

Abstract
Reninoma (juxtaglomerular cell tumor) is a rare cause of renin-mediated hypertension. We reported a 18 year old woman with history of hypertension for 3 years. Laboratory findings showed severe hypokalemia and markedly increased levels of renin and aldosterone. Kidney ultrasonography, abdominal computed tomography and magnetic resonance imaging revealed a small mass in the middle region of the right kidney.
The patient underwent nephron-sparing surgery; immunohistochemical results demonstrated typical features of reninoma. Postoperatively, blood pressure and potassium levels were normal at 1 month follow-up.
Keywords: hypertension, renin, reninoma, juxtaglomerular cell tumor, hypokalemia
INTRODUCTION
Reninoma, or renal juxtaglomerular apparatus tumor (JGA), is a rare benign renal neoplasm, but a well-described cause of secondary hypertension, characterized by excessive renin secretion causing secondary hypertension and hypokalemia (1).
Reninomas are usually diagnosed in adolescents and young adults. Reninoma-mediated hypertension is surgically treatable and should be considered for diagnosis in patients with high renin activity, refractory hypertension, and hypokalemia.
In this paper, we describe the case of reninoma in an adolescent girl who presented with a 3 years history of hypertension.
CASE REPORT
A 18 year-old woman was referred to our hospital for exploration of hypertension. She had been diagnosed with hypertension 3 years ago and was treated with angiotensin II receptor blocker (ARB) and calcium channel blocker. She had no personal or family history.
On admission blood pressure was 160/95 mmHg (with maximal values of BP up to 200 /100 mmHg during hospitalization) hypokalemia at 2.7 mEq/L, natremia was at 137 mEq/L, serum creatinine level was normal. Echocardiography was normal, without evidence of heart failure or aortic coarctation.
Target organ damage evaluation did not reveal any anomaly, urinary metanephrine levels were within normal range.
We therefore assessed plasma renin and aldosterone levels after all antihypertensive drugs had been withdrawn, plasma immunoreactive renin plasma (kit RIA of Cisbio) and aldosterone (kit RIA of Beckman Coulter) levels in supine position were 334.2 mUI/L (9-72) and 474 pg/mL (67-335) respectively. The results steered us towards a diagnosis of secondary aldosteronism with excess renin secretion.
Renal Doppler ultrasonography did not reveal direct or indirect signs of renal artery stenosis (normal velocimetric curves and resistivity index in each artery), computed tomography (CT) showed a homogeneous mass of 26 mm in size, in the middle pole of the right kidney. Magnetic resonance imaging (MRI) also revealed a 28 mm mass hypointense on T1-weighted image and a heterogeneous high signal in T2-weighted image (Fig. 1).
Figure 1.

T2 weighted magnetic resonance image.
However, selective venous sampling failed to show any significant difference in the renin levels between the right and the left renal vein (Table 1).
Table 1.
Renal vein sampling
| Sample | Renin level (RIA) | Ratio dominant /non-dominant | |
|---|---|---|---|
| Pre-captopril | Peripheral | 125 pg/mL | 1.07 |
| Left renal vein | 127 pg/mL | ||
| Right renal vein | 136 pg/mL | ||
| Post-captopril | Peripheral | 141 pg/mL | 1.04 |
| Left renal vein | 141 pg/mL | ||
| Right renal vein | 148 pg/mL |
The right kidney tumor was removed by partial nephrectomy. Gross examination of the specimen demonstrated a well-encapsulated, cortically based lesion measuring 3 cm in diameter (Fig. 2). The cut surface was gray-white in color, and hemorrhagic areas were identified. On microscopic examination the tumor cells were uniform with round nuclei and eosinophilic granular cytoplasm (Fig. 3). All tumor cells stained positive for CD34 (Fig. 4), but were negative for HMB-45, melanin A, cytokeratin and smooth muscle actin. Constellation of these histological and immunohistochemical features was consistent with the diagnosis of juxtaglomerular cell tumor (reninoma).
Figure 2.
