

Abstract
This study aimed to analyze the moderation and moderation effects of resilience on the anxiety, depression impact on post-traumatic growth (PTG) among breast cancer patients undergoing chemotherapy based on structural equation modeling, and confirmed whether resilience was a mediating and regulating variable between anxiety, depression, and post-traumatic growth. In addition, whether anxiety and depression have different effects on PTG under different levels of psychological resilience.
This cross-sectional study was conducted from November 2017 to January 2019, with subjects of 260 breast cancer patients undergoing chemotherapy in the department of breast and general surgery of a tertiary general hospital in Shanxi Province of China.
Data were collected according to the General Hospital Anxiety and Depression Scale, Connor-Davidson Resilience Scale, and the posttraumatic growth inventory. Estimated values of model path coefficients and significance test were performed to confirm the mediation effect. Hierarchical regression and simple slope test were used to analyze the regulation effect.
Resilience showed significant correlations with anxiety, depression and PTG (all P < .01). Estimated values of model path coefficients and significance test results indicated that the mediating role of resilience was remarkable and it could regulate anxiety, depression, and PTG.
The anxiety, depression and resilience affected their PTG of breast cancer patients during chemotherapy, suggesting the need to establish a cooperative mechanism based on the concept of multidisciplinary collaboration. Professional psychological intervention should be used to reduce anxiety and depression and to explore the potential of resilience to promote their PTG.
Keywords: anxiety, depression, post-traumatic growth, resilience, structural equation model
1. Introduction
The report of cancer statistics in 2019 of American Cancer Society (ACS) showed that breast cancer is top among 10 female cancers in the United States in 2019.[1] The 2018 National Cancer Report from China National Cancer Center [2] pointed out that breast cancer was the highest incidence of cancer in Chinese women. Positive and standardized treatment can significantly improve the quality of life of patients. However, breast cancer patients still have different levels of psychological problems during the various stages of disease treatment and adaptation. Depression has also become an important factor influencing suicide risk.[3] A controlled study that evaluated the psychological state of 36 young cancer patients and 435 healthy volunteers showed that cancer patients had more severe emotional distress and lower personal growth.[4]
As the continuous development of positive psychology, people have gradually changed views on traumatic events such as cancer. They believe that, in addition to negative effects, traumatic events will also bring positive changes, such as post-traumatic growth (PTG). After experiencing challenging life events or situations, it is a positive change in the psychological aspects.[5] The content of this change includes interpersonal relationship, new possibilities, personal power, mental changes, life enjoyment.[5]
Some Japanese researchers[6] found a negative impact of anxiety and depression on PTG while creating PTG predictive models in breast cancer patients, but others have reached different conclusions. In the study of 294 cancer patients in Dutch,[7] the study of 113 cancer patients in Malayia[8] and the study of 70 breast cancer patients in Cordova,[9] there was no relationship between PTG and negative emotions. The relationship between positive and negative emotions has also aroused attention in relevant meta-analysis,[10] and it has not been found that positive changes were related to anxiety levels. Researchers[11] in China used mood, anxiety, and depression questionnaires assessed patients’ emotions and indicated that negative emotions also had a positive effect on psychological rehabilitation of patients and that depression was not an exception. But there were still some studies[12] showing that positive emotions were conducive to promoting the individual's development of PTG.
Previous studies highlighted the involvement of sensory perception in emotional processes and in real life conditions, examined the unique sensory processing patterns of individuals with major affective disorders and their relationship with psychiatric symptomatology[13]
Resilience refers to the ability of individuals to cope with and adapt to difficulties successfully.[14] Kumpfer[15] theory of resilience holds that the level of psychological resilience of an individual will have a certain impact on the positive psychological state of the patient. When the individual interacts with the environment, he/she will instinctively choose those that are beneficial to the body and have a protective strategy to deal with the environment. The theoretical framework highlights the interaction between risk factors and protective factors. The resilience's factors include cognition, emotion, behavior, spirit, and body, which has contained the growth content of post-traumatic growth, and it can be used to evaluate patients whether they have the level and ability to adapt to the dilemma. At the same time, the resilience can be adjustable.
Chinese study[16] have confirmed that resilience can alleviate the psychological distress and stress of cancer patients, effectively relieve negative emotions such as fear and depression, provide more self-confidence and hope for cancer challenges. However, some researches in Israeli and Lebanon[15] have showed that the PTG score of individuals with high psychological resilience was rather low. The reason may be considered as that individuals with high psychological resilience were less likely to have serious psychological disorders such as PTSD after experiencing trauma.
From the perspective of the influence of anxiety, depression and resilience on PTG, there were different conclusions. At present, researches tend to analyze the relationship of anxiety, depression, resilience and PTG from a single aspect, lacking integrated quantitative analysis of 3 variables. It is important to select appropriate evaluation tools to evaluate and further explore the relationship between anxiety, depression, resilience, and PTG. Furthermore, there is still no study showing what makes anxiety and depression reach PTG. This study chose resilience as a mediator to explore the bridge of resilience in anxiety, depression and PTG development. In addition, this study also investigated the effects of anxiety and depression on PTG in breast cancer patients with different levels of resilience.
The main hypotheses of the study were the followings:
Hypothesis 1: Resilience is a mediator between anxiety, depression, and PTG among breast cancer patients undergoing chemotherapy.
Hypothesis 2: The effects of anxiety and depression on PTG may be different under different levels of resilience.
2. Material and methods
2.1. Ethics
All the participants were notified of the aim of the study and their right to attend or quit the investigation voluntarily, and they had signed written informed consent prior to the of the study. During the research process, researchers ensured that participants’ private information would be kept secret and that only summary data would be reported. The study has obtained approval from Ethics Committee of First Hospital of Shanxi Medical University, with approval No. 2018023.
