

Abstract
This study sought to investigate the recent incidence rate of myopia in Chinese junior high school students and analyze the effect of time spent outdoors on myopia, in addition to facilitating the prevention and control of myopia among students.
This study was derived from a national panel study, the China Education Panel Survey. We conducted three rounds of follow-up visits among 10,279 seventh grade students from 112 middle schools in 20 provinces in 2013. In total, 3571 students were selected for the analysis in 2020 by excluding those lost to follow-up and students who were myopic in the first round. The primary outcomes were the prevalence of myopia and the effect of time outdoors on myopia. The baseline characteristics of the included students were described, and the correlation between time spent outdoors and myopia in the three rounds of data was analyzed by a correlation chi-square test. Then, the generalized estimation equation (GEE) was used to estimate the influence of time spent outdoors on myopia after follow-up.
There were 3571 students with normal baseline vision, and 1508 (42.23%) students progressed from having a normal vision to myopia in the third round, of whom 706 (46.82%) were male and 802 (53.18%) were female. The results of the chi-square test showed that the time spent outdoors of all students and girls, specifically, was related to myopia (P < .05). Next, the GEE was used to analyze the influence of time spent outdoors on myopia after follow-up. After two model adjustments (individual and family-related characteristics of students), students with < 7 hours/week time spent outdoors retained a high myopia rate than ≥14 hours/week (OR = 1.250; 95% CI: 1.070–1.460). Among boys, there was no statistical correlation between time spent outdoors and myopia (P > .05). For girls, compared with students who spent ≥14 hours/week outdoors, students with <7 hours/week spent outdoors retained a higher myopia rate (OR = 1.355; 95%CI: 1.067–1.720).
Increased time spent outdoors can delay the development of myopia. In terms of gender, girls should be targeted to more effectively prevent and control the development and progression of myopia.
Keywords: children, myopia, time spent outdoors
1. Introduction
Myopia has become a major focus in the field of global public health.[1] Myopia not only affects physical and mental health, by causing retinal rupture, cataracts, and blindness, among others,[2] but also has a great impact on society. Statistical data demonstrate that the annual economic loss caused by uncorrected refractive errors is as high as US $220 billion, most of which is caused by myopia.[3] The World Health Organization released the first World Vision Report on October 8, 2019, revealing that over 2.2 billion people have a visual impairment or blindness worldwide.[4] It is estimated that the number of individuals with myopia globally will reach 4.758 billion (49.8% of the total population) by 2050. Furthermore, East Asia, such as China, Singapore, and South Korea, has the highest myopia rates, which are much higher than those in Europe and the United States.[5–9] China's myopia rate ranks first in the world, and its prevalence is the highest among the youth.[10] According to surveys by the National Health Commission and the Ministry of Education of the People's Republic of China and other departments, the overall rate of myopia among Chinese children and adolescents was 53.6% in 2018. Among them, 14.5% were 6-year-old children, 36.0% were primary school students, 71.6% were junior high school students, and 81.0% were high school students.[11] Studies have shown that increased time spent outdoors can effectively reduce the presence of myopia.[12–14] A longitudinal study by Jones et al found that the weekly time spent outdoors of myopic students (7.98 ± 6.54 hours) was lower than that of non-myopic students (11.65 ± 6.97 hours).[15] Adolescents can reduce their incidence of myopia by 2% for each additional hour of outdoor activity.[16] The “Guidelines for Appropriate Techniques for the Prevention and Control of Myopia in Children and Adolescents” formulated by the National Health Commission in 2019 mentions that schools, families, and communities work together to reduce long-term continuous myopia among children and adolescents and adopt a variety of measures to provide relevant conditions for children and adolescents, urging children and adolescents to engage in outdoor activities.[17] Teachers and parents should guide children in taking an active part in physical exercise, making children engage in more than 2 hours of daily day-time outdoor activities and suggesting that kindergarten-aged children should not engage in less than 3 such hours.[18] To this date, scholars have conducted extensive studies on myopia, time spent outdoors, and other factors,[19–22] but junior high school students have not been specifically targeted. Junior high school is a critical period in students’ growth and development, representing a transition in their academic burden. The myopia rate of junior high school students is significantly higher than that of primary school students. This paper selected the students with normal vision in grade 7 as the base point, re-investigated the students’ vision situation again after three years, and actually we obtained the changes of the students’ vision in three years of junior middle school.
Furthermore, this study further assessed the occurrence of myopia and the influence of time spent outdoors on myopia in junior high school students with normal eyesight over the course of 3 years to better inform the prevention and control of myopia among teenagers.
2. Methods
2.1. Study design and population
The China Education Panel Survey (CEPS) is a national panel survey project designed and implemented by the National Survey Research Center at Renmin University of China. The study was approved by the Ethics Committee of Renmin University of China. This survey uses a multi-stage probabilistic and scale proportional sampling method, having randomly selected representative 20 provinces, 28 districts and counties, 112 schools, 438 classes, and a total of 19487 students (10,279 in Grade 7 and 9208 in Grade 9) for follow-up surveys. The entire survey cycle is from 2013 to 2033. The specific details with regard to the implementation of the survey can be found in the literature.[23] In this study, seventh grade students with normal vision were selected at baseline as the research object. At the same time, data were selected from the baseline wave (the school year 2013–2014) and the third survey wave (in 2015–2016). In the end, a total of 3571 students (1931 boys and 1640 girls) who met the criteria were selected. Specific exclusion criteria are shown in Figure 1.
