharmacotherapy in the pediatric population; however, widespread clinical implementation is challenging.
Data on trends of the prevalence of relevant prescriptions over time are crucial to informing pharmacogenetic implementation. The utility of pharmacogenetic testing depends on the frequency of prescribed medications with an actionable association and can rapidly change with the introduction of new drugs, the availability of generics or different formulations, changes in pricing, revised FDA guidance, and decisions by health care payers, health care institutions, and prescribers. Prescribing trends can also inform which genes to test, the opportunity for reuse of results during a lifetime (when a second drug associated with the same gene is prescribed), and the use of multigene panel-based tests.
In 2013, the National Institutes of Health funded the IGNITE (Implementing Genomics in Practice) Network, including 6 member sites, 15 affiliate sites, and a coordinating center, to support the development, investigation, and dissemination of genomic-guided practice models that seamlessly integrate such data into the electronic health record (EHR).15 We leveraged the IGNITE Network to conduct a retrospective, longitudinal analysis of the annual prevalence of prescriptions for CPIC level A drugs among pediatric patients (aged <21 years) across multiple types of health systems and population demographics. Our objective was to assess potential opportunities for genotype-guided prescribing in pediatric populations among multiple health systems by examining the prevalence of prescriptions for each CPIC level A drug and estimating the prevalence of potentially actionable prescribing decisions.
Methods
Overview
This serial, cross-sectional study assessed prescribing prevalence patterns across 16 health systems. In lieu of transferring patient data from each site, each site summarized individual-level data in a standardized format using demographic, temporal, drug, and gene characteristics. Aggregate data were then provided for central analysis. We estimated prescribing prevalences for each CPIC level A drug per site and across calendar years. Because some sites did not have data for all years, we used logistic regression to estimate prevalences over time for each site. We then summarized results to calculate across-site prevalence of exposure for each drug, drug class, and gene of interest. Additional details on the methods are available in the eMethods in the Supplement. This report adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.16
Participating Sites
The work reported was developed within the IGNITE Pharmacogenetics Working Group.17 All member and affiliate sites with pediatric data were invited to participate in the study. All participating sites signed a collaborative agreement and obtained approval from their respective institutional review boards for all data abstraction and reporting. The need for informed consent was waived for this use of deidentified data.
Study Medications and Genes
At the time the study analysis was begun (June 5, 2018), the list of 39 CPIC level A drugs and 20 associated genes (eTable 1 in the Supplement) was obtained from the CPIC website (https://cpicpgx.org/genes-drugs/). Because 1 level A drug, tropisetron, is not available in the US, we studied 38 medications. Three medications (warfarin, clopidogrel, and simvastatin) had clinical pharmacogenetic testing available during the study time frame at some sites; thus, data about alternative therapies were also obtained to enable accurate assessment of pharmacogenetic opportunity. For each drug, the RxNorm term for the ingredient was used to generate a list of all medications and formulations, including combination therapies, containing that ingredient. Formulations without systemic exposure (eg, topical formulations) were excluded. The list of drug ingredients, RxNorm terms, and all compiled generic and brand-name medications containing CPIC level A drugs from an Epic Clarity system (EPIC Systems Corporation) was provided to each site for subsequent site-level validation and adjustment as needed to support complete data capture. Prescription data collected included both inpatient and outpatient exposures at all sites except as indicated in eTable 2 in the Supplement.
Data Collection and Aggregation
Collection of data including demographics and prescribing and encounter information was completed at each site and uniformly structured according to the study data dictionary. The annual number of unique individuals with encounters where a prescription may have been provided was reported by each site to serve as the denominator for prevalence estimates. R scripts were developed, tested, and disseminated to aggregate individual-level prescription data by specific characteristics. Similarly, corresponding R scripts were developed to capture the number of unique patients with at least 1 encounter (within each subgroup as defined by patient characteristics) to estimate annual prescribing prevalence; each site submitted aggregate data for analyses.
Statistical Analysis
Data were analyzed from June 5, 2018, to April 14, 2020. For demographic characteristics at each site, we calculated summary statistics on an annual basis and summarized prevalence estimates as the median across calendar years. We then combined site-specific summaries to obtain overall summaries as shown in Table 1.
Table 1. Characteristics of the Patient Populations Across 16 Sites Observed From 2011 to 2017a.
| Characteristic | Data |
|---|---|
| No. of sites | 16 |
| No. of academic medical centers | 12 |
| No. of community hospitals or clinic systems | 4 |
| Age, y | |
| 25th Percentile | 3.00 (2.00-3.75) |
| 50th Percentile | 8.00 (7.00-10.00) |
| 75th Percentile | 14.00 (12.00-16.25) |
| Female, % | 50.7 (47.4-67.7) |
| Race/ethnicity, % | |
| White | 62.3 (12.2-86.9) |
| Black | 18.0 (6.8-70.2) |
| Asian | 1.4 (0.2-11.3) |
| American Indian or Alaska Native | 0.2 (0.0-1.0) |
| Pacific Islander | 0.1 (0.0-1.1) |
| Other or unknown | 11.1 (2.6-58.2) |
| Unique patients with encounters per year | 96 597 (4790-799 964) |
| Sum of medians across sites | 2 866 887 |
| Unique patients with target prescriptions per yearb | 6057 (238-38 230) |
| Sum of medians across sites | 197 409 |
Unless otherwise indicated, data are expressed as median (range). Summary statistics were derived from site-level, across-year medians. For example, the median (range) of unique patients with encounters was derived by calculating the site-specific median number of encounters per year across observed years and then calculating the median (range) of the site-specific median values. For the 25th percentile of age summary, at each site, we calculated the 25th percentile of age each year and then used the median of those values. The median (range) is reported in the table as the across-sites median (range) of the site-specific median values for the 25th percentiles.
Target prescriptions defined as Clinical Pharmacogenetics Implementation Consortium level A drugs or alternative medications within the class.
