

Abstract
Background
The importance of creating an anatomic anterior cruciate ligament (ACL) reconstruction has been receiving significant attention. The best technique by which to achieve this anatomic reconstruction continues to be debated. The two most common methods are the transtibial (TT) and anteromedial (AM) techniques. Each has its advantages and disadvantages, and the literature comparing the two remains uncertain.
Questions/Purposes
In this prospective comparative study, we aimed to compare the ACL graft and tunnel angles achieved using the anatomic transtibial (TT) and anteromedial (AM) techniques; compare the ACL graft and tunnel angles in knees that have undergone ACL reconstruction and knees with intact ACLs; and determine whether differences in the graft or tunnel angle produce differences in clinical outcomes, as measured using both physical exam and patient-reported outcomes, after ACL reconstruction.
Methods
Patients who underwent primary ACL reconstruction with bone–tendon–bone grafts using a TT or AM technique were included. Femoral graft angle (FGA), tibial graft angle (TGA), and sagittal orientation of the reconstructed ACL and contralateral native ACL were measured on post-operative magnetic resonance imaging. Post-operatively, patients underwent measurement of knee stability and completed the Knee Injury and Osteoarthritis Outcome Score (KOOS) survey.
Results
Twenty-nine patients were enrolled (AM group, 14; TT group, 15); at follow-up, KOOS data were available for 26 patients (13 in each group). There were no differences in sagittal ACL graft angle between groups or in comparison with the normal knee. The FGA was more vertical after TT reconstructions; the TGA was comparable between groups. There were no significant differences in 2-year post-operative physical exam measurements or in KOOS scores.
Conclusion
Anatomic ACL angle was restored after reconstruction with both the TT and AM techniques, despite different FGAs. No significant differences in clinical outcome were noted between groups on physical exam or KOOS at 2 years after surgery. These results suggest that TT reconstruction results in a graft position similar to that seen in AM reconstruction and that the location of the intra-articular tunnel aperture matters more than the orientation of the tunnel.
Keywords: transtibial reconstruction, anteromedial reconstruction, anterior cruciate ligament reconstruction technique, tunnel angle, graft angle
Introduction
Increased emphasis is being placed on achieving anatomic anterior cruciate ligament (ACL) reconstruction (restoration of the ACL to its native dimensions). Surgical techniques are scrutinized to optimize ACL tunnel placement [12, 24]. Anatomic placement of the femoral tunnel and graft obliquity in the sagittal plane are crucial to success [49]. A graft placed too anterior in the sagittal plane can result in excessive tension on the graft and subsequent failure, and a vertical graft in the coronal plane has been shown to lead to suboptimal restoration of knee translation or rotational stability—and potential failure [14, 25, 28].
Transtibial (TT) reconstruction, the creation of the femoral tunnel through the tibial tunnel, remains a commonly used technique in ACL reconstruction [19]. This technique has been criticized because the femoral tunnel position is dependent on the tibial tunnel position, making restoration of anatomic femoral tunnel placement difficult [1]. Accordingly, femoral tunnel placement through an anteromedial (AM) portal with the knee in hyperflexion gained popularity because it allows independent tunnel positioning. Proponents suggest that the AM technique is better at reproducing coronal plane graft obliquity and a more anatomic graft because femoral tunnel placement is independent of the tibial tunnel [17, 20]. Potential pitfalls of an AM technique include the need for the knee to be in hyperflexion (necessitating qualified assistants), a short femoral tunnel, or posterior wall blowout [22]. Cadaveric studies have demonstrated that anatomic placement of the femoral tunnel can be achieved using the TT technique, but it is technically challenging [23, 36]. Modifications to the TT technique to allow for more anatomic placement have been described [2, 3, 36]. Clinical literature comparing these techniques suggests that they can produce similar clinical outcomes; however, few studies have evaluated the angle of the reconstructed ACL in relation to these tunnel positions [22]. The ACL footprint and ACL angle likely represent the main biomechanical variables to be studied, given that different femoral tunnel footprints lead to different biomechanical results [47].
The purposes of this prospective comparative study were to compare ACL graft angle and tunnel angles achieved using the TT and AM techniques; to compare ACL graft and tunnel angles in knees that have undergone ACL reconstruction and knees with intact ACLs; and to evaluate whether differences in graft or tunnel angle produce differences in clinical outcome after ACL reconstruction. We hypothesized that there would be no significant difference, when measured using magnetic resonance imaging (MRI), between the TT and AM techniques, as assessed by clinical outcome and ACL graft obliquity.
Materials and Methods
Eligible patients included those age 18 and older who underwent primary ACL reconstruction with a bone–tendon–bone (BTB) graft performed by one of two senior authors using either a TT or AM technique. Patients had to be willing to undergo post-operative MRI and clinical evaluation. Exclusion criteria included the following: concomitant medial collateral ligament, lateral collateral ligament, or posterior collateral ligament tears requiring reconstruction or repair; significant chondromalacia greater than grade III in any compartment; previous lower-limb surgery; history of arthritis (osteoarthritis or rheumatoid arthritis); noncompliance with rehabilitation protocol; signs of hyperlaxity; and concomitant meniscal injuries that required repair or a subtotal meniscectomy.
