

Advances in measurement theory and technology in medicine often provide the ability to examine phenomena formerly undetected (through improved resolution of measurement), to support theoretical progress (by providing the ability to discover new associations), and to enable more efficient studies (by reducing measurement error and increasing statistical power). Although the technology of momentary assessment has been available for years, it could be better used for addressing many questions in pain research. We therefore present this review on methods for collecting patients' pain experiences based on multiple assessments of momentary or near-momentary pain in people's everyday lives. We start with a rationale for the development of the techniques and then discuss selected design features of momentary research that make it particularly suited for pain researchers. This is followed by our take on how momentary designs can add to our understanding of pain. Next, we discuss recent studies that have successfully used momentary methods in pain research. We close by presenting ideas for future development of these methods.
1. Rationale and core principles
There are many reasons for collecting data with an Ecological Momentary Assessment (EMA) design in combination with or in lieu of retrospective questionnaires or interviews. (Momentary techniques go by various names including the Experience Sampling Method,11,13,52 Ecological Momentary Assessment,45,46,46,52 Intensive Longitudinal Assessment,2 and Real Time Data Capture,48 among others. For ease of exposition, we use the abbreviation EMA to refer to the family of momentary assessments). Table 1 presents the 4 core principles of EMA and their relevance for the study of pain. First, one may wish to ensure that study results are applicable to the real world and not limited to artificial or laboratory situations because results obtained in artificial situations often do not generalize to everyday life (ecological validity5).
Table 1.
Key features of EMA, their operationalization, and pain relevance.
| EMA feature | Operationalization | Pain-related relevance |
|---|---|---|
| Measurements are taken in the real-world to ensure ecological validity | Respondents are assessed outside of laboratory or clinical settings to capture people's experiences in their natural environment | Understanding how pain is experienced in daily life |
| Assessments are made of immediate experience to reduce errors of retrospection | With EMA, respondents assessed about their immediate experience (“right before the prompt”) With cEMA, respondents assessed over a brief period (“since the last prompt” or “over the last 2 hours”) |
Avoids rating difficulties for patients Reporting errors due to biases and issues with memory reduced by momentary measurement Rapid dynamics ideally studied with EMA, whereas infrequent occurrences or broader coverage ideally studied with cEMA |
| Assessment moments are carefully selected to meet the study objectives | A family of sampling schedules are available to meet various study design needs The length and daily density of assessments can be tailored to study design needs |
Random sampling is useful for obtaining a representative sample of pain experiences over time Event sampling is useful for evaluating response treatment effect where the event is medication taking (eg, fast-acting and slow-release medications) Hybrid sampling is useful for measuring the timing and duration of treatment side effects, and the frequency and contexts of pain flares |
| Multiple assessments are taken to enable investigation of within-person associations | Convenient and noninvasive data capture modalities are used for repeated measurement over days and weeks Various data capture modalities are available including specialized watches, PDAs, smartphone apps, and telephone-based interactive voice response* |
Can reveal pain temporal dynamics that are relevant for diagnostic purposes and clinical decision-making Can reveal diurnal cyclicity and prolonged episodes of heightened pain intensity Can reveal concurrent or temporally lagged within-person relationships between pain intensity and other pain-relevant constructs including catastrophizing,21 personality (eg, neuroticism or extraversion21,22), mental health (eg, anxiety and depression14,16), sleep,4,26 and activity12 Identification of contextual factors that alleviate (eg, rest and pleasant activities) or exacerbate (eg, stress and physical activity) pain levels |
Studies using PDAs usually involve providing participants with a designated device to collect the momentary assessments. Smartphone apps allow participants to download the software to collect the assessments on their own device. Telephone-based interactive voice response systems usually involve calling participants through an automated system that lets participants complete the momentary assessments through the phone keypad.
EMA, Ecological Momentary Assessment.