Prescribing Patterns Over Time
Not every site was able to provide data for all years included in the analysis. Thus, we used logistic regression to estimate site-specific prevalence of prescriptions from 2011 to 2017 for each of the following: (1) any CPIC level A medication; (2) at least 1, 2, 3, and 4 CPIC level A medications; (3) distinct classes of CPIC level A medications (eg, analgesics, statins, anticoagulants); (4) individual CPIC level A medications; and (5) medications with associated genes. Each model included site-by-year interactions, allowing us to estimate the annual site-specific prescription prevalences for each medication, which we combined across sites to obtain overall, annual prescription prevalences, as described below. Missing data for 2 or fewer consecutive years were assumed to be missing at random. When data were missing for more than 2 consecutive years, the time trend for the site was removed to avoid excessive extrapolation with a nonlinear function. Annual prescription prevalence is expressed per 100 000 unique individuals with at least 1 inpatient or outpatient encounter that year. Primary data analyses combined site-year prevalences across sites with each site weighted equally. Because of site-to-site variability in sample sizes (see eTable 2 in the Supplement), we performed a sensitivity analysis using patient weighting, which weighted sites in proportion to the number of patients with encounters at that site.
One challenge with these analyses was that not all sites contributed prescribing data for all years. Because the availability, or lack thereof, of prescribing data relied on an operational and compatible EHR system and was unlikely to be related to prescribing patterns themselves, we assumed the data were missing at random when sites were missing data for 1 or 2 consecutive years. If more than 2 consecutive years were missing within a site, we removed the site-specific time trend and estimated a single site-specific prevalence. Similarly, if there were fewer than 20 prescriptions for a medication in any year within a site, we removed the time trend for that site to avoid highly variable estimates and instead estimated a single site-specific prevalence across all years.
Prescribing Patterns by Demographic Characteristics
To examine the association of sex, race, and age with prescribing patterns, we used methods similar to those described above and detailed in the eMethods in the Supplement. For example, to estimate prescribing patterns across the age distribution, we removed terms for year and the site-by-year interaction and added a term for age using restricted cubic spline functions to the models above to permit nonlinear age trends. To estimate the frequency of actionable exposures based on demographic data, the frequency of actionable phenotypes by ancestry was extracted from the gene’s supplemental table on the CPIC website.7 For CYP2D6, activity scores of 1 were assigned the normal metabolizer phenotype, because this work predated the updated CYP2D6 genotype-to-phenotype translation guideline.18
Results
Study Cohort
Data from approximately 2.9 million pediatric patients (median age, 8 [interquartile range, 2-16] years; 50.7% female and 49.3% male; 62.3% White) were analyzed for a typical calendar year. Table 1 and eTable 2 in the Supplement describe characteristics of the 16 participating sites and demographic data for the pediatric populations with encounters. Twelve of the sites are academic medical centers, 2 of which contributed data from a community hospital or clinic system. Four sites are community hospitals or clinic systems. Six of the sites provided data from a free-standing children’s hospital. The 16 sites ranged in pediatric patient volume (median number of unique patients with encounters per year) from 4790 to 799 964 per year; the sum of these medians across all 16 sites is 2 866 887 individuals, representing the estimated annual number of individuals observed. The median number of unique patients per year with prescriptions for CPIC level A drugs or their alternatives ranged from 238 to 38 230; the sum of these annual medians is 197 409 individuals.
Prevalence of Exposure to CPIC Level A drugs
Figure 1A depicts the estimated annual prevalence of exposure to at least 1 CPIC level A drug per 100 000 patients, which ranged from 7987 to 10 629 during the study years. This prevalence increased from 7987 in 2011 to 10 415 in 2014, where it remained stable through 2017 (±200) (Figure 1A). The most prescribed CPIC level A drug was the antiemetic ondansetron (annual prevalence of exposure, 8107 [95% CI, 8077-8137] per 100 000 patients [Table 2]). The opioids tramadol (prescription prevalence, 295 [95% CI, 273-317] per 100 000 patients annually), codeine (571 [95% CI, 557-586] per 100 000 patients annually), and oxycodone (2116 [95% CI, 2097-2135] per 100 000 patients annually) were commonly prescribed. The antidepressants citalopram, escitalopram, and amitriptyline were also commonly prescribed (annual prevalence, approximately 250 per 100 000 patients each). There was wide variation across sites, from persistently less than 5000 to 30 000 or more prescriptions per 100 000 patients. In the sensitivity analysis using by-patient weighting, the estimated annual prevalences across all sites were lower (larger sites had lower prescription prevalence [eg, site 11]) and ranged from 5275 to 6892. When exposure to multiple CPIC level A drugs was assessed, we observed that the annual prevalence of exposure to at least 2 CPIC level A drugs increased from 1468 (in 2011) to 2157 (in 2017) per 100 000 patients (Figure 1B). The age of exposure to at least 1 CPIC level A drug, assessed using 2015 data, indicated an early peak around 5 years of age and a second increase in exposure around 15 years of age (eFigure 1 in the Supplement). Examination of specific drugs revealed that ondansetron exposure peaked at 4 to 5 years of age, and escitalopram exposure peaked at approximately 15 years of age (eFigure 2 in the Supplement).
Figure 1. Annual Prevalence of Exposure to at Least 1 Clinical Pharmacogenetics Implementation Consortium (CPIC) Level A Medication by Site and to 1 or More CPIC Level A Medications .