This was a single-blind, prospective trial in which the senior authors performed all surgery, with one surgeon (C.A.B.) performing reconstruction using an AM portal technique with straight guide and the second surgeon (N.N.V.) performing reconstruction using a TT technique. All reconstructions were done using a BTB graft harvested in the standard manner from the ipsilateral knee or from an allograft. Rehabilitation was similar between groups.
A total of 29 patients were enrolled in the study, 14 in the AM cohort and 15 in the TT cohort. Patient pre-operative demographics and time to surgery and follow-up did not significantly differ between cohorts (Table 1). One patient in the TT group underwent reconstruction 49 months after the initial injury. None of the patients reported smoking, diabetes mellitus, hypertension, or thyroid disorders, and none of the injuries was classified as a workers’ compensation injury. All patients received BTB grafts; autograft was used in five of 14 patients in the AM group, and 14 of 15 patients in the TT group (p = 0.002).
Table 1.
Demographic and clinical characteristics of patients (N = 29)
| Characteristic | AM (n = 14) | TT (n = 15) | p value |
|---|---|---|---|
| Age at surgery: years ± SD | 24.26 ± 3.62 | 23.79 ± 3.29 | 0.718 |
| Time to surgery: months ± SD | 1.57 ± 1.34 | 6.33 ± 12.56 | 0.170 |
| BMI ± SD | 25.69 ± 3.32 | 26.33 ± 6.31 | 0.738 |
| Side affected: no. |
Right 6 Left 8 |
Right 10 Left 5 |
0.272 |
| Sex |
Male 11 Female 3 |
Male 11 Female 4 |
> 0.999 |
AM anteromedial, TT transtibial, SD standard deviation, BMI body mass index (the weight in kilograms divided by the square of the height in meters)
All patients underwent post-operative MRI of their affected and unaffected knees at a minimum of 1 year after surgery, as well as a concurrent single visit for clinical evaluation with KT-1000 testing, laxity testing, examination of range of motion (ROM), and Knee Injury and Osteoarthritis Outcome Score (KOOS) evaluation. Unblinded trained research staff and an orthopedic sports medicine faculty member (B.J.M., C.B.J., N.N.V.) oversaw the follow-up. A follow-up interview was conducted at a minimum of 4.5 years to determine post-operative instability or revision surgery.
MRI was performed with a 1.0-T MR imager by using a quadrature coil. For the operative knee, an image in the coronal plane that best showed the femoral tunnel was used to measure the femoral graft angle (FGA), defined as the angle between the axis of the femoral tunnel and the joint line (Fig. 1). In the sagittal plane, an image that best showed the tibial tunnel was used to measure the tibial graft angle (TGA), defined as the angle between the axis of the tibial tunnel and a line perpendicular to the long axis of the tibia (Fig. 2). For the non-operative leg, images in the sagittal plane that showed the intact ACL were used to measure the sagittal ACL angle, defined as the angle between a line perpendicular to the long axis of the tibia and the orientation of the ACL fibers (Fig. 3).
Fig. 1.
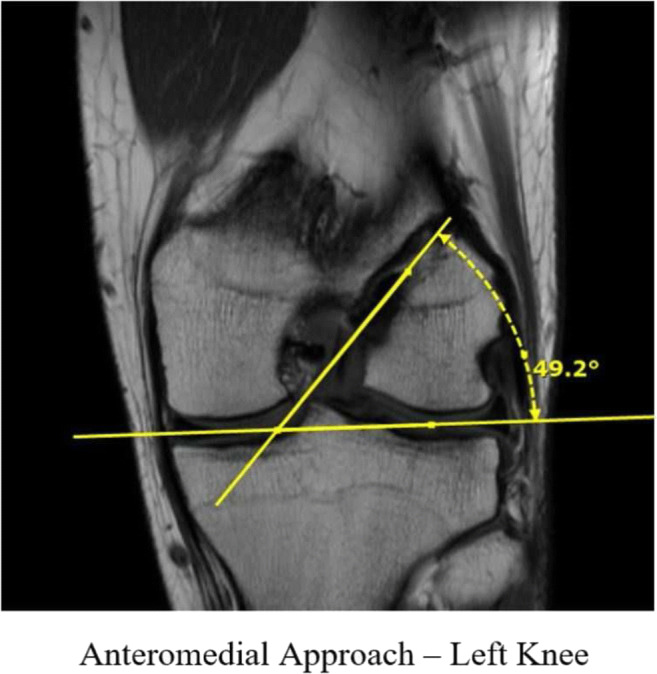
Post-operative 1.0-T magnetic resonance imaging showing coronal femoral graft angle measurements in the anteromedial approach. A line estimating the level of tibial plateau was used as an approximation of the joint line. A second line was then drawn through the femoral tunnel of the medial femoral condyle, and the angle between the lines was calculated to determine the femoral graft angle.
Fig. 2.
