

Abstract
The COVID‐19 pandemic and its global response have resulted in unprecedented and rapid changes to most people’s day‐to‐day lives. To slow the spread of the virus, governments have implemented the practice of physical distancing (“social distancing”), which includes isolation within the home with limited time spent outdoors. During this extraordinary time, nature around the home may play a key role in mitigating against adverse mental health outcomes due to the pandemic and the measures taken to address it. To assess whether this is the case, we conducted an online questionnaire survey (n = 3,000) in Tokyo, Japan, to quantify the association between five mental health outcomes (depression, life satisfaction, subjective happiness, self‐esteem, and loneliness) and two measures of nature experiences (frequency of greenspace use and green view through windows from home). Accounting for sociodemographic and lifestyle variables, we found that the frequency of greenspace use and the existence of green window views from within the home was associated with increased levels of self‐esteem, life satisfaction, and subjective happiness and decreased levels of depression, anxiety, and loneliness. Our findings suggest that a regular dose of nature can contribute to the improvement of a wide range of mental health outcomes. With the recent escalation in the prevalence of mental health disorders, and the possible negative impacts of the COVID‐19 pandemic on public mental health, our findings have major implications for policy, suggesting that urban nature has great potential to be used as a “nature‐based solution” for improved public health.
Keywords: ecosystem services, global change, nature‐based intervention, nature‐based solution, personalized ecology, public health, urban greenspace, urbanization
Introduction
Since the first case of the novel coronavirus disease (COVID‐19) was diagnosed in December 2019 in Wuhan, China, it has spread throughout the world with alarming speed. This has led to extensive and widespread efforts to contain its spread. Along with the widespread use of masks, many governments globally have encouraged or mandated the practice of isolation and physical distancing (so‐called “social distancing”; Lewnard and Lo 2020). The outcome of this is an unprecedented and rapid change in most people’s day‐to‐day lives with many people currently spending the majority of their time at home in isolation from others. While these measures are proven to be effective in reducing the spread of the disease, they are inevitably likely to have huge negative consequences for personal mental health and well‐being in both the short and long terms (Galea et al. 2020). Indeed, recent evidence suggests that the adoption of physical distancing, as well as fears of contracting the COVID‐19 virus, are likely resulting in mental disorders, such as depression and increased sense of loneliness (Killgore et al. 2020, Li and Wang 2020, Rajkumar 2020).
During this extraordinary time, nature around the home might play a key role in mitigating against the risk of adverse mental health outcomes. This hypothesis stems from growing empirical evidence of the human health and well‐being benefits of direct experiences with nature (Keniger et al. 2013, Russell et al. 2013, Hartig et al. 2014, Soga and Gaston 2016, Bratman et al. 2019). For example, visiting greenspaces is known to increase positive emotions such as life satisfaction, happiness, and self‐esteem (Pretty et al. 2005, MacKerron and Mourato 2013, Ambrey and Fleming 2014) as well as decrease negative emotions such as depression, anxiety, and stress (Roe et al. 2013, Shanahan et al. 2016). Indeed, recent studies reported that people’s use of urban greenspaces (e.g., parks, forests) has increased substantially after the COVID‐19 pandemic (e.g.. Derks et al. 2020, Venter et al. 2020), suggesting that these environments can serve as important health resources for urban residents (Slater 2020). It remains unknown, however, how proximity to nature contributes to mental health patterns during a times of crises such as the COVID‐19 pandemic. Knowledge gained in this area has the potential to inform the development of public health policies aimed at improving health of a population.
While not ideal, it is possible for people to receive mental health benefits from nature from within their homes without having to physically visit natural environments (Russell et al. 2013, Cox et al. 2017b ). One notable “less immediate” experience of nature (sensu Soga and Gaston 2020) is viewing nature through windows from the home. To a greater or lesser extent, and either consciously or unconsciously, most people can have this type of experience every day (Cox et al. 2017a , Soga and Gaston 2020). Recent studies showed that nature views through windows are associated with a wide range of improved mental health outcomes, such as increased life satisfaction and well‐being, attention restoration, and stress recovery (e.g., Dravigne et al. 2008, Gilchrist et al. 2015, Li and Sullivan 2016, Chang et al. 2020). Knowing how “more immediate” (physically present in a natural environment) and “less immediate” (viewing nature through a window) nature experiences are associated with improved mental health outcomes might allow us to design urban areas and nature‐based interventions and programs for “happier” urban populations.
We surveyed 3,000 residents of Tokyo, central Japan, the world’s largest megacity, to determine the association between five mental health outcomes (depression, life satisfaction, subjective happiness, self‐esteem, and loneliness) and two measures of nature experiences (visiting urban greenspaces and green view through windows from home). People’s mental health statuses are commonly affected by various sociodemographic and lifestyle factors, such as age, sex, and annual household income (Shanahan et al. 2016, Cox et al. 2017b ). Thus, we adjusted for socioeconomic and lifestyle variables in our analyses to facilitate the detection of the effects of nature experiences distinct from other potential confounding factors.
Methods
Study area
Tokyo has a human population of ~14.0 million and occupies an area of 2,194 km2 (Tokyo Metropolitan Government 2020). Tokyo was placed under a state of emergency due to the COVID‐19 crisis from 7 April until 25 May 2020. People were asked to refrain from non‐essential excursions and schools and businesses were requested to close unless necessary. This measure was not compulsory, however, with no legal weight and could not be enforced. Thus, while some facilities within parks, such as playgrounds and car parks were closed, people were still able to use public parks freely.