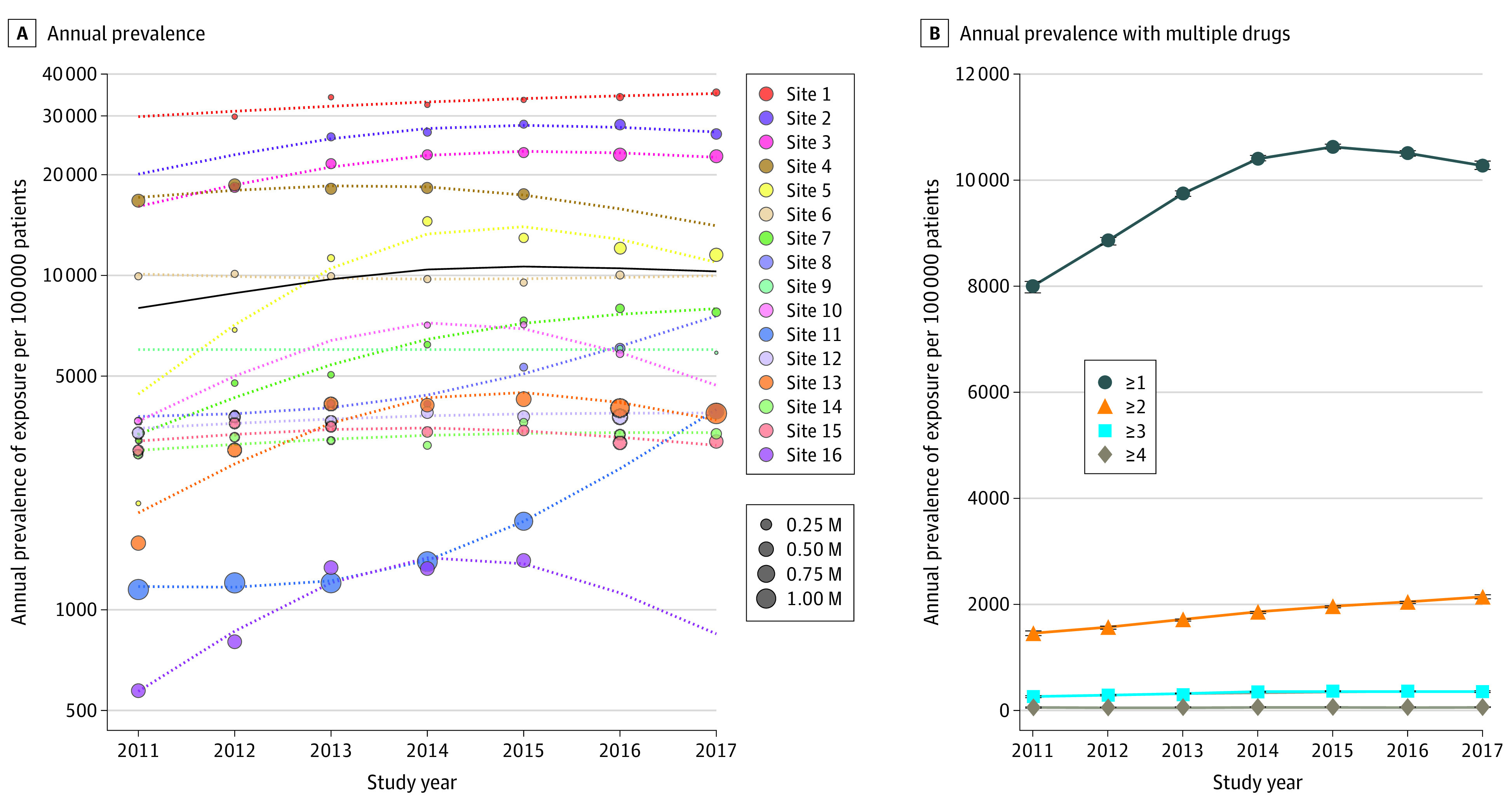
A, Each circle represents the observed prevalence of exposure for a given site on a log scale. Circles are absent for years when data were not available. The size of the circle is proportional to the number of patients who experienced at least 1 encounter in that year. The dotted lines represent the prevalence of exposure estimated from the model fit. The mean prevalence of exposure across all sites is shown by the solid black line. The 95% CIs for the mean is filled in gray but may be too narrow to observe. B, On a linear scale, the mean annual prevalence of exposure is stratified by the number of CPIC level A medications prescribed. The prevalence of exposure was estimated from the model. The whiskers indicate 95% CIs. M indicates million.
Table 2. Annual Estimated Prevalences per 100 000 Patients of Actionable Exposures.
| Medication by class | Annual prescription prevalence per 100 000 patients (95% CI) | Gene | Actionable phenotypea | Annual actionable gene-drug interaction prevalence per 100 000 patients (95% CI) |
|---|---|---|---|---|
| Antiemetic | ||||
| Ondansetron | 8107 (8077-8137) | CYP2D6 | UM | 325 (324-327) |
| Analgesic | ||||
| Oxycodone | 2116 (2097-2135) | CYP2D6 | PM, IM, UM | 356 (352-359) |
| Codeine | 571 (557-586) | CYP2D6 | PM, IM, UM | 98 (95-100) |
| Tramadol | 295 (273-317) | CYP2D6 | PM, IM, UM | 53 (49-57) |
| Antidepressant | ||||
| Citalopram | 283 (278-287) | CYP2C19 | PM, RM, UM | 94 (92-95) |
| Amitriptyline | 272 (267-277) | CYP2C19 | PM, RM, UM | 90 (89-92) |
| Amitriptyline | 272 (267-277) | CYP2D6 | PM, IM, UM | 46 (45-46) |
| Escitalopram | 259 (255-264) | CYP2C19 | PM, RM, UM | 86 (84-87) |
Abbreviations: IM, intermediate metabolizer; PM, poor metabolizer; RM, rapid metabolizer; UM, ultrarapid metabolizer.
CYP2D6 IM phenotype does not include the activity score of 1 or the updated activity score of the *10 allele as defined in the newest genotype-to-phenotype translation.18
Prevalence of Exposure by Drug Class and Changes Over Time
Figure 2A illustrates the annual prevalence for each of the most commonly prescribed CPIC level A drug classes. From 2011 to 2017, ondansetron was prescribed at an annual prevalence ranging from 5399 to 8191 per 100 000 patients; opioid analgesics were prescribed at annual prevalences ranging from 2548 to 2799 per 100 000 patients. Medications used for more specific indications, such as antivirals, were prescribed for a much smaller proportion of patients. Most of the utilization trends remained constant over time, with notable exceptions being decreases in clopidogrel use (from 25 to 13 per 100 000 patients) and codeine use (from 1233 to 271 per 100 000 patients) and an increase in oxycodone use (from 1475 to 2262 per 100 000 patients) (Figure 2). When sites were stratified by primary population, pediatric health systems mirrored this trend for both opioids, whereas primarily adult health systems did not show significant changes in the type of opioid used across study years (eFigure 3 in the Supplement). Primarily pediatric health systems tended to have substantially higher prescribing prevalences for opioids (mean [SD], 3542 [163] per 100 000 patients) than did primarily adult health systems (mean [SD], 1721 [109] per 100 000 patients).
Figure 2. Annual Prevalence of Exposure to Clinical Pharmacogenetics Implementation Consortium (CPIC) Level A Medications, Stratified by Drug Class and Individual Analgesics .