Second, one may be concerned about measurement bias associated with retrospective processes.3 This is especially likely when information is recalled over “long” periods (at least relative to the salience of the entity reported) and when relevant information is difficult to access.39 Such circumstances can result in the use of cognitive heuristics to answer questions.54 Ecological Momentary Assessment minimizes bias and noise by greatly reducing the period asked about.
Third, one may want to be sure that assessments of pain are a representative sampling of peoples' everyday experiences, emphasizing the importance of sampling frameworks for assessments. Just as we know that selection biases10,24 can occur when sampling individuals for a study, analogous processes can occur with sampling moments. An example makes the point: if we prompted participants regularly at 7 am, noon, and 6 pm, we would have biased our sample of moments towards detecting appetitive consumption. Considerable attention is therefore paid to sampling schedules in momentary research.
Finally, in almost all EMA studies, respondents are assessed many times. The objective is to capture the ebb and flow of the circumstances or contexts people are exposed to in everyday life, including where they are, what they are doing, whom they are with, and time of day. This allows for the evaluation of within-person effects and the temporal dynamics of interest. We know from laboratory and clinical studies that contextual factors can have considerable effects on pain levels, and EMA allows us to understand naturally occurring contexts.31
2. Design of ecological momentary assessment studies: sampling schedules, recall periods, and content
Ecological Momentary Assessment studies typically follow respondents over a period (eg, one week) and signal them throughout each day (eg, 6 times a day) according to a set of sampling rules (eg, randomly scheduled assessments) to respond to a brief set of questions (eg, answering 15 questions through a smartphone app) about the immediate circumstances (eg, pain intensity at the moment). There are dozens of study possibilities formed just by these design choices. The actual parameters chosen for a particular study will be directed by the questions at hand. If the hypothesis was about acute responses to a treatment, for instance, then patients might be asked to answer 10 randomly administered assessments (eg, a brief symptom inventory) each day 3 days before and after the treatment. Treatment studies tracking longer-term changes in symptoms might demand a several-week protocol with a lower frequency of daily assessments to manage participant burden.
Many other features of EMA designs must be considered including the construction of appropriate questions for the intended recall period, the length of each momentary assessment, procedures for reminding participants about missed assessments, determination of compliance rates, handling of missing data, and dealing with technical issues concerning administration modality.47,53 We focus on 2 topics central to EMA, sampling moments and recall period, to provide a clearer picture of momentary research.
The first is which moments one should sample. Over the years, a handful of schedules have been developed to serve various investigator needs.43 Random sampling schedules are useful for characterizing people's levels of pain, for example, by computing an average from many random pain intensity ratings (Truly random assessments spread throughout the day can result in an uneven temporal spread. For this reason, stratified random sampling is often used, wherein days are divided into segments and an assessment is randomly selected from within that segment). It provides a representative sampling of respondents' lives and is the most commonly used sampling method. Event-based sampling is useful for capturing discrete events or circumstances; in this case, an event prompts an assessment. If one was interested in how pain levels or flares were associated with unpleasant interactions at work, respondents could be instructed to complete a pain assessment whenever such interactions occur. Hybrid sampling schemes combine these and other sampling schedules to accomplish particular goals. Event assessment might be used to record when analgesics were taken and concurrent pain at that moment, which could be followed by a series of fixed-time assessments to track the pain response (as one might do in a laboratory experiment). Thoughtful and creative sampling of moments and events is a hallmark of EMA research.