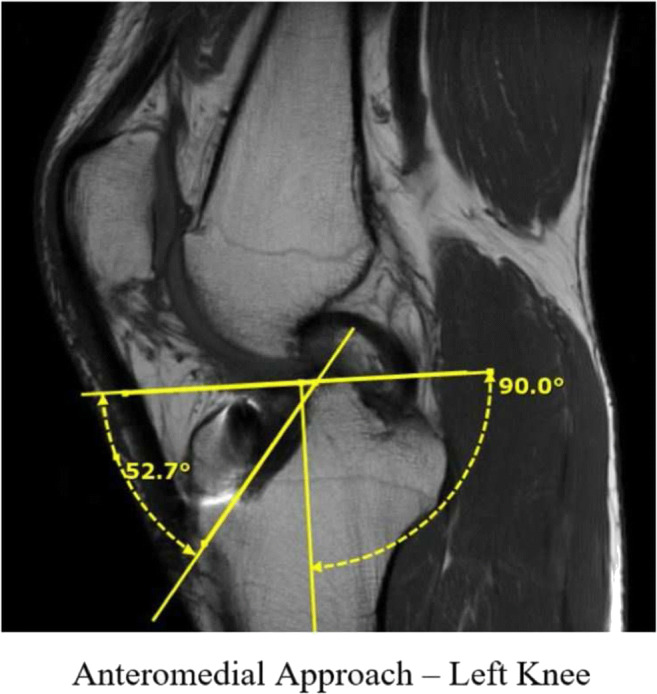
Post-operative 1.0-T magnetic resonance imaging showing sagittal tibial graft angle measurements in the anteromedial approach. The joint line was estimated by drawing a vertical line along the tibial axis using the tibial growth plate and compared with a line that was then drawn parallel to the tibial tunnel. The angle between the joint line and a line oriented parallel to the tibial tunnel was used to determine the tibial graft angle.
Fig. 3.
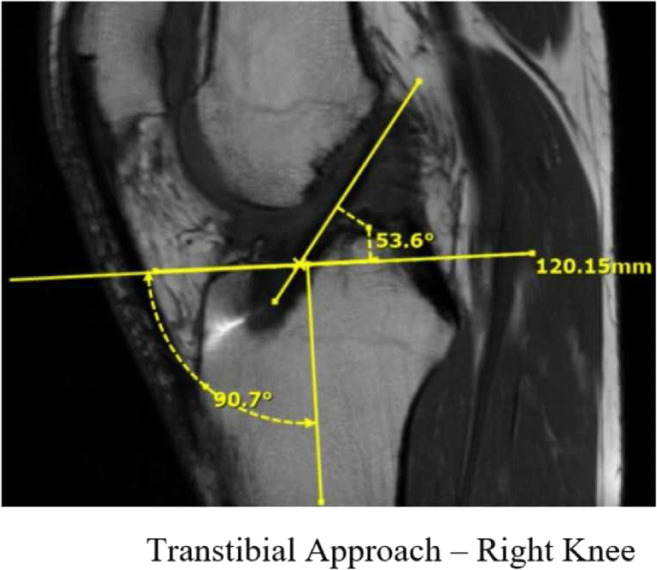
Post-operative 1.0-T magnetic resonance imaging showing anterior cruciate ligament (ACL) angle in the transtibial approach. Joint line approximations were consistent with tibial graft angle measurements; a line was placed parallel to the ACL. The angle between the joint line and a line oriented parallel to the ACL fibers was used to determine the ACL angle.
Statistical Analysis
Review of the MRI scans was performed by three blinded reviewers: two practicing fellowship-trained orthopedic surgeons (C.A.B., A.V.S.) and an orthopedic sports medicine fellow (J.C.). An intra-class correlation coefficient (ICC) was used to determine interobserver reliability. Data were analyzed with the IBM SPSS statistical package (version 12, Chicago, IL, USA). A t test was used for comparison of coronal and sagittal graft angles, KT-1000 data, and ROM. The Fisher exact test was used to examine differences in categorical data such as pivot–shift testing, return to sport or work, and complications between groups. Statistical significance was set at p ≤ 0.05.
Results
The post-operative clinical examination and MRI were performed at a mean of 24.50 ± 5.95 months in AM patients and 24.93 ± 8.92 months in TT patients (p = 0.880). In both cohorts, the ROM was similar between the operative and non-operative knees at 2 years after surgery, with no significant differences (Table 2). One patient in the AM group had a Lachman test score of 2A and positive pivot test; all other patients (both groups) had a Lachman score of 1A and a negative pivot–shift test (p > 0.99).
Table 2.
Physical examination outcomes at 2 years in AM and TT patients
| Motion/motion comparison | AM (n = 14) | TT (n = 15) | p value |
|---|---|---|---|
| Extension non-operative side | 4.29 ± 5.33 | 2.53 ± 1.85 | 0.240 |
| Extension operative side | 2.71 ± 4.66 | 1.33 ± 1.59 | 0.289 |
| Extension non-operative side minus operative side | 1.57 ± 1.65 | 1.20 ± 1.26 | 0.500 |
| Flexion non-operative side | 135.33 ± 3.82 | 136.31 ± 3.07 | 0.487 |
| Flexion operative side | 134.00 ± 2.59 | 135.92 ± 3.93 | 0.166 |
| Flexion non-operative side minus operative side | 1.14 ± 3.39 | 0.33 ± 1.80 | 0.423 |
AM anteromedial, TT transtibial
There were no statistically significant differences between the AM and TT groups in any of the KOOS subscores, including KOOS-ADL (activities of daily living), KOOS-Pain, KOOS-QOL (quality of life), KOOS-Sports, and KOOS-Symptoms (Table 3). All patients in the AM and TT groups reported a return to sport and work.
Table 3.