Figure 1.
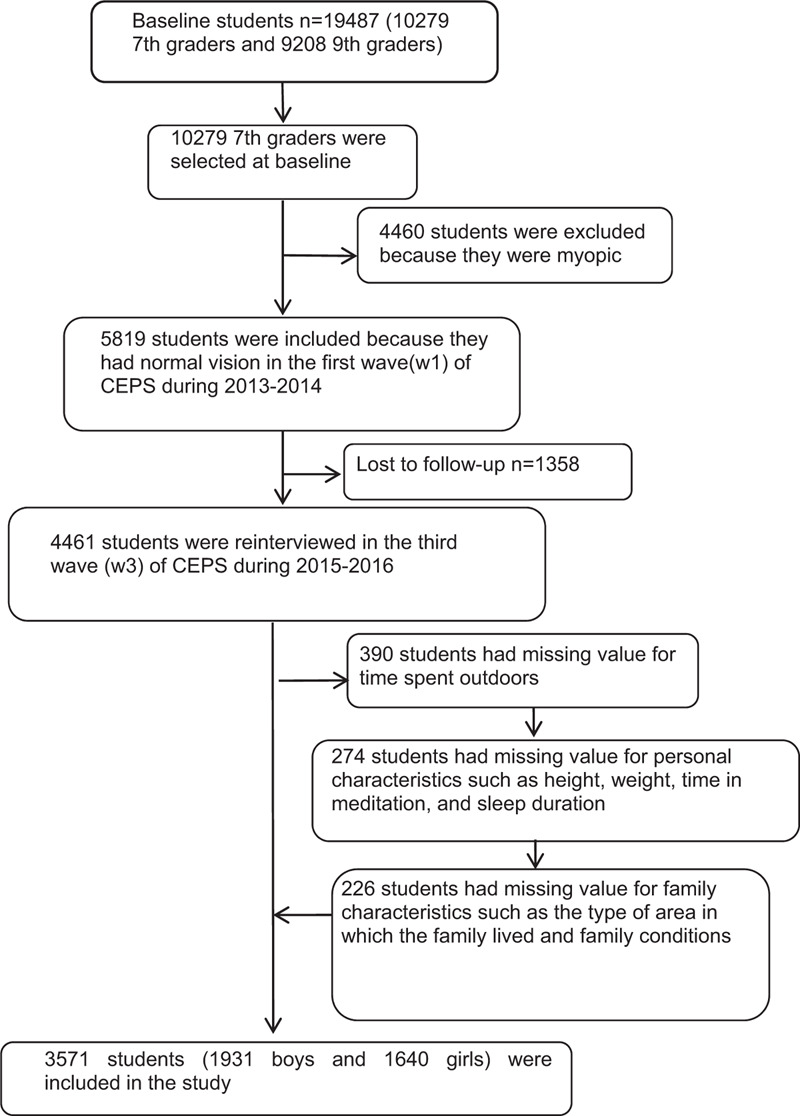
Participants’ flow in the study.
2.2. Data collection
The CEPS questionnaire included student questionnaire, parents questionnaire, homeroom teacher questionnaire, teacher questionnaire and headmaster questionnaire. The student questionnaire was about student basic information, academic growth, physical and mental health, social behavior development, growth and memory, etc; The parents questionnaire covered: family education, home-school relationship, school education, children's basic situation, problems of parents, family and community, etc; The questionnaire of head teacher included: head teacher work, teaching work, general work, personal and family questions, etc; The questionnaire for teachers included: teaching work, general work, personal and family questions, etc; The principal questionnaire included basic information of the school, basic information of junior high school students, basic information of junior middle school teachers, management work and personal basic information, etc.
This study selected student and parents questionnaire for waves 1 and 3, personal characteristics and family characteristics of students were collected by self-administered questionnaires. Personal characteristics included whether the students were only-children, as well as their gender, height, weight, time spent outdoors (hours/week), time in meditation (hours/week), sleep duration (hours/day), self-reported health status, time spent outdoors, and myopia prevalence after the follow-up, thereby allowing us to model the change in time spent outdoors change and the incidence of novel myopia cases. Students’ family characteristics included nationality, type of area in which the family lived, whether they lived with their parents, and family economic conditions. CEPS has been developed by experts over the course of multiple discussions, improved continuously through multiple trials, and finally successfully implemented throughout the country. Investigators have undergone rigorous professional training and qualification exams and signed confidentiality agreements. Investigators needed to conduct on-site supervisions and deliver explanations of interviewee-related issues, using a combination of on-site verification and telephone interviews to confirm that the questionnaires were being appropriately completed. The technical team then entered and organized the data, double-blinded. To complete the questionnaire, the consent of the interviewees (school leaders, teachers, parents, students) was required. If they did not consent, they were not included in the study sample.
