

Summary
Reducing sugar‐sweetened beverage (SSB) intake is an important dietary target, especially among socioeconomically disadvantaged ethnic minority adolescents. This review and meta‐analysis evaluated the effectiveness of behavioural interventions aiming to reduce SSB intake in socioeconomically disadvantaged ethnic minority adolescents and examined which behaviour change techniques (BCTs) were most effective. A systematic search was conducted using the PRISMA criteria. Quality assessments were done using the Cochrane criteria. In a narrative synthesis, studies were divided into effective and non‐effective, and relative effectiveness ratios of individual BCTs were calculated. Pooled standardized mean differences (SMDs) and their 95% confidence intervals were estimated with random‐effects models using cluster robust methods. Twenty‐two studies were included in the qualitative synthesis. A meta‐analysis (n = 19) revealed no significant between‐group differences in reduction of SSB intake. Five self‐regulatory BCTs had an effectiveness ratio >50%: feedback, goal‐setting, action planning, self‐monitoring and problem‐solving/barrier identification. The risk of bias assessments were judged to be moderate to high risk for randomized controlled trials (RCTs) studies and low to moderate for pre–post studies. There was no indication of publication bias. In conclusion, self‐regulatory BCTs may be effective components to change SSB behaviour. However, high‐quality research is needed to evaluate the effectiveness of behavioural interventions and identify BCTs effective for reducing SSB intake among disadvantaged adolescents with ethnic minority backgrounds.
Keywords: behavior change interventions, health inequalities, obesity, sugar‐sweetened beverages
1. INTRODUCTION
Adolescent overweight and obesity is a major public health priority because of its link to adverse short‐ and long‐term outcomes. 1 Compounding the seriousness of the adolescent overweight and obesity trend are stark disparities by ethnic minority status (i.e., residents with immigrant origins), with minority adolescents with low socioeconomic status (SES, e.g., parental education, occupation status or household income) being disproportionately affected by obesity. 2 In developed countries, higher overweight and obesity rates are reported among socioeconomically disadvantaged ethnic minority adolescents than in advantaged ethnic majority adolescents. 3 Given these findings, the increased risk of morbidities during adolescence and adulthood and the anticipated increase in socioeconomic disadvantage and ethnic diversity, effective prevention efforts are warranted to circumvent obesity‐related burden in these adolescents.
Disparities in sugar‐sweetened beverage (SSB) intake, defined as nondiet, non‐alcoholic and non‐dairy cold or warm drink with added sugars including sodas, diet drinks, fruit juices (excluding 100% fruit juice), flavoured juice drinks, sports drinks, energy drinks and sweetened tea and coffee, 4 have been suggested to be a contributing factor to the obesity epidemic. 5 A high intake of SSBs has been shown to be associated with adolescent obesity. 6 While health behaviors such as SSB intake are ultimately based on individual decisions, socio‐ecological models suggest that such behaviors are shaped and influenced by the social and physical contexts. 7 Therefore, it is widely acknowledged that the mechanisms underlying the observed differences in SSB intake are multifactorial, involving a complex web of interacting individual, sociocultural, and environmental factors. 8
Ethnic patterning in SSB intake might be explained by the multiple socioeconomic disadvantages that underserved adolescents face, including growing up in low‐educated households, interacting with peers who encourage obesogenic‐related dietary behaviors and living in segregated deprived areas characterized by a high density of obesogenic food outlets. 9 The inverse relationship between individual, family and area‐level indicators of SES is well established; with disadvantaged adolescents exhibiting poor dietary behaviors than their advantaged ethnic majority peers. 10 These findings are attributed to the fact that these adolescents are less health‐conscious, have limited nutritional knowledge due to individual or parental education level, and lack financial resources, which can restrict food choices. 11
Within the social and physical home environments, parental SSB intake, permissive food‐related parenting styles and home accessibility and availability of SSBs have been linked to a high SSB intake among disadvantaged minority adolescents. 12 Next to the family context, peers can also influence individual SSB intake. Seen from the group norm and socialization perspectives, 13 , 14 peers help to create norms concerning a behavior (e.g., what SSB behaviors are appropriate and socially acceptable). Given their developmental stage, peer influences are influential during middle adolescence (14–16 years of age). 7 Because this developmental stage is marked by a heightened need for peer approval and identity, it is assumed that peers could influence individual SSB intake possibly via negative peer modelling and conformity to pro‐SSB social norms. 7
Underserved adolescents, residing or attending schools located in low‐income, high ethnic minority and socially deprived neighborhoods, are found to have fewer health‐promoting social norms and are often characterized by a high density of obesogenic food environments. 15 , 16 Neighborhood‐level variables such as SSB availability, accessibility, affordability and disproportionate advertising and targeted marketing of SSBs in deprived areas have been linked to higher individual SSB intake and purchasing. 15 , 16 , 17
Because adolescents spend majority of their time in schools, school correlates of SSB intake have also been explored. School food environment and the obesogenic environment around schools in deprived neighborhoods have been shown to influence individual SSB behavior through increased availability, affordability, convenience and in‐store price promotion of SSBs. 15 , 16 , 18
Public health initiatives such as education campaigns, nutrition guidelines and school policies restricting sales of SSBs have been undertaken to reduce SSB intake. 19 Although important, initiatives that rely on educating or informing individuals are often not sufficient enough to engender behavior change, 20 given that humans are not rational and biased when it comes to their behaviors and recognizing the mindless nature of dietary behaviors. 21 Additionally, these initiatives address only one context and are often not theory driven. As a result, they are more likely to lead to intervention‐generated inequalities, 22 because evidence shows that disadvantaged groups with poor literacy skills are less receptive to interventions that rely on educating or informing individuals. 20 , 23 Recently, there has been a growing appreciation for using theory‐driven behavioral interventions defined as a coordinated set of activities designed to change specified behaviour patterns. 24 Theory‐based interventions not only provide a framework for designing interventions but also facilitate an understanding of the underlying mechanisms that drive behavior change. 24 Additionally, they can be used as a guide to identify behaviour change techniques (BCTs) described as the ‘active ingredients of an intervention designed to change behavior’. 25 To date, more than 93 BCTs have been identified. 26
Previous systematic reviews and meta‐analyses of behavioral interventions targeting adolescent SSB intake suggest that although these interventions lead to small reductions in SSB intake, more evidence regarding their effectiveness is needed. 4 , 27 , 28 , 29 Some limitations of existing reviews and meta‐analyses are that they have included adolescents from the general population or have examined the effectiveness of behavioral interventions within specific settings such as preventive eHealth interventions in school settings. 27 Thus far, there has been little research analysing the effectiveness of behavioral interventions and BCTs on reducing SSB intake in disadvantaged minority adolescents. In fact, a systematic review examining the impact of behavioral interventions of different health behaviors concluded that there was a ‘widespread paucity’ of evidence about the effectiveness of changing health behaviors (including dietary behaviors) in underserved groups. In light of these findings, the aims of this systematic review and meta‐analysis were twofold: (a) to review existing behavioral interventions aimed at reducing SSB intake among 12‐ to 18‐year‐old disadvantaged minority adolescents and (b) to identify active BCTs effective in reducing SSB intake.
2. METHODS
2.1. Search methodology, data screening, extraction and methodological assessments
The current systematic review and meta‐analysis is registered in PROSPERO (the International Prospective Register of Systematic Review, registration ID: CRD42018109645) and was conducted according to the PRISMA statement (available upon request). 30 A library specialist performed a systematic search with no date restrictions in MEDLINE (OVID), EMBASE, Web of Science, Cochrane Central Register of Controlled Trials and Google Scholar from inception to July 2018 (available upon request), for randomized controlled trials (RCTs), non‐RCTs, quasi‐experimental, pre–post studies, published in English, of behavioural interventions for reducing SSB intake, measured either subjectively or objectively at baseline and at post‐intervention, in 12‐ to 18‐year‐old disadvantaged ethnic minority adolescents (Table 1).
TABLE 1.
PICO framework for study eligibility
| Parameter | Inclusion criteria |
|---|---|
| Participants | Nonclinical socioeconomicallly disadvantaged ethnic minority adolescents aged 12–18 years. |
| Intervention | Behavioral interventions: |
| ‐ Targeting a reduction in SSB intake as one of the main intervention targets | |
| ‐ Delivered in any setting (e.g., home, school and communities) | |
| ‐ Using behavior change techniques (BCTs) designed to reduce SSB intake | |
| Comparison | Control groups with no intervention (e.g., usual care, active, waitlist) |
| Outcomes | Outcome measure is SSB defined as a non‐diet, non‐alcoholic and non‐dairy cold or warm drink, carbonated or still, with added sugars. Including fruit drinks. Nectars with <100% fruit. Sports and energy drinks, sweetened tea and coffee. 4 |
| Primary outcome measures | |
| ‐ Reduction in SSB consumption quantified as difference between pre‐ and post‐intervention and where possible follow up. Quantity of SSB consumed (ml of SSB consumed per day per week) and frequency of SSB consumed (e.g., percentage of participants consuming a given quantity of SSB), purchases of SSB, energy intake from SSB (e.g., total energy intake in kcal/day or per person) will be included | |
| ‐ Studies using different types of SSBs. the outcomes could be reported separately (e.g., soft drinks and sports drinks) or collectively (i.e., all types of SSBs) | |
| Secondary outcome measures | |
| ‐ Subjective changes in knowledge/attitude/beliefs related to SSB intake | |
| Study design | Randomized controlled trials (RCTs) (e.g., cRCTs). Quasi‐experimental (e.g., with pre–post designs) and one‐group pre–post studies. With baseline. Post‐intervention and where possible. Follow‐up data. |
| Exclusion criteria | |
| The following studies were excluded: | |
| ‐ Animal studies | |
| ‐ Studies conducted in adults | |
| ‐ Studies reporting only baseline data | |
| ‐ Case–control. Cohort. cross‐sectional and longitudinal studies | |
| ‐ Systematic reviews and meta‐analyses (to maintain consistency and because it is difficult to interpret results from previous meta‐analyses pooling estimates from RCTs using different control groups. We decided to exclude them from the current study | |
| ‐ Meetings/congress reports | |
Abbreviation: PICO, participant, intervention, control/comparison and outcomes; RCT, randomized controlled trials; SSB, sugar‐sweetened beverage.
To identify studies missed by the electronic search, one reviewer (S. S.) screened the reference lists of selected studies and of relevant reviews to retrieve studies that met the eligibility criteria. Where information was needed, authors were contacted to provide the missing data. Studies identified through the electronic search were exported to Endnote for removal of duplicates. Both reviewers (S. S. and E. G.), independently screened the abstracts, titles and full texts of retrieved studies. Interrater agreement of record screening and inclusion of studies between reviewers was 98%. Disagreements on eligibility were resolved through discussion. One reviewer (S. S.) extracted data of all included studies using an adapted Cochrane spreadsheet form.
Two reviewers (S. S. and E. G.) assessed the risk of bias of RCTs using the Cochrane risk of bias tool (RoB) 31 in Review Manager (Version 5.3 Cochrane, London, UK). One reviewer (S. S.) assessed the quality of non‐RCTs using the Newcastle–Ottawa Scale (NOS). 32 For the latter risk of bias assessment, a maximum of nine points was allocated for the least risk of bias in three domains: (a) selection of bias (max 4 points); (b) comparability of the study (max 2 points); and (c) ascertainment of exposure and outcomes (3 points). The scores were subsequently categorized as: high (0–3 points), moderate (4–6 points) or low (7–9 points).
2.2. Coding of BCTs
The BCT taxonomy v1 (BCTTv1) 26 was used to extract BCTs. One reviewer (S. S.) completed an online BCT course prior to coding of BCTs. A BCT was only coded if there was clear evidence of inclusion. Interventions targeting multiple behaviors (e.g., physical activity and dietary behaviors) where possible, BCTs related to SSB intake were coded. If this was not possible, only BCTs related to healthy eating were coded. BCTs present in intervention arms were recorded only. Studies using multiple intervention arms, the BCTs were extracted from each active intervention arm.
