

Abstract
School classrooms are noisy and reverberant environments, and the poor acoustics can be a barrier to successful learning in children, particularly those with multiple disabilities, auditory processing issues, and hearing loss. A new set of listening challenges have been imposed by the recent global pandemic and subsequent online learning requirements. The goal of this article is to review the impact of poor acoustics on the performance of children with auditory processing issues, mild hearing loss, and unilateral hearing loss. In addition, we will summarize the evidence in support of remote microphone technology by these populations.
Keywords: remote microphone, autism, auditory processing
Successful learning in school classrooms is highly dependent on the acoustical environment in which the learning occurs. However, an unoccupied classroom often has noise and reverberation levels exceeding the American National Standards Institute–recommended levels of 35 dBA and 0.6 to 0.7 seconds, respectively. 1 2 3 In occupied classrooms, noise levels can range from 60 to 80 dBA, while a teacher's voice may only be 65 dBA at a distance of 2 m. 4 5 Other children's voices can be even less intense than the teacher's voice during class discussions depending on the talker's physical distance to a listener. As a result, signal-to-noise ratios (SNRs) at the young learner's ears are often poor and will fluctuate based on the location of the primary talker relative to the child.
The recent global pandemic required students in the United States to engage in new and often uncharted online learning platforms with synchronous online teaching, asynchronous online lectures, external videos, and independent assignments. In addition to learning this new technology, this type of learning poses several additional educational challenges. First, parents, many of who have limited knowledge of teaching and have jobs, have become teachers for younger children or those who need one-on-one support. Second, students no longer engage with their teachers or peers to ask clarifying questions about assignments and tests. Third, children with hearing loss and auditory processing issues have unique listening needs. Similar to school, the home environment is a noisy place with appliances, multiple family members, and constant distraction. In addition, synchronous online learning may be difficult for children with hearing loss and auditory processing issues due to the reduced visual cues, inconsistent internet access and audio signals, and necessity to focus for extended periods of time, all of which add to listening fatigue experienced by these students. Closed captioning and other school-provided assistive technology may not be provided to support online learning.
The high levels of noise and reverberation present in classrooms and in some home environments are known to result in greater speech recognition deficits in children relative to adults, despite the presence of normal pure-tone hearing sensitivity. Neuman et al 6 reported that, on average, children with normal-hearing sensitivity, aged 6 to 11 years, require SNRs of +15 dB or greater to obtain 95% correct speech recognition with a reverberation time of 0.8 seconds, while young adults required only a +9 dB SNR. Furthermore, when comparing speech recognition (i.e., repeating what is heard) to comprehension (i.e., answering questions about a short passage) in the presence of background noise, large performance differences exist across measures. Specifically, Valente et al 7 reported that 8-year-olds scored an average of 97% correct on sentence recognition at a +7 dB SNR and 0.6-second reverberation time, but average comprehension scores were only 42% in the same listening condition. Comprehension is a higher-order auditory skill requiring greater cognitive resources and, therefore, is more susceptible to interference in the typical classroom environment due to the poor acoustic conditions. 7 Consequently, use of speech-recognition alone to evaluate impact of the acoustic environment may underestimate potential for poor educational outcomes due to impaired speech comprehension.
Typical classrooms have a variety of learners and do not consist solely of children with normal hearing. Classes often include children who have normal-hearing sensitivity with multiple disabilities, auditory processing issues, and hearing loss. The goal of this article is to review the impact of poor acoustics on the performance of children with auditory processing issues, mild hearing loss, and unilateral hearing loss. In addition, we will summarize the evidence in support of remote microphone technology (RMT) by these populations.
Populations with Normal Hearing and Auditory Processing Issues
Children who are diagnosed with auditory processing disorder (APD), autism spectrum disorder (ASD), attention-deficit hyperactivity disorder (ADHD), Friedreich's ataxia (FRDA), and dyslexia often have normal-hearing sensitivity but experience deficits in auditory processing and speech recognition relative to neurotypical peers. These auditory processing issues are often associated with poorer speech recognition in background noise, educational issues, and a host of other related challenges.
Speech Recognition and Processing Issues
The prevalence of APD is estimated to be two to three percent of children in the general population. 8 Children who are diagnosed with APD may exhibit auditory difficulties across many domains including temporal processing (i.e., timing aspects of stimuli), dichotic processing (i.e., binaural integration of speech between the ears), speech recognition in background noise, and observed listening behaviors. 8 9 In one study, children with APD had 10 to 20% worse average speech recognition scores in noise (0 and +3 dB SNR) compared with peers. 10 In addition to speech recognition deficits, Johnston and colleagues 9 reported that, on average, children with APD have significantly greater academic and listening difficulties and lower psychosocial function (e.g., external locus of control, difficulties with interpersonal relationships, anxiety, depression, and attention problems) than peers.
Children with ADHD and ASD show similar issues in auditory processing, cognitive skills, and executive function despite the different etiologies of the disorders. 11 12 13 14 15 16 17 18 19 For example, children with ASD, ADHD, or both, on average, have significantly poorer speech-in-noise thresholds by 2 to 5 dB relative to peers, and high-functioning children with ASD/ADHD also experience listening difficulties as determined via questionnaires. 12 15 16 20 Other studies report significant differences between children with ASD/ADHD and their typically-functioning peers on questionnaires or tests of percent-correct speech recognition; temporal processing of amplitude variations; and auditory attention, filtering, and sensitivity. 13 14 15 18 21 In particular, parents of children with ASD report their children have difficulty attending to auditory information, are distractible or cannot function in noise, and are unresponsive to auditory stimuli. 18 Auditory filtering, or the ability to hear speech stimuli and complete tasks in noise, is of particular importance to children with ASD because it is a significant predictor of higher academic performance and reduced attention deficits. 22
Children with FRDA represent another small population of school-aged children with auditory processing and speech-in-noise issues. FRDA is a neurodegenerative disease that may cause auditory neuropathy and steady decline across multiple sensory systems. Multiple studies show children with FRDA have abnormal temporal and spatial processing and poor speech recognition, particularly in background noise. 23 24 For instance, Rance et al 24 reported that children with FRDA exhibit significantly poorer average phoneme recognition scores in noise (22% at 0 dB SNR) relative to a control group (56%). The children with FRDA confirmed their difficulties communicating and listening in noise on a self-report questionnaire where their ratings were significantly poorer than a control group.
