

Abstract
OBJECTIVES:
To develop and test the validity and reliability of an Arabic version of the psychosocial impact of dental aesthetics questionnaire (PIDAQ).
MATERIALS AND METHODS:
The original English version was translated into Arabic, back-translated, pre-tested, and cross-culturally adapted before being administered to 205 individuals aged between 18–30 years from Medina, Saudi Arabia. Cronbach's alpha coefficient was used to test internal consistency, and the intraclass correlation coefficient (ICC) was used to assess test–retest reliability. Construct validity was assessed using factor analysis, and convergent validity was tested by comparing PIDAQ scores to the aesthetic components of the Dental Aesthetic Index (DAI) and Aesthetic Component of the Index of Orthodontic Treatment Need (IOTN-AC), while discriminant validity was assessed by comparing PIDAQ scores to participants' self-evaluation of orthodontic treatment need. Gender and age differences in the PIDAQ score were assessed.
RESULTS:
Cronbach's alpha coefficient was 0.940, corrected item-total correlation coefficients were between 0.509 and 0.719, and the ICC was 0.937. Principal component factor analysis extracted three domains, and factor loading ranged from 0.563 to 0.843. Total PIDAQ score and subscale scores had significant correlations with the DAI and IOTN-AC. The questionnaire discriminated well between participants who had a perceived need for orthodontic treatment and those with no perceived need. There were no significant age or gender differences in participants' PIDAQ scores.
CONCLUSIONS:
The Arabic version of the PIDAQ had excellent psychometric properties with sufficient reliability and validity to be used for the assessment of the orthodontic-related quality of life in young Arab adults.
Keywords: Aesthetics, Arabic psychometric tool, malocclusion, oral health-related quality of life, orthodontics
Introduction
The concept of oral health-related quality of life (OHRQoL) describes how oral health conditions affect individuals' general health and psychosocial well-being.[1,2] Oral health problems, such as malocclusion, negatively impact patients' quality of life.[3] Malocclusion affects not only patients' facial appearance and oral function but also their social interaction and self-confidence.[4] The social and psychological impacts of malocclusion are usually the major factors that motivate patients to seek orthodontic care.[5] An ideal orthodontic assessment, therefore, should allow for a subjective evaluation of OHRQoL, including patients' satisfaction concerning their malocclusion.[6] Assessing OHRQoL related to malocclusion provides a valid parameter to evaluate patients' perceptions of their need for orthodontic treatment[7,8] and to focus on appropriate treatment goals and outcomes beyond the limits of traditional clinician-based diagnostic measurements.[9]
Increased focus on the importance of OHRQoL for dental research and clinical practice has resulted in the development of various instruments to measure such information.[10] In 2006, Klages et al.[11] developed a questionnaire called the psychosocial impact of dental aesthetics questionnaire (PIDAQ), which is a valuable tool that measures OHRQoL in orthodontic patients. The PIDAQ gives valid and reliable information on patients' perceptions of their psychosocial well-being in terms of malocclusion. The PIDAQ was originally constructed to measure OHRQoL relating to malocclusion in young adults, as they are generally more concerned about aesthetics than older age groups and have a more stable self-concept than younger individuals.[11]
The PIDAQ, like most questionnaires, was developed in the English language, so the application of this tool in non-English speaking countries requires the development of an appropriate translation, including cultural and social adaptation without the loss of its psychometric properties.[12] Many translated versions of the PIDAQ have been developed and tested for their reliability and validity.[12,13,14,15] However, to the authors' best knowledge, there is no Modern Standard Arabic version of the PIDAQ. Modern Standard Arabic is the official language in all Arab countries, which includes most countries in the Middle East and North Africa. A Moroccan Arabic version of the PIDAQ has been published,[14] but this version was designed in Moroccan Arabic dialect, which restricts its use to the Moroccan population. A large number of people worldwide have Arabic as their first language, and this type of questionnaire is important, so the main aim of this study was to provide a psychosocial tool in Modern Standard Arabic that assesses orthodontics-related OHRQoL by translating, validating, and culturally adapting the original PIDAQ for young Arab adults.