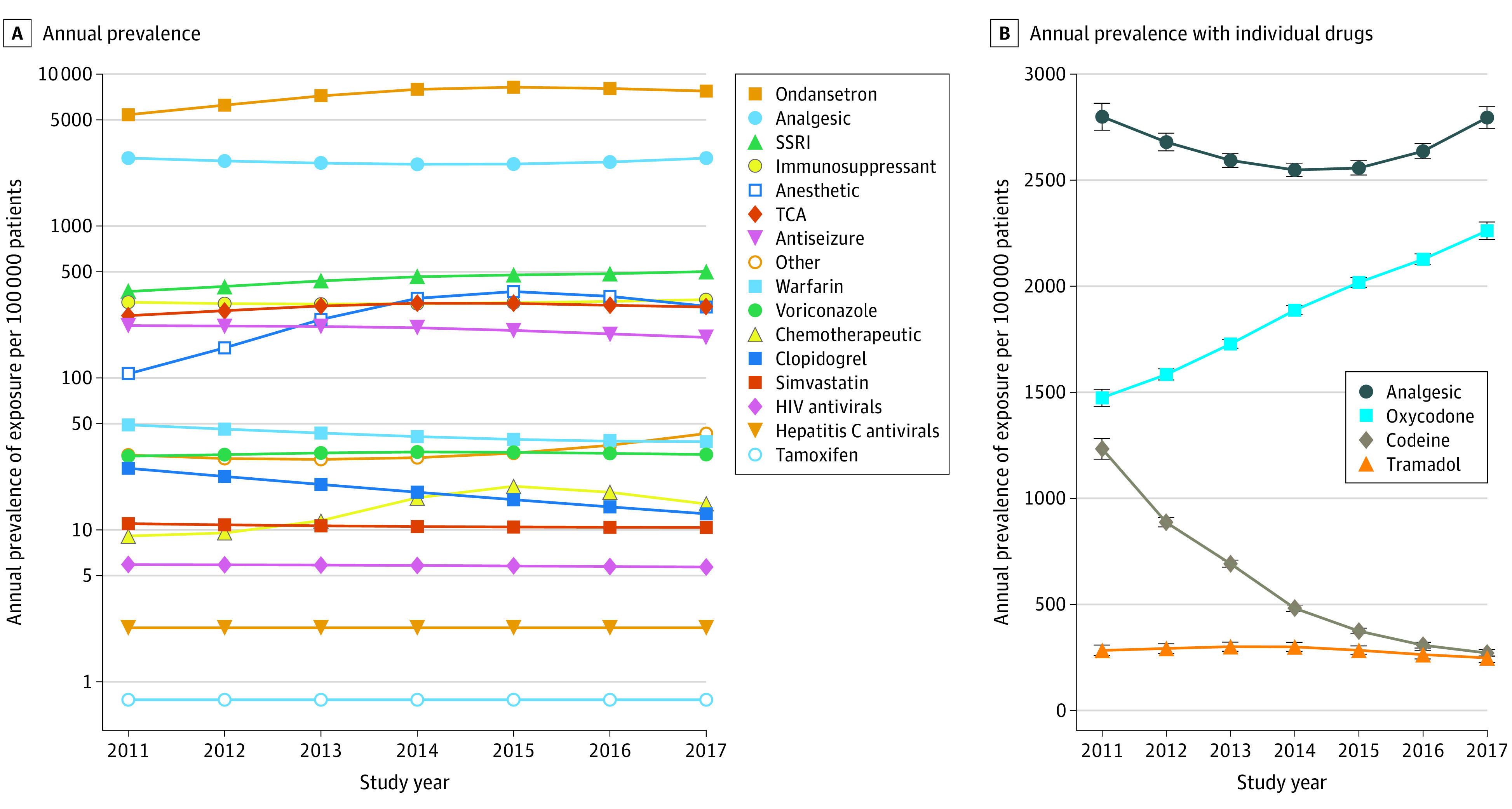
A, The annual prevalence of exposure for each drug or drug class was estimated from the model and is plotted on a log axis. If a drug class only had a single included drug, that drug was listed instead of the drug class. For example, ondansetron is listed instead of antiemetic medications. B, Annual prevalence of exposure for analgesics is plotted on a linear scale. The estimated prevalence of exposure for all analgesics was taken from the drug class model in part A, whereas those for oxycodone, codeine, and tramadol were taken from the individual drug models. The whiskers indicate 95% CIs. Non-CPIC level A analgesics were not included. SSRI indicates selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Estimated Prevalence of Actionable Exposures
Based on the prevalence of exposure to each CPIC level A drug, the race/ethnicity data of the cohort, and known frequencies of actionable genotypes and phenotypes in the populations, we estimated the prevalence of medication exposure among individuals with the relevant actionable phenotype. In this cohort, a total of 1335 actionable exposures per 100 000 pediatric patients were eligible for a genotype-guided intervention, had information been available. Although ondansetron was the most frequently prescribed CPIC level A drug for children, it was not the drug with the highest prevalence of actionable exposure. The prevalence at which this drug was prescribed to patients with actionable phenotypes (actionable exposure) was 325 patients per 100 000 patients, because only the ultrarapid metabolizer phenotype is actionable. Oxycodone had the highest estimated prevalence of actionable prescribing, with 356 per 100 000 pediatric patients (Table 2). CYP2D6 and CYP2C19 accounted for 1170 of the 1335 actionable exposures per 100 000 patients (87.6%).
Genes Associated With at Least 1 CPIC Level A Medication
Figure 3 shows the annual prevalence of exposure to CPIC level A medications stratified by the relevant gene associations. The most common gene associated with at least 1 prescribed CPIC level A medication prescription was CYP2D6 (GeneBank 1565), with more than 5000 patients per 100 000 in all years studied (Figure 3A). CYP2C19 (GeneBank 1557) and RYR1 (GeneBank 6261)/CACNA1S (GeneBank 779) remained a distant second and third, respectively, with an order of magnitude fewer patients (≤775 and ≤370 patients per 100 000, respectively). These genes remained the most commonly associated when exposure to at least 2 CPIC level A medications was assessed (Figure 3B). The annual prevalence of exposure to multiple CPIC level A medications metabolized by CYP2D6 exceeded 1200 patients per 100 000 in all years studied.
Figure 3. Annual Prevalence of Exposure to Clinical Pharmacogenetics Implementation Consortium (CPIC) Level A Medications Stratified by Gene.