Finally, in several studies, temporal processing and speech recognition in noise are poorer in children diagnosed with dyslexia or learning disabilities. 25 26 27 28 29 Ziegler and colleagues 29 reported that children with dyslexia showed significantly poorer (9% lower) average perception of vowel–consonant–vowel stimuli in noise relative to peers of the same age, and many other studies show similar or even greater deficits.
To summarize, many school-aged children with disabilities will have normal pure-tone hearing sensitivity but substantial auditory-processing issues that impact speech recognition and performance in school. The majority of studies discussed in this section were conducted in laboratory environments. As a result, performance in a real classroom will likely be even worse given the fluctuating levels of noise and reverberation and additional sensory distractions. Also, many of these children have multiple disabilities in addition to those discussed earlier, such as language disorder, anxiety, gastrointestinal issues, or sleep disorders that will contribute to their academic challenges. It will be important to consider the listening and auditory processing needs of each individual child with one or more disabilities to ensure that he or she is receiving an education in the least restrictive environment as outlined by the Individuals with Disabilities Education Act. 30
Remote Microphone Technology in Children with Normal-Hearing Sensitivity
RMT is one potential option to address the difficult acoustic classroom environments faced by young learners. Currently, the most common RMT options for normal-hearing populations are stand-alone digital modulation (DM) or frequency modulation (FM) systems manufactured by Phonak or Oticon ( Table 1 ; Figs. 1 and 2 ). These systems consist of a transmitter, transmitter microphone, and receivers with no built-in microphone coupled to small, unoccluding domes. These devices provide minimal amplification of sound from the transmitter, but they improve the SNR at the listener's ears. Tables 2 and 3 summarize published evidence to support the use of FM and DM technology for improving speech recognition, observed and perceived listening abilities, and other auditory behaviors in children who have APD, ASD, ADHD, language disorder, FRDA, and dyslexia. 9 15 16 17 19 20 24 31 32 33 34 35 36 37 38 Although we recommend use of a receiver on each ear to provide a balanced sound and optimal SNR, to date, there are no published studies that explore performance differences with one versus two receivers for these populations.
Table 1. Remote Microphone Technology Options for Children with Normal-Hearing Sensitivity, Mild Hearing Loss, and Unilateral Hearing Loss.
| Personal RM Systems Transmitter & Receiver | Design Integrated | • FM/DM receiver connects to dedicated device • Pros: Good connection; small • Cons: Works with only one specific HA; expensive for schools if student moves out of area |
| Universal | • FM/DM receiver for HA device with a device-specific adaptor (e.g., audio shoe) • Pros: Small; works with all devices • Cons: Adaptor susceptible to malfunction/ connection issues |
|
| Stand-Alone for Normal-Hearing Sensitivity (Transparent) | • FM/DM limited-gain receiver designed for normal pure-tone thresholds, but processing problems • Pros: Small; improves speech recognition in multiple populations; non-occluding • Cons: Children with tactile issues may not tolerate |
|
| Electromagnetic/Near Field Magnetic Imaging | • FM/DM/Infrared; requires neckloop & special receiver or ID with receiver • Pros: One receiver/ID sends to both HAs or earphones/buds; less expensive • Cons: May not have advanced signal processing; personal device must have telecoil or NFMI capability |
|
| Personal RM Accessory | Accessory Microphone | • DM; manufacturer-specific microphone; may be used with ID • Pros: No receiver if it's built into the HA (e.g., 2.4-GHz radio antenna); less expensive than RM systems • Cons: May use with only one manufacturer's HAs; may not contain advanced signal processing |
| Soundfield Systems | Desktop | • FM, Small speaker placed on child's desk • Pros: No equipment for child; less expensive than RM systems • Cons: Minimal gain, portability limited for young children; does not address classroom reverberation |
| Single-Speaker Classroom | • FM/DM, single loudspeaker placed in corner of room • Pros: No equipment for child; some improvement to SNR; less expensive than RM systems • Cons: Less gain than desktop; sound may not be equally distributed across room; does not address classroom reverberation; limited portability |
|
| Multiple-Speaker Classroom | • FM/DM, multiple loudspeakers placed around room • Pros: No equipment for child; some improvement to SNR; less expensive than RM systems • Cons: Less gain than desktop; unequal distribution of sound if installed incorrectly; does not address classroom reverberation; limited portability |
Abbreviations: DM = digital modulation transmission; HA = hearing aid; FM = frequency modulation transmission; ID = intermediary device; NFMI = near field magnetic induction; RM = remote microphone; SNR = signal-to-noise radio.
Figure 1.
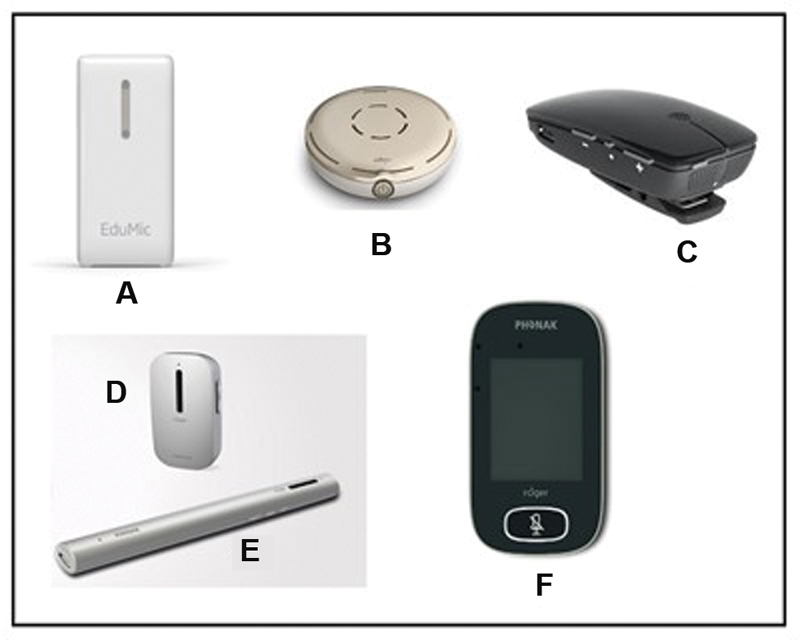
Examples of remote microphone digital transmitters or remote microphone accessories: ( A ) Oticon EduMic; ( B ) Phonak Roger Select; ( C ) ReSound Multi Mic; ( D ) Phonak Roger Clip-On Mic; ( E ) Phonak Roger Pen; ( f ) Phonak Roger Touchscreen Mic.