Materials and Methods
Ethics approval
This study was a descriptive cross-sectional validation study. The Research Ethics Committee of Taibah University College of Dentistry (TUCD-REC) approved this study with reference number (TUCDREC2017O329RAHarbi). All participants were volunteers and written informed consent was obtained before examinations and questionnaire administration.
PIDAQ description
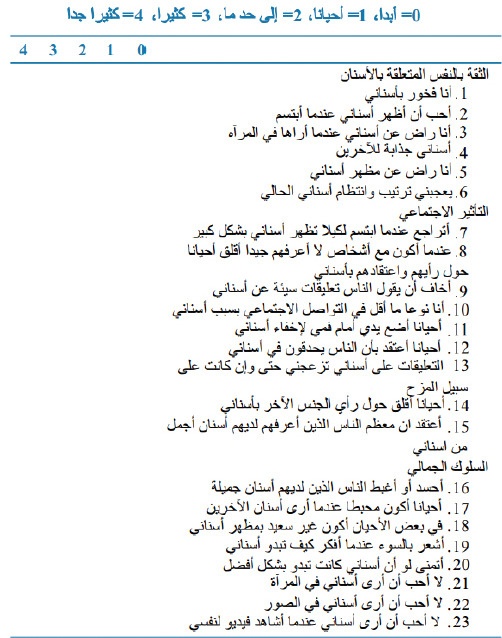
The PIDAQ is a 23-item psychometric scale.[11] The original version is composed of four subscales. These include one positive domain, dental self-confidence (six items), and three negative domains, social impact (eight items), psychological impact (six items), and esthetic concern (three items). A 5-point Likert scale is used for each item from 0 (not at all) to 1 (a little), 2 (somewhat), 3 (strongly), and 4 (very strongly). A score of 0 means that the item has no impact on the quality of life, while a score of 4 means that the item has the maximum impact on the quality of life. Scores from the positive domain are reversed to align them with scores from the other domains to produce a consistent measure of impact and to facilitate interpretation of the results.
Development of the Arabic version of the PIDAQ
Translation
The questionnaire was independently translated into Modern Standard Arabic by an orthodontist, a postgraduate dental student, and a dental student, all of whom were proficient in English and Arabic. The three versions were then discussed and evaluated. A translation for every item was agreed, forming the initial draft of the Arabic version of the PIDAQ.
Back translation
The draft was independently back-translated into English by two bilingual English teachers, both of whom were uninformed about the original scale. After back-translation, the teachers were given the original English version of the PIDAQ, which they compared with the back-translation, modifying it as necessary. This produced version I of the Arabic version of the PIDAQ.
Cross-cultural adaptation
A linguist, an orthodontist, and postgraduate dental students were asked for their comments on the popularity, clarity, and accuracy of the version I in terms of cultural relevance and purpose. After semantic and conceptual equivalence were assessed in comparison to the original questionnaire, version II of the Arabic of the PIDAQ was produced.
Pre-testing
Version II of the Arabic version of the PIDAQ was subjected to pilot testing with 16 young adults aged between 18 and 30 years (8 males and 8 females). Participants were asked what they understood of each item. The pilot test demonstrated that version II of the Arabic version of the PIDAQ had appropriate semantic and conceptual equivalence to the original tool with no need for further modification. Therefore, the final Arabic version of the PIDAQ was produced [Appendix].
Survey population
The study sample was composed of young adults with an age range from 18 to 30 years. In total, the study included 205 individuals, comprising both Saudis and non-Saudis (those with other Arabic nationalities) from Medina city, Saudi Arabia. Participation in the research was voluntary, and participants were visitors of Al Rashid Mega Mall during public awareness campaigns held on World Oral Health Days. Individuals with moderately to severely discolored anterior teeth, craniofacial anomalies, or previous orthodontic treatment were excluded from the survey. The survey used the final Arabic version of the PIDAQ, the aesthetic component of the Index of Orthodontic Treatment Need (IOTN-AC), and the Dental Aesthetic Index (DAI). All participants were asked if they perceived a need for orthodontic treatment. After 1 month, 18 participants were randomly selected for the retest.