Survey design
An online questionnaire survey delivered through a market research company (Rakuten Insight, Japan) was completed over a 3‐d period in early June 2020 by 3,000 adults who are enrolled in their survey database. Early June is a period of reasonably mild weather (prior to the rainy season and the onset of higher summer temperatures) when people are most likely to engage with nature around their home making it an ideal time to conduct the survey. The survey assessed three aspects of the relationship between mental health and nature experiences within Tokyo: (1) mental health (depression and anxiety, self‐esteem, life satisfaction, subjective happiness, and loneliness; Table 1); (2) levels of experiences with nature (frequency of greenspace use and green views from windows of home; Table 2); and (3) lifestyle and sociodemographic information (frequency of smoking, alcohol use, age, gender, annual household income; Table 3).
Table 1.
Five mental health outcomes considered in this study.
| Mental health outcome | Psychological scale used | Example questions | Mental health metric | Answer scale |
|---|---|---|---|---|
| Self‐esteem | Rosenberg Self‐Esteem Scale (Rosenberg 1965) |
“On the whole, I am satisfied with myself.” “I feel I do not have much to be proud of.” |
positive | Respondents were asked to rate the extent to which they agree with the 10 items on a four‐point scale, ranging from 0 (strongly disagree) to 4 (strongly agree) for positive items, and the scores reversed when the items are negative. The scores across the 10 items were summed, ranging from 0 to 40, with higher values indicating greater self‐esteem. |
| Life satisfaction | Liang’s (1984) version of the Life Satisfaction Index A (Neugarten et al. 1961) |
“This is the dreariest time of my life.” “I would not change my past life even if I could do.” |
positive | Respondents were asked to rate the extent to which they agree with the 11 items on a three‐point scale, ranging from 0 (disagree) to 2 (agree) for positive items, and the scores reversed when the items are negative. The scores across the 11 items were summed, ranging from 0 to 22, with higher values indicating greater life satisfaction. |
| Subjective happiness | Subjective Happiness Scale (Lyubomirsky and Lepper 1999) |
“In general, I consider myself: …” “Some people are generally very happy. They enjoy life regardless of what is going on, getting the most out of everything. To what extent does this characterization describe you?” |
positive | Respondents were asked to answer the four items on a seven‐point scale, ranging from 1 (very unhappy or not at all) to 7 (very happy to a great deal). The scores across the four items were summed, ranging from 4 to 28, with higher values indicating greater happiness. |
| Loneliness | UCLA Loneliness Scale (Version 3) (Russell 1996) |
“How often do you feel alone?” “How often do you feel close to people?” |
negative | Respondents were asked to answer the 20 items on a four‐point scale, ranging from 1 (never) to 4 (often) for negative items, and the scores reversed when the items are positive. The scores across the 20 items were summed, ranging from 20 to 80, with higher values indicating greater loneliness. |
| Depression and anxiety | 12‐item General Health Questionnaire (Goldberg and Williams 1988)† |
“Have you recently been able to concentrate on what you’re doing?” “Have you recently lost much sleep over worry?” |
negative | Respondents were asked to answer the 12 items. For each question, responses indicating distress score 1 and those indicating no or limited distress score 0. The scores across the 12 items were summed, ranging from 0 to 12, with higher values indicating greater symptoms of depression. |
We used the resultant variables as the response variables in our analysis.
This is the most extensively used self‐reporting instrument for measuring common mental disorders, such as depression and anxiety (Lundin et al. 2016).
Table 2.
Three measures of nature experiences used in this study; we used the resultant variables as predictor variables in our analysis.
| Measure | Question | Answer scale |
|---|---|---|
| Frequency of greenspace (“more immediate” experience) | During the last month (i.e., May), how many days in total did you visit neighborhood greenspace (e.g., parks, woodlands, grasslands)? | could range from 0 to 31 d |
| Duration of greenspace (“more immediate” experience) | During the last month (i.e., May), how much time did you spend in neighborhood greenspace on an average week? | no time; less than 1 h; 1–2 h; 2–4 h; 4–6 h; 6–8 h; 8–10 h; 10–12 h; over 12 h† |
| Green view through windows from home (“less immediate” experience) | In your house do you have a green view from the room in which you spend most of your time at home?‡ | green view, no green view |
For analysis we converted to a continuous variable: (0, 0.5, 1.5, 3, 5, 7, 9, 11, 12).
Green views included roadside trees, garden trees, parks, woodlands.
Table 3.
Five lifestyle and five socio‐demographic variables used in this study.
| Category and variable | Answer scale |
|---|---|
| Lifestyle variables | |
| Frequency of smoking | 0, none; 1, less than once a month; 2, one or two times per month; 3, two or three times per month; 4, one or two times per week; 5, three or four times per week; 6, five or six times per week; 7, every day |
| Frequency of drinking alcohol | 0, none; 1, less than once a month; 2, one or two times per month; 3, 2 or 3 times per month; 4, one or two times per week; 5, three or four times per week; 6, five or six times per week; 7, every day |
| Number of working days per week | could range from 0 to 7 days. |
| Presence of a pet (dog or cat) in the home | 1, presence; 0, absence |
| Number of children in the home | 0, none; 1, one child; 2, two children; 3, three children; 4, four children; 5, five children; 6, more than five children |
| Sociodemographic variables | |
| Sex | female; male |
| Age | age in years |
| Annual household income | 1, less than ¥3,000,000 (~US$30,000); 2, ¥3,000,000 – 5,000,000 (~US$50,000); 3, ¥5,000,000 – 7,000,000 (~US$70,000); 4, ¥7,000,000 – 10,000,000 (~US$100,000); 5, ¥10,000,000 – 15,000,000 (~US$150,000); 6, more than ¥15,000,000 (~US$150,000) |
| Housing type | owned house; owned flat; rented house; rented flat; other |
| Degree of income changes due to the COVID‐19 crisis | 1, greatly increased (more than double); 2, increased somewhat; 3, slightly increased; 4, generally unchanged; 5, slightly decreased; 6, decreased somewhat; 7, greatly decreased (less than one‐half) |
We used the resultant variables as some of the predictor variables in our analysis.