2.3. Measures of myopic
The questionnaire assessed whether the students were myopic. Considering that junior high school students already have basic cognition and judgment abilities, as well as various cost issues such as manpower and material resources, this study used questionnaires to obtain students’ vision status. In the questionnaire survey, students wearing glasses were asked about their degree of wearing glasses, and condition of their eyesight were recorded. For students without glasses, asking them whether they could see the handwriting on the blackboard clearly, whether they could see the distant objects clearly, if the vision was fuzzy, it would be judged as nearsightedness. Meanwhile, if the vision status information in a student's questionnaire was missing, we used the information in the parent questionnaire as a supplement to further reduce the lack of data.
2.4. Measures of time outdoors
Time spent outdoors in the questionnaire was measured by an assessment of the time spent playing outside, walking, engaging in various activities, and extracurricular sports activities, among others, when students attended school from Monday to Friday but not on weekends and vacation. Weekly time spent outdoors was calculated as: (hours spent on a weekday) × 5 + (hours spent on a weekend day) × 2.[12] Combined with the recommendations of the Chinese Center for Disease Control and Prevention on time spent outdoors, relevant previously published literature, and the distribution characteristics of the data samples in this study, time spent outdoors was divided into three levels: <7, 7–14, and ≥14 (hours/week).[15,18]
2.5. Covariates
Each variable in the questionnaire had a specific definition, as follows. Whether students were only-children was categorized as yes or no. Gender was categorized as male or female. Time spent in meditation included time spent engaged in homework, reading, tutoring class, watching TV, and playing online games, among others, when students went to school from Monday to Friday but not on weekends and vacation. According to previously published literature and the distribution characteristics of the data samples, time in meditation was categorized into <28, 28–56, and ≥56 (hours/week).[24] Weekly meditation time was calculated in the same way as time spent outdoors. Sleep duration was divided into three phases, <7, 7–9, and ≥9 (hours/day).[25] Overweight and obesity were classified as non-overweight/obese and overweight/obese according to the Chinese health standard “Screening for overweight and obesity in school-age children and adolescents,” with body mass index (BMI) = weight(kg)/height(m)2.[26] Self-health status was classified as very good, better, average, and not so good. Myopia status was categorized as yes and no. Nationality was divided into Han and Minority nationalities, and the type of area in which the family lived was categorized as city/county city center, city/county fringe, city/county urban-rural junction, towns outside the city/county, countryside, or others. Whether students lived with their parents was categorized as living with both, living with one party, and not living with either party. Family economic conditions were classified as richer, medium, and very difficult.
2.6. Statistical analysis
First, a descriptive statistical analysis was used to describe the characteristics of students with normal vision at baseline. Next, a correlation chi-square test was used to analyze the correlation between changes in the time students with normal vision spent outdoors and the occurrence of myopia 3 years later. Finally, a generalized estimation equation (GEE) was used to test the connection between the influence of time spent outdoors on myopia after follow-up depending on gender. We used a GEE because the parameter estimates in this model remained relatively stable, addressing the challenge related to the longitudinal data correlation and allowing us to simulate flexibly the impact of time on the results.[27] In Model l, the analysis was unadjusted for any variables. In Model 2, it was adjusted for the personal characteristics of the students, and in Model 3, it was adjusted as for Model 2, alongside further adjustment for students’ family characteristics. A P value <.05 was considered statistically significant.
3. Results
3.1. Characteristics of students with normal vision at baseline wave
A total of 3571 students were included at baseline, of whom 1931 (54.07%) were boys and 1640 (45.93%) were girls. There were 1447 (40.52%) only-children, including 850 (44.02%) males and 597 (36.40%) females. Students mostly spent ≥14 hours/week outdoors, accounting for 1495 (41.87%) of all students, of whom 854 (44.23%) were boys and 641 (39.09%) girls. Most students spent 28 to 56 hours/week in meditation, of whom 1467 (41.08%) were female and 917 (47.49%) were male. A relatively high proportion of girls, 601 (36.65%), spent <28 hours/week in meditation. Most students slept 7 to 9 hours/day, representing a total of 1995 (55.87%) students, of whom 1034 (53.55%) were boys and 961 (58.60%) were girls. Most students, 3101 (86.84%), were neither overweight nor obese, of whom 1568 (81.20%) were boys and 1533 (93.48%) were girls. Most students, 1447 (40.52%), had a good health status, of whom 806 (41.74%) were boys and 641 (39.09%) were girls. There were more Han students, amounting to 3265 (91.43%) overall, of whom 1775 (91.92%) were boys and 1490 (90.85%) were girls. There were more rural students, amounting to 1644 (46.04%), of whom 877 (45.42%) were males and 767 (46.77%) were females. More than 64% of students lived with their parents, and more than 68% of students had medium family conditions (Table 1).
Table 1.