2-year post-operative Knee Injury and Osteoarthritis Outcome Scores
| KOOS subsection | AM (n = 13) | TT (n = 13) | p value |
|---|---|---|---|
| Mean score out of 100 ± SD | Mean score out of 100 ± SD | ||
| KOOS-ADL | 97.90 ± 3.49 | 95.59 ± 9.60 | 0.405 |
| KOOS-Pain | 91.47 ± 8.33 | 86.90 ± 15.19 | 0.333 |
| KOOS-QOL | 79.46 ± 12.84 | 73.21 ± 23.31 | 0.388 |
| KOOS-Sports | 78.21 ± 16.94 | 78.62 ± 19.57 | 0.953 |
| KOOS-Symptoms | 83.93 ± 12.19 | 85.63 ± 12.14 | 0.715 |
KOOS Knee Injury and Osteoarthritis Outcome Score, AM anteromedial, TT transtibial, ADL activities of daily living, QOL quality of life
The final follow-up survey indicating instability or revision surgery was completed for 26 of 29 patients (AM group, 13; TT group, 13; p > 0.99), at 66.08 ± 6.89 months in AM patients and 66.85 ± 9.01 months in TT patients (p = 0.809). Two of the AM patients had instability: one experienced one episode of instability going down stairs; the other experienced instability because of a retear of his ACL while playing basketball. The latter was the only patient in either cohort to undergo revision surgery for instability. Two patients in the TT cohort experienced recurrent instability: one experienced six episodes of instability when going from sitting to standing (they resolved on their own); the other experienced 10 to 20 episodes of instability during quick movements such as cutting while running (they also resolved, after physical therapy). There were no statistically significant differences between groups in terms of incidence of instability and reoperation for graft failure (p > 0.99 and p = 0.483, respectively).
MRI was performed post-operatively in all patients. The sagittal plane ACL graft angle, TGA, and TGA–ACL angle were similar between the AM and TT groups; the FGA differed significantly between the two groups (Table 4). The ACL angle of the non-injured knee was similar between cohorts, and the difference between the angle of the reconstructed ACL and angle of the non-injured ACL was also similar within each cohort and between cohorts (Table 4). An ICC was calculated for each MRI metric between the three evaluators and correlated to the corresponding level of reliability (Table 5) [26].
Table 4.
2-year MRI results of AM and TT ACL reconstruction techniques
| MRI measurement | AM (14) | TT (15) | p value |
|---|---|---|---|
| Degrees ± SD | Degrees ± SD | ||
| FGA | 48.06 ± 4.74 | 57.28 ± 9.29 | 0.003 |
| TGA | 67.43 ± 6.66 | 62.61 ± 7.03 | 0.069 |
| ACL angle | 52.57 ± 4.75 | 52.41 ± 4.72 | 0.928 |
| ACL angle noninjured side | 50.83 ± 5.83 | 51.86 ± 2.96 | 0.566 |
| ACL angle reconstructed–ACL angle noninjured side | − 2.85 ± 5.94 | 1.07 ± 3.60 | 0.356 |
| TGA–ACL angle | 14.86 ± 9.59 | 10.20 ± 8.27 | 0.172 |
MRI magnetic resonance imaging, AM anteromedial, TT transtibial, ACL anterior cruciate ligament, FGA femoral graft angle, TGA tibial graft angle
Table 5.
ICC for 2-year MRI metrics
| MRI measurement | ICC | 95% CI | Level of reliability |
|---|---|---|---|
| FGA | 0.846 | 0.699–0.924 | Moderate to excellent |
| TGA | 0.776 | 0.621–0.880 | Moderate to good |
| ACL angle | 0.885 | 0.799–0.940 | Good to excellent |
| ACL angle noninjured side | 0.694 | 0.247–0.875 | Poor to good |
ICC intra-class correlation coefficient, MRI magnetic resonance imaging, CI confidence interval, FGA femoral graft angle, TGA tibial graft angle, ACL anterior cruciate ligament
Discussion
There are a number of important findings in this study: there was no difference in sagittal ACL angle between the AM and TT techniques; femoral tunnel placement via an AM technique led to greater femoral tunnel obliquity in the coronal plane, as compared with the TT technique; despite this difference in tunnel angle, there was no difference in sagittal ACL angle between the native ACL and the reconstructed ACL when the AM and TT techniques were employed; and there was no difference in clinical outcomes between the two techniques.
Some of the limitations of this study include a lack of pre-operative KOOS data, which means we were unable to accurately determine the change in KOOS scores between groups; however, the post-operative KOOS scores are excellent in both groups and consistent with other reported outcomes [9, 16]. Clinical follow-up was performed by unblinded staff, and graft type (autograft or allograft) had an uneven distribution between groups. These factors could introduce further bias to clinical outcome results. Another limitation is the possibility of inaccuracy of the MRI measurements. To improve accuracy, however, three blinded observers assessed the images. ICC was calculated, and readings had a good level of reliability for all but non-operative ACL measurement, which was rated as moderate. A post hoc power analysis was performed and averaged for KOOS and ROM clinical outcomes measures. This demonstrated a post hoc power of less than 50% for clinical outcomes; therefore, our study was likely underpowered to detect differences in clinical outcome measures. However, caution should be exercised when interpreting a post hoc power analysis [21, 29]. Finally, two surgeons performed the procedures using two separate techniques, which may have further introduced bias into the outcomes.