Esthetic component of Index of Orthodontic Treatment Need (IOTN-AC)
To assess participants' perception of dental esthetics and the severity of malocclusion, the IOTN-AC was used. This gave participants an unlimited amount of time to identify the photograph that most closely resembled their dentition from a sample of 10 black and white photographs that displayed varying degrees of malocclusion of the anterior teeth.[16] The sample was divided into three groups of photographs, grades 1 to 4 (no or little treatment need), grades 5 to 7 (moderate or borderline treatment need), and grades 8 to 10 (definite treatment need).
Dental Aesthetic Index (DAI)
The World Health Organization has recommended using the DAI to assess orthodontic treatment need.[17] The DAI used for the assessment of aesthetic and clinical aspects of occlusion assesses 10 occlusal characteristics that evaluate malocclusion.[18] The DAI score consists of four grades. Grade 1 (a score of 25 or less) indicates no or slight treatment need, grade 2 (a score from 26 to 30) indicates elective treatment need, grade 3 (a score from 31 to 35) indicates that treatment is highly desirable, and grade 4 (a score of 36 or more) indicates mandatory treatment.[19]
Statistical analysis
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS Inc., version 23, Chicago, IL, USA). The reliability of the scale was determined by testing internal consistency using Cronbach's alpha coefficient, Cronbach's alpha if item deleted, and the coefficient of correlation between items and the scale. The scale was considered reliable when alpha was more than 0.7. Test–retest reliability was assessed using the intraclass correlation coefficient (ICC).
Construct validity was assessed using factor analysis. The Kolmogorov–Smirnov test was conducted to check the normality of the variables. The data were not normally distributed. Therefore, non-parametric tests were applied. Convergent validity was assessed by comparing the total PIDAQ score and subscale scores with DAI grades and self-reported IOTN-AC scores using the Kruskal–Wallis test, while discriminant validity was tested using the Mann–Whitney test to compare PIDAQ scores with participants' self-evaluation of orthodontic treatment need. Other Mann–Whitney tests were used to compare the total PIDAQ score and subscale scores between males and females, while the Kruskal–Wallis test was used to compare the scores between three age groups (18–22 years, 23–26 years, and 27–30 years). All P values were considered significant when they were smaller than 0.05.
Results
A total of 205 young adults between 18 and 30 years old (mean age 23.93 ± 3.86) were included in this study. There was a 100% response rate and no missing data. Age and gender distribution within groups has been shown in [Table 1]. There were 108 (53.7%) Saudis and 97 (47.3%) non-Saudis (those with other Arabic nationalities). Of all participants, 114 (55.6%) perceived a need for treatment, whereas 91 (44.4%) perceived no need for treatment. Test-retest reliability was assessed by comparing data from 18 individuals with data obtained from them a month later.
Table 1.
Age and gender groups distribution of the sample
| Characteristics | n (%) |
|---|---|
| Age groups | |
| (18-22 years) | 78 (38.0%) |
| (23-26 years) | |
| (27-30 years) | 67 (32.7%) |
| 60 (29.3%) | |
| Gender groups | |
| Male | 98 (47.8%) |
| female | 107 (52.2%) |
Reliability
The internal consistency of the scale, evaluated by Cronbach's alpha coefficient, was 0.940, and the standardized Cronbach's alpha was 0.941. The values of Cronbach's alpha if item deleted ranged from 0.935 to 0.939 [Table 2]. Item and scale correlation coefficients were between r = 0.509 and r = 0.719. Principal component factor analysis extracted three subscales. Cronbach's alpha coefficients for the three subscales were 0.923 for social impact, 0.916 for dental self-confidence, and 0.892 for aesthetic attitude.
Table 2.