2.2. Participants
A convenience sampling method was used to select 260 breast cancer patients who underwent chemotherapy in the breast surgery ward of the First Hospital of Shanxi Medical University in China from November 2017 to January 2019. According to the requirements for constructing the structural model,[17] the number of samples is determined by the number of model observation variables, and the ratio of sample number to observed variables is at least between 10:1 and 15:1. Considering the 12 observation variables, a ratio of 15:1 to and 20% of follow-up loss rate, 216 cases of breast cancer patients was required in the model, and we actually included 260 cases of breast cancer patients. 244 valid questionnaires were recovered, and the effective recovery rate was 93.8%, 16 cases were not constructed and analyzed by structural equation modeling (as shown in Fig. 1).
Figure 1.
Flowchart of subject enrollment and screening.
These participants met the study criteria:
-
1)
pathological diagnosis of breast cancer, TNM stage I-IV patients
-
2)
age ≥18 years old
-
3)
the patients were informed with their diagnosis
-
4)
voluntary participation
-
5)
undergoing chemotherapy.
The exclusion criteria were as follows:
-
1)
recently encountered other major traumatic events (e.g., divorce, family death)
-
2)
other serious comorbidities (e.g., multiple cancers), and
-
3)
psychiatric diseases.
2.3. Measures
2.3.1. Post –traumatic growth questionnaire
PTG, the primary outcome variable, was measured by the post-traumatic growth inventory (PTGI), which was originally designed and developed by American psychologists Tedeschi and Calhoun[18] in 1996. The scale had been used in a reliability-effectiveness analysis on 204 breast cancer patients in China,[19] and it includes 5 dimensions: interpersonal relationship, new possibility, personal power, mental changes and life enjoyment, 21 items with a total score of 0 to 105 points. The higher the score, the higher the PTG level. Five factors can explain 67.85% of the variance, the total Cronbach α coefficient of the questionnaire is 0.926, and the half-fold reliability is 0.900.
2.3.2. Anxiety and depression questionnaire
The Chinese Hospital Anxiety and Depression Scale (HADS) was translated and revised according to foreign scales.[20] It consists of 2 subscales and 7 items of anxiety and depression in each subscale. The score of each item is 0 to 3, and the total score of each subscale is 0 to 21. The higher the score, the more severe the anxiety and depression. The Cronbach α coefficients of anxiety and depression subscales is 0.92 and 0.84, respectively.
2.3.3. Resilience questionnaire
The Connor-Davidson Resilience Scale (CD-RISC) was compiled by American scholars in 2003.[21] The Chinese version was compiled by Yu XN.[22] It covers 3 dimensions of tenacity, strength, and optimism, or a total of 25 entries. Using the Likert 5 rating, the total score is 0 to 100 points. The higher the score, the higher the level of psychological resilience. The Cronbach α coefficient of the scale is 0.91.
2.4. Data collection
Prior to data collection, the patients and their main caregivers were informed of detailed purpose and significance of the study and signed the informed consent voluntarily. The General Hospital Anxiety and Depression Scale and CD-RISC were completed during the hospitalization of patient on chemotherapy. The PTGI was completed after the patient's chemotherapy was completed. The data collection was carried out by 2 graduate students, and 2 trained head nurses assisted the process. The staffs reminded each other whether the mutual supervision was completed according to the prescribed time, ethical principles, and quality control regulations. The tutor conducted terminal quality control. Every Friday afternoon, members of the research team actively feedbacked the problems that arose during the data collection process, and common problems were discussed. Unify instructions were used during the process of collecting data, and the patients filled the questionnaires in the ward demonstration classroom. The data collectors explained the questions in detail for those unfamiliar to the questionnaires or having difficulty in writing. The questionnaires were taken back immediately after the completion and the data collected should be kept by a project leader and not be changed at will.
2.5. Statistical analysis
Pearson correlations was used for the univariate statistical analyses to investigate whether resilience is correlated with anxiety, depression and PTG. Data analysis was carried out using the statistical package SPSS 22.0 and AMOS 21.0, and P value ≤.05 was considered as statistically significant. Moreover, we constructed a structural equation model to clarify the relationship between anxiety, depression, mental resilience, and PTG, and derived the path coefficient. The structural equation hypothesis model used anxiety and depression as independent variables, psychological resilience as mediator, and PTG as dependent variable. All dimensions of the three scales were included in the structural equation model for path relationship and influence effect analysis. Maximum likelihood method was applied to data fitting and model fitting evaluation was performed using absolute fitting index and relative fitting index. Harman[23] single factor test was employed in the common method deviation calculation. Microsoft Office Excel 2007 was used to draw simple slope moderating figures analysis. The average score of each scale was analyzed by multiple regression.
3. Results
3.1. Common method deviation test
Using the method of Harman single factor to reduce dimensionality factor-non-rotation analysis for common method deviation test, we found that there are 12 factors with eigenvalues greater than 1. The odds of the first factor was 20.16%, lower than 40% of the standard by Podsakoff, indicating that there was no serious common method bias.[23]
3.2. Relationship among anxiety, depression, resilience, and PTG
In our study, correlational analyses showed that anxiety, depression, resilience, and PTG were related. Anxiety had a negative correlation with resilience and PTG (r = –0.237, P < .01 and r = -0.344, P < .01); so was depression (r = –0.283, P < .01 and r = –0.317, P < .01), but there was a significant positively correlation between resilience and post-traumatic growth (r = –0.379, P < .01) (Table 1).
Table 1.