Participants were also asked to provide a postcode of the area where they currently live so that the greenness of their current residential environment could be assessed (see Neighborhood greenness). The survey took approximately 20 minutes to complete per participant. Participation in the survey was considered as consent. The survey was anonymous and no identifiable details (e.g., name, address) were collected from the participants. This study was conducted with approval from the ethics committee of the University of Tokyo.
Mental health
Participants provided self‐reported information on five mental health outcomes (Table 1): depression and anxiety, self‐esteem, life satisfaction, subjective happiness, and loneliness.
To measure participants’ mental health outcomes, we used well‐established psychological scales (see Table 1 for more details). For all five health measures, we used the Japanese‐translated version of the scales.
Nature experience
For each respondent, we generated three measures of the experience of nearby nature (Table 2): frequency of greenspace use (“more immediate” experience), duration of greenspace use (“more immediate” experience), and green view through windows from home (“less immediate” experience).
Lifestyle and sociodemographic factors
We collected several lifestyle and sociodemographic variables that potentially affect people’s mental health (see Table 3 for the full list and description of the lifestyle and sociodemographic variables we used). Lifestyle variables included the frequency of smoking and drinking alcohol, number of working days per week, the presence of a pet in the home, and the number of children in the home. Sociodemographic variables included sex, age, annual household income, and housing type. With the sociodemographic section, we also asked the respondents to report the degree of income changes due to the COVID‐19 crisis, which was additionally used as a sociodemographic variable.
Neighborhood greenness
For each participant we measured the greenness of the home environment. To do so, we calculated the Normalization Different Vegetation Index (NDVI) within a 250‐m buffer around the centroid of each respondent’s postcode. NDVI, which is derived from satellite observations, is one of the most extensively applied vegetation indices for quantifying the presence, density, and condition of vegetation (Pettorelli et al. 2005). Recent studies showed that NDVI is a good predictor of general urban greenness (i.e., density of street trees) (e.g., Gascon et al. 2016, Reid et al. 2018). We chose a 250‐m buffer as a neighborhood zone because this is the distance that was considered to influence what a person can experience in their daily lives (Cox et al. 2017b ). In our preliminary analysis, we considered several different sizes of the buffer (e.g., 500 m, 1,000 m) and confirmed that the buffer size did not affect the results of the analysis essentially. All spatial analyses were performed using QGIS 3.10 software (Quantum GIS Development Team 2020). The NDVI data downloaded from the Copernicus Open Access HUB (data available online).4 We calculated NDVI values from Level‐1C images of the Sentinel‐2 mission (taken on 8 May 2017) that has spatial resolution of 10 m.
Statistical analysis
Since the frequency and duration of greenspace use were highly correlated (r(2,998) = 0.696, P < 0.0001), we only used the frequency measure in the latter analysis and termed this variable “greenspace use.”
To determine the key factors that predict mental health outcomes we fitted linear models (LMs) using the mental health metrics (Table 1) as our response variables and the green space use, green view (Table 2), neighborhood greenness (NDVI), lifestyle, and sociodemographic measures as predictors (Table 3). To allow direct comparisons, we scaled all our continuous predictors to have a mean of zero and a standard deviation of one. We also scaled our response variables in the same manner to aid interpretation and comparisons. We conducted a model averaging procedure using Akaike’s Information Criterion corrected for small sample sizes (AICc; Burnham and Anderson 2002). We fitted all subsets of a full model that contained all of our predictor variables and performed model averaging on all models within ΔAICc = 6 (Burnham and Anderson 2002, Anderson 2007). After averaging across the subset of models, we calculated the mean estimates and 95% confidence intervals for each explanatory variable. We plotted our results as effect sizes and interpreted predictors as significant if their 95% confidence intervals did not cross the zero‐effect line (du Prel et al. 2009, Welsh 2011). We used R version 4.0.2 for our analyses and plotting (R Core Team 2020) including the use of the plyr (Wickham 2011), forcats (Wickham 2018), MuMIn (Barton 2016), ggplot2 (Wickham 2009), and ggpubr (Kassambara 2018) packages.
Results
Data description
The full information on sociodemographic and lifestyle characteristics of the participants is shown in Appendix S1: Table S1. Our sample participants represented the full range of different age groups. The number of male and female participants was the same (1,500 of each). Among the 3,000 participants, there was marked variation in the five mental health outcomes (Fig. 1). The frequency of greenspace use varied widely across participants, but the majority of participants did not visit any greenspace in May 2020 (Fig. 2). Approximately 81% of the participants reported that their home had a view of nature (greenspace or trees; Fig. 2).
Fig. 1.
