

Abstract
Context
Sport specialization may contribute to sport injury and menstrual dysfunction in female high school distance runners. Despite the recent growth in sport specialization, including among high school–aged runners, the association of sport specialization with bone mineral density (BMD) remains poorly described.
Objective
To evaluate whether sport specialization was associated with BMD in female high school distance runners.
Design
Cross-sectional study.
Setting
Six high schools.
Patients or Other Participants
Sixty-four female runners (age = 15.6 ± 1.4 years) who competed in cross-country or track distance events and were not currently on birth control medication.
Main Outcome Measure(s)
Each runner completed a survey on menstrual history and sport participation. Height and weight were measured, and dual-energy x-ray absorptiometry was used to measure whole-body, spine, and hip BMD. Each runner was assigned a sport specialization status: low (participation in ≥1 nonrunning sport and distance-running sport(s) for ≤8 mo/y); moderate (participation in both distance-running sport(s) ≥9 mo/y and ≥1 nonrunning sport(s) or limited to distance-running sport(s) for ≤8 mo/y); or high (participation only in distance-running sport(s) for ≥9 mo/y). Multivariable logistic regression was performed to determine the adjusted odds ratio and 95% confidence interval for sport specialization to BMD values, adjusting for body mass index and gynecological age.
Results
Overall, 21.9%, 37.5%, and 40.6% of participants were high, moderate, or low sport specializers, respectively. Low BMD (spine or whole-body BMD z score < −1.0 [standardized by age and sex normative values]) was present in 23 (35.9%) runners. Compared with low sport specializers, high sport specializers were 5 times more likely (adjusted odds ratio = 5.42, 95% confidence interval = 1.3, 23.3; P = .02) to have low BMD.
Conclusions
A high level of sport specialization in high school female distance runners may be associated with a heightened risk for low BMD. Further investigation of this association is warranted due to the health concerns about low BMD in adolescent female runners.
Keywords: athletes, adolescent runners, menstrual dysfunction
Key Points
In this sample of high school female distance runners, a high level of sport specialization was associated with low bone mineral density.
The association between menstrual dysfunction and low bone mineral density was greatest among high sport specializers.
Encouraging diversity in sport activities outside of distance running, screening for and addressing menstrual dysfunction, and promoting strategies to optimize nutrition may be important for promoting bone health in adolescent female distance runners.
More than 3.4 million female athletes participated in interscholastic sports in the United States during the 2018–2019 school year. Of these, 707 600 competed in outdoor track and field (488 627 participants) and cross-country (269 295 participants), ranking them the first- and sixth-most popular sports, respectively, by participation levels.1
Although many health benefits are associated with sport participation, a subset of athletes may experience overuse injuries and adverse conditions, including impaired skeletal health. Researchers2–4 in several prospective studies have identified a high (ie, 34.0% to 52.0%) cumulative seasonal incidence of musculoskeletal injury in girls' interscholastic track and field athletes and cross-country runners.
Stress fractures represent particularly concerning overuse injuries to the bone from cyclic overload. Across all high school sports, girls' cross-country runners have the highest rate of stress fracture by athlete-exposures.5 Impaired bone health and associated behaviors related to sport have been suggested to contribute to this type of injury.6,7
Skeletal health is commonly assessed using measures of bone mineral density (BMD). Low BMD (defined as a BMD or bone mineral content z score < −1.0 in an athlete pursuing a weight-bearing sport)8 has been observed in subsets of youth runners, and the authors9,10 of several prospective studies have found associations among low BMD, stress fracture, and other musculoskeletal injuries among runners. One report11 on 89 high school female distance runners indicated that nearly one-third had a BMD z score < −1.0. Moreover, the runners with low BMD were almost 5 times more likely to incur a musculoskeletal injury than runners with normal BMD values.11 Investigators7 who studied 136 high school–aged runners (94 females) identified a body mass index (BMI) ≤17.5 kg/m2 or a combination of prior fracture and menstrual irregularities as risk factors for impaired BMD. Several factors have been suggested to contribute to low BMD among female runners, including menstrual dysfunction, low energy availability (EA), and low BMI.7,8,12
Sport specialization has been commonly defined as year-round intensive training in a single sport to the exclusion of other sports13 that can result in psychological stress and overuse injuries.13–15 Jayanthi et al13 proposed a classification for a continuum of sport specialization (low, medium, high) based on the following 3 criteria: (1) year-round training (training >8 mo/y), (2) the athlete chooses a single main sport, and (3) the athlete quits all other sports to focus on 1 sport. Sport specialization in distance running may be a risk factor for low BMD in that endurance athletes are likely to have low EA as related to the female athlete triad (Triad).10,11,16,17 The Triad is defined as the interrelationship of low EA, menstrual dysfunction, and low BMD.8,12 The underlying cause of the Triad is low EA.8,12 Low EA (which may occur with or without an eating disorder or disordered eating) and menstrual dysfunction have both been associated with low BMD.17–20 Additionally, overtraining has been considered a risk factor for menstrual dysfunction and hypothesized to be associated with a state of prolonged low EA.21 As year-round participation in endurance running would be classified as high sport specialization and potentially contribute to prolonged time in a low EA state and overtraining, high sport specialization could contribute to low BMD.