Correlations between anxiety, depression, resilience and post-traumatic growth in patients with breast cancer (r).
| Variables | Anxiety | Depression | Optimism | Tenacity | Power | Resilience | Interpersonal relationship | New possibility | Personal power | Mental changes | Life enjoyment | PTG |
| Anxiety | 1 | — | — | — | — | — | — | — | — | — | — | — |
| Depression | 0.909∗∗ | 1 | — | — | — | — | — | — | — | — | — | — |
| Optimism | –0.209∗∗ | –0.260∗∗ | 1 | — | — | — | — | — | — | — | — | — |
| Tenacity | –0.262∗∗ | –0.341∗∗ | 0.576∗∗ | 1 | — | — | — | — | — | — | — | — |
| Power | –0.205∗∗ | –0.239∗∗ | 0.457∗∗ | 0.595∗∗ | 1 | — | — | — | — | — | — | — |
| Resilience | –0.237∗∗ | –0.283∗∗ | 0.611∗∗ | 0.714∗∗ | 0.978∗∗ | 1 | — | — | — | — | — | — |
| Interpersonal relationship | –0.344∗∗ | –0.304∗∗ | 0.113∗ | 0.299∗∗ | 0.304∗∗ | 0.309∗∗ | 1 | — | — | — | — | — |
| New possibility | –0.237∗∗ | –0.221∗∗ | 0.009 | 0.177∗∗ | 0.132∗ | 0.131∗ | 0.755∗∗ | 1 | — | — | — | — |
| Personal power | –0.306∗∗ | –0.280∗∗ | 0.172∗ | 0.287∗∗ | 0.312∗∗ | 0.307∗∗ | 0.860∗∗ | 0.748∗∗ | 1 | — | — | — |
| Mental changes | –0.174∗ | –0.149∗ | 0.194∗∗ | 0.197∗∗ | 0.467∗∗ | 0.443∗∗ | 0.342∗∗ | 0.316∗∗ | 0.304∗∗ | 1 | — | — |
| Life enjoyment | –0.303∗∗ | –0.278∗∗ | 0.101∗ | 0.177∗∗ | 0.269∗∗ | 0.246∗∗ | 0.646∗∗ | 0.480∗∗ | 0.550∗∗ | 0.255∗∗ | 1 | — |
| PTG | –0.344∗∗ | –0.317∗∗ | 0.199∗ | 0.299∗∗ | 0.391∗∗ | 0.379∗∗ | 0.924∗∗ | 0.812∗∗ | 0.888∗∗ | 0.530∗∗ | 0.756∗∗ | 1 |
P < .05.
P < .01.—: blank.
3.3. The mediation role of resilience between anxiety, depression and PTG
The model was constructed using anxiety or depression as exogenous latent variable (independent variable), resilience as mediator variable, and PTG as endogenous latent variable (dependent variable). Each dimension of the three scales was an observed variable. The initial model has root mean square error of approximation > 0.1, relative fit index < 0.9, and was not well adapted. So we modified it by using Bias-corrected confidence intervals and relaxing the 2-dimensional variable limits of strength and mental change according to the maximum principle of the Modification Indices index to meet the normal adaptation criteria. Normed Chi-squared < 5, GFI, normed fit index, comparative fit index were all greater than 0.9, and root mean square error of approximation < 0.1, indicating good model fitting[24,25] (See Table 2 for each fitting index). The relationship between the relevant variables and the path coefficients were shown in Figure 2 and Figure 3. The significance test results of the path coefficient were shown in Table 3. The effects of anxiety, depression and resilience on PTG were shown in Table 4. Anxiety and depression could negatively predict resilience in a direct manner and the standardized estimated value of path coefficient was –0.388 (P < .05); what's more, the resilience had a positively predictive effect on PTG and the standardized estimate of the path coefficient was 0.253 (P < .05). It also showed that anxiety and depression were negatively predictive of PTG in an indirect manner with resilience as a mediator and the standardized estimate of path coefficient was –0.223 (P < .05). The overall effect of anxiety and depression on PTG was –0.321 (P < .05), and the direct effect was –0.223 (P < .05), suggesting that the effect of anxiety and depression on PTG could be partially buffered by the mediator of resilience, accounting for 30.53% of the total effect (indirect effect/total effect, –0.098/–0.321).
Table 2.
The evaluation index and fitting results of the overall fitting content of structural equation model.
| Fitting index | NC | NFI | RFI | IFI | TLI | CFI | RMSEA |
| Initial model | 4.072 | 0.916 | 0.881 | 0.935 | 0.908 | 0.934 | 0.112 |
| Modified model | 2.795 | 0.944 | 0.918 | 0.963 | 0.946 | 0.963 | 0.086 |
| Fitting standard | <5 | >0.9 | >0.9 | >0.9 | >0.9 | >0.9 | <0.1 |
Figure 2.
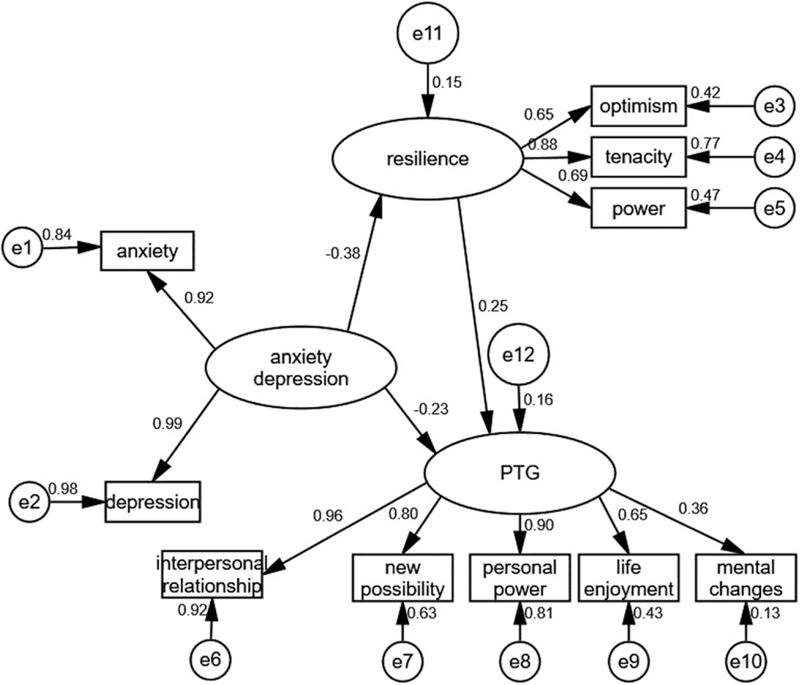
The initial model that resilience mediated partially between anxiety, depression, and post-traumatic growth growth.