Figure 2.
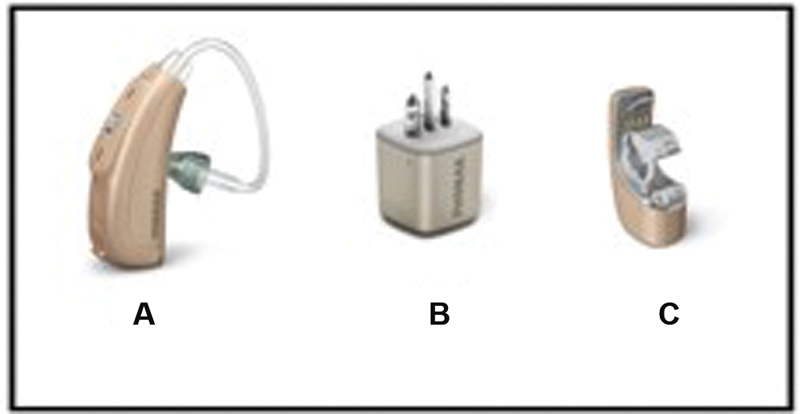
Examples of remote technology receivers that may be used by children with normal hearing, unilateral hearing loss, or mild hearing loss: ( A ) Phonak Roger Focus for children with normal-hearing sensitivity; ( B ) Phonak Roger X universal receiver for use with most hearing aids; ( C ) Phonak Roger design-integrated receiver for a specific device.
Table 2. Benefits of Remote-Microphone Technology in Children with ASD and ADHD.
| Disorder: Participants | Authors, year | Test measures: results |
|---|---|---|
| ASD: 10 ASD 10 controls |
Rance et al, 2014 15 |
•
Word recognition in noise
: significant 17 and 10% improvements with FM in ASD and control groups, respectively
• Questionnaires : better ratings with FM on child APHAB and teacher LIFE |
| ASD: 26 ASD |
Rance et al, 2017 31 |
•
Word recognition in noise
: significant 21% improvement with RM; performed at expected level for age with RM
• Questionnaires : perceived benefit with RM • Salivary cortisol concentration : decrease in stress levels when using RM |
| ASD: 12 ASD |
Schafer et al, 2016 20 |
•
Speech recognition in noise
: significant 4.6 dB improvements in 8 of the 12 children with RM
• Questionnaires : teachers, participants, and parents reported reduced listening difficulty with RM • Auditory working memory and comprehension : 12–13 point improvement in 7 of the 12 children with RM • ANL : accepted 8.6 dB more noise with RM |
| ASD: 15 ASD |
Schafer et al, 2019 32 |
•
Speech recognition in noise
: significant 36.3% improvement with RM
• Auditory processing test battery : 6 of the 9 subtests improved after RM use and training • ANL : significantly improved with RM • Spatial processing : significantly improved LiSN-S high-cue threshold in noise after RM use and training • Dichotic testing : significantly improved after RM use and training • Questionnaire : significantly improved LIFE-R after RM use and training |
| ASD: 22 ASD |
Schafer et al, 2019 33 |
•
Speech recognition in noise
: improved by 29% with RM
• Educational need : BKB-SIN, LIFE, sensory profile, and difficulty checklist used to document need. All showed need on 1–2 measures |
| ASD, ADHD: 7 ASD/ADHD 11 controls |
Schafer et al, 2013 16 |
•
Sentence recognition in noise
: significant 6 dB improvement with FM significantly worse than controls without FM; similar performance with FM
• Examiner-observed classroom behavior : improved on-task behaviors • Teacher CHAPS : improvement with FM |
| ASD, ADHD, LD, or SLI: 12 subjects |
Schafer et al, 2014 17 |
•
Sentence recognition in noise
: significant 65–86% improvement with RM
• Listening comprehension in noise : improved significantly with FM • Questionnaire : improved with FM–LIFE-R, CHILD, and parent CHILD |
| ADHD/ADD: 31 subjects |
Updike, 2006 19 |
•
Word recognition in noise
: significant 34% improvement with FM
• Teacher questionnaires : improvements in attention and listening skills |
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ANL, acceptable noise level; APHAB, abbreviated profile of hearing aid benefit; ASD, autism spectrum disorder; BKB-SIN, Bamford–Kowal–Bench speech-in-noise test; CHAPS, Children's Auditory Performance Scale; CHILD, Children's Home Inventory for Listening Difficulties; FM, frequency modulation system; LIFE-R, Listening Inventory for Education – Revised; LiSN-S, Listening in Spatialized Noise – Sentences Test; LD, language disorders; RM, remote microphone; SLI, specific language impairment.