Principal component analysis with an orthogonal rotation of PIDAQ scale and factor loadings of the items, cumulative variance for extracted factors, and α when item deleted
| Items in brief | Social impact | Dental self-confidence | Aesthetic attitude | α when item deleted |
|---|---|---|---|---|
| Hold back when I smile | 0.739 | 0.181 | 0.131 | 0.937 |
| What others think | 0.772 | 0.203 | 0.189 | 0.936 |
| Offensive remarks | 0.766 | 0.102 | 0.337 | 0.937 |
| Inhibited in social contacts | 0.649 | 0.098 | 0.366 | 0.935 |
| Hide my teeth | 0.703 | 0.107 | 0.277 | 0.937 |
| People stare | 0.705 | -0.038 | 0.289 | 0.937 |
| Irritated on remarks | 0.706 | 0.131 | 0.261 | 0.936 |
| Worry about opposite sex | 0.745 | 0.041 | 0.340 | 0.936 |
| Others have nicer teeth | 0.802 | 0.181 | 0.218 | 0.937 |
| Proud of teeth | 0.122 | 0.804 | 0.211 | 0.938 |
| Like to show teeth | 0.113 | 0.800 | 0.208 | 0.938 |
| Pleased to see teeth in mirror | 0.121 | 0.808 | 0.194 | 0.938 |
| Teeth are attractive | 0.028 | 0.787 | 0.220 | 0.939 |
| Satisfied with appearance | 0.139 | 0.843 | 0.247 | 0.937 |
| Find tooth position nice | 0.145 | 0.795 | 0.121 | 0.938 |
| Envy | 0.220 | 0.142 | 0.762 | 0.937 |
| Somewhat distressed | 0.363 | 0.204 | 0.694 | 0.936 |
| Somewhat unhappy | 0.262 | 0.245 | 0.584 | 0.937 |
| Feel bad | 0.370 | 0.216 | 0.697 | 0.935 |
| Wish teeth looked better | 0.229 | 0.305 | 0.563 | 0.937 |
| Don’t like teeth in mirror | 0.321 | 0.215 | 0.622 | 0.937 |
| Don’t like teeth in photo | 0.282 | 0.285 | 0.682 | 0.936 |
| Don’t like teeth on video | 0.304 | 0.177 | 0.678 | 0.936 |
| Percentage of Cumulative variance explained (rotated solution) | 24.503 | 43.938 | 63.329 |
In bold: Salient factor loadings
Reproducibility
Test–retest reliability, according to the ICC, was 0.937, and the ICCs of the three subscales were 0.948, 0.940, and 0.929.
Construct validity
In the factor analysis, the Kaiser-Meyer-Olkin measure of sampling adequacy was 0.935, Bartlett's test of sphericity was 3037.6 (P < 0.001), and three common factors were extracted with factor loadings from 0.563 to 0.843. The first factor contained items one to nine, which reflected the social impact of dental aesthetics. The second factor included items ten to fifteen of the original dental self-confidence subscale items. The third factor contained items 16 to 23, representing the impact of teeth appearance on aesthetic attitude. The cumulative variance for these three factors was 63.33% [Table 2].
Convergent validity
Statistically significant correlations (P < 0.001) were found in all total PIDAQ scores and all subscale scores when compared to IOTN-AC and DAI scores [Tables 3 and 4].
Table 3.
Comparison between scores of PIDAQ scale with a different IOTN-AC scores using Kruskal–Wallis tests
| PIDAQ scores | IOTN AC self-rating score | |||
|---|---|---|---|---|
| Score 1-4 (n=107) | Score 5-7 (n=56) | Score 8-10 (n=42) | P | |
| Social Impact (Mean±SD) | 6.74±6.58 | 8.59±5.90 | 14.05±9.44 | < 0.001 |
| Dental Self-Confidence (Mean±SD) | 11.48±5.72 | 11.52±6.13 | 15.67±6.05 | < 0.001 |
| Esthetics attitude (Mean±SD) | 8.07±6.63 | 9.68±6.78 | 15.14±7.96 | < 0.001 |
| Total PIDAQ (Mean±SD) | 26.29±15.60 | 29.88±15.37 | 44.86±18.28 | < 0.001 |
SD: Standard Deviation; PIDAQ: Psychosocial Impact of Dental Aesthetics Questionnaire; IOTN-AC: Index of Orthodontic Treatment Need
Table 4.