Authors of collective studies suggested that high school running may influence bone health and the risk for injury. Female athletes who participate in endurance sports are considered at elevated risk for low EA22 and low BMD.18 Therefore, female high school distance runners appear to be an important athletic population for examining the association between sport specialization and low BMD. Concern about sport specialization in this population is heightened by findings23 that female high school distance runners (ie, athletes whose main running event was 1600 m or longer) who were classified as high sport specializers were at a nearly 2-fold increased risk for musculoskeletal injury and 4-fold increased risk for menstrual dysfunction in the past year than distance runners who were classified as low sport specializers. To date, no researchers have reported on the association between sport specialization in high school–aged distance runners and low BMD.
Therefore, the purpose of our study was to examine the association between sport specialization and low BMD in high school female distance runners. We hypothesized that distance runners with a high level of sport specialization would have a higher likelihood of low BMD than distance runners who met the criteria for low sport specialization. We also hypothesized that an association between menstrual dysfunction and low BMD would be more strongly associated among distance runners classified as high sport specializers than among those classified as low sport specializers.
METHODS
The population consisted of female cross-country and track and field distance runners from 6 high schools in southern California who participated during the 2003–2004 interscholastic seasons and were from a larger study population described previously.11,24,25 Participants were aged 13 to 18 years,11,24,25 had reached menarche, and were not on medication, including hormonal contraceptives, that might influence menstrual status. A total of 64 athletes met the inclusion criteria and competed for their high school in cross-country (typically 5000 m), outdoor track distance (main running event[s] 1600 m or longer), or both sports. All 64 runners underwent a dual-energy x-ray absoptiometry (DXA) scan (Figure 1).18,23 These runners were from a larger sample of 170 athletes who participated in 8 interscholastic sports11,24,25 and completed questionnaires regarding competitive sport involvement and menstrual history. High school athletic directors and coaches in several local high school districts were contacted for approval to allow the research team to approach their runners regarding participation in the study's measures at the beginning of and throughout their interscholastic season. The research team administered the questionnaires to the runners in a room provided by the high school. Coaches were not present in the room during that time. To provide the runners confidentiality when supplying their information, the questionnaire used a numeric code identifier instead of the individual's name, and the runners were seated apart from each other so that they could not see each other's responses. One research assistant for every 6 to 8 athletes was available in the room to provide clarification as each athlete completed the questionnaire.11,24,25 All participants were measured, without shoes, for height and weight, using a digital scale (Health-O-Meter; Sunbeam Products Inc, Bridgeview, IL). The questionnaire was collected at the time of the height and weight measurement. Additionally, each athlete had her BMD evaluated. The study was approved by the San Diego State University Institutional Review Board. Written parental consent and athlete assent were obtained for those under age 18 before the athletes' participation. Athletes aged 18 and older provided written consent.
Figure 1.

Flow diagram for participant selection. Abbreviation: DXA, dual-energy x-ray absorptiometry.
Data Collection
Bone Mineral Density
Areal bone mineral density (BMD; g.cm−2) at the spine (L1–L4), total hip, femoral neck, and whole body were assessed by DXA using a Lunar DPX-NT densitometer (GE Healthcare Lunar, Madison, WI).20,24 Quality assurance (QA) tests were performed each morning of testing. The coefficient of variation in BMD in the study laboratory (30 participants measured twice) was 0.6% for the total hip, 1.2% for the spine (L1–L4), and 0.99% for the whole body, indicating excellent precision.20,24
Runners were categorized as having low BMD for their age if their BMD z score was <−1.0 at the spine or whole-body normalized to age-matched, sex-specific reference data from the GE/Lunar pediatric database.11
Sport Specialization
Each participant completed a questionnaire that included questions about competitive sports participation. Items addressed included (1) current participation in sport(s) and (2) prior participation in sports, including the total duration for each sport (years and months). If the athlete competed in track and field, she was asked to report the number of years and months she competed in distance, sprint, or field events.23 An athlete was classified as a distance runner if she competed in cross-country, outdoor track and field distance events (main running event[s] 1600 m or longer), or both.23
In this study, each distance runner was placed in 1 of 3 sport-specialization classifications23:
Low specialization: defined as participation in distance running (cross-country, track and field, or both) for ≤8 mo/y and participation in 1 or more other high school sport(s), excluding cross-country or track and field;
Moderate specialization: defined as participation in only distance-running sport(s) for ≤8 mo/y or participation in distance running sport(s) ≥9 mo/y and 1 or more other sport(s), excluding cross-country or track and field;
High specialization: defined as participation in distance-running sport(s) for ≥9 mo/y and no reported formal participation in other sports.
