

Abstract
Objective
To examine occupational heritability in medicine and changes in heritability over time, with Swedish population wide administrative data that allowed mapping family trees of physicians spanning up to three generations.
Design
Retrospective observational study.
Setting
Individual level administrative registry data from Sweden.
Participants
Physicians born in 1950-90 and living in Sweden at some time during 2001-16 (n=47 400).
Main outcome measures
The proportion of individuals with a completed medical degree with at least one parent who also trained in medicine, and the change in this proportion across birth cohorts. Additional analyses were conducted among other relatives (grandparents, aunts and uncles, and siblings) and for individuals with a law degree.
Results
For 27 788 physicians, where the educational background for both parents was known, 14% had a parent who was also a physician and 2% had two parents who were physicians. The proportion of physicians with at least one physician parent increased significantly over time, from 6% for physicians born in 1950-59 to 20% for physicians born in 1980-90 (P<0.001). The same pattern of increasing occupational heritability was not seen for individuals with law degrees.
Conclusions
In recent cohorts of physicians in Sweden, one in five had a parent who was also a physician, more than triple the proportion seen for physicians born three decades earlier. A similar pattern was not seen in lawyers, suggesting that increasing occupational heritability in medicine does not reflect intergenerational persistence of high paying degrees alone. Rather, for physicians in Sweden, medicine might increasingly run in families.
Introduction
Parents’ occupations might influence the career choice of their offspring through information, opportunities, and economic means. High degrees of occupational heritability in selective disciplines, such as medicine, could constrain socioeconomic mobility and negatively influence efforts to increase socioeconomic diversity in the workforce. In medicine, having physicians from a limited socioeconomic pool could affect patient health because research has reported the importance of similar socioeconomic and personal characteristics between physicians and patients for patient outcomes.1 2 3 4 5 If a large or growing proportion of physicians are from families of physicians, the diversity of the physician workforce might be limited. The extent to which medicine runs in families is, however, not known.
To assess the importance of these concerns in medicine, we used Swedish population wide administrative registry data. The family and educational records in these data allowed us to identify individuals who completed training in medicine (referred to as physicians in this report) and map family trees of these individuals spanning up to three generations. We analyzed how the proportion of physicians with at least one relative who also trained as a physician changed over time. For our primary outcome, we compared the proportion of physicians with at least one physician parent for physicians born in 1950-59 versus physicians born in 1980-90. Additional analyses examined these differences by year of birth, sex of the physician, and relatives other than parents. For our secondary outcome, we compared these trends with the analogous metric for individuals with training in law (referred to as lawyers in this report) to better understand whether growing heritability in medicine might simply reflect growing intergenerational persistence of high paying degrees and occupations.
Methods
Data and context
We used individual level administrative registry data from Sweden. Swedish registry data have been described previously.6 7 The dataset included educational records reported by educational authorities for 1990-2016, and individual level characteristics such as sex, year, and country of birth. Also, the data included precise family linkage information for all individuals born in 1950 or later who were alive and lived in Sweden between 2001 and 2016, and for their deceased relatives. With these data, we mapped out family trees of physicians spanning up to three generations. We identified these family linkages: parents (biological and adoptive), siblings, aunts and uncles, and grandparents. All data linkages were performed with deidentified individual keys that were created by Statistics Sweden for the registry data.
We defined an individual as a physician if they ever completed training in medicine according to the educational records of 1990-2016.8 Our baseline analysis included educational codes that capture clinical training in medical faculties (in Swedish, “Läkarutbildning”). We found largely the same patterns for an alternative definition of a physician that included both clinical and research focused degrees in medical faculties (eg, biomedicine) (appendix). A clinical medical degree in Sweden starts as an undergraduate degree that individuals apply for after finishing high school. The degree commonly takes six years to complete before new physicians start working in the healthcare system, most employed by public hospitals and clinics.8 For our secondary analyses, we similarly defined an individual as a lawyer if he or she ever completed (also undergraduate) training in law according to the educational records.
Primary statistical analysis
Our study population included all physicians born between 1950 and 1990 who were alive and lived in Sweden at some time between 2001 and 2016. For our primary statistical analysis, we restricted the study population to physicians where the parental educational background was available for both parents. For each birth cohort in this sample, we computed the proportion of physicians with at least one parent who was also a physician and, separately, the proportion of physicians with two parents who were physicians.