Table 3. Evidence Regarding Benefit of Remote-Microphone Technology in Children with Normal Hearing and Auditory Processing Disorder, Friedreich's Ataxia, and Dyslexia.
| Disorder: Participants | Author, year | Test measures: results |
|---|---|---|
| APD: 10 APD 13 controls |
Johnston et al, 2009 9 |
•
Sentence recognition in noise
: improved 10 dB with FM
• Parent SIFTER : worse academic ratings for APD group • Participant LIFE : improved after FM use • Psychosocial function BASC-2 : improved ratings for locus of control, anxiety, depression |
| APD: 28 subjects |
Smart et al, 2018 34 |
•
Speech in spatial noise
: improved 13% with FM
• Cortical auditory evoked potentials : use of FM reduced the impact of noise on P1 and N2 latencies and amplitude • Questionnaires : significantly better teachers and participant ratings with FM on LIFE |
| APD: 55 subjects 5 groups |
Sharma et al, 2012 35 |
•
Frequency pattern test
: improved in language and discrimination groups
• CELF-4 : improved core language scores for discrimination and discrimination + FM groups |
| Friedreich's ataxia: 10 subjects |
Rance et al, 2010 36 |
•
Word recognition in noise
: improved 27% with FM
• Child APHAB : less difficulty in noise and reverberation |
| Friedreich's ataxia: 19 ataxic 20 controls |
Rance et al, 2012 24 | • Speech perception : scores increased in ataxic participants with FM to the level of controls |
| Dyslexia: 38 subjects 19 used FM 19 dyslexia controls |
Hornickel et al, 2012 37 |
•
Phonological processing and reading
: improved after FM for 1 year for dyslexia group
• Speech ABR : improved neural consistency in FM group; greatest improvement in children who had improved phonological awareness |
| Reading delay: 23 with FM 23 controls |
Purdy et al, 2009 38 |
•
Teacher LIFE
: significantly improved classroom listening for FM group; no change for control group
• Participant LIFE : significantly improved classroom listening for difficult situations for FM group; no change for control group |
Abbreviations: APD, auditory processing disorder; APHAB, abbreviated profile of hearing aid benefit; BASC-2, Behavior Assessment System for Children, 2nd edition; CELF-4, Clinical Evaluation of Language Fundamentals; CHAPS, Children's Auditory Performance Scale; FM, frequency modulation system; LIFE, Listening Inventory for Education; SIFTER, Screening Instrument for Targeting Educational Risk.
In the majority of studies cited earlier, children used ear-level, wireless RMT with the exception of the Updike study where body-worn RMTs were used. 19 Across these studies, consistent increases in speech recognition in noise with RMT use were observed compared with results without the technology. Average increases in percent correct speech recognition ranged from 17 to 86%; average improvements in speech-in-noise thresholds ranged from 6 to 10 dB. Other measures employed in these studies included parent, child, and teacher questionnaires; tests of psychosocial function; listening comprehension in noise; phonological processing; observed classroom behavior; and electrophysiological measures. In the studies that included questionnaires, significant average improvements in classroom and home listening behaviors were reported by children, parents, or teachers. Notably, these measured and observed improvements were also supported by objective changes in electrophysiological responses to speech sounds in two separate populations, children with ASD and dyslexia. 37 39
Similar to children who use hearing aids, RMT for children with normal hearing should be fit and verified by a licensed audiologist. Suggested fitting, verification, and validation procedures of RMT in normal hearing populations are outlined in two previous studies. 33 40 In the most updated fitting recommendations, Schafer et al 33 described the need for real ear measures that account for the child's ear canal volume and hearing thresholds and also how to adjust the receiver volume to meet prescriptive targets. In addition, to validate the fittings, the use of speech recognition in noise testing and specific questionnaires is recommended, similar to the studies described in Tables 2 and 3 .
RMT is expensive, and, most often, funding to purchase RMT for classroom use is obtained in three ways: (1) special education funding with the device listed in the child's individualized education plan (IEP), (2) Section 504 41 funding in a school district, or (3) private pay by the parent. Most of the children discussed in this section will be receiving special education services, making the first option the best choice unless the family wishes to purchase the system. Section 504 is a law that attempts to eliminate educational or work barriers in agencies or activities that receive federal funding that could limit participation of people with disabilities. The evidence regarding auditory difficulties of children with processing problems (Section II) paired with the evidence provided in Table 2 and 3 may be used by audiologists and other related professionals to highlight educational need for RMT in these populations.
Populations with Mild and Unilateral Hearing Loss
Educational and Psychosocial Issues
Poor classroom listening environments affect all young learners, especially those with auditory processing difficulties. For children with hearing loss, the effects of poor acoustics on performance are even greater. 42 A body of research since the mid-20th century has established that children with mild and unilateral hearing loss are at risk for poor psychoeducational outcomes compared with typically-developing peers with normal hearing. 43 Domains where these children may be at risk include interpersonal relationships, academic achievement, reading, language skills, problem behaviors, self-esteem, attention, stress, and listening fatigue. Davis et al 44 found that children with permanent hearing loss and pure-tone averages (PTAs) less than 44 dB HL exhibited delays in vocabulary, difficulties with interpersonal relationships, and an elevated risk of behavioral problems such as aggression and impulsivity. One noteworthy finding of this study was that degree of academic or psychosocial concern for children with hearing loss was poorly predicted by PTA and that children with mild hearing loss faced similar risks of poor outcomes as their peers with moderate and severe hearing loss. Some of these reported difficulties may be attributed to differences in the standard of audiological care for children with mild hearing loss prior to universal newborn hearing screening. In previous decades, children with mild hearing loss were typically identified later and were less likely to wear hearing aids (or be fit bilaterally) as part of routine audiological management. 44 45 Nonetheless, full-time use of amplification remains a challenge in this population, and children with mild hearing loss are at an elevated risk of discontinuing hearing aid use over time relative to peers with more severe hearing loss. 46
Comparable psychoeducational risks associated with unilateral hearing loss have also been reported. 47 48 Children with unilateral hearing loss who generally demonstrated typical spoken language skills and attended mainstream classrooms nevertheless had increased risk of difficulties in educational progress, with 35% having failed at least one grade, a rate more than ten times higher than peers with normal hearing, bilaterally. 48 Previously, it was assumed that children with unilateral loss experienced minimal educational and communication difficulties and that preferential seating—an accommodation that all of the children in the study mentioned earlier received—was adequate to meet their listening needs. 49 The specific listening difficulties of children with unilateral hearing loss are thought to relate to diminished or absent binaural listening benefits such as binaural summation, head shadow, squelch, and localization unmasking when listening to speech in noise. 49 More recent work has confirmed the elevated risk of behavioral and academic concerns persists in children with unilateral hearing losses. 50