Figure 3.
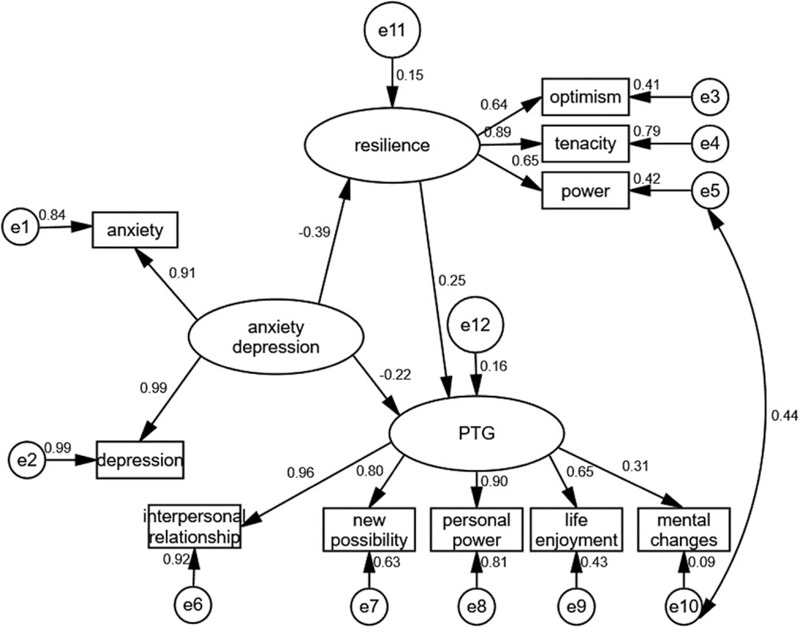
The modified model that resilience mediated partially between anxiety, depression, and post-traumatic growth.
Table 3.
Estimated values of model path coefficients and significance test results.
| Normalized path coefficient estimate | SE | CR | P | |
| Resilience<----Anxiety, Depression | –0.388 | 0.019 | –4.962 | .001 |
| PTG<----Resilience | 0.253 | 0.055 | 2.712 | .007 |
| PTG<----Anxiety, depression | –0.223 | 0.011 | –2.782 | .005 |
SE is the standard error of the estimated value.
CR is the critical ratio.
Table 4.
Effect value of anxiety, depression, resilience, and post-traumatic growth.
| Independent variable | Dependent variable | Direct effect | Indirect effect | Total effect |
| Anxiety, Depression | PTG | –0.223 | –0.098 | –0.321 |
| Resilience | PTG | 0.253 | 0.000 | 0.253 |
| Anxiety, Depression | resilience | –0.388 | 0.000 | –0.388 |
3.4. The moderating role of resilience in the anxiety, depression and PTG in patients with breast cancer
A stratified regression analysis was used to varify the effects of moderation, that is, to verify the existence of interactions. The first layer controlled the three general demographic data of family monthly income, disease staging, and marital status, the second layer added centralized anxiety, depression and resilience, and the third layer added centralized interactions of anxiety, depression and resilience. The results showed that after controlling the general demographic variables, the resilience had a significant effect on anxiety, depression and PTG among breast cancer patients (ΔR2 > 0, P < .05, 95% Bootstrap confidence interval did not include 0). The fitting effect index and regression coefficient of each moderating effect were shown in Table 5 and Table 6. The resilience score was higher than the high group (average score plus one standard deviation) and lower than the low group (average score minus 1 standard deviation), between the 2 was a medium group, describing by a simple slope moderation effect figure. The results showed that the anxiety and depression of patients with different levels of resilience had different effects on PTG, and the interaction was significant. It can be concluded that the effect of anxiety and depression on PTG in patients with high resilience was greater than that of patients with moderate or low resilience. In the same level of anxiety and depression, patients with high resilience can achieve greater PTG growth rates than those with moderate or low resilience. See Figure 4 and Figure 5.
Table 5.
Test of the moderation effect of resilience between anxiety and post-traumatic growth.
| Overall fit index | Regression coefficient significance | |||||||||
| Variables | F | R2 | ΔR2 | B | SE | β | t | P | Lower Bootstrap | Upper Bootstrap |
| The first layer | 12.025 | 0.168 | 0.168 | .000 | ||||||
| Constant term | 64.252 | 2.271 | — | 28.290 | .001 | 60.463 | 68.350 | |||
| Family monthly income level | 1.893 | 0.338 | 0.425 | 5.607 | .000 | 1.262 | 2.533 | |||
| Disease stage | –1.112 | 0.436 | –0.164 | –2.550 | .011 | –1.780 | –0.488 | |||
| Marital status | 1.183 | 0.459 | 0.165 | 2.577 | .011 | 0.150 | 2.200 | |||
| The second layer | 33.984 | 0.462 | 0.295 | .000 | ||||||
| Anxiety | –0.642 | 0.076 | –0.470 | –8.400 | .000 | –0.824 | –0.491 | |||
| Resilience | 0.145 | 0.042 | 0.178 | 3.480 | .001 | 0.053 | 0.276 | |||
| The third layer | 47.798 | 0.586 | 0.124 | 0.000 | ||||||
| (anxiety -251658240)∗(resilience -251658240) | –0.047 | 0.006 | –0.473 | –8.409 | 0.000 | –0.059 | –0.037 | |||
Table 6.