Characteristics of the baseline population.
| Number (%) | |||
| Characteristics | Females (n = 1640) | Males (n = 1931) | Total (n = 3571) |
| Personal characteristics | |||
| Whether the student were only-children | |||
| Yes | 597 (36.40) | 850 (44.02) | 1447 (40.52) |
| No | 1043 (63.60) | 1081 (55.98) | 2124 (59.48) |
| Time spent outdoors hours/week | |||
| <7 | 459 (27.99) | 535 (27.71) | 994 (27.84) |
| 7–14 | 540 (32.93) | 542 (28.07) | 1082 (30.30) |
| ≥14 | 641 (39.09) | 854 (44.23) | 1495 (41.87) |
| Time in meditation hours/week | |||
| <28 | 601 (36.65) | 455 (23.56) | 1056 (29.57) |
| 28–56 | 550 (33.54) | 917 (47.49) | 1467 (41.08) |
| ≥56 | 489 (29.82) | 559 (28.95) | 1048 (29.35) |
| Sleep duration (hours/day) | |||
| <7 | 110 (6.71) | 154 (7.98) | 264 (7.39) |
| 7–9 | 961 (58.60) | 1034 (53.55) | 1995 (55.87) |
| ≥9 | 569 (34.70) | 743 (38.48) | 1312 (36.74) |
| BMI | |||
| Non-overweight/obesity | 1533 (93.48) | 1568 (81.20) | 3101 (86.84) |
| Overweight/obesity | 107 (6.52) | 363 (18.8) | 470 (13.16) |
| Self-reported health status | |||
| Very good | 641 (39.09) | 806 (41.74) | 1447 (40.52) |
| Better | 590 (35.98) | 677 (35.06) | 1267 (35.48) |
| Average | 356 (21.71) | 376 (19.47) | 732 (20.50) |
| Not so good | 53 (3.23) | 72 (3.73) | 125 (3.50) |
| Family characteristics | |||
| Nationality | |||
| Han | 1490 (90.85) | 1775 (91.92) | 3265 (91.43) |
| Minority | 150 (9.15) | 156 (8.08) | 306 (8.57) |
| The type of area in which the family lived | |||
| City/county center | 479 (29.21) | 529 (27.40) | 1008 (28.23) |
| City/county fringe | 178 (10.85) | 243 (12.58) | 421 (11.79) |
| City/county urban-rural junction | 102 (6.22) | 124 (6.42) | 226 (6.33) |
| Towns outside the city/county | 87 (5.30) | 134 (6.94) | 221 (6.19) |
| Countryside | 767 (46.77) | 877 (45.42) | 1644 (46.04) |
| Others | 27 (1.65) | 24 (1.24) | 51 (1.43) |
| Whether students lived with their parents | |||
| Living with both | 1082 (65.98) | 1249 (64.68) | 2331 (65.28) |
| Living with one party | 307 (18.72) | 386 (19.99) | 693 (19.41) |
| Not living with either party | 251 (15.30) | 296 (15.33) | 547 (15.32) |
| Family economic conditions | |||
| Richer | 72 (4.39) | 121 (6.27) | 193 (5.40) |
| Medium | 1181 (72.01) | 1331 (68.93) | 2512 (70.34) |
| Very difficult | 387 (23.60) | 479 (24.81) | 866 (24.25) |
3.2. The rate of change in myopia was higher in junior middle school students
There were 3571 students with normal vision in the first wave (wave 1), and 1508 (42.23%) students progressed from having normal vision to myopia in the third wave (wave 3). There were a total of 706 (46.82%) boys and 802 (53.18%) girls. Figure 2 shows the relationship between changes in time spent outdoors and the incidence of new cases of myopia between waves 1 and 3. Myopia rates tended to decrease with increased time spent outdoors. A correlation chi-square test revealed that the amount of time both all students and female students’ time spent outdoors was related to myopia. A total of 2582 (1450 boys and 1132 girls) students altered the time they spent outdoors between waves 1 and 3. A total of 377 students’ time spent outdoors either remained stable at ≥7 hours/week or was decreased. Among these, there were 183 new myopia students, representing 48.54% of this cohort, among which 100 were female, accounting for 53.48%, and 83 were male, accounting for 43.68%. A total of 1067 students’ time spent outdoors remained stable, at 14 hours/week, between waves 1 and 3, while 398 students developed myopia, accounting for 37.30% of this cohort. Among these, there were 195 female myopic students, accounting for 44.42%, and 203 male myopic students, accounting for 32.32%.
Figure 2.