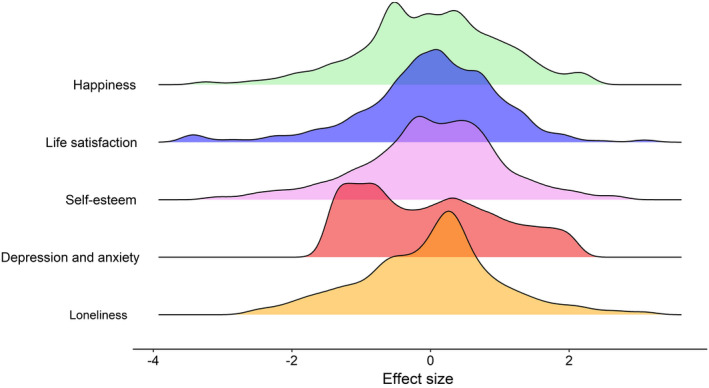
Distributions of answers given to the questions asked to assess participants’ mental health status (depression and anxiety, self‐esteem, life satisfaction, subjective happiness and loneliness). For the purposes of this plot, the metrics were rescaled to have a mean of zero and standard deviation of one. Note that depression and anxiety and loneliness were negative health metrics, with the higher values indicating poor health status (greater symptoms of depression and loneliness).
Fig. 2.
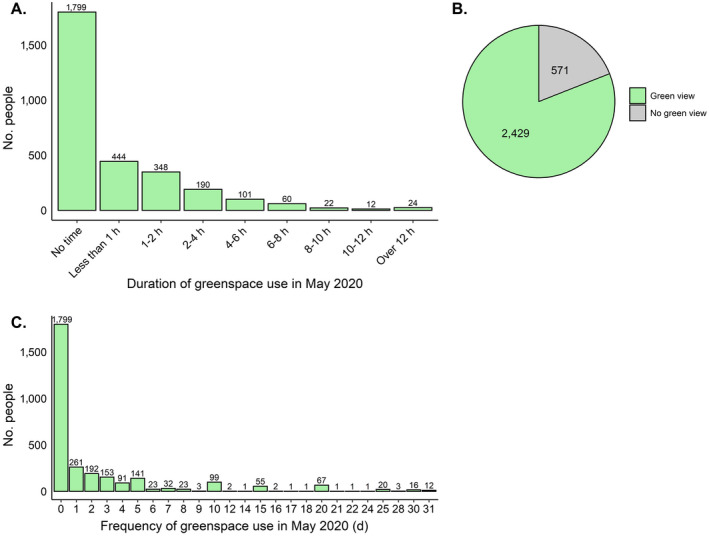
Frequencies of answers given to the questions asked to assess participants’ levels of nature experiences (A, duration of greenspace use; B, green view through windows from home; C, frequency of greenspace use). Numbers above the bars in panels A and C and in pie chart in panel B represent the numbers of people who answered the questions in that way.
Factors associated with mental health
Several of the variables were significantly associated with negative and positive effects on people’s mental health (note: variables that were interpreted as non‐significant for all of the five health metrics are omitted from the plots in Fig. 3; the detailed statistics of the LMs are summarized in Table S2). Both greenspace use and green view were significantly positively associated with an increase in self‐esteem, life satisfaction, and happiness (Fig. 3A) and negatively associated with loneliness and depression and anxiety (Fig. 3B). Neighborhood greenness was not related to any of the five health metrics (Table S2). A greater impact of the COVID‐19 pandemic on income was significantly associated with increased depression and anxiety. Smoking had a negative impact on happiness and was positively associated with increased depression and anxiety. Alcohol use was negatively associated with loneliness. Higher incomes were associated with increased self‐esteem, life satisfaction, and happiness and decreased loneliness and depression and anxiety. Males had more self‐esteem and less life satisfaction and happiness than females. Males also reported greater loneliness. Older people had more self‐esteem and happiness and less loneliness and depression and anxiety than younger people. Neighborhood greenness, number of children, number of working days per week, and owning a pet all had no significant relationship with any of the mental health metrics (Appendix S1: Table S2).
Fig. 3.
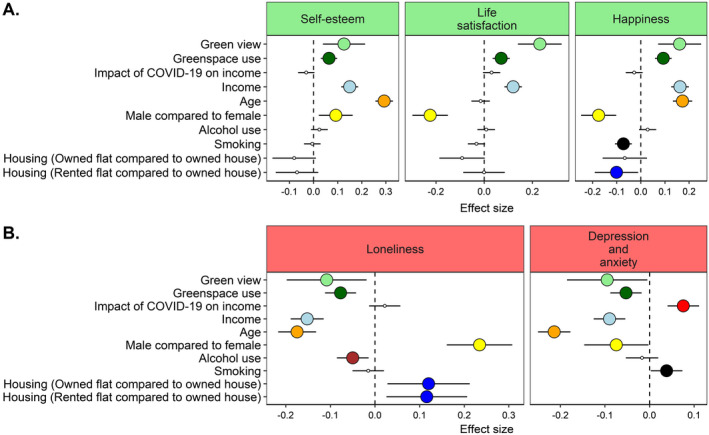
Model‐averaged coefficients (effect sizes) for all models below ΔAICc = 6 of all subsets of model that contains all of our predictor variables against the five mental health response variables (see Appendix S1: Appendix S1: Table S2). All continuous variables were scaled to enable direct comparisons. Shaded symbols represent significant effects. Error bars represent 95% confidence intervals. Predictors are interpreted as significant if their 95% confidence intervals do not cross the zero‐effect line (du Prel et al. 2009, Welsh 2011). Response variables plotted in panel A are positive mental health metrics and those plotted in panel B are negative mental health metrics. Predictors that were interpreted as not significant for all of the five metrics are not included on the plot (see Appendix S1: Appendix S1: Table S2).