2.3. Statistical analysis
The primary outcome was a reduction in SSB intake. Due to the variability in the measures used for SSB intake, a hierarchy was developed whereby the most empirically supported method in each study was preferred. Daily SSB servings were prioritized above volumetric measures or SSB consumed in the past month, because the latter would be prone to the wrong estimation and recall bias, respectively. Effect estimates, reported either separately for each type of SSB (e.g., soda and fruit juice) or collectively (all SSB types categorized into one group) were extracted. 33 , 34 , 35 , 36 Only studies that reported SSB intake at pre‐intervention and immediately at post‐intervention were included because most studies did not assess long‐term effectiveness. In studies with multiple intervention arms, each intervention arm was compared with the control arm at each time point. 37
In total, 15 studies reported mean SSB intake, 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 and four studies reported proportions of participants consuming a given quantity of SSBs. 33 , 34 , 50 , 51 Three studies were excluded because the change in SSB intake from baseline was not reported. 52 , 53 , 54 To combine different measures of SSB in one analysis, dichotomous measures were transformed using the Freeman–Tukey double arcsine transformation (i.e., transforming the sampling distribution to a stable normal distribution). 55 Transformed scores were subsequently used to calculate standardized mean differences (SMDs) between groups. For continuous variables, SMDs were calculated from the raw (untransformed) scores. Meta‐analysis was conducted to assess changes in reported SSB intake at pre‐ and at post‐intervention, and any changes in effect estimates from pre‐ to post‐intervention. For continuous SSB outcomes, means, standard deviations (SDs) and sample sizes were extracted for each time point from each group of each study. In cases where other summary statistics were reported (e.g., interquartile range, standard errors and confidence intervals [CIs]), these values were used to compute the missing SDs, as described by the Cochrane guidelines. 56
For each study, the difference in SSB intake at each time point between groups was estimated as the mean difference (mean intervention group at pretest—mean control group at pretest/pooled SD of both groups at pretest). To standardize the effect estimates, computed SMDs were estimated using Hedges' g statistics. 56 SMD effect estimates of 0.3, 0.5 and 0.8 were considered small, medium and large, respectively. 57 Pooled SMDs with their corresponding 95% CIs were estimated using random‐effects models. These models were used because by nature, behavioral interventions are considerable heterogeneous in terms of intervention features. To account for multiple measures per study, a series of multilevel models were investigated with nested random effects top level being the study, then treatment type and time period using REML estimation. Cluster robust meta‐analysis was performed to account for the dependency between multiple measures extracted from the same study. 58
Heterogeneity between studies was assessed using Cochran's Q test and I 2 statistic. 59 A significant Q test (p < 0.05) was suggestive of heterogeneity while I 2 estimates of 50%–75% and >75% were considered substantial to considerable heterogeneity, respectively. 59
Subgroup analyses were not feasible given that a minimum of 10 studies is required for a meaningful interpretation. 59 Instead, exploratory analyses were performed to examine the impact of potential moderators: study design (RCTs, non‐RCTs), intervention type (educational/behavioral, environmental), intervention component (single, multicomponent) and total number of BCTs used. Moderator levels with sample size smaller than two, that is, gender (female or male), use of theoretical framework (yes or no), type of theory used (behavioural or non‐behavioural), setting (school‐based or other), SSB measurement tool (self‐reported or objective) and control group (yes or no) were excluded from the analyses. Intervention duration was excluded as a potential moderator because most of included studies only assessed short‐term effects.
Publication bias was assessed by observation of funnel plots and using Eggers regression asymmetry test. 60 , 61 An asymmetric plot and p < 0.05 were considered to be suggestive of publication bias.
A sensitivity analysis was performed using fixed effects instead of random effects in the main meta‐analysis. All statistical analyses were conducted in R (v3.5.1, Vienna Austria), using the metafor and robust packages.
2.4. Narrative synthesis
Owning to the heterogeneity of BCTs included, a narrative synthesis was performed to identify most commonly used BCTs and types of BCTs associated with intervention effectiveness. Using the approach as Gardner et al., 62 studies were divided into ‘very effective’, ‘quite effective’ and ‘non‐effective’. Interventions were deemed ‘very effective’ and ‘quite effective’ if significant between‐group and within‐group differences in SSB intake were reported, respectively. An intervention was coded as ‘non‐effective’ if no significant within‐ or between‐group differences in SSB intake were reported. In line with other reviews 63 , 64 to identify BCTs associated with effective interventions, a percentage effectiveness ratio was calculated, whereby the number of times a BCT was a component of ‘very effective’ and ‘quite effective’ interventions was divided by the number of times a BCT was a component of all interventions. To avoid inflation of results from BCTs used on a few occasions, BCTs that were identified in a minimum of five studies were included in the analysis. 63 , 64
3. RESULTS
3.1. Study selection and characteristics
A total of 3,098 studies were identified in the initial search of which 1,396 duplicates were removed. After screening the titles and abstracts of 1,706 studies, 45 studies were selected for full‐text screening. At the final stage, 22 studies were included in the qualitative synthesis of which 19 were included in the meta‐analysis 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 (Figure 1). Three studies were excluded from the meta‐analysis because only baseline SSB intake was reported. 52 , 53 , 54
FIGURE 1.
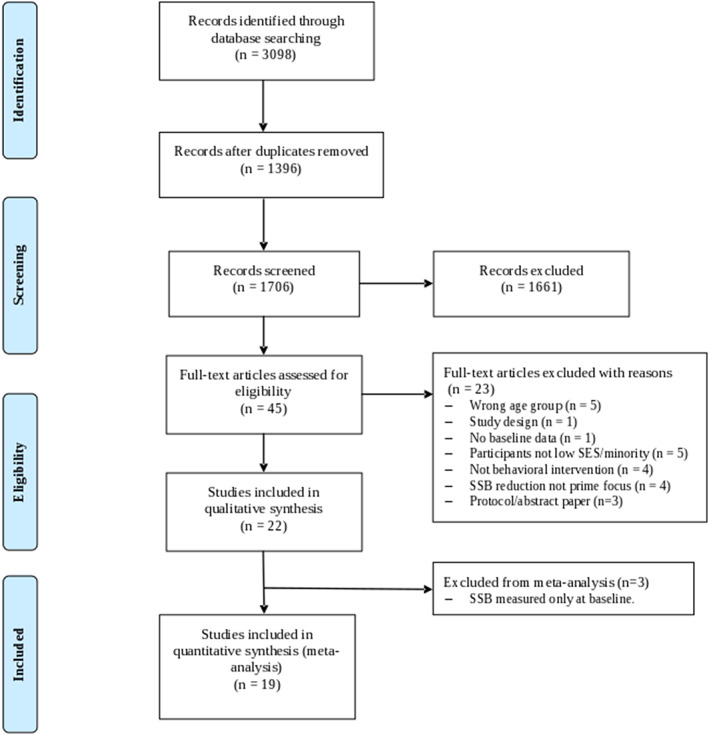
Study flowchart. SSB, sugar‐sweetened beverage
The characteristics of the included studies are summarized in Table 2. The sample size of the 22 studies ranged from 43 to 4,249, and comprised 19,934 participants with 14,104 individuals allocated to intervention and 5,830 individuals allocated to control arms. The mean age of participants was 13.65 years (SD 0.96) in the intervention arms 34 , 35 , 36 , 37 , 38 , 40 , 42 , 43 , 44 , 46 , 47 , 48 , 49 , 50 and 13.44 years in the control arms. 34 , 37 , 38 , 40 , 42 , 43 , 44 , 46 , 47 , 50 Thirteen studies were conducted in ‘healthy’ (i.e., nonclinical group) adolescents, 33 , 35 , 36 , 37 , 38 , 39 , 41 , 45 , 49 , 51 , 52 , 53 , 54 and nine studies were conducted in a mix of normal weight, overweight or at risk of overweight/obesity adolescents. 34 , 40 , 42 , 43 , 44 , 46 , 47 , 48 , 50 Three studies assessed SES based on individual‐level SES (i.e., education level), 43 , 47 , 50 three based on family‐level SES (i.e., parental education attainment and occupation status), 37 , 38 , 54 two studies based on household‐level SES (i.e., parental income), 39 , 48 four studies based on household‐level SES (eligibility for the national free/reduced school lunch programme), 33 , 41 , 42 , 45 eight studies based on neighborhood‐level SES, 34 , 35 , 36 , 40 , 49 , 51 , 52 , 53 and one study based on school‐level SES assessed by the Index of Community Socio‐Educational Advantage (ICSEA). 44 One study did not report participants' SES backgrounds. 46 Fifteen studies included ethnic diverse participants: African–American, 52 , 53 Latino/Hispanics, 41 a combination of Black/African–American, Latino/Hispanics, Asian/Pacific, Native American, 33 , 35 , 36 , 42 , 44 , 45 , 48 , 54 non‐Western, White and a mixed ‘other’ group. 34 , 39 , 46 , 50 Six studies mentioned including an ethnic diverse sample; however, participants' ethnic backgrounds were not reported. 37 , 38 , 40 , 43 , 47 , 49 One study assessed ethnicity based on language spoken at home. 51 Participants' education levels differed. Education levels were categorized as either middle, high or secondary schools, depending on where the study was conducted.
TABLE 2.