Test of the moderation effect of resilience between depression and post-traumatic growth.
| Overall fit index | Regression coefficient significance | |||||||||
| Variables | F | R2 | ΔR2 | B | SE | β | t | P | Lower Bootstrap | Upper Bootstrap |
| The first layer | 12.025 | 0.168 | 0.168 | .000 | ||||||
| Constant term | 64.252 | 2.271 | — | 28.290 | .001 | 60.527 | 68.313 | |||
| Family monthly income level | 1.893 | 0.338 | 0.425 | 5.607 | .000 | 1.280 | 2.574 | |||
| Disease stage | –1.112 | 0.436 | –0.164 | –2.550 | .011 | –1.752 | –0.469 | |||
| Marital status | 1.183 | 0.459 | 0.165 | 2.577 | .011 | 0.135 | 2.221 | |||
| The second layer | 33.147 | 0.456 | 0.289 | .000 | ||||||
| Depression | –0.745 | 0.091 | –0.472 | –8.189 | 0.000 | -0.935 | –0.581 | |||
| Resilience | 0.138 | 0.043 | 0.177 | 3.232 | 0.001 | 0.055 | 0.267 | |||
| The third layer | 42.400 | 0.557 | 0.101 | 0.000 | ||||||
| (depression -251658240)∗(resilience -251658240) | –0.051 | 0.007 | –0.428 | –7.328 | 0.000 | –0.065 | –0.036 | |||
Figure 4.
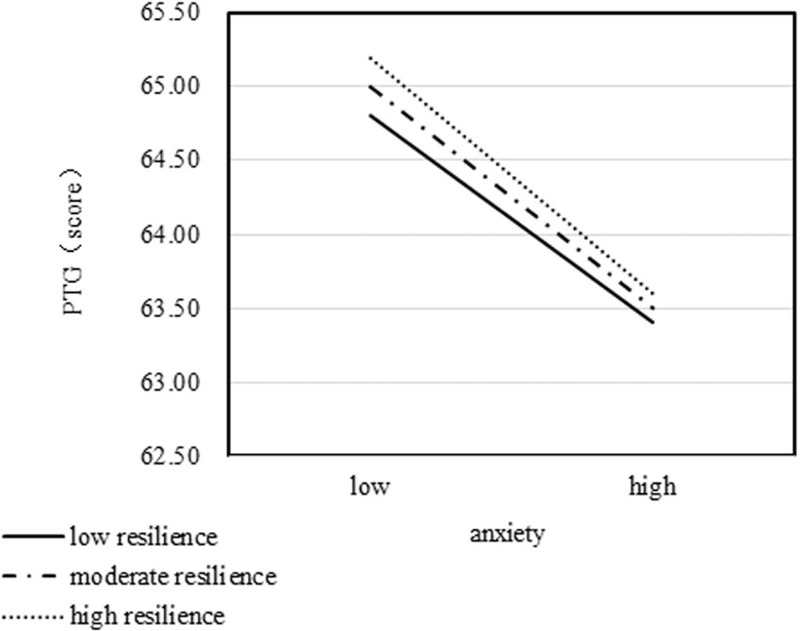
Effect of resilience on the relationship between anxiety and post-traumatic growth.
Figure 5.
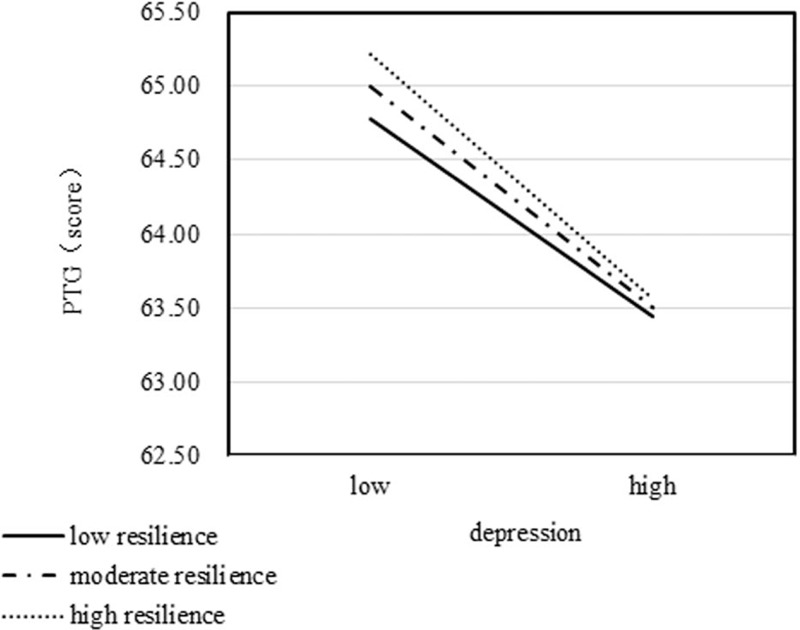
Effect of resilience on the relationship between depression and post-traumatic grow.
4. Discussion
4.1. Anxiety, depression, resilience, and PTG in patients with breast cancer during chemotherapy was relevant
Anxiety and depression were the most common psychological problems in patients with breast cancer.[26] Its existence can affect the physical and mental health of cancer patients. A good mental state or strong resilience can make a tumor patient take positive coping styles and overcome traumatic events that can cause adverse effects such as anxiety and depression. So, resilience could function as an index to evaluate the individual's psychological coping ability and degree of change in traumatic events. It was inseparable from the adverse psychological emotions such as anxiety and depression and the final physical and mental growth outcomes of breast cancer patients undergoing chemotherapy. This study was consistent with the results of Koutrouli study,[27] in which 202 patients with breast cancer were enrolled to construct a PTG-related factor predictive model.