We further computed the proportion of physicians in each birth cohort with at least one sibling, aunt or uncle, or grandparent who was also a physician. For each type of relative, we restricted the study population to physicians with at least one relative (of that type) whose educational background was available.
We computed the proportion of physicians with a physician relative for each birth cohort and for all birth cohorts combined. We also pooled individuals by 10 year birth cohorts: 1950-59, 1960-69, 1970-79, and 1980-90. We performed two sided hypothesis tests of equality for the proportion of physicians with a physician relative between the birth cohorts 1950-59 and 1980-90.
Finally, we investigated the differences between men and women for the proportion of physicians with at least one parent who also trained as a physician, an analysis conducted to assess whether male and female physicians differed in the diversity of their parents’ educational backgrounds. We used 95% confidence intervals (P<0.05) as a threshold for statistical significance. All analyses were performed with Stata statistical software.
Secondary analysis
We replicated our main analysis on a sample of lawyers who were born in 1950-90, lived in Sweden at some time during 2001-16, and where the educational background for both parents (or the respective relative of interest) was available. We investigated how the proportion of lawyers with at least one parent who also trained as a lawyer changed over time. The purpose of the analysis was to investigate whether any trends in occupational heritability among physicians were specific to the profession or reflected growing intergenerational persistence of high paying, high status occupations and degrees.
Results
Characteristics of the study population
Our study population included 47 400 individuals with a medical degree, born in 1950-90, and living in Sweden at some time during 2001-16. The educational background for both parents was available for 27 788 (59%) physicians (table 1). There were two reasons why information on parental education might be missing: for physicians born outside of Sweden, not being able to link these individuals to their parents was more likely; if parental linkage was available, but the parents died before 1990, the educational background of the parents was not available because our education records started in 1990. Hence parental education was more likely to be missing for older cohorts.
Table 1.
Characteristics of all physicians and of physicians where the educational background for both parents was known
| Physicians in study population (n=47 400)* | Physicians with educational background known for both parents (n=27 788)† | |
|---|---|---|
| Born in Sweden | 61.1 (28 982) | 92.8 (25 784) |
| Born in Europe (excluding Sweden) | 22.7 (10 757) | 3.1 (863) |
| Born in Asia | 12.3 (5843) | 3.3 (905) |
| Born in Africa | 1.6 (751) | 0.3 (87) |
| Year of birth (median) | 1972 | 1973 |
| Women | 49.7 (23 554) | 51.3 (14 253) |
Data are percentage (number) unless stated otherwise.
The study population comprised all individuals with a completed medical degree born in 1950-90 and living in Sweden at some time during 2001-16.
The study population was restricted to individuals where the educational background for both parents was known.
Among all physicians in the study population, 61% were born in Sweden, 23% were born in other European countries, and 12% were born in Asia. For physicians whose parental education was available for both parents, the percentage of individuals born outside of Sweden was much lower. In this sample, 93% of physicians were born in Sweden, they were younger (difference in median age, 1 year) than all physicians in the study population, and they were slightly more likely to be women (51% women compared with 50% women in the overall study population).
Occupational heritability in medicine
The proportion of physicians with at least one parent who had also trained as a physician increased over time (fig 1). For example, for physicians born in 1950, where the parental education was known for both parents, 5% had at least one parent who was a physician. For physicians born in 1990, 20% had at least one parent who was a physician, corresponding to an absolute increase of 15 percentage points and a relative increase of 300%. This finding could not be explained by changes in the proportion of physicians in the overall population of Sweden over time (appendix).
Fig 1.