Detailed summary of study characteristics of 22 studies reporting change in SSB intake
| Author, year country | Study aims | Study design | Setting provider | Length of intervention | Sample demographics | Intervention type Theory used | Intervention arm Control arm | BCTs used | SSB type SSB assessment | Overall conclusion |
|---|---|---|---|---|---|---|---|---|---|---|
|
Bleich et al. 2014 52 USA |
To examine whether caloric information reduces the quantity, volume and number of calories of SSB purchases among Black adolescents. | Case‐crossover RCT |
Setting: Corner store‐based Provider: Study staff |
intervention: 2 weeks Follow up: 6 weeks follow up |
Population: Healthy adolescents N: 433 boys, 383 girls Age: 12–18 years Education level: Middle & high schools SES measure: area‐level SES, stores in low‐SES neighbourhoods Ethnicity: Black/African–American |
Environmental Theory: NR |
Intervention group: Caloric signs on SSBs Control group: No caloric signs provided |
No BCTs |
SSBs: Soda, fruit drink, sport drink, vitamin water, and ‘hug’ (a fruit drink packaged in 8‐ounce bottles) Objective: registered sales data |
Significant reduction in SSB intake |
|
Bleich et al. 2012 53 USA |
To examine whether different forms of caloric information reduces the volume of SSB purchases among Black adolescents. | Case‐crossover RCT |
Setting: Corner store‐based Provider: Study staff |
intervention: 2 weeks Follow up: ? |
Population: Healthy adolescents N: 800 boys, 799 girls Age: 12–18 years Education level: Middle & high schools SES measure: area‐level SES, stores in low‐SES neighbourhoods Ethnicity: Black/African–American |
Environmental Theory: NR |
Intervention group: Caloric signs on SSBs Control group (inactive control): Receives no intervention |
No BCTs |
SSBs: Soda, fruit drink, sport drink, vitamin water, and ‘hug’ (a fruit drink packaged in 8‐ounce bottles) Objective: registered sales data |
Significant reduction in SSB intake |
|
Bogart et al. 33 2011 USA |
To pilot‐test an intervention aimed to translate school obesity‐prevention policies into practice with peer advocacy of healthy eating and school cafeteria changes. |
Quasi‐experimental (pre–post with a control group) |
Setting: School‐based Provider: Students |
intervention: 5 weeks Follow up: 1‐month follow up |
Population: Healthy adolescents N: 200 boys, 200 girls Mean age: 13 years (SD 0.5) Education level: seventh graders, middle schools SES measure: household income‐level SES, i.e., NFLP eligibility (77% NFLP eligible) Ethnicity: 68% Latino 17% Asian/Pacific 11% Black/African American 2% White 1% Native American 1% Other |
Educational/behavioural/environmental Theory: Diffusion theory Social cognitive theory Theory of planned behaviour Empowerment theory |
Intervention: School‐based peer‐led educational programme with: Peer leader component where peers are trained to model and promote healthy behaviours. School food changes in the environment which included improving canteen signage, providing posters explaining and displaying nutritional information. Control (inactive control): Receives no intervention |
2.2, 4.3, 5.1, 12.1, 13.1 |
SSBs: Soda, sports drinks and noncarbonated fruit drinks Subjective: Dietary survey |
Significant within‐group reduction in SSB intake. |
|
Collins et al. 34 2014 Australia |
To test the impact of a school‐based obesity prevention programme targeting adolescent girls of low socioeconomic position on dietary intake and behaviours | Cluster‐RCT |
Setting: School‐based Provider: School staff |
intervention: 12 months Follow up: 12 months follow up |
Population: Normal (58%) and at risk for OWOB sample N: 357 girls Mean age: 13.1 years (SD 0.44) Education level: High schools SES measure: area‐level SES, schools in low‐SES neighbourhoods Ethnicity: Australian: 153 (86%) European: 18 (10%) Other: 8 (4.6%) |
Education/behavioural Theory: Social cognitive theory |
Intervention: Handbook on nutrition and physical activity Three practical nutritional workshops Parental newsletters and text‐messaging Control (waitlist control) Receives intervention after intervention period ends |
2.3, 3.2, 5.1, 7.1 |
SSBs: Soda, fruit juice drinks and cordial concentrate Subjective: validated FFQ |
No significant between‐group reduction in SSB intake |
|
Contento et al. 2007 36 USA |
To evaluate the feasibility of a school‐based intervention (C3) on fostering healthful eating, physical activity and healthy weight through enhancing agency and competence among middle school students. |
Quasi‐experimental (pretest‐posttest with no control group) |
Setting: School‐based Provider: School staff |
intervention: 8 weeks |
Population: Healthy adolescents N: NR Mean age: 12 years (range 11–13) Education level: 7th graders, middle schools SES measure: Area‐level SES, schools in low‐SES neighbourhoods Ethnicity: 25% African American, 70% Hispanic 5% other |
Education/behavioural Theory: Extended theory of planned behaviour Self‐regulation theory Theory of planned behaviour |
Intervention: Inquiry‐based science education consisting of a 24‐session curriculum during which students learns how one's body works, how to set goals and learning skills to achieve goals Control: No control group |
1.1, 1.2, 1.4, 1.9, 2.3, 5.1, 10.11 |
SSBs: Carbonated/noncarbonated drinks Subjective: Validated FFQ |
Significant within‐group reduction in SSB intake |
|
Contento et al. 2010 35 USA |
To examine the impact of a curriculum intervention, choice, control, and change (C3), on energy balance‐related behaviours (EBRBs) such as decreasing SSB intake and on potential mediators of the behaviours. |
Cluster‐RCT (pre–post with a control group) |
Setting: School‐based Provider: School staff |
intervention: 1 year |
Population: Healthy adolescents N: 286 boys, 275 girls Mean age: 12 years (range 11–13) Education level: Middle schools (7th graders) SES measure: Household income‐level SES, i.e., NFLP eligibility (83% NFLP eligible) Ethnicity: 25% African American 70% Latino 5% others |
Educational/behavioural Theory: Social cognitive theory Self‐determination theory |
Intervention: Inquiry‐based education which consists of 24 sessions of 45 min addressing energy balance, educational activities for acting, potential motivational and behaviour change variables to enhance personal agency. Control (waitlist control): Receives intervention after intervention period ends |
1.1, 1.2, 1.4, 1.9, 2.3, 4.1, 5.1, 10.11 |
SSBs: Soft drinks, fruit drinks, sports drinks, iced tea, drink mixes Subjective: validated FFQ |
Significant between‐group reduction in SSB intake. |
|
Dubuy et al. 2012 38 Belgium |
To examine the impact of a curriculum intervention, choice, control, and change (C3), on energy balance‐related behaviours (EBRBs) such as decreasing SSB intake and on potential mediators of the behaviours. | Quasi‐experimental (pre–post with a control group) |
Setting: Schools Football clubs Provider: School staff |
intervention: 4 months |
Population: Healthy adolescents N: 146 boys, 19 girls Mean age: 12.6 years (SD 1.02) Education level: Elementary and secondary schools SES measure: Family‐level SES, i.e., parental education level Ethnicity: NR |
Educational/behavioural Theory: Elaboration likelihood model |
Intervention: Start clinic and end clinic: clinic activities encouraging healthy diet and physical activity (e.g., eating a healthy breakfast) school programme: 4‐month educational programme consisting of classroom activities on healthy diet and physical activity. Control (usual control): Receives regular curriculum |
1.8, 5.1, 6.1, 9.1 |
SSBs: Soft drinks Subjective: Validated FFQ |
No significant between‐group reduction in SSB intake. |
|
Ezendam et al. 2012 50 The Netherlands |
To evaluate the short‐ and long‐term effects of FATaintPHAT to prevent excessive weight gain among adolescents aged 12–13 years by improving their dietary behaviours (reducing SSB consumption), reducing sedentary behaviours and increasing PA. | Cluster‐RCT |
Setting: School‐based Provider: School staff |
intervention: 4 months Follow up: 2‐year follow up |
Population: Normal (75%) and at risk for OWOB sample N: 284 boys, 198 girls Mean age: 12.7 years (SD 0.7) Education level: General secondary schools SES measure: Individual‐level SES, i.e., education level (64% vocational) Ethnicity: 320 Western 165 non‐Western |
Educational/behavioural Theory: Precaution adoption process model Implementation intentions Theory of planned behaviour |
Intervention: Educational component: Online computer‐tailored intervention consisting of 8 lessons spread over 10 weeks. Each module consists of information about the behaviour‐health link, assessment of behaviour, tailored feedback on dietary and physical activity behaviours, and option to formulate an implementation intention to prompt specific goal setting and action planning. Control (usual control) Receives regular curriculum |
1.1, 1.2, 1.4, 2.2, 3.2, 4.1 5.1, 6.2 |
SSBs: Type SSB NR Subjective: Validated FFQ |
Significant between‐group reduction in SSB intake |
|
Foley et al. 2017 51 Australia |
To assess the impact of the SALSA programme on Year 10 SALSA peer leaders ‘dietary, physical activity and recreational screen time behaviours, and their intentions regarding these energy balance‐related behaviours (EBRBs) |
Quasi‐experimental (pre–post with no control group) |
Setting: School‐based Provider: Students |
intervention: NR |
Population: Healthy adolescents N: 150 boys, 265 girls Age: Range 13–16 years Education level: High schools SES measure: Area‐level SES, schools located in low‐SES neighbourhoods Ethnicity: Language spoken at home 70% English 19% Asian 6% Middle Eastern 5% Other |
Education/behavioural Theory: Social Cognitive Theory Empowerment education approach WHO Health Promoting School Framework |
Intervention: Peer education intervention: SALSA educators (university students) will train year 10 students as SALSA peer leaders. In teams of four, trained leaders will deliver 4 × 70 min lessons to their young peers in Year 8 using DVD, games and activities on how to make healthy dietary choices and be physically active Control: No control group | 1.1, 1.3, 1.4, 4.1, 6.1 |
SSBs: Type SSB NR Subjective: Validated FFQ |
Significant within‐group reduction in SSB intake |
|
French et al. 2011 39 USA |
To evaluate the effects of a family‐based intervention to prevent excess weight gain among a community‐based sample of households (HH) | cluster‐RCT |
Setting: Household‐based Provider: Study staff |
intervention: 6 months Follow up: 6 months |
Population: Healthy adolescents N: 75 boys and girls Age: 12–17 years old Education level: General secondary schools SES measure: Household‐level SES, i.e., parental income (34% ≤ $45,000/year) Ethnicity: 21% non‐White |
Education/behavioural Theory: NR |
Intervention: Home‐based programme which included 6 monthly: Face‐to‐face group sessions: 2 h group sessions on behavioural education, physical activity and healthy dietary choices, monthly newsletters and 12 home‐based activities and telephone support calls. Control (inactive control): Receives no intervention |
1.1, 1.2, 1.4, 2.3, 3.2, 6.2, 7.3, 10.3, 12.1, 12.5 |
SSBs: Type SSB NR Subjective: Validated FFQ |
No significant between‐group reduction in SSB intake. |
|
Haerens et al. 2007 37 Belgium |
To evaluate the effects of a middle‐school healthy eating promotion intervention combining environmental changes and computer‐tailored feedback, with and without an explicit parent involvement component. | Cluster‐RCT |
Setting: School‐based Provider: School staff |
intervention: 12 months Follow up: NR |
Population: Healthy adolescents N: Intervention arm 1: 734 boys, 491 girls Intervention arm 2: 849 boys, 156 girls Age: Intervention arm 1 13.04 (SD 0.79) intervention arm 2: 13.2 (SD 0.87) Education level: General secondary schools with technical/vocational training SES measure: Family‐level SES, i.e., parental occupation (68% of participants low‐SES) Ethnic background: Study mentions including ethnical diverse sample but participants' backgrounds are NR |
Education/behavioural/ Environmental Theory: Transtheoretical model Theory of planned behaviour |
Intervention: —Educational component aimed to promote healthy food choices and physical activity engagement ‐environmental changes: increasing the availability of healthy foods and restricting the availability of unhealthy foods by implementing policies. To increase fruit intake, fruits were sold at very low cost/provided free to all 7th and 8th graders. To increase water consumption, schools offered free drinking fountains ‐parental involvement: parents received newsletters on how to create supportive home environments for health behaviours. Control (inactive control) Receives no intervention |
1.2, 1.4, 2.2, 3.2, 4.1, 5.1, 6.1, 6.2, 12.1 |
SSBs: Soft drinks Subjective: Validated FFQ |
No significant between‐group reduction in SSB intake. |
|
Lane et al. 2018 40 USA |
To test the feasibility of KidsSmartER intervention on reducing SSB intake among 6th and 7th graders. |
Matched‐contact crossover RCT with no control group |
Setting: School‐based Provider: School and study staff |
intervention: 6 weeks Follow up: 3 months follow up |
Population: Normal (n = 12) and at risk for OWOB sample N: 17 boys, 26 girls Mean age: 11.7 years (SD 0.6) Education level: Middle schools SES measure: area‐level SES, schools located in low‐SES neighbourhoods Ethnicity: Racial/ethnic adolescents, backgrounds NR |
Education/behavioural Theory: Theory of planned behaviour |
Intervention: School‐based educational curriculum (6‐week 45‐min lesson given during science classes) with different components: Media literacy to encourage obtaining, interpreting and controlling the influence of media messages Public health literacy to obtain, interpret and act on information needed to make decisions benefitting the community. Control (active control) Control group received matched‐contact intervention |