Comparison between scores of PIDAQ scale with different DAI grades using Kruskal-Wallis tests
| PIDAQ scores | Dental Aesthetic Index grade | ||||
|---|---|---|---|---|---|
| Grade 1 (n=74) | Grade 2 (n=49) | Grade 3 (n=45) | Grade 4 (n=37) | P | |
| Social Impact (Mean±SD) | 5.84±5.92 | 8.18±5.43 | 9.60±7.77 | 14.24±9.64 | < 0.001 |
| Dental Self-Confidence (Mean±SD) | 10.54±5.76 | 12.06±5.61 | 12.78±6.34 | 15.81±5.83 | < 0.001 |
| Esthetics attitude (Mean±SD) | 7.46±6.71 | 9.53±6.29 | 11.16±7.22 | 14.08±8.57 | < 0.001 |
| Total PIDAQ (Mean±SD) | 23.84±15.39 | 29.88±12.85 | 33.53±17.31 | 44.14±19.79 | < 0.001 |
SD: Standard Deviation; PIDAQ: Psychosocial Impact of Dental Aesthetics Questionnaire; DAI: Dental Aesthetic Index
Discriminant validity
Significant differences were found (P < 0.001) by comparing total PIDAQ score and subscale scores according to participants' self-evaluation of orthodontic treatment need. All individuals in the perceived need group showed a significantly higher total PIDAQ score and significantly higher subscale scores when compared to those who perceived no need for orthodontic treatment [Table 5].
Table 5.
Mann-Whitney test of total PIDAQ and subscales scores between perceived need group and perceived no need group
| PIDAQ scores | Perception of orthodontic treatment need | ||
|---|---|---|---|
| Perceived need (n=114) | Perceived no need (n=91) | P | |
| Social Impact (Mean±SD) | 10.17±7.60 | 6.96±7.25 | < 0.001 |
| Dental Self-Confidence (Mean±SD) | 13.98±6.00 | 10.30±5.64 | < 0.001 |
| Esthetics attitude (Mean±SD) | 11.85±7.74 | 7.59±6.32 | < 0.001 |
| Total PIDAQ (Mean±SD) | 36.04±17.52 | 24.85±15.63 | < 0.001 |
SD: Standard Deviation; PIDAQ: Psychosocial Impact of Dental Aesthetics Questionnaire
There were no significant differences in total PIDAQ score or subscale scores between males and females and between age groups [Table 6].
Table 6.
Differences in total PIDAQ and subscales scores between age groups using Kruskal-Wallis tests, and between gender groups using Mann-Whitney test
| PIDAQ scores | Age groups | Gander groups | |||||
|---|---|---|---|---|---|---|---|
| 18-22 years (n=78) | 23-26 years (n=67) | 27-30 years (n=60) | P | Males (n=98) | Females (n=107) | P | |
| Social Impact (Mean±SD) | 8.53±7.49 | 8.87±7.62 | 8.88±7.83 | 0.969 | 7.80±6.96 | 9.61±8.07 | 0.138 |
| Dental Self-Confidence (Mean±SD) | 12.13±5.96 | 11.76±6.87 | 13.28±5.35 | 0.391 | 11.84±6.02 | 12.81±6.18 | 0.235 |
| Esthetics attitude (Mean±SD) | 9.62±7.23 | 9.58±8.00 | 10.83±7.10 | 0.358 | 9.37±6.52 | 10.50±8.19 | 0.591 |
| Total PIDAQ (Mean±SD) | 30.33±17.34 | 30.21±18.80 | 33.00±16.59 | 0.485 | 29.00±15.34 | 32.97±19.28 | 0.263 |
SD: Standard Deviation; PIDAQ: Psychosocial Impact of Dental Aesthetics Questionnaire
Discussion
In recent years, attention has been paid to using the concept of OHRQoL to improve clinical orthodontic practice and research.[20,21] The PIDAQ has proven to be a valuable tool for measuring OHRQoL in English-speaking orthodontic patients.[11] This study aimed to provide a version of the PIDAQ for young Arab adults. To make the questionnaire available for different cultural contexts while maintaining its psychometric properties, the original version of PIDAQ was not only translated into Modern Standard Arabic but also subjected to a cross-cultural adaptation process as suggested by the Project of International Quality of Life Assessment.[22]
The process of translating the PIDAQ was a meticulous four-step procedure that included translation, back-translation, cultural adaptation, and pre-testing. The Translation Committee was composed of an orthodontist, a postgraduate dental student, and a dental student, all of whom were proficient in English and Arabic. The translation process considered the suitability of the translated version for a wide range of Arabic dialects, Arabic nationalities, and the different levels of education present in the sample. Therefore, simple Modern Standard Arabic was used in the questionnaire. Back-translation from Arabic to English was conducted by two bilingual English teachers. A comparison of the back-translated version with the original showed a high level of similarity. The Cultural Adaptation Committee was composed of a linguist, an orthodontist, and postgraduate dental students. The translated questionnaire was evaluated for its agreement with the original version regarding semantic and conceptual equivalence. The expression of one term (envy) gave a feeling of hostility when translated into Arabic, so an Arabic synonym was used for this term. The results of the pre-test indicated that the quality of the translation was appropriate and adequate.