4.2. The mediating role of resilience between anxiety, depression and PTG
4.2.1. Anxiety and depression had direct and indirect negative effects on PTG
The anxiety and depression scores of breast cancer patients in this study were negatively correlated with PTG. The more severe the anxiety and depression of patients, the more unfavorable the development of PTG. The structural equation model showed that the total effect of anxiety and depression on PTG in breast cancer patients was –0.321. Anxiety and depression not only had a direct negative effect on PTG, but also indirectly affect PTG by resilience. Wittmann Victoria[28] 18-month longitudinal study of patients with changes in quality of life and psychological characteristics suggested that anxiety and depression were important predictors of PTG, and that low levels of anxiety and depression were important buffers for stress. Good psychological quality encouraged breast cancer patients to adapt to and respond to traumatic events quickly and enhance PTG levels. Kenne Sarenmalm E et al[29] found in a randomized controlled trial of 166 breast cancer patients that, both group and individual mindfulness-based stress reduction therapy alleviated anxiety and depression, suggesting that psychological intervention played an important role in reducing anxiety and depression. According to Guidelines on Chinese Cancer Psychotherapy issued by the China Cancer Anti-Cancer Association in 2016[20] and 2017 Breast Cancer Diagnosis and Treatment Guidelines and Specifications,[30] medical workers should comprehensively evaluate patients’ mental and physical problems throughout the process, and give positive psychological intervention or instruction to refer patients to the department of oncology psychology and psychiatry, thus establishing a multidisciplinary collaboration mechanism. The tumor and psychology related departments are supposed to work together to promote the psychological rehabilitation of cancer patients, and promote patients to grow positively as soon as possible.
Anxiety and depression had direct and indirect negative effects on PTG in breast cancer patients. Medical workers shall directly intervene negative emotions such as anxiety and depression, and try to explore the internal mechanisms that may affect the effects of anxiety and depression on PTG. Other negative emotions, such as anger, irritability, paranoia, personality disorder may also affect PTG and need further classification and comparison studies.
4.2.2. Resilience was a partial mediator variable affecting PTG in breast cancer patients
Structural equation model analysis showed that resilience had a direct positive effect on PTG, suggesting its new function as a partial mediator of PTG at the end of chemotherapy in breast cancer patients. It was found that one of the key factors in relieving the effects of anxiety and depression on PTG in patients with breast cancer during chemotherapy was good resilience. Patients with higher resilience may have lower levels of anxiety and depression, and were more likely to actively respond to and adjust for traumatic events, or to alleviate the adverse effects of anxiety and depression, develop to a good PTG mode. On the contrary, patients with low resilience were more susceptible to disease and poor family social function, aggravating the vicious circle of anxiety and depression, which was not conducive to the digging and exertion of positive psychological functions, leading to a decline in PTG levels. As the main body of breast cancer patients adhering to treatment, medical staff should encourage family caregivers to pay attention to patients’ psychological reactions. At the same time, there was also a need to call on professional psychologists to carry out relevant lecture activities, strengthen communication between patients, guide patients to release positive emotions, finally improving their PTG level. The breast cancer disease itself and the physical pain caused by chemotherapy had posed new challenges to patient's psychological state. It was of great significance to improve the plasticity of breast cancer patients in the face of traumatic events and improve the compliance of self-treatment diseases by regulating scientific psychological interventions. Li[31] constructed a structural equation model for the relationship between family resilience, family burden, quality of life and PTG in China, and found that family resilience played a part in mediating patients’ quality of life and PTG. Good family resilience can effectively alleviate the burden of family members’ care, indirectly relieve the patient's psychological burden and negative emotions, and promote PTG in the late stage of chemotherapy.
Parallel intermediary[32] refers to the relationship path in which more than 1 intermediate path is studied. The path relationship underlies the mechanism of parallel interaction. In the other hand, chained intermediary[33] refers to the multi-step relationship of the intermediate path in the study and presents multiple intermediaries of the chain-like order relationship. The partial mediating effect of resilience in this study suggested that anxiety and depression in breast cancer patients may achieve good psychosomatic development outcomes through other single mediators, or there may be parallel or single-step and multi-step chain mediation to promote changes in PTG levels. It is of great clinical value and significance to construct multi-level structural equation model, so further exploration can focus on the relationship between psychological symptoms and PTG and clarify the weight of mediating effect, which may contribute to better instruction of professional psychological intervention and helping breast cancer patients achieve the harmony between body and mind, individual and family.
4.2.3. Path analysis showed that the strength dimension of resilience was associated with the mental change dimension of PTG
The power dimension of resilience indicated that breast cancer patients with higher resilience score had a better psychological strength corresponding to the disease, could better adapt to and concentrate attention on changes, and clearly considered their own stresss after getting illness. This has a good effect on the patient's understanding of the spiritual world and improving his mental outlook, thereby increasing the level of PTG. The cross-dimensional correlation between strength and mental change highlighted the significant effect of the mediating variable on the PTG outcome variable. Catarina Ramos[34] conducted a multicenter randomized controlled trial of 205 non-metastatic (I-III) female breast cancer patients in Portugal. He had implemented 8 cycles of group psychological intervention and evaluated PTG level, stress perception, core belief, inner reflection, and social support during intervention, 6 months after intervention, and 12 months follow-up. The group's psychological intervention was found to be an important supplement to promote the ending of chemotherapy (6 months) and 12-month PTG levels in breast cancer patients. A reasonable explanation was mainly that psychological intervention firstly promoted patients’ attention to positive effects of their own diseases, thereby enhancing their ability to fight against disease and improve the spiritual world, instead of spending more energy and time worrying about the future. Even accepting chemotherapy, it could help patients form a good belief in treatment, overcome adverse stresss, strengthen inner reflection on post-traumatic stress disorder, better learn changes in their spiritual world, and proactively obtain better medical care and family support, enhance the sense of strength against disease, lead to good changes in mental outlook, and thus improve the level of PTG. Both studies suggested that the correlation between these 2 dimensions may be extended and applied to other cancer patients. The correlation between the acquisition of strength and the mental changes, the influencing factors and the intrinsic mechanism of breast cancer patients’ resistance to disease can be further explored through multi-center large sample data.