Menstrual Status
The preparticipation medical history form included questions regarding menstrual history.24 Menstrual dysfunction was defined as meeting 1 or more of the following criteria11,24,25: primary amenorrhea (age of menarche = 15 years of age or older), oligomenorrhea (<10 menstrual cycles per year at intervals >35 days over the past year), or secondary amenorrhea (≥3 consecutive months of missed menstrual cycles over the past year).8,12 Each runner was asked to report the use of medications, including oral contraceptive pills, that could affect menstrual function. Runners on medications known to affect menstrual function were excluded, as their menstrual function could not be accurately assessed. Gynecological age was defined as the difference between the runner's current age and her age of menarche.
Statistical Analysis
We used the χ2 test and analysis of variance to compare demographic characteristics (chronological age, race, grade), physical characteristics (height, weight, BMI), and menstrual history (age of menarche, gynecological age, number of menses in the past year) among sport-specialization groups. Measured height (m) and weight (kg) were used to calculate BMI. Body mass index was categorized using values associated with health outcomes9,10,12,16 including bone stress injury and low BMD: ≤17.5 kg/m2, 17.6 to 18.4 kg/m2, and ≥18.5 kg/m2.
Analysis of covariance with Bonferroni correction was computed to assess mean raw BMD values at the lumbar spine (L1–L4), total hip, femoral neck, and whole body, while adjusting for chronological age, BMI, and gynecological age, by sport-specialization group. Analysis of covariance with Bonferroni correction was also used to compare mean BMD z scores at the spine and total body, adjusting for BMI and gynecological age, by sport-specialization status. We calculated univariate odds ratios (ORs) and 95% confidence intervals (CIs) to determine associations between menstrual dysfunction and low BMD by sport-specialization classification.26 Multivariate logistic regression was performed to develop 2 adjusted models for ORs and 95% CIs addressing the associations between sport specialization and low BMD, adjusting for BMI and gynecological age with or without menstrual dysfunction.26
The analyses were conducted using SPSS (version 25.0; IBM Corp, Armonk, NY) with the α level set a priori at .05.
RESULTS
Characteristics of Distance Runners
Within the population of 64 runners, 14 (21.9%) were classified as high sport specializers and 24 (37.5%) and 26 (40.6%) as moderate and low sport specializers, respectively. By race or ethnicity, the sample was white (48.8%), followed by Hispanic or Latina (31.3%) and Asian or Pacific Islander (10.9%; Table 1). No differences were observed between racial or ethnic distribution and sport-specialization status (P = .33). When we considered the Female Triad Coalition classification for BMI,12 the percentage of low BMI (≤17.5 kg/m2) was not different in the low versus the high and moderate sport specializers (high = 7.1%, moderate = 14.3%, low = 0.0%, respectively, P = .21). No differences were observed for average age at menarche (P = .49) or number of menses in the past year (P = .92) by sport-specialization status.
Table 1.
Selected Demographic and Physical Characteristics by Sport-Specialization Status
| Characteristic |
Sport-Specialization Status |
P Valued |
|||
| Total (N = 64) | Lowa (n = 26) | Moderateb (n = 24) | Highc (n = 14) | ||
| Mean ± SD | |||||
| Age, y | 15.6 ± 1.4 | 15.4 ± 1.4 | 15.9 ± 1.4 | 15.3 ± 1.3 | .25 |
| Height, cm | 164.0 ± 6.0 | 164.2 ± 6.3 | 164.2 ± 5.8 | 163.4 ± 6.2 | .91 |
| Weight, kg | 56.5 ± 5.8 | 57.1 ± 7.0 | 56.4 ± 5.1 | 55.6 ± 4.8 | .74 |
| Age at menarche, y | 12.5 ± 1.1 | 12.5 ± 0.9 | 12.3 ± 1.1 | 12.8 ± 1.5 | .49 |
| Gynecological age, ye | 3.1 ± 1.7 | 2.9 ± 1.5 | 3.6 ± 1.9 | 2.5 ± 1.7 | .12 |
| No. of menses in past year | 10.8 ± 2.3 | 11.0 ± 2.3 | 10.7 ± 2.4 | 10.7 ± 2.5 | .92 |
| Body mass index | 21.0 ± 2.0 | 21.1 ± 1.7 | 21.0 ± 2.1 | 20.9 ± 2.4 | .95 |
| No. (%) |
|||||
| Body mass index category, kg·m−2 | |||||
| ≤17.5 | 3 (4.7) | 0 (0.0) | 2 (8.3) | 1 (7.1) | .21f |
| 17.6–18.4 | 4 (6.2) | 0 (0.0) | 2 (8.3) | 2 (14.3) | |
| ≥18.5 | 57 (89.1) | 26 (100.0) | 20 (83.4) | 11 (78.6) | |
| Race | |||||
| White | 31 (48.4) | 12 (46.2) | 12 (50.0) | 7 (50.0) | .33f |
| Hispanic | 20 (31.3) | 9 (34.6) | 5 (20.8) | 6 (42.9) | |
| African American | 5 (7.8) | 2 (7.7) | 3 (12.5) | 0 (0.0) | |
| Asian | 7 (10.9) | 3 (11.5) | 4 (16.7) | 0 (0.0) | |
| Other | 1 (1.6) | 0 (0.0) | 0 (0.0) | 1 (7.1) | |
| Grade | |||||
| 9 | 20 (31.2) | 11 (42.4) | 6 (25.0) | 3 (21.4) | .27f |
| 10 | 17 (26.6) | 5 (19.2) | 5 (20.8) | 7 (50.0) | |
| 11 | 11 (17.2) | 5 (19.2) | 5 (20.8) | 1 (7.2) | |
| 12 | 16 (25.0) | 5 (19.2) | 8 (33.4) | 3 (21.4) | |
Low: Distance running (cross-country [XC], track and field [TF], both) ≤8 mo/y competitive sport participation or training and 1 or more other sport(s) played.