The similar risks of poor psychoeducational outcomes in children with mild bilateral losses and children with unilateral hearing loss has led some researchers to group children with these two audiological profiles together. Bess et al 51 reported that children with thresholds between 20 and 40 dB HL—combined with children with unilateral hearing loss under the umbrella term of “minimal hearing loss”—experienced poorer social and/or emotional outcomes than peers with normal hearing, and 37% of children in this group failed at least one grade. Nonetheless, some recent studies have found that psychoeducational outcomes of school-age children with minimal hearing loss were not significantly different, on average, from their typically developing peers with normal hearing with the exception of teacher reports of attention. 52 In this case, the lack of mean group differences in psychoeducational outcomes has the potential to obscure the fact that individual children with mild hearing loss were more likely to score significantly below normative means on standard psychoeducational assessments than their peers with normal hearing. Furthermore, there is a lack of uniformity in what, if any, interventions and support children with mild and unilateral hearing loss receive given that they do not meet eligibility criteria for early intervention in some states, 53 and the developmental risks associated with mild and unilateral hearing loss are not universally understood or effectively communicated. For example, the use of the term “minimal” sensorineural hearing loss likely downplays the difficulties these listeners experience. 54
Issues with Speech Recognition
In spite of some improvements in the early detection and audiological management of mild and unilateral hearing loss, 52 the challenging listening conditions in typical classrooms remain an issue for these children. The poor acoustic conditions in typical classrooms—noise generated from inside the classroom, sound transmission from noise sources outside the classroom, effects of distance from the teacher/talker, and excessive reverberation within the instructional space—have long been suspected to negatively impact the listening environment and auditory learning of children with and without hearing loss. 55 Children with hearing loss in the range of 15 to 30 dB HL experience greater decrements in speech recognition scores with decreases in SNR than peers with normal hearing. 56 Similarly, Bess et al 57 reported greater decrements in speech perception scores with decreases in SNR in children with unilateral hearing loss than peers with normal hearing, particularly when speech was presented from the side of the affected ear.
Remote Microphone Technology in Children with Mild and Unilateral Hearing Loss
In light of the persistent risk of poor psychoeducation outcomes and elevated vulnerability of children with mild and unilateral hearing loss to poor acoustic conditions, the potential benefit from RMT—including RMT with and without the use of hearing aid—has received significant attention over the years. RMT options for children with mild and unilateral hearing loss are similar to those described in the previous section and are summarized in Table 1 and shown in Figs. 1 and 2 .
In the literature, two types of RMT, personal FM and desktop sound field systems, have been reported to promote better speech perception than classroom infrared sound field systems for children who use hearing aids. 58 Children with unilateral hearing loss have consistently been found to have better speech perception in quiet and noise across a range of listening conditions when using a personal FM compared with both contralateral routing of the offside signal (CROS) and standard hearing aids. 59 60 In addition to improved speech perception, even brief periods of FM use in the classroom have been associated with improvement in academic performance of children with minimal hearing loss per teacher's report. 61 A growing body of evidence also supports the use of RMT for families of children with hearing loss to improve access to communication in the home. 62 Though the effectiveness of RMT use in improving SNR is well established, the uptake of FM by students with unilateral loss is by no means universal, with one study finding that only 28% of students had ever used an FM in school, 50 and another that found only 5 out of 27 students with minimal hearing loss used hearing aids and/or FM in school. 52 Some potential challenges to use may include issues with physical comfort of ear-level devices, 61 though social stigma and lack of support from peers and instructors are commonly reported reasons for inconsistent or nonuse by students with hearing loss. 63 Additional research is needed on these populations with newer hearing technology to examine if some of these barriers still exist.
Conclusions and Future Trends in Rmt
Use of RMT holds significant potential benefits for children with normal, pure-tone hearing sensitivity but auditory processing issues, as well as for children with mild or unilateral hearing loss. Numerous studies support improved auditory or behavioral performance on one or more measures including speech recognition in background noise, observed or perceived listening behaviors, listening comprehension, psychosocial function, and phonological processing.
The primary limitations to using RMT are the cost and, at times, the inability to hear others while using the device. Most of the personal RMT used in school cost between $3,000 and $5,000 for two ear-level receivers and one transmitter. To ensure children hear classmates and class discussions, children with normal hearing will require unoccluding receivers (i.e., small domes) that still allow for some level of retention on the ear. For children with hearing loss, the best approach will be to fit a hearing aid and couple a FM/DM receiver directly to the aid to allow the child optimal audibility even when the RMT is not in use. When considering options for RMT use in the home, many manufacturers provide small clip-on microphones that connect directly to hearing aids. These clip-on microphones may be included with the purchase of the aid or available for about half the cost of the more sophisticated ones used in the educational classroom. In particular, these clip-on microphones may be the most feasible and affordable option for enhancing online learning when schools are unable to provide RMT at home.
In the future, lower-cost options may be available, in the form of smartphone applications. Currently, there do not appear to be any remote microphone software applications (apps) available for connectivity with hearing aids that can be downloaded on iPhone or Android smartphones that offer the features of the systems discussed without undesirable delay in the transmitted signal. However, there are two other options for apps when used with headphones rather than streaming to hearing aids with microphones ( Table 4 ). First, Bluetooth headphones or Bluetooth loudspeakers may be paired to smartphone apps (e.g., Microphone Live, Bluetooth Loudspeaker, or Microphone by Wonder Grace). The second and often hard-wired option is to download an amplifier app (e.g., Sound Amplifier, Volume Booster GOODEV, or HearYouNow—Your personal sound amplifier) to amplify sounds while the listener wears earphones or ear buds that are plugged into the smartphone. The authors of this article caution against the use of smartphone apps on an individual trial basis because (1) there is no evidence to support their use with these particular populations and (2) in the latter option, the amplifier will amplify the primary talker's voice as well as any background noise. It is possible that this type of app might be of benefit in a quieter home environment but may not improve the SNR at the listener's ear in a noisy environment and could actually degrade speech recognition performance relative to an unamplified condition. Overall, less expensive RMT options are expected in the future and, with supportive evidence, may be recommended for populations with auditory processing issues, mild hearing loss, and unilateral hearing loss.