4.3. Effect of anxiety and depression on PTG in breast cancer patients with different levels of resilience
The moderation effect mainly analyzes when the independent variable X would affect the dependent variable Y or whether it has a greater influence on Y.[35] Based on the principle of moderation effect, we further explored anxiety and depression had influenced PTG to what extent in breast cancer individuals with different levels of resilience. This study found that patients with high resilience of breast cancer had a greater impact on PTG than those with moderate or low resilience. With the same level of anxiety and depression, patients with high resilience can achieve greater PTG rates than those with moderate or low resilience. The reason for this phenomenon may be that the PTG level of patients with high resilience under the same anxiety and depression was itself high, so the group was healed faster than the moderate and low resilience patients. It was showed that when the anxiety and depression values become lower, the slope value of the simple slope figure was larger. Patients in group of high resilience of breast cancers had a rapid rate of decline in PTG even in the condition of severe anxiety and depression, thus having better outcomes than those with moderate or low resilience. A high level of resilience indicated that the breast cancer patients considered traumatic events more comprehensively, was able to take it more seriously and actively responded to the adverse effects caused by anxiety and depression. Mild psychological pain would attract their attention, impelled them to adopt a psychological coping strategy that tends to protect themselves, finally promoting their mental and physical development. In some breast cancer patients with high resilience, a slight change in anxiety and depression may lead to great fluctuations in PTG values, but in patients with low resilience, even if anxiety and depression were reduced, the extent of changes in their PTG levels will not be high. However, from the analysis of the slope value of the simple slope figure, it was found that no matter how the level of resilience changed, how the slope value decreased, the PTG level of patients with high resilience was higher than that of patients with low resilience.
4.4. Limitations
The results of this study had examined how well the structural equation model linked anxiety and depression with PTG through resilience. In addition, this study also explored the effects of anxiety and depression on PTG with different levels of resilience. However, several limitations of this study should be noted. First, in order to alleviate the effect of anxiety and depression on PTG from a wider perspective, more additional mediators should be examined by further studies, that is, whether the effects of anxiety and depression on PTG are influenced by other single intermediaries or chain mediators is worth exploring further. Second, this study was cross-sectional, and its conclusion should be verified in the future longitudinal study. Third, this study only discussed the relationship among breast cancer patients undergoing chemotherapy. Therefore, it is unclear whether the study's findings could apply to non-chemotherapeutic breast cancer patients. Future studies should evaluate whether similar results could be found among breast cancer patients at different stages of treatment. Due to the aforementioned limitations, the conclusion in the study should be reviewed cautiously.
5. Conclusion
Despite these limitations, this was the first time when the moderation and mediating role of resilience in the relationship between anxiety, depression, and PTG was investigated. These results could help us better learn the interactive mechanisms of anxiety, depression, and PTG among breast cancer patients on chemotherapy. The study also provided evidence that resilience plays a mediating role in anxiety, depression and PTG in breast cancer patients. At the same time, it was further tested by interaction effect that the effects of anxiety and depression on PTG in different states of resilience was different. The psychological problems of breast cancer patients should be paid more attention to, not only concerning about the impact of anxiety and depression on quality of life and treatment, but also focusing on the promoting factors of PTG. In addition, we should provide multi-angle and multi-channel supportive psychological care, guide patients to release positive emotions, mine their potential resilience, improve their level of resilience, stimulate their positive growth. That will provide a stronger support system for breast cancer patients to actively face cancer.
Acknowledgments
We thank all the participants who volunteered to share data and peers who helped to proofread the manuscript.
Author contributions
Linbo Li conceived the idea. Yongchao Hou and Xueliang wei performed the statistical analyses and wrote the first draft of the manuscript.
Fengying Kang and Linbo Li played a major role in the field survey. All the authors have checked and approved the final manuscript.
Conceptualization: Linbo Li, Fengying Kang.
Data curation: Linbo Li, Yongchao Hou.
Formal analysis: Xueliang Wei.
Investigation: Linbo Li, Yongchao Hou, Xueliang Wei.
Methodology: Linbo Li, Fengying Kang.
Software: Xueliang Wei.
Writing – original draft: Linbo Li, Yongchao Hou.
Writing – review & editing: Linbo Li, Fengying Kang.
Footnotes
Abbreviation: PTG = post-traumatic growth.
How to cite this article: Li L, Hou Y, Li L, Hou Y, Kang F, Wei X. The mediating and moderating roles of resilience in the relationship between anxiety, depression, and post-traumatic growth among breast cancer patients based on structural equation modeling: An observational study. Medicine. 2020;99:50(e23273).