1.1, 1.2, 3.2, 5.1, 5.3, 6.1, 13.1 |
SSBs: Soda, energy/sports drinks, coffee with cream/sugar, sweet tea, and sweetened fruit juice Subjective: Validated FFQ |
Significant within‐group reduction in SSB intake. |
|
Majumdar et al. 2013 41 USA |
To evaluate the efficacy of a game on decreasing intake of processed snacks (e.g., chips, candy) and SB among adolescents attending low‐income schools. | Pretest‐posttest‐matched design with a control group |
Setting: School‐based Provider: Game |
intervention: 1 month |
Population: Healthy adolescents N: boys, 88 girls Age range: 11 to >13 years Education level: 6th and 7th graders in middle schools SES measure: Household‐income based on NSLP eligibility (78% NSLP eligible) Ethnicity: 63% Latino/Hispanics |
Education/behavioural Theory: Social Cognitive Theory Self‐determination theory |
Intervention: game‐based educational programme consisting of 24 lessons targeting dietary and physical activity behaviours Control (active control): Control receives a different game (WhyWille) game which did contain active intervention components |
1.1, 1.2, 1.4, 2.3, 4.4, 5.1, 7.1 |
SSBs: Type SSB NR Subjective: Validated FFQ |
Significant between‐group reduction in SSB intake. |
|
Neumark‐Sztainer et al 2010 42 USA |
To evaluate the impact of a school‐based intervention aimed at preventing weight‐related problems in adolescent girls. | RCT |
Setting: School‐based Provider: Study staff |
intervention: ? Follow up: ? |
Population: Normal (17%) and at risk for OWOB sample N: 356 girls Mean age: 17.5 years (SD 1.13) Education level: High schools SES measure: Household‐income based on NSLP eligibility (58% NSLP eligible) Ethnicity: 32.4% African–American/Black 27% White 16.5% Hispanic 8% Mixed/other 3.3% American Indian |
Education/behavioural Theory: Extensive formative research Social cognitive theory Transtheoretical Model |
Intervention: Educational component consisting of nutrition and social support/self‐empowerment sessions individual counselling sessions, one‐week lunch brunch and parent outreach. Control (active control) Receives a different intervention |
1.1, 1.2, 3.2, 4.1, 5.1, 8.1, 11.2 |
SSBs: Soda, fruit drinks, sports drinks, sweetened tea and coffee Subjective: 24‐h recall |
No significant between‐group reduction in SSB intake. |
|
Singh et al. 2009 43 The Netherlands |
To evaluate the efficacy of a multicomponent intervention on reducing SSB intake in both short and long‐term terms among Dutch adolescents. | cluster‐RCT |
Setting: School‐based Provider: Study staff |
intervention: 8 months Follow up: 12 months |
Population: Normal (71.8%) and at risk for OWOB sample N: 295 boys, 337 girls Mean age: 12.8 years (SD 0.5) Education level: Prevocational secondary schools SES measure: Individual‐level SES, i.e., education level Ethnicity: Author mentions including a diverse ethnic sample but participants backgrounds NR |
Education/behavioural/ environmental Theory: Intervention mapping |
Intervention: —Educational programme covering 11 lessons on biology and physical education —Environmental change options such as encouraging schools to offer additional physical education classes and advice for schools on changes in and around school cafeterias Control (usual control): Receives regular curriculum |
1.2, 1.4, 2.2, 2.3, 3.2, 4.1, 5.1, 6.2, 7.1, 7.3, 8.1, 8.7, 10.3, 12.1, 12.5 |
SSBs: Soft drinks and fruit juices Subjective: Validated dietary questionnaire |
Significant between‐group reduction in SSB intake. |
|
Smith et al. 2014 44 Australia |
To evaluate the impact of the Active Teen Leaders Avoiding Screen‐time (ATLAS) intervention for adolescent boys, an obesity prevention intervention using smartphone technology. | cluster‐RCT |
Setting: School‐based Provider: Study staff |
intervention: 8 months Follow up: 18 months |
Population: Normal (61%) and at risk for OWOB sample N: 361 boys Mean age: 12.7 years (SD 0.5) Education level: High schools SES measure: School‐level SES, i.e., based on ICSEA. Ethnicity: 80.6% Australian 12.2% European 0.6% African 2.2% Asian 4.4% Other |
Education/behavioural Theory: Social cognitive theory Self‐determination theory |
Intervention: Teach professional development parents and parental newsletters Students research‐led seminars Enhanced school sports sessions Lunchtime physical activity‐mentoring sessions Smartphone app and Website Control (waitlist): Receives intervention after intervention period ends |
1.1, 1.2, 1.4, 1.8, 2.2, 2.3, 3.2, 4.1, 5.1, 6.1, 8.7, 10.3, 10.11, 13.1 |
SSBs: Type SSB NR Subjective: Validated dietary/physical activity questionnaire |
Significant between‐group reduction in SSB intake. |
|
Smith et al. 2014 45 USA |
To evaluate the efficacy of a school‐based intervention on SSB consumption among Appalachian high school students. | Quasi‐experimental (pre–post with no control group) |
Setting: School‐based Provider: Students |
intervention: 4 weeks Follow up: 1‐month follow up |
Population: Healthy adolescents N: 73 boys, 113 girls Mean age: 15.8 years (SD 1.8) Education level: 9–12 graders, high schools SES measure: Household‐income based on NSLP‐eligibility (40% NSLP‐eligible) Ethnicity: 94.6% White/Caucasian 3% Black/African–American 0.5% Native American 0.5% Asian American 1% > Other |
Education/behavioural Theory: NR |
Intervention: Educational programme on media messaging, media coverage of SSBs, written information for school newsletters and local newspapers about SSBs Control: No control group |
5.1, 8.2, 10.11 |
SSBs: Pop/soda sweetened tea, sweetened coffee drinks, fruit drinks (excluding 100% juice), sports drinks, and energy drinks Subjective: Survey |
Significant within‐group reduction in SSB intake. |
|
Spook et al. 2016 46 The Netherlands |
To pilot the effects of balance IT, a self‐regulation game on dietary intake and PA among secondary vocational students. |
cluster‐RCT (pre–post with a control group) |
Setting: School‐based Provider: Game |
intervention: 4 weeks |
Population: Normal (75%) and at risk for OWOB sample N: 39 boys, 66 girls Mean age: 16.7 years (SD 1.10) Education level: Lower vocational secondary schools SES measure: NR Ethnicity: 27% non‐Dutch |
Education/behavioural Theory: Self‐regulation theory Intervention mapping |
Intervention: Tailored educational game in which participants are asked to set graded tasks. Users are asked to monitor and evaluate their goals on a daily/weekly basis. Each day, users are prompted with their goals. Visual feedback on self‐reported goal attainment is provided for each goal set. Users are also asked to formulate implementation intentions (these implementation intentions can be set as reminder prompts). Social support is provided through the Balance IT Forum. Control (waitlist) Receives the intervention after intervention period ends |
1.1, 1.2, 1.4, 2.2, 2.3, 3.2, 7.1, 10.3 |
SSBs: Soft drinks Subjective: Validated FFQ |
No significant between‐group reduction in SSB intake. |
|
VanEpps et al. 2016 54 USA |
To test the extent to which warning labels for SSBs can influence adolescents' beliefs and hypothetical choices | RCT |
Setting: Lab‐based Provider: Web‐based |
intervention: ? Follow up: ? |
Population: Healthy adolescents N: 1,094 boys, 1,108 girls Mean age: 15 years Education level: 5th–12th graders, middle‐high schools SES measure: Family‐level SES based on parental education level (9.6% with maternal education <high school degree, 6.5% participants with paternal education <high school degree). Ethnicity: 31.6% Hispanic 62.9% White 33.6% Black 1.8% Asian 2.1% Native American 0.3% Hawaiian 4.5% Other |
Educational/behavioural Theory: NR |
Intervention: A hypothetical vending machine setting in which users receive 6 warning conditions (e.g., SAFETY WARNING: Drinking beverages with added sugar(s) contributes to obesity, diabetes, and tooth decay) Control (inactive): Receives no intervention |
no BCTs |
SSB definition: Type SSB NR Subjective: Survey |
Significant reduction in SSB intake. |
|
Nassau et al. 2014 47 The Netherlands |
To evaluate the impact of the DOiT‐implementation programme on adolescents' adiposity and energy balance‐related behaviours. | cluster‐RCT |
Setting: School‐based Provider: Study staff |
Follow up: 20‐month follow up |
Population: Normal (72%) and at risk for OWOB sample N: 428 boys, 483 females Mean age: 12.8 years Education level: prevocational secondary schools SES measure: Individual‐level SES based on education level Ethnicity: Author mentions including a diverse ethnic sample but participants backgrounds NR |
Education/behavioural/environmental Theory: Intervention Mapping |
Intervention Educational programme covering 11 lessons on biology and physical education environmental change options such as encouraging schools to offer additional physical education classes and advice for schools on changes in and around school cafeterias. Control (usual): Receives regular curriculum) |
1.2, 1.4, 2.2, 2.3, 3.2, 4.1, 5.1, 6.2, 7.1, 7.3, 8.1, 8.7, 10.3, 12.1, 12.5 |
SSB definition: Type SSB NR Subjective: Validated dietary questionnaire |
Significant within‐group reduction in SSB intake. |
|
Whittemore et al. 48 2012 USA |
To compare the effectiveness of two school‐based internet obesity prevention programmes on dietary and physical activity behaviours | cluster‐RCT |
Setting: School‐based Provider: Web‐based |
intervention: 3 months Follow up: 6 months follow up |
Population: Normal (61%) and at risk for OWOB sample N: 77 boys, 130 girls Mean age: 15.2 years (SD 0.69) Education level: High schools SES measure: Household‐level SES based on parental income (42% with an income <40.000) Ethnicity: 37% White 21.6% Hispanic 28.9% African–American 12.3% Other |
Education/behavioural Theory: Theory of interactive technology Social learning theory |
Intervention: School‐based web educational programme composed of two components: HealtheTeen: Students receive lessons on goal‐setting, self‐monitoring, health coaching and social networking. HealtheTeen + CST: Includes similar lessons as HealtheTeen but also lessons on coping skills training, social problem, solving, stress reduction, assertive communication and conflict solving. Control (usual) Receives regular curriculum |
1.1, 1.2, 2.2, 2.3, 3.2, 5.1, 6.1, 8.1, 9.1, 11.2 |
SSB definition: Soda and fruit juice Subjective: Validated dietary questionnaire |
Significant between‐group reduction in SSB intake. |
|
Winett et al, 1999 49 USA |
To test the efficacy of the programme with multiple groups of 9th‐ and l0th‐grade girls on reducing calories from SSB. |
Quasi‐experimental (pre–post with a control group) |
Setting: School‐based Provider: School staff |
intervention: ? |
Population: Healthy adolescents N: 103 girls Mean age: 14.9 years Education level: 9th and 10th graders, high school SES measure: Area‐level SES, schools located in low‐SES neighbourhoods Ethnicity: NR |
Education/behavioural Theory: Social cognitive theory |
Intervention: School‐based educational programme which focuses on dietary and physical activity behaviours. Control (usual): Receives regular curriculum |
1.1, 1.5, 2.2, 2.3, 5.1, 6.3 |
SSB definition: Soda Subjective: 24‐h recall and validated FFQ |
Significant between‐group reduction in SSB intake. |
Abbreviations: FQs, food frequency questionnaires; NR, not reported; NSLP, national school free/reduced lunch programme; OWOB, overweight/obese, SEIFA, socioeconomic index for areas; SES, socioeconomic status; SSB, sugar‐sweetened beverage; RCTs, randomized controlled trials; WHO, World Health Organization.
Thirteen studies were conducted in the United States, 33 , 35 , 36 , 39 , 40 , 41 , 42 , 45 , 48 , 49 , 52 , 53 , 54 three in Australia, 34 , 44 , 51 two in Belgium 37 , 38 and four in the Netherlands. 43 , 46 , 47 , 50 Fifteen studies used RCT designs, and seven studies used pre–post designs. Seventeen studies were school‐based interventions, 33 , 34 , 35 , 36 , 37 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 one study was school and football‐based intervention, 38 two store‐based, 52 , 53 one home‐based 39 and one lab‐based. 54 The total number of intervention arms was 33 with the majority of studies being one‐arm interventions (n = 18; range 1–6 arms). Intervention duration ranged from 2 weeks to 9 months and follow up from 1–20 months. Studies were classified as educational/behavioral (e.g., nutritional education on SSB), environmental (e.g., changes in the physical context) or both. Fifteen studies were classified as educational/behavioral interventions, 34 , 35 , 36 , 38 , 40 , 41 , 42 , 44 , 45 , 46 , 48 , 49 , 50 , 51 , 54 two as environmental 52 , 53 and five as both. 33 , 37 , 39 , 43 , 47 Seventeen interventions were theory‐driven, of which six were based on one behavioral theory 34 , 38 , 40 , 43 , 49 and 11 based on a combination of behavioral theories. 33 , 35 , 36 , 37 , 41 , 42 , 44 , 46 , 48 , 50 , 51 Five studies did not use any behavioral theories. 39 , 45 , 52 , 53 , 54 Common behavioral theories were social cognitive theory (n = 8) and theory of planned behavior (n = 5). Two studies measures SSB intake objectively (sales data), 52 , 53 and 20 studies assessed SSB subjectively using validated food frequency questionnaires (FFQs), food surveys, dietary questionnaires and 24‐h recalls. 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 , 54
Fourteen studies 33 , 34 , 35 , 36 , 37 , 38 , 40 , 42 , 43 , 45 , 48 , 49 , 52 , 53 reported type of beverages included in its definition of SSBs. 4 Eight studies did not report the type of beverages included but reported only measuring SSBs. 36 , 39 , 41 , 44 , 47 , 50 , 51 , 54 Majority of the studies had a general SSB category without specifying the impact of the intervention per SSB type. Most of studies only measured whether or not the intervention was effective in reducing SSB consumption.