The internal consistency of the Arabic version was good. Cronbach's alpha coefficient was 0.940, which is higher than the 0.7 threshold[23] and higher than the original and Spanish versions of the PIDAQ.[11,24] The alpha if item deleted coefficient signified good internal consistency of items because deletion of any item did not improve Cronbach's alpha. Corrected item-total correlation indicated that all items were significantly correlated with each other, as it was more than 0.5 for every item and ranged from 0.509 to 0.719. Test-retest reliability was high (0.937), which demonstrated the excellent reliability of the Arabic version of the PIDAQ.
Construct validity was assessed using factor analysis. When subjecting the 23 items to principal component factor analysis with orthogonal rotation, three common factors were extracted. The first extracted common factor, social impact, consisted of nine items, which contained the same eight items of the corresponding dimension of the original version, plus a ninth item, “I think most people I know have nicer teeth than I do,” which was under “psychological impact” in the original version of the PIDAQ. The second common factor, dental self-confidence, was composed of the same items of the corresponding dimension of the original version of the PIDAQ. The third common factor contained all items of the psychological impact and aesthetic concern dimensions of the original version except one item, “I think most people I know have nicer teeth than I do,” which was included in the first common factor. Results for the third common factor were almost the same as those of the Chinese version of the PIDAQ, which grouped psychological impact and aesthetic concern within one common factor named “aesthetics attitude,” because the word “attitude” represented the meaning of both factors.[15]
Using a threshold of eigenvalues greater than 1, factor analysis with orthogonal rotation resulted in the extraction of three common factors. Factor analysis with the number of factors fixed at four resulted in just one item being included in the fourth factor, which was “I wish my teeth looked better.” This result seemed unreasonable because this item was in the third factor in the original version and should not be divided. Overall, three factors had better item factor loading and more reasonable results.
As mentioned before, the three common factors in the Arabic version of the PIDAQ were similar to those found in the Chinese version[15] but were different from the four domains found in the original and the Spanish and Turkish versions. However, the cumulative variance for the three factors model was 63.33%, which was higher than the cumulative variance of the four-factor models of the other PIDAQ versions.[11,13,24] This means that the Arabic version of the PIDAQ had good construct validity, and differences in the distribution of items and the number of domains between the Arabic version and other versions, including the original, may be attributed to variations in cultural background, style of expression, and the Arab population's perception and understanding of items.
Convergent validity of the Arabic version of the PIDAQ was assessed using the IOTN-AC and DAI. Results indicated good convergent validity of the scale because the total PIDAQ score and its subscale values correlated significantly with IOTN-AC and DAI values, where higher IOTN-AC and DAI values correlated with higher PIDAQ values [Tables 3 and 4]. Moreover, the scale had good discriminant validity in all groups included in this study as shown by the significantly higher total PIDAQ score and higher subscale scores for all individuals who perceived a need for orthodontic treatment, compared to those who perceived no need for orthodontic treatment [Table 5].