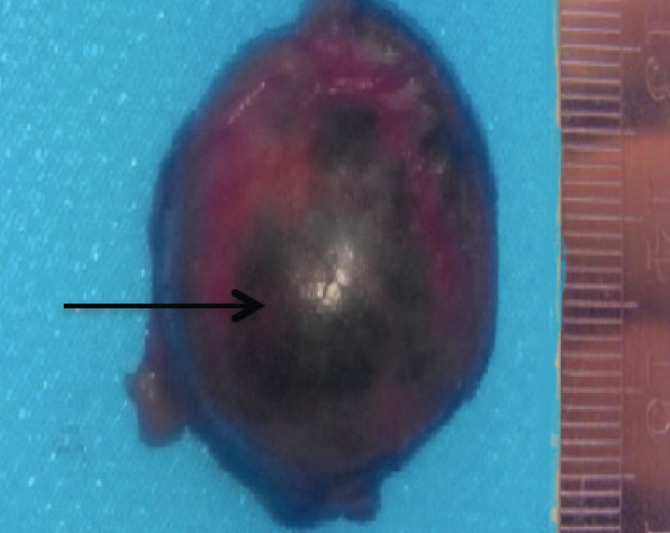
Gross examination with foci of haemorrhage (arrow).
Figure 3.

Microscopic examination: round or oval cells with abundant eosinophilic cytoplasm and hemangiopericytic vascularisation.
Figure 4.

Tumor cells stained positive for CD34.
One week after tumor resection, serum potassium level (4.5 mmol/L) returned to normal. Ambulatory blood pressure monitoring was completely normal without any antihypertensive agent after 1 month, and the level of plasma immunoreactive renin and aldosterone decreased to 50 mUI/L (9-72) and 290 pg/mL (67-335) respectively.
DISCUSSION
Reninoma is a rare case of secondary hypertension. The first case was described by Robertson in 1967 (1). Approximately 100 cases of reninoma have been published to date (2-4). Mean age at diagnosis was 27 years (range 6 -69 years) (3). The most common symptom among patients diagnosed with reninoma is headache (3, 5), followed by dizziness, nausea, polyuria, and nocturia. Mean blood pressure of reported reninoma patients is 201/130 mm Hg with a mean duration of hypertension of 47 months (range: 0–23 years; median: 24 months)(3).
Hypokalemia was detected in 85% of previously reported patients, with a mean serum K level of 2.9 mEq/L (6). Imaging tools are used to diagnose and localize the renal mass. Kidney ultrasonography and Doppler study is the first choice in the search for a renal mass or artery stenosis. These are hypoechoic, homogeneous, sometimes isoechoic formations with adjacent parenchyma (7). These tumours are not always found by this examination.
Computed tomography is the most reliable method for tumor localization (7). Unenhanced scans may not detect small isodense lesions. MRI is also highly effective in differential diagnosis between reninoma and other renal tumors.
Renal venous sampling seems to be a reliable diagnostic tool for the lateralization of the tumor by differences of plasma renin activity of at least 1.5 (3). Moreover, in some case reports, the renal vein catheterisation failed to provide adequate localisation of the tumor (8), essentially located at the surface of the kidney, when most of the tumor blood is collected into the peripheral veins and not in the renal vein (5, 7). This is the case of our patient.
Conservative surgery is justified because these tumors are mostly benign. Only one metastatic case has been reported to date (9).
Reninoma is usually confirmed by either positive immune-staining of renin or electron microscopic identification of renin granules (10). Specific immunohistochemical appearance of reninoma is positive staining for renin, actin, vimentin, and CD34 (11). These histologic findings are typical and help to diagnose differentially between JCT and other renal tumors. The most specific electron microscopic findings are rhomboid crystalline protogranules or amorphous homogeneous, electron-dense mature granules.
In conclusion, the discovery of a juxtaglomerular cell tumor constitutes a life-saving diagnosis for the patient.
Reninoma should be considered in patients with refractory hypertension with or without hypokalemia and high renin activity. Endocrine tests and imaging studies are helpful in identifying the lesion. Nephron-sparing surgery is becoming the preferred treatment.
Conflict of interest
The authors declare that they have no conflict of interest.