The second topic is the length of the period queried in an EMA assessment. Asking about the moment just before a prompt eliminates retrospection and the associated bias. This is ideal for understanding immediate pain. However, one often has interest in relatively infrequently occurring daily events (eg, taking of medication) that are unlikely to be recorded with random sampling of immediate moments. The coverage model of momentary reporting (cEMA33) extends the reporting period to the last several hours or since the last time the individual was prompted (an extended period chosen by the researcher), so that much more of the day is sampled. The disadvantage of cEMA is that recollection of experiences even over relatively brief periods can distort information (including how individuals choose to summarize pain over the period).33
Finally, we note that the content addressed in momentary studies to date has been diverse: it includes self-reports of a wide variety of inner states (eg, pain, stress, depression, anxiety, daydreaming, emotions, and loneliness), behaviors (eg, sleeping, eating, drinking, cigarette smoking, urination, medication, sex, social interactions, work activities, commuting, social media, and reading), symptoms (eg, aches, tingling, itching, headaches, muscle pain, coughing, shortness of breath, and nausea), and environments (eg, current place, inside/outside, temperature, air pollution, and time of day) and objective data including physiological states (eg, blood pressure, heart rate, and glucose levels), behavior (eg, activity level), and environment characteristics (eg, air quality and noise level). In some studies, both self-reports and objective measures are obtained allowing for a dynamic view of biopsychosocial processes.43 Many of these constructs may be of interest to pain researchers and could be studied concurrently with momentary pain measures. Regarding momentary studies of pain, the construct that has been most studied is pain severity, which is consistent with severity being the central construct in traditional pain assessments for both research and clinical applications. However, to obtain a full understanding of the pain experience, we recommend that other facets of pain be assessed with momentary methods, including sensory characteristics, emotional responses to pain, catastrophizing, pain-related behavior, and the impact on physical and social function.
A large number of resources are available for readers who would like in-depth treatment of many of the topics covered in this topical review1,2,33,43,44,51; in this article, we review several issues about momentary studies that we think are especially relevant for pain researchers and clinicians.
3. How momentary studies can enhance our understanding of pain
Momentary studies have considerable potential for enhancing our understanding of pain, and Table 2 presents a summary of the types of associations that can be investigated (Ref. 1), including associations that are unique to high-density EMA data.
Table 2.
Applications of momentary data for pain research.
| Application | Pain experience variables* | Research question examples |
|---|---|---|
| Summarizing pain experiences over time | Average pain intensity†,6 | What is a participant's average pain level? |
| What are the between-person differences in average pain level? | ||
| Variability in pain intensity†,35 | What is participant's variability of pain level? | |
| What are the between-person differences in variability of pain levels? | ||
| Other summary measures (eg, maximum pain level, amount of time in pain, average pain after wake-up)†,40 | What proportion of time did the participant experience pain? | |
| What was the participant's maximum pain over the day? | ||
| How do participants differ in pain after waking up? | ||
| Modeling the effect of time on pain experience | Average starting level of pain†,20 | What is the participant's level of pain at the beginning of the investigation (eg, at the beginning of the EMA monitoring period, week, or day)? |
| How do patients differ in their level of pain at the beginning of the time scale under investigation (eg, at baseline in a clinical trial)? | ||
| Rate of change in pain level†‡,30,37 | How has the participant's pain level changed across the time scale under investigation (eg, over the course of the EMA monitoring period, over the week, or over the course of the day [ie, diurnal rhythm])? | |
| Modeling within-person processes | Concurrent or lagged effects29,34 | How does negative affect relate to pain levels and how does it predict changes in pain levels over time? |
| Individual's dynamic change in pain state42,49 | What is the short-term effect of a treatment decision on a patient's pain trajectory? | |
| How frequently does a patient oscillate between high and low pain states? | ||
| How long does a specific pain state persist? |
This table was adapted from the study by Bolger et al.1
Example studies are cited.
All these applications may be used to investigate within-person states and between-person differences.
Primary application for EMA in clinical trials.
EMA, Ecological Momentary Assessment.
An intriguing feature of EMA is that it encourages a perspective of pain as a dynamic phenomenon. Individuals certainly differ in how much pain they experience on average, yet it is less known that there are surprisingly large amounts of variability in those levels and that there are often systematic temporal patterns in pain (Fig. 1). Ecological Momentary Assessment enhances the ability to quantify, predict, and possibly influence the ebb and flow of pain; this has been viewed as a paradigm shift in pain research.56
Figure 1.