When comparisons were made between males and females and between age groups, results showed no statistically significant differences in total PIDAQ score or subscale scores [Table 6]. A similar conclusion was reported in the literature.[11,25] However, results regarding gender differences disagreed with those of two previous studies, which found that females expressed more impact of malocclusion than males in psychological impact[26] and social impact subscales.[27] However, another study found no difference in impact between males and females, though it reported that the younger the age, the more the psychological effect.[9] Cultural differences between populations and differences in age groups, sample sizes, distribution of items, and the number of domains between PIDAQ versions might explain such disagreement.
This study was conducted in Medina city, which contains adequate cultural and ethnic diversity because it included a large number of different Arabic nationalities. People from different parts of this city usually attend the location in which the population was sampled; therefore, the sample was considered representative of the target population.
Conclusion
The Arabic version of the PIDAQ developed in this study demonstrated excellent psychometric properties with sufficient reliability and validity. This questionnaire provides a useful tool to evaluate the OHRQoL of orthodontic patients in the young adult Arabic-speaking population to assess treatment needs and changes in orthodontic-related OHRQoL during treatment and to enhance treatment outcomes. This tool has the potential to improve orthodontic research and clinical applications related to malocclusion and its social and psychological impacts as perceived by patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors would like to thank Dr. Asma Marghalani and Dr. Khairiah Madani for their collaboration in data collection.
Appendix
Arabic version of PIDAQ
References
- 1.Sischo L, Broder HL. Oral health-related quality of life: What, why, how, and future implications. J Dent Res. 2011;90:1264–70. doi: 10.1177/0022034511399918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Group TW. The World Health Organization quality of life assessment (WHOQOL): Development and general psychometric properties. Soc Sci Med. 1998;46:1569–85. doi: 10.1016/s0277-9536(98)00009-4. [DOI] [PubMed] [Google Scholar]
- 3.Silva LF, Thomaz EB, Freitas HV, Pereira AL, Ribeiro CC, Alves CM. Impact of Malocclusion on the quality of life of Brazilian adolescents: A population-based study. PLoS One. 2016;11:e0162715. doi: 10.1371/journal.pone.0162715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen M, Feng ZC, Liu X, Li ZM, Cai B, Wang DW. Impact of malocclusion on oral health – related quality of life in young adults. Angle Orthod. 2015;85:986–91. doi: 10.2319/101714-743.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.De Oliveira CM, Sheiham A. The relationship between normative orthodontic treatment need and oral health - related quality of life. Community Dent Oral Epidemiol. 2003;31:426–36. doi: 10.1046/j.1600-0528.2003.00002.x. [DOI] [PubMed] [Google Scholar]
- 6.Hassan AH, Amin HE. Association of orthodontic treatment needs and oral health-related quality of life in young adults. Am J Orthod Dentofacial Orthop. 2010;137:42–7. doi: 10.1016/j.ajodo.2008.02.024. [DOI] [PubMed] [Google Scholar]
- 7.Slade GD. Measuring Oral Health and Quality of Life. Chapel Hill, NC: University of North Carolina; 1997. [Google Scholar]
- 8.De Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004;31:20–7. doi: 10.1179/146531204225011364. [DOI] [PubMed] [Google Scholar]
- 9.Masood Y, Masood M, Zainul NN, Araby NB, Hussain SF, Newton T. Impact of malocclusion on oral health related quality of life in young people. Health Qual Life Outcomes. 2013;11:25. doi: 10.1186/1477-7525-11-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Masood M, Masood Y, Saub R, Newton JT. Need of minimal important difference for oral health-related quality of life measures. J Public Health Dent. 2014;74:13–20. doi: 10.1111/j.1752-7325.2012.00374.x. [DOI] [PubMed] [Google Scholar]