In most studies, the intervention was compared with a treatment as usual control (n = 7), waitlist control (n = 4), active control (n = 3), inactive control (n = 3) or no control (n = 5).
3.2. Risk of bias of included studies
The risk of bias of RCTs is summarized in Figures 2 and 3. There was a low risk of bias for attrition bias (n = 10, 67%), reporting bias (n = 13, 87%) and other bias (n = 8, 53%). However, for most studies, the risk associated with blinding of assessors (n = 15, 100%) was high. In addition, majority of studies were deemed to have an unclear risk of bias due to insufficient descriptions related to randomization (n = 10, 67%), allocation concealment (n = 12, 80%) and blinding of participants and research staff (n = 5, 33%). Overall, the risk of the included RCTs was deemed moderate to high risk of bias.
FIGURE 2.
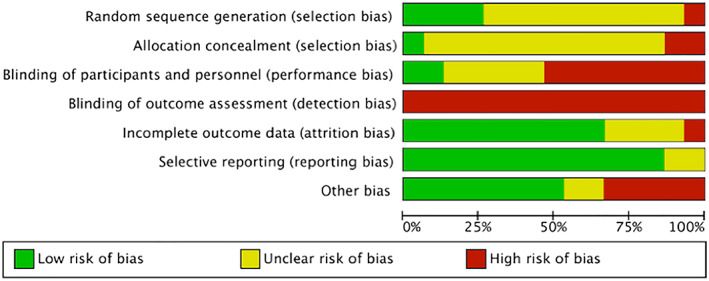
The overall risk of bias assessment of included randomized controlled trials (RCTs)
FIGURE 3.
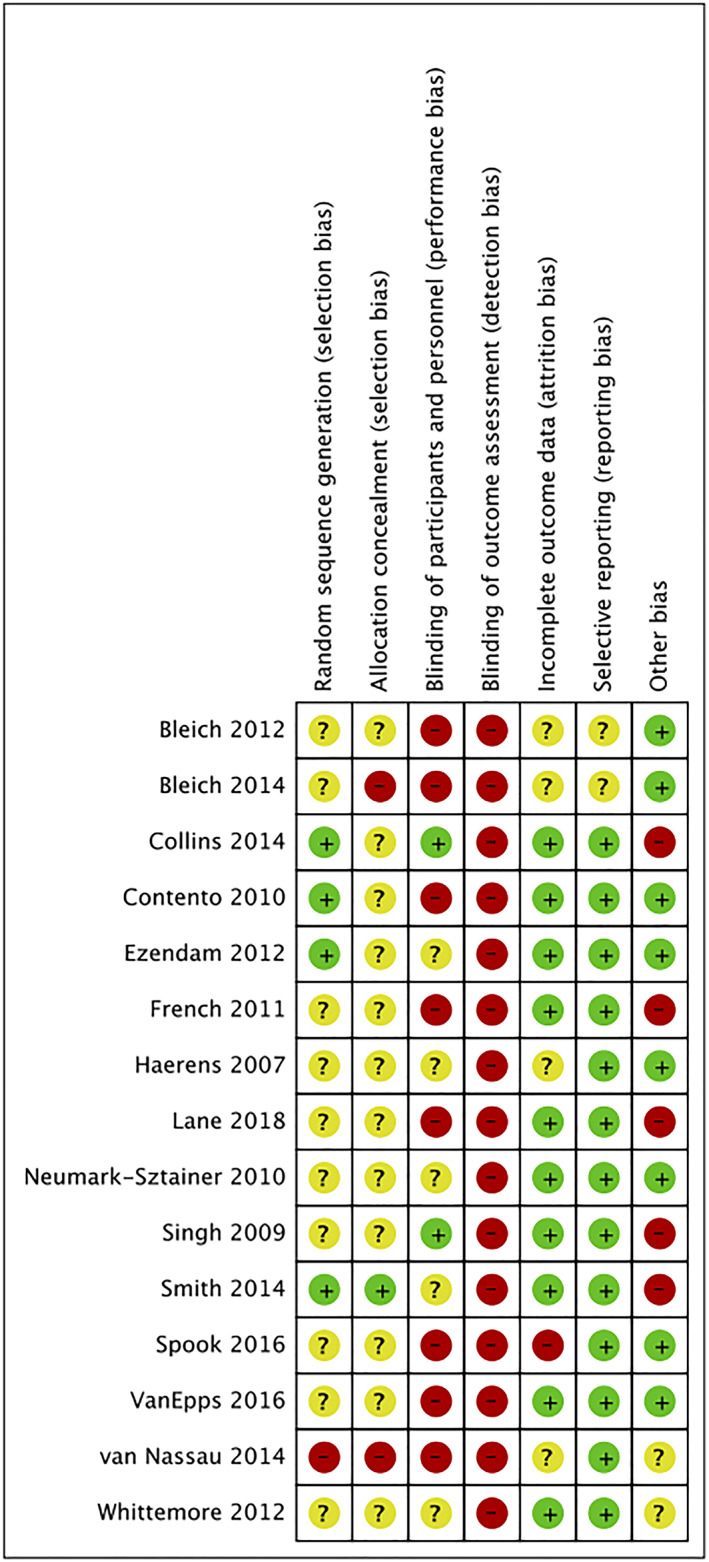
Risk of bias summaries for randomized controlled trials (RCTs)
The risk of bias of non‐RCTs was evaluated using the Newcastle–Ottawa tool and is presented in Figure 4. Four studies were judged to have a ‘moderate’ risk of bias, two were rated as having a ‘low’ risk of bias and one ‘high’ risk of bias.
FIGURE 4.
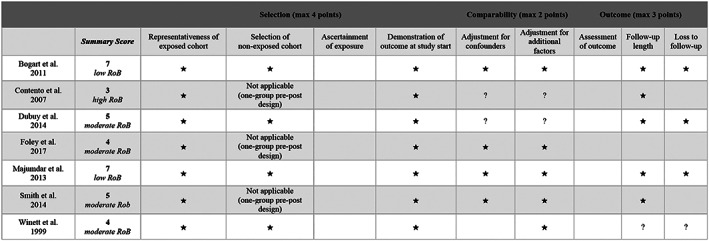
Quality assessment of nonrandomized controlled trials based on the Newcastle–Ottawa quality tool
3.3. Meta‐analysis: Effectiveness of interventions on reducing SSB intake
Forest plots of individual study effects at pre‐ and at post‐intervention are presented in Figures 5 and 6, respectively. Cluster‐robust models revealed no significant change in SSB intake between groups at pre‐intervention (g = −0.24, 95% CI [−0.80, 0.32], p = 0.36), and at post‐intervention (g = −0.23, 95% CI [−0.76,0.29], p = 0.35). In addition, we observed no significant change in SSB intake between groups from pre‐ to post‐intervention (F (1, 13) = 0.00, p = 0.99). At pre‐intervention, results of the multilevel models showed no significant change in SSB intake between groups (g = −0.18, 95% CI [−0·58, 0·22], p = 0.37). Heterogeneity was substantial (Q (df = 16), 889.73, I 2 = 99%). Likewise, at post‐intervention, there was no significant change in SSB intake between groups (g = −0.30, [95% CI [−0.75, 0.14], p = 0.19), and heterogeneity was substantial (Q (df = 15), 898.27, I 2 = 99%). Inspection of the forest plots (Figures 5 and 6) revealed three studies that were identified as outliers. 33 , 34 , 50 To check if results would change after removing the three influential studies, we reran the primary meta‐analysis. Results of the multilevel models showed no significant change in SSB intake between groups at pre‐intervention (g = 0.12, 95% CI [−0.02, 0.25], p = 0.08), at post‐intervention (g = −0.31, 95% CI [0.78, 0.15], p = 0.16), and from pre‐ to post‐intervention (F (1, 11) = 4.77, p = 0.06).
FIGURE 5.
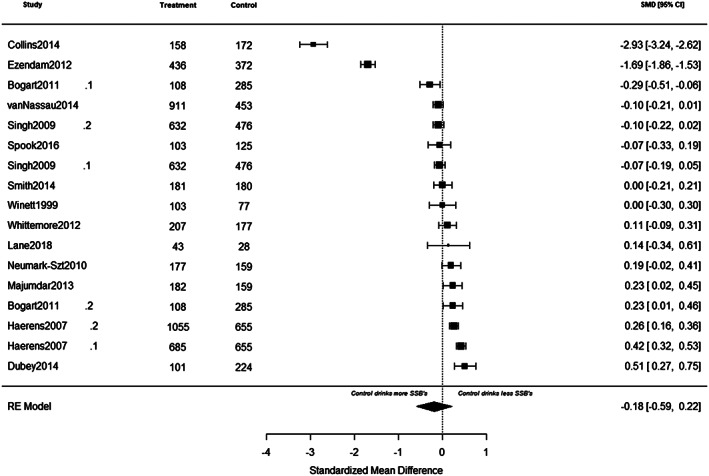
A summary of individual study effects at pre‐intervention. The comparison between intervention and control groups at pre‐intervention are derived from separate random‐effects models. Hedges' g point estimates are represented by filled squares, and the filled diamond represents the estimated summary effect sizes (standardized mean difference). Error bars and diamond width represents the 95% confidence intervals. Positive values represent favouring the intervention whereas negative values represent favouring the control groups
FIGURE 6.
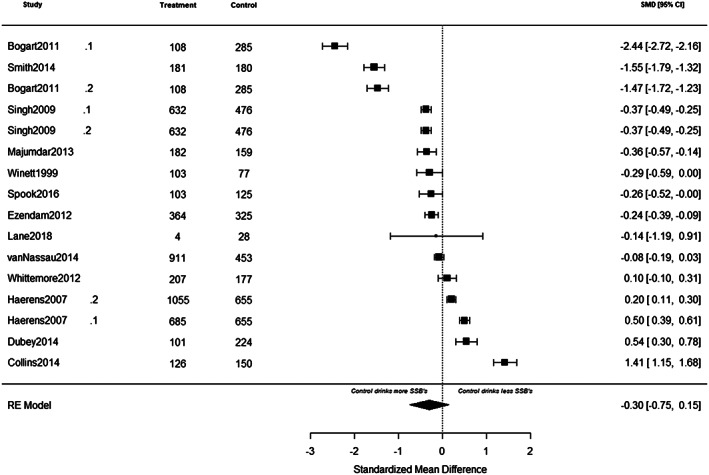
A summary of individual study effects at post‐intervention. The comparison between intervention and control groups at pre‐intervention are derived from separate random‐effects models. Hedges' g point estimates are represented by filled squares, and the filled diamond represents the estimated summary effect sizes (standardized mean difference). Error bars and diamond width represents the 95% confidence intervals. Positive values represent favouring the intervention whereas negative values represent favouring the control groups
Separate random‐effects models were used to assess the effects of potential moderators. No significant moderating effects of study design (RCT vs. non‐RCT), intervention type (educational/behavior vs. environmental), intervention component (single vs. multicomponent) and total number of BCTs were observed. Re‐analysing the primary analyses after excluding influential studies revealed different results. There was a significant moderating effect of intervention type on SSB intake at post‐intervention (QM (df = 1) = 7.26, p = 0.01), with interventions with an educational/behavioral component showing a reduction in SSB intake (β = −0.54, SE = 1.76, p < 0.01) relative to interventions with an environmental component (β = 0.29, SE = 0.25, p = 0.26).
Visual inspection of funnel plots (Figures 7 and 8) using the Egger regression asymmetry test suggested no evidence of publication bias to higher values (p > 0.05).
FIGURE 7.