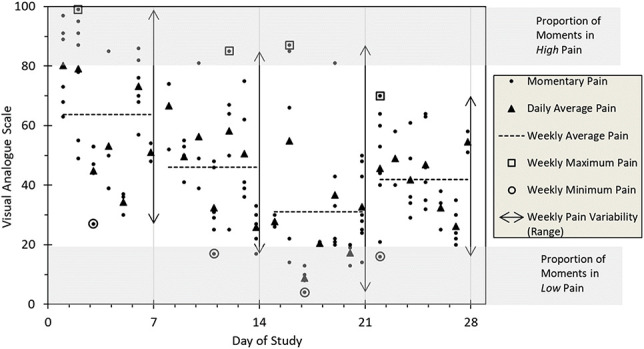
Variability in Pain Intensity and selected summary statistics that can be computed from EMA to characterize a patient's pain in daily life. X-axis ticks represent 28 sequential days of EMA monitoring for a single fibromyalgia patient. EMA, Ecological Momentary Assessment.
For acute pain, a natural application is tracking dynamic changes in postsurgical pain within and across days with momentary assessments, as illustrated in a recent study.49 This study analyzed momentary pain reports of over 8000 patients, which were recorded by medical staff every 4 hours on postoperative days 1 through 7 and documented in patients' electronic medical records. Using Markov Chain modeling, they were able to predict the course of pain states during postoperative recovery. In the future, Markov decision processes could be used to determine the choice of action at each time point (ie, at each step of the Markov Chain) that leads to the fastest recovery.
In chronic pain research, repeated momentary data provide the basis for creating numerous summary statistics to characterize variations of a patient's pain in daily life. Simple statistics such as the maximum or minimum weekly pain level, the proportion of moments a patient typically spends at high or at low pain levels on a given day, or the SD (ie, magnitude of fluctuations) around a patient's average pain level are just a few examples.45 Borrowing from statistical models in research on emotion regulation, novel summary statistics have been developed to capture a patient's pain variability from EMA, including the probability a patient experiences acute changes in pain35,41 and the relative durability of pain at elevated vs lower levels.42 Such summary statistics of symptom variability could enhance accurate classification of chronic pain conditions18 and facilitate detection of effective treatments. Women with fibromyalgia have, for example, shown more variability in fatigue levels compared to women with rheumatoid arthritis and osteoarthritis, highlighting important differences between conditions.57 Pain variability has also been shown to moderate treatment effects in several studies,17,32,50 which may lead to tailored treatment approaches for patients with different pain patterns. Finally, reducing momentary pain exacerbations and effectively managing pain fluctuations represent key elements of psychosocial and some pharmacological treatments; therefore, pain variability may represent a valuable endpoint in clinical trials.35,40,45
These examples demonstrate some of the uses of momentary data in the pain field. We suspect that imaginative scientists and clinicians will generate many more provocative applications for investigating pain and a myriad of social and biological factors.
4. Recent pain Ecological Momentary Assessment studies
Through 2016, over 100 reports used momentary pain assessments as shown in a recent review.33 To update that report, we searched for EMA studies over the past 5 years published in PAIN and in the Journal of Pain. Eleven original articles were found that reported results from 9 different projects (see Supplemental Table 1, available at http://links.lww.com/PAIN/B159).6,7,9,15,19,28,38,42,49,55 All the studies were observational designs and most investigated pain intensity,9,15,19,28,34,38,42,49,55 pain interference,7,19,27 and pain behavior,19 or examined relationships between pain and other domains (such as sleep55 or social support9). One study took a more methodological approach investigating the feasibility of promising statistical models.42 The flexibility of EMA designs for studies of pain is evident in these studies.
We can infer why investigators chose momentary methodologies for their studies. A focus on within-person associations was apparent in all the analyses performed, and pain experiences aggregated over individuals for between-person analyses were evident in a small number of studies. In a series of studies, Burns7,8,19 investigated the interactions between married couples of whom one or both experienced chronic pain. This “within-couples” design allowed the authors to show that increases in pain catastrophizing of patients were positively associated with spouse reports of patient pain behavior in concurrent and lagged analyses. In lagged analyses, Mun34 used a structural equation modeling framework to investigate whether morning pain catastrophizing and afternoon pain severity sequentially mediated the relationship between previous night nonrestorative sleep and end-of-day activity interference. It should be clear that addressing questions like these would not be possible without repeated, momentary assessment data.