Restoration of normal ACL anatomy and function is the primary goal of anatomic ACL reconstruction, and although placement of both the tibial and femoral tunnels is important, restoration of the native femoral tunnel has received more attention [1, 25, 31, 39]. Femoral tunnel position and obliquity in ACL reconstruction has been hypothesized to be an important factor in restoring rotational stability to the knee [28, 31, 42]. Some researchers argue that creating the femoral tunnel through an AM portal is more anatomic [1, 13, 25, 48], although others have suggested an oblique femoral tunnel can be achieved via a TT technique as well [37]. A vertically oriented graft can stabilize anterior tibial translation but has been shown to result in persistent pivot shift and inferior Lysholm knee scores [28].
Our argument that the TT and AM techniques can both be anatomic relies on the ability to restore an anatomic footprint, regardless of tunnel obliquity. Several cadaveric studies reported that the TT technique is not able to restore rotational stability to the same degree as the AM portal technique [8, 31, 41, 47]. However, the intra-articular tunnel apertures of the TT technique in these studies were not at the anatomic ACL footprint and may have created grafts that were no longer at a native angle.
Studies to date that have compared the imaging outcomes of AM and TT techniques have shown that AM leads to a lower FGA [5, 15, 18, 35, 46]. Although there are concerns about impingement with vertical femoral tunnel placement, we found no evidence of this during surgery or in clinical follow-up, with post-operative extension being similar in both groups [43]. Measuring the FGA involves the femoral tunnel and not the graft itself. Although the tunnel angle in the AM and TT techniques may differ, the location of the tunnel aperture on the femoral condyle may be similar, which would result in similar ACL angles. This difference is incompletely accounted for if one measures only the FGA. There are few studies evaluating not only the tunnel angle but also the ACL angle between AM and TT techniques. Our study demonstrated that the graft angle is similar between the TT and AM techniques, as well as to the native ACL on the contralateral knee. We believe that the position of the tunnel aperture, and thus the graft angle, is more relevant to clinical outcomes than the angle of the tunnel. This should be measured in future comparative studies. In addition, measurement of the sagittal plane graft angle will reveal common errors in TT reconstruction, such as posterior placement of the tibial tunnel or vertical placement of the femoral tunnel, both of which create an increased graft angle in the sagittal plane.
Some meta-analyses and systematic reviews support the assertion that there are few clinical differences between the two femoral tunnel drilling techniques [4, 7, 10, 27, 31–34, 40, 45, 52]. However, results of other analyses conflict with that contention, showing AM superiority with higher proportions of negative Lachman and pivot–shift tests, and better Lysholm and International Knee Documentation Committee (IKDC) scores [6, 11, 30, 50]. Other reviews offer a more mixed picture, with AM providing superior IKDC subjective scores but similar IKDC objective scores and pivot–shift test, Lachman test, Lysholm, and Tegner activity scale scores [53]. In terms of graft failure, research has shown mixed results, with some studies suggesting no correlation between AM and TT techniques and others showing higher failure with AM technique [10, 38, 44, 45, 51]. This variation in results could be due to technical difficulties with the different techniques.
The technique modifications in the TT technique used to achieve anatomic tunnel placement are important to highlight and are supported by basic science data [36]. First, the starting point on the tibia must be located in a place that allows access to an anatomic position on the femur. This is highlighted by selection of 52° on the tibial guide, which corresponds to the native ACL angle. Second, the tibial tunnel position must be placed anatomically and more anterior to the locations traditionally described for the TT technique. This is best referenced using the native ACL stump. Posterior positioning of the tibial tunnel will result in a greater graft angle in the sagittal plane. Third, the discrepancy between the size of the tunnel and the diameter of the femoral offset guide can be taken advantage of to allow increased obliquity to access the lateral wall footprint position on the femur [36]. This is only applicable to tunnel sizes greater than 8 mm [2]. Last, the integrity of the tibial tunnel must be preserved during femoral tunnel reaming. The use of a half-fluted reamer to access the femur allows the reamer to enter to the joint without posteriorizing the tibial tunnel position [3].
This study is unique in that we were able to correlate both imaging and clinical outcomes in patients undergoing ACL reconstruction using an AM portal or an anatomic TT technique. In this study population, the TGA and ACL angles were similar between the AM and TT techniques, although the femoral tunnel angle was much smaller with the AM approach than with the TT approach. Clinical outcome scores were not different between the two groups. Therefore, it could be suggested that the skilled performance of these techniques—in which a tunnel aperture well approximated to the ACL anatomic footprint is ensured—is more important than the choice of technique [40].
In conclusion, anatomic ACL angle is restored after reconstruction with the TT and AM techniques, despite different FGAs. No significant difference in clinical outcome was noted between groups on physical examination or KOOS at 2 years post-operatively. These data suggest that TT reconstruction achieves a graft position similar to that with the AM technique and that location of the intra-articular tunnel aperture matters more than the orientation of the tunnel.
Compliance with Ethical Standards
Conflict of Interest
Austin V. Stone, MD, PhD; Jorge Chahla, MD, PhD; Brandon J. Manderle, MD; and Alexander Beletsky, BA, declare that they have no conflicts of interest. Charles A. Bush-Joseph, MD, reports editorial or governing board membership at the American Journal of Sports Medicine and American Orthopaedic Society for Sports Medicine, stock or stock options from Cresco Labs, and educational support from Medwest Associates, outside the submitted work. Nikhil N. Verma, MD, reports research support from Arthrex, Inc.; publishing royalties from Arthroscopy and Vindico Medical-Orthopedics Hyperguide; research support from DJ Orthopaedics and Orthospace; board or committee membership from the American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, and Arthroscopy Association of North America; editorial or governing board membership at Journal of Knee Surgery and SLACK Incorporated; stock or stock options from CyMedica and Omeros; and personal fees and stock or stock options from Minivasive, outside the submitted work.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was obtained from all patients for being included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Footnotes
Level of Evidence: Level IV: Prospective Comparative Cohort Study.