Discussion
Key findings
The COVID‐19 epidemic has created a stressful environment for most people around the globe (Galea et al. 2020). We have demonstrated that the experiences of nearby nature (both less and more immediate) can help prevent poor mental health during such a stressful time, or at least, not make it worse. We found that the degree of self‐esteem, life satisfaction, and subjective happiness were all positively related to the frequency of greenspace use around the home and green views through windows at home. We also showed reduced levels of loneliness and depression and anxiety in people who use greenspace frequently and live at the home with a green view. These results suggest that urban nature can be used as a “nature‐based solution” for improved public health (van den Bosch and Sang 2017). This is especially relevant during the COVID‐19 pandemic, when people are experiencing increased levels of stress and are confined in isolation in their homes.
We found consistent positive associations between frequency of greenspace use and the five measures of mental health outcomes. There are several possible pathways through which greenspace use promotes mental health outcomes. The first, and most direct one, is the added health benefits of direct interactions with nature (Keniger et al. 2013, Hartig et al. 2014, Bratman et al. 2019). Visiting urban green space delivers multi‐sensory experiences for a person, such as the sight and sound of birds and the scent of flowers (Soga and Gaston 2020), which can improve their mental health status through various human senses (Franco et al. 2017). Second, greenspace use is likely to encourage people to undertake physical exercise (so‐called “green exercise”), which in turn contributes to improving mental health (Pretty et al. 2005). Third, urban greenspace provides opportunities to interact with other members of local communities (e.g., friends), which is likely to ameliorate loneliness and improve well‐being (Maas et al. 2009). While this third pathway might have less of an influence than ordinarily due to social distancing practices implement during the pandemic, we do believe that interactions such as simply seeing other people or signaling to others from an acceptable distance, will help lessen adverse mental impacts from social distancing. Of course, these three major pathways are likely to not act independently of each other but are likely to work synergistically.
People with homes with a view of nature (greenspace or trees) reported better mental status for all of the mental health measures we considered. Although the causal relationships are not easily untangled, at face value this implies that viewing nature through a window can promote a person’s improved mental health outcomes. This interpretation is consistent with many studies that demonstrate a positive association between nature views from windows and improved mental health and well‐being (e.g., Dravigne et al. 2008, Gilchrist et al. 2015, Li and Sullivan 2016, Chang et al. 2020). Of course, nature close to the home likely affects a person’s mental health through pathways other than just sight (the view from the window). For example, roadside trees enhance the abundance and diversity of birds around home, which is likely to increase people’s frequency of listening to bird songs (Cox et al. 2017b ). This in turn might improve people’s mental health as listening to bird songs are known to be associated with improved mental health, such as attention restoration and stress recovery (e.g., Ratcliffe et al. 2013, Benfield et al. 2014). An interesting direction for future research is therefore to determine the underlying mechanisms for the relationship between nature close to the home and improved mental health.
Surprisingly, the effect of a green view on people’s mental health was generally greater than that of the use of greenspace. This is an important result as it suggests that less immediate experiences with nature can have comparable benefits to human health and well‐being compared to more immediate ones. One likely reason for our result could be that we conducted the surveys during the COVID‐19 pandemic, a time when people were advised to stay at home in isolation, and thus less immediate nature experiences might greatly outnumber the more immediate ones. Our result might also be associated with the timing of our surveys: we asked participants to report their behavioral patterns for May, which is one of the most comfortable seasons in Japan. At this time, many people might have opened windows within their homes and experienced the nearby nature more directly. Given that most of the literature on the relationship between nature experiences and mental health is concerned with more immediate experiences of nature, our results are enlightening and suggest that more attention should be paid to less immediate experiences with nature.
Of course, one can argue that the presence of a green view through windows is an alternative measure of neighborhood greenness, and the latter factor is what actually affects people’s mental health. In our study, green view through windows and NDVI were significantly associated with each other in a fitted linear model (Appendix S1: Fig. S1), so we acknowledge the uncertainty in our results. If, however, green views through windows itself is a driver of the health benefits that flow from nearby nature, then urban greening policies must go well beyond merely increasing the number of roadside trees and greenspace coverage and also focus on arranging the placement of these green components to maximize people’s personalized levels of nature (Gaston et al. 2018). Future research to understand how the placement of greenspaces and trees affects people’s nature experiences, and associated benefits for mental health, will be necessary to determine how nature‐based interventions can be designed to improve health and well‐being for urban populations.
The five mental health measures we used are likely to be interrelated in multiple ways. Depression, for example, is usually associated with diminished life satisfaction and happiness, as the former might be, at least partly, the cause of the latter (Headey et al. 1993, Milevsky et al. 2007, Beutel et al. 2010). For the same reason, loneliness is known to be a strong predictor of the severity of depressive and anxious symptoms (Adams et al. 2004, Teo et al. 2018). These facts suggest that improved health outcomes derived from nature experiences typically do not occur in isolation, but rather simultaneously with others. This raises the possibility that direct interactions with nature contribute not only towards improving specific targeted health outcomes, but also have many secondary (spill‐over) effects on human health and well‐being.