References
- 1.Robertson P, Klidjian A, Harding L, Walters G, Lee M, Robb-Smith A. Hypertension due to a renin-secreting renal tumour. The American Journal of Medicine. 1967;43(6):963–976. doi: 10.1016/0002-9343(67)90256-2. [DOI] [PubMed] [Google Scholar]
- 2.Kuroda N, Maris S, Monzon FA, Tan PH, Thomas A, Petersson FB, Gatalica Zoran, Ghazalpour Anatole, Ryan P. Bender, Petr Grossmann, Michal Michal, Marian Svajdler, Zdenka Ovcak, Milan Hora,Ondrej Hes. Juxtaglomerular cell tumor: a morphological, immunohistochemical and genetic study of six cases. Human Pathology. 2013;44(1):47–54. doi: 10.1016/j.humpath.2012.04.006. [DOI] [PubMed] [Google Scholar]
- 3.Wong L, Hsu TH, Perlroth MG, Hofmann LV, Haynes CM, Katznelson L. Reninoma: case report and literature review. Journal of Hypertension. 2008;26(2):368–373. doi: 10.1097/HJH.0b013e3282f283f3. [DOI] [PubMed] [Google Scholar]
- 4.Gu WJ, Zhang LX, Jin N, Ba JM, Dong J, Wang DJ, Li J, Wang XL, Yang GQ, Lu ZH, Dou JT, Lu JM, Mu YM. Rare and curable renin-mediated hypertension: a series of six cases and a literature review. Journal of Pediatric Endocrinology and Metabolism. 2015 doi: 10.1515/jpem-2015-0025. [DOI] [PubMed] [Google Scholar]
- 5.Gottardo F, Cesari M, Morra A, Gardiman M, Fassina A, Dal Bianco M. A kidney tumor in an adolescent with severe hypertension and hypokalemia: an uncommon case–case report and review of the literature on reninoma. Urologia Internationalis. 2010;85(1):121–124. doi: 10.1159/000314339. [DOI] [PubMed] [Google Scholar]
- 6.Friedman K, Wallis T, Maloney KW, Hendrickson RJ, Mengshol S, Cadnapaphornchai MA. An unusual cause of pediatric hypertension. The Journal of Pediatrics. 2007;151(2):206–212. doi: 10.1016/j.jpeds.2007.04.015. [DOI] [PubMed] [Google Scholar]
- 7.Corvol P, Pinet F, Plouin P-F, Bruneval P, Menard J. Renin-secreting tumors. Endocrinology and Metabolism Clinics of North America. 1994;23(2):255–270. [PubMed] [Google Scholar]
- 8.Baruch D, Corvol P, Alhenc-Gelas F, Dufloux M, Guyenne T, Gaux J-C, Raynaud A, Brisset J M, Duclos JM, Menard J. Diagnosis and treatment of renin-secreting tumors. Report of three cases. Hypertension. 1984;6(5):760–766. doi: 10.1161/01.hyp.6.5.760. [DOI] [PubMed] [Google Scholar]
- 9.Duan X, Bruneval P, Hammadeh R, Fresco R, Eble JN, Clark JI, Vigneswaran W T, Flanigan R C, Picken M M. Metastatic juxtaglomerular cell tumor in a 52-year-old man. The American Journal of Surgical Pathology. 2004;28(8):1098–1102. doi: 10.1097/01.pas.0000126722.29212.a7. [DOI] [PubMed] [Google Scholar]
- 10.Lindop G, Stewart J, Downie T. The immunocytochemical demonstration of renin in a juxtaglomerular cell tumour by light and electron microscopy. Histopathology. 1983;7(3):421–431. doi: 10.1111/j.1365-2559.1983.tb02255.x. [DOI] [PubMed] [Google Scholar]
- 11.Kim HJ, Kim CH, Choi YJ, Ayala AG, Amirikachi M, Ro JY. Juxtaglomerular cell tumor of kidney with CD34 and CD117 immunoreactivity: report of 5 cases. Archives of Pathology & Laboratory Medicine. 2006;130(5):707–711. doi: 10.5858/2006-130-707-JCTOKW. [DOI] [PubMed] [Google Scholar]