Work performed at: Midwest Orthopaedics at Rush
References
- 1.Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):194–199. doi: 10.1007/s001670100198. [DOI] [PubMed] [Google Scholar]
- 2.Bhatia S, Korth K, Van Thiel GS, et al. Effect of tibial tunnel diameter on femoral tunnel placement in transtibial single bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):51–57. doi: 10.1007/s00167-014-3307-8. [DOI] [PubMed] [Google Scholar]
- 3.Bhatia S, Korth K, Van Thiel GS, et al. Effect of reamer design on posteriorization of the tibial tunnel during endoscopic transtibial anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(6):1282–1289. doi: 10.1177/0363546513483534. [DOI] [PubMed] [Google Scholar]
- 4.Chalmers PN, Mall NA, Cole BJ, Verma NN, Bush-Joseph CA, Bach BR., Jr Anteromedial versus transtibial tunnel drilling in anterior cruciate ligament reconstructions: a systematic review. Arthroscopy. 2013;29(7):1235–1242. doi: 10.1016/j.arthro.2013.02.015. [DOI] [PubMed] [Google Scholar]
- 5.Chang CB, Choi JY, Koh IJ, Lee KJ, Lee KH, Kim TK. Comparisons of femoral tunnel position and length in anterior cruciate ligament reconstruction: modified transtibial versus anteromedial portal techniques. Arthroscopy. 2011;27(10):1389–1394. doi: 10.1016/j.arthro.2011.06.013. [DOI] [PubMed] [Google Scholar]
- 6.Chen H, Tie K, Qi Y, Li B, Chen B, Chen L. Anteromedial versus transtibial technique in single-bundle autologous hamstring ACL reconstruction: a meta-analysis of prospective randomized controlled trials. J Orthop Surg Res. 2017;12:167. doi: 10.1186/s13018-017-0671-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen Y, Chua KH, Singh A, et al. Outcome of single-bundle hamstring anterior cruciate ligament reconstruction using the anteromedial versus the transtibial technique: a systematic review and meta-analysis. Arthroscopy. 2015;31(9):1784–1794. doi: 10.1016/j.arthro.2015.06.001. [DOI] [PubMed] [Google Scholar]
- 8.Debandi A, Maeyama A, Hoshino Y, et al. The effect of tunnel placement on rotational stability after ACL reconstruction: evaluation with use of triaxial accelerometry in a porcine model. Knee Surg Sports Traumatol Arthrosc. 2013;21(3):589–595. doi: 10.1007/s00167-012-1961-2. [DOI] [PubMed] [Google Scholar]
- 9.Duffee A, Magnussen RA, Pedroza AD, Flanigan DC, Group M. Kaeding CC. Transtibial ACL femoral tunnel preparation increases odds of repeat ipsilateral knee surgery. J Bone Joint Surg Am. 2013;95(22):2035–2042. doi: 10.2106/JBJS.M.00187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Eysturoy NH, Nielsen TG, Lind MC. Anteromedial portal drilling yielded better survivorship of anterior cruciate ligament reconstructions when comparing recent versus early surgeries with this technique. Arthroscopy. 2019;35(1):182–189. doi: 10.1016/j.arthro.2018.08.030. [DOI] [PubMed] [Google Scholar]
- 11.Franceschi F, Papalia R, Rizzello G, Del Buono A, Maffulli N, Denaro V. Anteromedial portal versus transtibial drilling techniques in anterior cruciate ligament reconstruction: any clinical relevance? A retrospective comparative study. Arthroscopy. 2013;29(8):1330–1337. doi: 10.1016/j.arthro.2013.05.020. [DOI] [PubMed] [Google Scholar]
- 12.Fu FH, van Eck CF, Tashman S, Irrgang JJ, Moreland MS. Anatomic anterior cruciate ligament reconstruction: a changing paradigm. Knee Surg Sports Traumatol Arthrosc. 2015;23(3):640–648. doi: 10.1007/s00167-014-3209-9. [DOI] [PubMed] [Google Scholar]
- 13.Gavriilidis I, Motsis EK, Pakos EE, Georgoulis AD, Mitsionis G, Xenakis TA. Transtibial versus anteromedial portal of the femoral tunnel in ACL reconstruction: a cadaveric study. Knee. 15(5):364–367. [DOI] [PubMed]
- 14.Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;7(3):189–198. doi: 10.5435/00124635-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Guler O, Mahirogullari M, Mutlu S, Cerci MH, Seker A, Cakmak S. Graft position in arthroscopic anterior cruciate ligament reconstruction: anteromedial versus transtibial technique. Arch Orthop Trauma Surg. 2016;136(11):1571–1580. doi: 10.1007/s00402-016-2532-7. [DOI] [PubMed] [Google Scholar]
- 16.Hamrin Senorski E, Sundemo D, Murawski CD, et al. No differences in subjective knee function between surgical techniques of anterior cruciate ligament reconstruction at 2-year follow-up: a cohort study from the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3945–3954. doi: 10.1007/s00167-017-4521-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hantes ME, Dailiana Z, Zachos VC, Varitimidis SE. Anterior cruciate ligament reconstruction using the Bio-TransFix femoral fixation device and anteromedial portal technique. Knee Surg Sports Traumatol Arthrosc. 2006;14(5):497–501. doi: 10.1007/s00167-005-0705-y. [DOI] [PubMed] [Google Scholar]
