

Dear Editor,
We read with interest the article by Kuria et al. titled, “Bone scintigraphy imaging of cardiac amyloidosis,”[1] in which scintigraphic findings lend credence to the diagnosis of clinically suspected amyloid transthyretin (ATTR)-related cardiac amyloidosis (CA). Nevertheless, several potential pitfalls should be emphasized in the imaging of ATTR-CA by bone scintigraphy (BS) with technetium-99m (99mTc)-labeled bone-seeking radiopharmaceuticals. The tracer methylene diphosphonate (99mTc-MDP) is not recommended for such imaging due to its low sensitivity for detecting ATTR-CA. In the largest multicenter study involving 1217 patients, BS with 3,3-diphosphono-1,2-propanodicarboxylic acid (99mTc-DPD), pyrophosphate (99mTc-PYP), or hydroxy MDP (99mTc-HMDP) had >99% sensitivity and 86% specificity for detecting ATTR-CA, with false-positive scans in patients with light chain (AL) CA (lowering the overall accuracy to 88.2%–89.8%) [Figure 1].[2] Besides amyloidosis, abnormal diffuse cardiac radiotracer accumulation during BS has been attributed to extensive myocardial infarction, unstable angina pectoris, alcoholic cardiomyopathy, adriamycin-induced cardiotoxicity, pericarditis, pericardial tumors, and hypercalcemia.[3] In addition to uptake in the heart, whole-body BS, especially with 99mTc-DPD or 99mTc-HMDP, enables localization of extracardiac sites of amyloid deposition. However, abnormal soft tissue and/or organ uptake of bone-seeking radiopharmaceuticals can be seen in diseases other than amyloidosis.[3] Moreover, it should also be noted that increased extraskeletal accumulation in the region of the heart and/or other soft tissues is not necessarily pathological. In general, diffusely increased soft tissue uptake on BS (including blood-pool activity and accompanied by diffusely decreased skeletal uptake) is observed in chronic renal failure, osteoporosis, bisphosphonate therapy or infiltrated injection, and to problems with the radiopharmaceuticals per se.[3,4] Indeed, a well-known pitfall of 99mTc-PYP imaging is residual/prolonged cardiac blood-pool activity probably due to its slower blood and soft tissue clearance. Single-photon emission computed tomography imaging should be routinely performed to discern myocardial from extracardiac uptake. Radiochemical impurities in 99mTc-labeled radiopharmaceuticals may also cause persistent activity in the cardiac blood pool. Apparent cardiac retention of bone imaging agents accompanied by visualization of other organs has been described in the setting of altered biodistribution, either related to improper radiopharmaceutical preparation (after the addition of dextrose water instead of normal saline) or to drug-radiopharmaceutical interactions following intravenous iron therapy.[4,5] These conditions may lead to erroneous diagnoses [Figures 2 and 3]. A rather underestimated issue, albeit significant in clinical praxis, is that in many articles published in the literature using radiopharmaceuticals, quality control testing of radiopharmaceuticals is not mentioned. Finally, and perhaps most importantly, the exact mechanism of localization of 99mTc-labeled bone-seeking radiopharmaceuticals in ATTR-CA remains unknown (although it has been theorized to be associated with high calcium content in ATTR amyloid).
Figure 1.
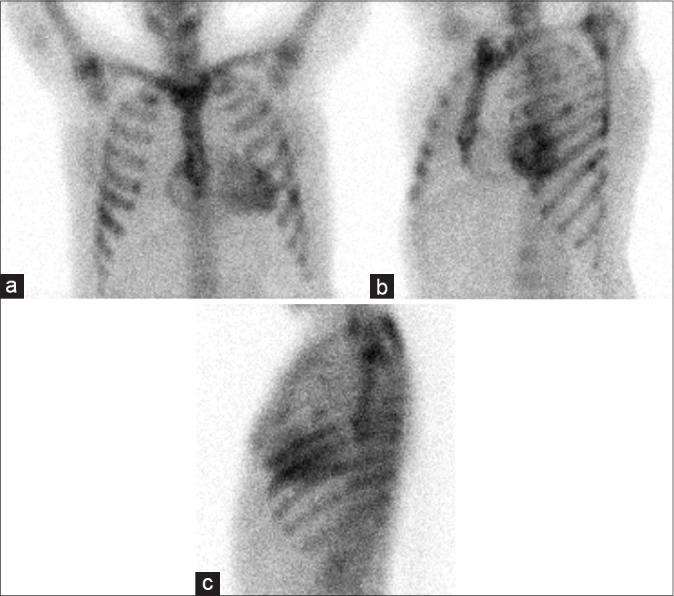
Bone scan performed 3-h after the administration of technetium-99m-hydroxy methylene diphosphonate in a 58-year-old female with systemic/cardiac involvement due to AL amyloidosis associated with multiple myeloma. Moderate diffuse myocardial uptake is seen on anterior (a), left anterior oblique (b), and left lateral (c) planar views of the thorax, presumably due to the high calcium content of amyloid, although this is not common in cardiac amyloidosis-AL. In addition, uptake in the ribs is noted, which was considered to represent bone lesions from multiple myeloma
Figure 2.
