

Summary
Mindfulness and slow eating techniques are commonly recommended to achieve weight loss within behavioural weight management programmes; yet the role of these eating strategies on acute energy intake (EI) and satiety are not clear. This study investigated the effects of mindful and slow eating strategies on acute EI and satiety. Twenty‐four participants were randomized to one of three eating conditions (EAT, MIND, SLOW). For the EAT condition, participants were instructed to eat as they normally would for both test meal sessions. For the SLOW condition, participants were instructed to eat as they normally would for their first test meal session and to slow their eating for the second test meal session. For the MIND condition, participants were instructed to eat as they normally would during their first test meal session and were given brief instructions on mindful eating for their second test meal session. For each condition, participants were provided ad libitum access to a test meal, and EI was calculated based upon food consumed. Participants rated their level of satiety following each meal. There were no significant differences in EI between eating strategy conditions. There was a trend towards a decrease in energy intake in the MIND condition compared with the EAT condition and a prevention of increased intake in the SLOW condition. There were no significant differences in ratings of satiety between conditions. Although, neither mindful nor slow eating strategies significantly decreased acute EI or satiety; the results suggest that both strategies blunted the increase in EI observed in EAT that occurred across two eating episodes, which may suggest that these strategies can be important for modifying eating behaviour that may contribute to body weight regulation. Additional appropriately designed studies investigating these strategies appear warranted to confirm these findings.
Keywords: eating strategies, energy intake, mindfulness, slow eating
Abbreviations
- ANCOVA
analysis of covariance
- ANOVA
analysis of variance
- BMI
body mass index
- EI
energy intake
- MEQ
Mindful Eating Questionnaire
- PANAS
Positive and Negative Affect Scale
- TFEQ
Three Factor Eating Questionnaire
- VAS
Visual Analogue Scale
1. INTRODUCTION
Rates of obesity are increasing in the United States. 1 Many strategies are being implemented across different types of behavioural weight management programmes in an attempt to combat this rise, including reduced eating rate and a practice in mindful eating. Reduced eating rate is a strategy that is frequently used in standard behavioural weight loss interventions. It has been postulated that increased ingestion rate is positively associated with body weight 2 , 3 ; yet one prospective trial found that faster eating or a change in eating speed was not associated with increased risk for obesity at 3 years. 4 Strategies to reduce eating speed have included decreasing bite size, 3 , 5 , 6 , 7 , 8 utilizing smaller utensils, 5 increasing chewing frequency, 5 or creating within meal pauses by taking sips of water or putting utensils down between bites. 3 , 5 , 8 However, evidence regarding the effect of slower eating rate on energy intake is varied in that some studies suggest an associated with a decrease in caloric intake, 5 , 8 whereas others show either no effect 6 , 7 , 9 , 10 or an increase in intake. 11 , 12
Mindfulness is an approach that has been implemented in behavioural interventions for weight management and eating behaviour. 13 , 14 It is often incorporated as part of acceptance‐based behavioural treatments where the focus is acceptance of negative experiences and promotion of behaviours aligning with goals rather than total the avoidance of negative experiences that is often the emphasis in standard behavioural weight management programmes. 15 Mindful eating has been defined as “the nonjudgmental awareness of physical and emotional sensations while eating or in a food‐related environment.” 16 Mindfulness‐based eating interventions employ the basic principles that involve awareness to internal cues (i.e., hunger and satiety) to avoid overconsumption and utilizing external cues (reducing portion sizes and distractions while eating, and eating slowly) to assist in achieving awareness. 16 Mindfulness‐based interventions have been shown to reduce energy intake, 17 change obesity‐related eating behaviours, 18 and result in decreased weight. 19
Few studies have attempted to examine the effect of strategies to reduce eating rate and prompt mindful eating on acute energy intake. Thus, the current study compared strategies to reduce eating rate and elicit mindful eating to a control condition to examine the effects on acute energy intake and subjective ratings of satiety. We hypothesized that energy intake would be lower and perceived satiety would be greater when comparing both of these strategies to the control condition.
2. MATERIALS AND METHODS
2.1. Participants
This study recruited 24 participants. Eligibility criteria included age of 18–55 years, a BMI between 18.5 and <40.0 kg/m2, and ability to provide informed consent. Participants were excluded from the study for the following reasons: (1) currently pregnant and/or lactating or pregnant and/or lactating during the previous 6 months; (2) current diagnosis of an eating disorder or current treatment for other psychological issues, taking psychotropic medications, or having received treatment with psychotropic medications within the previous 6 months; (3) current diagnosis of any medical condition that may alter metabolism (i.e., thyroid disease) and/or current use of medications that could affect weight or eating patterns (i.e. synthroid); (4) reporting irregular menstrual cycles (<25 days or >35 days between cycles); (5) previous or current mindfulness practice (>1 day of meditation per week over the past month); (6) self‐report of current slow rate of eating (self‐report of “very slow” usual eating rate compared to other people); (7) allergy to any food ingredient included in the preload and condition meals (i.e., dairy and gluten); (8) dislike of any food included in the preload and condition meals (i.e., macaroni and cheese and meal replacement shakes); (9) currently trying to lose or gain weight; and (10) history of bariatric surgery.