5. Momentary assessment innovations
The ability to conduct real-time, momentary assessment in people's everyday lives informs our understanding of the pain experience in new ways. Beyond this, though, has been the development of methods for using momentary assessments in innovative ways that may be of interest to the pain community. First, technology developed for capturing pain assessments can be harnessed to provide rapid feedback to clinicians about the status of their patients. Such technologies have already been implemented in other areas (eg, weight loss, anxiety, and diabetes management) and have the potential for enhancing timely communication between patients and providers in the field of pain management, with the obvious goal of allowing quicker responses to changing clinical states.23,52 In a framework of diverse clinical data (ie, laboratory results, apparatus-based findings, and medical records) and other monitoring devices (ie, activity or sleep tracker), EMA could be a promising add-on that might improve the prediction of individual pain states.25
A second promising development is the use of momentary, real-time information for directing immediate treatment paradigms, often using the same technology used for assessments. Ecological Momentary Interventions 23 and Just-In-Time Adaptive Interventions 36 are terms referring to smart systems that use momentary, real-time assessments to initiate and tailor interventions to each individual. These approaches are grounded in the idea that the right kind of treatment at the right time can enhance outcomes. As an example, momentary assessments of mood, stress, location, and activities could be used to forecast periods of susceptibility (eg, pain flares and exacerbations) to decide when to deliver momentary interventions. Alternatively, individuals' coping or activity patterns could be used to determine which type of intervention to deliver with Just-In-Time Adaptive Intervention. Although research on the development of these novel intervention methods is in its early stages, they hold considerable potential for pain management and research.
6. Conclusion
This brief review provided readers with an understanding of the rationale for Ecological Momentary Assessment, an overview of the mechanics of momentary assessment, showed how this methodology has been used in pain research, and discussed how it may be incorporated into future research and practice.
Conflict of interest statement
A.A. Stone is a senior scientist with the Gallup Organization and a consultant with Adelphi Values, Inc. The remaining authors have no conflicts of interest to declare.
Acknowledgments
Supported by NIA R37AG057685 (A.A. Stone, P.I.), NIAMS R01AR066200 (A.A. Stone and S. Schneider, MPIs), and DFG OB437/2-1 Research Fellowship (recipient: A. Obbarius).
Appendix A. Supplemental digital content
Supplemental digital content associated with this article can be found online at http://links.lww.com/PAIN/B159.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
References
- [1].Bolger N, Davis A, Rafaeli E. Diary methods: capturing life as it is lived. Annu Rev Psychol 2003;54:579–616. [DOI] [PubMed] [Google Scholar]
- [2].Bolger N, Laurenceau JP. Intensive longitudinal methods: An introduction to diary and experience sampling research. New York, Guilford Press, 2013. [Google Scholar]
- [3].Bradburn NM, Rips LJ, Shevell SK. Answering autobiographical questions: the impact of memory and inference on surveys. Science 1987;236:151–67. [DOI] [PubMed] [Google Scholar]
- [4].Bromberg MH, Connelly M, Anthony KK, Gil KM, Schanberg LE. Prospective mediation models of sleep, pain, and daily function in children with arthritis using ecological momentary assessment. Clin J Pain 2016;32:471–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Brunswik E. Systematic and representative design of psychological experiments. Berkeley: University of California Press, 1941. [Google Scholar]