Moderate: Distance running (XC, TF, both) only ≤8 mo/y competitive sport participation or training or distance running (XC, TF, both) ≥9 mo/y competitive sport participation or training and 1 or more other sport(s) played.
High: Distance running only (XC, TF, both) for ≥9 mo/y competitive sport participation or training.
Analysis of variance.
Gynecological age = chronological age − age of menarche.
χ2 test.
Bone Mineral Density by Sport-Specialization Status
After adjusting for chronological age, gynecological age, and BMI, high sport specializers had a lower average BMD of the lumbar spine than low sport specializers (P = .04, Table 2). High sport specializers also had lower mean BMD values of the total hip, femoral neck, and whole body than low sport specializers, but these were not different (all P values > .05). A trend was present for a lower BMD z score of the lumbar spine among high sport specializers than among low sport specializers after controlling for BMI and gynecological age (P = .06). Twenty-three (35.9%) runners had low BMD (z score < −1.0). High sport specializers had a greater percentage of low BMD (z score < −1.0; 57.1%) than the moderate (41.7%) or low (19.2%) specializers (P = .04; Figure 2).
Table 2.
Bone Mineral Density by Sport-Specialization Status in High School Female Distance Runners
| Characteristic |
Sport-Specialization Status, Mean ± SD |
P Value |
|||
| Total (N = 64) |
Lowa (n = 26) |
Moderateb (n = 24) |
Highc (n = 14) |
||
| Bone mineral density, g/cm2 | |||||
| Spine (L1–L4) | 1.107 ± 0.104 | 1.144 ± 0.106 | 1.086 ± 0.856 | 1.072 ± 0.115 | .04d |
| Total hip | 1.088 ± 0.109 | 1.121 ± 0.916 | 1.061 ± 0.137 | 1.074 ± 0.072 | .19d |
| Femoral neck | 1.108 ± 0.102 | 1.152 ± 0.085e | 1.074 ± 0.113e | 1.100 ± 0.853 | .08d |
| Whole body | 1.133 ± 0.073 | 1.149 ± 0.075 | 1.128 ± 0.075 | 1.114 ± 0.065 | .35d |
| z score | |||||
| Spine | −0.4 ± 1.1 | 0.0 ± 1.0 | −0.7 ± 0.9 | −0.7 ± 1.4 | .06f |
| Whole body | 0.3 ± 0.9 | 0.6 ± 0.9 | 0.2 ± 0.9 | 0.2 ± 0.9 | .32f |
Low: Distance running (cross-country [XC], track and field [TF], both) ≤8 mo/y competitive sport participation or training and 1 or more other sport(s) played.
Moderate: Distance running (XC, TF, both) only ≤8 mo/y competitive sport participation or training or distance running (XC, TF, both) ≥9 mo/y competitive sport participation or training and 1 or more other sport(s) played.
High: Distance running only (XC, TF, both) for ≥9 mo/y competitive sport participation or training.
Analysis of covariance adjusted for chronological age, body mass index, and gynecological age.
P = .03 with Bonferroni correction compared with high sport specialization.
Analysis of covariance adjusted for body mass index and gynecological age.
Figure 2.
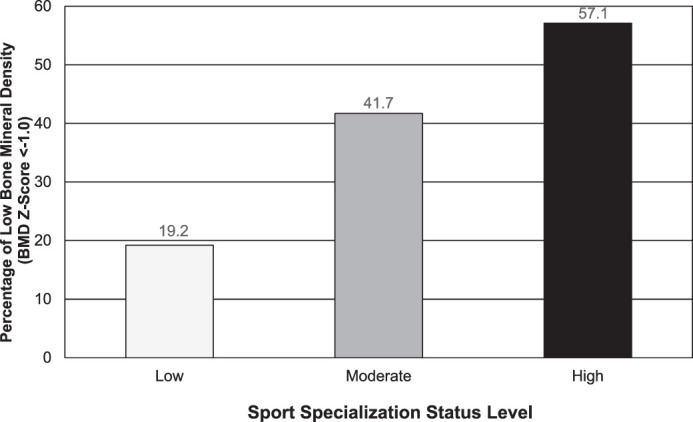
Percentage of low bone mineral density (BMD z score <−1.0) by sport-specialization level among female high school distance runners (low sport specialization = distance running [cross-country (XC), track and field (TF), both] ≤8 mo/y competitive sport participation or training and 1 or more other sport[s] played; moderate sport specialization = distance running [XC, TF, both] only ≤8 mo/y competitive sport participation or training or distance running [XC, TF, both] ≥9 mo/y competitive sport participation or training and 1 or more other sport[s] played; high sport specialization = distance running only [XC, TF, both] for ≥9 mo/y competitive sport participation or training).