Recruitment efforts attempted to identify an equal number of participants by both sex and obesity status (BMI < 30.0 kg/m2 or BMI ≥ 30.0 kg/m2). Individuals deemed to be potentially eligible based on initial screening attended an orientation visit to obtain informed consent and to complete additional baseline assessments to confirm eligibility. The Institutional Review Board at the University of Pittsburgh approved all study procedures.
2.2. Experimental design
This study implemented a randomized experimental design with participants engaging in two acute eating episodes that were separated by at least 2 days but no more than 4 days. Visits were conducted between days 7 and 21 of a female participant's menstrual cycle in order to minimize the effect of hormone concentrations on satiety outcome measures. Random assignment, with stratification by sex and obesity status, was to one of the three experimental conditions with all participants being exposed to the control condition for the first experimental session and the control condition, slow eating strategies, or mindful strategies for the second experimental session. Participants followed the study protocol depicted in Figure 1, and specific protocols for each conditioned are described below.
FIGURE 1.
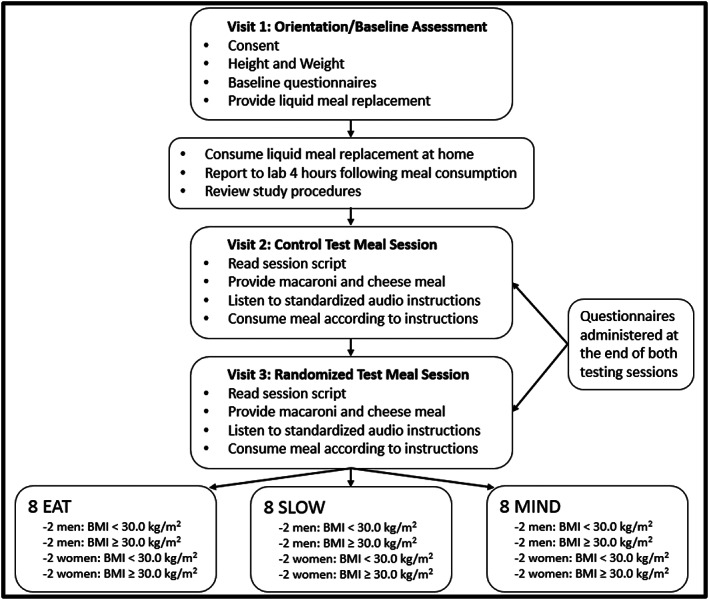
Consort diagram
Described below is the first eating episode that is control eating strategy condition (EAT); whereas for the second experimental session (Visit 3), the participant was randomized to follow the protocol for EAT, the slow eating strategy condition (SLOW), or the mindful eating strategy condition (MIND). A number of designs were considered, and the rationale for this design includes the following:
The use of the EAT condition for the first experimental condition was included to allow participants to acclimate to the laboratory environment for an eating episode prior to the second experimental session to minimize the potential impact of only having one eating episode occur in the laboratory, which could have also impacted the results.
The use of EAT also allowed us to compare the effect of each eating episode that occurred in the second eating episode to the same control rather than just comparing EAT, SLOW, and MIND cross‐sectionally.
A counter‐balanced design was also considered. However, it was decided to use EAT as the first eating episode rather than allowing SLOW or MIND to be used as the first eating episode followed by EAT for some participants. This decision was made so that SLOW and MIND would not influence EAT, which served as the control, when EAT may have occurred as the second eating episode.
The ordering of test meal sessions in the study allowed us to see not only differences among the EAT, MIND, and SLOW groups, but also if the conditions actually impacted the way participants ate. We attempted to control for this threat through randomization of what condition would occur at the second test meal session; thus, any repeat testing effects would be similar among conditions.
2.3. Procedure
2.3.1. Orientation/baseline assessment visit (Visit 1)
During screening, participants underwent assessment of height (measured to the nearest 0.1 cm using a wall mounted stadiometer) and weight (measured to the nearest 0.1 kg using a digital scale) and completed questionnaires to confirm other eligibility criteria and to obtain demographic information. To further characterize participants by levels of dietary restraint, as this construct has the potential to impact some aspects of eating behaviour, 6 , 20 each individual also completed the Three‐Factor Eating Questionnaire (TFEQ). 21
After the completion of the assessment visit, in order to standardize energy intake and volume prior to each test meal session, participants were provided with a liquid meal replacement shake. Participants were instructed to consume this as their only food in the morning of their test meal sessions. The macronutrient composition of this meal replacement was 350 calories, 28% fat, 57% carbohydrate, and 15% protein. Participants were given the following pretesting guidelines: (1) consume the liquid meal replacement 4 h prior to their scheduled testing time, (2) abstain from all other food or beverages, with the exception of water, on the morning of the testing session, and (3) abstain from structured moderate‐to‐vigorous intensity physical activity, alcohol, and caffeine for 12 h prior to their visit.