Limitations
Despite the major strengths of our analysis, we recognize several limitations. First, although we found a clear relationship between experiences of nearby nature and mental health, we were not able to determine a cause‐and‐effect relationship between these variables due to the cross‐sectional nature of our study design. Indeed, we could not exclude the possibility that people with better mental health might use greenspaces more frequently and choose houses with green views. Thus, additional studies using more longitudinal designs are needed (e.g., White et al. 2013). Second, this study relied on self‐reported data, which may lead to reporting bias, such as under‐or over‐reporting of the true health outcomes or recall bias. To overcome this limitation, we recommend additional studies that use more objective health measures (e.g., Gidlow et al. 2016). Third, as participation to our survey was voluntary, there is the potential for non‐response bias where participants who chose to take part in the survey have different personal characteristics compared with those who chose not to participate. Indeed, it is well known that people with poorer health tend to avoid participating in health surveys (van Loon et al. 2003), raising the possibility of an underestimation of the prevalence of mental health problems that actually occur. However, the aim of our study is not to estimate the magnitude of mental health problems during the COVID‐19 pandemic but to examine the association between various personal factors and mental health outcomes, and the latter is found to be less affected by non‐response bias (van Loon et al. 2003, Cheung et al. 2017). Last, since the benefits of nature experiences vary among regions with different socioeconomic and cultural backgrounds (Saw et al. 2015), caution must be applied when attempting to generalize conclusions to populations outside of Tokyo. We therefore recommend that similar studies should be undertaken in other regions globally.
Conclusions
Globally, the prevalence of mental health problems (particularly depression) is increasing at an alarming rate. Indeed, the WHO has stated that untreated mental health problems account for more than 10% of the total global burden of disease and have projected that, by 2030, mental health problems will be the leading cause of mortality and morbidity globally (World Health Assembly 2012). Unfortunately, this situation is likely exacerbated by the COVID‐19 pandemic, with probable huge emotional costs to, and quality of life impacts on, people, which can increase risk factors for mental health problems (Galea et al. 2020). Given these conditions, our results have potentially major implications for healthcare policy, as they suggest that urban nature (roadside trees and public greenspace) has the potential to prevent or ameliorate risk factors for mental health. Given the associated benefits of the provision of multiple ecosystem services, such as improving carbon storage, ameliorating the heat island effect, and conserving local biodiversity (Lovell and Taylor 2013, Stott et al. 2015), maintaining and enhancing green infrastructure in cities offers wide‐ranging benefits to the society where they would be felt most.
Supporting information
Appendix S1
Acknowledgments
M. Soga was funded by the Japan Society for the Promotion of Science (grant no. 20H04375), the Toyota Foundation (D19‐R‐0102), the Kurita Water and Environment Foundation (grant no. 19E029), and the Kurata Grants awarded by the Hitachi Global Foundation (grant no. 1399). M. J. Evans was funded by the Japan Society for the Promotion of Science as a Postdoctoral Research Fellow (P19084).
Soga, M. , Evans M. J., Tsuchiya K., and Fukano Y.. 2021. A room with a green view: the importance of nearby nature for mental health during the COVID‐19 pandemic. Ecological Applications 31(2):e02248. 10.1002/eap.2248
Corresponding Editor: David S. Schimel.
Footnotes
Data Availability
Data are available on Figshare: https://doi.org/10.6084/m9.figshare.12941729.
Literature Cited
- Adams, K. B. , Sanders S., and Auth E. A.. 2004. Loneliness and depression in independent living retirement communities: risk and resilience factors. Aging & Mental Health 8:475–485. [DOI] [PubMed] [Google Scholar]
- Ambrey, C. , and Fleming C.. 2014. Public greenspace and life satisfaction in urban Australia. Urban Studies 51:1290–1321. [Google Scholar]
- Anderson, D. R. 2007. Model based inference in the life sciences: a primer on evidence. Springer Science & Business Media, New York, New York, USA. [Google Scholar]
- Barton, K. 2016. Multi‐model inference.R package version 1.15.6. https://cran.r‐project.org/package=MuMIn
- Benfield, J. A. , Taff B. D., Newman P., and Smyth J.. 2014. Natural sound facilitates mood recovery. Ecopsychology 6:183–188. [Google Scholar]
- Beutel, M. E. , Glaesmer H., Wiltink J., Marian H., and Brähler E.. 2010. Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 13:32–39. [DOI] [PubMed] [Google Scholar]
- Bratman, G. N. , et al. 2019. Nature and mental health: an ecosystem service perspective. Science Advances 5:eaax0903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnham, K. P. , and Anderson D. R.. 2002. Model selection and multimodel inference: a practical information‐theoretic approach. Springer, New York, New York, USA. [Google Scholar]
- Chang, C. C. , Oh R. R. Y., Le Nghiem T. P., Zhang Y., Tan C. L., Lin B. B., Gaston K. J., Fuller R. A., and Carrasco L. R.. 2020. Life satisfaction linked to the diversity of nature experiences and nature views from the window. Landscape and Urban Planning 202:103874. [Google Scholar]