Associations Between Menstrual Dysfunction and Low BMD by Sport-Specialization Status
Overall, menstrual dysfunction was strongly associated with low BMD (OR = 3.74; 95% CI = 1.2, 11.9; P = .02, Table 3). Although no statistically significant associations between menstrual dysfunction and low BMD were noted by sport-specialization status, a trend was suggested among the high sport specializers (OR = 6.00; 95% CI = 0.6, 63.8; P = .16).
Table 3.
Associations Between Menstrual Dysfunction (MD) and Low Bone Mineral Density (BMD; Z Score <−1.0) by Sport-Specialization Status
| Menstrual Statusa |
Total |
Sport-Specialization Status |
||||||||||
| Lowb |
Moderatec |
Highd |
||||||||||
| Low BMD |
95% CI |
Low BMD |
95% CI |
Low BMD |
95% CI |
Low BMD |
95% CI |
|||||
| No. (%) |
OR |
No. (%) |
OR |
No. (%) |
OR |
No. (%) |
OR |
|||||
| Eumenorrheic | 47 (27.7) | 1.00 | Referent | 22 (13.6) | 1.00 | Referent | 19 (42.1) | 1.00 | Referent | 6 (33.3) | 1.00 | Referent |
| MD | 17 (58.8) | 3.74e | 1.2, 11.9e | 4 (50.0) | 1.92 | 0.6, 63.6 | 5 (40.0) | 0.92 | 0.1, 6.8 | 8 (75.0) | 6.00 | 0.6, 61.8 |
| P value | 0.02e | 0.16 | 0.67 | 0.16 | ||||||||
Abbreviations: CI, confidence interval; NA, not applicable; OR, odds ratio.
Runners who reported primary amenorrhea, cycles > 35 days apart, or ≥3 consecutive missed menstrual cycles in the past year.
Low: Distance running (cross-country [XC], track and field [TF], both) ≤8 mo/y competitive sport participation or training and 1 or more other sport(s) played.
Moderate: Distance running (XC, TF, both) only ≤8 mo/y competitive sport participation or training or distance running (XC, TF, both) ≥9 mo/y competitive sport participation or training and 1 or more other sport(s) played.
High: Distance running only (XC, TF, both) for ≥9 mo/y competitive sport participation or training.
Boldface indicates statistical significance.
Low BMD by Sport-Specialization Status
In the first multivariate model, after adjusting for gynecological age and BMI, high sport specializers were 5 times more likely (OR = 5.42; 95% CI = 1.3, 23.3; P = .02) to have low BMD than low sport specializers (Table 4). However, in the second multivariate model, after adjusting for gynecological age and BMI and controlling for menstrual dysfunction, high sport specializers trended (P = .09) toward a greater likelihood of low BMD than low sport specializers (OR = 3.77; 95% CI = 0.8, 17.5).
Table 4.
Likelihood of Low Bone Mineral Density (BMD; Z Score <−1.0) by Sport-Specialization Status With and Without Adjustment for Gynecological Age
| Model Sport-Specialization Status |
n |
Low BMD, % |
Odds Ratio |
95% Confidence Interval |
P Value |
| Model 1a | |||||
| Lowb | 26 | 19.2 | 1.00 | Reference | |
| Moderatec | 24 | 41.7 | 3.18 | 0.9, 11.8 | .08 |
| Highd | 14 | 57.1 | 5.42f | 1.3, 23.3f | .02f |
| Model 2e | |||||
| Lowb | 26 | 19.2 | 1.00 | Reference | |
| Moderatec | 24 | 41.7 | 2.95 | 0.8, 11.4 | .12 |
| Highd | 14 | 57.1 | 3.77 | 0.8, 17.5 | .09 |
Abbreviations: n, number at risk for low BMD.
Model 1 adjusted for body mass index and gynecological age.
Low: Distance running (cross-country [XC], track and field [TF], both) ≤8 mo/y competitive sport participation or training and 1 or more other sport(s) played.
Moderate: Distance running (XC, TF, both) only ≤8 mo/y competitive sport participation or training or distance running (XC, TF, both) ≥9 mo/y competitive sport participation or training and 1 or more other sport(s) played.
High: Distance running only (XC, TF, both) for >9 mo/y competitive sport participation or training.
Model 2 adjusted for body mass index, gynecological age, and menstrual status.
Boldface indicates statistical significance.
DISCUSSION
The purpose of our study was to determine whether sport-specialization status was associated with low BMD among high school female distance runners. Using modified criteria for the definition of sport specialization,13 our findings suggested that female distance runners classified as high sport specializers were more likely to have low BMD. Although menstrual dysfunction and low BMD were associated, sport-specialization status trended toward being associated with low BMD, even when we accounted for menstrual dysfunction. These findings indicate that multiple factors associated with sport specialization may contribute to low BMD in female distance runners.