2.3.2. Experimental sessions (Visits 2 and 3)
Participants reported to the research centre on the morning of their experimental sessions and adherence to the pretesting guidelines (see above) were verified. If a participant did not adhere to the guidelines, he/she was rescheduled for another date. The participant was escorted to a small, private room and was seated alone, with all personal items placed in a locked drawer. Procedures were reviewed with the participant, and a member of the study staff reads a standardized script with information and instructions regarding the experimental condition that was being implemented during that study visit. The first experimental session (Visit 2) involved all participants following the protocol described below for the EAT; whereas for the second experimental session (Visit 3), the participant was randomized to follow the protocol for either EAT, SLOW, or MIND. The specific details of these conditions are described below.
2.3.3. EAT experimental condition
This condition involved participants listening to a standardized audio recording that contained information for the test meal including instructions to eat until “comfortably full” and to consume water ad libitum during the session. In addition, a neutral, non‐eating–related audio passage on the national park system was played for the first experimental session, and if randomized to EAT for the second experimental session, the neutral, non‐eating–related passage was about tiny vacation homes.
2.3.4. SLOW experimental condition
The SLOW experimental condition consisted of participation in slow eating strategies during the test meal. A standardized audio recording instructed participants to eat until they are “comfortably full” and to consume water ad libitum during the session. The recording also contained information for the test meal including instructions to put their fork down in between bites, chew each bite at least 15–30 times, and swallow completely before picking up their fork for the next bite.
2.3.5. MIND experimental condition
The MIND experimental condition consisted of participation in mindful eating strategies during the test meal. The standardized audio recording instructed participants to eat until they are “comfortably full” and to use the provided water to cleanse their palate between bites. The recording also contained instructions on how to consume the meal mindfully, including taking deep breaths, staying aware of and rating their hunger, and savouring the meal by focusing on the taste, smell, texture, and colour of the food.
2.3.6. Food used for the test meal
To standardize meals across time and between groups and to ensure participants could eat until “comfortably full,” preportioned, packaged, family‐size microwavable macaroni and cheese portions were served. This family‐sized commercially available macaroni and cheese food contained 1550 calories with a macronutrient composition of 46% fat, 36% carbohydrate, and 17% protein. Test meals were prepared via microwave according to package instructions. After each experimental condition, the amount of food consumed was measured to determine energy intake and the amount of water consumed was quantified. In an effort to mask participants to the primary outcome (energy intake during each test meal), meal satisfaction and enjoyment were assessed on a visual analogue scale following each experimental condition.
2.3.7. Assessing compliance to experimental procedures
All experimental sessions were video recorded for later review using a hidden camera. The video was reviewed to confirm the duration of the eating session and that no situations occurred during the experimental session that would deem any of the data to be considered invalid (e.g., disposing of food or water other than through consuming it). The video recording was also used to confirm adherence to the slow eating strategy for those in the SLOW condition. Adherence in the SLOW condition was a priori defined as engaging in the prescribed strategies for ≥80% of the session.
Following the second experimental session, all participants completed the Mindful Eating Questionnaire (MEQ). 22 This questionnaire was used to assess whether there were differences in mindful eating between the three experimental conditions (EAT, SLOW, and MIND) and whether participants in MIND were engaging in mindful eating. A MEQ score of ≥2.5 was defined a priori as a threshold for defining engagement in mindful eating.
2.3.8. Affect, hunger, and satiety
To assess the impact of other factors that have been suggested to influence energy intake, such as emotional stress and changes in psychological factors, 20 the Positive and Negative Affect Scale (PANAS) 23 was utilized as a process measure both prior to and following the eating session during each experimental visit. Specifically, to investigate the potential effects of eating in a laboratory setting on psychological factors across groups, alertness and attentiveness scores from the PANAS were measured. After completion of each test meal session, the participant also reported their hunger and satiety using visual analogue scales (VAS).
2.4. Statistical analysis
A power analysis was performed using G*Power version 3.1.9.2 (Faul, Erdfelder, Lang & Buchner, Universität Kiel, Germany) to estimate the sample size needed to detect a meaningful difference in energy intake between the experimental conditions. A clinically meaningful difference in energy intake between the experimental conditions was defined as 65 kcal, and a standard deviation of 155 kcal that was reported in a prior study of eating rates. The work published by Andrade et al 9 was used to inform the sample size estimate for this current study, with the prior work reporting a standard deviation of 155 kcal and a sample size of 30 to investigate the effects of eating slowing on energy intake and appetite. Thus, using a standard deviation of 155 kcal between eating conditions, the current study assumed that that 65 kcal would be a clinically meaningful difference in energy intake between the experimental conditions, which would result in an effect size of 0.42. Assuming α of 0.05, statistical power of at least 80%, a plausible correlation between repeated measures (r = 0.50), and sphericity (ε = 1.0), it was estimated that eight participants per condition (N = 24 total) would be required for this study.
Data were examined for normality and homogeneity of variance. Data that were not normally distributed were transformed or analysed using nonparametric methods. All statistical analyses were performed using SPSS for Windows (SPSS Inc., Chicago, IL) with statistical significance defined at p < 0.05.