Table 4. Summary of Apps that may be Used with Headphones or Loudspeakers.
| Name | Platform | Cost | QR Code | Description |
|---|---|---|---|---|
| Microphone live | iOS | Free |
|
Phone or tablet microphone amplifies speech via Bluetooth headset/loudspeakers, headphones, or ear buds |
| Bluetooth loudspeaker | iOS Android |
Free |

|
Phone or tablet microphone amplifies speech via Bluetooth headset/loudspeakers, headphones, or ear buds |
| Microphone by Wonder Grace | Android | Free |

|
Phone or tablet microphone amplifies speech via Bluetooth headset/loudspeakers, headphones, or ear buds |
| Sound amplifier | Android | Free |

|
Phone or table microphone used to amplify sound to wired headphones |
| Volume booster GOODEV | Android | Free |

|
Phone or tablet microphone amplifies speech via Bluetooth headset/loudspeakers, headphones, or ear buds |
| HearYouNow—Your personal sound amplifier | iOS | Free |
|
Phone can be used as personal sound amplifier with ear buds |
Footnotes
Conflict of Interest The first author has received research grant funding from two hearing device manufacturers, Phonak and Oticon.
References
- 1.American National Standards Institute . Melville, NY: 2010. Acoustical Performance Criteria, Design Requirements, and Guidelines for Schools, Part 1: Permanent Schools (No. ANSI S12.60–2010) [Google Scholar]
- 2.Knecht H A, Nelson P B, Whitelaw G M, Feth L L. Background noise levels and reverberation times in unoccupied classrooms: predictions and measurements. Am J Audiol. 2002;11(02):65–71. doi: 10.1044/1059-0889(2002/009). [DOI] [PubMed] [Google Scholar]
- 3.Nelson E L, Smaldino J, Erle S, Garstecki D.Background noise levels and reverberation times in old and new elementary school classrooms J Educ Audiol 2007/20081416–22. [Google Scholar]
- 4.Cruckley J, Scollie S, Parsa V. An exploration of non- quiet listening at school. J Educ Audiol. 2011;17:23–35. [Google Scholar]
- 5.Olsen W O. Average speech levels and spectra in various speaking/listening conditions: a summary of the Pearson, Bennett, & Fidell (1977) report. Am J Audiol. 1998;7(02):21–25. doi: 10.1044/1059-0889(1998/012). [DOI] [PubMed] [Google Scholar]
- 6.Neuman A C, Wroblewski M, Hajicek J, Rubinstein A. Combined effects of noise and reverberation on speech recognition performance of normal-hearing children and adults. Ear Hear. 2010;31(03):336–344. doi: 10.1097/AUD.0b013e3181d3d514. [DOI] [PubMed] [Google Scholar]
- 7.Valente D L, Plevinsky H M, Franco J M, Heinrichs-Graham E C, Lewis D E. Experimental investigation of the effects of the acoustical conditions in a simulated classroom on speech recognition and learning in children. J Acoust Soc Am. 2012;131(01):232–246. doi: 10.1121/1.3662059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chermak G D. Deciphering auditory processing disorders in children. Otolaryngol Clin North Am. 2002;35(04):733–749. doi: 10.1016/s0030-6665(02)00056-7. [DOI] [PubMed] [Google Scholar]
- 9.Johnston K N, John A B, Kreisman N V, Hall J W, III, Crandell C C. Multiple benefits of personal FM system use by children with auditory processing disorder (APD) Int J Audiol. 2009;48(06):371–383. doi: 10.1080/14992020802687516. [DOI] [PubMed] [Google Scholar]
- 10.Lagacé J, Jutras B, Giguère C, Gagné J P. Speech perception in noise: exploring the effect of linguistic context in children with and without auditory processing disorder. Int J Audiol. 2011;50(06):385–395. doi: 10.3109/14992027.2011.553204. [DOI] [PubMed] [Google Scholar]
- 11.Neely R J, Green J L, Sciberras E, Hazell P, Anderson V. Relationship between executive functioning and symptoms of attention-deficit/hyperactivity disorder and autism spectrum disorder in 6–8 year old children. J Autism Dev Disord. 2016;46(10):3270–3280. doi: 10.1007/s10803-016-2874-6. [DOI] [PubMed] [Google Scholar]
- 12.Alcántara J I, Weisblatt E J, Moore B C, Bolton P F. Speech-in-noise perception in high-functioning individuals with autism or Asperger's syndrome. J Child Psychol Psychiatry. 2004;45(06):1107–1114. doi: 10.1111/j.1469-7610.2004.t01-1-00303.x. [DOI] [PubMed] [Google Scholar]
- 13.Corbett B A, Constantine L J.Autism and attention deficit hyperactivity disorder: assessing attention and response control with the integrated visual and auditory continuous performance test Child Neuropsychol 200612(4-5):335–348. [DOI] [PubMed] [Google Scholar]
- 14.Gomez R, Condon M. Central auditory processing ability in children with ADHD with and without learning disabilities. J Learn Disabil. 1999;32(02):150–158. doi: 10.1177/002221949903200205. [DOI] [PubMed] [Google Scholar]
- 15.Rance G, Saunders K, Carew P, Johansson M, Tan J. The use of listening devices to ameliorate auditory deficit in children with autism. J Pediatr. 2014;164(02):352–357. doi: 10.1016/j.jpeds.2013.09.041. [DOI] [PubMed] [Google Scholar]
- 16.Schafer E C, Mathews L, Mehta S. Personal FM systems for children with autism spectrum disorders (ASD) and/or attention-deficit hyperactivity disorder (ADHD): an initial investigation. J Commun Disord. 2013;46(01):30–52. doi: 10.1016/j.jcomdis.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 17.Schafer E C, Traber J, Layden P. Use of wireless technology for children with auditory processing disorders, attention-deficit hyperactivity disorder, and language disorders. Semin Hear. 2014;35(03):193–205. [Google Scholar]