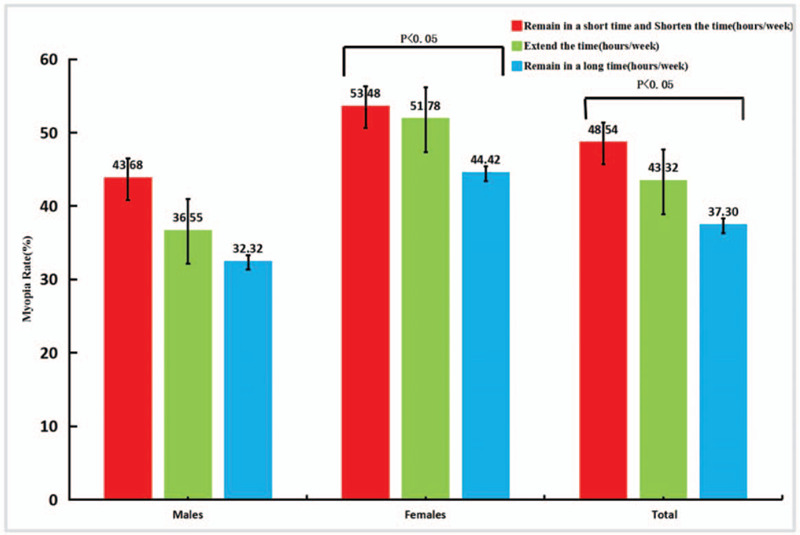
Relationship between changes of time spent outdoors of students and myopia incidence in w1-w3.
3.3. Students who spent more time outdoors had a lower rate of myopia than those who spent less time outdoors
Table 2 shows the influence of time spent outdoors on myopia after follow-up. In Model 1 (unadjusted for any variables), time spent outdoors had a negative correlation with the myopia rate of students. Compared with ≥14 hours/week time spent outdoors, students who spent <7 hours/week outdoors were more prone to developing myopia (unadjusted OR = 1.313; 95% CI: 1.154–1.495). In Model 2, after controlling for students’ personal characteristics, compared with ≥14 hours/week time spent outdoors, students who spent <7 hours/week time outdoors had a higher myopia rate (OR = 1.237; 95% CI: 1.062–1.441), while students who spent 7 to 14 hours/week did not have a significant relationship with myopia rate (P = .189). In Model 3, after adjusting for students’ personal characteristics and family characteristics, compared with ≥14 hours/week time spent outdoors, students who spent <7 hours/week outdoors retained high myopia rates (OR = 1.250; 95% CI: 1.070–1.460).
Table 2.
A longitudinal association between the time spent outdoors of students and myopia rate at follow-up (n = 3571).
| Model 1∗ | Model 2† | Model 3‡ | ||||
| Time spent outdoors hours/week | B | OR (95% CI) | B | OR (95% CI) | B | OR (95% CI) |
| Total | ||||||
| <7 | 0.272 | 1.313 (1.154,1.495) | 0.213 | 1.237 (1.062–1.441) | 0.223 | 1.250 (1.070–1.460) |
| 7–14 | −0.047 | 0.954 (0.826–1.102) | 0.041 | 1.041 (0.886–1.224) | 0.047 | 1.048 (0.890–1.234) |
| ≥14 | Reference | Reference | Reference | |||
unadjusted for any variables.
adjusted for students’ personal characteristics: whether the students were only-children, gender, height, weight, time in meditation (hours/week), sleep duration (hours/day), self-reported health status, etc.
adjusted for students’ personal characteristics: whether the students were only-children, gender, height, weight, time in meditation (hours/week), sleep duration (hours/day), self-reported health status, etc.; students’ family characteristics: nationality, the type of area in which the family lived, whether they lived with their parents, family economic conditions, etc.
3.4. Compared with boys, increasing time spent outdoors among girls was more effective in preventing myopia
Table 3 shows the time spent outdoors of students of different genders and the effect on myopia after follow-up. In Model 1 (unadjusted for any variables), for boys, compared with ≥14 hours/week time spent outdoors, boys who spent <7 hours/week outdoors were more likely to develop myopia (unadjusted OR = 1.121; 95% CI: 0.940–1.336), but this was not statistically significant. Among girls, in comparison to those who spent ≥14 hours/week outdoors, girls who spent <7 hours/week outdoors were more likely to develop myopia (unadjusted OR = 1.625; 95% CI: 1.334–1.979). In Model 2, after adjusting for students’ personal characteristics, among boys, there was no statistical correlation between time spent outdoors and myopia (P > .05); among girls, compared with ≥14 hours/week time spent outdoors, girls who spent <7 hours/week outdoors had higher myopia rates (OR = 1.358; 95% CI: 1.074–1.718). In Model 3, after adjusting for students’ personal and family characteristics, among boys, there was no statistical correlation between time spent outdoors and myopia (P > .05), while, among girls, compared with ≥14 (hours/week) time spent outdoors, girls who spent <7 hours/week outdoors retained higher myopia rates (OR = 1.355; 95% CI: 1.067–1.720).
Table 3.
A longitudinal association between the time spent outdoors of students of different genders and myopia rate at follow-up (n = 3571).
| Model 1∗ | Model 2† | Model 3‡ | ||||
| Time spent outdoors hours/week | B | OR (95% CI) | B | OR (95% CI) | B | OR (95% CI) |
| Males | ||||||
| <7 | 0.114 | 1.121 (0.940–1.336) | 0.158 | 1.171 (0.953–1.439) | 0.168 | 1.183 (0.960–1.457) |
| 7–14 | −0.211 | 0.810 (0.665–0.986) | −0.100 | 0.904 (0.727–1.125) | −0.091 | 0.913 (0.732–1.139) |
| ≥14 | Reference | Reference | Reference | |||
| Females | ||||||
| <7 | 0.485 | 1.625 (1.334–1.979) | 0.306 | 1.358 (1.074–1.718) | 0.304 | 1.355 (1.067–1.720) |
| 7–14 | 0.170 | 1.185 (0.954–1.472) | 0.233 | 1.263 (0.986–1.618) | 0.227 | 1.255 (0.976–1.614) |
| ≥14 | Reference | Reference | Reference | |||
unadjusted for any variables.