One‐way analysis of variance (ANOVA) was used to examine demographic characteristics between participants randomized to each of the experimental conditions. Energy intake during the test meals was analysed using 3 × 2 repeated measures ANOVA (condition × time). When appropriate, post hoc analysis with Bonferroni adjustment for multiple comparisons was performed to further probe difference between the experimental conditions. Similar analyses were performed to assess satiety and eating duration. Pearson or Spearman correlations or ANOVAs were used to examine which descriptive variables should be considered as covariates. If a significant correlation was detected between any of the selected demographic variables and energy intake or satiety, then that variable was included as a covariate in the analysis. If the interpretation of the findings changed when the covariate was included, then those findings are reported.
3. RESULTS
3.1. Participant characteristics
Characteristics for the total sample of participants and for participants randomized to each of the experimental condition are shown in Table 1. There were no significant differences between groups for age, BMI, sex, race, ethnicity, education, and measures of dietary restraint. By design, an equal number of males and females were randomized into each condition (Figure 1). Participants were not equally distributed among BMI classifications with 10 participants classified as normal weight (BMI: 18.5 to <25.0 kg/m2), two participants classified as overweight (BMI: 25.0 to <30.0 kg/m2), three participants classified as Class I obese (BMI: 30.0 to <35.0 kg/m2), and nine participants classified as Class II obese (BMI: 35.0 to <40.0 kg/m2).
TABLE 1.
Baseline characteristics of participants
| All Groups (n = 24) | EAT (n = 8) | MIND (n = 8) | SLOW (n = 8) | p Value a | |
|---|---|---|---|---|---|
| Age, y b | 24.0 (21.0, 31.8) [20.0–54.0] | 24.0 (21.0, 31.3) [20.0–44.0] | 28.0 (22.0, 33.5) [21.0–54.0] | 21.5 (21.0, 24.8) [21.0–33.0] | 0.292 |
| BMI, kg/m 2 b | 29.1 (24.3, 36.7) [21.0–39.3] | 31.7 (25.2, 37.2) [22.0–37.3] | 29.1 (24.4, 35.7) [22.3–39.2] | 27.4 (23.5, 38.2) [21.0–39.3] | 0.906 |
| Sex c | |||||
| Male | 12 (50.0%) | 4 (50.0%) | 4 (50.0%) | 4 (50.0%) | 1.00 |
| Female | 12 (50.0%) | 4 (50.0%) | 4 (50.0%) | 4 (50.0%) | |
| Race c | |||||
| Asian | 4 (16.7%) | 1 (12.5%) | 1 (12.5%) | 2 (25.0%) | 0.828 |
| Black | 4 (16.7%) | 1 (12.5%) | 2 (25.0%) | 1 (12.5%) | |
| White | 16 (66.7%) | 6 (75.0%) | 5 (62.5%) | 5 (62.5%) | |
| Ethnicity c | |||||
| Hispanic | 1 (4.2%) | 0 (0%) | 0 (0%) | 1 (12.5%) | 0.385 |
| Non‐Hispanic | 23 (95.8%) | 8 (100%) | 8 (100%) | 7 (87.5%) | |
| Education c | |||||
| Some high school | 1 (4.2%) | 1 (12.5%) | 0 (0%) | 0 (0%) | 0.108 |
| High School graduate or GED | 3 (12.5%) | 2 (25.0%) | 0 (0%) | 1 (12.5%) | |
| Some college or Associate Degree | 8 (33.3%) | 2 (25.0%) | 2 (25.0%) | 4 (50.0%) | |
| College graduate or Baccalaureate Degree | 9 (37.5%) | 2 (25.0%) | 4 (50.0%) | 3 (37.5%) | |
| Masters or Doctoral Degree | 3 (12.5%) | 1 (12.5%) | 2 (25.0%) | 0 (0%) | |
| Cognitive restraint construct d | 8.3 ± 4.1 | 6.5 ± 4.7 | 8.4 ± 4.3 | 10.1 ± 2.9 | 0.222 |
| Disinhibition construct d | 5.5 ± 2.7 | 5.3 ± 3.1 | 5.9 ± 2.5 | 5.3 ± 2.8 | 0.877 |
| Hunger construct d | 5.6 ± 3.0 | 5.8 ± 2.9 | 6.0 ± 3.2 | 5.0 ± 3.2 | 0.800 |
p value for comparison between EAT, MIND, and SLOW.
Data presented as median (25th and 75th percentiles) (range).
Data presented as n (percentile).
Data presented as mean ± standard deviation.
3.2. Correlations between primary endpoints and descriptive variables
Additional analyses showed that BMI, age, education, dietary disinhibition, and cognitive dietary restraint measured at baseline were not significantly correlated with differences in energy intake or satiety at either test meal session. The hunger construct was found to be significantly correlated with satiety following the first test meal session (r = 0.525, p = 0.008) but did not change the interpretation of the findings. Therefore, these variables were not included as covariates in the final analysis.