- 18.Hantes ME, Zachos VC, Liantsis A, Venouziou A, Karantanas AH, Malizos KN. Differences in graft orientation using the transtibial and anteromedial portal technique in anterior cruciate ligament reconstruction: a magnetic resonance imaging study. Knee Surg Sports Traumatol Arthrosc. 2009;17(8):880–886. doi: 10.1007/s00167-009-0738-8. [DOI] [PubMed] [Google Scholar]
- 19.Harner CD, Fu FH, Irrgang JJ, Vogrin TM. Anterior and posterior cruciate ligament reconstruction in the new millennium: a global perspective. Knee Surg Sports Traumatol Arthrosc. 2001;9(6):330–336. doi: 10.1007/s001670100230. [DOI] [PubMed] [Google Scholar]
- 20.Harner CD, Honkamp NJ, Ranawat AS. Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy. 2008;24(1):113–115. doi: 10.1016/j.arthro.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 21.Hoenig JM, Heisey DM. The abuse of power: the pervasive fallacy of power calculations for data analysis. Am Stat. 2001;55(1):19–24. [Google Scholar]
- 22.Hussin EA, Aldaheri A, Alharbi H, Farouk HA. Modified transtibial versus anteromedial portal techniques for anterior cruciate ligament reconstruction, a comparative study. Open Access J Sports Med. 2018;9:199–213. doi: 10.2147/OAJSM.S157729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jennings JK, Leas DP, Fleischli JE, D’Alessandro DF, Peindl RD, Piasecki DP. Transtibial versus anteromedial portal ACL reconstruction: is a hybrid approach the best? Orthop J Sports Med. 2017;5(8):2325967117719857. doi: 10.1177/2325967117719857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Karlsson J, Irrgang JJ, van Eck CF, Samuelsson K, Mejia HA, Fu FH. Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 2: clinical application of surgical technique. Am J Sports Med. 2011;39(9):2016–2026. doi: 10.1177/0363546511402660. [DOI] [PubMed] [Google Scholar]
- 25.Kaseta MK, DeFrate LE, Charnock BL, Sullivan RT, Garrett WE., Jr Reconstruction technique affects femoral tunnel placement in ACL reconstruction. Clin Orthop Relat Res. 2008;466(6):1467–1474. doi: 10.1007/s11999-008-0238-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lee DW, Kim JG, Lee JH, Park JH, Kim DH. Comparison of modified transtibial and outside-in techniques in anatomic single-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2018;34(10):2857–2870. doi: 10.1016/j.arthro.2018.05.041. [DOI] [PubMed] [Google Scholar]
- 28.Lee MC, Seong SC, Lee S, et al. Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction. Arthroscopy. 2007;23(7):771–778. doi: 10.1016/j.arthro.2007.04.016. [DOI] [PubMed] [Google Scholar]
- 29.Levine M, Ensom MH. Post hoc power analysis: an idea whose time has passed? Pharmacotherapy. 2001;21(4):405–409. doi: 10.1592/phco.21.5.405.34503. [DOI] [PubMed] [Google Scholar]
- 30.Liu A, Sun M, Ma C, et al. Clinical outcomes of transtibial versus anteromedial drilling techniques to prepare the femoral tunnel during anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2017;25(9):2751–2759. doi: 10.1007/s00167-015-3672-y. [DOI] [PubMed] [Google Scholar]
- 31.Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o’clock and 10 o’clock femoral tunnel placement. 2002 Richard O’Connor Award paper. Arthroscopy. 2003;19(3):297–304. doi: 10.1053/jars.2003.50084. [DOI] [PubMed] [Google Scholar]
- 32.MacDonald P, Kim C, McRae S, Leiter J, Khan R, Whelan D. No clinical differences between anteromedial portal and transtibial technique for femoral tunnel positioning in anterior cruciate ligament reconstruction: a prospective randomized, controlled trial. Knee Surg Sports Traumatol Arthrosc. 2018;26(5):1335–1342. doi: 10.1007/s00167-017-4664-x. [DOI] [PubMed] [Google Scholar]
- 33.Mulcahey MK, David TS, Epstein DM, Alaia MJ, Montgomery KD. Transtibial versus anteromedial portal anterior cruciate ligament reconstruction using soft-tissue graft and expandable fixation. Arthroscopy. 201430(11):1461–1467. [DOI] [PubMed]
- 34.Özer M, Özer H, Selek H, et al. Radiological and functional comparison of single-bundle anterior cruciate ligament reconstruction: transtibial versus anteromedial technique. Turk J Med Sci. 2018;48(3):455–461. doi: 10.3906/sag-1702-119. [DOI] [PubMed] [Google Scholar]
- 35.Pascual-Garrido C, Swanson BL, Swanson KE. Transtibial versus low anteromedial portal drilling for anterior cruciate ligament reconstruction: a radiographic study of femoral tunnel position. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):846–850. doi: 10.1007/s00167-012-1988-4. [DOI] [PubMed] [Google Scholar]
- 36.Piasecki DP, Bach BR, Jr, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011;39(6):1306–1315. doi: 10.1177/0363546510397170. [DOI] [PubMed] [Google Scholar]
- 37.Pinczewski LA, Salmon LJ, Jackson WF, von Bormann RB, Haslam PG, Tashiro S. Radiological landmarks for placement of the tunnels in single-bundle reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br. 2008;90(2):172–179. doi: 10.1302/0301-620X.90B2.20104. [DOI] [PubMed] [Google Scholar]