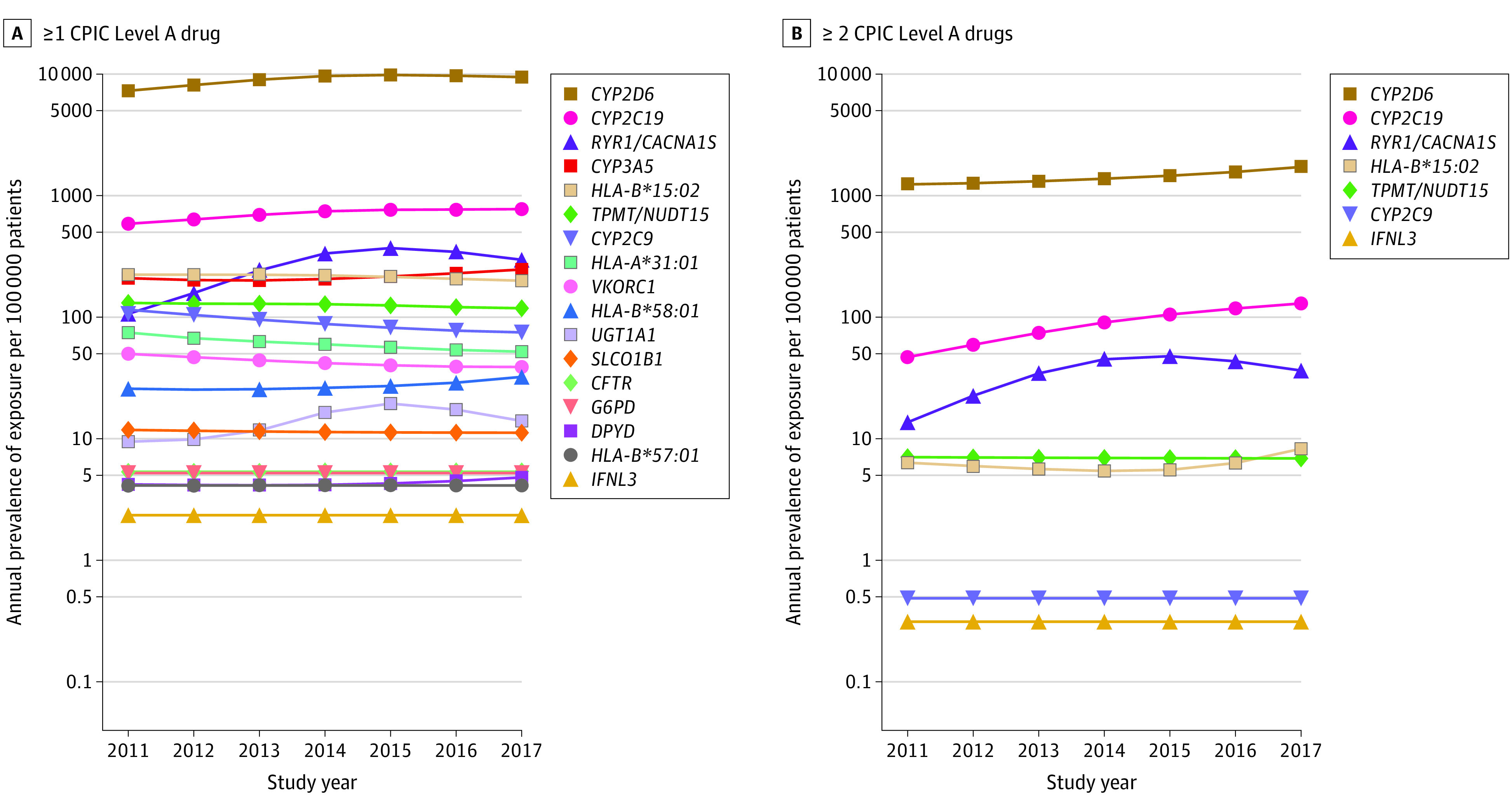
A, Annual prevalence of exposure to at least 1 CPIC level A medication plotted on a log scale, stratified by the associated gene. B, Annual prevalence of exposure of at least 2 CPIC level A medications. The rate of exposure was estimated from the model and is displayed on a log scale.
Discussion
To our knowledge, this is the first study to describe the prescribing of CPIC level A medications in pediatric patients among diverse sites in the US. The primary findings are that prescriptions for CPIC level A drugs are common (annual prescribing prevalence of approximately 8000 to 11 000 per 100 000 patients) in pediatrics and may be relevant to a broad spectrum of therapeutic areas, the importance of which may differ across institutions. Overall, we estimate that more than 1.3% of patients (>1300 per 100 000) would have potential recommendations for or may require drug selection or dosing changes based on current guidelines and pharmacogenetic testing results alone. Of the 20 relevant genes, CYP2D6 and CYP2C19 had the largest potential effect, because they affect commonly prescribed analgesics and antidepressants as well as the antiemetic ondansetron in the pediatric setting.
Our study focused on patients younger than 21 years, with most aged 3 to 14 years. Pediatric-specific analyses are important to quantify patterns of prescribing, highlight knowledge gaps, and quantify the potential effect of pharmacogenetics based on age, demographic characteristics, and drugs within pediatrics. One single-center study19 reported similar prevalences of prescribing, which differed from prevalences in adults.20 A 5-year study across Alberta, Canada,21 demonstrated that codeine-containing medications and ondansetron were the most commonly prescribed medications with pharmacogenetic-based prescribing guidelines in pediatric patients.