- 18.Tomchek S D, Dunn W. Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am J Occup Ther. 2007;61(02):190–200. doi: 10.5014/ajot.61.2.190. [DOI] [PubMed] [Google Scholar]
- 19.Updike C D. The use of FM systems for children with attention deficit disorder. J Educ Audiol. 2006;13:7–14. [Google Scholar]
- 20.Schafer E C, Wright S, Anderson C. Assistive technology evaluations: Remote-microphone technology for children with autism spectrum disorder. J Commun Disord. 2016;64:1–17. doi: 10.1016/j.jcomdis.2016.08.003. [DOI] [PubMed] [Google Scholar]
- 21.Mangeot S D, Miller L J, McIntosh D N. Sensory modulation dysfunction in children with attention-deficit-hyperactivity disorder. Dev Med Child Neurol. 2001;43(06):399–406. doi: 10.1017/s0012162201000743. [DOI] [PubMed] [Google Scholar]
- 22.Ashburner J, Ziviani J, Rodger S. Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. Am J Occup Ther. 2008;62(05):564–573. doi: 10.5014/ajot.62.5.564. [DOI] [PubMed] [Google Scholar]
- 23.Rance G, Fava R, Baldock H.Speech perception ability in individuals with Friedreich ataxia Brain 2008131(Pt 8):2002–2012. [DOI] [PubMed] [Google Scholar]
- 24.Rance G, Corben L, Delatycki M. Auditory processing deficits in children with Friedreich ataxia. J Child Neurol. 2012;27(09):1197–1203. doi: 10.1177/0883073812448963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bradlow A R, Kraus N, Hayes E. Speaking clearly for children with learning disabilities: sentence perception in noise. J Speech Lang Hear Res. 2003;46(01):80–97. doi: 10.1044/1092-4388(2003/007). [DOI] [PubMed] [Google Scholar]
- 26.Calcus A, Deltenre P, Colin C, Kolinsky R. Peripheral and central contribution to the difficulty of speech in noise perception in dyslexic children. Dev Sci. 2018;21(03):e12558. doi: 10.1111/desc.12558. [DOI] [PubMed] [Google Scholar]
- 27.Nittrouer S, Krieg L M, Lowenstein J H. Speech recognition in noise by children with and without dyslexia: How is it related to reading? Res Dev Disabil. 2018;77:98–113. doi: 10.1016/j.ridd.2018.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Vanvooren S, Poelmans H, De Vos A, Ghesquière P, Wouters J. Do prereaders' auditory processing and speech perception predict later literacy? Res Dev Disabil. 2017;70:138–151. doi: 10.1016/j.ridd.2017.09.005. [DOI] [PubMed] [Google Scholar]
- 29.Ziegler J C, Pech-Georgel C, George F, Lorenzi C. Speech-perception-in-noise deficits in dyslexia. Dev Sci. 2009;12(05):732–745. doi: 10.1111/j.1467-7687.2009.00817.x. [DOI] [PubMed] [Google Scholar]
- 30.Individuals with Disabilities Education Improvement Act of 2004Vol Public Law 108–446;2004
- 31.Rance G, Chisari D, Saunders K, Rault J L. Reducing listening-related stress in school-aged children with autism spectrum disorder. J Autism Dev Disord. 2017;47(07):2010–2022. doi: 10.1007/s10803-017-3114-4. [DOI] [PubMed] [Google Scholar]
- 32.Schafer E C, Gopal K V, Mathews L. Effects of auditory training and remote microphone technology on the behavioral performance of children and young adults who have autism spectrum disorder. J Am Acad Audiol. 2019;30(05):431–443. doi: 10.3766/jaaa.18062. [DOI] [PubMed] [Google Scholar]
- 33.Schafer E C, Gopal K V, Mathews L, Kaiser K, Canale E, Creech A. Verification and validation of remote-microphone technology on children and college-age adults who have autism spectrum disorder. J Educ Ped Rehab Audiol. 2019;24:1–7. [Google Scholar]
- 34.Smart J L, Purdy S C, Kelly A S. Impact of personal frequency modulation systems on behavioral and cortical auditory evoked potential measures of auditory processing and classroom listening in school-aged children with auditory processing disorder. J Am Acad Audiol. 2018;29(07):568–586. doi: 10.3766/jaaa.16074. [DOI] [PubMed] [Google Scholar]
- 35.Sharma M, Purdy S C, Kelly A S. A randomized control trial of interventions in school-aged children with auditory processing disorders. Int J Audiol. 2012;51(07):506–518. doi: 10.3109/14992027.2012.670272. [DOI] [PubMed] [Google Scholar]
- 36.Rance G, Corben L A, Du Bourg E, King A, Delatycki M B. Successful treatment of auditory perceptual disorder in individuals with Friedreich ataxia. Neuroscience. 2010;171(02):552–555. doi: 10.1016/j.neuroscience.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 37.Hornickel J, Zecker S G, Bradlow A R, Kraus N. Assistive listening devices drive neuroplasticity in children with dyslexia. Proc Natl Acad Sci U S A. 2012;109(41):16731–16736. doi: 10.1073/pnas.1206628109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Purdy S C, Smart J L, Baily M, Sharma M. Do children with reading delay benefit from the use of personal FM systems in the classroom? Int J Audiol. 2009;48(12):843–852. doi: 10.3109/14992020903140910. [DOI] [PubMed] [Google Scholar]
- 39.Gopal K V, Schafer E C, Mathews L. Effects of auditory training on electrophysiological measures in individuals with autism spectrum disorder. J Am Acad Audiol. 2020;31(02):96–104. doi: 10.3766/jaaa.18063. [DOI] [PubMed] [Google Scholar]