Bone Mineral Density by Sport-Specialization Status
By BMD z scores, more than one-third (35.9%) of the distance runners met the criterion for low BMD (BMD z score < −1.0). Previous reports7,10,11,17 demonstrated that female distance runners may have impaired bone density despite participating in land-based sports. Sport specialization in long-distance running did appear to be associated with low BMD. When we adjusted for gynecological age and BMI, high sport specializers were 5 times more likely to have low BMD, and moderate sport specializers trended toward a 3-fold higher likelihood of low BMD than low sport specializers. When assessed by regional anatomy, high sport specializers had lower mean BMD at the lumbar spine than low sport specializers. Further, although nonstatistically significant trends were observed, high sport specializers had lower mean femoral neck and spine values than low sport specializers. To our knowledge, no prior authors have reported BMD by sport-specialization status at the high school level. Multiple factors may explain these findings, including behaviors associated with long-distance running that place athletes at elevated risk for low BMD (eg, low EA and menstrual dysfunction). Moreover, long-distance running is a less osteogenic sport than ball sports with high impact and multidirectional loading.27
Menstrual Dysfunction and Low BMD by Sport-Specialization Status
Menstrual dysfunction has been associated with low BMD in a variety of high school sports,20,24 including running.7,28 A significant association between menstrual dysfunction and low BMD was present; however, this association was no longer statistically significant when sport-specialization status was taken into account. Investigators of studies in collegiate16,29 and high school sport populations30 identified menstrual dysfunction as more common in endurance sports and sports emphasizing leanness. They postulated that low EA in these sports (eg, cross-country running, long-distance running track events, and swimming) may contribute to menstrual dysfunction.30 Further, among collegiate athletes, both Triad risk factors and the type of impact loading in sport contributed to lower BMD values.31 The small sample size in our study may have led to the findings being underpowered to detect differences. Alternatively, the results may be explained by a complex relationship of multiple interactions of sport exposure with associated behaviors and menstrual dysfunction contributing to low BMD.
Limitations
Despite the novelty of our results, some limitations are notable. The cross-sectional design may have been limited by recall bias. A second limitation may be that the current sport-specialization definition may lack the sensitivity to accurately determine associations with adverse outcomes such as low BMD, menstrual dysfunction, or running-related injury in runners. More specific measures of training volume (ie, running mileage per day or week, hours run per week) were not obtained, and the definition for sport specialization does not account for the intensity of sport participation (intensity of running mileage, overlapping or simultaneous multisport participation) that may contribute to menstrual dysfunction and low BMD.
The study population was relatively small, and that may have limited the statistical comparisons. Participants were from southern California high schools and may not represent runners in other geographic areas of the United States (eg, size of school and team, weather and training ability, nutritional practices). Therefore, additional studies of larger samples in different geographic regions are needed. Also, as the authors32,33 of recent studies suggested, male runners may also be affected by the Triad. Future studies of the relationship between sport specialization and low BMD should include male runners to determine if an association exists as well as to examine sex-specific differences.
Implications
The findings from our study suggest that high sport specialization in long-distance running may be a risk factor for impaired bone health. As researchers9–11 of several prospective studies found relationships between low BMD and stress fractures or other musculoskeletal injuries among adult or adolescent runners, the potential effects of low BMD in this population are concerning. Screening for risk factors of low BMD is important, particularly high sport specialization in long-distance runners. Encouraging diversity of sport activities outside of running, screening for and addressing menstrual dysfunction, and promoting strategies to optimize nutrition may be important during adolescence, a time of peak bone mass accrual.34 Participation in ball sports may promote skeletal health.35 Evidence-based guidelines are needed to guide safe participation among high school runners. Parents, coaches, physicians, and sports health care professionals must work together to ensure the safe participation of adolescent runners, especially given that early sport specialization is increasing in the United States.14
CONCLUSIONS
In this population of 64 high school female distance runners, high sport specialization was associated with an increased likelihood of low BMD. These findings suggest that coaches, school administrators, physicians, and sports medicine providers may need to educate runners and their parents on how specializing only in distance-running sport(s) 9 months or more per year may be detrimental to the athletes' bone health. All high school female distance runners should receive regular management by a physician to evaluate and manage their menstrual health and nutritional counseling to ensure adequate EA. Additionally, incorporating activities known to optimize bone mass (such as jumping or ball sports) throughout the year is highly recommended for youth runners.
ACKNOWLEDGMENTS
This research was supported in part by the National Athletic Trainers' Association Research & Education Foundation (Grant 903GGP005) and the Graduate Division & Research Affairs, San Diego State University. We thank the high school athletic directors, coaches, athletic trainers, and runners for their cooperation and participation in the study.
REFERENCES
- 1.2018–19 High School Athletics Participation Survey. National Federation of State High School Associations Web site. http://www.nfhs.org/media/1020412/2018-19_participation_survey.pdf Accessed October 2019.