CYP2D6- and CYP2C19-associated drugs were the most commonly prescribed and represented most actionable exposures (87.6%). This includes all CPIC guideline recommendations, including those rated as optional in the guideline. Institutions have implemented clinical testing of these genes to guide drug or dose selection in pediatric patients.22,23,24,25,26 CPIC guidelines are available for the CYP2D6 substrates ondansetron,27 select opioids,28,29 tricyclic antidepressants,30,31 atomoxetine,12 tamoxifen,32 and selective serotonin reuptake inhibitors33; there are also CPIC guidelines for the CYP2C19 substrates tricyclic antidepressants,30,31 selective serotonin reuptake inhibitors,33 clopidogrel,34,35 and voriconazole.11 Initial data support the utility of CYP2D6 or CYP2C19 genotype-guided therapies for pediatrics24,25,26 and are anticipated from the IGNITE II Pragmatic Trials Network.36
CYP2D6 and CYP2C19 are also the genes most commonly associated with exposure to 2 or more CPIC level A drugs, indicating a potential for reuse of pharmacogenetic test results (particularly multigene tests), even within 1 year. Our observed prevalence of exposure to multiple CPIC level A drugs (<300 per 100 000 patients) is an underestimate of the true prevalence, because we were only able to aggregate data within single years. Opportunities for additional genotype-guided prescribing are likely to occur in subsequent years. For example, a child may have a pharmacogenetic test performed in response to prescription for a medication (eg, CYP2C19 testing for escitalopram). If this test examines a panel of genes and these results are included in the EHR with associated clinical decision support, they could be used preemptively at the point of prescribing all future medications related to those genes (eg, granisetron could be used instead of ondansetron for acute nausea in a patient with a CYP2D6 ultrarapid metabolizer phenotype). This illustrates the potential longitudinal utility of pharmacogenetic test results from childhood even into adulthood, which can be further facilitated by enhanced EHR interoperability, enabling dissemination of laboratory results across health care systems.37 These opportunities for genotype-guided prescribing will likely go unrecognized unless pediatricians receive adequate education and training in pharmacogenetics.
Changes in prescriptions over time were most prominent for analgesics. Codeine use declined after the 2013 FDA public warning against using the drug after tonsillectomy and/or adenoidectomy38; the FDA added a contraindication to codeine use in children younger than 12 years in 2017.39 Some clinicians support CYP2D6 testing to preserve codeine as an option for children by excluding those who have poor or ultrarapid metabolizer phenotypes and are therefore at increased risk for poor analgesic response or respiratory depression, respectively.25,40 The decrease in codeine prescriptions mirrors an increase in oxycodone use, approved for children 11 years or older in 201741; its off-label use in children was common before that date and was generally considered acceptable. Compared with morphine, oxycodone is associated with a reduced frequency of adverse effects, particularly delirium.42,43,44 These characteristics, combined with increased liability concerns and lack of pharmacogenetic testing, suggest a shift in analgesic utilization toward oxycodone as a preferable option in pediatric patients in the US but not in Canada.21 Unlike with codeine, the CYP2D6 genotype is not strongly associated with observed oxycodone response,45,46,47 but oxycodone and its active metabolite oxymorphone can lead to opioid dependence,48,49 raising reasonable concerns.
Limitations
Several limitations of this study should be noted. Only CPIC level A medications and prespecified alternatives were extracted from the EHR; therefore, we have an incomplete picture of the prescribing patterns of other medications (eg, sertraline, which is included in a CPIC guideline33 but is level B). The CPIC level A designations change over time; since the initiation of this project, several additional medications commonly used in pediatric patients (eg, atomoxetine,12 ibuprofen,50 and proton pump inhibitors51) are now designated level A and have CPIC guidelines. On the other hand, oxycodone was designated as level A but has been downgraded owing to evolving evidence. Metabolizer status assignments are also evolving. Reclassification of individuals with CYP2D6 activity scores of 1 from normal to intermediate metabolizers, per recently updated CYP2D6 translation guidelines,18 would result in a higher prevalence of actionable exposures to the associated medications. The generalizability of our findings is affected by the preponderance of academic medical centers; we used equal weighting across sites to avoid underrepresentation of the smaller, community-based health centers (relative to some of the very large academic medical centers). Individual site data may be more informative for some applications, given the variability across sites, and our efforts may not have led to a study population representative of all communities. Use of 1000 Genomes or other publicly available data52 to estimate actionability may also affect generalizability. Drug indications were not considered in our analysis, which may affect actionability and feasibility of pharmacogenomic implementation. Not all CPIC level A drugs have robust pediatric data, and extrapolation from adults to children warrants caution. Although activity for certain drug-metabolizing enzymes (eg, CYP2D6) is fully mature by early childhood, evidence suggests that activity for other enzymes (eg, CYP2C19) may be increased in children relative to adults.53,54 With respect to reuse of pharmacogenetic results over time, it would be of great interest to observe individual patients for longer than 1 year; however, our aggregated data precluded this analysis. The analyses included missing data from sites and some very low exposure prevalences requiring extrapolation, which may introduce error. Encounter data (denominator) and prescription data (numerator) required separate data extractions, precluding explicit confirmation that every individual with a prescription is represented in the encounter data.
Conclusions
The findings of this serial cross-sectional study suggest that opportunities for pharmacogenetic implementation among pediatric patients in the US are abundant. For pediatric institutions interested in implementing pharmacogenetic testing, the utility will likely be greatest for CYP2C19 and CYP2D6, particularly for the antiemetic ondansetron, analgesics, and antidepressants.