adjusted for students’ personal characteristics: whether the students were only-children, height, weight, time in meditation (hours/week), sleep duration (hours/day), self-reported health status, etc.
adjusted for students’ personal characteristics: whether the students were only-children, height, weight, time in meditation (hours/week), sleep duration (hours/day), self-reported health status, etc.; students’ family characteristics: nationality, the type of area in which the family lived, whether they lived with their parents, family economic conditions, etc.
4. Discussion
In 3 waves of surveys, we analyzed the new incidence of myopia in 3571 normal-vision students at baseline wave and 1508 (42.23%) students who progressed from normal vision to myopia. Simultaneously, the vertical relationship between time spent outdoors and myopia of this cohort of students was analyzed. After 2 model adjustments (adjusting for personal and family characteristics), we found that time spent outdoors and myopia were still correlated. This result was consistent with previous studies, which showed that time spent outdoors had a negative effect on myopia. Increasing time spent outdoors could effectively suppress the progression of myopia.[13,28,29] For example, in a cohort study, Guggenheim et al found that what was closely related to the occurrence and development of adolescent myopia was the time spent outdoors, rather than the intensity of the activity.[30] Studies by Rose and others have shown that 29.1% of Chinese adolescents living in Singapore had myopia, compared to only 3.3% of Chinese people of the same age living in Sydney. This investigation found that Chinese teenagers living in Sydney spent 13.8 hours per week outdoors, compared with 3.1 hours in Singapore.[31]
Some scholars have found that the outdoor environment had a unique protective effect on myopia. These effects included a relatively flat diopter terrain in outdoor scenes, spacious outdoor visual spaces, high luminosity outdoors, and particular blue light components.[32,33] Some studies have also pointed out that sunlight outdoors can stimulate the retina to release dopamine and slow the development of myopia.[34] In addition, outdoor sunlight may easily promote the body's secretion of dopamine, slowing down eye lengthening and reducing the rate of myopia.[35] In a randomized controlled trial, Wang et al found that exposure to natural outdoor light could reduce myopia caused by defocusing. In addition, the exposure of rhesus monkeys to sunlight in early childhood could promote their normal development in adulthood, thereby reducing the risk of myopic refractive errors.[32] The results of Ashby et al showed that, compared with conventional experimental lighting conditions (500 lux), chicks exposed to sunlight and artificial light (15,000 lux) were less likely to develop myopia.[36] Scott et al found that children with greater average daily light exposure experienced a slower axial eye growth in an 18-month longitudinal study.[37] Wu et al found, in a Taiwanese prospective intervention study, that the new incidence rate of myopia (8.41%) in students in the outdoor activity intervention group was lower than that in the control group (17.65%). Outdoor activities interventions for non-myopic students are effective in enabling the prevention and control of myopia.[38] This article further assessed the relationship between time spent outdoors and myopia according to gender. Compared with boys, girls had a higher risk of developing myopia. This was consistent with certain previous research results.[39–41] After two model adjustments of the generalized estimation equation, among girls, time spent outdoors in a short period of time still maintained high rates of myopia. Among boys, after controlling for other factors, the impact of boys’ time spent outdoors on myopia was less obvious. This could be attributed to a number of factors. First, there were physiological differences between boys and girls. Studies have found that estrogen affected the expression of more than 600 genes in corneal epithelial cells.[42] In addition, corneal thickness was positively related to myopia diopter.[43] The junior high school stage is a critical period for student development. Due to the effects of growth hormones and estrogen, girls’ growth and development would reach a peak, and organ functional disorders might cause changes to the eye and other tissue structures.[44,45] This may be the reason for which myopia rates were higher in girls than boys in junior high school. Second, due to the fierce social competition and the high expectations of parents, Chinese middle school students have a heavy academic burden and educational pressure.[1] Some surveys showed that 73.1% of Chinese junior high school students have overtime schoolwork, and 38.1% of students engage in extracurricular tutorial classes.[46] At the same time, girls undergo puberty earlier than boys.[44,45] Girls also tend to reach educational milestones earlier than boys, showing longer reading and writing times at close distances, and engaging in relatively fewer outdoor activities. On the contrary, the vast majority of boys spent more time outdoors and less time in meditation. There similar times spent outdoors lead to insignificant differences in myopia. The second reason is that boys’ myopia is controlled by multiple behaviors, and its mechanism of impact has not yet been clarified. In terms of preventing myopia, it is suggested that girls should be key targets, to better enable the prevention and control of myopia.
However, this study had several limitations. Firstly, the data collected in this article was sourced from student self-filled questionnaires. There may have been memory or non-respondent biases as such. Secondly, only the time spent outdoors was assessed. The activity intensity and the activity intervals were not considered. In the future, outdoor activity intensity and other factors can be further assessed.