- 38.Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind MC. Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: results from the Danish Knee Ligament Reconstruction Register. Arthroscopy. 2013;29(1):98–105. doi: 10.1016/j.arthro.2012.09.009. [DOI] [PubMed] [Google Scholar]
- 39.Rayan F, Nanjayan SK, Quah C, Ramoutar D, Konan S, Haddad FS. Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J Orthop. 2015;6(2):252–262. doi: 10.5312/wjo.v6.i2.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rezazadeh S, Ettehadi H, Vosoughi AR. Outcome of arthroscopic single-bundle anterior cruciate ligament reconstruction: anteromedial portal technique versus transtibial drilling technique. Musculoskelet Surg. 2016;100(1):37–41. doi: 10.1007/s12306-015-0392-x. [DOI] [PubMed] [Google Scholar]
- 41.Riboh JC, Hasselblad V, Godin JA, Mather RC., 3rd Transtibial versus independent drilling techniques for anterior cruciate ligament reconstruction: a systematic review, meta-analysis, and meta-regression. Am J Sports Med. 2013;41(11):2693–2702. doi: 10.1177/0363546513506979. [DOI] [PubMed] [Google Scholar]
- 42.Scopp JM, Jasper LE, Belkoff SM, Moorman CT., 3rd The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004;20(3):294–299. doi: 10.1016/j.arthro.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 43.Simmons R, Howell SM, Hull ML. Effect of the angle of the femoral and tibial tunnels in the coronal plane and incremental excision of the posterior cruciate ligament on tension of an anterior cruciate ligament graft: an in vitro study. J Bone Joint Surg Am. 2003;85(6):1018–1029. doi: 10.2106/00004623-200306000-00006. [DOI] [PubMed] [Google Scholar]
- 44.Svantesson E, Sundemo D, Hamrin Senorski E, et al. Double-bundle anterior cruciate ligament reconstruction is superior to single-bundle reconstruction in terms of revision frequency: a study of 22,460 patients from the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3884–3891. doi: 10.1007/s00167-016-4387-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Tejwani SG, Prentice HA, Wyatt RWB, Jr, Maletis GB. Femoral tunnel drilling method: risk of reoperation and revision after anterior cruciate ligament reconstruction. Am J Sports Med. 2018;46(14):3378–3384. doi: 10.1177/0363546518805086. [DOI] [PubMed] [Google Scholar]
- 46.Tompkins M, Cosgrove CT, Milewski MD, Brockmeier SF, Hart JM, Miller MD. Anterior cruciate ligament reconstruction femoral tunnel characteristics using an accessory medial portal versus traditional transtibial drilling. Arthroscopy. 2013;29(3):550–555. doi: 10.1016/j.arthro.2012.10.030. [DOI] [PubMed] [Google Scholar]
- 47.Tudisco C, Bisicchia S. Drilling the femoral tunnel during ACL reconstruction: transtibial versus anteromedial portal techniques. Orthopedics. 2012;35(8):e1166–e1172. doi: 10.3928/01477447-20120725-14. [DOI] [PubMed] [Google Scholar]
- 48.Venosa M, Delcogliano M, Padua R, Alviti F, Delcogliano A. Femoral tunnel positioning in anterior cruciate ligament reconstruction: anteromedial portal versus transtibial technique—a randomized clinical trial. Joints. 2017;5(1):34–38. doi: 10.1055/s-0037-1601413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Vignos MF, Kaiser JM, Baer GS, Kijowski R, Thelen DG. American Society of Biomechanics Clinical Biomechanics Award 2017: non-anatomic graft geometry is linked with asymmetric tibiofemoral kinematics and cartilage contact following anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon). 2018;56:75–83. doi: 10.1016/j.clinbiomech.2018.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wang H, Fleischli JE, Zheng NN. Transtibial versus anteromedial portal technique in single-bundle anterior cruciate ligament reconstruction: outcomes of knee joint kinematics during walking. Am J Sports Med. 2013;41(8):1847–1856. doi: 10.1177/0363546513490663. [DOI] [PubMed] [Google Scholar]
- 51.Yabroudi MA, Björnsson H, Lynch AD, et al. Predictors of revision surgery after primary anterior cruciate ligament reconstruction. Orthop J Sports Med. 2016;4(9):2325967116666039. doi: 10.1177/2325967116666039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Youm YS, Cho SD, Lee SH, Youn CH. Modified transtibial versus anteromedial portal technique in anatomic single-bundle anterior cruciate ligament reconstruction: comparison of femoral tunnel position and clinical results. Am J Sports Med. 2014;42(12):2941–2947. doi: 10.1177/0363546514551922. [DOI] [PubMed] [Google Scholar]
- 53.Zhang Q, Kou Y. Yuan Z. A meta-analysis on anterior cruciate ligament reconstruction: is modified transtibial technique inferior to independent drilling techniques? Exp Ther Med. 2018;16(3):1790–1799. doi: 10.3892/etm.2018.6395. [DOI] [PMC free article] [PubMed] [Google Scholar]