- [6].Burns JW, Gerhart J, Post KM, Smith DA, Porter LS, Buvanendran A, Fras AM, Keefe FJ. Spouse criticism/hostility toward partners with chronic pain: the role of spouse attributions for patient control over pain behaviors. J Pain 2018;19:1308–17. [DOI] [PubMed] [Google Scholar]
- [7].Burns JW, Gerhart JI, Post KM, Smith DA, Porter LS, Schuster E, Buvanendran A, Fras AM, Keefe FJ. The communal coping model of pain catastrophizing in daily life: a within-couples daily diary study. J Pain 2015;16:1163–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Burns JW, Post KM, Smith DA, Porter LS, Buvanendran A, Fras AM, Keefe FJ. Spouse criticism and hostility during marital interaction: effects on pain intensity and behaviors among individuals with chronic low back pain. PAIN 2018;159:25–32. [DOI] [PubMed] [Google Scholar]
- [9].Crockett KB, Turan B. Moment-to-moment changes in perceived social support and pain for men living with HIV: an experience sampling study. PAIN 2018;159:2503–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Crombie IK, Davies HT, Macrae WA. Cut and thrust: antecedent surgery and trauma among patients attending a chronic pain clinic. PAIN 1998;76:167–71. [PubMed] [Google Scholar]
- [11].Csikszentmihalyi M, Larson R. Validity and reliability of the experience-sampling method. J Nerv Ment Dis 1987;175:526–36. [DOI] [PubMed] [Google Scholar]
- [12].Cushing CC, Kichline T, Blossom JB, Friesen CA, Schurman JV. Tailoring individualized evaluation of pediatric abdominal pain using ecological momentary assessment (EMA): a pilot study testing feasibility and acceptability. Clin J Pain 2019;35:859–68. [DOI] [PubMed] [Google Scholar]
- [13].DeVries M. Investigating mental disorders in their natural settings: introduction to the special issue. J Nervious Ment Dis 1987;175:509–13. [DOI] [PubMed] [Google Scholar]
- [14].Dickens C, McGowan L, Dale S. Impact of depression on experimental pain perception: a systematic review of the literature with meta-analysis. Psychosomat Med 2003;65:369–75. [DOI] [PubMed] [Google Scholar]
- [15].Eather A, Kenardy J, Healy KL, Haynes M, Sterling M. How are pain and traumatic stress symptoms related in acute whiplash-associated disorders? An investigation of the role of pain-related fear in a daily diary study. PAIN 2019;160:1954–66. [DOI] [PubMed] [Google Scholar]
- [16].Egloff N, Wegmann B, Juon B, Stauber S, von Känel R, Vögelin E. The impact of anxiety and depressive symptoms on chronic pain in conservatively and operatively treated hand surgery patients. J Pain Res 2017;10:259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Farrar JT, Troxel AB, Haynes K, Gilron I, Kerns RD, Katz NP, Rappaport BA, Rowbotham MC, Tierney AM, Turk DC, Dworkin RH. Effect of variability in the 7-day baseline pain diary on the assay sensitivity of neuropathic pain randomized clinical trials: an ACTTION study. PAIN 2014;155:1622–31. [DOI] [PubMed] [Google Scholar]
- [18].Fillingim RB, Loeser JD, Baron R, Edwards RR. Assessment of chronic pain: domains, methods, and mechanisms. J Pain 2016;17:T10–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Gerhart JI, Burns JW, Bruehl S, Smith DA, Post KM, Porter LS, Schuster E, Buvanendran A, Fras AM, Keefe FJ. Variability in negative emotions among individuals with chronic low back pain: relationships with pain and function. PAIN 2018;159:342–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Glaros A, Owais Z, Lausten L. Reduction in parafunctional activity: a potential mechanism for the effectiveness of splint therapy. J Oral Rehabil 2007;34:97–104. [DOI] [PubMed] [Google Scholar]
- [21].Goubert L, Crombez G, Van Damme S. The role of neuroticism, pain catastrophizing and pain-related fear in vigilance to pain: a structural equations approach. PAIN 2004;107:234–41. [DOI] [PubMed] [Google Scholar]