- 40.Schafer E C, Bryant D, Sanders K. Fitting and verification of frequency modulation systems on children with normal hearing. J Am Acad Audiol. 2014;25(06):529–540. doi: 10.3766/jaaa.25.6.3. [DOI] [PubMed] [Google Scholar]
- 41.United States Health and Human Services Discrimination on the basis of disabilityAccessed April 14, 2020 at:https://www.hhs.gov/civil-rights/for-individuals/disability/index.html
- 42.Hawkins D B, Yacullo W S. Signal-to-noise ratio advantage of binaural hearing aids and directional microphones under different levels of reverberation. J Speech Hear Disord. 1984;49(03):278–286. doi: 10.1044/jshd.4903.278. [DOI] [PubMed] [Google Scholar]
- 43.Winiger A M, Alexander J M, Diefendorf A O. Minimal hearing loss: from a failure-based approach to evidence-based practice. Am J Audiol. 2016;25(03):232–245. doi: 10.1044/2016_AJA-15-0060. [DOI] [PubMed] [Google Scholar]
- 44.Davis J M, Elfenbein J, Schum R, Bentler R A. Effects of mild and moderate hearing impairments on language, educational, and psychosocial behavior of children. J Speech Hear Disord. 1986;51(01):53–62. doi: 10.1044/jshd.5101.53. [DOI] [PubMed] [Google Scholar]
- 45.Shepard N T, Davis J M, Gorga M P, Stelmachowicz P G. Characteristics of hearing-impaired children in the public schools: part I--demographic data. J Speech Hear Disord. 1981;46(02):123–129. doi: 10.1044/jshd.4602.123. [DOI] [PubMed] [Google Scholar]
- 46.Walker E A, McCreery R W, Spratford M. Trends and predictors of longitudinal hearing aid use for children who are hard of hearing. Ear Hear. 2015;36(01) 01:38S–47S. doi: 10.1097/AUD.0000000000000208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Bess F H, Tharpe A M. Unilateral hearing impairment in children. Pediatrics. 1984;74(02):206–216. [PubMed] [Google Scholar]
- 48.Bess F H, Tharpe A M. Case history data on unilaterally hearing-impaired children. Ear Hear. 1986;7(01):14–19. doi: 10.1097/00003446-198602000-00004. [DOI] [PubMed] [Google Scholar]
- 49.Bess F H, Tharpe A M. An introduction to unilateral sensorineural hearing loss in children. Ear Hear. 1986;7(01):3–13. doi: 10.1097/00003446-198602000-00003. [DOI] [PubMed] [Google Scholar]
- 50.Lieu J E, Tye-Murray N, Fu Q. Longitudinal study of children with unilateral hearing loss. Laryngoscope. 2012;122(09):2088–2095. doi: 10.1002/lary.23454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bess F H, Dodd-Murphy J, Parker R A. Children with minimal sensorineural hearing loss: prevalence, educational performance, and functional status. Ear Hear. 1998;19(05):339–354. doi: 10.1097/00003446-199810000-00001. [DOI] [PubMed] [Google Scholar]
- 52.Porter H, Sladen D P, Ampah S B, Rothpletz A, Bess F H. Developmental outcomes in early school-age children with minimal hearing loss. Am J Audiol. 2013;22(02):263–270. doi: 10.1044/1059-0889(2013/13-0013). [DOI] [PubMed] [Google Scholar]
- 53.Holstrum W J, Gaffney M, Gravel J S, Oyler R F, Ross D S. Early intervention for children with unilateral and mild bilateral degrees of hearing loss. Trends Amplif. 2008;12(01):35–41. doi: 10.1177/1084713807312172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bess F H. School-aged children with minimal sensorineural hearing loss. Hear J. 2009;52(05):10–12. [Google Scholar]
- 55.Crum M A, Matkin N D. Room acoustics: The forgotten variable? Lang Speech Hear Serv Sch. 1976;7(02):106–110. [Google Scholar]
- 56.Crandell C C. Speech recognition in noise by children with minimal degrees of sensorineural hearing loss. Ear Hear. 1993;14(03):210–216. doi: 10.1097/00003446-199306000-00008. [DOI] [PubMed] [Google Scholar]
- 57.Bess F H, Tharpe A M, Gibler A M. Auditory performance of children with unilateral sensorineural hearing loss. Ear Hear. 1986;7(01):20–26. doi: 10.1097/00003446-198602000-00005. [DOI] [PubMed] [Google Scholar]
- 58.Anderson K L, Goldstein H. Speech perception benefits of FM and infrared devices to children with hearing aids in a typical classroom. Lang Speech Hear Serv Sch. 2004;35(02):169–184. doi: 10.1044/0161-1461(2004/017). [DOI] [PubMed] [Google Scholar]
- 59.Kenworthy O T, Klee T, Tharpe A M. Speech recognition ability of children with unilateral sensorineural hearing loss as a function of amplification, speech stimuli and listening condition. Ear Hear. 1990;11(04):264–270. doi: 10.1097/00003446-199008000-00003. [DOI] [PubMed] [Google Scholar]
- 60.Updike C D. Comparison of FM auditory trainers, CROS aids, and personal amplification in unilaterally hearing impaired children. J Am Acad Audiol. 1994;5(03):204–209. [PubMed] [Google Scholar]
- 61.Tharpe A M, Ricketts T, Sladen D P. Chicago: Phonak AG; 2003. FM Systems for Children with Minimal to Mild Hearing Loss. ACCESS: Achieving Clear Communication Employing Sound Solutions; pp. 191–197. [Google Scholar]
- 62.Benítez-Barrera C R, Angley G P, Tharpe A M. Remote microphone system use at home: impact on caregiver talk. J Speech Lang Hear Res. 2018;61(02):399–409. doi: 10.1044/2017_JSLHR-H-17-0168. [DOI] [PubMed] [Google Scholar]
- 63.Franks J L.Why do students with hearing impairment resist wearing FM amplification?(Master's Thesis, Eastern Michigan University, Ypsilanti, Michigan, USA). 2008. Accessed September 24, 2020 at:https://commons.emich.edu/theses/205/