- Cheung, K. L. , Peter M., Smit C., de Vries H., and Pieterse M. E.. 2017. The impact of non‐response bias due to sampling in public health studies: a comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health 17:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox, D. T. C. , Hudson H. L., Shanahan D. F., Fuller R. A., and Gaston K. J.. 2017a. The rarity of direct experiences of nature in an urban population. Landscape and Urban Planning 160:79–84. [Google Scholar]
- Cox, D. T. C. , Shanahan D. F., Hudson H. L., Plummer K. E., Siriwardena G. M., Fuller R. A., Anderson K., Hancock S., and Gaston K. J.. 2017b. Doses of neighborhood nature: the benefits for mental health of living with nature. BioScience 67:147–155. [Google Scholar]
- Derks, J. , Giessen L., and Winkel G.. 2020. COVID‐19‐induced visitor boom reveals the importance of forests as critical infrastructure. Forest Policy and Economics 118:102253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dravigne, A. , Waliczek T. M., Lineberger R. D., and Zajicek J. M.. 2008. The effect of live plants and window views of green spaces on employee perceptions of job satisfaction. HortScience 43:183–187. [Google Scholar]
- du Prel, J.‐B. , Hommel G., Röhrig B., and Blettner M.. 2009. Confidence interval or p‐value?: Part 4 of a series on evaluation of scientific publications. Deutsches Ärzteblatt International 106:335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franco, L. S. , Shanahan D. F., and Fuller R. A.. 2017. A review of the benefits of nature experiences: more than meets the eye. International Journal of Environmental Research and Public Health 14:864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galea, S. , Merchant R. M., and Lurie N.. 2020. The mental health consequences of COVID‐19 and physical distancing: The need for prevention and early intervention. JAMA Internal Medicine 180:817–818. [DOI] [PubMed] [Google Scholar]
- Gascon, M. , Cirach M., Martínez D., Dadvand P., Valentín A., Plasència A., and Nieuwenhuijsen M. J.. 2016. Normalized difference vegetation index (NDVI) as a marker of surrounding greenness in epidemiological studies: the case of Barcelona city. Urban Forestry & Urban Greening 19:88–94. [Google Scholar]
- Gaston, K. J. , Soga M., Duffy J. P., Garrett J. K., Gaston S., and Cox D. T.. 2018. Personalised ecology. Trends in Ecology & Evolution 33:916–925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gidlow, C. J. , Randall J., Gillman J., Smith G. R., and Jones M. V.. 2016. Natural environments and chronic stress measured by hair cortisol. Landscape and Urban Planning 148:61–67. [Google Scholar]
- Gilchrist, K. , Brown C., and Montarzino A.. 2015. Workplace settings and wellbeing: greenspace use and views contribute to employee wellbeing at peri‐urban business sites. Landscape and Urban Planning 138:32–40. [Google Scholar]
- Goldberg, D. , and Williams P.. 1988. A user’s guide to the General Health Questionnaire. NFER‐Nelson, Windsor, UK. [Google Scholar]
- Hartig, T. , Mitchell R., De Vries S., and Frumkin H.. 2014. Nature and health. Annual Review of Public Health 35:207–228. [DOI] [PubMed] [Google Scholar]
- Headey, B. , Kelley J., and Wearing A.. 1993. Dimensions of mental health: life satisfaction, positive affect, anxiety and depression. Social Indicators Research 29:63–82. [Google Scholar]
- Kassambara, A. 2018. ggpubr: ‘ggplot2’ Based Publication Ready Plots. R package version 0.2. https://CRAN.R758project.org/package=ggpubr
- Keniger, L. E. , Gaston K. J., Irvine K. N., and Fuller R. A.. 2013. What are the benefits of interacting with nature? International Journal of Environmental Research and Public Health 10:913–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killgore, W. D. , Cloonen S. A., Taylor E. C., and Dailey N. S.. 2020. Loneliness: a signature mental health concern in the era of COVID‐19. Psychiatry Research 290:113117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewnard, J. A. , and Lo N. C.. 2020. Scientific and ethical basis for social‐distancing interventions against COVID‐19. Lancet Infectious Diseases 20:631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, D. , and Sullivan W. C.. 2016. Impact of views to school landscapes on recovery from stress and mental fatigue. Landscape and Urban Planning 148:149–158. [Google Scholar]
- Li, L. Z. , and Wang S.. 2020. Prevalence and predictors of general psychiatric disorders and loneliness during COVID‐19 in the United Kingdom. Psychiatry Research 291:113267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang, J. 1984. Dimensions of the Life Satisfaction Index A: a structural formulation. Journal of Gerontology 5:613–622. [DOI] [PubMed] [Google Scholar]
- Lovell, S. T. , and Taylor J. R.. 2013. Supplying urban ecosystem services through multifunctional green infrastructure in the United States. Landscape Ecology 28:1447–1463. [Google Scholar]
- Lundin, A. , Hallgren M., Theobald H., Hellgren C., and Torgén M.. 2016. Validity of the 12‐item version of the General Health Questionnaire in detecting depression in the general population. Public health 136:66–74. [DOI] [PubMed] [Google Scholar]
- Lyubomirsky, S. , and Lepper H.. 1999. A measure of subjective happiness: preliminary reliability and construct validation. Social Indicators Research 46:137–155. [Google Scholar]
- Maas, J. , Van Dillen S. M., Verheij R. A., and Groenewegen P. P.. 2009. Social contacts as a possible mechanism behind the relation between green space and health. Health & Place 15:586–595. [DOI] [PubMed] [Google Scholar]
- MacKerron, G. , and Mourato S.. 2013. Happiness is greater in natural environments. Global Environmental Change 23:992–1000. [Google Scholar]
- Milevsky, A. , Schlechter M., Netter S., and Keehn D.. 2007. Maternal and paternal parenting styles in adolescents: associations with self‐esteem, depression and life‐satisfaction. Journal of Child and Family Studies 16:39–47. [Google Scholar]
- Neugarten, B. L. , Havighurst R. J., and Tobin S. S.. 1961. The measurement of life satisfaction. Journal of Gerontology 16:85–89. [DOI] [PubMed] [Google Scholar]