- [22].Harkins SW, Price DD, Braith J. Effects of extraversion and neuroticism on experimental pain, clinical pain, and illness behavior. PAIN 1989;36:209–18. [DOI] [PubMed] [Google Scholar]
- [23].Heron KE, Smyth JM. Ecological momentary interventions: incorporating mobile technology into psychosocial and health behaviour treatments. Br J Health Psychol 2010;15:1–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Karos K, Alleva JM, Peters ML. Pain, please: an investigation of sampling bias in pain research. J Pain 2018;19:787–96. [DOI] [PubMed] [Google Scholar]
- [25].Kelly J, Gooding P, Pratt D, Ainsworth J, Welford M, Tarrier N. Intelligent real-time therapy: harnessing the power of machine learning to optimise the delivery of momentary cognitive–behavioural interventions. J Ment Health 2012;21:404–14. [DOI] [PubMed] [Google Scholar]
- [26].Kikuchi H, Yoshiuchi K, Yamamoto Y, Komaki G, Akabayashi A. Does sleep aggravate tension-type headache? an investigation using computerized ecological momentary assessment and actigraphy. Biopsychosoc Med 2011;5:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Kratz AL, Braley TJ, Foxen-Craft E, Scott E, Murphy JF, III, Murphy SL. How do pain, fatigue, depressive, and cognitive symptoms relate to well-being and social and physical functioning in the daily lives of individuals with multiple sclerosis? Arch Phys Med Rehabil 2017;98:2160–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Kratz AL, Ehde DM, Bombardier CH, Kalpakjian CZ, Hanks RA. Pain acceptance decouples the momentary associations between pain, pain interference, and physical activity in the daily lives of people with chronic pain and spinal cord injury. J Pain 2017;18:319–31. [DOI] [PubMed] [Google Scholar]
- [29].Kratz AL, Murphy SL, Braley TJ. Pain, fatigue, and cognitive symptoms are temporally associated within but not across days in multiple sclerosis. Arch Phys Med Rehabil 2017;98:2151–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Litt MD, Shafer DM, Ibanez CR, Kreutzer DL, Tawfik-Yonkers Z. Momentary pain and coping in temporomandibular disorder pain: exploring mechanisms of cognitive behavioral treatment for chronic pain. PAIN 2009;145:160–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Malenbaum S, Keefe FJ, Williams AC, Ulrich R, Somers TJ. Pain in its environmental context: implications for designing environments to enhance pain control. PAIN 2008;134:241–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Martini C, Yassen A, Krebs‐Brown A, Passier P, Stoker M, Olofsen E, Dahan A. A novel approach to identify responder subgroups and predictors of response to low‐and high‐dose capsaicin patches in postherpetic neuralgia. Eur J Pain 2013;17:1491–501. [DOI] [PubMed] [Google Scholar]
- [33].May M, Junghaenel DU, Ono M, Stone AA, Schneider S. Ecological momentary assessment methodology in chronic pain research: a systematic review. J Pain 2018;19:699–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Mun CJ, Davis MC, Campbell CM, Finan PH, Tennen H. Linking nonrestorative sleep and activity interference through pain catastrophizing and pain severity: an intraday process model among individuals with fibromyalgia. J Pain 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Mun CJ, Suk HW, Davis MC, Karoly P, Finan P, Tennen H, Jensen MP. Investigating intraindividual pain variability: methods, applications, issues, and directions. PAIN 2019;160:2415–29. [DOI] [PubMed] [Google Scholar]
- [36].Nahum-Shani I, Smith SN, Spring BJ, Collins LM, Witkiewitz K, Tewari A, Murphy SA. Just-in-Time adaptive interventions (JITAIs) in mobile health: key components and design principles for ongoing health behavior support. Ann Behav Med 2018;52:446–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Odawara M, Hashizume M, Yoshiuchi K, Tsuboi K. Real-time assessment of the effect of biofeedback therapy with migraine: a pilot study. Int J Behav Med 2015;22:748–54. [DOI] [PubMed] [Google Scholar]