- 2.Pierpoint LA, Williams CM, Fields SK, Comstock RD. Epidemiology of injuries in United States high school track and field: 2008–2009 through 2013–2014. Am J Sports Med. 2016;44(6):1463–1468. doi: 10.1177/0363546516629950. [DOI] [PubMed] [Google Scholar]
- 3.Rauh MJ, Margherita AJ, Rice SG, Koepsell TD, Rivara FP. High school cross country running injuries: a longitudinal study. Clin J Sport Med. 2000;10(2):110–116. doi: 10.1097/00042752-200004000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Rauh MJ, Koepsell TD, Rivara FP, Margherita AJ, Rice SG. Epidemiology of musculoskeletal injuries among high school cross-country runners. Am J Epidemiol. 2006;163(2):151–159. doi: 10.1093/aje/kwj022. [DOI] [PubMed] [Google Scholar]
- 5.Changstrom BG, Brou L, Khodaee M, Braund C, Comstock RD. Epidemiology of stress fracture injuries among US high school athletes, 2005–2006 through 2012–2013. Am J Sports Med. 2015;43(1):26–33. doi: 10.1177/0363546514562739. [DOI] [PubMed] [Google Scholar]
- 6.Barrack MT, Rauh MJ, Nichols JF. Prevalence of and traits associated with low BMD among female adolescent runners. Med Sci Sports Exerc. 2008;40(12):2015–2021. doi: 10.1249/MSS.0b013e3181822ea0. [DOI] [PubMed] [Google Scholar]
- 7.Tenforde AS, Fredericson M, Sayres LC, Cutti P, Sainani KL. Identifying sex-specific risk factors for low bone mineral density in adolescent runners. Am J Sports Med. 2015;43(6):1494–1504. doi: 10.1177/0363546515572142. [DOI] [PubMed] [Google Scholar]
- 8.Nattiv A, Loucks AB, Manore MM, et al. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867–1882. doi: 10.1249/mss.0b013e318149f111. [DOI] [PubMed] [Google Scholar]
- 9.Kelsey JL, Bachrach LK, Procter-Gray E, et al. Risk factors for stress fracture among young female cross-country runners. Med Sci Sports Exerc. 2007;39(9):1457–1463. doi: 10.1249/mss.0b013e318074e54b. [DOI] [PubMed] [Google Scholar]
- 10.Barrack MT, Gibbs JC, De Souza MJ, et al. Higher incidence of bone stress injuries with increasing female athlete triad risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med. 2014;42(4):949–958. doi: 10.1177/0363546513520295. [DOI] [PubMed] [Google Scholar]
- 11.Rauh MJ, Barrack M, Nichols JF. Associations between the female athlete triad and injury among high school runners. Int J Sports Phys Ther. 2014;9(7):948–958. [PMC free article] [PubMed] [Google Scholar]
- 12.De Souza MJ, Nattiv A, Joy E, et al. 2014 Female Athlete Triad Coalition consensus statement on treatment and return to play of the female athlete triad: 1st International Conference held in San Francisco, CA, May 2012, and 2nd International Conference held in Indianapolis, IN, May 2013. Clin J Sport Med. 2014;24(2):96–119. doi: 10.1097/JSM.0000000000000085. [DOI] [PubMed] [Google Scholar]
- 13.Jayanthi NA, LaBella CR, Fischer D, Pasulka J, Dugas LR. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med. 2015;43(4):794–801. doi: 10.1177/0363546514567298. [DOI] [PubMed] [Google Scholar]
- 14.Bell DR, Post EG, Trigsted SM, Hetzel S, McGuine TA, Brooks MA. Prevalence of sport specialization in high school athletics: a 1-year observational study. Am J Sports Med. 2016;44(6):1469–1474. doi: 10.1177/0363546516629943. [DOI] [PubMed] [Google Scholar]
- 15.DiFiori JP, Benjamin HJ, Brenner JS, et al. Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Br J Sports Med. 2014;48(4):287–288. doi: 10.1136/bjsports-2013-093299. [DOI] [PubMed] [Google Scholar]
- 16.Tenforde AS, Carlson JL, Chang A, et al. Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Am J Sports Med. 2017;45(2):302–310. doi: 10.1177/0363546516676262. [DOI] [PubMed] [Google Scholar]
- 17.Barrack MT, Rauh MJ, Nichols JF. Cross-sectional evidence of suppressed bone mineral accrual among female adolescent runners. J Bone Miner Res. 2010;25(8):1850–1857. doi: 10.1002/jbmr.63. [DOI] [PubMed] [Google Scholar]
- 18.Barrack MT, Van Loan MD, Rauh MJ, Nichols JF. Physiologic and behavioral indicators of an energy deficiency in female adolescent runners with elevated bone turnover. Am J Clin Nutr. 2010;92(3):652–659. doi: 10.3945/ajcn.2009.28926. [DOI] [PubMed] [Google Scholar]