3.3. Effect of condition on study outcomes
3.3.1. Process measures
The MEQ score following the second experimental session was compared between the EAT, MIND, and SLOW conditions, and there was no difference between these conditions (p = 0.692), indicating that MIND did not report eating more mindfully than either SLOW or EAT. Review of the video recordings showed that all participants in SLOW met the criteria of compliance to engaging in slow eating strategies ≥80% of the session, and in fact, participants were 100% compliant to engaging in the slow eating strategies.
To examine if general awareness increased across eating strategy conditions and over time (between experimental sessions), a repeated measures ANOVA was performed using change in alertness and attentiveness scores as measured by the PANAS. Alertness and attentiveness did not change over time (alertness p = 0.112, attentiveness p = 0.279). There was no significant difference in change in alertness or change in attentiveness among eating strategy conditions (alertness p = 0.616, attentiveness p = 0.450).
3.3.2. Meal duration
Meal duration was transformed using the natural log due to nonnormal distribution (data presented in Figure 2 have been back transformed to aid in interpretation). There was a significant session effect (p = .004) with the meal during the second experimental session being of longer duration when compared to the first experimental session. There was also a significant condition × time interaction effect (p = 0.019). Post hoc analysis indicated that meal duration was significantly longer during the second experimental session in SLOW (median = 12.3 [25th and 75th percentiles: 10.7, 18.7] min) compared to EAT (8.1 [6.5, 9.6] min) (p = 0.005) but not compared to MIND (11.2 [8.3, 17.7] min) condition (p = 0.548).
FIGURE 2.
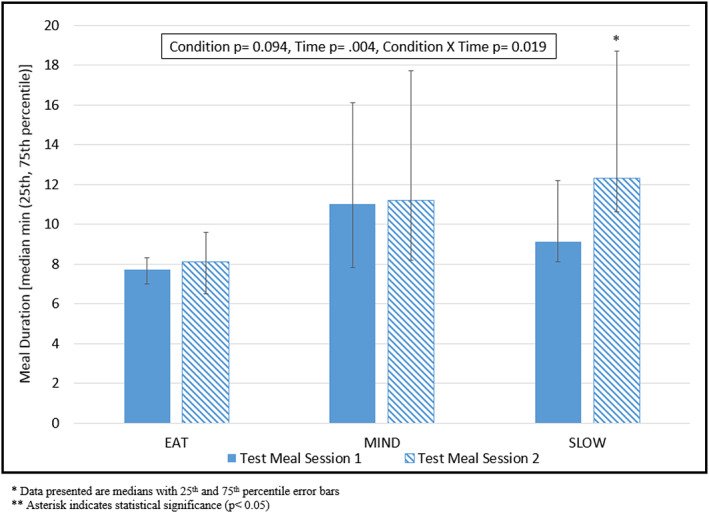
Condition differences in meal duration (min) between test meal sessions
3.3.3. Energy intake
Energy intake at the first experimental session was significantly different between Black and White participants, with White participants having a higher energy intake (p = 0.019). When race considered as a covariate the pattern of the results for the ANOVA and ANCOVA did not differ, and therefore, the results of the ANOVA are presented. There were no significant differences in energy intake across eating strategy conditions at either of the experimental sessions (see Figure 3). There was a nonsignificant decrease in energy intake from the first to the second experimental session in MIND (−64.4 ± 178.4 kcals), with nonsignificant increases in energy intake from the first to the second experimental session in SLOW (2.6 ± 107.9 kcals) and EAT (98.3 ± 169.6 kcals).
FIGURE 3.
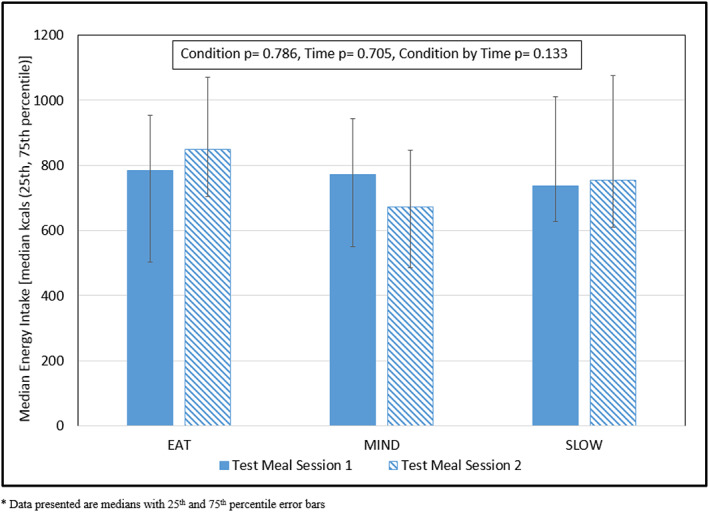
Condition differences in energy intake (kcals) between test meal sessions
3.3.4. Satiety
There were no significant differences in subjective ratings of satiety (via VAS) between the conditions (EAT, MIND, and SLOW) (p = 0.258) (see Table S1). Results were similar when baseline hunger was included in an ANCOVA model (data not shown). However, there was a significant main effect of time on subjective ratings of hunger (via VAS) following the test meal between the first and second test meal sessions (p < 0.001) with the second test meal session resulting in decreased ratings of hunger compared with the first test meal session (see Table S2).