- Pettorelli, N. , Vik J. O., Mysterud A., Gaillard J. M., Tucker C. J., and Stenseth N. C.. 2005. Using the satellite‐derived NDVI to assess ecological responses to environmental change. Trends in Ecology & Evolution 20:503–510. [DOI] [PubMed] [Google Scholar]
- Pretty, J. , Peacock J., Sellens M., and Griffin M.. 2005. The mental and physical health outcomes of green exercise. International Journal of Environmental Health Research 15:319–337. [DOI] [PubMed] [Google Scholar]
- Quantum GIS Development Team . 2020. Quantum GIS geographic information system (3.10). [Open source geospatial foundation project]. http://qgis.osgeo.org
- R Core Team 2020. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. www.R‐project.org [Google Scholar]
- Rajkumar, R. P. 2020. COVID‐19 and mental health: a review of the existing literature. Asian Journal of Psychiatry 52:102066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ratcliffe, E. , Gatersleben B., and Sowden P. T.. 2013. Bird sounds and their contributions to perceived attention restoration and stress recovery. Journal of Environmental Psychology 36:221–228. [Google Scholar]
- Reid, C. E. , Kubzansky L. D., Li J., Shmool J. L., and Clougherty J. E.. 2018. It’s not easy assessing greenness: a comparison of NDVI datasets and neighborhood types and their associations with self‐rated health in New York City. Health & Place 54:92–101. [DOI] [PubMed] [Google Scholar]
- Roe, J. J. , Thompson C. W., Aspinall P. A., Brewer M. J., Duff E. I., Miller D., Mitchell R., and Clow A.. 2013. Green space and stress: evidence from cortisol measures in deprived urban communities. International Journal of Environmental Research and Public Health 10:4086–4103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg, M. 1965. Society and the adolescent self‐image. Princeton University Press, Princeton, New Jersey, USA. [Google Scholar]
- Russell, D. W. 1996. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. Journal of Personality Assessment 66:20–40. [DOI] [PubMed] [Google Scholar]
- Russell, R. , Guerry A. D., Balvanera P., Gould R. K., Basurto X., Chan K. M., Klain S., Levine J., and Tam J.. 2013. Humans and nature: how knowing and experiencing nature affect well‐being. Annual Review of Environment and Resources 38:473–502. [Google Scholar]
- Saw, L. E. , Lim F. K., and Carrasco L. R.. 2015. The relationship between natural park usage and happiness does not hold in a tropical city‐state. PLoS ONE 10:e0133781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shanahan, D. F. , Bush R., Gaston K. J., Lin B. B., Dean J., Barber E., and Fuller R. A.. 2016. Health benefits from nature experiences depend on dose. Scientific Reports 6:28551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slater, S. J. 2020. Recommendations for keeping parks and green space accessible for mental and physical health during COVID‐19 and other pandemics. Preventing Chronic Disease 17:200204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soga, M. , and Gaston K. J.. 2016. Extinction of experience: the loss of human–nature interactions. Frontiers in Ecology and the Environment 14:94–101. [Google Scholar]
- Soga, M. , and Gaston K. J.. 2020. The ecology of human–nature interactions. Proceedings of the Royal Society B 287:20191882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stott, I. , Soga M., Inger R., and Gaston K. J.. 2015. Land sparing is crucial for urban ecosystem services. Frontiers in Ecology and the Environment 13:387–393. [Google Scholar]
- Teo, A. R. , Marsh H. E., Forsberg C. W., Nicolaidis C., Chen J. I., Newsom J., Saha S., and Dobscha S. K.. 2018. Loneliness is closely associated with depression outcomes and suicidal ideation among military veterans in primary care. Journal of Affective Disorders 230:42–49. [DOI] [PubMed] [Google Scholar]
- Tokyo Metropolitan Government . 2020. https://www.metro.tokyo.lg.jp/tosei/hodohappyo/press/2020/07/02/01.html
- van den Bosch, M. , and Sang Å. O.. 2017. Urban natural environments as nature‐based solutions for improved public health – a systematic review of reviews. Environmental Research 158:373–384. [DOI] [PubMed] [Google Scholar]
- van Loon, A. J. M. , Tijhuis M., Picavet H. S. J., Surtees P. G., and Ormel J.. 2003. Survey non‐response in the Netherlands: effects on prevalence estimates and associations. Annals of Epidemiology 13:105–110. [DOI] [PubMed] [Google Scholar]
- Venter, Z. , Barton D., Gundersen V., Figari H., and Nowell M.. 2020. Urban nature in a time of crisis: recreational use of green space increases during the COVID‐19 outbreak in Oslo, Norway. Environmental Research Letters 15:104075. [Google Scholar]
- Welsh, A. H. 2011. Aspects of statistical inference. John Wiley & Sons, New York, New York, USA. [Google Scholar]
- White, M. P. , Alcock I., Wheeler B. W., and Depledge M. H.. 2013. Would you be happier living in a greener urban area? A fixed‐effects analysis of panel data. Psychological Science 24:920–928. [DOI] [PubMed] [Google Scholar]
- Wickham, H. 2009. ggplot2: Elegant graphics for data analysis. Springer‐Verlag, New York, New York¸USA. [Google Scholar]
- Wickham, H. 2011. The split‐apply‐combine strategy for data analysis. Journal of Statistical Software 40:1–29. [Google Scholar]
- Wickham, H. 2018. Forcats: Tools for working with categorical variables (factors). https://CRAN.Rproject.org/package=forcats
- World Health Assembly . 2012. Global burden of mental disorders and the need for a comprehensive, coordinated response from health and social sectors at the country level: report by the Secretariat. World Health Organization. https://apps.who.int/iris/handle/10665/78898
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1
Data Availability Statement
Data are available on Figshare: https://doi.org/10.6084/m9.figshare.12941729.