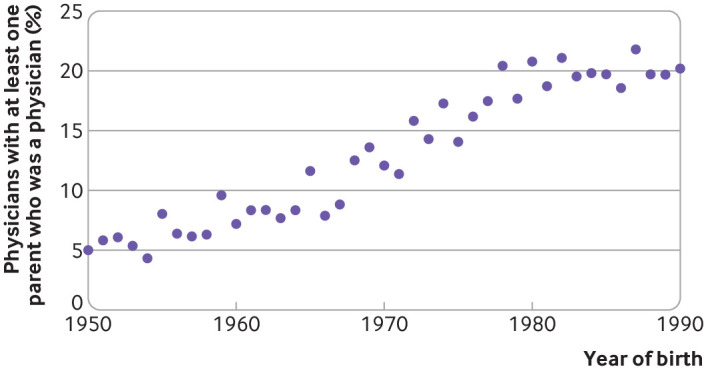
Percentage of individuals with a medical degree, by year of birth, with at least one parent who also had a medical degree. The sample was restricted to physicians in the study population where the educational background for both parents was available
Table 2 and figure 2 show the trends in occupational heritability in medicine, according to decade of birth. For physicians across all 1950-90 birth cohorts whose parental education was known, 14% had a parent who was also a physician and 2% had two parents who were physicians. The proportion of physicians with at least one physician parent increased over time, from 6% for physicians born in 1950-59 to 20% for physicians born in 1980-90 (P<0.001). We found a similar trend for individuals with two parents who were physicians. Whereas 1% of physicians born in 1950-59 had two parents who were physicians, this increased to 4% for physicians born in 1980-90 (P<0.001).
Table 2.
Occupational heritability among physicians
| Years of birth | 1950-59 v 1980-90, P value* | |||||
|---|---|---|---|---|---|---|
| All | 1950-59 | 1960-69 | 1970-79 | 1980-90 | ||
| Educational background available for both parents (No) | 27 788 | 5660 | 5522 | 7440 | 9166 | |
| At least one parent was a physician (%) | 14.0 | 6.4 | 9.5 | 15.9 | 20.0 | <0.001 |
| Both parents were physicians (%) | 2.5 | 0.9 | 1.0 | 2.7 | 4.2 | <0.001 |
| Educational background known for at least one sibling (No) | 29 066 | 7046 | 5786 | 7352 | 8882 | |
| At least one sibling was a physician (%) | 13.6 | 14.0 | 13.7 | 14.1 | 12.9 | 0.05 |
| Educational background available for at least one aunt or uncle (No) | 18 360 | 568 | 3538 | 6558 | 7696 | |
| At least one aunt or uncle was a physician (%) | 8.9 | 1.6 | 5.8 | 8.6 | 11.0 | <0.001 |
| Educational background known for at least one grandparent (No) | 18 061 | 508 | 3240 | 6512 | 7801 | |
| At least one grandparent was a physician (%) | 2.4 | 0 | 0.5 | 2.1 | 3.5 | <0.001 |
Overview of occupational heritability in medicine for physicians in the study population, born in 1950-90, by decade of birth. The four types of relatives were: parents, siblings, aunts or uncles, and grandparents. For each type of relative, the study population was restricted to individuals with at least one relative whose educational background was known. For the analysis involving parents, the study population was restricted to physicians where the educational background for both parents was available.
P value for a two sided t test for difference in means between individuals with a medical degree born in 1950-59 and 1980-90.
Fig 2.

Overview of occupational heritability in medicine for physicians born in 1950-59 and 1980-90. Four types of relatives spanning three generations were considered: siblings, parents, aunts and uncles, and grandparents of the physician. For each type of relative, the study population of physicians was restricted to individuals with at least one relative whose educational background was known. For the statistics on parents, the study population was restricted to physicians where the educational background for both parents was known
We found that of 29 066 physicians with at least one sibling whose educational background was known, 14% had a sibling who was also a physician. Among 18 360 physicians with at least one aunt or uncle whose educational background was available, 9% had an aunt or uncle who was a physician. For 18 061 physicians with at least one grandparent whose educational background was known, 2% had at least one grandparent with a medical degree. Except for siblings, the proportions of physicians with these more distant relatives who were physicians increased over time.
We found no significant difference between male and female physicians in the proportion with a physician parent. In 13 535 male physicians, 14.3% had at least one parent with a medical education compared with 13.8% in female physicians (P=0.25).