4. DISCUSSION
Results from this investigation revealed that there were no significant differences in acute energy intake or satiety when participants were instructed to engage in strategies intended to slow their eating rate (SLOW) or to eat mindfully (MIND) compared with a no‐strategy control group (EAT). Participants in the MIND condition consumed 64 fewer calories when engaging in mindful eating compared to eating ad libitum until experiencing the feeling of fullness; however, this difference in energy intake was not statistically significant. Moreover, although SLOW resulted in a slower rate of eating compared to EAT, this also did not result in a difference in acute energy intake or satiety. Thus, these findings result in the rejection of the hypothesis that acute energy intake would be lower and satiety would be greater in both MIND and SLOW compared to EAT in this study.
Although there were no differences between MIND and SLOW compared to EAT for energy intake or satiety, SLOW resulted in longer eating duration (median = 12.3 min) compared to EAT (median = 8.1 min), but MIND (median = 11.2 min) did not differ from either SLOW or EAT. The reason that this increase in eating duration for SLOW did not result in differences in energy intake or satiety compared to EAT may be due to not achieving a meal duration of 20 min, which has been shown to be the duration needed to influence satiety. 24 , 25 , 26 , 27 Although previous research has shown differences in energy intake 5 and satiety 5 , 9 , 28 between slow and quick eating conditions, in the current study, EAT was instructed to eat at their normal pace and was not instructed to specifically eat at a quick pace.
Factors known to impact energy intake and satiety beyond that of eating rate may also explain the results observed in this study. For example, the current investigation utilized a brief mindful eating practice that included a short breathing meditation, rating of physiological hunger, and instruction to focus on the sensory experience of eating. This approach, however, did not involve chronic training in mindfulness practice, and participants in MIND did not report that they were engaging in more mindful eating in their second experimental session compared to their first experimental session. The brevity of the mindfulness training may have minimized the impact that this strategy had on energy intake and satiety in MIND. Therefore, future studies may need to consider how chronic training in mindfulness practice influences acute energy intake and satiety.
Another factor that may have influenced the results observed was the large portion size of food that was presented to participants during the eating episodes during their experimental sessions. This hypothesis is consistent with prior studies that have reported that food portion size may influence the effect of mindfulness on both energy intake and satiety. 29 , 30 , 31 Therefore, future studies may need to examine how varying portion sizes influence the effect that mindfulness practice has on acute energy intake and satiety.
This study included aspects that may be perceived as strengths that include the presence of a control condition, participants with a broad range of BMI and age, inclusion of both sexes and of different race/ethnicity, a controlled breakfast meal, and a repeated measures design. There are, however, limitations of this study that should be considered. One limitation of this study is that we were not powered to detect between‐condition differences in effect size of <0.42 (i.e., <65 kcal). Thus, although our null conclusion is supported for this small‐moderate effect size, we are unable to draw conclusions about smaller effects which could be clinically meaningful. Moreover, the sample size estimate does not allow for comparisons across other demographic characteristics. Thus, the data from this study should be used to further inform the sample size estimates for future studies of this type. Additional limitations may include the use of subjective measures of hunger and satiety, eating examined within controlled laboratory setting, effect of repeat testing during the second test meal session, and lack of variety in the foods available during the acute experimental sessions. These factors should be considered in the design of future studies examining how various eating strategies influence acute energy intake and satiety.
As indicated above, although not statistically significant, the MIND condition did result in a median of 64 kcal less in the second experimental session compared to the first experimental session. There is the potential for this relatively small but lower energy intake of 64 kcal, resulting from mindful eating to contribute to a clinically meaningful influence on chronic energy intake. For example, it has been suggested that as little as 100 kcal less per day may be sufficient to prevent chronic weight gain. 32 Average weight gain in American adults is suggested to be approximately 0.5–0.8 kg/year. 33 A 64 kcal decrease in each meal throughout the day could result in a daily decrease of over 180 kcal and weekly decrease of over 1200 kcal. Over time, this decrease could be meaningful at both the individual and population levels for preventing annual weight gain and slowing increasing rates of obesity, particularly when combined with other positive health behaviours. 34
The finding that the EAT condition resulted in a nonsignificant increase of 98 kcal could be the result of repeat testing effects. It is possible that participants became more comfortable with the laboratory‐based testing during the second test meal session. However, randomization of participants during the second test meal session would mitigate this potential threat to external validity. In the SLOW condition, although no decrease in energy intake was realized, eating slowly did seem to have a protective effect against an increase in energy intake in that participants in the SLOW condition ate approximately the same number of calories at each session. Because SLOW did not result in increased intake, it may be a potentially useful strategy for weight management.