- 19.Barrack MT, Rauh MJ, Barkai HS, Nichols JF. Dietary restraint and low bone mass in female adolescent endurance runners. Am J Clin Nutr. 2008;87(1):36–43. doi: 10.1093/ajcn/87.1.36. [DOI] [PubMed] [Google Scholar]
- 20.Nichols JF, Rauh MJ, Barrack MT, Barkai HS. Bone mineral density in female high school athletes: interactions and type of mechanical loading. Bone. 2007;41(3):371–377. doi: 10.1016/j.bone.2007.05.003. [DOI] [PubMed] [Google Scholar]
- 21.Dueck CA, Manore MM, Matt KS. Role of energy balance in athletic menstrual dysfunction. Int J Sport Nutr. 1996;6(2):165–190. doi: 10.1123/ijsn.6.2.165. [DOI] [PubMed] [Google Scholar]
- 22.Loucks AB. Low energy availability in the marathon and other endurance sports. Sports Med. 2007;37(4–5):348–352. doi: 10.2165/00007256-200737040-00019. [DOI] [PubMed] [Google Scholar]
- 23.Rauh MJ, Tenforde AS, Barrack MT, Rosenthal MD, Nichols JF. Associations between sport specialization, running-related injury, and menstrual dysfunction among high school distance runners. Athl Train Sports Health Care. 2018;10(6):260–269. doi: 10.3928/19425864-20180918-01. [DOI] [Google Scholar]
- 24.Nichols JF, Rauh MJ, Lawson MJ, Ji M, Barkai HS. Prevalence of the female athlete triad syndrome among high school athletes. Arch Pediatr Adolesc Med. 2006;160(2):137–142. doi: 10.1001/archpedi.160.2.137. [DOI] [PubMed] [Google Scholar]
- 25.Rauh MJ, Nichols JF, Barrack MT. Relationships among injury and disordered eating, menstrual dysfunction, and low bone mineral density in high school athletes: a prospective study. J Athl Train. 2010;45(3):243–252. doi: 10.4085/1062-6050-45.3.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rauh MJ, Macera CA, Marshall SW. Applied sports injury epidemiology. In: Magee DJ, Manske RC, Zachazewski JE, Quillen WS, editors. Athletic and Sports Issues in Musculoskeletal Rehabilitation. St. Louis, MO: Elsevier Saunders;; 2011. pp. 730–772. [Google Scholar]
- 27.Tenforde AS, Fredricson M. Influence of sports participation on bone health: a review of the literature. PM R. 2011;3(9):861–867. doi: 10.1016/j.pmrj.2011.05.019. [DOI] [PubMed] [Google Scholar]
- 28.Gibbs JC, Nattiv A, Barrack MT, et al. Low bone density risk is higher in exercising women with multiple triad risk factors. Med Sci Sports Exerc. 2014;46(1):167–176. doi: 10.1249/MSS.0b013e3182a03b8b. [DOI] [PubMed] [Google Scholar]
- 29.Beals KA, Hill AK. The prevalence of disordered eating, menstrual dysfunction, and low bone mineral density among US collegiate athletes. Int J Sport Nutr Exerc Metab. 2006;16(1):1–23. doi: 10.1123/ijsnem.16.1.1. [DOI] [PubMed] [Google Scholar]
- 30.Nichols JF, Rauh MJ, Barrack MT, Barkai HS, Pernick Y. Disordered eating and menstrual irregularity in high school athletes in lean-build and nonlean-build sports. Int J Sport Nutr Exerc Metab. 2007;17(4):364–377. doi: 10.1123/ijsnem.17.4.364. [DOI] [PubMed] [Google Scholar]
- 31.Tenforde AS, Carlson JL, Sainani KL, et al. Sport and triad risk factors influence bone mineral density in collegiate athletes. Med Sci Sports Exerc. 2018;50(12):2536–2543. doi: 10.1249/MSS.0000000000001711. [DOI] [PubMed] [Google Scholar]
- 32.Tenforde AS, Barrack MT, Nattiv A, Fredericson M. Parallels with the Female Athlete Triad in male athletes. Sports Med. 2016;46(2):171–182. doi: 10.1007/s40279-015-0411-y. [DOI] [PubMed] [Google Scholar]
- 33.Barrack MT, Fredericson M, Tenforde AS, Nattiv A. Evidence of a cumulative effect for risk factors predicting low bone mass among male adolescent athletes. Br J Sports Med. 2017;51(3):200–205. doi: 10.1136/bjsports-2016-096698. [DOI] [PubMed] [Google Scholar]
- 34.Tenforde AS, Nattiv A, Ackerman K, Barrack MT, Fredericson M. Optimising bone health in the young male athlete. Br J Sports Med. 2017;51(3):148–149. doi: 10.1136/bjsports-2016-097000. [DOI] [PubMed] [Google Scholar]
- 35.Tenforde AS, Sainani KL, Carter Sayres L, Milgrom C, Fredericson M. Participation in ball sports may represent a prehabilitation strategy to prevent future stress fractures and promote bone health in young athletes. PM R. 2015;7(2):222–225. doi: 10.1016/j.pmrj.2014.09.017. [DOI] [PubMed] [Google Scholar]