eMethods. Statistical Analysis Details
eTable 1. CPIC Level A Drugs and Associated Genes Included in Study
eTable 2. Characteristics of the Patient Populations and Sites’ Description
eFigure 1. Annual Prevalence of Exposure to at Least 1 CPIC Level A Drug by Age Differs by Hospital Type
eFigure 2. Prevalence of Exposure for Ondansetron and Escitalopram by Age
eFigure 3. Prevalence of Exposure to Analgesics by Age Stratified by Hospital Type
References
- 1.Relling MV, Evans WE. Pharmacogenomics in the clinic. Nature. 2015;526(7573):343-350. doi: 10.1038/nature15817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.US Food and Drug Administration. Table of pharmacogenomic biomarkers in drug labeling. Updated August 18, 2020. Accessed March 16, 2020. https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling
- 3.US Food and Drug Administration Table of pharmacogenetic associations. Published February 25, 2020. Accessed March 31, 2020. https://www.fda.gov/medical-devices/precision-medicine/table-pharmacogenetic-associations
- 4.Relling MV, Klein TE. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin Pharmacol Ther. 2011;89(3):464-467. doi: 10.1038/clpt.2010.279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Relling MV, Klein TE, Gammal RS, Whirl-Carrillo M, Hoffman JM, Caudle KE; The Clinical Pharmacogenetics Implementation Consortium . The Clinical Pharmacogenetics Implementation Consortium: 10 years later. Clin Pharmacol Ther. 2020;107(1):171-175. doi: 10.1002/cpt.1651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Caudle KE, Klein TE, Hoffman JM, et al. . Incorporation of pharmacogenomics into routine clinical practice: the Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline development process. Curr Drug Metab. 2014;15(2):209-217. doi: 10.2174/1389200215666140130124910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.CPIC: Clinical Pharmacogenetics Implementation Corsortium. Modified September 30, 2020. Accessed March 31, 2020. https://cpicpgx.org/
- 8.Rieder MJ, Carleton B. Pharmacogenomics and adverse drug reactions in children. Front Genet. 2014;5(April):78. doi: 10.3389/fgene.2014.00078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ramsey LB, Brown JT, Vear SI, Bishop JR, Van Driest SL. Gene-based dose optimization in children. Annu Rev Pharmacol Toxicol. 2020;60(1):311-331. doi: 10.1146/annurev-pharmtox-010919-023459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McLaughlin MJ, Wagner J, Shakhnovich V, Carleton B, Leeder JS. Considerations for implementing precision therapeutics for children. Clin Transl Sci. 2019;12(2):140-150. doi: 10.1111/cts.12607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moriyama B, Obeng AO, Barbarino J, et al. . Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for CYP2C19 and voriconazole therapy. Clin Pharmacol Ther. 2017;102(1):45-51. doi: 10.1002/cpt.583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brown JT, Bishop JR, Sangkuhl K, et al. . Clinical Pharmacogenetics Implementation Consortium guideline for cytochrome P450 (CYP)2D6 genotype and atomoxetine therapy. Clin Pharmacol Ther. 2019;106(1):94-102. doi: 10.1002/cpt.1409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Johnson JA, Caudle KE, Gong L, et al. . Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for pharmacogenetics-guided warfarin dosing: 2017 update. Clin Pharmacol Ther. 2017;102(3):397-404. doi: 10.1002/cpt.668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wagner JB, Abdel-Rahman S, Van Haandel L, et al. . Impact of SLCO1B1 genotype on pediatric simvastatin acid pharmacokinetics. J Clin Pharmacol. 2018;58(6):823-833. doi: 10.1002/jcph.1080 [DOI] [PubMed] [Google Scholar]
- 15.Weitzel KW, Alexander M, Bernhardt BA, et al. ; IGNITE Network . The IGNITE network: a model for genomic medicine implementation and research. BMC Med Genomics. 2016;9(1):1. doi: 10.1186/s12920-015-0162-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi: 10.1371/journal.pmed.0040296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cavallari LH, Beitelshees AL, Blake KV, et al. ; The IGNITE Pharmacogenetics Working Group . The IGNITE Pharmacogenetics Working Group: an opportunity for building evidence with pharmacogenetic implementation in a real-world setting. Clin Transl Sci. 2017;10(3):143-146. doi: 10.1111/cts.12456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Caudle KE, Sangkuhl K, Whirl-Carrillo M, et al. . Standardizing CYP2D6 genotype to phenotype translation: consensus recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin Transl Sci. 2020;13(1):116-124. doi: 10.1111/cts.12692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Samwald M, Xu H, Blagec K, et al. Incidence of exposure of patients in the United States to multiple drugs for which pharmacogenomic guidelines are available. PLoS One. 2016;11(10):e0164972. doi: 10.1371/journal.pone.0164972 [DOI] [Google Scholar]
- 20.Chanfreau-Coffinier C, Hull LE, Lynch JA, et al. . Projected prevalence of actionable pharmacogenetic variants and level A drugs prescribed among US Veterans Health Administration pharmacy users. JAMA Netw Open. 2019;2(6):e195345. doi: 10.1001/jamanetworkopen.2019.5345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fan M, Yarema MC, Box A, Hume S, Aitchison KJ, Bousman CA. Identification of high-impact gene-drug pairs for pharmacogenetic testing in Alberta, Canada. Pharmacogenet Genomics. 2020. doi: 10.1097/FPC.0000000000000418 [DOI] [PubMed] [Google Scholar]
- 22.Cavallari LH, Van Driest SL, Prows CA, et al. ; IGNITE Network . Multi-site investigation of strategies for the clinical implementation of CYP2D6 genotyping to guide drug prescribing. Genet Med. 2019;21(10):2255-2263. doi: 10.1038/s41436-019-0484-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ramsey LB, Prows CA, Zhang K, et al. . Implementation of pharmacogenetics at Cincinnati Children’s Hospital Medical Center: lessons learned over 14 years of personalizing medicine. Clin Pharmacol Ther. 2019;105(1):49-52. doi: 10.1002/cpt.1165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cicali EJ, Blake K, Gong Y, et al. . Novel implementation of genotype-guided proton pump inhibitor medication therapy in children: a pilot, randomized, multisite pragmatic trial. Clin Transl Sci. 2019;12(2):172-179. doi: 10.1111/cts.12589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gammal RS, Crews KR, Haidar CE, et al. . Pharmacogenetics for safe codeine use in sickle cell disease. Pediatrics. 2016;138(1):e20153479. doi: 10.1542/peds.2015-3479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Teusink A, Vinks A, Zhang K, et al. . Genotype-directed dosing leads to optimized voriconazole levels in pediatric patients receiving hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2016;22(3):482-486. doi: 10.1016/j.bbmt.2015.11.011 [DOI] [PubMed] [Google Scholar]