5. Conclusions
This study was based on a cohort survey of junior high school students in China. We found that longer periods spent outdoors played a vital role in the prevention and control of myopia among students. In terms of gender, increasing time spent outdoors among girls statistically significantly reduced myopia, but this statistical association did not exist in boys. Scholars should pay more attention to time spent engaged in outdoor activities and analyze its value in the further research on healthy lifestyles. This study shows that during three years period, the factors influencing students’ myopia rates changed little, even though, in reality, the increase in students’ growth and development and the academic burden are associated with a certain degree of change in their visual acuity. As such, in future studies, more thorough studies based on a larger number and duration of follow-ups can be carried out.
Acknowledgments
The authors thank the government, schools, parents, students, and staff who contributed to the survey.
Author contributions
Conceptualization: Li Zhao
Funding acquisition: Li Zhao
Investigation: linjie Zhang
Methodology: Xiao yang Dong
Resources: Wei dong Wang, Li Zhao
Supervision: Li Zhao
Writing – original draft: linjie Zhang
Writing – review & editing: linjie Zhang, Wei dong Wang, Xiao yang Dong, Li Zhao, Peng Jia, Ronghai Wang
Footnotes
Abbreviations: CEPS = The China Education Panel Survey, CI = confidence interval, GEE = the generalized estimation equation, OR = odds ratio.
How to cite this article: Zhang L, Wang W, Dong X, Zhao L, Peng, J, Wang R. Association between time spent outdoors and myopia among junior high school students: a 3-wave panel study in China. Medicine. 2020;99:50(e23462).
LZ and WW contributed equally to this study.
This study was supported by China Education Panel Study: Junior High Cohort, Science Foundation of Renmin University of China (CEPS201911SK08).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
References
- [1].Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet 2012;379:1739–48. [DOI] [PubMed] [Google Scholar]
- [2].Wong TY, Ferreira A, Hughes R, et al. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: an evidence-based systematic review. Am J Ophthalmol 2014;157:9–25. e12. [DOI] [PubMed] [Google Scholar]
- [3].Smith TS, Frick KD, Holden BA, et al. Potential lost productivity resulting from the global burden of uncorrected refractive error. Bull World Health Organ 2009;87:431–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].World Health Organization. World vision report. https://www.who.int/zh/news-room/detail/08-10-2019-who-launches-first-world-report-on-vision. [access date May 27, 2020]. [Google Scholar]
- [5].Wu JF, Bi HS, Wang SM, et al. Refractive error, visual acuity and causes of vision loss in children in Shandong, China. The Shandong Children Eye Study. PLoS One 2013;8:e82763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016;123:1036–42. [DOI] [PubMed] [Google Scholar]
- [7].Ding BY, Shih YF, Lin LLK, et al. Myopia among schoolchildren in East Asia and Singapore. Surv Ophthalmol 2017;62:677–97. [DOI] [PubMed] [Google Scholar]
- [8].Jung SK, Lee JH, Kakizaki H, et al. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in Seoul, South Korea. Invest Ophthalmol Vis Sci 2012;53:5579–83. [DOI] [PubMed] [Google Scholar]
- [9].Lim HT, Yoon JS, Hwang SS, et al. Prevalence and associated sociodemographic factors of myopia in Korean children: the 2005 third Korea National Health and Nutrition Examination Survey (KNHANES III). Jpn J Ophthalmol 2012;56:76–81. [DOI] [PubMed] [Google Scholar]
- [10].Health China Action Promotion Committee.Health China Action (2019-2030). http://www.nhc.gov.cn/guihuaxxs/s3585u/201907/e9275fb95d5b4295be8308415d4cd1b2.shtml. [access date May 27, 2020]. [Google Scholar]
- [11].Zhang Y. The 2018 national survey on myopia among children and adolescents. Commission NH; 2019. [Google Scholar]
- [12].Guo Y, Liu LJ, Xu L, et al. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology 2013;120:277–83. [DOI] [PubMed] [Google Scholar]
- [13].Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol 2017;95:551–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in china: a randomized clinical trial. JAMA 2015;314:1142–8. [DOI] [PubMed] [Google Scholar]
- [15].Jones LA, Sinnott LT, Mutti DO, et al. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci 2007;48:3524–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Sherwin JC, Reacher MH, Keogh RH, et al. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology 2012;119:2141–51. [DOI] [PubMed] [Google Scholar]
- [17].National Health Commission. A Guide to Appropriate Techniques for Prevention and Control of Myopia in Children and Adolescents. http://www.nhc.gov.cn/jkj/s5898bm/201910/c475e0bd2de444379402f157523f03fe.shtml. [access date May 27, 2020]. [Google Scholar]
- [18].Chinese Center For Disease Control And Prevention.Core information on health education for children and adolescents with myopia prevention and control. http://www.nhc.gov.cn/jkj/s5898bm/201903/b74839d7967a4aae81a0bff216528262.shtml. [access date May 27, 2020]. [Google Scholar]