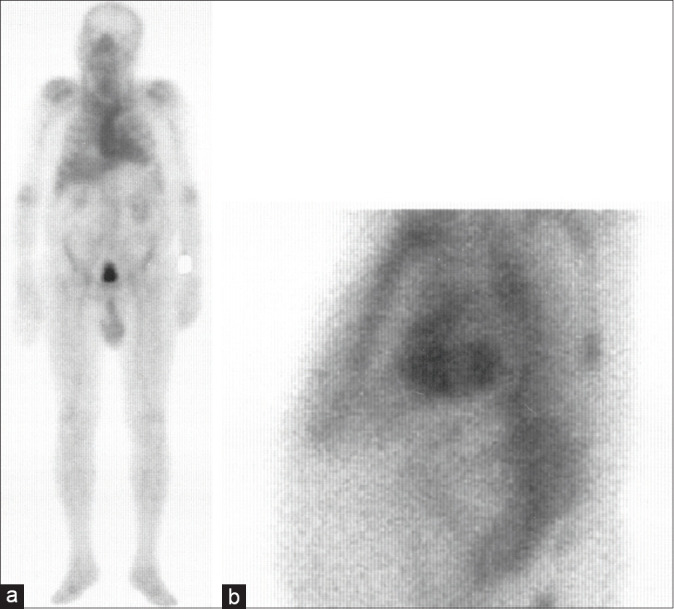
Total-body anterior (a) technetium-99m-hydroxy methylene diphosphonate bone image at 3-h after radiopharmaceutical preparation with dextrose water in an 89-year-old male demonstrates altered distribution with increased uptake in the heart and major blood vessel, liver, and spleen accompanied by decreased bone uptake. The static left lateral image (b) showed cardiac uptake that conformed to the morphology of the left ventricle
Figure 3.

Whole-body anterior view technetium-99m-hydroxy methylene diphosphonate images at 3-h after iv injection in an 82-year-old female who had recently been treated with parenteral iron chelation, shows unexpected findings of significant cardiac, major blood vessel, hepatic, renal, and splenic activity with a reduction in skeletal activity
It is important to emphasize that BS should be used in patients with a high index of suspicion for ATTR-CA, based on clinical data and paraclinical test results; otherwise, the posttest probability may be diluted significantly.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kuria IM, Gitau SN, Makhdomi KB. Bone scintigraphy imaging of cardiac amyloidosis. World J Nucl Med. 2019;18:314–6. doi: 10.4103/wjnm.WJNM_9_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation. 2016;133:2404–12. doi: 10.1161/CIRCULATIONAHA.116.021612. [DOI] [PubMed] [Google Scholar]
- 3.Gnanasegaran G, Cook G, Adamson K, Fogelman I. Patterns, variants, artifacts, and pitfalls in conventional radionuclide bone imaging and SPECT/CT. Semin Nucl Med. 2009;39:380–95. doi: 10.1053/j.semnuclmed.2009.07.003. [DOI] [PubMed] [Google Scholar]
- 4.Vallabhajosula S, Killeen RP, Osborne JR. Altered biodistribution of radiopharmaceuticals: Role of radiochemical/pharmaceutical purity, physiological, and pharmacologic factors. Semin Nucl Med. 2010;40:220–41. doi: 10.1053/j.semnuclmed.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 5.Qutbi M, Shafiei B, Khoshbakht S, Asadi A, Neshandar Asli I. An unexpected and less recognized altered distribution on bone scintigraphy; possibility of99m Tc dextrose complex as a cause. Clin Nucl Med. 2017;42:952–7. doi: 10.1097/RLU.0000000000001857. [DOI] [PubMed] [Google Scholar]