This was a tightly controlled laboratory‐based investigation into the impact of two eating strategies on acute energy intake and satiety. Due to the laboratory‐based setting, the results of this study, statistically significant or not, are limited in generalizability to a natural eating setting. Social interaction, environment, portion size, and food selection, among others, are all factors that affect energy intake. 35 , 36 Accounting for the small sample size of this investigation, it is possible that a statistically significant decrease in energy intake from either strategy may be realized in a larger sample. Therefore, future studies investigating the effectiveness of these strategies should consider implementing an assortment of variations including a larger sample size, variable designs, variety of food choice, specific meal duration to be achieved, or longer duration of mindful eating training.
AUTHOR CONTRIBUTIONS
A.P.S., K.K.D., and J.M.J. conceived experiments and were involved in study design. A.P.S. and K.K.D. carried out data collection. A.P.S. and B.B.G. completed data analysis. A.P.S., K.K.D., J.M.J., and E.M.V. were involved with data interpretation. All authors were involved in writing the paper and had final approval of the submitted and published versions.
CONFLICT OF INTEREST
Dr Jakicic discloses that he is a member of the Scientific Advisory Board for WW (formerly Weight Watchers International, Inc.). The other authors have no conflicts of interest to disclose.
Supporting information
Table S1. Condition differences in energy served between test meal sessions
Table S2. Condition differences in energy intake between test meal sessions
Table S3. Condition differences in meal duration between test meal sessions
Table S4. Condition differences in subjective ratings of hunger between test meal sessions
Table S5. Condition differences in subjective ratings of satiety between test meal sessions
Table S6. Difference in energy intake between test meal sessions by subject and condition
Figure S1. Mean difference* in energy intake between test meal sessions among subjects
ACKNOWLEDGEMENTS
The investigators of this project would like to acknowledge the commitment of the staff and students at the Physical Activity and Weight Management Research Center.
This research was supported by the University of Pittsburgh School of Education and the University of Pittsburgh Council of Graduate Students in Education. These funding sources had no involvement in the study design, collection, analysis, and interpretation of the data, writing of the report, or decision to submit the article for publication.
Simonson AP, Davis KK, Barone Gibbs B, Venditti EM, Jakicic JM. Comparison of mindful and slow eating strategies on acute energy intake. Obes Sci Pract. 2020;6:668–676. 10.1002/osp4.441
REFERENCES
- 1. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity and Severe Obesity Among Adults. USA: U.S. Department of Health and Human Resources, Centers for Disease Control and Prevention, National Center for Health Statistics; 2020:2017‐2018. [Google Scholar]
- 2. Ohkuma T, Hirakawa Y, Nakamura U, Kiyohara Y, Kitazono T, Ninomiya T. Association between eating rate and obesity: a systematic review and meta‐analysis. Int J Obes (Lond). 2015;39:1589‐1596. [DOI] [PubMed] [Google Scholar]
- 3. Spiegel TA, Wadden TA, Foster GD. Objective measurement of eating rate during behavioral treatment of obesity. Behav Ther. 1992;22:61‐67. [Google Scholar]
- 4. Leong SL, Gray A, Horwath CC. Speed of eating and 3‐year BMI change: a nationwide prospective study of mid‐age women. Public Health Nutr. 2015;1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Andrade AM, Greene GW, Melanson KJ. Eating slowly led to decreases in energy intake within meals in healthy women. J am Diet Assoc. 2008;108:1186‐1191. [DOI] [PubMed] [Google Scholar]
- 6. Privitera GJ, Cooper KC, Cosco AR. The influence of eating rate on satiety and intake among participants exhibiting high dietary restraint. Food Nutr Res. 2012;56(1):10202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ferriday D, Bosworth ML, Lai S, et al. Effects of eating rate on satiety: a role for episodic memory? Physiol Behav. 2015;152:389‐396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Almiron‐Roig E, Tsiountsioura M, Lewis HB, Wu J, Solis‐Trapala I, Jebb SA. Large portion sizes increase bite size and eating rate in overweight women. Physiol Behav. 2015;139:297‐302. [DOI] [PubMed] [Google Scholar]
- 9. Andrade AM, Kresge DL, Teixeira PJ, Baptista F, Melanson KJ. Does eating slowly influence appetite and energy intake when water intake is controlled? Int J Behav Nutr Phys Act. 2012;9:135‐135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Martin CK, Anton SD, Walden H, Arnett C, Greenway FL, Williamson DA. Slower eating rate reduces the food intake of men, but not women: implications for behavioral weight control. Behav Res Ther. 2007;45:2349‐2359. [DOI] [PubMed] [Google Scholar]
- 11. Yeomans MR, Gray RW, Mitchell CJ, True S. Independent effects of palatability and within‐meal pauses on intake and appetite ratings in human volunteers. Appetite. 1997;29:61‐76. [DOI] [PubMed] [Google Scholar]