- [38].Okun M, Karoly P, Mun CJ, Kim H. Pain-contingent interruption and resumption of work goals: a within-day diary analysis. J Pain 2016;17:65–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Robinson MD, Clore GL. Belief and feeling: evidence for an accessibility model of emotional self-report. Psychol Bull 2002;128:934–60. [DOI] [PubMed] [Google Scholar]
- [40].Schneider S, Junghaenel D, Ono M, Broderick J, Stone AA. Detecting treatment effects in clinical trials with different indices of pain intensity derived from ecological momentary assessment. J Pain. In press. [DOI] [PMC free article] [PubMed]
- [41].Schneider S, Junghaenel DU, Keefe FJ, Schwartz JE, Stone AA, Broderick JE. Individual differences in the day-to-day variability of pain, fatigue, and well-being in patients with rheumatic disease: associations with psychological variables. PAIN 2012;153:813–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Schneider S, Junghaenel DU, Ono M, Stone AA. Temporal dynamics of pain: an application of regime-switching models to ecological momentary assessments in patients with rheumatic diseases. PAIN 2018;159:1346–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol 2008;4:1–32. [DOI] [PubMed] [Google Scholar]
- [44].Stone AA, Shiffman S, Atienza A, Nebeling L. The science of real-time data capture: Self-reports in health research. New York: Oxford University Press, 2007. [Google Scholar]
- [45].Stone AA, Broderick JE, Schneider S, Schwartz JE. Expanding options for developing outcome measures from momentary assessment data. Psychosom Med 2012;74:387–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Stone AA, Shiffman S. Ecological momentary assessment (EMA) in behavioral medicine. Ann Behav Med 1994;16:199–202. [Google Scholar]
- [47].Stone AA, Shiffman S. Capturing momentary, self-report data: a proposal for reporting guidelines. Ann Behav Med 2002;24:236–43. [DOI] [PubMed] [Google Scholar]
- [48].Stone AA, Shiffman S, Atienza A, Nebling L, editors.The science of real-time data capture: Self-reports in health research. New York: Oxford University Press, 2007. [Google Scholar]
- [49].Tighe PJ, Bzdega M, Fillingim RB, Rashidi P, Aytug H. Markov chain evaluation of acute postoperative pain transition states. PAIN 2016;157:717–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Treister R, Honigman L, Lawal OD, Lanier RK, Katz NP. A deeper look at pain variability and its relationship with the placebo response: results from a randomized, double-blind, placebo-controlled clinical trial of naproxen in osteoarthritis of the knee. PAIN 2019;160:1522–8. [DOI] [PubMed] [Google Scholar]
- [51].Trull TJ, Ebner-Priemer U. Ambulatory assessment. Annu Rev Clin Psychol 2013;9:151–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Trull TJ, Ebner-Priemer UW. Using experience sampling methods/ecological momentary assessment (ESM/EMA) in clinical assessment and clinical research: introduction to the special section. Psychol Assess 2009;21:457–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Trull TJ, Ebner-Priemer UW. Ambulatory Assessment in psychopathology research: a review of recommended reporting guidelines and current practices. J Abnormal Psychol 2020;129:56–63. [DOI] [PubMed] [Google Scholar]
- [54].Tversky A, Kahneman D. Availability—heuristic for judging frequency and probability. Cogn Psychol 1973;5:207–32. [Google Scholar]
- [55].Whibley D, Braley TJ, Kratz AL, Murphy SL. Transient effects of sleep on next-day pain and fatigue in older adults with symptomatic osteoarthritis. J Pain 2019;20:1373–82. [DOI] [PubMed] [Google Scholar]
- [56].Winger JG, Vilardaga JCP, Keefe FJ. Indices of pain variability: a paradigm shift. PAIN 2019;160:2411–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Zautra AJ, Fasman R, Parish BP, Davis MC. Daily fatigue in women with osteoarthritis, rheumatoid arthritis, and fibromyalgia. PAIN 2007;128:128–35. [DOI] [PubMed] [Google Scholar]