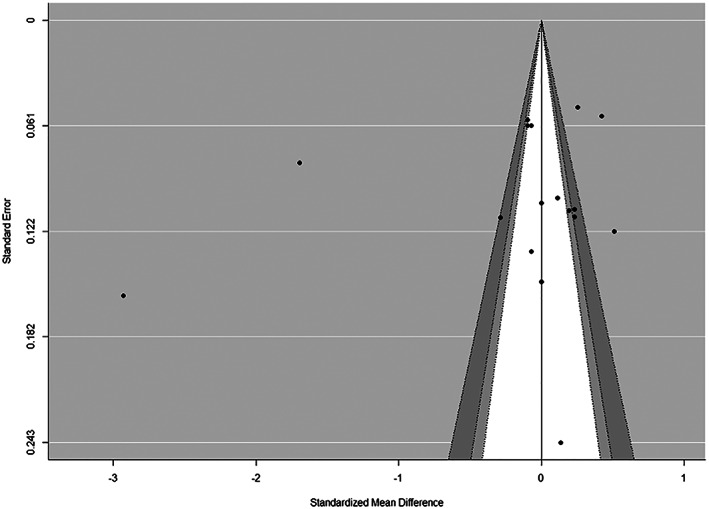
Contour‐enhanced funnel plots for sugar‐sweetened beverage (SSB) intake at pre‐intervention. In these plots, individual study effect estimates are plotted against standard errors to determine whether statistically significant studies are overrepresented in the included studies. The light grey area denotes p values between 0.1 and 0.05, the dark grey region captures p values between 0.05 and 0.01, and the white region includes p values greater than 0.1. Because there is no overrepresentation of studies within the light and dark grey regions, this is suggestive of low/no publication bias
FIGURE 8.
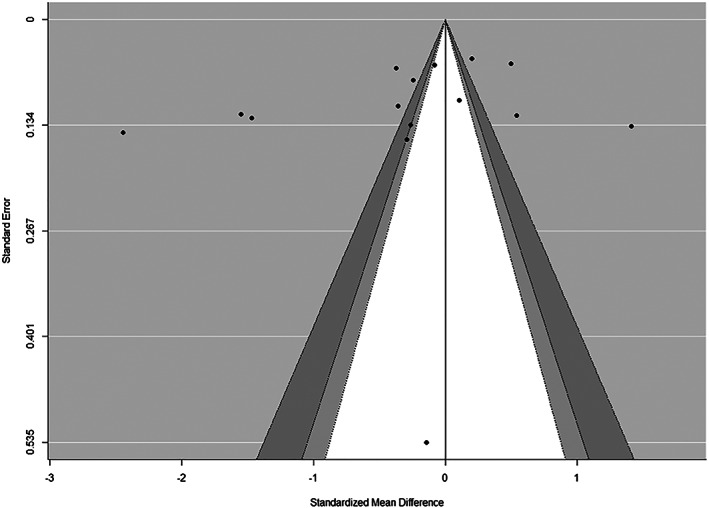
Contour‐enhanced funnel plots for sugar‐sweetened beverage (SSB) intake at post‐intervention. In these plots, individual study effect estimates are plotted against standard errors to determine whether statistically significant studies are overrepresented in the included studies. The light grey area denotes p values between 0.1 and 0.05, the dark grey region captures p values between 0.05 and 0.01, and the white region includes p values greater than 0.1. Because there is no overrepresentation of studies within the light and dark grey regions, this is suggestive of low/no publication bias
3.4. Effectiveness of BCTs (narrative synthesis)
Table 3 summarizes the BCTs identified in included studies and applied in the 33 active interventions arms. Of the 93 empirical BCTs, 30 were coded one or more times with a total of 153 BCTs coded across the active intervention arms. Three studies did not use BCTs. 52 , 53 , 54 The median number of BCTs used in all studies was seven (range: 3–15). A median of eight BCTs (range: 7–8) was used in four single‐component interventions. 35 , 36 , 40 , 50 A median of seven BCTs (range: 3–15) was used in 15 multicomponent interventions. 33 , 34 , 37 , 38 , 39 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 51 The most frequently used BCTs included information on health consequences (n = 16), problem‐solving and/or barrier identification (n = 13), and goal‐setting of behavior (n = 12). Studies classified as educational/behavioral used less BCTs (median = 7, range: 3–14) compared with studies classified as educational/behavior/environmental (median = 10 BCTs, range: 5–15). Seven studies were deemed ‘very effective’, 35 , 41 , 43 , 44 , 48 , 49 , 50 six ‘quite effective’ 33 , 36 , 40 , 45 , 47 , 51 and six ‘non‐effective’. 34 , 37 , 38 , 39 , 42 , 46 ‘Very effective’ studies used more BCTs (mean = 4.0, SD = 1.9) compared with ‘non‐effective’ studies (mean = 3.0, SD = 1.0) (Table 4).
TABLE 3.
Frequencies of behavior change techniques used in included studies
| Behavior change technique | N | % |
|---|---|---|
| 1.1 Goal setting (behavior) | 12 | 36.4 |
| 1.2 Problem solving/barrier identification | 13 | 39.4 |
| 1.3 Goal setting (outcome) | 1 | 3.0 |
| 1.4 Action planning (including implementation intention) | 11 | 33.3 |
| 1.5 Review behavior goals | 1 | 3.0 |
| 1.8 Behavioral contract | 2 | 6.1 |
| 1.9 Commitment | 2 | 6.1 |
| 2.2 Feedback on behavior | 9 | 27.3 |
| 2.3 Self‐monitoring of behavior | 11 | 33.3 |
| 3.2 Social support (practical) | 11 | 33.3 |
| 4.1 Instruction on how to perform the behavior | 8 | 24.2 |
| 4.3 Re‐attribution | 1 | 3.0 |
| 4.4 Behavioral experiments | 1 | 3.0 |
| 5.1 Information about health consequences | 16 | 48.5 |
| 5.2 Information about social and environmental consequences | 1 | 3.0 |
| 6.1 Modelling/demonstration of the behavior | 6 | 18.2 |
| 6.2 Social comparison | 5 | 15.2 |
| 6.3 Information about others approval | 1 | 3.0 |
| 7.1 Prompts/cues | 5 | 15.2 |
| 7.3 Reduce prompts/cues | 3 | 9.1 |
| 8.1 Behavioral/practice/rehearsal | 4 | 12.1 |
| 8.2 Behavior substitution | 1 | 3.0 |
| 8.7 Graded tasks | 3 | 9.1 |
| 9.1 Credible source | 2 | 6.1 |
| 10.3 Nonspecific reward (includes positive reinforcement) | 6 | 18.2 |
| 10.11 Future punishment (includes threat) | 4 | 12.1 |
| 11.2 Reduce negative emotions | 2 | 6.1 |
| 12.1 Restructuring the physical environment | 5 | 15.2 |
| 12.5 Adding objects to the environment | 3 | 9.1 |
| 13.1 Identification of self as role model | 3 | 9.1 |
TABLE 4.
Frequency of behavior change techniques coded in ‘very effective’, ‘quite effective’ and ‘non‐effective’ studies
| Behaviour change technique | Very effective studies (n = 7) | Quite effective studies (n = 6) | Non‐effective studies (n = 6) |
|---|---|---|---|
| 1.1 Goal setting (behavior) | 6 | 3 | 3 |
| 1.2 Problem solving/barrier identification | 6 | 3 | 4 |
| 1.4 Action planning (including implementation intention) | 5 | 3 | 3 |
| 2.2 Feedback on behavior | 5 | 2 | 2 |
| 2.3 Self‐monitoring of behavior | 6 | 2 | 3 |
| 3.2 Social support (practical) | 4 | 2 | 5 |
| 4.1 Instruction on how to perform the behavior | 4 | 2 | 2 |
| 5.1 Information about health consequences | 7 | 5 | 4 |
| 6.1 Modelling/demonstration of the behavior | 2 | 2 | 2 |
| 6.2 Social comparison | 2 | 1 | 2 |
| 7.1 Prompts/cues | 2 | 1 | 2 |
| 10.3 Non‐specific reward (includes positive reinforcement) | 3 | 1 | 2 |
| 12.1 Restructuring the physical environment | 1 | 2 | 2 |
Note: Studies are deemed ‘very effective’ if between‐group differences in SSB intake were reported, ‘quite effective’ if within‐group changes in SSB intake were reported, and ‘non‐effective’ if no between nor within‐group changes in SSB intake were reported.
The percentage effectiveness ratio of the BCTs is presented in Figure 9. In total, 13 BCTs had an effectiveness ratio >50%. The BCTs with the highest effectiveness ratio were feedback on behavior (n = 8/9, 78%), goal‐setting of behavior (n = 9/12, 75%), instruction on how to perform a behavior (n = 6/8, 75%), health consequences (n = 12/16, 75%), followed by action planning including implementation intention (n = 8/11, 73%), self‐monitoring of behavior (n = 8/11, 73%) and problem‐solving and/or barrier identification (n = 9/13, 69%).
FIGURE 9.
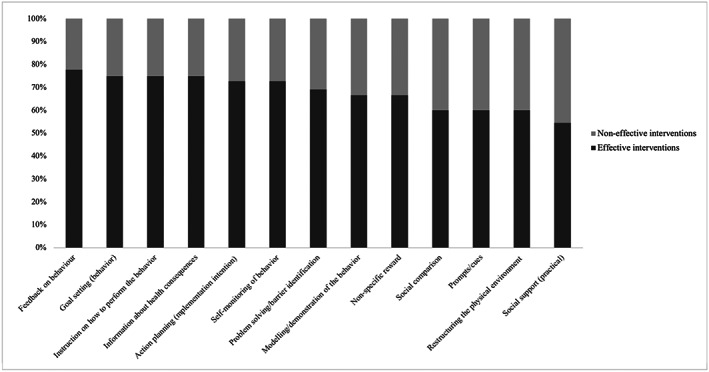
Percentage effectiveness of behavior change techniques (BCTs)
4. DISCUSSION
The aims of the current review were twofold: (a) to examine the effectiveness of behavioral interventions aimed at reducing SSB intake among 12‐ to 18‐year socioeconomically disadvantaged ethnic minority adolescents and (b) to identify which BCTs contribute to a reduction in SSB intake in this target group. In total, 22 studies aiming to reduce SSB intake were identified, of which 19 were included in a meta‐analysis. Most importantly, the most effective BCTs identified in the narrative synthesis of this review were feedback on behavior, goal‐setting of behavior, instruction on how to perform the behavior, information about health consequences, action planning including implementation intention, self‐monitoring of behavior, problem‐solving and/or barrier identification and modelling/demonstration of the behavior.
Overall, our meta‐analysis showed that behavioral interventions were not effective in reducing SSB intake, which is in line with another systematic review and meta‐analysis. 27 In their meta‐analysis, Champion et al. 27 included four studies and found no evidence found no evidence of effectiveness of interventions on reducing SSB intake. However, in their review, Champion et al. 27 included adolescents from the general population, used only one SSB measure, and included only school‐based eHealth interventions. Further, in contrast to our meta‐analysis, the meta‐analyses of two previous reviews 4 , 28 reported that behavioral interventions lead to a small‐sized reduction in SSB intake, but with considerable heterogeneity.