Occupational heritability among lawyers
We adapted our analysis to lawyers, a similarly high skilled discipline. We studied 55 258 lawyers who were born in 1950-90, lived in Sweden at some time during 2001-16, and had parents whose educational background was known. In contrast with the findings for medicine, the proportion of lawyers with at least one parent who had also trained as a lawyer was constant over time (fig 3). On average, 7% of lawyers had a parent who was also a lawyer. Occupational heritability for lawyers and physicians was similar for individuals born in 1950: 7% of lawyers had a lawyer parent and 5% of physicians had a physician parent. Occupational heritability for lawyers remained at 7% for individuals born in 1990 whereas for physicians, heritability increased to 20% for individuals born in the same year. The growth in heritability for lawyers, measured as the proportion of lawyers with at least one parent who was a lawyer in the 1950-59 cohorts versus the 1980-90 cohort, was not significant (table A1).
Fig 3.
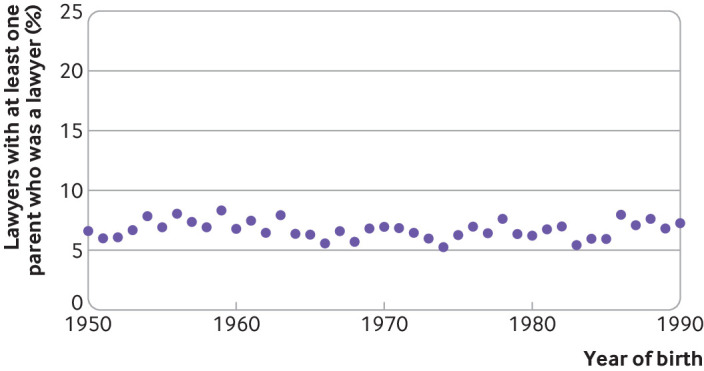
Percentage of individuals with a law degree, by year of birth, with at least one parent who also had a law degree. The study population of lawyers was defined similarly to the study population of physicians. The study population of lawyers was restricted to individuals where the educational background for both parents was known
Discussion
Principal findings
From individual level Swedish administrative educational and family linkage records, we found that in recent cohorts of physicians in Sweden, one in five had a parent who was also a physician, a significant increase from physicians born three decades earlier. This finding suggests an increasing number of physicians are from a concentrated group of physician families. A similar pattern was not seen for lawyers, suggesting that occupational heritability in medicine does not reflect intergenerational persistence of high paying, high prestige occupations and educational degrees alone.
Our findings do not imply that occupational heritability in medicine is distinct from socioeconomic heritability. In medicine, however, the concern about socioeconomic diversity in the physician workforce has been highlighted from an equity and diversity perspective, and also because of growing evidence that physician diversity and the similarity in personal and socioeconomic backgrounds between patients and physicians might affect patient outcomes.1 2 3 4 5 Our analysis showed an increasing number of physicians from families with other physicians, rather than an increasing proportion of physicians from families with more diverse economic and educational backgrounds. Our findings are consistent with older, smaller studies that reported similar proportions of medical students with a physician parent. For example, a study of Danish administrative data for 2002-07 for medical school entrants found that 12-16% of students had a physician parent. A study of Norwegian registry data reported that about 8% of medical students had parents who were physicians.9 10
Limitations of the study
Our study had several limitations. First, we examined one country, Sweden. Sweden consistently ranks at the top of the Organization for Economic Co-operation and Development (OECD) countries for intergenerational social mobility.11 Thus Sweden represents a case study of occupational heritability in medicine in one of the most socioeconomically mobile societies.
Second, data were missing for parental education for some physicians born outside of Sweden. A broader examination of socioeconomic diversity in the physician workforce would include the socioeconomic backgrounds of individuals who immigrated to Sweden as physicians or who later become physicians.
Third, our analysis did not identify the mechanism for the increasing occupational heritability in medicine, which could result from several factors: a growing effect of early childhood exposure to physician parents on future occupational choice and increased access to resources through parental professional or social networks (eg, children of physicians might be more likely to participate in clinical or laboratory internships through connections from their physician parents). Uncovering the exact mechanism that underlies our findings is important for future research.
Conclusions
We used individual level administrative educational and family linkage records from Sweden to map family trees of physicians spanning up to three generations. For recent cohorts, we found that one in five physicians had a parent who was also educated as a physician, nearly triple the proportion for physicians born three decades earlier. We did not find a comparable pattern for lawyers, however, suggesting that increasing occupational heritability in medicine does not reflect intergenerational persistence of high paying, high prestige occupations alone.