- 11.Klages U, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J Orthod. 2006;28:103–11. doi: 10.1093/ejo/cji083. [DOI] [PubMed] [Google Scholar]
- 12.Sardenberg F, Oliveira AC, Paiva SM, Auad SM, Vale MP. Validity and reliability of the Brazilian version of the psychosocial impact of dental aesthetics questionnaire. Eur J Orthod. 2011;33:270–5. doi: 10.1093/ejo/cjq066. [DOI] [PubMed] [Google Scholar]
- 13.Aglarci C, Baysal A, Demirci K, Dikmen F, Aglarci AV. Translation and validation of the Turkish version of the psychosocial impact of dental aesthetics questionnaire. Korean J Orthod. 2016;46:220–7. doi: 10.4041/kjod.2016.46.4.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bourzgui F, Serhier Z, Sebbar M, Diouny S, Othmani MB, Ngom PI. Adaptation and validation of the Moroccan Arabic version of the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) Saudi Dent J. 2015;27:180–6. doi: 10.1016/j.sdentj.2014.11.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lin H, Quan C, Guo C, Zhou C, Wang Y, Bao B. Translation and validation of the Chinese version of the psychosocial impact of dental aesthetics questionnaire. Eur J Orthod. 2013;35:354–60. doi: 10.1093/ejo/cjr136. [DOI] [PubMed] [Google Scholar]
- 16.Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11:309–20. doi: 10.1093/oxfordjournals.ejo.a035999. [DOI] [PubMed] [Google Scholar]
- 17.World Health Organization. Oral Health Surveys: Basic Methods. Geneva: World Health Organization; 1997. [Google Scholar]
- 18.Cons NC, Jenny J, Kohout FJ. DAI: The Dental Aesthetic Index. Iowa City, Iowa: College of Dentistry, University of Iowa; 1986. [Google Scholar]
- 19.Jenny J, Cons NC. Comparing and contrasting two orthodontic indices, the index of orthodontic treatment need and the dental aesthetic index.Am. J Orthod Dentofacial Orthop. 1996;110:410–6. doi: 10.1016/s0889-5406(96)70044-6. [DOI] [PubMed] [Google Scholar]
- 20.Dos Santos PR, Meneghim MD, Ambrosano GM, Vedovello Filho M, Vedovello SA. Influence of quality of life, self-perception, and self-esteem on orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2017;151:143–7. doi: 10.1016/j.ajodo.2016.06.028. [DOI] [PubMed] [Google Scholar]
- 21.Ghijselings I, Brosens V, Willems G, Fieuws S, Clijmans M, Lemiere J. Normative and self-perceived orthodontic treatment need in 11-to 16-year-old children. Eur J Orthod. 2014;36:179–85. doi: 10.1093/ejo/cjt042. [DOI] [PubMed] [Google Scholar]
- 22.Aaronson NK, Acquadro C, Alonso J, Apolone G, Bucquet D, Bullinger M, et al. International quality of life assessment (IQOLA) project. Qual Life Res. 1992;1:349–51. doi: 10.1007/BF00434949. [DOI] [PubMed] [Google Scholar]
- 23.Kline RB. Principles and Practice of Structural Equation Modeling. New York, NY: The Guilford Press; 2015. [Google Scholar]
- 24.Montiel-Company JM, Bellot-Arcís C, Almerich-Silla JM. Validation of the psychosocial impact of dental aesthetics questionnaire (Pidaq) in Spanish adolescents. Med Oral Patol Oral Cir Bucal. 2013;18:e168–73. doi: 10.4317/medoral.18324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Aikins EA. Self-perception of malocclusion among Nigerian adolescents using the aesthetic component of the IOTN. Open Dent J. 2012;6:61–6. doi: 10.2174/1874210601206010061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bellot-Arcís C, Almerich-Silla JM. Psychosocial impact of malocclusion in Spanish adolescents. Korean J Orthod. 2013;43:193–200. doi: 10.4041/kjod.2013.43.4.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ilijazi-Shahiqi D, Mehmeti B, Kelmendi J, Krasniqi D, Kamberi B, Anic-Milosevic S. Validity and reliability of the psychosocial impact of dental aesthetics questionnaire in Kosovar adolescents. Int J Adolesc Med Health. 2020;2020:1–6. doi: 10.1515/ijamh-2019-0038. [DOI] [PubMed] [Google Scholar]