There are several possible explanations for the mixed findings. First, previous reviews 4 , 27 , 28 included adolescents from the general population, whereas we primarily included disadvantaged minority adolescents, given that SSB intake is more common in these groups than in the general adolescent population. 3 Evidence suggests that one‐size‐fits‐all interventions that are delivered in the same way to advantaged and disadvantaged groups may unintentionally lead to intervention‐generated inequalities. 22 White et al. 65 state that resultant inequalities can be generated at multiple points throughout the intervention process. For instance, compliance with behavioral interventions may be lower among underserved groups because they lack resources (e.g., finances and knowledge), are less health‐conscious and have less supportive social and physical environments. The corollary is that interventions that are tailored to the needs of these groups will more likely be effective to change dietary behaviors. Moreover, underserved adolescents are often underrepresented in intervention studies because they are difficult to recruit and generally often hard to reach. A possible reason for why these groups may not engage in intervention studies is because they are hindered by pressing daily struggles. Daily struggles such as coming from poor households, residing in unstable social and physical environments, perceiving discrimination, and dealing with financial scarcity can impose burdens on the mind, leaving less ‘mental’ room which in turn can deflect the adolescents' interests to change their unhealthy dietary behaviors. 66 Second, another factor that can explain the observed difference in findings is possibly related to the heterogeneity in the measures of SSBs used. For example, previous reviews 4 , 27 , 28 only included studies that reported volumetric measures of SSB intake (e.g., ml of SSBs consumed per day/week). In contrast to these reviews, given that there is no consensus on a clear definition of SSB intake, we did not set any criteria on how individual consumption of SSB needed to be reported in the articles. For the current meta‐analysis, we considered frequency measures of SSB intake (e.g., SSB consumed per day) and proportion of individuals who reported consuming a given quantity of SSB. Moreover, given the definition of SSBs, which includes a host of drinks such as soda, diet drinks, flavoured juice drinks, sports drinks and sweetened coffee and tea, 4 we also included effect estimates reported either individually for each type of SSB (e.g., soft drinks and energy drinks) or collectively (e.g., all types of SSB grouped into one category). Finally, in contrast to the review by Champion et al., 27 we included behavioral interventions implemented at the household, neighborhood, school, store and community levels.
In the narrative review, we compared individual BCTs in effective and non‐effective interventions to identify BCTs that were associated with intervention effectiveness. Thirteen BCTs had an effectiveness ratio >50% of which five included the self‐regulatory BCTs derived from the control theory. 67 These included feedback on behavior (n = 8/9, 78%), goal‐setting of behavior (n = 9/12, 75%), action planning including implementation intention (n = 8/11, n = 73%), self‐monitoring of behavior (n = 8/11, 73%) and problem solving and/or barrier identification (n = 9/13, 69%). An example of the BCT feedback on behavior, is to provide tailored feedback on whether or not participants met their goal of drinking less SSBs per week, to provide evaluative feedback on participants progress of drinking less SSBs per week or providing informative feedback with strategies on how to overcome barriers to reduce SSB intake. Examples of the BCTs goal‐setting, action planning including implementation intention, self‐monitoring and problem‐solving and/or barrier identification are (a) to specify and set a goal to reduce individual SSB intake by one serving per day or per week; (b) to make a plan and specify when and where one would consume less SSBs; (c) to record and monitor one's SSB intake; and (d) to provide situations where consuming less SSBs would be challenging and prompt participants to identify solutions and strategies to overcome barriers preventing them from drinking less SSBs. These results are comparable with previous reviews and meta‐analyses, which found that self‐regulatory BCTs were associated with better dietary and physical activity behavior. 29 , 63 , 68 , 69 , 70 , 71 Further, the BCTs instruction on how to perform a behavior (n = 6/8, 75%) and information about health consequences (n = 12/16, 75%) were also found to be effective. An example of the BCT provision of instruction is to provide participants specific instructions on how they can reduce their SSB intake. The effectiveness of the BCT providing instruction is similar to another review supporting the efficacy of providing instructions for improving dietary outcomes in adults. 72 The BCT health consequences can be used, for example, to provide factual information on health consequences related to prolonged intake of SSBs. In a comparable review, this BCT was commonly used in educational/behavioral school‐based interventions. 29
This review has several strengths. To the best of our knowledge, no review to date has examined the effectiveness of behavioral interventions targeting SSB intake in socioeconomically disadvantaged ethnic minority adolescents. Further, the novelty of this review is that we are the first to explore which BCTs are associated with effective interventions in this diverse sample of adolescents. This is another strength, just as the robust method applied to code the BCTs, using the most comprehensive taxonomy available.
Although the findings of this review and meta‐analysis add new knowledge to the scientific literature, there are several limitations that need to be addressed. First, our meta‐analysis was based on a small number of studies, and significant heterogeneity was present between the studies. Second, high or unclear risk existed regarding blinding of assessors, randomization allocation and concealment of participants/research staff, and overall, we deemed the risk of bias to be moderate to high for RCTs and low to moderate for non‐RCTs. Third, given the insufficient quantity of studies, it was not possible to conduct proper moderator analyses. Instead, we conducted exploratory analyses to assess the impact of potential moderators. However, due to the considerable amount of heterogeneity observed, the findings of these analyses should be interpreted with caution. Fourth, given that different BCTs and theoretical frameworks were used in included studies, it was not possible to examine, for instance, which specific BCTs and BCT combinations were effective in reducing SSB intake. Fifth, examining the long‐term maintenance of the effects of behavioral interventions on SSB intake was not possible in the meta‐analysis because most studies had short follow up. Sixth, coding of BCTs was problematic due to inconsistencies in reporting of BCTs. In this review, a stringent coding strategy was used. A BCT was coded as present, only if it was sufficiently described or the authors referred to a BCT taxonomy. The problematic issue related to coding of BCTs has been identified in previous reviews. 63 , 64 Further, there was an overrepresentation of studies conducted in the USA, which limits generalizability to other contexts (e.g., built environment) and continents (e.g., differences in cultural and migration history of minorities in Europe). Finally, only studies reported in English were reviewed, meaning eligible studies in other languages may have been missed.
This review highlights important directions for future research. First, more high‐quality studies examining the effectiveness of behavioral interventions among disadvantaged minority adolescents are warranted. Second, future research should consider the unique conditions and background factors (self‐efficacy, cultural values and norms) that characterize this target group when designing interventions for them. Third, given that a large part of the heterogeneity remains unexplained, well‐powered future studies are needed to conduct proper subgroup analyses to identify potential moderators influencing intervention effectiveness. Fourth, because it was not possible to identify which specific BCTs or BCT combinations were effective in changing SSB behavior, future investigation is warranted. Moreover, although 77% of the included studies reported using a theoretical framework, there was inconsistent and incomplete information on how different theories were operationalized in intervention design and implementation of the included studies. Thus, future work should be transparent and provide complete information on how specific types of theory/theories are used in intervention design and implementation of behavioral interventions targeting underserved adolescents. Fifth, given that long‐term effects of included behavioral interventions could not be explored, additional research is needed to examine whether changes in SSB behavior are sustained over time. Sixth, to help identify active BCTs, future research should provide a checklist of BCTs used in their studies as supplementary materials. This will not only ease the process of identifying active BCTs but will also aid in the development of possibly effective and replicable behavioral interventions.
Further, this review demonstrates several BCTs in reducing SSB intake in underserved adolescents. Based on the narrative synthesis, individual BCTs with greater effectiveness were those that targeted participants' self‐regulatory skills such as feedback on behavior, goal‐setting, self‐monitoring, action planning including implementation intention and problem‐solving/barrier identification. Overall, these findings suggest that providing individuals personalized feedback which they can translate into behavior change as well as enhancing their self‐regulatory capacity to make them more autonomous about their own behaviors may be more effective rather than offering them generic behavioral interventions. Therefore, in order to effectively facilitate behavior change, researchers should consider incorporating skill‐building and self‐regulatory BCTs not only to curb SSB intake but also to avoid unintended consequences (i.e., increased intake of sports drinks or energy drinks). Possible ways to curb SSB intake and avoid unintended consequences could be, for example, to promote consumption of tap water, provide tap water access (installing bottle fillers/fountain drinking water units) or to provide bottled water coolers installed within schools. Finally, given the heterogeneous nature of the included studies, studies reported changes in SSB intake differently. For example, some studies reported changes in one or more than one type of SSBs, had unclear totals for SSBs or had unclear definition of SSBs. Thus, it is plausible, for example, that while frequency of SSB intake reduced, volumetric measures of SSBs or an intake in other SSBs (e.g., sport drinks and energy drinks that are popular among adolescents) increased, which were not measured or reported. Therefore, given the lack of consensus on how to measure individual SSB intake, it is important that efforts are made to establish a clear definition of SSB. In addition, given that different types of SSBs exists, authors are encouraged to include all types of SSBs that meet the definition of SSB and report the impact of an intervention on each type of SSB separately as this will facilitate a better understanding of the kind of effect behavioral interventions would have on the different types of SSBs.
In sum, the findings of the review indicate that behavioral interventions that may be effective for the general adolescent population may not be effective for socioeconomically disadvantaged ethnic minority adolescents. Thus, further high quality‐research is needed to develop behavioral interventions tailored to the needs of this target group to effectively reduce SSB intake. Further, our findings demonstrate that self‐regulatory BCTs congruent with the control theory may be effective components for reducing SSB intake in underserved adolescents. However, given the lack of studies including each BCT, this review could not identify active BCTs associated with intervention effectiveness. Thus, more research is needed before confirming which BCTs can be considered having a greater effect than others.
CONFLICT OF INTEREST STATEMENT
The authors have no relevant interests to declare.
AUTHOR CONTRIBUTION
S. S. and E. G. contributed to the original idea and research questions to be reviewed. S. S. and E. G. wrote the initial draft of the manuscript. S. S. was involved in data extraction, coding and interpretation of BCTs, determined methodological quality of included studies, analysed the data and contributed to the subsequent drafts of the manuscript. J. J. was involved in all statistical analyses. A. S., G. N., J. W. and S. D. provided essential guidance and supervision at all stages of the review. All authors have read and approved the final manuscript.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the assistance of the biomedical information specialist, Mr Wichor Bramer from the Erasmus Medical University, in conducting the literature search for this review.