- 12. McCrickerd K, Forde CG. Consistency of eating rate, oral processing behaviours and energy intake across meals. Nutrients. 2017;9:891–902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Hepworth NS. A mindful eating group as an adjunct to individual treatment for eating disorders: a pilot study. Eat Disord. 2010;19:6‐16. [DOI] [PubMed] [Google Scholar]
- 14. Kristeller JL, Hallett CB. An exploratory study of a meditation‐based intervention for binge eating disorder. J Health Psychol. 1999;4:357‐363. [DOI] [PubMed] [Google Scholar]
- 15. Forman EM, Butryn ML, Juarascio AS, et al. The mind your health project: a randomized controlled trial of an innovative behavioral treatment for obesity. Obesity. 2013;21:1119‐1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Monroe JT. Mindful eating principles and practice. American Journal of Lifestyle Medicine. 2015;217–220, 1559827615569682. [Google Scholar]
- 17. Dalen J, Smith BW, Shelley BM, Sloan AL, Leahigh L, Begay D. Pilot study: mindful eating and living (MEAL): weight, eating behavior, and psychological outcomes associated with a mindfulness‐based intervention for people with obesity. Complement Ther Med. 2010;18:260‐264. [DOI] [PubMed] [Google Scholar]
- 18. Timmerman GM, Brown A. The effect of a mindful restaurant eating intervention on weight management in women. J Nutr Educ Behav. 2012;44:22‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. O'Reilly G, Cook L, Spruijt‐Metz D, Black D. Mindfulness‐based interventions for obesity‐related eating behaviours: a literature review. Obes Rev. 2014;15:453‐461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Benelam B. Satiation, satiety and their effects on eating behaviour. Nutrition Bulletin. 2009;34:126‐173. [Google Scholar]
- 21. Rahula W. What the Buddha Taught. New York: Grove Weidenfeld; 1959. [Google Scholar]
- 22. Framson C, Kristal AR, Schenk JM, Littman AJ, Zeliadt S, Benitez D. Development and validation of the mindful eating questionnaire. J am Diet Assoc. 2009;109:1439‐1444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ostafin BD, Robinson MD, Meier BP. Handbook of Mindfulness and Self‐Regulation. New York City, NY: Springer; 2015. [Google Scholar]
- 24. Rolls BJ. Sensory‐specific satiety. Nutr Rev. 1986;44:93‐101. [DOI] [PubMed] [Google Scholar]
- 25. Liddle RA, Goldfine ID, Rosen MS, Taplitz R, Williams J. Cholecystokinin bioactivity in human plasma. Molecular forms, responses to feeding, and relationship to gallbladder contraction. Journal of Clinical Investigation. 1985;75:1144–1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Moran TH, Kinzig KP. Gastrointestinal satiety signals II. Cholecystokinin. American Journal of Physiology‐Gastrointestinal and Liver Physiology. 2004;286:G183‐G188. [DOI] [PubMed] [Google Scholar]
- 27. Cummings DE, Overduin J. Gastrointestinal regulation of food intake. J Clin Investig. 2007;117:13‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Koidis F, Brunger L, Gibbs M, Hampton S. The effect of eating rate on satiety in healthy and overweight people—a pilot study. e‐SPEN Journal. 2014;9:e54‐e58. [Google Scholar]
- 29. Forman EM, Shaw JA, Goldstein SP, et al. Mindful decision making and inhibitory control training as complementary means to decrease snack consumption. Appetite. 2016;103:176‐183. [DOI] [PubMed] [Google Scholar]
- 30. Cavanagh K, Vartanian LR, Herman CP, Polivy J. The effect of portion size on food intake is robust to brief education and mindfulness exercises. J Health Psychol. 2014;19:730‐739. [DOI] [PubMed] [Google Scholar]
- 31. Arch JJ, Brown KW, Goodman RJ, Della Porta MD, Kiken LG, Tillman S. Enjoying food without caloric cost: the impact of brief mindfulness on laboratory eating outcomes. Behav Res Ther. 2016;79:23‐34. [DOI] [PubMed] [Google Scholar]
- 32. Hill JO, Peters JC, Wyatt HR. Using the energy gap to address obesity: a commentary. J am Diet Assoc. 2009;109:1848‐1853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Dutton GR, Kim Y, Jacobs DR Jr, et al. 25‐year weight gain in a racially balanced sample of US adults: the CARDIA study. Obesity. 2016;24:1962‐1968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Jakicic JM, Powell KE, Campbell WW, et al. Physical activity and the prevention of weight gain in adults: a systematic review. Med Sci Sports Exerc. 2019;51:1262‐1269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Kral TV, Rolls BJ. Energy density and portion size: their independent and combined effects on energy intake. Physiol Behav. 2004;82:131‐138. [DOI] [PubMed] [Google Scholar]
- 36. Forde CG. From perception to ingestion; the role of sensory properties in energy selection, eating behaviour and food intake. Food Quality and Preference. 2018;66:171‐177. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Condition differences in energy served between test meal sessions
Table S2. Condition differences in energy intake between test meal sessions
Table S3. Condition differences in meal duration between test meal sessions
Table S4. Condition differences in subjective ratings of hunger between test meal sessions
Table S5. Condition differences in subjective ratings of satiety between test meal sessions
Table S6. Difference in energy intake between test meal sessions by subject and condition
Figure S1. Mean difference* in energy intake between test meal sessions among subjects