- 27.Bell GC, Caudle KE, Whirl-Carrillo M, et al. . Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin Pharmacol Ther. 2017;102(2):213-218. doi: 10.1002/cpt.598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Crews KR, Gaedigk A, Dunnenberger HM, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin Pharmacol Ther. 2014;95(4):376-382. doi: 10.1038/clpt.2013.254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Crews KR, Gaedigk A, Dunnenberger HM, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin Pharmacol Ther. 2012;91(2):321-326. doi: 10.1038/clpt.2011.287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hicks JK, Swen JJ, Thorn CF, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clin Pharmacol Ther. 2013;93(5):402-408. doi: 10.1038/clpt.2013.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hicks JK, Sangkuhl K, Swen JJ, et al. . Clinical Pharmacogenetics Implementation Consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin Pharmacol Ther. 2017;102(1):37-44. doi: 10.1002/cpt.597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Goetz MP, Sangkuhl K, Guchelaar HJ, et al. . Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 and tamoxifen therapy. Clin Pharmacol Ther. 2018;103(5):770-777. doi: 10.1002/cpt.1007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hicks JK, Bishop JR, Sangkuhl K, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 and CYP2C19 genotypes and dosing of selective serotonin reuptake inhibitors. Clin Pharmacol Ther. 2015;98(2):127-134. doi: 10.1002/cpt.147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Scott SA, Sangkuhl K, Stein CM, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin Pharmacol Ther. 2013;94(3):317-323. doi: 10.1038/clpt.2013.105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Scott SA, Sangkuhl K, Gardner EE, et al. ; Clinical Pharmacogenetics Implementation Consortium . Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and clopidogrel therapy. Clin Pharmacol Ther. 2011;90(2):328-332. doi: 10.1038/clpt.2011.132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.National Human Genome Research Institute. Implementing Genomics in Practice (IGNITE) II: Pragmatic Clinical Trials Network (PTN). Updated September 29, 2020. Accessed April 1, 2020. https://www.genome.gov/Funded-Programs-Projects/Implementing-Genomics-in-Practice-IGNITE-2-Pragmatic-Clinical-Trials-Network
- 37.Hoffman JM, Flynn AJ, Juskewitch JE, Freimuth RR. Biomedical data science and informatics challenges to implementing pharmacogenomics with electronic health records. Annu Rev Biomed Data Sci. 2020;3(1):289-314. doi: 10.1146/annurev-biodatasci-020320-093614 [DOI] [Google Scholar]
- 38.US Food and Drug Administration Safety review update of codeine use in children; new boxed warning and contraindication on use after tonsillectomy and/or adenoidectomy. Published August 15, 2012. Accessed March 31, 2020. https://www.fda.gov/media/85072/download
- 39.US Food and Drug Administration FDA restricts use of prescription codeine pain and cough medicines and tramadol pain medicines in children; recommends against use in breastfeeding women. Updated September 21, 2015. Accessed March 31, 2020. https://www.fda.gov/media/104268/download
- 40.Gammal RS, Caudle KE, Quinn CT, et al. . The case for pharmacogenetics-guided prescribing of codeine in children. Clin Pharmacol Ther. 2019;105(6):1300-1302. doi: 10.1002/cpt.1260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Yang YT, Chen B, Bennett CL. FDA approval of extended-release oxycodone for children with severe pain. Pediatrics. 2016;137(5):e20160205. doi: 10.1542/peds.2016-0205 [DOI] [PubMed] [Google Scholar]
- 42.Maddocks I, Somogyi A, Abbott F, Hayball P, Parker D. Attenuation of morphine-induced delirium in palliative care by substitution with infusion of oxycodone. J Pain Symptom Manage. 1996;12(3):182-189. doi: 10.1016/0885-3924(96)00050-4 [DOI] [PubMed] [Google Scholar]
- 43.Riley J, Eisenberg E, Müller-Schwefe G, Drewes AM, Arendt-Nielsen L. Oxycodone: a review of its use in the management of pain. Curr Med Res Opin. 2008;24(1):175-192. doi: 10.1185/030079908X253708 [DOI] [PubMed] [Google Scholar]
- 44.Schmidt-Hansen M, Bennett MI, Arnold S, Bromham N, Hilgart JS. Oxycodone for cancer-related pain. Cochrane Database Syst Rev. 2017;8(8):CD003870. doi: 10.1002/14651858.CD003870.pub6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Pöyhiä R, Seppälä T, Olkkola KT, Kalso E. The pharmacokinetics and metabolism of oxycodone after intramuscular and oral administration to healthy subjects. Br J Clin Pharmacol. 1992;33(6):617-621. doi: 10.1111/j.1365-2125.1992.tb04090.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lalovic B, Phillips B, Risler LL, Howald W, Shen DD. Quantitative contribution of CYP2D6 and CYP3A to oxycodone metabolism in human liver and intestinal microsomes. Drug Metab Dispos. 2004;32(4):447-454. doi: 10.1124/dmd.32.4.447 [DOI] [PubMed] [Google Scholar]
- 47.Otton SV, Wu D, Joffe RT, Cheung SW, Sellers EM. Inhibition by fluoxetine of cytochrome P450 2D6 activity. Clin Pharmacol Ther. 1993;53(4):401-409. doi: 10.1038/clpt.1993.43 [DOI] [PubMed] [Google Scholar]
- 48.Comer SD, Sullivan MA, Whittington RA, Vosburg SK, Kowalczyk WJ. Abuse liability of prescription opioids compared to heroin in morphine-maintained heroin abusers. Neuropsychopharmacology. 2008;33(5):1179-1191. doi: 10.1038/sj.npp.1301479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Dart RC, Surratt HL, Cicero TJ, et al. . Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015;372(3):241-248. doi: 10.1056/NEJMsa1406143 [DOI] [PubMed] [Google Scholar]
- 50.Theken KN, Lee CR, Gong L, et al. . Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and nonsteroidal anti-inflammatory drugs. Clin Pharmacol Ther. 2020;108(2):191-200. doi: 10.1002/cpt.1830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Lima JJ, Thomas CD, Barbarino J, et al. . Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2C19 and proton pump inhibitor dosing. Clin Pharmacol Ther. Published online August 8, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Huddart R, Fohner AE, Whirl-Carrillo M, et al. . Standardized biogeographic grouping system for annotating populations in pharmacogenetic research. Clin Pharmacol Ther. 2019;105(5):1256-1262. doi: 10.1002/cpt.1322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hines RN. Ontogeny of human hepatic cytochromes P450. J Biochem Mol Toxicol. 2007;21(4):169-175. doi: 10.1002/jbt.20179 [DOI] [PubMed] [Google Scholar]
- 54.Hines RN. Developmental expression of drug metabolizing enzymes: impact on disposition in neonates and young children. Int J Pharm. 2013;452(1-2):3-7. doi: 10.1016/j.ijpharm.2012.05.079 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods. Statistical Analysis Details
eTable 1. CPIC Level A Drugs and Associated Genes Included in Study
eTable 2. Characteristics of the Patient Populations and Sites’ Description
eFigure 1. Annual Prevalence of Exposure to at Least 1 CPIC Level A Drug by Age Differs by Hospital Type
eFigure 2. Prevalence of Exposure for Ondansetron and Escitalopram by Age
eFigure 3. Prevalence of Exposure to Analgesics by Age Stratified by Hospital Type