The authors have no funding and conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Siegel Rebecca L, Miller Kimberly D, Jemal Ahmedin. Cancer statistics, 2019. CA Cancer J Clin 2019. 7–34. [DOI] [PubMed] [Google Scholar]
- [2].National Cancer Center. The 2018 National Cancer Report (2018). (EB/OL) (2018-02) (03-27-2018). Available at: http://www.360doc.com/content/18/0327/11/4485830_7405 65648.shtml [Google Scholar]
- [3].Batya EY, Caterina M, Giorgio R, et al. Extreme sensory processing patterns and their relation with clinical conditions among individuals with major affective disorders. Psychiatry Res 2016. 112–8. [DOI] [PubMed] [Google Scholar]
- [4].Monteiro S, Torres A, Morgadinho R, et al. Psychosocial outcomes in young adults with cancer: emotional distress, quality of life and personal growth. Arch Psychiatr Nurs 2013. 299–305. [DOI] [PubMed] [Google Scholar]
- [5].Tedeschi RG, Cann A, Taku K, et al. The posttraumatic growth inventory: a revision integrating existential and spiritual change. J Trauma Stress 2017. 11–8. [DOI] [PubMed] [Google Scholar]
- [6].Tomita M, Takahashi M, Tagaya N, et al. Structural equation modeling of the relationship between posttraumatic growth and psychosocial factors in women with breast cancer. Psychooncology 2017. 1198–204. [DOI] [PubMed] [Google Scholar]
- [7].Jaarsma TA, Pool G, Sanderman R, et al. Psychometric properties of the Dutch version of the posttraumatic growth inventory among cancer patients. Psychooncology 2006. 911–20. [DOI] [PubMed] [Google Scholar]
- [8].Schroevers MJ, Teo I. The report of posttraumatic growth in Malaysian cancer patients: relationships with psychological distress and coping strategies. Psychooncology 2008. 1239–46. [DOI] [PubMed] [Google Scholar]
- [9].Cordova MJ, Cunningham LL, Carlson CR, et al. Posttraumatic growth following breast cancer: a controlled comparison study. Health Psychol 2001. 176–85. [PubMed] [Google Scholar]
- [10].Helgeson VS, Reynolds KA, Tomich PL. A meta-analytic review of benefit finding and growth. J Consult Clin Psychol 2006. 797–816. [DOI] [PubMed] [Google Scholar]
- [11].Ma LL, Liu L, Wu LH, et al. Negative mood and post-traumatic growth in breast cancer patients: a longitudinal research. J Nurs 2016. 53–6. [Google Scholar]
- [12].Lim JW. The role of post-traumatic growth in promoting healthy behavior for couples coping with cancer. Support Care Cancer 2019. 829–38. [DOI] [PubMed] [Google Scholar]
- [13].Maurizio P, Marco I, Dorian AL, et al. The associations among childhood maltreatment “male depression” and suicide risk in psychiatric patients. Psychiatry Res 2014. 571–8. [DOI] [PubMed] [Google Scholar]
- [14].American Psychology Association. The road to resilience: What is resilience (2012) (EB/OL) (08-18-2012). Avaliable at: http://www.apa.org/helpcenter/road-resilience.aspx. [Google Scholar]
- [15].Kumpfer KL, Summerhays JF. Prevention approaches to enhance resilience among high-risk youth: comments on the papers of Dishion & Connell and Greenberg. Ann N Y Acad Sci 2006. 151–63. [DOI] [PubMed] [Google Scholar]
- [16].Gao W, Song SY, Bai HY, et al. Quality of life and its related factors in caregivers of patients with breast cancer. Chin J Pract Nurs 2018. 1686–91. [Google Scholar]
- [17].Wolf EJ, Harrington KM, Clark SL, et al. Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas 2013. 913–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress 1996. 455–71. [DOI] [PubMed] [Google Scholar]
- [19].Dong L, Hu Y, Xu GH, et al. Reliability and validity of the Chinese version of post-traumatic growth inventory scale in breast cancer survivors. J Nurs Sci 2013. 21–3. [Google Scholar]
- [20].China Cancer Society Professional Committee on Cancer Psychology. Guide to Chinese Cancer Psychotherapy (M). Beijing: People's Medical Publishing House; 2017. [Google Scholar]
- [21].Connor KM, Davidson JRT. Development of a new resilience scale: the Connor -Davidson resilience scale (CD-RISC). Depress Anxiety 2003. 76–82. [DOI] [PubMed] [Google Scholar]
- [22].Yu X, Zhang J. Factor analysis and psychometric evaluation of the Connor-Davidson resilience scale (CD-RISC) with Chinese people. Soc Behav Pers Int J 2007. 19–30. [Google Scholar]
- [23].Podsakoff PM, MacKenzie SB, Lee JY, et al. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol 2003. 879–903. [DOI] [PubMed] [Google Scholar]
- [24].Su H, Wang L, Li Y, et al. The mediating and moderating roles of self-acceptance and self-reported health in the relationship between self-worth and subjective well-being among elderly Chinese rural empty-nester: An observational study. Medicine 2019. e16149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Bagheri HM, Etemadinezhad S, Khanjani N, et al. Evaluating the relationship between job stress and job satisfaction among female hospital nurses in Babol: An application of structural equation modeling. Health Promot Perspect 2018. 102–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Schou BI, Faye-Schjøll HH. Pessimism predicts anxiety and depression in breast cancer survivors. A five-year follow-up study. Psychooncology 2019. 1314–20. [DOI] [PubMed] [Google Scholar]
- [27].Koutrouli N, Anagnostopoulos F, Potamianos G. Posttraumatic stress disorder and posttraumatic growth in breast cancer patients: a systematic review. Women Health 2012. 503–16. [DOI] [PubMed] [Google Scholar]
- [28].Wittmann V, Látos M, Horváth Z, et al. What contributes to long-term quality of life in breast cancer patients who are undergoing surgery? Results of a multidimensional study. Qual Life Res 2017. 2189–99. [DOI] [PubMed] [Google Scholar]
- [29].Kenne SE, Mårtensson LB, Andersson BA, et al. Mindfulness and its efficacy for psychological and biological responses in women with breast cancer. Cancer Med 2017. 1108–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].China Anti-Cancer Association Breast Cancer Professional Committee. China Anti-Cancer Association Breast Cancer Diagnosis and Treatment Guidelines and Regulations (2017 Edition). China Oncol 2017. 695–759. [Google Scholar]
- [31].Li Y, Qiao Y, Luan X, et al. Family resilience and psychological well-being among Chinese breast cancer survivors and their caregivers. Eur J Cancer Care (Engl) 2019. e12984. [DOI] [PubMed] [Google Scholar]
- [32].Jones CL, Jensen JD, Scherr CL, et al. The health belief model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Commun 2015. 566–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Elise BG, Siller LA. Child maltreatment, school bonds, and adult violence: a serial mediation model. J Interpers Violence 2018;5:886260518805763. [DOI] [PubMed] [Google Scholar]
- [34].Ramos C, Leal I, Tedeschi RG. Protocol for the psychotherapeutic group intervention for facilitating posttraumatic growth in nonmetastatic breast cancer patients. BMC Womens Health 2016. 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Roeder KM, Cole DA, Sinclair KR, et al. Sensitive periods for the effect of peer victimization on self-cognition: moderation by age and gender. Dev Psychopathol 2014;(4 Pt 1):1035–48. [DOI] [PubMed] [Google Scholar]