- [19].Huang L, Kawasaki H, Liu Y, et al. The prevalence of myopia and the factors associated with it among university students in Nanjing: A cross-sectional study. Medicine (Baltimore) 2019;98:e14777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Zhou J, Xu Y, Li M, et al. Preoperative refraction, age and optical zone as predictors of optical and visual quality after advanced surface ablation in patients with high myopia: a cross-sectional study. BMJ Open 2018;8:e023877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Marchese A, Carnevali A, Sacconi R, et al. Retinal pigment epithelium humps in high myopia. Am J Ophthalmol 2017;182:56–61. [DOI] [PubMed] [Google Scholar]
- [22].Kobashi H, Kamiya K, Igarashi A, et al. Two-years results of small-incision lenticule extraction and wavefront-guided laser in situ keratomileusis for Myopia. Acta Ophthalmol 2018;96:e119–26. [DOI] [PubMed] [Google Scholar]
- [23].Tan Z, Min J, Xue H, et al. Parenting practices and overweight status of junior high school students in China: A nationally representative study of 19,487 students from 112 schools. Prev Med 2018;107:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Saxena R, Vashist P, Tandon R, et al. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). PLoS One 2017;12:e0189774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Shi Z, Taylor AW, Gill TK, et al. Short sleep duration and obesity among Australian children. BMC Public Health 2010;10:609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Screening for overweight and obesity among school-age children and adolescents. 2018. [Google Scholar]
- [27].Zeger SL, Liang KY, Albert PS. Models for longitudinal data: a generalized estimating equation approach. Biometrics 1988;44:1049–60. [PubMed] [Google Scholar]
- [28].French AN, Morgan IG, Mitchell P, et al. Risk factors for incident myopia in Australian schoolchildren: the Sydney adolescent vascular and eye study. Ophthalmology 2013;120:2100–8. [DOI] [PubMed] [Google Scholar]
- [29].Wu PC, Chen CT, Lin KK, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology 2018;125:1239–50. [DOI] [PubMed] [Google Scholar]
- [30].Guggenheim JA, Northstone K, McMahon G, et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest Ophthalmol Vis Sci 2012;53:2856–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Rose KA, Morgan IG, Smith W, et al. Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch Ophthalmol 2008;126:527–30. [DOI] [PubMed] [Google Scholar]
- [32].Wang Y, Ding H, Stell WK, et al. Exposure to sunlight reduces the risk of myopia in rhesus monkeys. PLoS One 2015;10:e0127863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Smith EL, 3rd, Hung LF, Huang J. Protective effects of high ambient lighting on the development of form-deprivation myopia in rhesus monkeys. Invest Ophthalmol Vis Sci 2012;53:421–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Cui D, Trier K, Munk Ribel-Madsen S. Effect of day length on eye growth, myopia progression, and change of corneal power in myopic children. Ophthalmology 2013;120:1074–9. [DOI] [PubMed] [Google Scholar]
- [35].McCarthy CS, Megaw P, Devadas M, et al. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Exp Eye Res 2007;84:100–7. [DOI] [PubMed] [Google Scholar]
- [36].Ashby R, Ohlendorf A, Schaeffel F. The effect of ambient illuminance on the development of deprivation myopia in chicks. Invest Ophthalmol Vis Sci 2009;50:5348–54. [DOI] [PubMed] [Google Scholar]
- [37].Read SA, Collins MJ, Vincent SJ. Light exposure and eye growth in childhood. Invest Ophthalmol Vis Sci 2015;56:6779–87. [DOI] [PubMed] [Google Scholar]
- [38].Wu PC, Tsai CL, Wu HL, et al. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology 2013;120:1080–5. [DOI] [PubMed] [Google Scholar]
- [39].Gong JF, Xie HL, Mao XJ, et al. Relevant factors of estrogen changes of myopia in adolescent females. Chin Med J (Engl) 2015;128:659–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Vitale S, Sperduto RD, Ferris FL., 3rd Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol 2009;127:1632–9. [DOI] [PubMed] [Google Scholar]
- [41].Zhou WJ, Zhang YY, Li H, et al. Five-year progression of refractive errors and incidence of myopia in school-aged children in Western China. J Epidemiol 2016;26:386–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Suzuki T, Richards SM, Liu S, et al. Influence of sex on gene expression in human corneal epithelial cells. Mol Vis 2009;15:2554–69. [PMC free article] [PubMed] [Google Scholar]
- [43].Kuai Y. The relationship of corneal thickness and diopter in patients with ophthalmobrachytes. presented at: Public Med Forum Mag; 2006. [access date May 27, 2020]. [Google Scholar]
- [44].Lam DS, Leung KS, Mohamed S, et al. Regional variations in the relationship between macular thickness measurements and myopia. Invest Ophthalmol Vis Sci 2007;48:376–82. [DOI] [PubMed] [Google Scholar]
- [45].Wang AL. Eye protection during the women's special period. PLA Health (in Chinese) 2005;1:19. [Google Scholar]
- [46].Song NQ, Yang X. Quantitative analysis of overburdened schoolwork for primary and middle school students. Educ Res 2014;25–30. [Google Scholar]