Shagiwal SS, Groenestein E, Schop‐Etman A, et al. Effectiveness of behavioral interventions and behavior change techniques for reducing soft drink intake in disadvantaged adolescents: A systematic review and meta‐analysis. Obes Sci Pract. 2020;6:708–734. 10.1002/osp4.452
REFERENCES
- 1. Wright CM, Parker L, Lamont D, Craft AW. Implications of childhood obesity for adult health: findings from thousand families cohort study. BMJ. 2001;323:1280‐1284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wang Y, Beydoun MA. The obesity epidemic in the United States—gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta‐regression analysis. Epidemiol Rev. 2007;29:6‐28. [DOI] [PubMed] [Google Scholar]
- 3. Krueger PM, Reither EN. Mind the gap: race/ethnic and socioeconomic disparities in obesity. Curr Diab Rep. 2015;15(11):95 10.1007/s11892-015-0666-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Vargas‐Garcia EJ, Evans CEL, Prestwich A, Sykes‐Muskett BJ, Hooson J, Cade JE. Interventions to reduce consumption of sugar‐sweetened beverages or increase water intake: evidence from a systematic review and meta‐analysis. Obes Rev. 2017;18:1350‐1363. [DOI] [PubMed] [Google Scholar]
- 5. Deren K, Weghuber D, Caroli M, et al. Consumption of sugar‐sweetened beverages in paediatric age: a position paper of the European Academy of Paediatrics and the European Childhood Obesity Group. Ann Nutr Metab. 2019;74:296‐302. [DOI] [PubMed] [Google Scholar]
- 6. Luger M, Lafontan M, Bes‐Rastrollo M, Winzer E, Yumuk V, Farpour‐Lambert N. Sugar‐sweetened beverages and weight gain in children and adults: a systematic review from 2013 to 2015 and a comparison with previous studies. Obes Facts. 2017;10:674‐693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Story M, Neumark‐Sztainer D, French S. Individual and environmental influences on adolescent eating behaviors. J Am Diet Assoc. 2002;102:S40‐S51. [DOI] [PubMed] [Google Scholar]
- 8. Watts AW, Miller J, Larson NI, Eisenberg ME, Story MT, Neumark‐Sztainer D. Multicontextual correlates of adolescent sugar‐sweetened beverage intake. Eat Behav. 2018;30:42‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lee H, Harris KM, Lee J. Multiple levels of social disadvantage and links to obesity in adolescence and young adulthood. J Sch Health. 2013;83:139‐149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Desbouys L, Mejean C, De Henauw S, Castetbon K. Socio‐economic and cultural disparities in diet among adolescents and young adults: a systematic review. Public Health Nutr. 2019;1‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Mackenbach JD, Nelissen KGM, Dijkstra SC, et al. A systematic review on socioeconomic differences in the association between the food environment and dietary behaviors. Nutrients. 2019;11(9):2215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bogart LM, Cowgill BO, Sharma A, et al. Parental and home environmental facilitators of sugar‐sweetened beverage consumption among overweight and obese Latino youth. Acad Pediatr. 2013;13(4):348‐355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Cialdini RB, Goldstein NJ. Social influence: compliance and conformity. Annu Rev Psychol. 2004;55:591‐621. [DOI] [PubMed] [Google Scholar]
- 14. Harris J. Where is the child's environment: a group socialization theory of development. Psychol Rev. 1995;102:458‐489. [Google Scholar]
- 15. Calloway EE, Parks CA, Bowen DJ, Yaroch AL. Environmental, social, and economic factors related to the intersection of food security, dietary quality, and obesity: an introduction to a special issue of the Translational Behavioral Medicine journal. Transl Behav Med. 2019;9:823‐826. [DOI] [PubMed] [Google Scholar]
- 16. Kumanyika S, Grier S. Targeting interventions for ethnic minority and low‐income populations. Future Child. 2006;16:187‐207. [DOI] [PubMed] [Google Scholar]
- 17. Cassady DL, Liaw K, Miller LM. Disparities in obesity‐related outdoor advertising by neighborhood income and race. J Urban Health. 2015;92:835‐842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Timmermans J, Dijkstra C, Kamphuis C, et al. ‘Obesogenic’ school food environments? An urban case study in the Netherlands. Int J Environ Res Public Health. 2018;15(4):1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Muth N, Dietz W, Magge S, et al. American Academy of Pediatrics, Section on Obesity, Committee on Nutrition, American Heart Association. Public policies to reduce sugary drink consumption in children and adolescents. Pediatrics. 2019;143(4):e20190282. [DOI] [PubMed] [Google Scholar]
- 20. Robertson A. Obesity and inequities. Guidance for addressing inequities in overweight and obesity. World Health Organization. 2014. http://www.euro.who.int/en/publications/abstracts/obesity-and-inequities.-guidance-for-addressing-inequities-in-overweight-and-obesity
- 21. Hansen PG, Skov LR, Skov KL. Making healthy choices easier: regulation versus nudging. Annu Rev Public Health. 2016;37:237‐251. [DOI] [PubMed] [Google Scholar]
- 22. Michie S, Jochelson K, Markham WA, Bridle C. Low‐income groups and behaviour change interventions: a review of intervention content, effectiveness and theoretical frameworks. J Epidemiol Community Health. 2009;63:610‐622. [DOI] [PubMed] [Google Scholar]
- 23. McGill R, Anwar E, Orton L, et al. Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health. 2015;15:457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Michie S, Carey RN, Johnston M, et al. From theory‐inspired to theory‐based interventions: a protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Ann Behav Med. 2018;52:501‐512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Michie S, Richardson M, Johnston M, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46:81‐95. [DOI] [PubMed] [Google Scholar]
- 27. Champion K, Parmenter B, McGowan C, et al. Effectiveness of school‐based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: a systematic review and meta‐analysis. Lancet Digit Health. 2019;1:e206‐e221. [DOI] [PubMed] [Google Scholar]
- 28. Rahman A, Jomaa L, Kahale LA, Adair P, Pine C. Effectiveness of behavioral interventions to reduce the intake of sugar‐sweetened beverages in children and adolescents: a systematic review and meta‐analysis. Nutr Rev. 2018;76:88‐107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Vezina‐Im LA, Beaulieu D, Belanger‐Gravel A, et al. Efficacy of school‐based interventions aimed at decreasing sugar‐sweetened beverage consumption among adolescents: a systematic review. Public Health Nutr. 2017;20:2416‐2431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62:e1‐e34. [DOI] [PubMed] [Google Scholar]
- 31. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343(7829):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Wells G, Shea B, O'Connell D, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of non‐randomised studies in meta‐analyses. 2014.
- 33. Bogart LM, Elliott MN, Uyeda K, Hawes‐Dawson J, Klein DJ, Schuster MA. Preliminary healthy eating outcomes of SNaX, a pilot community‐based intervention for adolescents. J Adolesc Health. 2011;48:196‐202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Collins CE, Dewar DL, Schumacher TL, Finn T, Morgan PJ, Lubans DR. 12 Month changes in dietary intake of adolescent girls attending schools in low‐income communities following the NEAT Girls cluster randomized controlled trial. Appetite. 2014;73:147‐155. [DOI] [PubMed] [Google Scholar]
- 35. Contento IR, Koch PA, Lee H, Calabrese‐Barton A. Adolescents demonstrate improvement in obesity risk behaviors after completion of choice, control & change, a curriculum addressing personal agency and autonomous motivation. J Am Diet Assoc. 2010;110:1830‐1839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Contento IR, Koch PA, Lee H, Sauberli W, Calabrese‐Barton A. Enhancing personal agency and competence in eating and moving: formative evaluation of a middle school curriculum‐choice, control, and change. J Nutr Educ Behav. 2007;39:S179‐S186. [DOI] [PubMed] [Google Scholar]
- 37. Haerens L, De Bourdeaudhuij I, Maes L, Vereecken C, Brug J, Deforche B. The effects of a middle‐school healthy eating intervention on adolescents' fat and fruit intake and soft drinks consumption. Public Health Nutr. 2007;10:443‐449. [DOI] [PubMed] [Google Scholar]
- 38. Dubuy V, De Cocker K, De Bourdeaudhuij I, et al. Evaluation of a real world intervention using professional football players to promote a healthy diet and physical activity in children and adolescents from a lower socio‐economic background: a controlled pretest‐posttest design. BMC Public Health. 2014;14:457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. French SA, Gerlach AF, Mitchell NR, Hannan PJ, Welsh EM. Household obesity prevention: take action—a group‐randomized trial. Obesity (Silver Spring). 2011;19:2082‐2088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Lane H, Porter KJ, Hecht E, Harris P, Kraak V, Zoellner J. Kids SIP smartER: a feasibility study to reduce sugar‐sweetened beverage consumption among middle school youth in Central Appalachia. Am J Health Promot. 2018;32:1386‐1401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Majumdar D, Koch PA, Lee H, Contento IR, Islas‐Ramos AD, Fu D. “Creature‐101”: a serious game to promote energy balance‐related behaviors among middle school adolescents. Games Health J. 2013;2:280‐290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Neumark‐Sztainer DR, Friend SE, Flattum CF, et al. New moves‐preventing weight‐related problems in adolescent girls a group‐randomized study. Am J Prev Med. 2010;39:421‐432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Singh AS, Chin APMJ, Brug J, van Mechelen W. Dutch obesity intervention in teenagers: effectiveness of a school‐based program on body composition and behavior. Arch Pediatr Adolesc Med. 2009;163:309‐317. [DOI] [PubMed] [Google Scholar]
- 44. Smith JJ, Morgan PJ, Plotnikoff RC, et al. Smart‐phone obesity prevention trial for adolescent boys in low‐income communities: the ATLAS RCT. Pediatrics. 2014;134:e723‐e731. [DOI] [PubMed] [Google Scholar]
- 45. Smith LH, Holloman C. Piloting “sodabriety”: a school‐based intervention to impact sugar‐sweetened beverage consumption in rural Appalachian high schools. J Sch Health. 2014;84:177‐184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Spook J, Paulussen T, Kok G, van Empelen P. Evaluation of a serious self‐regulation game intervention for overweight‐related behaviors (“Balance It”): a pilot study. J Med Internet Res. 2016;18(9):225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. van Nassau F, Singh AS, Cerin E, et al. The Dutch Obesity Intervention in Teenagers (DOiT) cluster controlled implementation trial: intervention effects and mediators and moderators of adiposity and energy balance‐related behaviours. Int J Behav Nutr Phys Act. 2014;11(1):158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Whittemore R, Jeon S, Grey M. An internet obesity prevention program for adolescents. J Adolesc Health. 2013;52:439‐447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Winett R, Roodman A, Winett S. The effects of the Eat4Life internet‐based health behavior program on the nutrition and activity practices of high school girls. J Gender Culture Health. 1999;4:239‐254. [Google Scholar]
- 50. Ezendam N, Brug J, Oenema A. Evaluation of the web‐based computer‐tailored FATaintPHAT intervention to promote energy balance among adolescents: results from a school cluster randomized trial. Arch Pediatr Adolesc Med. 2012;166:248‐255. [DOI] [PubMed] [Google Scholar]
- 51. Foley BC, Shrewsbury VA, Hardy LL, et al. Evaluation of a peer education program on student leaders' energy balance‐related behaviors. BMC Public Health. 2017;17:695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Bleich SN, Barry CL, Gary‐Webb TL, Herring BJ. Reducing sugar‐sweetened beverage consumption by providing caloric information: how Black adolescents alter their purchases and whether the effects persist. Am J Public Health. 2014;104:2417‐2424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Bleich SN, Herring BJ, Flagg DD, Gary‐Webb TL. Reduction in purchases of sugar‐sweetened beverages among low‐income Black adolescents after exposure to caloric information. Am J Public Health. 2012;102:329‐335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. VanEpps EM, Roberto CA. The influence of sugar‐sweetened beverage warnings: a randomized trial of adolescents' choices and beliefs. Am J Prev Med. 2016;51:664‐672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Stat. 1950;21:607‐611. [Google Scholar]
- 56. Higgins JP, Thomas J, Chandler J, et al. (Eds). Cochrane Handbook for Systematic Reviews of Interventions. UK: John Wiley & Sons; 2019. [Google Scholar]
- 57. Cohen J. A power primer. Psychol Bull. 1992;112:155‐159. [DOI] [PubMed] [Google Scholar]
- 58. Hedges LV, Tipton E, Johnson MC. Robust variance estimation in meta‐regression with dependent effect size estimates. Res Synth Methods. 2010;1:39‐65. [DOI] [PubMed] [Google Scholar]
- 59. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Stat Med. 2002;21:1539‐1558. [DOI] [PubMed] [Google Scholar]
- 60. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ. 1997;315:629‐634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Rothstein H, Sutton AJ, Borenstein M. (Eds). Publication Bias in Meta‐analysis: Prevention, Assessment and Adjustments. Hoboken, NJ: John Wiley & Sons Inc; 2005:1–7. [Google Scholar]
- 62. Gardner B, Smith L, Lorencatto F, Hamer M, Biddle SJ. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health Psychol Rev. 2015;10:89‐112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Ashton LM, Sharkey T, Whatnall MC, et al. Effectiveness of interventions and behaviour change techniques for improving dietary intake in young adults: a systematic review and meta‐analysis of RCTs. Nutrients. 2019;11(4):825 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Martin J, Chater A, Lorencatto F. Effective behaviour change techniques in the prevention and management of childhood obesity. Int J Obes (Lond). 2013;37:1287‐1294. [DOI] [PubMed] [Google Scholar]
- 65. White M, Adams J, Heywood P. How and why do interventions that increase health overall widen inequalities within populations? In: Babones SJ, ed. Social Inequality and Public Health. Bristol: Policy Press; 2013:65‐82. [Google Scholar]
- 66. Mullainathan S, Shafir E. (Eds). Scarcity: Why Having too Little Means so Much. Macmillan; 2013. [Google Scholar]
- 67. Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality‐social, clinical, and health psychology. Psychol Bull. 1982;92:111‐135. [PubMed] [Google Scholar]
- 68. Deliens T, Van Crombruggen R, Verbruggen S, De Bourdeaudhuij I, Deforche B, Clarys P. Dietary interventions among university students: a systematic review. Appetite. 2016;105:14‐26. [DOI] [PubMed] [Google Scholar]
- 69. Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta‐regression. Health Psychol. 2009;28:690‐701. [DOI] [PubMed] [Google Scholar]
- 70. Plotnikoff RC, Costigan SA, Williams RL, et al. Effectiveness of interventions targeting physical activity, nutrition and healthy weight for university and college students: a systematic review and meta‐analysis. Int J Behav Nutr Phys Act. 2015;12(1):1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta‐regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Whatnall MC, Patterson AJ, Ashton LM, Hutchesson MJ. Effectiveness of brief nutrition interventions on dietary behaviours in adults: a systematic review. Appetite. 2018;120:335‐347. [DOI] [PubMed] [Google Scholar]