What is already known on this topic
Intergenerational persistence in educational achievement is well documented
Occupational heritability in selective disciplines, such as medicine, has received comparably less attention, despite concerns about socioeconomic diversity in the physician workforce and growing evidence that physician diversity might affect patient outcomes
What this study adds
The study examined occupational heritability in medicine from educational records of individuals born in 1950-90 and living in Sweden at some time during 2001-16, and their deceased relatives, allowing mapping of family trees of physicians spanning up to three generations
In recent cohorts of physicians in Sweden, one in five physicians had a parent who was also a physician, more than triple the proportion seen for physicians born three decades earlier
A similar pattern was not found among lawyers, suggesting that increasing occupational heritability in medicine does not reflect intergenerational persistence of high paying degrees alone but rather that medicine might increasingly run in families
Web extra.
Extra material supplied by authors
Web appendix: Online appendix
Contributors: All authors contributed to the design and conduct of the study, data collection and management, analysis and interpretation of the data; and preparation, review, or approval of the manuscript. ABJ supervised the study and is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: Support was provided by the Office of the Director, National Institutes of Health (1DP5OD017897, ABJ) and the National Institute on Aging (R21AG0528, PP and MP). The research conducted was independent of any involvement from the sponsor of the study. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Institutes of Health and National Institute on Aging for the submitted work; ABJ reports receiving consulting fees unrelated to this work from Pfizer, Hill Rom Services, Bristol Myers Squibb, Novartis, Amgen, Eli Lilly, Vertex Pharmaceuticals, AstraZeneca, Celgene, Tesaro, Sanofi Aventis, Biogen, Precision Health Economics, and Analysis Group; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study was exempt from human subject review, and participant consent was waived by the Stanford institutional review board. Ethics approval was obtained from the regional ethics board in Stockholm.
Data sharing: No additional data available. PP had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
ABJ affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies are disclosed.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Alsan M, Garrick O, Graziani G. Does diversity matter for health? Experimental evidence from Oakland. Am Econ Rev 2019;109:4071-111 10.1257/aer.20181446. [DOI] [Google Scholar]
- 2. Greenwood BN, Carnahan S, Huang L. Patient-physician gender concordance and increased mortality among female heart attack patients. Proc Natl Acad Sci U S A 2018;115:8569-74. 10.1073/pnas.1800097115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Institute of Medicine Unequal treatment: confronting racial and ethnic disparities in health care. National Academies Press, 2003. 10.17226/12875. [DOI] [PubMed] [Google Scholar]
- 4. Thornton RL, Powe NR, Roter D, Cooper LA. Patient-physician social concordance, medical visit communication and patients’ perceptions of health care quality. Patient Educ Couns 2011;85:e201-8. 10.1016/j.pec.2011.07.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. van Ryn M, Burke J. The effect of patient race and socio-economic status on physicians’ perceptions of patients. Soc Sci Med 2000;50:813-28. 10.1016/S0277-9536(99)00338-X [DOI] [PubMed] [Google Scholar]
- 6. Persson P, Rossin-Slater M. Family ruptures, stress, and the mental health of the next generation. Am Econ Rev 2018;108:1214-52. 10.1257/aer.20141406 [DOI] [PubMed] [Google Scholar]
- 7. Ludvigsson JF, Svedberg P, Olén O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol 2019;34:423-37. 10.1007/s10654-019-00511-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Lindgren S, Brännström T, Hanse E, et al. Medical education in Sweden. Med Teach 2011;33:798-803. 10.3109/0142159X.2011.570816 [DOI] [PubMed] [Google Scholar]
- 9. O’Neill L, Vonsild MC, Wallstedt B, Dornan T. Admission criteria and diversity in medical school. Med Educ 2013;47:557-61. 10.1111/medu.12140 [DOI] [PubMed] [Google Scholar]
- 10. Hansen MN. [Social background in recruitment of medical students.] J Norwegian Med Assoc 2005;125:2213-5. [PubMed] [Google Scholar]
- 11. OECD A family affair: intergenerational social mobility across OECD countries Economic policy reforms 2010: going for growth. OECD Publishing, 2010;166-83. 10.1787/growth-2010-38-en. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Web appendix: Online appendix